Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
|
|
|
- Delphia Morton
- 5 years ago
- Views:
Transcription

1 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018

2 Financial and Other Disclosures Off-label use of drugs, devices, or other agents: None or FILL IN HERE; including your local regulatory agency, such as FDA, EMA, etc. Data from IRB-approved human research is presented [or state: is not ] I have the following financial interests or relationships to disclose: Pfizer Roche Genentech Ipsen Novartis BMS Disclosure code C, S C C C C C 2


3 CARMENA investigated the role of CN SURTIME the sequence of CN
4 SURTIME and CARMENA included patients who require sunitinib Time to targeted therapy in patients with low-volume but non-resectable metastatic disease after CN N=28 from an institutional database of 202 primary mrcc patients Median timo to TT 14 months Bex et al., GU ASCO, J Clin Oncol 34, 2016 (suppl 2S; abstr 604)
5 Study design R Immediate Nephrectomy Deferred Nephrectomy N E P H R E C T O M Y Cycle 1 (6 wk) Cycle 2 Cycle 3 Cycle 4 Progression status at week 16 Cycle 1 (6 wk) Cycle 2 N E P H R E C T Cycle 3 (4 wk) O M Y Progression status at week 28 Cycle 4 Cycle 5 Progression status every 12 weeks = Sunitinib = Progression status 4 weeks after CN 5
6 Baseline characteristics Immediate nephrectomy (N=50) Deferred nephrectomy (N=49) Median age (years) Performance status (WHO) - WHO 0 36 (72.0%) 31 (63.3%) - WHO 1 14 (28.0%) 18 (36.7%) Male 41 (82.0%) 39 (79.6%) MSKCC intermediate risk 43 (86.0%) 44 (89.8%) 2 measurable metastatic sites 43 (86.0%) 46 (93.9%) Mean (SD) primary tumor size (mm) 93.1 (37.8) 96.8 (31.3) 6
7 Week 16 evaluation (+/-15 days window) Week 28 evaluation (+/-15 days window) Progression-free survival (ITT) HR (95%CI)=0.88 (0.56, 1.37), p=0.569 Stratified by WHO performance status (0 versus 1) Progression-free status at w28 (±15 days) Immediate nephrectomy (N=50) Deferred nephrectomy (N=49) Progression-free at week (42.0%) 21 (42.9%) Deferred [95% CI] [28.2% 56.8%] [28.8% 57.8%] p-value (one-sided Fisher exact test) 0.61 Immediate Progression week 28 or treatment failure 25 (50.0%) 24 (49.0%) Not assessable 4 (8.0%) 4 (8.2%) 7
 Immediate nephrectomy (N=50) Deferred nephrectomy (N=49) Survival status Dead 35 (70.0) 28 (57.")
8 Overall Survival (ITT) Immediate Deferred HR (95%CI)=0.57 (0.34, 0.95), p=0.032 Stratified by WHO performance status (0 versus 1) Immediate nephrectomy (N=50) Deferred nephrectomy (N=49) Survival status Dead 35 (70.0) 28 (57.1) Reason of death Progression Surgery related toxicity 1 0 Progression and surgery related toxicity 1 0 Cardiovascular disease (not due to toxicity or progression) 1 0 Other (not due to toxicity or progression) 1 0 Unknown 1 3 8
9 Overall survival after week 16 (%) Overall Survival Landmark analysis at week PD before w16 No PD before w Months Patients-at-Risk Excluded- Immediate Deferred Immediate Deferred Assessment of progression status at week 16 prior to planned CN in the deferred arm 9

10 Patient disposition Presented By Arnaud Mejean at 2018 ASCO Annual Meeting

11 Patient characteristics (1) Presented By Arnaud Mejean at 2018 ASCO Annual Meeting

12 Overall <br />survival (ITT) Presented By Arnaud Mejean at 2018 ASCO Annual Meeting

13 Overall survival (ITT) Presented By Arnaud Mejean at 2018 ASCO Annual Meeting

14 Overall survival by patient population Presented By Arnaud Mejean at 2018 ASCO Annual Meeting

15 Secondary nephrectomy in Arm B (sunitinib alone) Presented By Arnaud Mejean at 2018 ASCO Annual Meeting
16 Conclusions from both SURTIME and CARMENA Despite its limitations, CARMENA is a practice changing trial and SURTIME complements the results Patients with poor risk MSKCC should not undergo CN Patients with intermediate MSKCC risk who require systemic therapy should not undergo immediate CN but receive sunitinib first
17 Finally, open questions remain Should CN be performed at a later stage in all patients except those who progress (SURTIME) or only when necessary (CARMENA)? First-line therapy with nivolumab plus ipilimumab will replace sunitinib for intermediate and poor risk patients. Will we need new studies or treat patients with primary metastatic RCC with the tumour in place followed by resection when necessary?
18 OS probability Immune checkpoint inhibitors have changed the RCC treatment landscape CheckMate-025: Nivolumab vs everolimus in second-line mrcc Real-world setting in n=264 Dutch patients from a 2 nd -line nivolumab registry Overall survival Median OS, months (95% CI) Nivolumab (n=410): 25.0 (21.8 NE) Everolimus (n=411): 19.6 ( ) HR 0.73 (98.5% Cl ) P= Time, months CI, confidence interval; HR, hazard ratio; NE, not estimable; OS, overall survival; PFS, progression-free survival. Motzer RJ et al. N Engl J Med. 2015;373: , Verhaart et a., ASCO 1-5 June, 2018
19 Checkpoint inhibitor combination trials in first-line an embarassment of riches Study Sponsor N Therapy Endpoint Subtype MK Merck Sharp & Dohme 840 Pembrolizumab 200 mg IV Q3W PLUS axitinib PFS central 5 mg PO BID review 426/KEYNOTE-426 vs OS NCT ¹ sunitinib 50 mg PO QD 4/2 weeks JAVELIN Renal 101 NCT ¹ Pfizer 583 Avelumab administered at 10 mg/kg IV Q2W in combination with axitinib, 5 mg PO BID vs sunitinib given at 50 mg PO QD 4/2 weeks PFS, OS clear cell component with or without sarcomatoid features clear cell component NCT ¹ Hoffmann-La Roche 900 Atezolizumab as a fixed dose of 1200 mg via IV infusion on days 1 and 22 of each 42-day plus bevacizumab 15 mg/kg via IV infusion on days 1 and 22 of each 42-day cycle vs sunitinib given at 50 mg PO QD 4/2 weeks Checkmate 214 NCT ¹ Bristol-Myers Squibb 1070 Nivolumab 3 mg/kg combined with ipilimumab 1 mg/kg solutions IV Q3W for 4 doses then nivolumab 3 mg/kg solutions IV Q2W vs sunitinib given at 50 mg PO QD 4/2 weeks NCT ¹ Eisai Inc. 735 Lenvatinib 18 mg PO QD, plus everolimus 5 mg PO, QD or lenvatinib 20 mg PO QD, plus pembrolizumab 200 mg IV, Q3W vs sunitinib 50 mg PO QD 4/2 weeks PFS investigator reviewed OS in participants with detectable PD- L1 PFS OS PFS, OS clear cell histology and/or a component of sarcomatoid carcinoma clear-cell component clear-cell component Checkmate 9ER NCT Bristol-Myers Squibb 1014 Nivolumab 3 mg/kg combined with ipilimumab 1 mg/kg solutions IV and cabozantinib (triplet) vs nivolumab 3 mg/kg solutions IV and cabozantinib vs sunitinib given at 50 mg PO QD 4/2 weeks PFS, OS clear-cell component

20 UPDATED EAU GUIDELINES RECOMMENDATIONS FOR THE TREATMENT OF FIRST-LINE METASTATIC CLEAR-CELL RENAL CANCER.
21
22

23 Immune combination leads to a high complete response rate
 and ORR and PFS in favorable risk")
24 OS in the ITT (including favorable IMDC risk) and ORR and PFS in favorable risk

25 OS data of CheckMate 214 per PD-L1 status Slide 26 Presented by Motzer et al., SITC 2017

26 Immotion 151 trial of atezolizumab plus bevacizumab versus sunitinib in patients with clear-cell or sarcomatoid mrcc Study Design

27 Baseline Characteristics CheckMate 214 included by IMDC risk factors of which 23 % favorable, 61% intermediate and 17% poor risk Presented By Robert Motzer at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
28 Progression-Free Survival in PD-L1+ Presented By Robert Motzer at 2018 Genitourinary Cancers Symposium

29 PFS and ORR by IRC Presented By Robert Motzer at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
30 Overall Survival in ITT Presented By Robert Motzer at 2018 Genitourinary Cancers Symposium

31 Treatment-related AEs<br /> 20% frequency in either arm and > 5% difference between arms Presented By Robert Motzer at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care

32 PD-1 Blockade Based Combinations in mrcc:<br />Are they Additive or Synergistic? Presented By David McDermott at 2018 Genitourinary Cancers Symposium: Translating Evidence to Multidisciplinary Care
33 Results in context CheckMate 214 and IMmotion 151 used different PD- L1 IHC staining OS benefit in CheckMate 214 independent of PD-L1 tumour expression IMmotion 151 lacks mature OS data and no significant PFS difference across all PD-L1 groups in IRC



34 Immotion 150 biomarker analysis Transscriptome map of angiogenesis and immuneassociated genes in RCC McDermott et al., AACR 2017

35 Sunitinib Demonstrated Improved PFS in AngiogenesisHigh Subset vs AngiogenesisLow Subset

")
36 Molecular subtypes of clear cell RCC are associated with sunitinib response in the metastatic setting ccrcc1/ccrcc4 tumors: lower RR, shorter PFS and OS than ccrcc2/ccrcc3 tumors (P = 0.005, and , respectively) when treated with sunitinib. ccrcc4: strong inflammatory, Th1-oriented but suppressive immune microenvironment, with high expression of PDCD1 (PD-1) and its ligands Beuselinck et al., Clin Cancer Res 2015; Escudier et al, 2018 Genitourinary Cancers Symposium
37 Conclusion If no drug-related contraindications present the IMDC prognostic model is currently the only tool for patient selection based on higher level of evidence Tumor or immune-cell PD-L1 expression reveal trends but checkpoint inhibition is effective irrespective of expression Angiogenic or immune-inflammatory genotypes are emerging but have not been tested in phase 3 Clinical subgroup analysis is interesting but cross-trial comparisons should not be done
38 Metastatic Urothelial cancer (UCC) chemotherapy Gemcitabine/Cisplatin vs MVAC (MTX/Vinblastine/Doxorubicine/Ci splatin) standard MVAC vs accelerated MVAC J Clin Oncol; 23 (2005) Eur J Can 42:50 (2006)
39 Platinum-refractory UCC Vinflunine vs Best Supportive Care Bellmunt J et al. JCO 2009;27:
40 EAU MMIBC Update

41 Feb 2016 After platinum-treatment: Response rate 15%
 Stratification Factors No. of risk factors b (0 vs. 1/2/3) Liver metastases (yes vs.")
42 Key Eligibility Criteria a muc with progression during or following platinum-based chemotherapy 2 prior lines of therapy Measurable disease per RECIST v1.1 ECOG PS 0-1 Evaluable sample for PD-L1 testing TCC histology as primary component (N = 931) Stratification Factors No. of risk factors b (0 vs. 1/2/3) Liver metastases (yes vs. no) PD-L1 status (0/1 vs. 2/3) Chemotherapy (vinflunine vs. taxanes) R 1:1 Atezolizumab 1200 mg q3w Chemotherapy (investigator s choice) Vinflunine q3w Docetaxel q3w Paclitaxel q3w Loss of clinical benefit No crossover permitted per protocol RECIST v1.1 progression Survival followup
 12-mo OS Rate (95% CI) 46% (37, 56) 80 Chemothera py 88/118 10.6 mo (8.4, 12.2) 41% (32, 50) 60 40 20 0 No. at Risk Atezolizum ab Chemother apy HR = 0.87 (95% CI: 0.63, 1.21) P = 0.")
43 Overall Survival Powles T, et al. EAS 2017, Lancet IMvigor211. OS Analysis: PDL1 IC2/3 (Prim endpoint) 100 Atezolizuma b Events / Patient s Median OS (95% CI) 72/ mo (8.6, 15.5) 12-mo OS Rate (95% CI) 46% (37, 56) 80 Chemothera py 88/ mo (8.4, 12.2) 41% (32, 50) No. at Risk Atezolizum ab Chemother apy HR = 0.87 (95% CI: 0.63, 1.21) P = Months
44 Overall Survival OS Analysis: ITT Population 100 Events / Patient s Median OS (95% CI) 12-mo OS Rate (95% CI) Atezolizuma b Chemothera py 324/ / mo (7.8, 9.6) 8.0 mo (7.2, 8.6) 39% (35, 44) 32% (28, 37) HR = 0.85 (95% CI: 0.73, 0.99) P = Months No. at Risk Atezolizumab Chemotherapy Median follow-up duration in ITT population: 17.3 mo (range, 0 to 24.5 mo) Powles T, et al. EAS 2017, Lancet IMvigor211.

45 KEYNOTE-045: Pembrolizumab vs Investigator s choice chemo Bellmunt J, et al, NEJM 2017; ASCO-GU 2018

46 Metastatic UCC - cisplatin-ineligible ORR 41 vs 30% PFS 5.8 vs 4.2 months OS 9.3 vs 8.1 months

47 Jan 2017 Cisplatinineligible: Response rate 24%

48 Biomarker Findings and Mature Clinical Results From KEYNOTE-052: First-Line Pembrolizumab in Cisplatin-ineligible Advanced Urothelial Cancer Presented By Peter O''Donnell at 2017 ASCO Annual Meeting

49 Confirmed Objective Response Rate
50 ± anti-ctla4 ± chemotherapy Trial Ongoing studies first line Design Number of patients Primary endpoint(s) IMvigor130 (NCT ) R Atezolizumab Atezolizumab + platinum/gemcitabine Platinum/gemcitabine + placebo 1200 PFS, OS KEYNOTE-361 Pembrolizumab (NCT ) 990 PFS, OS Pembrolizumab + R platinum/gemcitabine Platinum/gemcitabine + placebo DANUBE (NCT ) R Durvalumab Durvalumab + tremelimumab Platinum/gemcitabine 1000 PFS, OS CheckMate 901 (NCT ) R Nivolumab + ipilimumab Platinum/gemcitabine + placebo 735 PFS, OS
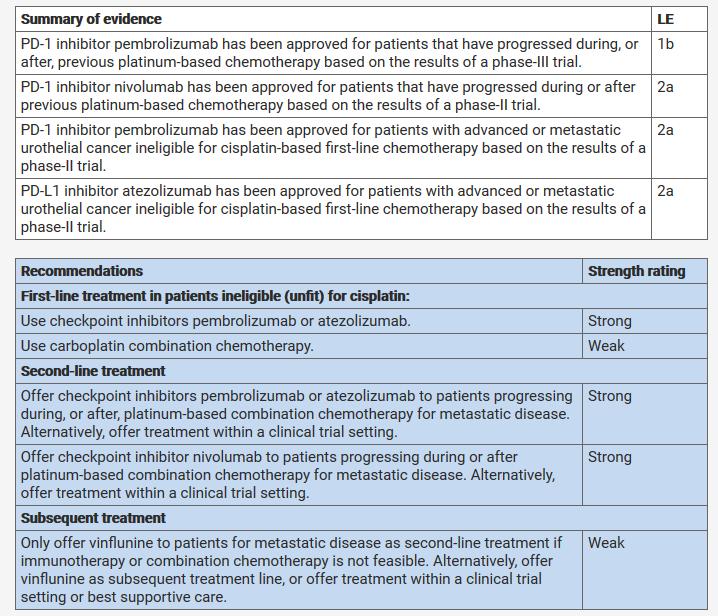
51 Conclusion EMA and FDA approved pembrolizumab and atezolizumab based on phase 2 data for cisplatin ineligble patients. However, in ongoing studies these patients had poorer outcome in unselected populations than on chemotherapy. This resulted in changing the EMA and FDA label for PD-L1 positives. PD-L1 selection is controversial: no association with pembro in 2 nd line whereas it was the reverse for atezolizumab Based on phase I/II and phase Ib trials, durvalumab and avelumab (PD-1/PD-L1 inhibitors) are currently only approved for this indication in the United States
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Immunotherapy for the Treatment of Kidney and Bladder Cancer
 Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY FOR THE RIGHT PATIENT
 Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA. Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA
 UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
Challenging Genitourinary Tumors: What s New in 2017
 Challenging Genitourinary Tumors: What s New in 2017 David J. Vaughn, MD Genitourinary Medical Oncology Professor Please note that some of the studies reported in this presentation were presented as an
Challenging Genitourinary Tumors: What s New in 2017 David J. Vaughn, MD Genitourinary Medical Oncology Professor Please note that some of the studies reported in this presentation were presented as an
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
I Kid(ney) You Not: Updates on Renal Cell Carcinoma
 You Not: Updates on Renal Cell Carcinoma") Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Innovaciones en el tratamiento del ca ncer renal. Enrique Grande
 Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
NEXT GENERATION DRUGS IN KIDNEY CANCER. Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden
 NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Renal Cell Carcinoma: Navigating a Maze of Choices
 Renal Cell Carcinoma: Navigating a Maze of Choices Sumanta Kumar Pal, M.D. Associate Professor Department of Medical Oncology & Experimental Therapeutics Co-Director, Kidney Cancer Program City of Hope
Renal Cell Carcinoma: Navigating a Maze of Choices Sumanta Kumar Pal, M.D. Associate Professor Department of Medical Oncology & Experimental Therapeutics Co-Director, Kidney Cancer Program City of Hope
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Immunotherapy for Genitourinary Cancers
 Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia
 Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia New target, new agent (James Brugarolas) Atezolizumab + Bevacizumab and PD-L1
Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia New target, new agent (James Brugarolas) Atezolizumab + Bevacizumab and PD-L1
Renal Cell Cancer: Present and Future. Bernard Escudier, Gustave Roussy
 Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request Disclosures
Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request Disclosures
Recent Advances in Lung Cancer: Updates from ASCO Updates from ESMO, AACR and ASCO
 Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Recent Advances in Lung Cancer: Updates from ASCO 2018 Updates from ESMO, AACR and ASCO Charu Aggarwal, MD, MPH Assistant Professor of Medicine Division of Hematology-Oncology Abramson Cancer Center University
Metastatic renal cancer (mrcc): Evidence-based treatment
: Evidence-based treatment") Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Advanced Bladder Cancer: Check Mate or Check Point Inhibitors
 Advanced Bladder Cancer: Check Mate or Check Point Inhibitors Daniel P Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow
Advanced Bladder Cancer: Check Mate or Check Point Inhibitors Daniel P Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow
Lung Cancer Immunotherapy
 Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Challenges in systemic treatment for metastatic bladder cancer. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Challenges in systemic treatment for metastatic bladder cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University OS PCG 15.8 vs GC 12.7 NS Cisplatin ineligible Second-line chemotherapy
Challenges in systemic treatment for metastatic bladder cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University OS PCG 15.8 vs GC 12.7 NS Cisplatin ineligible Second-line chemotherapy
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game?
 Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Disclosure. Astellas. Research funding. Advisory board (to institute) Roche/Genentech Astra Zeneca/Medimmune Astellas
 Roche/Genentech Astra Zeneca/Medimmune Astellas") Disclosure Activity Company Research funding Advisory board (to institute) Astellas Roche/Genentech Astra Zeneca/Medimmune Astellas Immunotherapy for urothelial cell carcinoma A NEW HOPE Michiel van der
Disclosure Activity Company Research funding Advisory board (to institute) Astellas Roche/Genentech Astra Zeneca/Medimmune Astellas Immunotherapy for urothelial cell carcinoma A NEW HOPE Michiel van der
Media Release. Basel, 6 th February 2018
 Media Release Basel, 6 th February 2018 Phase III IMmotion151 study showed Roche's TECENTRIQ (atezolizumab) and Avastin (bevacizumab) reduced the risk of disease worsening or death by 26 percent in certain
Media Release Basel, 6 th February 2018 Phase III IMmotion151 study showed Roche's TECENTRIQ (atezolizumab) and Avastin (bevacizumab) reduced the risk of disease worsening or death by 26 percent in certain
Sequencing of therapies in mrcc. Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC
 Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Integrating novel therapy in advanced renal cell carcinoma
 Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Integrating Immunotherapy into Urologic Oncology: The New Urothelial Cancer Paradigm
 Immunotherapy in Urothelial Cancer: Where are We Now & Where are We Going? Arjun Balar, MD Director of Genitourinary Medical Oncology Program NYU Langone Medical Center New York, NY Bladder Cancer Therapeutic
Immunotherapy in Urothelial Cancer: Where are We Now & Where are We Going? Arjun Balar, MD Director of Genitourinary Medical Oncology Program NYU Langone Medical Center New York, NY Bladder Cancer Therapeutic
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Bristol-Myers Squibb. Request for Educational Activity (RFE)
") Bristol-Myers Squibb Independent Medical Education Request for Educational Activity (RFE) Date RFP Code Therapeutic Area Areas of Interest Educational Design Intended Audience Budget Accreditation Geographic
Bristol-Myers Squibb Independent Medical Education Request for Educational Activity (RFE) Date RFP Code Therapeutic Area Areas of Interest Educational Design Intended Audience Budget Accreditation Geographic
Urothelial Carcinoma Highlights
 Urothelial Carcinoma Highlights Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano European Association of Urology Research Foundation Disclosures Consulting or Advisory Role: Company:
Urothelial Carcinoma Highlights Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano European Association of Urology Research Foundation Disclosures Consulting or Advisory Role: Company:
Tumori Genito-Urinari. Fabio Calabrò Oncologia Medica Azienda Ospedaliera San Camillo Forlanini
 Tumori Genito-Urinari Fabio Calabrò Oncologia Medica Azienda Ospedaliera San Camillo Forlanini Prostate cancer treatment paradigm is evolving PROSTATE CANCER TREATMENT PARADIGMIS EVOLVING Non metatasticcrpc
Tumori Genito-Urinari Fabio Calabrò Oncologia Medica Azienda Ospedaliera San Camillo Forlanini Prostate cancer treatment paradigm is evolving PROSTATE CANCER TREATMENT PARADIGMIS EVOLVING Non metatasticcrpc
Immunotherapy in GU Cancers. Dr Ravindran Kanesvaran Medical Oncologist National Cancer Centre Singapore
 Immunotherapy in GU Cancers Dr Ravindran Kanesvaran Medical Oncologist National Cancer Centre Singapore 1 Disclosures Speaker Bureau: Pfizer, J&J, Sanofi, Novartis, MSD Advisory Board/ Consultant: GSK,
Immunotherapy in GU Cancers Dr Ravindran Kanesvaran Medical Oncologist National Cancer Centre Singapore 1 Disclosures Speaker Bureau: Pfizer, J&J, Sanofi, Novartis, MSD Advisory Board/ Consultant: GSK,
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea
 Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Evan J. Lipson, M.D.
 Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Urothelial Cancers- New Strategies. Sandy Srinivas.MD Stanford University
 Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients
 A Phase II Study of With or Without Bevacizumab vs in Untreated Metastatic Renal Cell Carcinoma Patients David McDermott, 1 Michael Atkins, 2 Robert Motzer, 3 Brian Rini, 4 Bernard Escudier, 5 Lawrence
A Phase II Study of With or Without Bevacizumab vs in Untreated Metastatic Renal Cell Carcinoma Patients David McDermott, 1 Michael Atkins, 2 Robert Motzer, 3 Brian Rini, 4 Bernard Escudier, 5 Lawrence
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO
 AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO Montse Domènech Althaia, Xarxa Assistencial i Universitària Manresa Urothelial Cancer Therapeutics FDA approved drugs for bladder
AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO Montse Domènech Althaia, Xarxa Assistencial i Universitària Manresa Urothelial Cancer Therapeutics FDA approved drugs for bladder
Renal Cell (RCC) and Bladder Carcinoma (TCC)
 and Bladder Carcinoma (TCC)") Renal Cell (RCC) and Bladder Carcinoma (TCC) Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Disclosures Compensated lectures: BMS, Ipsen,
Renal Cell (RCC) and Bladder Carcinoma (TCC) Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Disclosures Compensated lectures: BMS, Ipsen,
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Disclosures. Immunotherapyin Head & NeckCancer. Actual landscape of systemic treatment in HNSCC. Head andneckcanceris an immunogeneic tumor
 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Cytoreductive Nephrectomy
 Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Advances in the Treatment of Renal Cell Carcinoma
 Advances in the Treatment of Renal Cell Carcinoma Developed in collaboration Learning Objectives Upon completion, participants should be able to: Identify patients with metastatic renal cell carcinoma
Advances in the Treatment of Renal Cell Carcinoma Developed in collaboration Learning Objectives Upon completion, participants should be able to: Identify patients with metastatic renal cell carcinoma
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients
 Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Tratamiento adyuvante y neoadyuvante del cáncer renal en Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet.
 Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Atezolizumab Adjuvant Study: Medical Oncologist Perspective. Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center
 Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial
: Results of a phase I trial") Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
IMMUNE CHECKPOINT BLOCKADE IN UROTHELIAL CANCER
 IMMUNE CHECKPOINT BLOCKADE IN UROTHELIAL CANCER Elizabeth R. Plimack MD MS Director, Genitourinary Clinical Research Associate Professor, Hematology/Oncology Fox Chase Cancer Center, Temple Health Neoadjuvant
IMMUNE CHECKPOINT BLOCKADE IN UROTHELIAL CANCER Elizabeth R. Plimack MD MS Director, Genitourinary Clinical Research Associate Professor, Hematology/Oncology Fox Chase Cancer Center, Temple Health Neoadjuvant
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Debaters For The Evening:
 Your Debaters For The Evening: Current State of Immune Checkpoint Blockade in Selected Types of Solid Tumors Jeffery Weber, MD, PhD Naiyer A. Rizvi, MD Current State of ICI in Melanoma and Bladder Cancers
Your Debaters For The Evening: Current State of Immune Checkpoint Blockade in Selected Types of Solid Tumors Jeffery Weber, MD, PhD Naiyer A. Rizvi, MD Current State of ICI in Melanoma and Bladder Cancers
Highlights STOMACH CANCER
 UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
UPDATES and NEWS from the Gastrointestinal Cancers Symposium in San Francisco Roma, 10-11 Febbraio 2017 Highlights STOMACH CANCER Lorenzo Fornaro, MD Unit of Medical Oncology 2 Azienda Ospedaliero-Universitaria
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
The Therapeutic Landscape in Advanced Renal Cell Carcinoma
 The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
Linee guida terapeutiche oncologiche. Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona
 Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA
 IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA Kathleen Mahoney, M.D., Ph.D. Instructor of Medicine, Harvard Medical School Attending, Beth Israel Deaconess
IMMUNE CHECKPOINT THERAPY FOR GENITOURINARY CANCERS: KIDNEY CANCER AND TRANSITIONAL CELL CARCINOMA Kathleen Mahoney, M.D., Ph.D. Instructor of Medicine, Harvard Medical School Attending, Beth Israel Deaconess
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER
 PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients
 A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients Viktor Grünwald, 1 David McDermott, 2 Michael Atkins, 3 Robert Motzer, 4
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients Viktor Grünwald, 1 David McDermott, 2 Michael Atkins, 3 Robert Motzer, 4
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Alternativas de Futuro en Cáncer Renal Enrique Grande
 Alternativas de Futuro en Cáncer Renal Enrique Grande Hospital Ramón y Cajal de Madrid The ncreasingly Challenging Field of mrcc Sorafenib (US 2005, EU 2006) 3,4 Sunitinib (US & EU 2006) 3,4 Early 1940s:
Alternativas de Futuro en Cáncer Renal Enrique Grande Hospital Ramón y Cajal de Madrid The ncreasingly Challenging Field of mrcc Sorafenib (US 2005, EU 2006) 3,4 Sunitinib (US & EU 2006) 3,4 Early 1940s:
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018
 Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Optimizing treatment for metastatic bladder cancer in chemotherapy-resistant urothelial carcinoma. Moran Gadot M.D SHEBA Medical Center ISRAEL
 Optimizing treatment for metastatic bladder cancer in chemotherapy-resistant urothelial carcinoma Moran Gadot M.D SHEBA Medical Center ISRAEL Disclosures none All (eligible) patients should get chemotherapy
Optimizing treatment for metastatic bladder cancer in chemotherapy-resistant urothelial carcinoma Moran Gadot M.D SHEBA Medical Center ISRAEL Disclosures none All (eligible) patients should get chemotherapy
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy
: Biomarkers for Immunotherapy") Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Roche presents updated results for investigational cancer immunotherapy atezolizumab in advanced bladder cancer
 Media Release Basel, 8 January 2016 Roche presents updated results for investigational cancer immunotherapy atezolizumab in advanced bladder cancer Higher expression of PD-L1 (programmed death-ligand 1)
Media Release Basel, 8 January 2016 Roche presents updated results for investigational cancer immunotherapy atezolizumab in advanced bladder cancer Higher expression of PD-L1 (programmed death-ligand 1)
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations
 Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration