OVERVIEW OF THE DIAGNOSIS AND TREATMENT OF GI NETS
|
|
|
- Theresa Murphy
- 5 years ago
- Views:
Transcription
1 OVERVIEW OF THE DIAGNOSIS AND TREATMENT OF GI NETS Dr Christos G. Toumpanakis MD PhD FRCP FEBGH Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University College of London Neuroendocrine Tumour Unit - ENETS Centre of Excellence ROYAL FREE HOSPITAL, London, UK


2 NEUROENDOCRINE CELLS Peptide hormone-producing cells that share a neural-endocrine phenotype Cells that form glands - Adenohypophysis - Parathyroids - Paraganglia - Adrenal medulla Cell Type Localisation Products D cells GI tract Somatostatin Enterochromaffin GI tract Serotonin, Substance P Enterochromaffin-like GI Tract Histamine G cells Stomach and duodenum Gastrin VIP cells GI Tract VIP A cells Pancreas Glucagon B cells Pancreas Insulin Chromaffin Adrenals Catecholamines C cells Thyroid Calcitonin Cells that are diffusely distributed - Skin - Thyroid - Lung - Thymus - Genitourinary tract - GI tract - Pancreas Image from:
3 Rare May secrete hormones NETs Usually Slow growing May have somatostatin receptors Usually can be treated with more than one options
4 INCIDENCE OF NEUROENDOCRINE TUMOURS (NETS) OVER TIME, BY SITE AND BY DISEASE STAGE Reproduced with permission from Dasari A, et al. JAMA Oncol 2017;3(10): Copyright 2017 American Medical Association. All rights reserved.

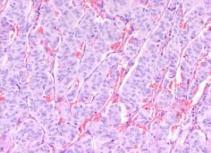
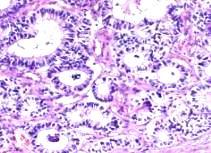
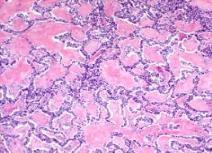
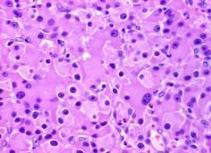
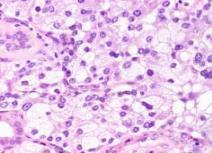
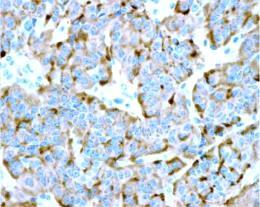
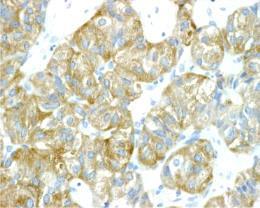
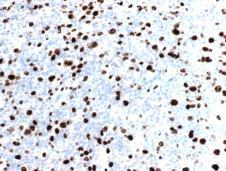
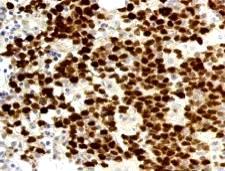
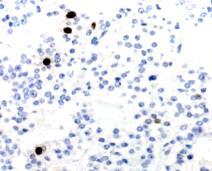
5 HISTOPATHOLOGICAL ASSESSMENT OF NETS Cell morphology Immunohistochemistry General markers Chromogranin, synaptophysin, cytokeratin Peptide hormones (serotonin) Receptors Ki67 (to assess tumour grading) (marker of proliferation, showing how many cells are in cycle) Courtesy of the Royal Free Hospital, London, Histopathology Lab database. Klöppel G. Best Pract Res Clin Endocr Metabol 2007;21:15 31.
 3a. Neuroendocrine tumours of G3 grade (Ki67 >20%): well differentiated 3b.")
6 HISTOPATHOLOGICAL CLASSIFICATION OF NETS WHO 2017 CLASSIFICATION 1. Well-differentiated neuroendocrine tumours of G1 grade (Ki67 <2%) 2. Well-differentiated neuroendocrine tumours of G2 grade (Ki %) 3a. Neuroendocrine tumours of G3 grade (Ki67 >20%): well differentiated 3b. Neuroendocrine carcinoma, NEC (Ki67 >20%): poorly differentiated (small or large cell) + TNM staging SilverScreen / Alamy Stock Photo World Health Organization 2017.

7 NET HETEROGENEITY Intra-tumoural phenotypic heterogeneity is frequently observed in GEP-NETs Most primary small bowel NETs are G1 tumours (Ki67<2%) However, when these tumours metastasize to the liver, they may become highly proliferative More than two-thirds of the patients who had G1 primary tumour developed G2 or G3 liver metastases Shi C, et al. Am J Clin Pathol 2015; 143(3): , by permission of the American Society for Clinical Pathology.
8 CLINICAL CLASSIFICATION OF NETS Pancreatic neuroendocrine tumours Gastrointestinal neuroendocrine tumours Carcinoids foregut midgut hindgut Up to 10% associated with adenocarcinoma Functional or Non-functional Functional or Non-functional Solcia E, et al. WHO 2002.
9 TYPES OF GASTRIC NETS Type I Type ΙΙ Type ΙΙΙ Relative frequency 70 80% 5 6% 14 25% Features Usually multiple (<10mm) Usually multiple (<10mm) Usually solitary (> 20mm) Ass. diseases Atrophic gastritis ΜΕΝ-1/ Gastrinoma No Histology G1 G1 G2 / G3 Serum Gastrin Raised Raised Normal Gastric p H Alkaline Hyperacid Normal Metastases < 5 % 10 30% % Tumour related deaths - < 10% 25 30%

 License (https://creativecommons.org/licenses/by-nc/4.0/) Image from Dermatology Oasis.")
10 DUODENAL NEUROENDOCRINE TUMOURS 1 3 % of all duodenal neoplasms Five types: Non-functional d-nens (positive immunohistochemistry for serotonin and calcitonin) Duodenal gastrinomas Somatostatinomas Duodenal gangliocytic paragangliomas High-grade poorly differentiated neuroendocrine carcinomas 90% are located in D1 and D2 >75% are measuring <2 cm Lymph nodal metastases are noted: 20 60% 20% are located in peri-ampullary region (18% are associated with von-reckinhausen s disease) Copyright Sato Y, et al. Published by Baishideng Publishing Group Inc. All rights reserved. Distributed under the terms of the Creative Commons Attribution-Noncommercial (CC BY-NC 4.0) License ( Image from Dermatology Oasis. Available at: Accessed February 2018 Delle Fave G, et al. ENETS Consensus Guidelines for the management of patients with gastroduodenal neoplasms. Neuroendocrinology 2012;95(2): Reproduced with permission from S. Karger AG, Basel. Sato Y, et al. World J Gastroenterol 2016;22(30):
11 DIAGNOSIS OF NETS History and clinical examination Biochemical tests Imaging studies (for localisation of primary and metastatic lesions) Histology - gold standard

12 CLINICAL PRESENTATION (1) SPECIFIC SYMPTOMS MIDGUT NETs (in 5% of bronchial NETs and 1% of pancreatic NETs) Image courtesy of Dr. Christos G. Toumpanakis Carcinoid syndrome Flushing, diarrhoea, bronchospasm, carcinoid heart disease % of patients with liver metastases 5% of patients with carcinoid syndrome do not have liver metastases Carcinoid crisis Severe symptoms of carcinoid syndrome + hypotension during procedures that involve GA, as well as in TAE, and when the patient is on inotropes
:378-81.")
13 CARCINOID HEART DISEASE May develop in 20 50% of patients, with carcinoid syndrome Main cause of death in 40 50% of patients Involves mainly the right valves of the heart May be present even in asymptomatic patients Valve replacement in a selected group of patients Image courtesy of Dr. Christos G. Toumpanakis Battacharyya S, Toumpanakis CG, et al. Am J Cardiol 2008;101(3):


14 CLINICAL PRESENTATION (2) NON-SPECIFIC SYMPTOMS Dyspepsia Chronic abdominal pain Weight loss Symptoms compatible with IBS Etc, etc.. So Tumours are diagnosed incidentally: a. During surgery b. During endoscopy c. On imaging studies and guided biopsy of tumour lesions
15 BIOCHEMICAL TESTS (BIOMARKERS): NON-SPECIFIC - CHROMOGRANIN-A (CGA) Sensitivity: 60-90%, Specificity: % Correlate with tumour burden Independent factor of survival in midgut NETs Not raised in: May be raised in non-nets situations: Rectal NETs Poorly differentiated NECs Chronic PPI use Atrophic gastritis IBD Renal failure Cirrhosis Other cancers Modlin IM, et al. Ann Surg Oncol 2010.
16 BIOCHEMICAL TESTS (BIOMARKERS): SPECIFIC a) 24 hour urinary 5-HIAA (metastatic midgut NETs) Please note that certain foods like banana, avocado, aubergine, pineapple, plum, walnut and some drugs like paracetamol, fluorouracil, methysergide, naproxen and caffeine, may cause false positive results, whilst other drugs like levodopa or phenothiazines may cause false negative results. b) Role of Gastrin in differentiation of types of Gastric NETs
17 USEFULNESS OF N-TERMINAL PRO-BRAIN NATRIURETIC PEPTIDE AS A BIOMARKER OF THE PRESENCE OF CARCINOID HEART DISEASE 200 patients with midgut NETs underwent cardiac ECHO and estimation of N-terminal pro-brain natriuretic peptide 19.5% had ECHO findings consistent with CHD NT pro-bnp levels were significantly higher (p<0.001) in patients with carcinoid heart disease Sensitivity and specificity for cut-off level of 260pg/ml was 92% and 91%. NT pro-bnp levels had positive correlation with CHD score (r: 0.81, p<0.001) and NYHA scale (p<0.001) Reprinted from Am J Cardiol, 102(7), Bhattacharyya S, et al. Usefulness of N-terminal Pro Brain Natriuretic Peptide as a Biomarker of the Presence of Carcinoid Heart Disease, Copyright 2008, with permission from Elsevier.
18 NOVEL BIOMARKERS
19 CIRCULATING TUMOUR CELLS (CTCS) AS PROGNOSTIC MARKERS IN NEUROENDOCRINE TUMOURS Presence of CTCs was associated with increased burden, increased tumour grade, and elevated serum chromogranin A The presence of one CTC was associated with worse PFS and overall survival Within tumour grades, presence of CTCs was able to define a poor prognostic subgroup CTCs are a promising prognostic marker for patients with NETs and should be assessed in the context of clinical trials with defined tumour subtypes and therapy Different types of NETs (midgut, pancreatic) with same cut-off (one CTC) as predicting a worse outcome applied, whilst evidence from other cancers suggested the correct cut-off varied depending on tumour type. Khan MS, et al. J Clin Oncol, 31(3), 2013: Reprinted with permission American Society of Clinical Oncology. All rights reserved.
20 EARLY CHANGES IN CIRCULATING TUMOUR CELLS Are associated with response and survival following treatment of metastatic neuroendocrine neoplasms 138 patients with metastatic NENs (G1/G2) commencing therapy were prospectively recruited First post-treatment time point (PT1): 3 5 weeks Group A: 0 CTCs at baseline and PT1 Group B: >50% reduction from baseline Group C: <50% reduction or increase 0 CTCs at PT1: only 4% progressed >8 CTCs at PT1: 65% progressed CTCs No Median Survival mo 0 Not reached at > Early post-treatment CTC change is associated with radiologic response and survival, presenting an opportunity to explore biomarker-led sequencing studies in patients with NENs Reprinted from Clin Cancer Research 2015, 22(1) , Khan MS, et al. Early Changes in Circulating Tumor Cells Are Associated with Response and Survival Following Treatment of Metastatic Neuroendocrine Neoplasms. with permission from AACR.
 was developed High sensitivity (85 98%) and specificity (93")
 is derived from the PCR data Values ranged from 0 to 8; a value of >2 is a positive tumour score Reprinted by")

21 MAAA PCR-BASED TEST (NETEST) Multianalyte with Algorithm Analysis Assay Using gene microarray-based approaches of both malignant NET tissue and blood, a PCR-based 51 marker signature (multigene test) was developed High sensitivity (85 98%) and specificity (93 97%) for the detection of intestinal and p NETs in circulating blood Not affected by age, gender, ethnicity, fasting or PPIs A NET score (0 8) is derived from the PCR data Values ranged from 0 to 8; a value of >2 is a positive tumour score Reprinted by permission from Springer Customer Service Centre GmbH: Springer Nature, Am J Gastroenterol, The Clinical Utility of a Novel Blood-Based Multi- Transcriptome Assay for the Diagnosis of Neuroendocrine Tumors of the Gastrointestinal Tract, Modlin IM, et al. Copyright 2015.
![NETEST POTENTIAL CLINICAL APPLICATIONS Can it define the effectiveness of operative resection and loco-regional [TA(C)E, RFA] treatments?](/docs-images/92/108437803/images/22-2.jpg "35 patients with GEP-NET (mainly G1 & G2) were included Surgery was performed in 27 (1) to remove primary tumour, including loco-regional lymph nodes (n = 21); (2) for debulking (n = 4); and (3) for")
22 NETEST POTENTIAL CLINICAL APPLICATIONS Can it define the effectiveness of operative resection and loco-regional [TA(C)E, RFA] treatments? 35 patients with GEP-NET (mainly G1 & G2) were included Surgery was performed in 27 (1) to remove primary tumour, including loco-regional lymph nodes (n = 21); (2) for debulking (n = 4); and (3) for suspicion of NET 8 subjects had loco-regional treatments (TAE = 3, TACE: 3, RFA = 3) for hepatic metastases The NETest was scaled as minimal activity risk <14%, low activity risk 14 47%, and high activity risk >47%. Surgery significantly reduced scores in each of these groups 4 (27%) developed disease recurrence locoregionally at 6 months identified by imaging ( 68 Gasomatostatin receptor-based PET). At 1 month after surgery, all 4 patients exhibited increased NETest scores (median, 30%; range 13-87%) For group III, the pre-ablation NETest scores were elevated (76.2 ± 4.4%) and reduced after treatment Reprinted from Surgery 159(1), Modlin IM, et al. Blood measurement of neuroendocrine gene transcripts defines the effectiveness of operative resection and ablation strategies, Copyright 2016, with permission from Elsevier.

:8-17. Paulsen SR, et al. Radiographics 2006;26(3):641 57.")
23 CONVENTIONAL IMAGING IN NETS Images courtesy of Dr Christos G.Toumpanakis Image from Paulsen RD, et al. Spiral CT and MRI: can reveal the primary site in ~30 70% and distal metastases in 90% of patients CT enterography: can detect the primary small bowel NET with sensitivity 85% and specificity 97% Ricke J, et al. European J Radiol 2001;37(1):8-17. Paulsen SR, et al. Radiographics 2006;26(3): Copyright 2006 Radiological Society of North America


:264 75 Rondonotti E, et al.")
24 ENDOSCOPIC ULTRASOUND & WIRELESS SMALL BOWEL CAPSULE ENDOSCOPY Endoscopic ultrasound Can assess depth of invasion of stomach, duodenal, rectal wall Wireless small bowel capsule endoscopy May have a role for detection of occult small bowel NETs Jensen RT, Neuroendocrinology 2004;80 Suppl 1:23 7; Tucker ON, et al. Br J Surg 2006;93(3): Rondonotti E, et al. Endoscopy 2008;40(6):488 9

25 SOMATOSTATIN RECEPTORS IN NETS Carcinoid tumours: sst2>sst5>sst1>sst3&4 Gastrinomas: sst2>sst5=sst1>sst3>sst4 Insulinomas: sst5>sst3>sst2>sst4>sst1 NFPETS: sst2>sst3>sst1>sst5>sst4 Glucagonomas/MCT/phaeo: sst2>sst1>sst5=sst4>ssst3 From N Engl J Med, Lamberts SW, et al. Octreotide, 334: Copyright 1996 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.


26 ΟCTREOSCAN Reveals the primary in 50-80% and the metastases 95% of patients Can predict the response with somatostatin analogues Low sensitivity in poorly-differentiated NETs, small duodenal gastrinomas and insulinomas Ant Post Images courtesy of Dr. Christos G. Toumpanakis Warner RR. Gastroenterology 2005;128(6):
 Image courtesy of Dr. Christos G. Toumpanakis Eriksson B, et al. Ann N Y Acad Sci 2002;970:159 69 Binderup T, et al.")
27 THE ROLE OF 18F-FDG-PET IN NETS 18 F- FDG PET is useful for evaluation of extent of disease: a) In poorly differentiated G3 tumours b) In tumours with high Ki67 10%,and no Octreoscan uptake It seems that intense 18F- FDG uptake by tumour lesions predicts survival (one study) Image courtesy of Dr. Christos G. Toumpanakis Eriksson B, et al. Ann N Y Acad Sci 2002;970: Binderup T, et al. Clin Cancer Res 2010;16(3): Abgral R, et al. J Clin Endocrinol Metab 2011;96(3):665 71
28 PET SCANS SPECIFIC FOR NETS PET with 68 Ga-somatostatin analogues 68 Ga DOTATATE 68 Ga DOTATOC 68 Ga DOTANOC Better sensitivity than OCTREOSCAN, CT More expertise is needed in interpretation of its results, in view of its physiological uptake 18 F-DOPA PET 11 C 5-HTP PET Image from: Toumpanakis CG, et al. Neuroendocrinology 2014;99: Copyright 2014, Karger Publishers, Basel, Switzerland For GI-NETs, 18F-DOPA PET was found to be more sensitive than 11C-5-HTP PET (98% vs. 89%), whilst just the opposite was noted in patients with pnets A cyclotron is required Sensitivity seems to be inferior to 68Ga PET studies Sundin A, et al. Neuroendocrinology 2007; Gabriel M, et al. J Nucl Medicine 2007; Frilling A, et al. Ann Surg 2010.

29 HEPATIC METASTASES IN THE SAME PATIENT Hepatic metastases from NET (68Ga-octreotate PET, left) Colorectal cancer (FDG-PET, right) in the same patient Image courtesy of Dr. Christos G. Toumpanakis Use of molecular imaging to differentiate liver metastasis of colorectal cancer metastasis from neuroendocrine tumour origin Desai AP, et al. J Clin Gastroenterol. 2011;45(1):e8-11.




30 COMBINATION OF PETS FOR NET HETEROGENEITY Ga68 Ga68 FDG FDG Images courtesy of Dr. Christos G. Toumpanakis
31 NOVEL MOLECULAR IMAGING
 in a patient with NET of unknown origin (G2). Reprinted from Best Pract Res Clin Endocrinol Metab, 30(1), Baumann T, et al.")
32 IMAGING WITH SOMATOSTATIN RECEPTOR ANTAGONISTS Comparison of 111In-DTPA-octreotide scintigraphy (SSTR2 agonist), 111In-DOTA-BASS scintigraphy (SSTR2 antagonist), and 111In-DOTA-JR11 scintigraphy (SSTR2 antagonist) in a patient with NET of unknown origin (G2). Reprinted from Best Pract Res Clin Endocrinol Metab, 30(1), Baumann T, et al. Gastroenteropancreatic neuroendocrine tumours (GEP-NET) Imaging and staging, Copyright 2016, with permission from Elsevier.

33 Image courtesy of Dr. Christos G. Toumpanakis with consent Image courtesy of Dr. Christos G. Toumpanakis



34 AS REQUIRED IMAGING MODALITIES Parathyroid scan MRI spine, most sensitive technique for demonstrating bone metastases MRI pituitary Images courtesy of Dr. Christos G. Toumpanakis. Kos-Kudla B, et al. Neuroendocrinology 2010;91(4):
35 DIAGNOSTIC ALGORITHM History clinical examination Chromogranin-A 5-HIAA NT-pro BNP Cardiac ECHO FDG-PET scan High-grade tumours Suspected tumour heterogeneity Suspected second malignancy Triple phase CT c/a/p Or MRI Somatostatin Receptor Scintigraphy (Ga-68 PET OctreoScan) Tissue diagnosis MRI liver MRI spine CT/MRI enterography S.B capsule endoscopy EUS Commencement of treatment Clinical, biochemical and radiological follow-up
36

37 TREATMENT OF NETS A. Medical control of patient s symptoms B. Resection of tumour primary and if possible, metastatic lesions C. Control of tumour growth in cases of advanced disease D. Improvement and maintenance of patient s quality of life.




38 SOMATOSTATIN ANALOGUES Octreotide LAR Accessed May 2018 Lanreotide autogel
39 SOMATOSTATIN ANALOGUES IN CARCINOID SYNDROME First and best choice medications 1,2 Reduce flushing >70% 1,2 Reduce diarrhoea >60% 1,2 Biochemical response ~50% 1,2 Prospective cross over analysis of 33 patients 3 No differences between octreotide and lanreotide in symptom control or biochemical response 3 SST Inhibition of hormone secretion by the tumour SST 1. Shah T & Caplin M, Best Pract Res Clin Gastroenterol. 2005; 2. Plockinger U & Wiedenmann B, Best Pract Res Clin End Metab 2007; 3. O Toole D, et al. Cancer 2000.

40 INTERFERON-ALPHA FOR CARCINOID SYNDROME SYMPTOMS CONTROL RFH Interferon Data 2 24 pts, in combination with SSTA Diarrhoea improved 45% Flushing improved in 54% No statistically significant decrease of 5-HIAA levels Of the 19 patients given alpha-interferon in combination with octreotide, 72% showed significant reduction in urinary 5-HIAA for a median of 10 months 1 27% of patients discontinued treatment at 3 months, due to AE A symptomatic improvement was seen in 49% 1 The combination was well tolerated 1 1. Janson ET & Oberg K, Acta Oncol 1993; 2. Mirvis E, et al. Anticancer Research 2015.

 Ca 2+ channel Hormone 1. Feelders RA, et al.")
41 PASIREOTIDE (SOM230) Pasireotide is a novel multireceptor-targeted somatostatin analogue with high binding affinity for somatostatin receptor subtypes 1, 2, 3 and 5 1 Preclinical models have shown that pasireotide can influence tumour cell growth via effects on apoptosis and angiogenesis 1 Hormone Ca 2+ Ca 2+ Ca 2+ - Ca 2+ Voltage Ca 2+ camp Secretion (frequently) K + K + K + K + channel channel Adenyl cyclase PTPase SHP-1 SHP-2 PTPᶯ Caspase 8 Wt P53 ERK1/2 Bax ph i Endonuclease Apoptosis Somatostatin G Gβ GƔ + SSTR + ERK1/2 P27 Kip1 + - PLCβ/IP 3 Cell growth + ER Ca 2+ Secretion (infrequently) Ca 2+ channel Hormone 1. Feelders RA, et al. Drugs Today (Barc) 2013;49:89 103
42 PHASE III STUDY OF PASIREOTIDE LAR VS. OCTREOTIDE LAR IN PATIENTS WITH METASTATIC MIDGUT NET Blinded treatment period of 6 months NET patients with carcinoid syndrome symptoms inadequately controlled by maximum doses of currently available SSAs 1:1 randomisation Pasireotide LAR 60 mg IM every 28 days x 6 months with dose to 40 mg for tolerability (n=53) Octreotide LAR 40 mg IM every 28 days x 6 months with dose to 30 mg for tolerability (n=57) Primary endpoint: symptom control (month 6) Secondary endpoints: tumour response, PFS, safety Trial was terminated early based on interim analysis demonstrating futility for primary endpoint (symptom response at month 6) Wolin EM, et al. J Clin Oncol 2013;31:(suppl; abstr 4031); identifier NCT


43 ΙN ADDITION TO SSA, TELOTRISTAT ETIPRATE INHIBITS SEROTONIN PRODUCTION AND ALLEVIATES SYMPTOMS Serotonin Hormonal syndrome flushing, diarrhoea... 5-HIAA Urine 5-HIAA: 5-hydroxyindole acetic acid SSA somatostatin analogue SSTR somatostatin receptor Serotonin Tryptophan- Hydroxylase Tryptophan 5-Hydroxytryptophan (5-HTP) Serotonin (5-HT) NET-Cell Telotristat etiprate SSTR SSA
44 TELESTAR PHASE 3 STUDY DESIGN 3- to 4-week run-in (n=135) Run in: Evaluation of bowel movement (BM) frequency 1:1:1 R Placebo TID (n=45) Telotristat etiprate 250 mg TID (n=45) Telotristat etiprate 500 mg TID* (n=45) Telotristat etiprate 500 mg TID Evaluation of primary endpoint: Reduction in number of daily BMs from baseline (averaged over 12-week double-blind treatment phase) All patients required to be on SSA at enrollment and continue SSA therapy throughout study period Kulke M, et al. J Clin Oncol 2017;35(1):14 23
45 TELESTAR RESULTS: REDUCTION IN MEAN DAILY BOWEL MOVEMENT FREQUENCY AT BASELINE AND WEEK 12 17% 28% 36% Mild nausea: 15% Mild depression: 15 20% Kulke M, et al. J Clin Oncol 35(1), 2017: Reprinted with permission 2017, American Society of Clinical Oncology. All rights reserved.
46 SURVIVAL OF PATIENTS With bowel bypass (12) versus failed resection (17) versus no resection (80) versus resection (210) Study supported by UKI-NETS 5 UKI NET centres 360 patients RP NR ByP FR Median survival 9.92 years 4.68 years 5.61 years 6.74 years Deaths due to fibrosisrelated cachexia RP 4.78% NR,ByP, FR 12.72% Republished with permission of Society for Endocrinology from Endocr Relat Cancer, Ahmed A, et al. 16(7), 2009; permission conveyed through Copyright Clearance Center, Inc



47 MESENTERIC FIBROSIS IN MIDGUT NETS Episodes of sub-acute bowel obstruction Diet modification Hydronephrosis Ureteric stents Malnutrition Nutritional supplements, enteral feeding, TPN? Small bowel bacterial overgrowth Antibiotics Recurrent ascites, ectopic varices SMV stenting? Images courtesy of Dr. Christos G. Toumpanakis Toumpanakis CG, et al. BSG 2006; Naik et al. ENETS 2014.
48 CONTROL OF TUMOUR GROWTH FOR ADVANCED INOPERABLE GASTRO-INTESTINAL NETS Medical therapy Somatostatin analogues (SSAs) Interferon-α Molecular targeted therapies mtor inhibitors Systemic chemotherapy Loco-regional therapy Radiofrequency ablation (RFA) Embolization/chemoembolization/ radioembolization Nuclear medicine and radiation Tumour-targeted, radioactive therapy: PRRT using: 177 Lu DOTATATE External radiation (for bone/brain metastases)
49 OCTREOTIDE LAR IN PATIENTS WITH METASTATIC NEUROENDOCRINE MIDGUT TUMOURS PROMID placebo-controlled, double-blind, randomized study Median time to progression: 14.3 months in LAR group vs. 6 months in placebo After 6 m of treatment: Stable disease in 66.7% of LAR vs. 37.2% of placebo Most favorable effect in patients with low-hepatic tumour load and resected primary tumour Rinke A, et al. J Clin Oncol 27, 2009: Reprinted with permission American Society of Clinical Oncology. All rights reserved.
50 PRIMARY ENDPOINT: PFS PFS and tumour growth with Lanreotide Autogel in patients with enteropancreatic NETs: Results from CLARINET, a randomised, double-blind, placebo-controlled study 62% 22% Time (months) (ITT, N=204) P-value derived from stratified log-rank test; HR derived from Cox proportional hazard model. HR, hazard ratio; ITT, intention-to-treat. From N Engl J Med, Caplin ME, et al. Lanreotide in Metastatic Enteropancreatic Neuroendocrine Tumors, 371(3): Copyright 2014 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
51 RESULTS OF PHASE III STUDY OF PASIREOTIDE LAR VS. OCTREOTIDE LAR In patients with metastatic midgut NET There was no difference in symptoms control between the two arms Overall there was no difference in disease control (CR+PR+SD) between the two arms Pasireotide LAR demonstrated a benefit in tumour shrinkage Prolongation of PFS by 5 months was observed in patients treated with pasireotide LAR (11.8 vs. 6.8 months) Wolin EM, et al. Drug Des Dev Ther 2015;9: Licensed under Creative Commons Attribution Non Commercial (unported, v3.0) available at
52 COMBINATION OF SOMATOSTATIN ANALOGUES WITH INTERFERON Study No of pts Primary Combination SD % PR / CR % Frank M, et al. 21 Pancreatic / midgut OCT + INF-α 62 5 Fjällskog ML, et al. 16 pancreatic OCT + INF-α >80 Kölby L, et al. 68 Midgut OCT + INF-α Faiss S, et al. 80 Foregut/ midgut / hindgut Arnold R, et al. 105 Pancreatic Midgut LAN or INF-α or LAN+ INF-α OCT or OCT + INF-α Reduced risk in tumour progression No benefit in survival No benefit of the combination More adverse effects No superior to monotherapy In PFS & OS Frank M, et al. Am J Gastroenterol 1999; Fjällskog ML, et al. Med Oncol 2002; Kölby L, et al. Br J Surg 2003; Faiss S, et al. J Clin Oncol 2003; Arnold R, et al. Clin Gastroenterol Hepatol 2005

53 SYSTEMIC CHEMOTHERAPY Platinum-based chemotherapy is the treatment of first choice in GEP-NECs with good RR but short PFS A 55% cut-off level of Ki67 seems promising predictive factor of response in NECs Streptozocin-based regimens induce responses ONLY in 15% of small bowel NETs Ki67 by itself cannot predict response in well-diff NETs Chemotherapy could be an option to be the preferred option in type III gastric NETs with rapid symptomatic and radiological progression; however, prospective studies are needed Kouvaraki MA, et al. J Clin Oncol 22(23), 2004: Reprinted with permission American Society of Clinical Oncology. All rights reserved. Toumpanakis CG, et al. Best Pract Res Clin End Metab 2007; Sorbye et al. the NORDIC NEC study, Ann Oncol 2013.

54 Sunitinib Everolimus Reprinted from Gastroenterology, 135(5), Metz D, Jensen R. Gastrointestinal Neuroendocrine Tumors: Pancreatic Endocrine Tumors, Copyright 2008, with permission from Elsevier.
55 RADIANT-4 STUDY DESIGN Patients with well-differentiated (G1/G2), advanced, progressive, nonfunctional NET of lung or GI origin (N = 302) Absence of active or any history of carcinoid syndrome Pathologically confirmed advanced disease Enrolled within 6 months from radiologic progression R A N D O M I S E 2:1 Everolimus 10 mg/day N = 205 Placebo N = 97 Treated until PD, intolerable AE, or consent withdrawal Endpoints: Primary: PFS (central) Key Secondary: OS Secondary: ORR, DCR, safety, HRQoL (FACT-G), WHO PS, NSE/CgA, PK Stratified by: Prior SSA treatment (yes vs. no) Tumour origin (stratum A vs. B)* WHO PS (0 vs. 1) *Based on prognostic level, grouped as: Stratum A (better prognosis) appendix, caecum, jejunum, ileum, duodenum, and NET of unknown primary. Stratum B (worse prognosis) lung, stomach, rectum, and colon except caecum. Crossover to open label everolimus after progression in the placebo arm was not allowed prior to the primary analysis. Yao JC, et al. Lancet 2016;387(10022):968 77
56 PRIMARY ENDPOINT: PFS BY CENTRAL REVIEW 52% reduction in the relative risk of progression or death with everolimus vs. placebo HR=0.48 (95% CI, ); P< P-value is obtained from the stratified one-sided log-rank test; Hazard ratio is obtained from stratified Cox model. Reprinted from The Lancet, 387(10022), Yao JC, et al. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): a randomised, placebo-controlled, phase 3 study, Copyright 2016, with permission from Elsevier.
 1,2 Partial response: ~50% 1,2 Survival benefit?")
 2 Mortality 3 IV octreotide infusion pre- and")


57 TRANSARTERIAL HEPATIC EMBOLIZATION AND CHEMOEMBOLIZATION Symptomatic benefit (40 80%) 1,2 Partial response: ~50% 1,2 Survival benefit? 1,2 Morbidity (carcinoid crisis, fever, pain, hepatic failure, intestinal ischaemia) 2 Mortality 3 IV octreotide infusion pre- and posttherapy in midgut carcinoids 3 Careful selection of patients 3 Images courtesy of Dr. Christos G. Toumpanakis 1. Brown KT, et al. J Vasc Interv Radiol 1999;10(4): ; 2. Chamberlain et al. J Am Coll Surg 2000;190: ; 3. Toumpanakis CG, et al. Best Pract Res Clin End Metab 2007.


58 OTHER ABLATION THERAPIES Radio-frequency ablation Laser-induced thermotherapy Cryotherapy Ethanol ablation Reprinted from Gastroenterology, 134(6), El-Serag HB, et al. Diagnosis and Treatment of Hepatocellular Carcinoma, Copyright 2008 with permission from Elsevier Brachytherapy

59 SST ANALOGUE TARGETED RADIOTHERAPY Mechanism of action Isotope + Sst analogue Somatostatin receptor Tumour cell Tumour cell The β-emitter labelled somatostatin analogue delivers a lethal radiation dose to the tumour cell
60 NETTER-1 STUDY OBJECTIVES AND DESIGN Aim Evaluate the efficacy and safety of LUTATHERA + SSAs (symptoms control) compared to Octreotide LAR 60mg (off-label use) in patients with inoperable, somatostatin receptor positive, midgut NET, progressive under Octreotide LAR 30mg (label use) Design International, multicentre, randomised, comparator-controlled, parallel-group n = 116 n = 113 Treatment and assessments Progression-free survival (RECIST criteria) every 12 weeks 4 administrations of 7.4 GBq of LUTATHERA every 8 weeks + SSAs (symptom control) Octreotide LAR (high dose 60mg every 4 weeks) 5 Years follow up Baseline progression according to RECIST 1.1 criteria The median time between the oldest pre-baseline and the baseline scans (used to determine the progression at enrolment) was 11.4 months for patients in the LUTATHERA arm and 11.7 months for the control arm Strosberg J, et al. N Engl J Med 2017;376(2):
61 PFS, OS AND SUBGROUP ANALYSIS IN NETTER-1 Adverse effects Nausea: 59% Vomiting: 47% Anaemia:14% Neutropenia: 6% Thrombocytopenia: 25% NO RENAL TOXICITY From N Engl J Med, 376(2), Strosberg J, et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors, Copyright 2017 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
62 OBJECTIVE RESPONSE IN NETTER-1 Response category 177 Lu-dotatate group (n=101) Complete response, n (%) 1 (1) 0 Partial response, n (%) 17 (17) 3 (3) Objective response Objective Tumor Response* No. with response 18 3 Control group (n=100) P-value Rate, % (95% CI) (10 25) 3 (0 6) <0.001 Learning point from NETTER-1 trial PRRT with 177 Lu-dotatate can control tumour growth in G1/G2 advanced and progressive midgut NETs with quite good objective response rates *The objective response rate was defined as the percentage of patients who had a response according to Response Evaluation Criteria in Solid Tumors (RECIST) #(sum of partial responses and complete responses). Patients for whom no post-baseline computed tomography (CT) or magnetic resonance imaging (MRI) scans or central response data were available (15 patients in the 177Lu-Dotatate group and 13 patients in the control group) were excluded from this analysis (trial is still ongoing). P-value calculated using Fisher s exact text. Strosberg J, et al. NEJM 2017;376:125 35
63 LONG-TERM EFFICACY OF LU-177 DOTATATE IN GEP-NETS Tumour type N CR PR SD ORR DoR (months) n % n % N % n % 95% CI Median 95% CI All* % % % % 40% 50% Bronchial % 7 37% 11 58% 7 37% 16% 62% Pancreatic % 74 56% 47 35% 81 61% 52% 69% Foregut** % 6 50% 4 33% 7 58% 28% 85% Midgut % 58 32% % 61 33% 27% 41% Hindgut % 6 46% 6 46% 6 46% 19% 75% Tumour type N PFS Time (months) OS Time (months) Median 95% CI Median 95% CI All* Bronchial Pancreatic Foregut** Midgut Hindgut CR: Complete Response PR: Partial Response SD: Stable Disease ORR: Overall Radiological Response PFS: Progression Free Survival OS: Overall Survival Brabander T, et al. Clin Cancer Res. 2017



:593 600. Available at: https://journals.lww.")
64 EARLY EFFICACY OF AND TOXICITY FROM LU-177 DOTATATE TREATMENT In patients with progressive metastatic GEP-NET Kaplan-Meier chart of PFS for the whole cohort Objective response: 13% Disease stabilization: 64% Estimated median PFS was 28 months, 95% CI: months Pencharz D, et al. Early efficacy of and toxicity from lutetium-177-dotatate treatment in patients with progressive metastatic NET Nucl Med Commun 2017;38(7): Available at:
65 COMBINATION OF SOMATOSTATIN ANALOGUES WITH OTHER AGENTS IN MIDGUT NETS CARCINOIDS Octreotide LAR + bevacizumab Octreotide LAR + PEG - INF No of pts SD % PR/CR % PFS % (18 w) CARCINOIDS Octreotide LAR + placebo Octreotide LAR + everolimus PFS 11.3 months 16.4 months RADIANT-2 trial No difference in partial response No difference in disease stabilization More adverse effects in combination group Yao JC, et al. J Clin Oncol 2008;26(8): ; Reprinted from The Lancet, 378 (9808), Pavel ME, et al. Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): a randomised, placebo-controlled, phase 3 study, , Copyright 2011, with permission from Elsevier.



66 WHICH TREATMENT AND FOR WHOM Patient s clinical status, comorbidities and preferences Tumour histology Location of primary Positive uptake in Octreoscan or Ga-68 PET Tumour burden Tumour status Presence of carcinoid heart disease and/or mesenteric fibrosis Predictive molecular markers? Cost??
67 G3 GEP-NETS Patient s performance status 0-2 Systemic chemotherapy Platinum-based chemotherapy [Temozolomide-based chemotherapy (if Ki67 < 55%)] Disease progression 2 nd Line Systemic Chemotherapy (FOLFOX, FOLFIRI) Well differentiated G3 GEP-NETs PRRT? Molecular targeted? Sorbye H, et al. Cancer 2014; ENETS Guidelines 2016.
68 Biopsies of surrounding mucosa Serum gastrin No atrophic gastritis Normal serum gastrin ΤYPE III Atrophic gastritis Hypergastrinaemia ΤYPE I No atrophic gastritis Hypergastrinaemia ΤYPE II In localised disease Surgical resection In advanced disease Systemic treatment Management algorithm of gastric NETs >2 cm Invasion beyond Submucosa Lymph nodes? Local resection +/- antrectomy or +/- somatostatin analogues 1-2 cm No vascular invasion No deep invasion G1 Endoscopic resection <1 cm >1 cm Resection, if symptomatic or Somatostatin analogues Annual endoscopic surveillance Delle Fave G, et al. Neuroendocrinology. 2016;103(2):

69 ENETS 2016 CONSENSUS GUIDELINES FOR DUODENAL NETS Delle Fave G, et al. ENETS Consensus Guidelines Update for Gastroduodenal Neuroendocrine Neoplasms. Neuroendocrinology. 2016;103(2): With permission from S. Karger AG, Basel.
70 ENETS 2016 CONSENSUS GUIDELINES FOR INTESTINAL NETS Pavel M, et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016;103(2): With permission from S. Karger AG, Basel.
71 Dieticians Hepatobiliary & GI surgery Specialist NET Nurses Endocrinology NET patient Pathology Genetics Cardiology Oncology Radiology & Nuclear Medicine Gastroenterology Palliative care & Pain control

72 MULTI-DISCIPLINARY TEAM (MDT) APPROACH FOR NETS Accurate diagnosis & staging Evaluation of performance status & quality of life Consensus agreement on treatment plan Continuous reassessment, discussion and peer review of the individualised treatment plan
73 THANK YOU!
NET εντέρου Τι νεότερο/ Νέες μελέτες. Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ
 NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS
 TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
Nuevas alternativas en el manejo de TNE avanzados
 Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies
 Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal
 Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal Incidence per 100,000 EPIDEMIOLOGY Incidence rates of neuroendocrine tumors by primary tumor site 1.4 1.2 1.0 0.8 0.6
Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal Incidence per 100,000 EPIDEMIOLOGY Incidence rates of neuroendocrine tumors by primary tumor site 1.4 1.2 1.0 0.8 0.6
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS
 OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
Pancreatic Neuroendocrine Tumours
 UCLH Cancer Collaborative Pancreas Update Meeting 12 th July 2017 Pancreatic Neuroendocrine Tumours Dr. Christos Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior
UCLH Cancer Collaborative Pancreas Update Meeting 12 th July 2017 Pancreatic Neuroendocrine Tumours Dr. Christos Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Telotristat Ethyl (etiprate) : a new kid on the block Dr. Christos G. Toumpanakis MD PhD FRCP
 : a new kid on the block Dr. Christos G. Toumpanakis MD PhD FRCP") Telotristat Ethyl (etiprate) : a new kid on the block Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University College of London Neuroendocrine
Telotristat Ethyl (etiprate) : a new kid on the block Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University College of London Neuroendocrine
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Hot of the press. Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ
 Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology
 Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
Recent developments of oncology in neuroendocrine tumors (NETs)
") Recent developments of oncology in neuroendocrine tumors (NETs) Marc Peeters MD, PhD Coordinator Multidisciplinary Oncological Center Antwerpen (MOCA) Head of the Oncology Department UZA, Professor in
Recent developments of oncology in neuroendocrine tumors (NETs) Marc Peeters MD, PhD Coordinator Multidisciplinary Oncological Center Antwerpen (MOCA) Head of the Oncology Department UZA, Professor in
2015: Year in Review Results of Recent Trials
 2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer
 WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
Evaluation and Management of Neuroendocrine Tumors
 Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC
 Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Selection of Appropriate Treatment
 Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
An Overview of NETS. Richard R.P. Warner M.D
 An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
GEP NET: algoritmo terapeutico. Dottor Nicola Fazio
 GEP NET: algoritmo terapeutico Dottor Nicola Fazio Basi per il trattamento Caratteristiche del paziente Caratteristiche del tumore P.S., sindrome, comorbidità Differenziazione, Ki-67 Imaging morfologico
GEP NET: algoritmo terapeutico Dottor Nicola Fazio Basi per il trattamento Caratteristiche del paziente Caratteristiche del tumore P.S., sindrome, comorbidità Differenziazione, Ki-67 Imaging morfologico
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
Diagnosing and monitoring NET
 Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
Lu 177-Dotatate (Lutathera) Therapy Information
 Therapy Information") Lu 177-Dotatate (Lutathera) Therapy Information Information for Lu 177-dotatate therapy also known as Lutathera, for the treatment of metastatic midgut neuroendocrine tumor and other metastatic neuroendocrine
Lu 177-Dotatate (Lutathera) Therapy Information Information for Lu 177-dotatate therapy also known as Lutathera, for the treatment of metastatic midgut neuroendocrine tumor and other metastatic neuroendocrine
NICaN Pancreatic Neuroendocrine Tumour SACT protocols. 1.0 Dr M Eatock Final version issued
 Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες
 NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
EXOCRINE: 93% Acinar Cells Duct Cells. ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others
 EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
A New Proposal for Metabolic Classification of NENs Stefano Severi IRST Meldola Italy
 RADIONUCLIDE THERAPY AND ALLIED SCIENCE President: Giovanni Paganelli Chairman: Maria Salvato Baltimore USA Domenico Barone Meldola Italy A New Proposal for Metabolic Classification of NENs Stefano Severi
RADIONUCLIDE THERAPY AND ALLIED SCIENCE President: Giovanni Paganelli Chairman: Maria Salvato Baltimore USA Domenico Barone Meldola Italy A New Proposal for Metabolic Classification of NENs Stefano Severi
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Treatment algorithm Neuroendocrine tumours. Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece
 Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Octreotide LAR in neuroendocrine tumours a summary of the experience
 Endocrinology in oncology Review article Octreotide LAR in neuroendocrine tumours a summary of the experience Agnieszka Kolasińska-Ćwikła, MD, PhD Department of Chemotherapy, Oncology Clinic, Maria Sklodowska-Curie
Endocrinology in oncology Review article Octreotide LAR in neuroendocrine tumours a summary of the experience Agnieszka Kolasińska-Ćwikła, MD, PhD Department of Chemotherapy, Oncology Clinic, Maria Sklodowska-Curie
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives
 Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Background. Capdevila J, et al. Ann Oncol. 2018;29(Suppl 8): Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):
: Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):") Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Peptide Receptor Radionuclide Therapy (PRRT) of NET
 of NET") Peptide Receptor Radionuclide Therapy (PRRT) of NET Dr. Tuba Kendi Associate Prof of Radiology, Mayo Clinic, Rochester, MN 2014 MFMER slide-1 Relevant Financial Relationship(s) None Off Label Usage None
Peptide Receptor Radionuclide Therapy (PRRT) of NET Dr. Tuba Kendi Associate Prof of Radiology, Mayo Clinic, Rochester, MN 2014 MFMER slide-1 Relevant Financial Relationship(s) None Off Label Usage None
Strategies in the Management of Neuroendocrine Tumors. Dr. Jean Maroun Dr. Elena Tsvetkova
 Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy
 Imaging and Peptide Receptor Radionuclide Therapy") Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy Lawrence Saperstein, M.D. Assistant Professor of Radiology and Biomedical Imaging Chief, Nuclear
Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy Lawrence Saperstein, M.D. Assistant Professor of Radiology and Biomedical Imaging Chief, Nuclear
Peptide Receptor Radionuclide Therapy using 177 Lu octreotate
 Peptide Receptor Radionuclide Therapy using 177 Lu octreotate BLR Kam, Erasmus Medical Centre, Rotterdam DJ Kwekkeboom, Erasmus Medical Centre, Rotterdam Legal aspects As 177 Lu-[DOTA 0 -Tyr 3 ]octreotate
Peptide Receptor Radionuclide Therapy using 177 Lu octreotate BLR Kam, Erasmus Medical Centre, Rotterdam DJ Kwekkeboom, Erasmus Medical Centre, Rotterdam Legal aspects As 177 Lu-[DOTA 0 -Tyr 3 ]octreotate
Pancreatic NeuroEndocrine Tumors. Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium
 Pancreatic NeuroEndocrine Tumors Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Epidemiology Overall incidence 1.8 to 2.6 SEER, Europe Peak in 5 th and 6 th decade Incidence
Pancreatic NeuroEndocrine Tumors Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Epidemiology Overall incidence 1.8 to 2.6 SEER, Europe Peak in 5 th and 6 th decade Incidence
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS)
") FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS) Gilda s Club Quad Cities November 5 th, 2018 Joseph Dillon, MD Neuroendocrine Tumor Clinic University of Iowa Hospitals & Clinics
FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS) Gilda s Club Quad Cities November 5 th, 2018 Joseph Dillon, MD Neuroendocrine Tumor Clinic University of Iowa Hospitals & Clinics
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
GEP NEN. Personalised approach. Curative and Palliative Surgery. ESMO Preceptorship Programme Neuroendocrine Neoplasms Lugano April 2018
 GEP NEN Personalised approach Curative and Palliative Surgery ESMO Preceptorship Programme Neuroendocrine Neoplasms Lugano 13 14 April 2018 Professor Andrea Frilling Department of Surgery and Cancer Imperial
GEP NEN Personalised approach Curative and Palliative Surgery ESMO Preceptorship Programme Neuroendocrine Neoplasms Lugano 13 14 April 2018 Professor Andrea Frilling Department of Surgery and Cancer Imperial
Specialised Services Policy CP66: 68-gallium DOTA- peptide scanning for the Management of Neuroendocrine Tumours (NETs)
") Specialised Services Policy CP66: Management of Neuroendocrine Tumours (NETs) Document Author: Assistant Planner for Cancer and Blood Executive Lead: Director of Quality and Nursing Approved by: Management
Specialised Services Policy CP66: Management of Neuroendocrine Tumours (NETs) Document Author: Assistant Planner for Cancer and Blood Executive Lead: Director of Quality and Nursing Approved by: Management
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid
 Neuroendocrine Tumors and Lung Carcinoid") Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary)
") NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Cynthia Card (Staff Medical Oncologist, University of Calgary)
NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Cynthia Card (Staff Medical Oncologist, University of Calgary)
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors
 At the Cutting Edge Received: February 29, 2016 Accepted: April 12, 2016 Published online: April 16, 2016 Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors Adrian Lee
At the Cutting Edge Received: February 29, 2016 Accepted: April 12, 2016 Published online: April 16, 2016 Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors Adrian Lee
Case Presentation. Marianne Ellen Pavel. Charité University Medicine Berlin. ESMO Preceptorship on GI Neuroendocrine Tumors
 Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
TUMORES NEUROENDOCRINOS. Miguel Navarro. Salamanca
 TUMORES NEUROENDOCRINOS Miguel Navarro. Salamanca Introduction to Neuroendocrine Tumours (NETs) NETs are relatively RARE At least 40 different entities are described arising in different organs. Different
TUMORES NEUROENDOCRINOS Miguel Navarro. Salamanca Introduction to Neuroendocrine Tumours (NETs) NETs are relatively RARE At least 40 different entities are described arising in different organs. Different
Le target therapy nei Tumori Neuroendocrini
 Le target therapy nei Tumori Neuroendocrini Take home messages Franco Grimaldi SOC Endocrinologia e Malattie del Metabolismo Nutrizione Clinica Azienda Ospedaliero-Universitaria Santa Maria della Misericordia
Le target therapy nei Tumori Neuroendocrini Take home messages Franco Grimaldi SOC Endocrinologia e Malattie del Metabolismo Nutrizione Clinica Azienda Ospedaliero-Universitaria Santa Maria della Misericordia
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique
 Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique By Professor Kjell Öberg, M.D., Ph.D. Dept. of Endocrine Oncology, University Hospital, Uppsala, Sweden Nashville Oct. 2011 Hallmarks
Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique By Professor Kjell Öberg, M.D., Ph.D. Dept. of Endocrine Oncology, University Hospital, Uppsala, Sweden Nashville Oct. 2011 Hallmarks
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Gastrinoma: Medical Management. Haley Gallup
 Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Grade 2 Ileum NET with liver and bone metastasis
 Grade 2 Ileum NET with liver and bone metastasis BERNARDO MARQUES ENDOCRINOLOGY DEPARTMENT PORTUGUESE INSTITUTE OF ONCOLOGY - COIMBRA April 2018, Lugano, Switzerland JPB, male, 67 years old April 2015
Grade 2 Ileum NET with liver and bone metastasis BERNARDO MARQUES ENDOCRINOLOGY DEPARTMENT PORTUGUESE INSTITUTE OF ONCOLOGY - COIMBRA April 2018, Lugano, Switzerland JPB, male, 67 years old April 2015
The PET-NET Study 2016 CNETS Grant Award
 The PET-NET Study 2016 CNETS Grant Award CANM Meeting April 21, 2017 Hagen Kennecke, MD, MHA, FRCPC Medical Oncology, BC Cancer Agency Associate Professor, University of British Columbia Raja Ampat, Indonesia
The PET-NET Study 2016 CNETS Grant Award CANM Meeting April 21, 2017 Hagen Kennecke, MD, MHA, FRCPC Medical Oncology, BC Cancer Agency Associate Professor, University of British Columbia Raja Ampat, Indonesia
QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors
 QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors Abstract C-33 Strosberg J, Wolin E, Chasen B, Kulke M, Bushnell D, Caplin M, Baum RP, Kunz P, Hobday
QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors Abstract C-33 Strosberg J, Wolin E, Chasen B, Kulke M, Bushnell D, Caplin M, Baum RP, Kunz P, Hobday
Addison's disease Neuroendocrine tumors Paraneoplastic syndromes
 Addison's disease Neuroendocrine tumors Paraneoplastic syndromes Miklós Tóth Professor of Medicine and Endocrinology 9 th April, 2018 Semmelweis University 2nd Department of Medicine Addison's disease
Addison's disease Neuroendocrine tumors Paraneoplastic syndromes Miklós Tóth Professor of Medicine and Endocrinology 9 th April, 2018 Semmelweis University 2nd Department of Medicine Addison's disease
Neuroendocrine Tumour Theranostics
 Neuroendocrine Tumour Theranostics Lisa Bodei Director of Targeted Radionuclide Therapy Molecular Imaging and Therapy Service Memorial Sloan Kettering Cancer Center New York Friday, April 13, 2018 Disclosure
Neuroendocrine Tumour Theranostics Lisa Bodei Director of Targeted Radionuclide Therapy Molecular Imaging and Therapy Service Memorial Sloan Kettering Cancer Center New York Friday, April 13, 2018 Disclosure
SUPPLEMENTARY INFORMATION
 Supplementary Table 1. Therapies for non-men1 pancreatic neuroendocrine tumours (NETs) (published after 2011) Somatostatin analogues Tumour type a Intervention Number of participants/information available
Supplementary Table 1. Therapies for non-men1 pancreatic neuroendocrine tumours (NETs) (published after 2011) Somatostatin analogues Tumour type a Intervention Number of participants/information available
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Management of Neuroendocrine Tumors
 Management of Neuroendocrine Tumors Professor Barbro Eriksson Department of Endocrine Oncology ENETS Centre of Excellence Uppsala University Hospital Diagnostic Challenges in NET Heterogeneous group of
Management of Neuroendocrine Tumors Professor Barbro Eriksson Department of Endocrine Oncology ENETS Centre of Excellence Uppsala University Hospital Diagnostic Challenges in NET Heterogeneous group of
Theranostics in Nuclear Medicine
 Theranostics in Nuclear Medicine Patrick FLAMEN, MD, PhD Head Nuclear Medicine Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) n Theranostics in Nuclear Medicine n A form of (nuclear) diagnostic
Theranostics in Nuclear Medicine Patrick FLAMEN, MD, PhD Head Nuclear Medicine Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) n Theranostics in Nuclear Medicine n A form of (nuclear) diagnostic
Recent Advances in Gastrointestinal Cancers
 Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Diagnosis abnormal morphology and /or abnormal biochemistry
 Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
SURGERY OF NETS. Iakovos N Nomikos MD FACS. Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece
 SURGERY OF NETS Iakovos N Nomikos MD FACS Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece Epidemiology 5-fold increase in occurrence of NETS over past 30 years
SURGERY OF NETS Iakovos N Nomikos MD FACS Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece Epidemiology 5-fold increase in occurrence of NETS over past 30 years
SOMATOSTATIN RECEPTORS IN HEPATOCELLULAR CARCINOMA. Marie LEQUOY Saint-Antoine Hospital, Department of Hepatology, Paris, France
 SOMATOSTATIN RECEPTORS IN HEPATOCELLULAR CARCINOMA Marie LEQUOY Saint-Antoine Hospital, Department of Hepatology, Paris, France Somatostatin : SST Somatostatin (SST) protein : 2 active forms (alternative
SOMATOSTATIN RECEPTORS IN HEPATOCELLULAR CARCINOMA Marie LEQUOY Saint-Antoine Hospital, Department of Hepatology, Paris, France Somatostatin : SST Somatostatin (SST) protein : 2 active forms (alternative
Pancreatic polypeptide secreting tumors an institutional experience and review of the literature
 ORIGINAL ARTICLE Pancreatic polypeptide secreting tumors an institutional experience and review of the literature Angela Tatiana Alistar 1, Michelle Kang Kim 2, Richard Warner 2, Erin Moshier 3, Randall
ORIGINAL ARTICLE Pancreatic polypeptide secreting tumors an institutional experience and review of the literature Angela Tatiana Alistar 1, Michelle Kang Kim 2, Richard Warner 2, Erin Moshier 3, Randall
Tumor markers. Chromogranin A. Analyte Information
 Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case
 Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
Commonly Encountered Neuro-Endocrine Tumors of the Gut
 Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
CRITICAL ANALYSIS OF NEN GUIDELINES. G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines
 CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
Type 2 gastric neuroendocrine tumor: report of one case
 Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
NET del pancreas ben differenziato: la terapia oncologica. Alfredo Berru: Università degli Studi di Brescia Azienda Ospedaliera Spedali Civili Brescia
 NET del pancreas ben differenziato: la terapia oncologica Alfredo Berru: Università degli Studi di Brescia Azienda Ospedaliera Spedali Civili Brescia Systemic treatment op:ons Somatosta:n analogues Interpheron
NET del pancreas ben differenziato: la terapia oncologica Alfredo Berru: Università degli Studi di Brescia Azienda Ospedaliera Spedali Civili Brescia Systemic treatment op:ons Somatosta:n analogues Interpheron
Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works.
 Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works. Arturo Loaiza-Bonilla, MD, FACP Assistant Professor of Clinical Medicine
Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works. Arturo Loaiza-Bonilla, MD, FACP Assistant Professor of Clinical Medicine
New Developments in the Care and Management of Patients with Gastroenteropancreatic Neuroendocrine Tumors Dr. Tim Asmis The Ottawa Hospital Cancer
 New Developments in the Care and Management of Patients with Gastroenteropancreatic Neuroendocrine Tumors Dr. Tim Asmis The Ottawa Hospital Cancer Centre MD, FRCPC CAGPO September 2018 Disclosures Consultant
New Developments in the Care and Management of Patients with Gastroenteropancreatic Neuroendocrine Tumors Dr. Tim Asmis The Ottawa Hospital Cancer Centre MD, FRCPC CAGPO September 2018 Disclosures Consultant
Prognostic factors and treatment of gastroenteropancreatic G3 neuroendocrine carcinomas.
 Prognostic factors and treatment of gastroenteropancreatic G3 neuroendocrine carcinomas. Halfdan Sorbye Medical Oncologist Professor, MD Dept of Oncology Haukeland Univ Hospital Bergen, Norway Gastroenteropancreatic
Prognostic factors and treatment of gastroenteropancreatic G3 neuroendocrine carcinomas. Halfdan Sorbye Medical Oncologist Professor, MD Dept of Oncology Haukeland Univ Hospital Bergen, Norway Gastroenteropancreatic
Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases
 Case Report Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases Wei Wang 1,2,3 *, Sharvesh Raj Seeruttun 1,2,3 *, Cheng Fang 1,2,3, Zhiwei Zhou 1,2,3
Case Report Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases Wei Wang 1,2,3 *, Sharvesh Raj Seeruttun 1,2,3 *, Cheng Fang 1,2,3, Zhiwei Zhou 1,2,3
Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective
 from a Specialised Nursing Perspective") Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective Avril Hull, Auckland District Health Board, New Zealand Kate Wakelin, Unicorn Foundation, Australia Philippa Davies,
Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective Avril Hull, Auckland District Health Board, New Zealand Kate Wakelin, Unicorn Foundation, Australia Philippa Davies,
lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications
 oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications") lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications 8 June 2018 The Scottish Medicines Consortium (SMC) has completed its assessment
lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications 8 June 2018 The Scottish Medicines Consortium (SMC) has completed its assessment
Tumori Neuroendocrini - Imaging perioperatorio. Annibale Versari Medicina Nucleare, Az.Osp. S.Maria Nuova-IRCCS - Reggio Emilia
 Tumori Neuroendocrini - Imaging perioperatorio Annibale Versari Medicina Nucleare, Az.Osp. S.Maria Nuova-IRCCS - Reggio Emilia Imaging medico-nucleare=imaging molecolare Le immagini sono espressione delle
Tumori Neuroendocrini - Imaging perioperatorio Annibale Versari Medicina Nucleare, Az.Osp. S.Maria Nuova-IRCCS - Reggio Emilia Imaging medico-nucleare=imaging molecolare Le immagini sono espressione delle
SIRT in the Management of Metastatic Neuroendocrine Tumors
 SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
Update on Surgical Management of NETs
 Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---