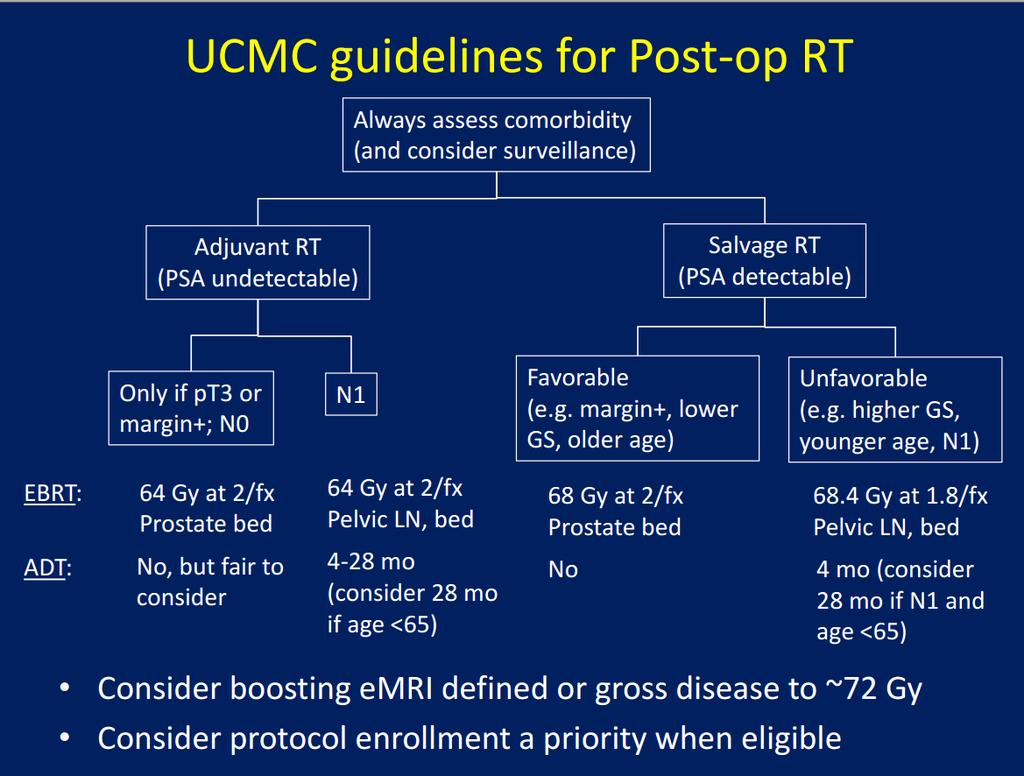
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
|
|
|
- Neal Jackson
- 5 years ago
- Views:
Transcription




1 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
2 Introduction
3
4
5
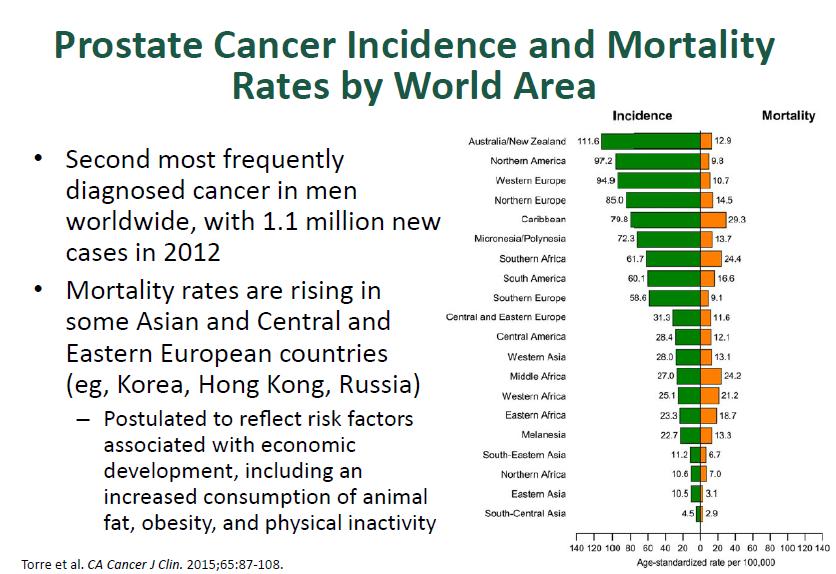
6 Introduction 1/3 of patients with localized disease will present with treatment failure within 5 years of treatment. Huggins and Hodges in 1941 demonstrated the benefit of androgen dependence of PC. For M1 disease, hormone therapy is the mainstay of treatment. In an attempt to improve results for localized cancer

7
8 Risk Categories Defined in various ways Commonest categorization: Low: PSA < 10, GS < 6, and < T2a Intermediate: PSA 10-20, GS 7, or T2b T2c High: PSA >20, GS > 8, or T3 Very High T3b, T4 Metastases stage M1 Very Low Risk : Added in 2010 PSA <10, GS 6, T1C, PSA density < 0.15 ng/ml/g, < 3 cores positive with 50% cancer in each core
9

10 Not free margin, seminal invade, extracapsular extend, detectable PSA
")
11 Diagnostic Pathology (2016) 11:25
 demonstrated that orchiectomy or estrogen dramatically affected prostate")
12 Prostate cancer is an androgen-dependent malignant disease. Drs. Huggins and Hodges (Nobel prize) demonstrated that orchiectomy or estrogen dramatically affected prostate cancer regression and palliation of symptoms in 1941.


13 Androgen Regulation of Prostate Hypothalamus-pituitary-gonadal axis 1,2 Adapted from Fast Facts: Prostate Cancer by Roger S Kirby and Manish I Patel Eighth edition Adapted from Lamb, ; Denmeade, Lamb AD, et al. Trends Urol Mens Health. 2013;4(3): Denmeade SR. Holland-Frei Cancer Medicine. 8th ed. Philadelphia, PA: AACR Publications; 2010:
14 Androgens Testosterone is the primary circulating androgen, with approximately 90% produced by Leydig cells in the testes and 10% produced by the adrenal cortex. Only 3% of circulating testosterone is unbound and functionally active the remainder is bound and sequestered by sex-hormone binding globulin and albumin. Following diffusion into the cytoplasm, testosterone is converted by the enzyme 5α-reductase to DHT, which has a five-fold higher affinity for the LBD of AR
15 Hormone Therapies for Prostate Cancer LHRH agonists. leuprolide (Enantone,Lupron, Eligard), goserelin (Zoladex), Triptorerin LHRH antagonists eg Degarelix Androgen Receptor targeted.. eg Casodex, Flutamide, Enzalutamide Steroids.. eg Prednisone, Dexa Estrogens eg Stilboestrol Cyp 17 inhibitors. eg Abiraterone
16 Efficacy of GnRH agonist to suppress testosterone
17 In long-term studies, leuprorelin effectively maintained testosterone below castration levels Leuprorelin effectively maintains testosterone below castration levels in patients with advanced cancer 1 Adapted from Kienle, Key results The median baseline testosterone level before treatment was 350 ng/dl and level decreased to 21 ng/dl after 1 month, staying within the castration range for the entire observation period (45 months). 1 Long-term follow-up (63 months) of serum testosterone levels confirmed no decline in efficacy of leuprorelin monthly injections Kienle E, et al. Urol Int. 1996;56(Suppl 1):S23-S30.
18 In long-term studies, 3mo vs 6 mo effectively maintained testosterone below castration levels In long-term studies, leuprorelin effectively maintains testosterone below castration levels 1 Key results Median testosterone levels ranged from ng/dl for the 3M and 6M arms. Median PSA 3M arm: ng/ml 6M arm: ng/ml Testosterone response rates ( 50 ng/dl) at 12 months 3M arm: 100% 6M arm: 98% Testosterone response rates ( 20 ng/dl) at 12 months 3M arm: 81% 6M arm: 90% 3M, 3 months; 6M, 6 months. Adapted from Tunn, Tunn UW, et al. Prostate Cancer Prostatic Dis. 2009;12(1):83-87.
19 Metastatic group : ANDROGEN ABLATION LHRH Agonists T Surge vs Orchiectomy Leuprolide vs Orchiectomy Impact on Mean Serum T Levels Level MIU/mL Leuprolide Orchiectomy Day Time from First Dose Week Smith JA. Urology. 1985;25:106. With permission from Elsevier Science.

20 GnRh antagonist: no flare up However, practical shortcomings have limited clinical studies.
21

22
23
24

25

26
27
28 1: AA alone is inferior to RT + AA
 PSA > 20 ng/ml + Gleason")

29 1205 patients locally advanced (T3 or T4) n=1057; or (T2) with either PSA > 40 ng/ml (n=119) PSA > 20 ng/ml + Gleason score >/= 8 (n=25) median follow-up was 6 0 years ADT = bilateral orchiectomy or LHRH agonist (initially given with 2 weeks of AA)
30 Primary outcome: overall survival HR 0 77, 95% CI
31 disease-specific survival
32 Cumulative incidence of disease-specific survival
33 quality-of-life scores over time for symptom measures
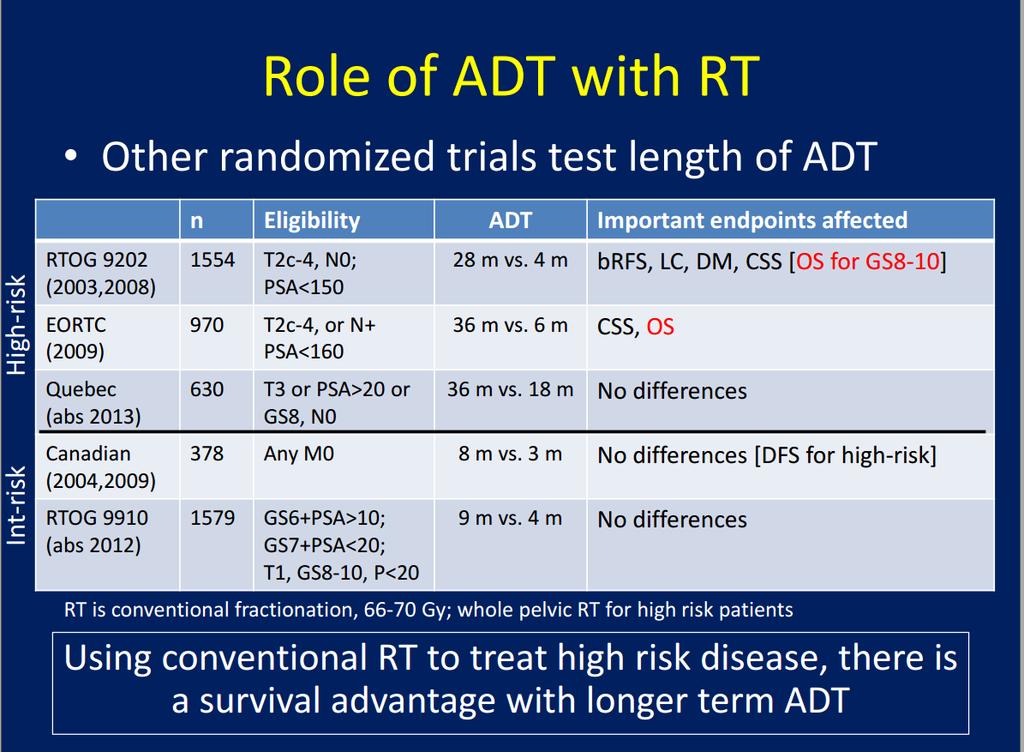
34 High risk group AA alone is inferior to RT + AA Intergroup Study (NCIC, MRC, SWOG, ECOG) (Lancet, 2011, JCO 2015) Phase III: AA vs. AA + RT T3-T4, T2 + PSA > 40, or T2 + PSA > 20 + GS > 8 RT: 45 Gy to pelvic nodes; Gy to prostate/sem. ves. Accrued 1205 patients between 1995 and 2005 Follow-up: 6 years At 7 years AA AA +RT Overall survival 66% 74% (p<0.001) (HR =0.77) Prostate cancer-specific survival 81% 91% (p<0.001) (HR=0.46) Tumor progression 42% 16%
35 JCO, VOLUME 33, NUMBER 19, JULY
36 RT alone is inferior to RT + AA
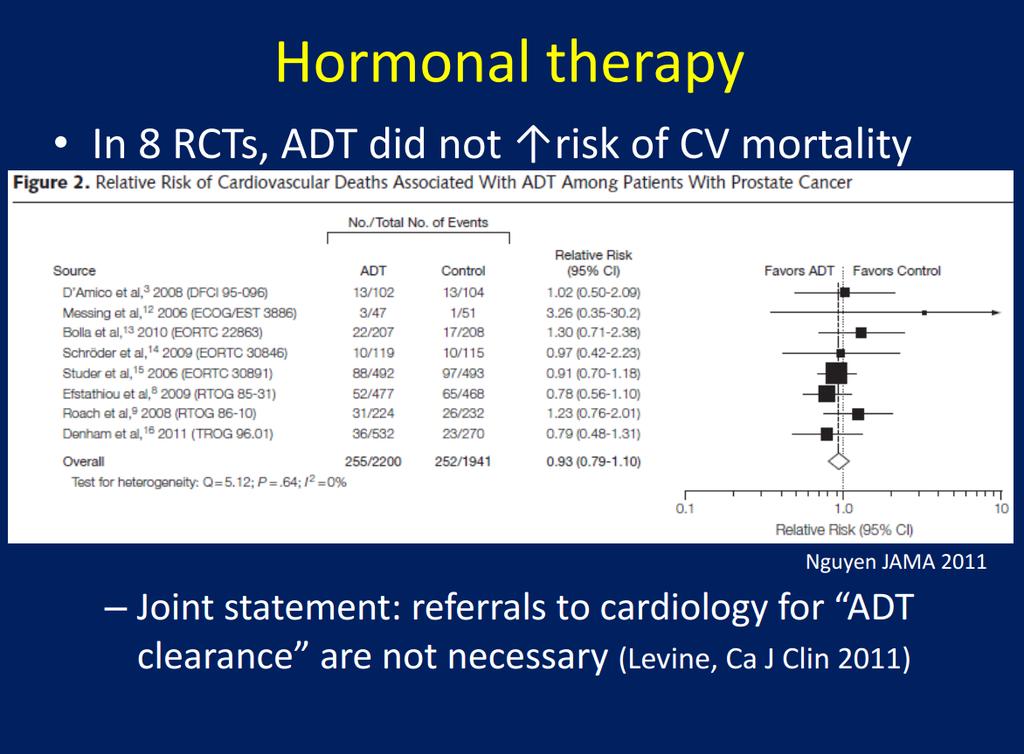
37 RT alone is inferior to RT + AA EORTC (Lancet, 2002) (Lancet Oncol, 2010) Phase III: RT vs. RT + 3 years adjuvant AA 415 patients; Median age: 71 years T3-4 or T1-2 with WHO Grade 3 Median follow-up: 9.1 years RT vs. RT + 3 yr adj. AA 10-year overall survival 39.8% 58.1% 10-year cause specific survival 69.6% 89.7% 10-year clinical DFS 22.7% 47.7% 10-year local failure 23.5% 6% 5-year bdfs (Lancet, 2002) 45% 76% * No difference in cardiovascular mortality

38 Lancet Onco, October 7, 2010
39 Long-term AA is superior to shortterm neoadjuvant/concurrent AA
40 RTOG 9202 (JCO, 2008) Phase III: 4 mos neoadj./conc. AA + RT vs. 4 mos neoadj./conc. AA + RT + 24 mos adj. AA 1521 patients; T2c-T4 and PSA <150; 4% had positive node Median follow-up: 11.3 years for alive patients Neoadj/Conc AA + RT vs. RT + Adj AA 10-year overall survival 51.6% 53.9% 10-year cause specific survival 83.9% 88.7% (p=0.004) 10-year disease free survival 13.2% 22.5% 10-year local failure 22.2% 12.3% 10-year distant metastasis 22.8% 14.8%

41 JCO, VOLUME 26 NUMBER 15 MAY
42
43 Long-term adjuvant AA is superior to short-term adjuvant AA
44 EORTC (NEJM, 2009) Phase III: RT + 6 mos adj. AA vs. RT + 3 yrs adj. AA Non-inferiority design 970 patients; median age: 69 years T2C-T4 any N or T1c-T2b pn1-n2 Median follow-up: 6.4 years RT + 6mos AA vs. RT + 3 yrs AA 5-year overall survival 81% 84.8% (HR=1.42, CI ) 5-year cause specific survival 95.3% 96.8% (HR=1.71, CI )
45
46 Short ADT vs Long ADT
47 Mean score of QoL A. Insomnia B. hot flush C. Reduced interest in sex D. Reduced sex activity E. Overall QoL

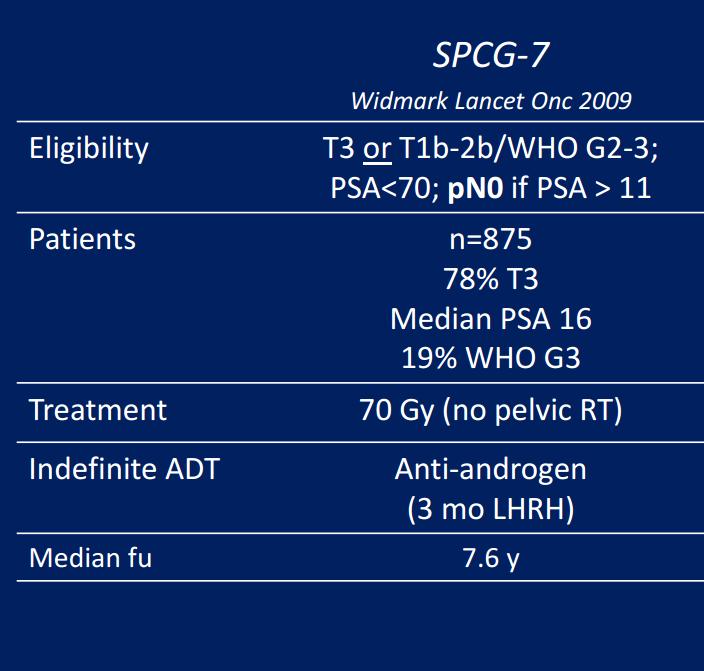
48 5. Single AA is not recommend SPCG-7 study used anti-androgens which would not be considered adequate androgen deprivation therapy
49
50 SPCG-7 study 875 patients Locally advanced (T3; 78%; PSA<70; N0; M0) randomly :439 endocrine treatment alone (3 months of GnRH agonist +AA followed by flutamide until PD VS endocrine treatment combined with RT 70 Gy. (436 patients). The primary endpoint was PC-specific survival
51 Follow-up of 7 6 years, 79 vs 37 (combined) men died of prostate cancer. 10 years for pc-specific mortality was 23 9% vs 11 9% ( 95% CI %), for a relative risk of 0 44 ( ). At 10 years overall mortality was 39 4% vs 29 6% (CI %), for a relative risk of 0 68 ( ). 10 years for PSA recurrence was substantially higher in men in the endocrine-alone group (74 7% vs 25 9%, p<0 0001; HR 0 16; ). After 5 years, urinary, rectal, and sexual problems were slightly more frequent in the endocrine plus radiotherapy group.
52 Cumulative incidence of (A) PSA recurrence, (B) death from prostate cancer, and (C) death from any cause Vol 373 January 24, 2009
53 GUIDELINE

54
55
56

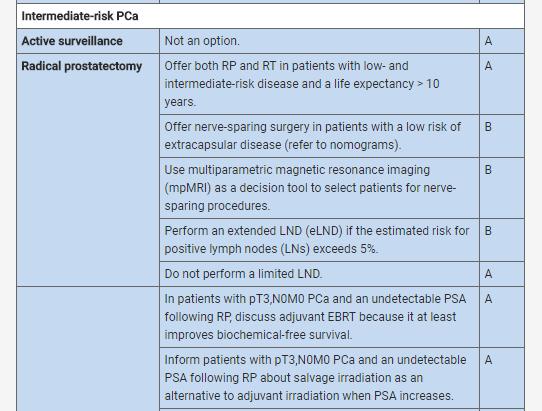
57 Intermediate risk PC: EAU 2016
58

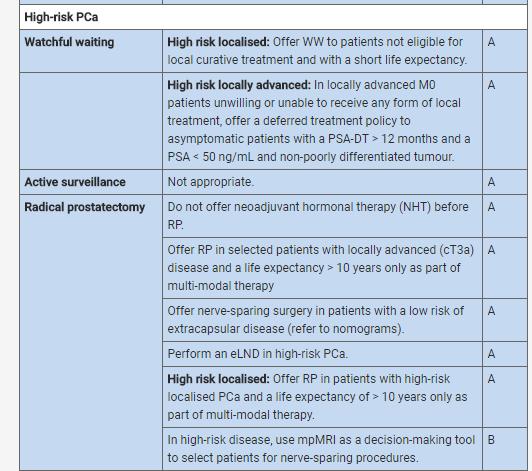
59 High Risk PC: EAU guideline
60
61
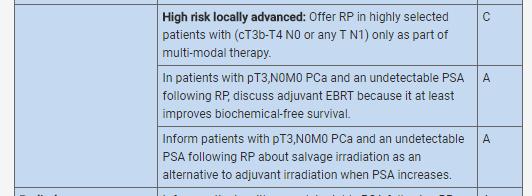
62 Comparing with surgery: no RCT High risk : cat B

63 EAU guidelines
64

65
66
67
68
69

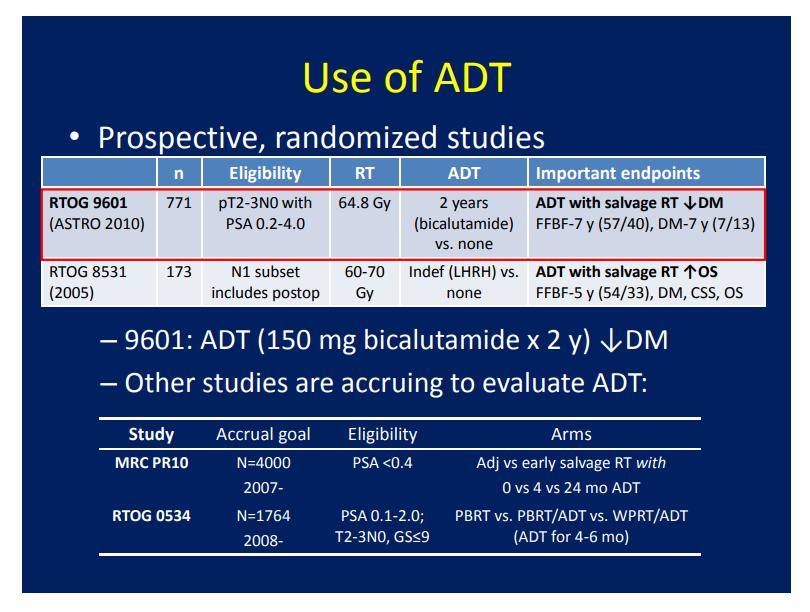
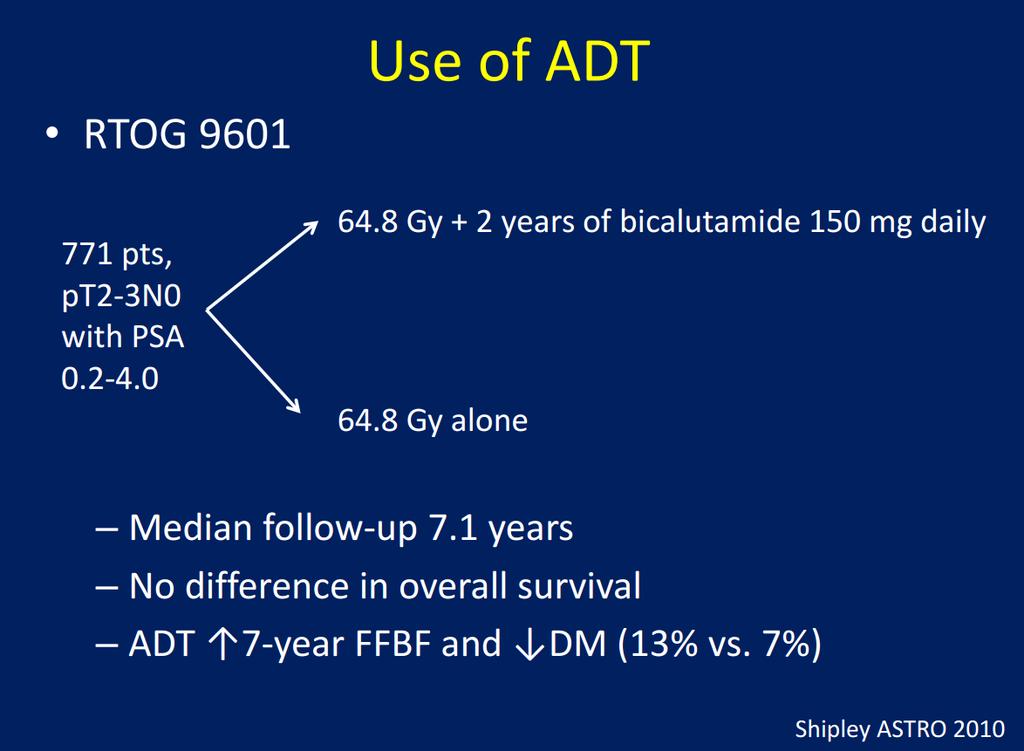
70 760 case post prostatectomy + LN ( T2,3 and node negative) then PSA rising to ng/ml RT + bicalutamide 150 mg/d * 24 months VS Rt + placebo
71 F/U 13 years OS at 12 years: 76.3% vs 71.3 % ( HR0.77, P 0.04) 12 year incidence of death from PC 5.8% vs 13.4% P Distant metastases at 12 year : 14.5% vs 23.0% (P 0.005) AE from RT similar in 2 groups Gynecomastia 69.7 % vs 10.9%
72

73


74
 เป นการร กษา adjuvant + RT in High risk or very high risk ไม")
75 National drug list ตามประกาศบ ญช ยาหล กแห งชาต 2560 ยา Leuprorelin 11.25, 22.5 และยา Triptorelin 11.25mg เป นยาบ ญช ง. เป นการร กษา Adjuvant + Rt in intermediate risk ไม เก น 6เด อน(2cycles) เป นการร กษา adjuvant + RT in High risk or very high risk ไม เก น 2ป (8 cycles)
76 Summary Role of RT + ADT well established by RCTs High risk: Long term ADT superior to short term ADT Dose RT escalation improves outcomes Waiting results of new treatment study: IMRT, new drugs Adding 24 months of AA to salvage RT improving OS and reducing cancer death


77
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate Cancer in comparison to Radiotherapy alone:
 Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
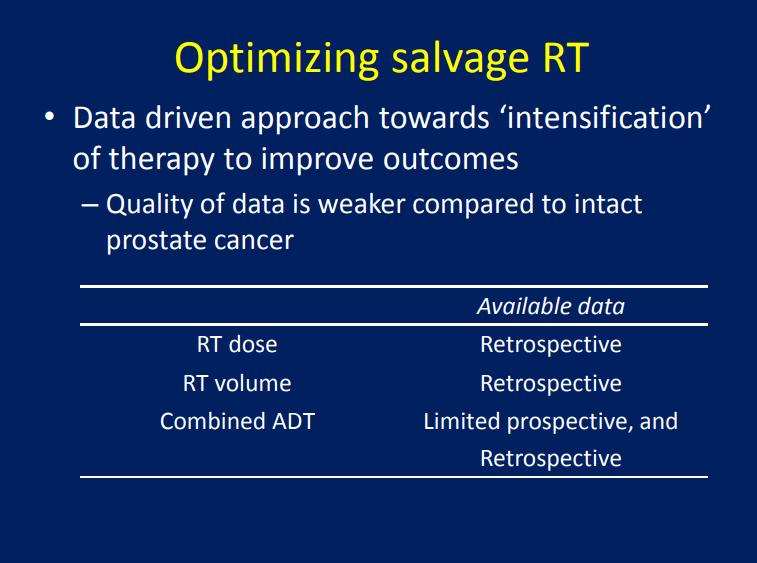
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
Androgen Deprivation Therapy A Question of Timing
 Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression
Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
majority of the patients. And taking an aggregate of all trials, very possibly has a modest effect on improved survival.
 Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Risk of renal side effects with ADT. E. David Crawford University of Colorado, Aurora, CO, USA
 Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer*
 Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Intermittent Androgen Suppression - A standard of care or a good second choice?
 Intermittent Androgen Suppression - A standard of care or a good second choice? Dr Nicholas Buchan Uro-oncology Fellow Olympic Medal Standings Gold Silver Bronze USA 9 15 13 Germany 10 13 7 Canada 14 7
Intermittent Androgen Suppression - A standard of care or a good second choice? Dr Nicholas Buchan Uro-oncology Fellow Olympic Medal Standings Gold Silver Bronze USA 9 15 13 Germany 10 13 7 Canada 14 7
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer
 Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
Urologic Oncology: Seminars and Original Investigations 30 (2012) 3 15
 3 15") Urologic Oncology: Seminars and Original Investigations 30 (2012) 3 15 Review article The multi-disciplinary management of high-risk prostate cancer Jonathan C. Picard, M.D. a, *, Ali-Reza Golshayan, M.D.
Urologic Oncology: Seminars and Original Investigations 30 (2012) 3 15 Review article The multi-disciplinary management of high-risk prostate cancer Jonathan C. Picard, M.D. a, *, Ali-Reza Golshayan, M.D.
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Prostate Cancer Case Study 2. Medical Student Case-Based Learning
 Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer
 Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer 100 80 60 Cancer Death Rates for Men, US 1930-2002 Rate Per 100,000 Lung William K. Oh, M.D. 40 Stomach Colon & rectum Prostate
Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer 100 80 60 Cancer Death Rates for Men, US 1930-2002 Rate Per 100,000 Lung William K. Oh, M.D. 40 Stomach Colon & rectum Prostate
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
ERLEADA (apalutamide) oral tablet
 oral tablet") ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Francesco Bertoldo. Metabolic Bone Diseases and Osteoncology Unit DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY
 DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY Francesco Bertoldo Metabolic Bone Diseases and Osteoncology Unit Department of Medicine University di Verona EPIDEMIOLGY OF PROSTATE CANCER Prostate
DRUG INDUCED S OSTEOPOROSIS: ANDROGEN DEPRIVATION THERAPY Francesco Bertoldo Metabolic Bone Diseases and Osteoncology Unit Department of Medicine University di Verona EPIDEMIOLGY OF PROSTATE CANCER Prostate
When radical prostatectomy is not enough: The evolving role of postoperative
 When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
The Current State of Hormonal Therapy for Prostate Cancer
 The Current State of Hormonal Therapy for Prostate Cancer The Current State of Hormonal Therapy for Prostate Cancer Beth A. Hellerstedt, MD; Kenneth J. Pienta, MD Dr. Hellerstedt is Fellow, Division of
The Current State of Hormonal Therapy for Prostate Cancer The Current State of Hormonal Therapy for Prostate Cancer Beth A. Hellerstedt, MD; Kenneth J. Pienta, MD Dr. Hellerstedt is Fellow, Division of
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer
 Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Review of Polish and international guidelines on hormonal therapy in localized prostate cancer
 Review article NOWOTWORY Journal of Oncology 2016, volume 66, number 5, 403 407 DOI: 10.5603/NJO.2016.0071 Polskie Towarzystwo Onkologiczne ISSN 0029 540X www.nowotwory.edu.pl Review of Polish and international
Review article NOWOTWORY Journal of Oncology 2016, volume 66, number 5, 403 407 DOI: 10.5603/NJO.2016.0071 Polskie Towarzystwo Onkologiczne ISSN 0029 540X www.nowotwory.edu.pl Review of Polish and international
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Applications of Quality of Life Outcomes in Three Recent NCIC CTG Trials: What Every New Clinician-Investigator Wants to Know
 Workshop # 5 Applications of Quality of Life Outcomes in Three Recent NCIC CTG Trials: What Every New Clinician-Investigator Wants to Know M. Brundage and H. Richardson Outline Nature of QOL data a brief
Workshop # 5 Applications of Quality of Life Outcomes in Three Recent NCIC CTG Trials: What Every New Clinician-Investigator Wants to Know M. Brundage and H. Richardson Outline Nature of QOL data a brief
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Manipulating Hormones: Androgen Suppression in Prostate Cancer Patients
 Focus on CME at the University of Queen s ManitobaUniversity Manipulating Hormones: Androgen Suppression in ostate Cancer Patients By D. Robert Siemens, MD, FRCSC Case A 62-year old man presents with complaints
Focus on CME at the University of Queen s ManitobaUniversity Manipulating Hormones: Androgen Suppression in ostate Cancer Patients By D. Robert Siemens, MD, FRCSC Case A 62-year old man presents with complaints
To treat or not to treat: When to treat! A case presentation
 To treat or not to treat: When to treat! A case presentation Filip Ameye, MD,Phd Universitary Hospitals Leuven, Belgium Departement of Urology Prostate Center A case presentation Pt. 76 y. Mild LUTS (07/1999)
To treat or not to treat: When to treat! A case presentation Filip Ameye, MD,Phd Universitary Hospitals Leuven, Belgium Departement of Urology Prostate Center A case presentation Pt. 76 y. Mild LUTS (07/1999)
Androgen Deprivation Therapy Its impact and the nursing role. Jane Thacker Uro-Oncology Nurse Specialist
 Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Radiation with oral hormonal manipulation for non-metastatic, intermediate or high risk prostate cancer in men 70 and older or with comorbidities
 Radiation with oral hormonal manipulation for non-metastatic, intermediate or high risk prostate cancer in men 70 and older or with comorbidities Prostate cancer is predominately a disease of older men,
Radiation with oral hormonal manipulation for non-metastatic, intermediate or high risk prostate cancer in men 70 and older or with comorbidities Prostate cancer is predominately a disease of older men,
EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER
 EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER Abraham Morgentaler, MD Director and Founder Men s Health Boston Associate Clinical Professor Harvard Medical School And the Urology
EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER Abraham Morgentaler, MD Director and Founder Men s Health Boston Associate Clinical Professor Harvard Medical School And the Urology
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository:
 This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/103187/ This is the author s version of a work that was submitted to / accepted
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/103187/ This is the author s version of a work that was submitted to / accepted
Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy).
.") Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER
 PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
reviews LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate therapy
 reviews therapy LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate Martin I. Resnick, MD, Lester Persky Professor and Chief, Department of Urology, Case Western Reserve University School
reviews therapy LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate Martin I. Resnick, MD, Lester Persky Professor and Chief, Department of Urology, Case Western Reserve University School
Medical Treatments for Prostate Cancer
 Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels?
 ORIGINAL PAPER DOI: 10.4081/aiua.2017.4.282 Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels? Murat Bagcioglu
ORIGINAL PAPER DOI: 10.4081/aiua.2017.4.282 Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels? Murat Bagcioglu
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Androgen deprivation therapy: New concepts. Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto
 Androgen deprivation therapy: New concepts Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto Clinical Research funding: 1. Bayer/Algeta 2. Ferring 3. Abbott 4. GSK 5. EMD Serono
Androgen deprivation therapy: New concepts Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto Clinical Research funding: 1. Bayer/Algeta 2. Ferring 3. Abbott 4. GSK 5. EMD Serono
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
The Spa Hotel, Tunbridge Wells Friday 23 rd March Platinum sponsor
 The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice
 european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
SRO Tutorial: Prostate Cancer Clinics
 SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
Edward P. Gelmann, MD
 Prostate Cancer Edward P. Gelmann, MD Prostate Cancer Etiology and Ep pidemiology Screening Pathology Staging Localized Disease Metastatic Disease normal prostate epithelium GSTP1 CpG island hypermethylation
Prostate Cancer Edward P. Gelmann, MD Prostate Cancer Etiology and Ep pidemiology Screening Pathology Staging Localized Disease Metastatic Disease normal prostate epithelium GSTP1 CpG island hypermethylation
Final Appraisal Report. Ferring Pharmaceuticals Ltd. Advice No: 2109 December Recommendation of AWMSG
 Final Appraisal Report Degarelix (Firmagon ) for the treatment of advanced hormone-dependent prostate cancer Ferring Pharmaceuticals Ltd Advice No: 2109 December 2009 Recommendation of AWMSG Degarelix
Final Appraisal Report Degarelix (Firmagon ) for the treatment of advanced hormone-dependent prostate cancer Ferring Pharmaceuticals Ltd Advice No: 2109 December 2009 Recommendation of AWMSG Degarelix
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Use of Ovarian Suppression and Ablation in Breast Cancer Treatment
 Use of Ovarian Suppression and Ablation in Breast Cancer Treatment Dr Marina Parton Consultant Medical Oncologist Royal Marsden and Kingston Hospitals Overview Breast cancer phenotypes Use of ovarian manipulation
Use of Ovarian Suppression and Ablation in Breast Cancer Treatment Dr Marina Parton Consultant Medical Oncologist Royal Marsden and Kingston Hospitals Overview Breast cancer phenotypes Use of ovarian manipulation
Oligometastasis. Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie?
 Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of