Stomach. R.B. Kolachalam, MD
|
|
|
- Arron Ball
- 5 years ago
- Views:
Transcription
1 Stomach R.B. Kolachalam, MD
2
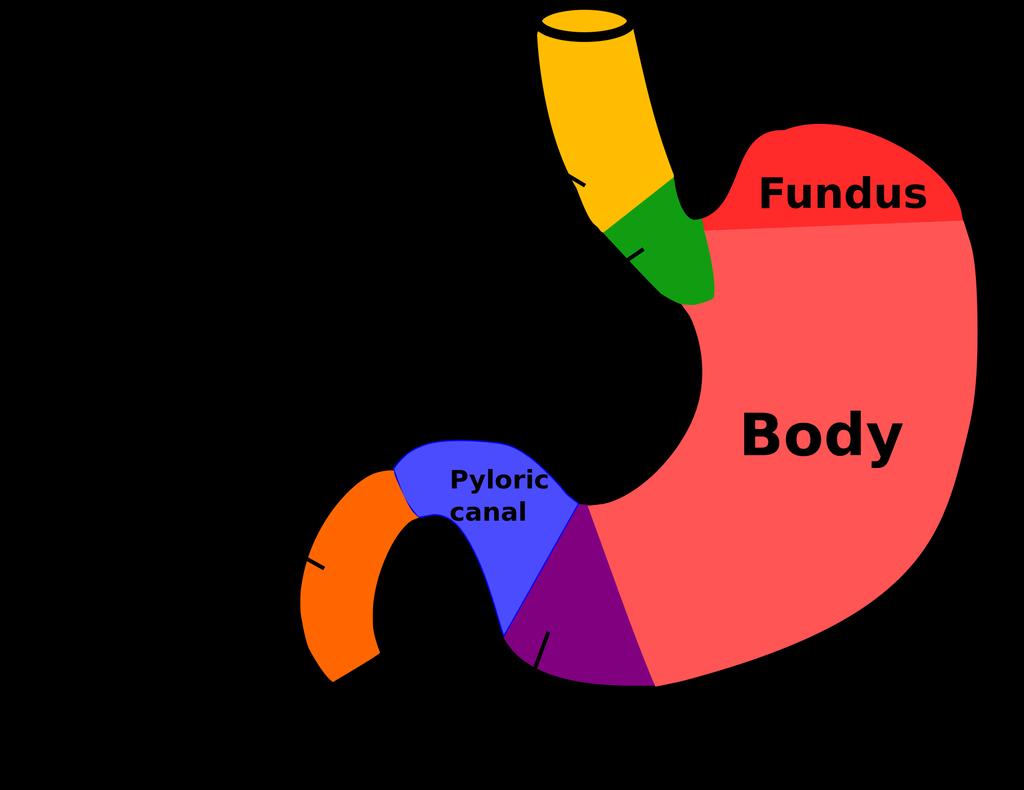
3 Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum
4 Gastric Anatomy body of the stomach: site of mechanical agitation of food fundus: site of receptive relaxation
5 Arterial blood supply of the stomach Primarily from the Celiac artery left, and right gastric arteries right and left gastoduodenal arteries aberrant /replaced left hepatic artery from the left gastric artery (15-24%)
6 Arterial supply to the gastric conduit in esophagectomy is primarily based on the right gastroepiploic artery
7 Venous and lymphatic drainage corresponds to the arterial supply veins empty either directly into the portal vein or into one of its tributaries, the splenic or SMV Lymphatics form anastomosis in the gastric wall-hence the 5cm requirements for resection
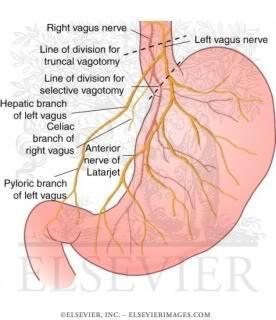
8 Innervation of the Stomach left vagus-anterior, right vagus-posterior (LARP) Anterior and Posterior Nerves of Laterjet Crows feet at the incissura criminal Nerve of Grassi
9
10 Physiologic consequences of Vagotomy BAO-reduced by 80% exogenous stimulants (pentagastrin) -50 to 70% decrease endogenous stimulation-down by 70% altered emptying-loss of receptive relaxation of fundus leads to accelerated emptying of liquids
11 Gastric Physiology parietal cells-acid and intrinsic factor chief cells (pepsinogeneral is a chief) - pepsinogen G cells-gastrin ECL cells-histamine-stimulates parietal cells via cyclic AMP
12 Gastric physiology-cont secretin- s cells in duodenum and jejunuminhibits release of gastrin, gastric acid secretion and gastric motility. Bombesin (GRP) universl on switch. Somatostatin- off switch E-mycin stimulates motility through activation of motilin receptors
13 Gastric physiology Secretin: paradoxical increase in serum gastrin levels in patients with gastrinoma
14 H.Pylori implicated in : peptic ulcer disease chronic gastric atrophy and intestinal metaplasia-gastric cancer Malt lymphoma
15 H.pylori only human bacterium to persistently infect the stomach binds only to gastric-type of epithelium regardless of location 90-95% of DU and 70-75% of gastric ulcers are H.pylori positive Only 10-15% of infected people develop peptic ulcerations and only 1% develop gastric cancers.
16 H.pylori: virulence factors vacuolating cytotoxin A (VacA) cytotoxin-associated gene A(CagA)
17 H.pylori testing Invasive and non-invasive tests urea breath test, test of choice for documentation of H.pylori eradication
18 H.pylori treatment proton pump inhibitors, usually with two antibiotics, usually clarithromycin and flagyl,or amoxicillin. combination of antibiotics more effective, therapy for 7 or 14 days eradication rates over 90%
19 Gastric ulcer type 1: type A blood, other types associated with type O. on lesser curve. low acid secretion type 2: 2 ulcers-du, and lesser curve. High acid type 3: pre-pyloric. high associated type 4: high lesser curve-not associated with high acid type 5: NSAID induced, not related to H.pylori, no specific location
20 Gastric ulcer management unlike DU, less association with H. pylori, and reduced acid secretion medical management is to eradicate h.pylori. multiple biopsies needed to exclude malignant
21 Gastric ulcer-surgical therapy type 1 (60%): distal gastrectomy with B-1. Vagotomy not needed type 2, and 3 behave like DU and are treated as such. type 4: distal gastrectomy with extension along the lesser curve (Pauchet procedure),or Rouxen-Y. no vagotomy needed
22 Duodenal ulcers eradication of H. pylori reduces the recurrence rates to 6% prevalence of H.pylori lower in patients with complicated DU
23 Surgical management of DU? only indication for elective surgery-intractable recurrent symptoms of DU despite adequate medical treatment in the absence of H.pylori patients at high risk for ulcer complications (transplant recipients, steroid or NSAID dependency, giant ulcer)
24 Surgical management of DU parietal vagotomy-lower morbidity, but higher recurrence rates truncal vagotomy and B 1, or drainage procedures.
25 Complications of Peptic ulcers 1. Hemorrhage 2. Perforation 3. Gastric outlet obstruction
26 Hemorrhage from peptic ulcer disease initial resuscitation and medical management early endoscopy to assess the cause and severity, and treat endoscopically if possible prevention of recurrences with H.pylori eradication continued hemodynamic instability may need interventional radiology techniques or surgery
27 Bleeding Gastric ulcers need excisional therapy-distal gastrectomy with B-1, or in unstable patients ulcer excision or oversewing of the ulcer
28 Bleeding Duodenal ulcer three point ligation, and pyloroplasty. truncal vagotomy in stable patients H.pylori eradication
29 Complications of ulcer disease: perforation DU- omental patch closure, with post-operative H.pylori eradication GU- partial gastrectomy is prefered. In high risk patients-ulcer excision, or biopsy and over sew
30 Gastric outlet obstruction the most common cause of GOO in adults is malignancy Endoscopy is needed to rule out malignancy correction of acid and electrolyte imbalances, and hydration is key. make sure the patient is nutritionally optimized, and gastric tone regained. only 40% of patients have sustained improvement in 3 months distal gastrectomy is the usual operation of choice
31 Gastric Cancer Incidence is decreasing. M>F. Africanamerican>White 55% present with locally advanced or metastatic disease proximal gastric cancer s increasing
32 Gastric cancer: Histological subtypes: Intestinal diffuse
33 Intestinal type of Gastric Cancer distal stomach elderly atrophic gastritis, and diets high in nitrates, and nit rose compounds
34 Diffuse gastric cancer younger patients no identifiable precursor predilection for the cardia diffuse thickening worse prognosis not associated with H.pylori
35 Gastric cancer staging locoregional disease (AJCC stage 1-3) and systemic disease (AJCC stage 4) CT accuracy 70% for advanced disease and 44% for early disease EUS-superior to CT in the regional staging. Staging laparoscopy
36 Gastric Cancer: Controversies in surgical management Extent of gastric resection extent of lymph node dissection optima approach to proximal lesions role of splenectomy and adjacent organ resection role of neoadjuvant therapy for locally advanced gastric tumors
37 Extent of gastric resection R0 has survival benefit proximal margins of 5-6cm, with frozen section no benefit for total gastrectomy in distal cancers total gastrectomy for most cancers of the funds and proximal stomach esophagogastrectomy for tumors of the cardia and the GEJ
38 Lymph node dissection for gastric cancer D1,D2, or D3 dissection 15 nodes needed for pathological staging resection of pancreatic tail, spleen reserved for direct involvement
39 Adjuvant therapy of Gastric cancer combined chemoradiation is the standard adjuvant therapy in US. Adjuvant therapy is avoided in R0 resections in Europe.
40 Neoadjuvant therapy: Gastric cancer NCCN recommends neoadjuvant therapy for locally advanced (T3 or node + disease on EUS)
41 Gastric lymphoma non-hodgkin type B symptoms rare risk factors-h.pylori, immunosuppression, celiac disease, IBD, and HIV infection
42 Gastric lymphoma: management shift away from surgical management even in localized disease (stomach and perigastric nodes) 45% are MALT lymphoma s-treated with anti-h.pylori therapy. for localized persistent therapy radiation or chemotherapy is used for the 55% of high grade lymphoma s -treated with chemo and radiation surgery only for bleeding or perforation complications
43 GIST tumors stomach is the most common site-70% from the precursor of the interstitial cells of Cajal diagnosis is by staining for the KIT receptor (CD 117)- 95%.
44 GIST tumors avoid biopsy for resectable lesions tumor size and mitosis most important prognostic factors Negetive margins. no node dissection for moderate to high risk recurrence, adjuvant Imatinib-selective KIT inhibitor also used for borderline resectable lesions before surgery
45 Gastric Carcinoid three types. type 1 associated with chronic atrophic gastritis. type 2: associated with ZE syndrome and MEN- 1 type 3: (sporadic), biologically aggressive, no hypergastrinoma.
46 Gastric Carcinoid tumors endoscopic or open resection for type 1 and 2 tumors type 3 require gastric resection with ELND.
47
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcers. Dr V. Roudnitsky KCH
 Perforated peptic ulcers Dr V. Roudnitsky KCH Peptic ulcer disease Peptic ulcers are focal defects in the gastric or duodenal mucosa that extend into the submucosa or deeper Caused by an imbalance between
Perforated peptic ulcers Dr V. Roudnitsky KCH Peptic ulcer disease Peptic ulcers are focal defects in the gastric or duodenal mucosa that extend into the submucosa or deeper Caused by an imbalance between
OPERATIVE TREATMENT OF ULCER DISEASE
 Página 1 de 8 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Página 1 de 8 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
STOMACH and DUODENUM DISEASE
 STOMACH and DUODENUM DISEASE STOMACH ANATOMY In the living and upright posture, the stomach is a j-shaped. It has two surfaces, two curvatures and two openings. Esophagus Fundus cardia Pylorus B o d y
STOMACH and DUODENUM DISEASE STOMACH ANATOMY In the living and upright posture, the stomach is a j-shaped. It has two surfaces, two curvatures and two openings. Esophagus Fundus cardia Pylorus B o d y
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
KK College of Nursing Peptic Ulcer Badil D ass Dass, Lecturer 25th July, 2011
 KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
Update on the pathological classification of gastritis. Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada
 Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
AN ARGUMENT FOR SURGERY FOR GASTRINOMA. Lauren Wilson R1 General Surgery
 AN ARGUMENT FOR SURGERY FOR GASTRINOMA Lauren Wilson R1 General Surgery WHAT IS A GASTRINOMA? Gastrin secreting cells derived from multipotential stem cells of endodermal origin or enteroendocrine cells
AN ARGUMENT FOR SURGERY FOR GASTRINOMA Lauren Wilson R1 General Surgery WHAT IS A GASTRINOMA? Gastrin secreting cells derived from multipotential stem cells of endodermal origin or enteroendocrine cells
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
B Breast cancer, managing risk of lobular, in hereditary diffuse gastric cancer, 51
 Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ.
 Professor of Surgery, Taibah Univ.") By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Patient. Male 76 year old C.C: abdominal pain
 Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Stomach and duodenum Omar alnoubani MD,MRCS
 Stomach and duodenum Omar alnoubani MD,MRCS asymmetrical, pearshaped,most proximal abdominal organ of the digestive tract. Cardia connected to esophagus. Fundus bounded superiorly by diaphragm and laterally
Stomach and duodenum Omar alnoubani MD,MRCS asymmetrical, pearshaped,most proximal abdominal organ of the digestive tract. Cardia connected to esophagus. Fundus bounded superiorly by diaphragm and laterally
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
GASTRIC CANCER. Joyce Au SUNY Downstate Grand Rounds July 11, 2013
 GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
Done by: Dina Sawadha & Mohammad Abukabeer
 Done by: Dina Sawadha & Mohammad Abukabeer The stomach *the stomach is a dilated part of the gastro intestinal tract, it's "J" shape. *the lower surface of the stomach ( the greater curvature ) reaches
Done by: Dina Sawadha & Mohammad Abukabeer The stomach *the stomach is a dilated part of the gastro intestinal tract, it's "J" shape. *the lower surface of the stomach ( the greater curvature ) reaches
It passes through the diaphragm at the level of the 10th thoracic vertebra to join the stomach
 The esophagus is a tubular structure (muscular, collapsible tube ) about 10 in. (25 cm) long that is continuous above with the laryngeal part of the pharynx opposite the sixth cervical vertebra The esophagus
The esophagus is a tubular structure (muscular, collapsible tube ) about 10 in. (25 cm) long that is continuous above with the laryngeal part of the pharynx opposite the sixth cervical vertebra The esophagus
5. Which component of the duodenal contents entering the stomach causes the most severe changes to gastric mucosa:
 Gastro-intestinal disorders 1. Which are the most common causes of chronic gastritis? 1. Toxic substances 2. Chronic stress 3. Alimentary factors 4. Endogenous noxious stimuli 5. Genetic factors 2. Chronic
Gastro-intestinal disorders 1. Which are the most common causes of chronic gastritis? 1. Toxic substances 2. Chronic stress 3. Alimentary factors 4. Endogenous noxious stimuli 5. Genetic factors 2. Chronic
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY PEPTIC ULCER DISEASE PC Bornman RS Du Toit EPIDEMIOLOGY AND PATHOGENESIS The prevalence of duodenal ulcer disease has a variable geographical distribution and differs
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY PEPTIC ULCER DISEASE PC Bornman RS Du Toit EPIDEMIOLOGY AND PATHOGENESIS The prevalence of duodenal ulcer disease has a variable geographical distribution and differs
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Subepithelial Lesions of the Gut: When Should I Worry?
 Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
TUMORS OF THE STOMACH AND SMALL BOWEL
 gastrointestinal tract and abdomen TUMORS OF THE STOMACH AND SMALL BOWEL L. Mark Knab, MD, David J. Bentrem, MD, FACS, and Jeffrey D. Wayne, MD, FACS * Gastric Adenocarcinoma The incidence of gastric carcinoma
gastrointestinal tract and abdomen TUMORS OF THE STOMACH AND SMALL BOWEL L. Mark Knab, MD, David J. Bentrem, MD, FACS, and Jeffrey D. Wayne, MD, FACS * Gastric Adenocarcinoma The incidence of gastric carcinoma
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Gastrinoma: Medical Management. Haley Gallup
 Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Emergency Operations for Bleeding Duodenal Ulcer:A simple option to consider Case Report Abstract Key words Case Report
 Vtáx exñéüà :A simple option to consider: Case Report Gamal E H A El Shallaly, Eltayeb A Ali, Suzan Salih Abstract We report a 46 years-old man who had severe bleeding from a posterior duodenal ulcer (DU)
Vtáx exñéüà :A simple option to consider: Case Report Gamal E H A El Shallaly, Eltayeb A Ali, Suzan Salih Abstract We report a 46 years-old man who had severe bleeding from a posterior duodenal ulcer (DU)
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Rare GI Malignancies
 Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Helicobacter and gastritis
 1 Helicobacter and gastritis Dr. Hala Al Daghistani Helicobacter pylori is a spiral-shaped gram-negative rod. H. pylori is associated with antral gastritis, duodenal (peptic) ulcer disease, gastric ulcers,
1 Helicobacter and gastritis Dr. Hala Al Daghistani Helicobacter pylori is a spiral-shaped gram-negative rod. H. pylori is associated with antral gastritis, duodenal (peptic) ulcer disease, gastric ulcers,
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
BY DR NOMAN ULLAH WAZIR
 BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
The Nobel Prize in Physiology or Medicine for 2005
 The Nobel Prize in Physiology or Medicine for 2005 jointly to Barry J. Marshall and J. Robin Warren for their discovery of "the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer
The Nobel Prize in Physiology or Medicine for 2005 jointly to Barry J. Marshall and J. Robin Warren for their discovery of "the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer
Our gut reactions to food or, gut reactions - to food
 Key concepts in Digestion. Our gut reactions to food or, gut reactions to food Prof. Barry Campbell Cellular & Molecular Physiology email: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl Swallowing
Key concepts in Digestion. Our gut reactions to food or, gut reactions to food Prof. Barry Campbell Cellular & Molecular Physiology email: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl Swallowing
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
PRIMARY GASTRIC LYMPHOMA: CASE REPORT WITH REVIEW OF LITERATURE
 PRIMARY GASTRIC LYMPHOMA: CASE REPORT WITH REVIEW OF LITERATURE Rana K. Sherwani, *Kafil Akhtar, Noorin Zaidi, Anjum Ara Department of Pathology, J.N. Medical College, Aligarh Muslim University, Aligarh,
PRIMARY GASTRIC LYMPHOMA: CASE REPORT WITH REVIEW OF LITERATURE Rana K. Sherwani, *Kafil Akhtar, Noorin Zaidi, Anjum Ara Department of Pathology, J.N. Medical College, Aligarh Muslim University, Aligarh,
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adherence, to bismuth quadruple therapy, 543 546 Adjuvant therapy, probiotics as, 567 569 Age factors, in gastric cancer, 611 612, 616 AID protein,
Note: Page numbers of article titles are in boldface type. A Adherence, to bismuth quadruple therapy, 543 546 Adjuvant therapy, probiotics as, 567 569 Age factors, in gastric cancer, 611 612, 616 AID protein,
Disease of the Stomach
 Disease of the Stomach Jack Bragg, D.O., F.A.C.O.I. Associate Professor of Internal Medicine Division of Gastroenterology University of Missouri School of Medicine Columbia, Missouri I have no disclosures
Disease of the Stomach Jack Bragg, D.O., F.A.C.O.I. Associate Professor of Internal Medicine Division of Gastroenterology University of Missouri School of Medicine Columbia, Missouri I have no disclosures
Pancreas and Biliary System
 Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
CLINICAL EFFECTIVENESS
 Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Re-audit of gastrointestinal tract specimens with respect to compliance with RCPath guidelines Dr Manisha Ram Dr Moina Kadri Background epidemiology and aetiology Over the past 20 years there has been
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
Association of Helicobacter pylori infection with Atrophic gastritis in patients with Dyspepsia
 ADVANCES IN BIORESEARCH Adv. Biores., Vol 8 [3] May 2017: 137-141 2017 Society of Education, India Print ISSN 0976-4585; Online ISSN 2277-1573 Journal s URL:http://www.soeagra.com/abr.html CODEN: ABRDC3
ADVANCES IN BIORESEARCH Adv. Biores., Vol 8 [3] May 2017: 137-141 2017 Society of Education, India Print ISSN 0976-4585; Online ISSN 2277-1573 Journal s URL:http://www.soeagra.com/abr.html CODEN: ABRDC3
Peptic Ulcer Disease Update
 Peptic Ulcer Disease Update Col Pat Storms RAM 2005 Disclosure Information 84th Annual AsMA Scientific Meeting Col Patrick Storms I have no financial relationships to disclose. I will discuss the following
Peptic Ulcer Disease Update Col Pat Storms RAM 2005 Disclosure Information 84th Annual AsMA Scientific Meeting Col Patrick Storms I have no financial relationships to disclose. I will discuss the following
Original Report. Carcinoid Tumors of the Stomach: A Clinical and Radiographic Study
 Aaron J. Binstock 1 C. Daniel Johnson 1 David H. Stephens 1 Ricardo V. Lloyd 2 Joel G. Fletcher 1 Received July 25, 2000; accepted after revision September 29, 2000. 1 Department of Radiology, Mayo Clinic,
Aaron J. Binstock 1 C. Daniel Johnson 1 David H. Stephens 1 Ricardo V. Lloyd 2 Joel G. Fletcher 1 Received July 25, 2000; accepted after revision September 29, 2000. 1 Department of Radiology, Mayo Clinic,
Definition gastritis
 Gastritis Definition The term gastritis is used to denote inflammation associated with mucosal injury Gastritis is mostly a histological term that needs biopsy to be confirmed Gastritis is usually due
Gastritis Definition The term gastritis is used to denote inflammation associated with mucosal injury Gastritis is mostly a histological term that needs biopsy to be confirmed Gastritis is usually due
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Epidemiology of Peptic Ulcer Disease
 Epidemiology of Peptic Ulcer Disease Introduction Peptic Ulcer Disease (PUD) is disruption of the mucosal integrity of the stomach and/or duodenum leading to a local defect or excavation due to active
Epidemiology of Peptic Ulcer Disease Introduction Peptic Ulcer Disease (PUD) is disruption of the mucosal integrity of the stomach and/or duodenum leading to a local defect or excavation due to active
Helicobacter Pylori Testing HELICOBACTER PYLORI TESTING HS-131. Policy Number: HS-131. Original Effective Date: 9/17/2009
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Helicobacter pylori: Diagnosis, treatment and risks of untreated infection
 Helicobacter pylori: Diagnosis, treatment and risks of untreated infection Klaus Mönkemüller Department of Gastroenterology, Hepatology und Infectius Diseases Otto-von-Guericke University, Magdeburg bb
Helicobacter pylori: Diagnosis, treatment and risks of untreated infection Klaus Mönkemüller Department of Gastroenterology, Hepatology und Infectius Diseases Otto-von-Guericke University, Magdeburg bb
How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective. Aravind Suppiah; Sarah K.
 How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective Aravind Suppiah; Sarah K. Thompson ANZGOSA database Commenced 2010; 1469 cases (2002 2014)
How the ANZGOSA audit can benefit your practice: a look at GIST surgery from an Australian and NZ perspective Aravind Suppiah; Sarah K. Thompson ANZGOSA database Commenced 2010; 1469 cases (2002 2014)
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT.
 PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
The Spleen. Dr Fahad Ullah
 The Spleen BY Dr Fahad Ullah Spleen The spleen is an largest lymphoid organ shaped like a shoe that lies relative to the 9th and 11th ribs and is located in the left hypochondrium. Thus, the spleen is
The Spleen BY Dr Fahad Ullah Spleen The spleen is an largest lymphoid organ shaped like a shoe that lies relative to the 9th and 11th ribs and is located in the left hypochondrium. Thus, the spleen is
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Peptic Ulcer Disease: Zollinger-Ellison Syndrome
 GASTROINTESTINAL PHYSIOLOGY 235 Case 41 Peptic Ulcer Disease: Zollinger-Ellison Syndrome Abe Rosenfeld, who is 47 years old, owns a house painting business with his brothers. The brothers pride themselves
GASTROINTESTINAL PHYSIOLOGY 235 Case 41 Peptic Ulcer Disease: Zollinger-Ellison Syndrome Abe Rosenfeld, who is 47 years old, owns a house painting business with his brothers. The brothers pride themselves
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori
 Gut and Liver, Vol. 6, No. 2, April 2012, pp. 270-274 CASE REPORT Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori Soo-Kyung Park, Hwoon-Yong Jung, Do Hoon Kim,
Gut and Liver, Vol. 6, No. 2, April 2012, pp. 270-274 CASE REPORT Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori Soo-Kyung Park, Hwoon-Yong Jung, Do Hoon Kim,
-12. -Renad Habahbeh. -Dr Mohammad mohtasib
 -12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
-12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
Diagnosis abnormal morphology and /or abnormal biochemistry
 Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
2nd week. preexam. GIT system. Atyaf group. Qs team
 2nd week preexam GIT system Qs team 2nd week 2009 Atyaf group بسم االله الرحمن الرحيم 1) a patient with autoimmune gastritis. He is not likely to develop: A. H.pylori colonization. B. pernicious anemia.
2nd week preexam GIT system Qs team 2nd week 2009 Atyaf group بسم االله الرحمن الرحيم 1) a patient with autoimmune gastritis. He is not likely to develop: A. H.pylori colonization. B. pernicious anemia.
Gastric Tumors Dr. Taha
 Gastric Tumors Dr. Taha BENIGN TUMORS: Leiomyomas: smooth muscle tumors, equal in men /women, typically located in the middle &distal stomach. Can grow into the lumen with secondary ulceration & bleeding.
Gastric Tumors Dr. Taha BENIGN TUMORS: Leiomyomas: smooth muscle tumors, equal in men /women, typically located in the middle &distal stomach. Can grow into the lumen with secondary ulceration & bleeding.
CT EVALUATION OF GASTRIC LESIONS:
 CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
AATS Focus on Thoracic Surgery: Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017?
 AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Overview of digestion or, gut reactions - to food
 Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions - to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology e-mail: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
Key concepts in Digestion. Indigestion module Overview of digestion or, gut reactions - to food Prof. Barry Campbell Gastroenterology Cellular & Molecular Physiology e-mail: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl
GI Pharmacology. Dr. Alia Shatanawi 5/4/2018
 GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Z Gastroenterol. 1983 Mar;21 Suppl:111-6. [Effect of antacids on intestinal motility]. [Article in German] Wienbeck M, Erckenbrecht J, Strohmeyer G. Abstract
GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Z Gastroenterol. 1983 Mar;21 Suppl:111-6. [Effect of antacids on intestinal motility]. [Article in German] Wienbeck M, Erckenbrecht J, Strohmeyer G. Abstract
THE SURGEON S LIBRARY
 THE SURGEON S LIBRARY THE HISTORY AND SURGICAL ANATOMY OF THE VAGUS NERVE Lee J. Skandalakis, M.D., Chicago, Illinois, Stephen W. Gray, PH.D., and John E. Skandalakis, M.D., PH.D., F.A.C.S., Atlanta, Georgia
THE SURGEON S LIBRARY THE HISTORY AND SURGICAL ANATOMY OF THE VAGUS NERVE Lee J. Skandalakis, M.D., Chicago, Illinois, Stephen W. Gray, PH.D., and John E. Skandalakis, M.D., PH.D., F.A.C.S., Atlanta, Georgia
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Proximal Gastric Vagotomy Without Drainage for Treatment of Perforated Duodenal Ulcer
 GASTROENTEROLOGY 1982;179-83 Proximal Gastric Vagotomy Without Drainage for Treatment of Perforated Duodenal Ulcer PAUL H. JORDAN, Jr. Surgical Services of the Cora and Webb Mading Department of Surgery,
GASTROENTEROLOGY 1982;179-83 Proximal Gastric Vagotomy Without Drainage for Treatment of Perforated Duodenal Ulcer PAUL H. JORDAN, Jr. Surgical Services of the Cora and Webb Mading Department of Surgery,
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
594 Lewin, Weinstein, and Riddell s Gastrointestinal Pathology and Its Clinical Implications
 594 Lewin, Weinstein, and Riddell s Gastrointestinal Pathology and Its Clinical Implications Figure 13-20. Stages in the natural history of H. pylori. Biopsies from the antrum are on the left and the oxyntic
594 Lewin, Weinstein, and Riddell s Gastrointestinal Pathology and Its Clinical Implications Figure 13-20. Stages in the natural history of H. pylori. Biopsies from the antrum are on the left and the oxyntic
Laparoscopy-assisted D2 radical distal subtotal gastrectomy
 Masters of Gastrointestinal Surgery Laparoscopy-assisted D2 radical distal subtotal gastrectomy Xiaogeng Chen, Weihua Li, Jinsi Wang, Changshun Yang Department of Tumor Surgery, Fujian Provincial Hospital,
Masters of Gastrointestinal Surgery Laparoscopy-assisted D2 radical distal subtotal gastrectomy Xiaogeng Chen, Weihua Li, Jinsi Wang, Changshun Yang Department of Tumor Surgery, Fujian Provincial Hospital,
Acid-Peptic Diseases of the Stomach and Duodenum Including Helicobacter pylori and NSAIDs Prof. Sheila Crowe
 Acid-Peptic Diseases of the Stomach and Duodenum Including Helicobacter pylori and NSAIDs 1 Division of Gastroenterology UC San Diego School of Medicine Clinical presentations of Helicobacter pylori infection
Acid-Peptic Diseases of the Stomach and Duodenum Including Helicobacter pylori and NSAIDs 1 Division of Gastroenterology UC San Diego School of Medicine Clinical presentations of Helicobacter pylori infection