Adjuvant endocrine therapy (essentials in ER positive early breast cancer)
|
|
|
- Simon Tyler Palmer
- 5 years ago
- Views:
Transcription



1 Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics
2 Outline Picking optimal adjuvant endocrine therapy for premenopausal women Picking optimal adjuvant endocrine therapy for post-menopausal women Who benefits from endocrine therapy?










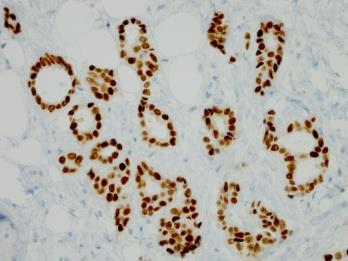
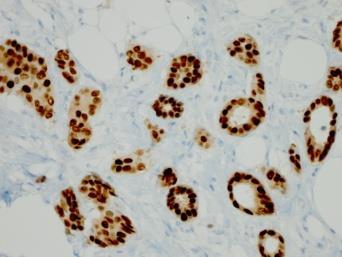
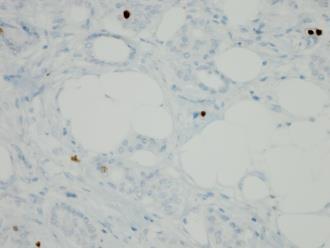
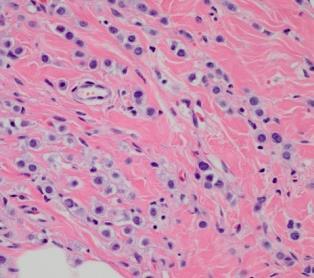
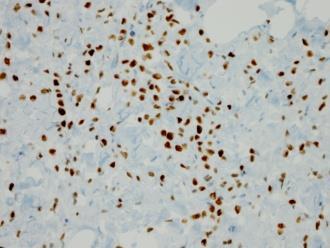

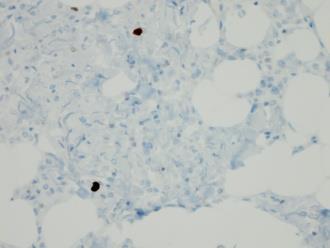
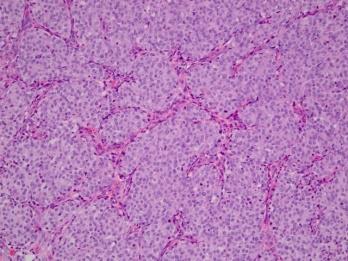
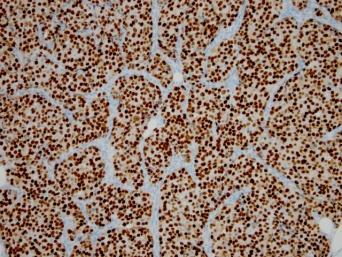
3 H&E ER PR Ki67 A. Ductal Grade 1 ER 100% PR 100% Ki67 7% B. Ductal Grade 2 ER 95% PR 60% Ki67 15% C. Ductal Grade 3 ER 70% PR <1% Ki67 30% D. Lobular Grade 1 ER 100% PR 100% Ki67 <5% E. Lobular Grade 2 ER 100% PR <1% Ecadherin neg * E-cadherin
4 Grade/ER and Prognostic factors Histologic Grade Low ( I of III) Intermediate (II of III) High (III of III) Biomarkers ER expression to to ++ Genetic / Genomic / multipanel markers PR expression ++ to to to ++ Proliferation (Ki-67 / S phase fraction) Low (<10%) Intermediate (10-20%) High (>20%) HER2 Overexpression Never Occasional Occasional 21-gene recurrence score Intrinsic subtype Low (< 18) Luminal A Intermediate (18-25) Luminal B Genomic Grade Lower Higher IHC4 Lower Higher risk MammaPrint Low High High ( >25) Tumor DNA ploidy Mostly diploid Mostly aneuploid
5 Adjuvant ET in ER+ EBC: premenopausal What is the role of ovarian function suppression (OFS) for women receiving tamoxifen? SOFT and E3193 What is the role of aromatase inhibitors (AI) for women treated with OFS? SOFT, TEXT and ABCSG 12 What is the role of chemotherapy in women receiving combined endocrine therapy? PERCHE
6 SOFT: SUPPRESSION of OVARIAN FUNCTION TRIAL 3047 Patients Randomized in ITT (Dec Jan 2011) Two Patient Cohorts No Chemotherapy (47%) Premenopausal, within 12 weeks of surgery (Median time since surgery = 1.8 months) Prior Chemotherapy (53%) Premenopausal* after completing chemotherapy; Randomization within 8 months of completion (Median time since surgery = 8.0 months) *According to locally-determined E 2 level in premenopausal range R A N D O M I Z E Median follow-up=5.6 y Tamoxifen x 5y Tamoxifen+OFS x 5y Exemestane+OFS x 5y Primary Analysis (n= 2033) OFS=ovarian function suppression (oophorectomy, triptorelin or XRT) (n=1018) (n=1015) (n=1014)
7 SOFT: SUPPRESSION of OVARIAN FUNCTION TRIAL 5.6 years median follow-up Primary analysis in overall population not significant (p=0.10) Multivariable Cox model HR=0.78 (95% CI ) p=0.03 > 95% overall survival Francis et al, N Engl J Med, 2015
8 SOFT: SUPPRESSION of OVARIAN FUNCTION TRIAL T+OFS v T: 19% relative reduction in recurrence, p=0.09 E+OFS v T: 36% relative reduction in recurrence with 5-yr BCFI >90% Francis et al, N Engl J Med, 2015

 Tamoxifen+OFS x 5y Exemestane+OFS x 5y Median follow-up 5.")
9 Enrolled: Nov03-Apr11 Premenopausal 12 wk after surgery Planned OFS ± Planned chemo Premenopausal 12 wk after surgery No chemo OR Remain premenopausal 8 mo after chemo TEXT and SOFT Joint Analysis R A N D O M I Z E R A N D O M I Z E TAMOXIFEN AND EXEMESTANE TRIAL (N=2672) Tamoxifen+OFS x 5y Exemestane+OFS x 5y SUPPRESSION OF OVARIAN FUNCTION TRIAL (N=3066) TEXT SOFT Tamoxifen x 5y Tamoxifen+OFS x 5y Exemestane+OFS x 5y Joint Analysis (N=4690) Tamoxifen+OFS x 5y Exemestane+OFS x 5y Median follow-up 5.7yr OFS=ovarian function suppression
10 TEXT and SOFT Joint Analysis Difference 3.8% at 5 years 5.7 years median follow-up Pagani et al, N Engl J Med, 2014
11 Accrual ABCSG 12 1,803 premenopausal breast cancer patients Endocrine-responsive (ER and/or PR positive) Stage I&II, <10 positive nodes Neoadjuvant chemo only Treatment duration: 3 years Surgery (+RT) Goserelin 3.6 mg q28d Median Gnant et follow-up=94 al NEJM 2009 mo Randomize 1 : 1 : 1: 1 Median age (yrs) 45 T1 tumor 75% N0 66% Grade 1/2 75% Preop chemo 5% Tamoxifen 20 mg/d Tamoxifen 20 mg/d + Zoledronic acid 4 mg q6m Anastrozole 1 mg/d Anastrozole 1 mg/d + Zoledronic acid 4 mg q6m Gnant et al, Ann Oncol, 2014
12 TAM ANA TAM ANA ABCSG 12 HR vs Tam 1.13 ( ) P=0.33 HR vs Tam 1.63 ( ) P=0.03 Importance of BMI? Gnant et al, Ann Oncol, 2014
13 Reconciling Results of SOFT, TEXT, ABCSG-12 Shared strengths Focus on premenopausal patients Limited to ER and/or PR-positive tumors Incorporated tamoxifen in some fashion Some limitations Different AIs exemestane vs anastrozole Different forms of OFS Different treatment duration 3 vs 5 yr Different patient characteristics Use and timing of chemotherapy Variable duration of follow-up
14 Adjuvant ET for premenopausal Not every premenopausal woman needs chemotherapy. Several evidence-based choices now available: Tamoxifen X 5-10 yr (ATLAS, attom) Tamoxifen X 5 yr to AI X 5 yr (MA-17) OFS + Tamoxifen (SOFT, E3193) OFS + AI (SOFT/TEXT) Tamoxifen alone X 5-10 yr sufficient for low risk women
15 Adjuvant ET for premenopausal Consider use of OFS+Tamoxifen or OFS+AI for higher risk women like: Chemotherapy recipients who remain premenopausal Multiple positive nodes Age < 35 yrs Optimal duration of OFS-based therapy uncertainsuggest 3-5 years Long term follow-up of pivotal trials for adherence, toxicity & benefit critical
16 Adjuvant ET for premenopausal Adequacy of OFS with LHRH agonists Role of oophorectomy vs OFS Use of bisphosphonates Role of obesity and other host factors Better predictive biomarkers
17 Endocrine therapy: Postmenopausal Years Since Diagnosis Trials Oxford Overview ATAC, BIG 1-98 TAM AI BIG 1-98 AI TAM IES, BIG 1-98, ITA, ARNO, ABCSG8, NSAS BC-03, TEAM TAM AI MA.17, NSAPB B-33, ABCSG 6a TAM AI ATLAS, ATTOM TAM TAM
18 Prognostic factors Type Factor Risk Early recurrence years 0-5 Stage Tumor size Larger > Smaller Histopathology Molecular Signatures Nodal status Positive > Negative Grade Higher > Lower Proliferation (Ki67) Higher > Lower ER / PgR expression Lower > Higher IHC4 Higher > Lower Recurrence score Higher > Lower Intrinsic subtype Luminal B > A ROR Higher > Lower BCI Higher > Lower EndoPredict Higher > Lower
19 Prognostic factors Type Factor Risk Early Late recurrence Recurrence years 0-5 years 5-10 Stage Tumor size Larger > Smaller Nodal status Positive > Negative Histo- Grade Higher > Lower pathology Proliferation (Ki67) Higher > Lower ER / PgR expression Lower > Higher IHC4 Higher > Lower Molecular Recurrence score Higher > Lower Signatures Intrinsic subtype Luminal B > A ROR Higher > Lower BCI Higher > Lower EndoPredict Higher > Lower
20 Risk Factors Associated with Early Recurrence in BIG 1-98 Risk Factor Measurement Hazard Ratio P value T Stage > 2 cm vs < 2 cm N Stage 4+ vs < vs < LVI + vs Grade 3 vs vs ER / PgR +/- vs +/ < Mauriac L, et al. Ann Oncol 2007;18: /+ vs +/ < 0.001
21 10-Year EFS % Risk Factors Associated with Grade Late Recurrence Stage 1 Stage 2 Stage 3
22 Risk Factors Associated with Late Recurrence RS Group N (%) of pts % distant recurrence 5 to 10 years Low 289 (58%) 4.7% 6.8% Intermediate 111 (22%) 4.1% 11.2% High 97 (20%) 12.6% 16.4% Wolmark N, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 11024) % distant recurrence 5 to 15 years
23 # of genes tested Genomic Tools CT yes or CT no Recurrence Score Oncotype Dx GENE70 MammaPrint Tissue used FFPE Fresh frozen/ffpe Sampling technique Samples used in development Genomic Grade Index MapQuant Dx Prosigna CE PAM50 ROR Breast Cancer Index (BCI SM ) qrt-pcr 447 N0/+ ER+/- HER2+ Tam +/- Chemo +/- DNA microarrays 78 N0 ER+/- HER2+ untreated Fresh frozen/ffpe FFPE FFPE qrt-pcr ncounter qrt-pcr 64 N0 ER+ HER2+? Tam +/- Subtypes: 514 N0/+; ER+/-; HER2+/- with mixed therapy ROR: 304 N0/+; ER+/-; HER2+/- tumor samples w/o adj. therapy 314 N0 ER+ HER2+ Tam treated
24 TransATAC: ROR Score Discriminates Recurrence Risk Within Nodal Subgroups Patients, % Node-Negative Patients Luminal A, nodes 0 Luminal B, nodes Follow-up Time, years Node-negative, luminal B patients had a higher risk of RFS events (HR = 4.8 [ ]) % Without Distant Recurrence Node-Positive Patients (1-3 nodes) Luminal A 1-3 node (132) Luminal A, 4+ nodes (31) Luminal B, 1-3 nodes(69) Luminal B, 4+ nodes (20) Follow-up Time, years Luminal B patients with 1 to 3 positive nodes had a higher risk of RFS events (HR = 2.0 [ ]) Dowsett, M. et al. J Clin Oncol. 2013;31(22): Similar results were seen in patients with 4+ positive nodes (HR = 3.4 [ ])
25 Probability of distant recurrence-free survival (%) ABCSG-8: PAM50 Analysis after 10 years FU Low Intermediate High 96.7% ( ) Follow-up time (years) Risk Group Patients (%) Number of Events through 10 years Estimated Percentage without Recurrence at 10 years (95%) 498 (34%) % ( ) 478 (32%) % ( ) 502 (34%) % ( ) Total 1,478 (100%) % ( ) 79.9% ( )
26 Risk and choice There are no predictive markers to guide choices about the type or duration of adjuvant endocrine therapy In the absence of predictive markers, most clinical recommendations are made by extrapolating results from large clinical experiments onto the assessment of risk based prognostic features In lower risk patients, treatment outcomes are more similar regardless of choices In higher risk patients, optimizing the type / duration may make more difference The patient s voice and history are critical and essential in these choices
27 Initial Choice: Years 0-5 Adjuvant endocrine therapy is essential AI-based therapy is preferred Caveats: Sequential outcomes essentially the same Differences in outcome are small, especially for lower risk patients Differences in patient experiences are marked and should affect clinical management
28 Later Choices: Years 5 and beyond Extended adjuvant endocrine therapy should be discussed with all women and encouraged for many Caveats: Is extended therapy a general principle or unique to patients with 5 years of tamoxifen? There are no data for use of AI beyond 5 years I do consider ongoing AI treatment for women at higher risk even in the absence of data For women with good prognosis tumors, in particular, the benefits of extended therapy may be quite modest Patients are uniquely positioned to tell you their preferences Knowing that they have a choice is quite empowering for patients
29 Decision process beyond 5 years Gauge approx LT risk based on stage / biology Assess symptoms Would you consider ongoing endocrine therapy for modest but real benefits and persistent side effects? Yes Maybe No Extended adjuvant therapy Continue therapy; reassess periodically based on symptoms and data Stop at 5 years
30 Clinical conversation Baseline 0.6 cm, N0, grade 1, ER+ / PR+ Low Risk Intermediate Risk High Risk 2.1 cm, N0, grade 2, ER+ PR lo Initial AI or tamoxifen AI or tam AI AI Extended Probably not Probably yes Yes 1.8 cm, 4+ LN, grade 2, ER+ PR+
 of 25 or Less.")
31 A Phase III, Randomized Clinical Trial of Standard Adjuvant Endocrine Therapy +/- Chemotherapy in Patients with Positive Nodes, ER+ and HER2- Breast Cancer With Recurrence Score (RS) of 25 or Less. Opened 2011, Estimated Accrual = 4000
 N=2100 Discordant cases Clin-Path HIGH 70-gene LOW Use Clin-Path risk to decide Chemo or not Clin-Path LOW 70-gene HIGH R1 Clinical-pathological and 70-gene both LOW risk")
32 Evaluate Clinical-Pathological Risk and 70-Gene Signature Risk 55% 35% 10% N=3300 N=600 Clinical-pathological and 70-gene both HIGH risk Chemotherapy EORTC-BIG MINDACT TRIAL 6,600 Women with N0-3+ (Results expected 2014/15) N=2100 Discordant cases Clin-Path HIGH 70-gene LOW Use Clin-Path risk to decide Chemo or not Clin-Path LOW 70-gene HIGH R1 Clinical-pathological and 70-gene both LOW risk Use 70-gene risk to decide Chemo or not Albain, KS. St. Gallen 2013 Potential CT sparing in 20-28% pts Endocrine therapy

33 TAILORx Study Design ECOG/Inter-group PI: J. A. Sparano Secondary Study Group 1 RS < 11 ~29% of Population ARM A Hormonal Therapy Alone Albain, KS. St. Gallen 2013 ARM B 21 Gene RS Assay REGISTER Specimen Banking Primary Study Group RS ~44% of Population ER+/HER2-/Node- RANDOMIZE n = 4390 Stratified by: T, menopausal status, planned CT/RT Hormonal Therapy Alone ARM C Chemotherapy + Hormonal Therapy Accrual completed on Oct 25 th 2010 Target: 10,000 expected to report in Secondary Study Group 2 RS > 25 ~27% of Population ARM D Chemotherapy + Hormonal Therapy
34 Prospective Validation of a 21-Gene Expression Assay in Breast Cancer Sparano JA et al. N Engl J Med 2015;373:
35 Generally YES High grade High Ki67 Low ER and PR Bad Signature Luminal B or surrogate Early recurrence risk Consider CT Disease Burden Chemotherapy M A Y B E Consider: Preference Comorbidity Generally NO Low grado Low Ki67 High ER e PR Good signature Luminal A or surrogate Late recurrence risk Limited indication To CT

36 Treatment recommendations
37 Treatment options Clinical grouping Therapy Note ER positive & HER2-negative ( luminal disease ) Luminal A Like Endocrine therapy SOFT e TEXT according to menopausal status Premenopausal low risk Tamoxifen 5 years Premenopausal others Postmenopausal low risk Postmenopausal Luminal B-like Factors supporting omission of CT in luminal B like Tamoxifen 5 10 years with OFS or exemestane with OFS Tamoxifen 5 years AI (consider extended adjuvant therapy) Chemotherapy and ET SOFT e TEXT No evidence of AI beyond 5 years Good prognosis Gene signature
38 Thank you
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER
 OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER Aleix Prat, MD PhD Medical Oncology Department Hospital Clínic of Barcelona University of Barcelona esmo.org Disclosures Advisory role for
OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER Aleix Prat, MD PhD Medical Oncology Department Hospital Clínic of Barcelona University of Barcelona esmo.org Disclosures Advisory role for
Early Stage Disease. Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center
 SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension?
 Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension? Ivana Sestak, PhD Centre for Cancer Prevention Wolfson Institute of Preventive Medicine Queen Mary University London
Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension? Ivana Sestak, PhD Centre for Cancer Prevention Wolfson Institute of Preventive Medicine Queen Mary University London
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland
 What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
(Neo-) adjuvant endocrine therapy
 adjuvant endocrine therapy") (Neo-) adjuvant endocrine therapy F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board of Directors & Chair NR Committee
(Neo-) adjuvant endocrine therapy F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board of Directors & Chair NR Committee
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI
 Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI UOC Oncologia Medica, A.O. Papardo, Messina Dir. Prof. V. Adamo BREAST CANCER Brain Adjuvant Medical Therapies
Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI UOC Oncologia Medica, A.O. Papardo, Messina Dir. Prof. V. Adamo BREAST CANCER Brain Adjuvant Medical Therapies
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer
 Node Positive Breast Cancer") Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Session thématisée Les Innovations diagnostiques en cancérologie
 10 èmes Journées Scientifiques du Cancéropôle Nord-Ouest 10-12 mai 2017, Deauville Session thématisée Les Innovations diagnostiques en cancérologie Les signatures multigéniques pronostiques dans le cancer
10 èmes Journées Scientifiques du Cancéropôle Nord-Ouest 10-12 mai 2017, Deauville Session thématisée Les Innovations diagnostiques en cancérologie Les signatures multigéniques pronostiques dans le cancer
Emerging Approaches for (Neo)Adjuvant Therapy for ER+ Breast Cancer
Adjuvant Therapy for ER+ Breast Cancer") Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Adjuvant Endocrine Therapy: How Long is Long Enough?
 Adjuvant Endocrine Therapy: How Long is Long Enough? Harold J. Burstein, MD, PhD Dana-Farber Cancer Institute Harvard Medical School Boston, Massachusetts hburstein@partners.org I have no conflicts to
Adjuvant Endocrine Therapy: How Long is Long Enough? Harold J. Burstein, MD, PhD Dana-Farber Cancer Institute Harvard Medical School Boston, Massachusetts hburstein@partners.org I have no conflicts to
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA
 ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA THE NATURAL HISTORY OF HORMONE RECEPTOR- POSITIVE BREAST CANCER IS VERY LONG Recurrence hazard rate 0.3 0.2 0.1 0 ER+ (n=2,257)
ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA THE NATURAL HISTORY OF HORMONE RECEPTOR- POSITIVE BREAST CANCER IS VERY LONG Recurrence hazard rate 0.3 0.2 0.1 0 ER+ (n=2,257)
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Use of Ovarian Suppression and Ablation in Breast Cancer Treatment
 Use of Ovarian Suppression and Ablation in Breast Cancer Treatment Dr Marina Parton Consultant Medical Oncologist Royal Marsden and Kingston Hospitals Overview Breast cancer phenotypes Use of ovarian manipulation
Use of Ovarian Suppression and Ablation in Breast Cancer Treatment Dr Marina Parton Consultant Medical Oncologist Royal Marsden and Kingston Hospitals Overview Breast cancer phenotypes Use of ovarian manipulation
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Profili di espressione genica
 Profili di espressione genica Giampaolo Bianchini MD Ospedale San Raffaele, Milan - Italy Gene expression profiles Transcriptomics Gene DNA mrna mirnas Protein metilation Metabolite Genomics Transcriptomics
Profili di espressione genica Giampaolo Bianchini MD Ospedale San Raffaele, Milan - Italy Gene expression profiles Transcriptomics Gene DNA mrna mirnas Protein metilation Metabolite Genomics Transcriptomics
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY
 Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY Methodology The test is based on the reported 50-gene classifier algorithm originally named PAM50 and is performed on the ncounter Dx Analysis System
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY Methodology The test is based on the reported 50-gene classifier algorithm originally named PAM50 and is performed on the ncounter Dx Analysis System
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY
 Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY GENE EXPRESSION PROFILING WITH PROSIGNA What is Prosigna? Prosigna Breast Cancer Prognostic Gene Signature Assay is an FDA-approved assay which provides
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY GENE EXPRESSION PROFILING WITH PROSIGNA What is Prosigna? Prosigna Breast Cancer Prognostic Gene Signature Assay is an FDA-approved assay which provides
Adjuvant Endocrine Therapy in Pre- and Postmenopausal Patients
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Endocrine Therapy in Pre- and Postmenopausal Patients Adjuvant Endocrine Therapy in Pre- and Postmenopausal Patients
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Endocrine Therapy in Pre- and Postmenopausal Patients Adjuvant Endocrine Therapy in Pre- and Postmenopausal Patients
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
A new way of looking at breast cancer tumour biology
 A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
Endocrine Therapy in Premenopausal Breast Cancer. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology
 Endocrine Therapy in Premenopausal Breast Cancer Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology Ovarian Ablation or Suppression vs. Not in ER + or ER UK Breast Cancer
Endocrine Therapy in Premenopausal Breast Cancer Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology Ovarian Ablation or Suppression vs. Not in ER + or ER UK Breast Cancer
OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER
 OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER STEPHEN E. JONES, M.D. US ONCOLOGY RESEARCH THE WOODLANDS, TX TOPICS PREMENOPAUSAL BREAST CANCER POSTMENOPAUSAL BREAST CANCER THE FUTURE TOPICS PREMENOPAUSAL
OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER STEPHEN E. JONES, M.D. US ONCOLOGY RESEARCH THE WOODLANDS, TX TOPICS PREMENOPAUSAL BREAST CANCER POSTMENOPAUSAL BREAST CANCER THE FUTURE TOPICS PREMENOPAUSAL
Breast Cancer Assays of Genetic Expression in Tumor Tissue
 Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/02/2008 Line(s) of Business: Current Effective Date Section: 05/25/2018 Other Miscellaneous
Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/02/2008 Line(s) of Business: Current Effective Date Section: 05/25/2018 Other Miscellaneous
San Antonio Breast Cancer Symposium 2013
 15 th Annual Advances in Oncology Navigating Breast Cancer Therapeutics: Early and Late Stage Disease Scott Christensen, MD Professor, Hematology/Oncology UC Davis Comprehensive Cancer Center 15th Annual
15 th Annual Advances in Oncology Navigating Breast Cancer Therapeutics: Early and Late Stage Disease Scott Christensen, MD Professor, Hematology/Oncology UC Davis Comprehensive Cancer Center 15th Annual
Luminal early breast cancer: (neo-) adjuvant endocrine therapy
 adjuvant endocrine therapy") CAMPUS GROSSHADERN CAMPUS INNENSTADT KLINIK UND POLIKLINIK FÜR FRAUENHEILKUNDE UND GEBURTSHILFE DIREKTOR: PROF. DR. MED. SVEN MAHNER Luminal early breast cancer: (neo-) adjuvant endocrine therapy Nadia
CAMPUS GROSSHADERN CAMPUS INNENSTADT KLINIK UND POLIKLINIK FÜR FRAUENHEILKUNDE UND GEBURTSHILFE DIREKTOR: PROF. DR. MED. SVEN MAHNER Luminal early breast cancer: (neo-) adjuvant endocrine therapy Nadia
Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013
 Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013 Changing Phases claudin low Lum A Lum B Basal Her2 NIH Consensus Development Panel,
Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013 Changing Phases claudin low Lum A Lum B Basal Her2 NIH Consensus Development Panel,
Choosing between different hormonal therapies. Rudy Van den Broecke UZ Ghent
 Choosing between different hormonal therapies Rudy Van den Broecke UZ Ghent What is the golden standard in premenopausal hormonal sensitive early breast cancer? Ovarian Suppression alone 5 years Tamoxifen
Choosing between different hormonal therapies Rudy Van den Broecke UZ Ghent What is the golden standard in premenopausal hormonal sensitive early breast cancer? Ovarian Suppression alone 5 years Tamoxifen
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer
 The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
Kathy Albain, MD. Chemotherapy in Luminal Breast Cancer: Who Benefits? Loyola University Chicago Stritch School of Medicine
 Chemotherapy in Luminal Breast Cancer: Who Benefits? Kathy Albain, MD Loyola University Chicago Stritch School of Medicine, Director, Breast Clinical Research Program, Cardinal Bernardin Cancer Center,
Chemotherapy in Luminal Breast Cancer: Who Benefits? Kathy Albain, MD Loyola University Chicago Stritch School of Medicine, Director, Breast Clinical Research Program, Cardinal Bernardin Cancer Center,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 67 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 67 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Considerations in Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 1/2019 Origination: 1/2006 Next Review: 9/2019 Policy
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 1/2019 Origination: 1/2006 Next Review: 9/2019 Policy
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 9/2018 Origination: 1/2006 Next Review: 9/2019 Policy
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 9/2018 Origination: 1/2006 Next Review: 9/2019 Policy
CARCINOMA DELLA MAMMELLA La scelta del trattamento adiuvante: utilità clinica dei tests genomici
 CARCINOMA DELLA MAMMELLA La scelta del trattamento adiuvante: utilità clinica dei tests genomici Dott.ssa Gaia Griguolo DiSCOG-Università di Padova IOV Istituto Oncologico Veneto I.R.C.C.S. Tutor: Prof.
CARCINOMA DELLA MAMMELLA La scelta del trattamento adiuvante: utilità clinica dei tests genomici Dott.ssa Gaia Griguolo DiSCOG-Università di Padova IOV Istituto Oncologico Veneto I.R.C.C.S. Tutor: Prof.
Current Status and Future Development of Tools for Prognosis and Prediction - USA
 Current Status and Future Development of Tools for Prognosis and Prediction - USA John H. Ward, MD Professor of Medicine University of Utah School of Medicine Huntsman Cancer Institute October18, 2009
Current Status and Future Development of Tools for Prognosis and Prediction - USA John H. Ward, MD Professor of Medicine University of Utah School of Medicine Huntsman Cancer Institute October18, 2009
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Terapia Hormonal da Paciente Premenopausa
 I Congresso de Oncologia D Or 5 e 6 de julho de 2013 Terapia Hormonal da Paciente Premenopausa Antonio C. Wolff, MD, FACP, FASCO Professor de Oncologia Programa de Câncer de Mama Johns Hopkins University
I Congresso de Oncologia D Or 5 e 6 de julho de 2013 Terapia Hormonal da Paciente Premenopausa Antonio C. Wolff, MD, FACP, FASCO Professor de Oncologia Programa de Câncer de Mama Johns Hopkins University
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Rationale For & Design of TAILORx. Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York
 Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Updates From San Antonio Breast Cancer Symposium 2017
 Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Should premenopausal HR+ve breast cancer receive LHRH?
 Should premenopausal HR+ve breast cancer receive LHRH? Hesham Elghazaly, MD Prof. Clinical Oncology, Ain Shams University President of the BGICS Should premenopausal HR+ve breast cancer receive LHRH? NO?
Should premenopausal HR+ve breast cancer receive LHRH? Hesham Elghazaly, MD Prof. Clinical Oncology, Ain Shams University President of the BGICS Should premenopausal HR+ve breast cancer receive LHRH? NO?
Optimal Treatment of Hormone Receptor Positive Disease
 San Francisco, CA United States January 27, 2018 San Francisco, CA USA January 27, 2018 Optimal Treatment of Hormone Receptor Positive Disease JO CHIEN, MD Associate Professor of Medicine UCSF School of
San Francisco, CA United States January 27, 2018 San Francisco, CA USA January 27, 2018 Optimal Treatment of Hormone Receptor Positive Disease JO CHIEN, MD Associate Professor of Medicine UCSF School of
MP Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients With Breast Cancer. Related Policies None
 Medical Policy Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients With Breast BCBSA Ref. Policy: 2.04.36 Last Review: 11/15/2018 Effective Date: 02/15/2019 Section:
Medical Policy Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients With Breast BCBSA Ref. Policy: 2.04.36 Last Review: 11/15/2018 Effective Date: 02/15/2019 Section:
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 55 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 55 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
The Role of Novel Assays in the Prediction of Benefit from Extended Adjuvant Endocrine Therapy for Breast Cancer
 The Role of Novel Assays in the Prediction of Benefit from Extended Adjuvant Endocrine Therapy for Breast Cancer Erin Roesch, MD, and Claudine Isaacs, MD Abstract Endocrine therapy in the adjuvant setting
The Role of Novel Assays in the Prediction of Benefit from Extended Adjuvant Endocrine Therapy for Breast Cancer Erin Roesch, MD, and Claudine Isaacs, MD Abstract Endocrine therapy in the adjuvant setting
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
She counts on your breast cancer expertise at the most vulnerable time of her life.
 HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
Seigo Nakamura,M.D.,Ph.D.
 Seigo Nakamura,M.D.,Ph.D. Professor of Surgery Director of Breast Center Showa University Hospital Chairman of the board of directors Japan Breast Cancer Society Inhibition of Estrogen-Dependent Growth
Seigo Nakamura,M.D.,Ph.D. Professor of Surgery Director of Breast Center Showa University Hospital Chairman of the board of directors Japan Breast Cancer Society Inhibition of Estrogen-Dependent Growth
Clinical utility of multigene profiling assays in early-stage breast cancer
 PRACTICE GUIDELINE CLINICAL UTILITY OF MULTIGENE PROFILING ASSAYS, Chang et al. Clinical utility of multigene profiling assays in early-stage breast cancer M.C. Chang md phd,* L.H. Souter phd, S. Kamel-Reid
PRACTICE GUIDELINE CLINICAL UTILITY OF MULTIGENE PROFILING ASSAYS, Chang et al. Clinical utility of multigene profiling assays in early-stage breast cancer M.C. Chang md phd,* L.H. Souter phd, S. Kamel-Reid
Update on New Perspectives in Endocrine-Sensitive Breast Cancer. James R. Waisman, MD
 Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer
![SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer](/thumbs/95/125806264.jpg "SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer") SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer Charles Moertel Lecture May 12, 2017 Gini Fleming Charles Moertel Founder of NCCTG Dedication to high quality clinical
SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer Charles Moertel Lecture May 12, 2017 Gini Fleming Charles Moertel Founder of NCCTG Dedication to high quality clinical
Disclosures. ASCO Highlights Breast Cancer. Associa4on of Northern California Oncologists 8/25/14
 ASCO Highlights 2014 Associa4on of Northern California Oncologists Breast Cancer Sco+ Christensen, MD Professor, Hematology/Oncology UC Davis Comprehensive Cancer Center Disclosures 1 Outline Novel TherapeuFcs/Early
ASCO Highlights 2014 Associa4on of Northern California Oncologists Breast Cancer Sco+ Christensen, MD Professor, Hematology/Oncology UC Davis Comprehensive Cancer Center Disclosures 1 Outline Novel TherapeuFcs/Early
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 47 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 47 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 54 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 54 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
The Current Status and the Future Prospects of Multigene testing in Europe
 The Current Status and the Future Prospects of Multigene testing in Europe Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam St. Gallen Recommendations 2009 =
The Current Status and the Future Prospects of Multigene testing in Europe Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam St. Gallen Recommendations 2009 =
The Oncotype DX Assay A Genomic Approach to Breast Cancer
 The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
Giuseppe Viale for the BIG 1 98 Collaborative and International Breast Cancer Study Groups
 Central Review of ER, PgR and HER2 in BIG 1 98 Evaluating Letrozole vs. Letrozole Tamoxifen vs. Tamoxifen Letrozole as Adjuvant Endocrine Therapy for Postmenopausal Women with Hormone Receptor Positive
Central Review of ER, PgR and HER2 in BIG 1 98 Evaluating Letrozole vs. Letrozole Tamoxifen vs. Tamoxifen Letrozole as Adjuvant Endocrine Therapy for Postmenopausal Women with Hormone Receptor Positive
Кой има полза от адювантна ендокринна терапия при карцином на гърда с какво и колко дълго?
 Кой има полза от адювантна ендокринна терапия при карцином на гърда с какво и колко дълго? д-р Красимир Койнов МБАЛ Сердика, София Декларация Консултации и хонорари: Roche, Boerhinger Ingelheim, Astra
Кой има полза от адювантна ендокринна терапия при карцином на гърда с какво и колко дълго? д-р Красимир Койнов МБАЛ Сердика, София Декларация Консултации и хонорари: Roche, Boerhinger Ingelheim, Astra
(Neo-) adjuvant endocrine therapy
 adjuvant endocrine therapy") (Neo-) adjuvant endocrine therapy F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board of Directors & NR Committee Chair
(Neo-) adjuvant endocrine therapy F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board of Directors & NR Committee Chair
Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers
 日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
Mechanisms of Resistance to. Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center
 Mechanisms of Resistance to Hormonal Therapy Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Antagonizing Estrogen Dependent Growth Premenopausal
Mechanisms of Resistance to Hormonal Therapy Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Antagonizing Estrogen Dependent Growth Premenopausal
GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN
 GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN Adam Brufsky, MD, PhD Professor of Medicine Associate Chief, Hematology-Oncology Associate Director, Clinical Investigation University
GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN Adam Brufsky, MD, PhD Professor of Medicine Associate Chief, Hematology-Oncology Associate Director, Clinical Investigation University
ESMO Breast Cancer Preceptorship Singapore November Special Issues in Treatment of Young Women with Breast Cancer
 ESMO Breast Cancer Preceptorship Singapore November 2017 Special Issues in Treatment of Young Women with Breast Cancer Prudence Francis MD Peter MacCallum Cancer Centre Melbourne, Australia Conflict of
ESMO Breast Cancer Preceptorship Singapore November 2017 Special Issues in Treatment of Young Women with Breast Cancer Prudence Francis MD Peter MacCallum Cancer Centre Melbourne, Australia Conflict of
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Oncotype DX MM /01/2008. HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
 of Service: Office") Oncotype DX Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
Oncotype DX Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
1 INTRODUCTION REVIEW ARTICLE
 Received: 12 December 2016 Revised: 15 December 2016 Accepted: 15 December 2016 DOI 10.1002/jso.24561 REVIEW ARTICLE Selecting postoperative adjuvant systemic therapy for early stage breast cancer: A critical
Received: 12 December 2016 Revised: 15 December 2016 Accepted: 15 December 2016 DOI 10.1002/jso.24561 REVIEW ARTICLE Selecting postoperative adjuvant systemic therapy for early stage breast cancer: A critical
A case of a BRCA2-mutated ER+/HER2 breast cancer during pregnancy
 ESMO Preceptorship Programme Breast Cancer Lisbon 16,17 September 2016 Emanuela Risi Sandro Pitigliani Medical Oncology Department Hospital of Prato, Istituto Toscano Tumori, Prato, Italy A case of a BRCA2-mutated
ESMO Preceptorship Programme Breast Cancer Lisbon 16,17 September 2016 Emanuela Risi Sandro Pitigliani Medical Oncology Department Hospital of Prato, Istituto Toscano Tumori, Prato, Italy A case of a BRCA2-mutated
Breast Cancer Assays of Genetic Expression in Tumor Tissue
 Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/16/2016
Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/16/2016
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
Lessons Learnt from Neoadjuvant Hormone Therapy. 10 Lessons Learnt from Neoadjuvant Endocrine Therapy. Lesson 1
 Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy. Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh
 Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Lessons Learnt from Neoadjuvant Hormone Therapy Mike Dixon Clinical Director Breakthrough Research Unit Edinburgh 10 Lessons Learnt from Neoadjuvant Endocrine Therapy 10 Lessons Learnt from Neoadjuvant
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Medical Policy Manual Genetic Testing, Policy No. 42 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Next Review: December 2018 Last Review:
Medical Policy Manual Genetic Testing, Policy No. 42 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Next Review: December 2018 Last Review:
A Prospective Comparison of the 21-Gene Recurrence Score and the PAM50-Based Prosigna in Estrogen Receptor-Positive Early-Stage Breast Cancer
 Adv Ther (2015) 32:1237 1247 DOI 10.1007/s12325-015-0269-2 ORIGINAL RESEARCH A Prospective Comparison of the 21-Gene Recurrence Score and the PAM50-Based Prosigna in Estrogen Receptor-Positive Early-Stage
Adv Ther (2015) 32:1237 1247 DOI 10.1007/s12325-015-0269-2 ORIGINAL RESEARCH A Prospective Comparison of the 21-Gene Recurrence Score and the PAM50-Based Prosigna in Estrogen Receptor-Positive Early-Stage
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2011 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2011 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón
 Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón Universidad Complutense Madrid The new technologies
Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón Universidad Complutense Madrid The new technologies
The TAILORx Trial: A review of the data and implications for practice
 The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
Jules Bordet Institute, Brussels, Belgium Université Libre de Bruxelles Breast International Group (BIG aisbl), Chair ESMO President
, Chair ESMO President") Symposium «Evaluation of the Belgian Cancer Plan» Brussels, November 26th, 2012 Personalized oncology in Europe: only a dream if national health systems do not get involved in diagnostics and pivotal cancer
Symposium «Evaluation of the Belgian Cancer Plan» Brussels, November 26th, 2012 Personalized oncology in Europe: only a dream if national health systems do not get involved in diagnostics and pivotal cancer
Adjuvant Endocrine Therapy in Premenopausal Patients
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Endocrine Therapy in Premenopausal Patients Adjuvant Endocrine Therapy in Premenopausal Patients Version 2002: Scharl
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Endocrine Therapy in Premenopausal Patients Adjuvant Endocrine Therapy in Premenopausal Patients Version 2002: Scharl
Genomic platforms in breast cancer
 Genomic platforms in breast cancer Prof. Miguel Martín Instituto de Investigación Sanitaria Hospital Gregorio Marañón Universidad Complutense Madrid mmartin@geicam.org Disclosure Dr. Martin has received
Genomic platforms in breast cancer Prof. Miguel Martín Instituto de Investigación Sanitaria Hospital Gregorio Marañón Universidad Complutense Madrid mmartin@geicam.org Disclosure Dr. Martin has received
MammaPrint, the story of the 70-gene profile
 MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
TAILORx: Established and Potential Implications for Clinical Practice
 TAILORx: Established and Potential Implications for Clinical Practice Joseph A. Sparano, MD Study Chair, TAILORx Vice-Chair, ECOG-ACRIN Cancer Research Group Hello Healthcare Summit Berlin, Germany March
TAILORx: Established and Potential Implications for Clinical Practice Joseph A. Sparano, MD Study Chair, TAILORx Vice-Chair, ECOG-ACRIN Cancer Research Group Hello Healthcare Summit Berlin, Germany March
Adjuvan Chemotherapy in Breast Cancer
 Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
Long Term Toxicity of Endocrine Therapy for premenopausal women with ER positive breast cancer
 Global Breast Cancer Conference 2017 21 st Apr, 2017@Chezu Island Long Term Toxicity of Endocrine Therapy for premenopausal women with ER positive breast cancer Shinji Ohno, M.D., Ph.D., F.A.C.S. Breast
Global Breast Cancer Conference 2017 21 st Apr, 2017@Chezu Island Long Term Toxicity of Endocrine Therapy for premenopausal women with ER positive breast cancer Shinji Ohno, M.D., Ph.D., F.A.C.S. Breast
THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE. Dr Husam Marashi 03/02/2017
 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE Dr Husam Marashi 03/02/2017 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER TODAY S TALK: CENTRE EXPERIENCE
THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE Dr Husam Marashi 03/02/2017 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER TODAY S TALK: CENTRE EXPERIENCE
Genomic Profiling of Tumors and Loco-Regional Recurrence
 1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer
 Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
DIAGNOSTICS ASSESSMENT PROGRAMME
 DIAGNOSTICS ASSESSMENT PROGRAMME Evidence overview Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10) This overview summarises the key issues
DIAGNOSTICS ASSESSMENT PROGRAMME Evidence overview Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10) This overview summarises the key issues
Prognostic and Predictive Factors
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Prognostic and Predictive Factors Prognostic and Predictive Factors Version 2002: Thomssen / Harbeck Version 2003 2009: Costa
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Prognostic and Predictive Factors Prognostic and Predictive Factors Version 2002: Thomssen / Harbeck Version 2003 2009: Costa