To Screen or Not To Screen: Cancer Screening Outside Organized Programs
|
|
|
- Blaise Clifton Dalton
- 5 years ago
- Views:
Transcription


1 To Screen or Not To Screen: Cancer Screening Outside Organized Programs Dr. Ed Kucharski, Southeast Toronto FHT Dr. Lisa Del Giudice, Sunnybrook Academic FHT Dr. Genevieve Chaput, McGill University Health Centre
2 Faculty/Presenter Disclosure Faculty: "To Screen or Not To Screen: Cancer Screening Outside Organized Programs Dr. Genevieve Chaput, McGill University Health Centre Dr. Lisa Del Giudice, Cancer Care Ontario, Regional Primary Care Cancer Lead, DFCM University or Toronto Dr. Ed Kucharski, Cancer Care Ontario, Regional Primary Care Cancer Lead, DFCM University or Toronto
3 Disclosure of Commercial Support Relationship with commercial interests: There is no affiliation (financial or otherwise) with a pharmaceutical, medical device or communications organization. 3
4 Mitigating Potential Bias Not applicable 4
5 Learning Objectives Participants will be able to list the risks and benefits of cancer screening outside of organized programs. Participants will appropriately counsel patients, select tests and follow-up on results when the evidence is not clear. Participants will be provided with a list of resources that can help patients in making an informed decision about cancer screening. 5

6 trcp.ca

7 CCFP Cancer Care Committee
8 Number of new cases Why prevention is so important? 90,000 80,000 Estimated ,000 60,000 Additional cases due to aging of the population 50,000 40,000 Additional cases due to population growth 30,000 Change in cancer risk 20,000 Baseline cancer incidence (1981 level) 10, Year *Prevention is the only way to reduce cancer incidence
9 Video for Healthcare Providers: English: French:
10 What is My CancerIQ Website designed for the public to help understand their risk for cancer and what they can do to help lower that risk Developed by Cancer Care Ontario (CCO) and funded by the Ministry of Health and Long-Term Care (MOHLTC) Consists of a series of questionnaires by cancer type (~5 min each) Answers that are common across questionnaires will be prepopulated in the same session 10

11 Homepage FULLY BILINGUAL SITE Social media Risk Assessments About the tool Fact sheet for each cancer + links FAQ for healthcare providers Subscribe for updates About CCO Legal & Privacy Contact FAQ 11
12 Prostate Cancer Screening 12
13 Case 1: John You have a taken over a new practice and are meeting a number of your new patients. You meet John (age 63) who has been getting a PSA test done every year to make sure everything is alright. You want to care for him appropriately and start off on the right foot. What do you do? 13
14 Prostate Cancer Screening There is considerable debate regarding screening for prostate cancer using the PSA test Most commonly diagnosed cancer in men (after skin cancer) and third leading cause of cancer death in men
15 Prostate Cancer Screening No organized programs in Canada Prostate cancer screening policies for example, in Ontario PSA testing is covered under certain circumstances, not screening PSA is funded in all provinces and territories Opportunistic screening is the mainstay of screening offered by primary care providers
16 Prostate Cancer Screening CTFPHC Recommendations (2014) For men aged less than 55 years, we recommend not screening for prostate cancer with the prostate-specific antigen test. Strong recommendation; low quality evidence For men aged years, we recommend not screening for prostate cancer with the prostate-specific antigen test. Weak recommendation; moderate quality evidence For men 70 years of age and older, we recommend not screening for prostate cancer with the prostate-specific antigen test. Strong recommendation; low quality evidence Endorsement: This clinical practice guideline has been endorsed by the CFPC
17 1,000 MEN SCREENED 102 MEN WILL BE DIAGNOSED WITH PROSTATE CANCER of these 102 prostate cancers would not have caused illness or death. Because of uncertainty about whether their cancer will progress, most men will choose treatment and may experience complications of treatment. 5 men will die from prostate cancer despite undergoing PSA screening. 178 MEN WITH A POSITIVE PSA IN WHOM FOLLOW UP TESTING DOES NOT IDENTIFY PROSTATE CANCER 1 1 man will escape death from prostate cancer because he underwent PSA screening. 720 MEN WILL HAVE A NEGATIVE PSA TEST 4 4 of these 178 will experience biopsy complications such as infection and bleeding severe enough to require hospitalization. 17
18 Pearls (and what to do with John) Mike Evans PSA Video Prostate Cancer Canada talks about a baseline PSA Reducing risk with healthy diet and exercise (Pearls: What Not to Do List)
19
20 Lung Cancer Screening 20

21 Case 2: James 65 year old male No personal history of cancer No family history of lung cancer Smoker for 31 years and smokes ~20 cigarettes per day Hasn t attempted to quit within the past 12 months Lived in a large city for 10 or more years No history of asbestos, chemical or other occupational exposures 21
22 Burden of Lung Cancer Most common cause of cancer death Most commonly diagnosed cancer in Canada Approximately will be diagnosed and will die in a given year Mortality is extremely high for late stages compared to earlier stages
23 Evidence for Lung Cancer Screening for People at High Risk National Lung Screening Trial evidence: Randomized controlled trial with >50,000 participants 20% reduction in lung cancer mortality over 6 years with LDCT
24 Lung Cancer Screening No fully implemented organized programs in Canada Pilots in Ontario Opportunistic screening is the mainstay of screening offered by primary care providers in seven provinces Business cases/proposals for screening in BC, AB, NS, PEI, NB

25 Cancer Care Ontario Recommendations Cancer Care Ontario recommends: Screening should be organized LDCT for high risk populations Chest X-ray should not be used Embedding smoking cessation in screening program



26 Lung Cancer Screening for People at High Risk in Ontario Cancer Care Ontario conducting pilot in 3 sites Sites with level 1 thoracic surgery centres and Lung Diagnostic Assessment Programs Started April 2017 and data collected over 2 years Results of evaluation will inform provincial program New pilot for Toronto Feb 2019 For more information, contact your Regional Primary Care Lead / Regional Aboriginal Cancer Lead
27 Screening Outside of Cancer Care Ontario s Pilot Lung cancer screening should only occur through an organized screening program If not organized, screening may not occur in appropriate populations, at recommended interval, with appropriate follow-up or with quality monitoring Can only ensure high-quality organized lung cancer screening at pilot sites
28 However.CTFPHC Says: Low Dose CT Recommendation: For adults aged 55 to 74 years with at least a 30 pack-year smoking history, who currently smoke or quit less than 15 years ago, we recommend annual screening with LDCT up to three consecutive times. Weak recommendation; low quality evidence Screening should ONLY be carried out in health care setting with expertise in early diagnosis and treatment of lung cancer
29 Pearls and what to do with James? If in Ontario with a pilot, refer him there! Don t do a CXR Mycanceriq.ca Smoking cessation: my favourites are smokers helpline and Mike Evans Video Alberta TOPS information
30 Alberta College of Family Physicians (ACFP) Tools for Practice Bottom Line: Benefit from screening for lung cancer with LDCT has been demonstrated in only one trial, without a usual care group. The high number of false positives, which require further, sometimes invasive investigations, is worrisome. Smoking cessation should remain the priority to decrease lung cancer mortality.
31 Colorectal Cancer Screening 31
32 CRC Case Study: Part A You are seeing Rahm, a 53 year old man Rahm has heard about colonoscopy examination through a friend on his baseball team and would like to have one What questions should you ask him first to determine if colonoscopy is the appropriate screening modality for him? 32
33 CRC Case Study: Part A What questions should you ask Rahm to determine if colonoscopy is the appropriate screening modality for him? Family History History of IBD CRC Symptoms CRC Signs 33
34 CRC Case Study: Part A Rahm reports that his father was just diagnosed with colorectal cancer at the age of 75 What do you recommend to Rahm? (age of initiation, modality and how often if normal) 34
35 CRC Screening Recommendation: Colonoscopy Colonoscopy is Recommended if: 1 or more first-degree relatives with a history of colorectal cancer Begin at age 50, or 10 years earlier than age relative was diagnosed, whichever is first Re-screening interval is dependent on family history o Relative diagnosed before age 60 screen every 5 years o Relative diagnosed at/after age 60 screen every 10 years
36 CRC Case Study: Part B What if Rahm denied any symptoms that were suspicious for colorectal cancer or family history of colorectal cancer, what risks are associated with screening colonoscopies? 36
37 Colonoscopy-Associated Complications Ontario n=67,632 Bleeding 1 in 671 Perforation 1 in 1,695 Death 1 in 13,513 Colonoscopy is not a benign procedure Rabeneck L., et. al., Gastroenterology 2008;
38 CRC Case Study: Part B After hearing about these risks, Rahm begins to lose interest in having a colonoscopy and asks what other options does he have for colorectal cancer screening? 38
39 CTFPHC 2016 CRC Screening Guidelines Average Risk Recommendations: Screen adults aged 60 to 74 with FOBT (either gfobt or FIT) every two years OR flexible sigmoidoscopy every 10 years Strong recommendation; moderate quality evidence Screen adults aged 50 to 59 with FOBT (either gfobt or FIT) every two years OR flexible sigmoidoscopy every 10 years Weak recommendation; moderate quality evidence Do not screen adults aged 75 years and over Weak recommendation; low quality evidence Do not using colonoscopy as a screening test for CRC Weak recommendation; low quality evidence

40 Provincial and Territorial Programs

41 Provincial and Territorial Programs

42 Transition to FIT in Ontario Cancer Care Ontario is working on changes to the Colon Cancer Check program for the transition to screening with FIT for average risk individuals Until FIT is launched, gfobt remains the recommended CRC screening test in Ontario for people at average risk 42
43 CRC Case Study: Part B Rahm asks how does Fecal Immunochemical Testing (FIT) compare to colonoscopy in terms of performance and possible risks? 43
44 Diagnostic Yield- Intention to Screen Colonoscopy n=26,703 FIT n=26,599 P-value CRC Detection Advanced adenoma detection # needed to screen to find 1 CRC # needed to scope to find 1 CRC Not significant < Complication rate <0.001 Quintero E., et. al., NEJM 2012;366:
45 CRC Case Study: Part C What if Rahm (with no family history) in the end insists on and completes a screening colonoscopy, when should he have his next CRC screening test and with what modality if his screening colonoscopy is: Normal One Hyperplastic polyp One to Two Tubular Adenomas One Tubulovillous Adenoma 45
46 Screening After Normal Colonoscopy Case control studies show patients with a previous negative colonoscopy have a 74-76% lower risk of CRC than those without previous colonoscopy risk reduction persists 10-20y This also applies to patients who have had a low risk adenoma and subsequent normal colonoscopy Brenner et al. Gastroenterology Brenner et al. Gut
47 Reduced mortality risk after low risk adenoma Loberg et al found a 25% significant relative risk reduction in CRC mortality in patients found to have a low risk adenoma compared to the general population Standardized mortality ratio = 0.75 (95% CI: ) Loberg et al. N Engl J Med
48 CRC Case Study: Part C What if Rahm in the end insists on and completes a screening colonoscopy, when should he have his next CRC screening test and with what modality if his screening colonoscopy is: Normal FIT/FOBT 10 yrs One Hyperplastic polyp FIT/FOBT 10 yrs One to Two Tubular Adenomas FIT/FOBT?TBD One Tubulovillous Adenoma Colonoscopy as per endoscopist 48
49 Cervical Cancer Screening HPV 49
50 Case Study Cervical: Part A You are seeing Ashley, a 32 year old woman who has never had cervical cancer screening. She suffers from vulvodynia and is worried about having a speculum exam She completed three doses of Gardasil 4 eight years ago and is hoping that she does not even need a pap She first became sexually active seven years ago and has only been in same sex relationships 50
51 Case Study Cervical: Part A Should Ashley re-booster (3 doses) with Gardasil 9? 51
52 HPV Booster Vaccines Gardasil 9 Booster after Gardasil 4? No current recommendation for additional 9vHPV doses after completion of series of 4vHPV or 2vHPV Protective benefit against additional 5 HPV types in 9vHPV mostly limited to females (only small % HPV male cancer due to extra HPV 5 types) Safety local reaction redness at site Cost-effective to vaccinate wrt quality-adjusted life year gained 52
53 Case Study Cervical: Part A Does Ashley need any screening given that she has received HPV vaccination prior to any sexual activity and she has only had relationships with women? 53
54 Case Study Cervical: Part A Despite Ashley having had HPV vaccination, she should continue to be screened according to current recommendations Currently a lack of evidence to suggest otherwise
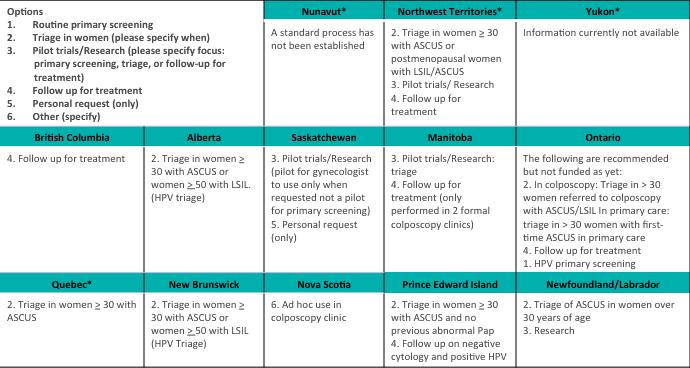
55 CTFPHC 2013 Cervical Screening Guidelines Recommendations for women: Aged 25 to 29: routine screening every 3 years (pap) Weak recommendation; moderate quality evidence Aged 30 to 69: routine screening every 3 years (pap) Strong recommendation; high quality evidence Aged 70 who have been adequately screened (i.e., 3 successive negative Pap tests in the last 10 years), routine screening may cease If not adequately screened continue screening until 3 negative test results have been obtained Weak recommendation; low quality evidence
56 Case Study Cervical: Part A Does Ashley need any screening given that she has only had relationships with women? 56
57 Cervical Screening LGBQT Lower rates of screening in this population Women who have sex with women: same screening regimen as women who have sex with men Transgender men with a cervix: screen according to guidelines
58 Case Study Cervical: Part B Ashley heard that HPV causes cervical cancer and asks why can t we just test for HPV? She is hoping this would be a blood test. Is she correct? 58
59 Cervical Cancer and HPV Over 99% of cervical cancer dysplasia is caused by the Human Papilloma Virus (HPV) Over 80% of sexually active people will acquire HPV in their lifetime Most HPV infections are transient; about 90% will clear in <2 years Cervical cancers occur due to persistent infection with high risk (oncogenic) types of HPV
60 Screening for Cervical Cancer and Premalignant Lesions Abnormal pap tests detect cervical cell changes that are a result of HPV infections Testing for HPV directly does exist 60
61 HPV for Primary Cervical Cancer Screening Strong evidence to support HPV as the primary screening modality for cervical cancer International and national RCTs to support this HPV testing will eventually become the primary screening modality for cervical cancer Must be implemented within a publically funded organized program Available patient-pay basis ~ $90 per test
62 HPV for Primary Cervical Cancer Screening HPV DNA testing is not currently used for primary screening within organized screening programs in Canada However, several provinces and territories have begun to implement or are piloting HPV testing for the purposes of triage or follow-up after treatment, or are piloting its use for primary screening. 62
63
64 What to expect with HPV Primary Screening Recommendations: Start cervical screening with HPV testing at age 25 Collect cells from the cervix to test for the presence of HPV Screening with HPV testing should occur at fiveyear intervals after an initial negative result
65 What to expect with HPV Primary Screening Recommendations: Cease screening in women age 70 who have had an adequate and negative screening history in the prior 10 years (i.e. two negative five-yearly HPV tests) Continue screening women > 65 years who do not meet these requirements at recommended intervals, until two negative tests
66 HPV testing and abnormal cervical cytology Until there is a publically funded primary HPV screening program, expect HPV testing to be increasingly used to manage women with pap abnormalities 66
67 Case Study Cervical: Part C Ashley undergoes a pap which shows ASCUS The sample is further tested for HPV and found to be high risk HPV DNA positive She is referred to colposcopy and managed there for ~2 years Her gynecologist then discharges her back to you When should she have her next cervical screening test?
68 HPV Exit Testing If high risk HPV oncogene-negative at exit, the woman is at or below population risk and can resume routine screening If HPV-positive at exit, she is at elevated risk and should have more frequent testing; at present annual surveillance is recommended
69 Case Study Cervical: Part E What if Ashley had never been vaccinated against HPV. Is it worthwhile for her to get the vaccine now that she has already acquired HPV? 69
70 HPV Vaccination After Colposcopy There is currently no evidence to support the development of a natural HPV immunity In one study women who were vaccinated after the LEEP were 2/3 less likely to have recurrent disease caused by the same HPV genotype In addition these women received protection against other HPV genotypes in the vaccine A growing body of evidence supports the efficacy of HPV vaccination for all age groups (there is no longer an upper age limit) 70
71 Ovarian Cancer Screening 71
72 Case Study Ovarian: Mary You are seeing Mary, a 54 year old woman who received an from her sister She printed up the for you to see It says that ovarian cancer is deadly and can be prevented with a simple blood test called Ca125. It advises women to go to their doctor and insist on having it done The advises to forward the to 10 women that you care about 72
73 Canadian Task Force on Preventative Health Care: Ovarian Cancer Screening In 2013, the CTFPHC issued a critical appraisal report for the Screening for Ovarian Cancer: U.S. Preventative Services Task Force Reaffirmation Recommendation Statement (2013): High quality guideline that can be used to guide preventative care in Canada Recommendation Grade D = recommend against the service. Moderate or high certainty that the service has no benefit or that harms outweigh the benefits 73
74 Canadian Task Force on Preventative Health Care: Ovarian Cancer Screening Screening for ovarian cancer in asymptomatic women is not recommended: Support USPSTF recommendation against screening with transvaginal ultrasonography or CA-125 Absence of evidence to support the effects of screening on mortality Harms of screening high, outweighing any small potential benefit Transvaginal ultrasonography + CA-125 are associated with high false-positive rate: For every 100 women with positive screening result, only 1 has ovarian cancer False-positive test results may lead to unnecessary surgeries and surgical complications Lack of evidence to support regular bimanual pelvic examination for ovarian cancer screening 74
75 Ovarian Cancer Symptoms Despite current evidence against ovarian cancer screening, clinical vigilance is important Symptoms are vague, common ones include: Bloating Feeling full quickly or loss of appetite Abdominal or pelvic discomfort or pain Urinary changes Less common symptoms include: Fatigue, gas, indigestion, nausea, irregular menstrual cycle, changes in bowel habits, changes in weight 75
76 Increased Risk of Ovarian Cancer Increasing age (over 50 years of age) Family history of breast, uterine, ovarian or colorectal cancers Ashkenazi Jewish descent (increased risk of BRCA gene mutation) Known BRCA 1 or BRCA 2 gene mutation or Lynch Syndrome **Refer for genetics**
77 Useful resource ovarian cancer Canadian Task Force on Preventative Health Care (2013 report) U.S. Preventative Services Task Force: Evidence update ovarian cancer screening Ovarian cancer screening recommendation The Canadian Agency for Drugs and Technologies in Health r%20screening%20final.pdf
78 Breast Cancer Screening 78
79 Breast Cancer in Canada In 2017, estimated Canadian women diagnosed with breast cancer 25% of all new cancer cases in women in 2017 Breast cancer = most frequently diagnosed cancer in women 1 in 8 women will develop it in their lifetime The majority of breast cancers (51%) occur in women ages year survival is high = 87% Canadian Cancer Statistics, 2018
80 Canadian Task Force on Preventative Health Care Guidelines (2011, upcoming update 2018) For average risk women: For women aged we recommend not routinely screening with mammography. (Weak recommendation; moderate quality evidence) For women aged years we recommend routinely screening with mammography every 2 to 3 years. (Weak recommendation; moderate quality evidence) For women aged we recommend routinely screening with mammography every 2 to 3 years. (Weak recommendation; low quality evidence) For detailed information:
81 Canadian Task Force on Preventative Health Care Guidelines (2011, upcoming update 2018) Average risk is defined as: No personal history of breast cancer No 1 st degree relative family history of breast cancer No known mutations in BRCA1/BRCA2 genes No previous exposure of radiation to chest wall For detailed information:
82 Breast Cancer Screening Programs in Canada Nunavut* Northwest Territories 2003 Program start date Program name Agency responsible for program administration 2008 Breast Screening Program, Stanton Territorial Health Authority Breast Screening Program, Hay River Health and Social Services Authority Stanton Territorial Health Authority Hay River Health and Social Services Authority Yukon 1990 Yukon Mammography Program Government of Yukon (Yukon Hospital Corporation) British Columbia 1988 BC Cancer Breast Screening BC Cancer Agency Alberta 1990 Alberta Breast Cancer Screening Program (ABCSP) Alberta Health Services Saskatchewan 1990 Screening Program for Breast Cancer Saskatchewan Cancer Agency Manitoba 1995 BreastCheck CancerCare Manitoba Ontario 1990 Ontario Breast Screening Program (OBSP) Cancer Care Ontario Québec 1998 Programme québécois de dépistage du cancer du sein (PQDCS) New Brunswick 1995 New Brunswick Breast Cancer Screening Services Ministère de la Santé et des Services sociaux New Brunswick Cancer Network (NB Department of Health) Nova Scotia 1991 Nova Scotia Breast Screening Program IWK Health Authority Prince Edward Island 1998 PEI Breast Screening Program Health PEI Newfoundland and Labrador *No organized screening program available in Nunavut 1996 Breast Screening Program for Newfoundland and Labrador Eastern Health, Cancer Care Program Slide reproduced from: Canadian Partnership Against Cancer. Breast Cancer Screening in Canada: Environmental Scan [Internet]. Toronto (ON): Canadian Partnership Against Cancer; 2017 [cited ( )]. Available from: ( 82
83 Provincial and Territorial Breast Cancer Screening Clinical Practice Guidelines For asymptomatic women at average risk: Nunavut* Start age Interval Stop age Exclusion criteria Northwest Territories Begin at age 50 (age accepted by physician referral for initial screen but not actively recruited) Yukon Begin at age 50 (age accepted by self-referral but not actively recruited) For women aged annual recall For women aged biennial recall For women aged biennial recall 74 (age 75+ accepted by self referral, but not recalled) 75 Personal history of breast cancer; no NWT healthcare coverage; no primary healthcare provider; acute symptoms; breast implants; breastfeeding in last 3 months Previous breast cancer; breast implants; signs or symptoms of breast cancer British Columbia Begin at age 50 (age accepted by self-referral but not actively recruited) For women aged biennial recall For women aged biennial recall 74 (age 75+ accepted by self referral but not actively recruited or recalled) Previous breast cancer; breast implants *No organized screening program available in Nunavut Slide reproduced from: Canadian Partnership Against Cancer. Breast Cancer Screening in Canada: Environmental Scan [Internet]. Toronto (ON): Canadian Partnership Against Cancer; 2017 [cited ( )]. Available from: ( 83
84 Provincial and Territorial Breast Cancer Screening Clinical Practice Guidelines For asymptomatic women at average risk: Alberta Start age Interval Stop age Exclusion criteria Begin at age 50 (age accepted with physician referral for the first screen) For women aged annual recall For women aged biennial recall 74 Women less than age 40; signs or symptoms of breast cancer; requiring follow-up with diagnostic imaging; requiring work-up for an unknown primary malignancy or possible metastatic disease to the breast or axilla; known diagnosis/history of breast cancer; men Saskatchewan Begin at age 50 (age 49 accepted to mobile unit if turning 50 in same calendar year) Manitoba Begin at 50 (ages accepted to mobile unit with physician referral) For women aged biennial recall For women aged biennial recall For women aged biennial recall 75+ Breast cancer in last 5 years; breast implants 74 (age 75+ accepted by self referral but not actively recruited or recalled) Previous breast cancer; breast implants; had a mammogram in the last 12 months Ontario Begin at age 50 For women aged biennial recall 74 (women 75+ can be screened but require a physician referral; not actively recruited or recalled by the OBSP) Acute breast symptoms; previous breast cancer; breast implants; mastectomy; had a mammogram in the last 11 months Slide reproduced from: Canadian Partnership Against Cancer. Breast Cancer Screening in Canada: Environmental Scan [Internet]. Toronto (ON): Canadian Partnership Against Cancer; 2017 [cited ( )]. Available from: ( 84
85 Provincial and Territorial Breast Cancer Screening Clinical Practice Guidelines For asymptomatic women at average risk: Start age Interval Stop age Exclusion criteria (e.g. no previous breast cancer) Québec Begin at age 50 (accept ages only with physician referral, at a program designated screening or referral centre) For women aged biennial recall 69 (age 70+ only with a physician referral, at a program designated screening or referral centre) Previous breast cancer New Brunswick Begin at age 50 (age accepted only with physician or nurse practitioner referral) For women aged biennial recall 74 (age 74+ only with a physician or nurse practitioner referral) Previous breast cancer Nova Scotia Begin at age 50 (age accepted by selfreferral but not actively recruited) For women aged annual recall For women aged biennial recall 70+ Breast implants; previous breast cancer; signs or symptoms of breast cancer Prince Edward Island Begin at age 40 (accepted by self - referral) For women aged annual recall For women aged biennial recall 74 Previous breast cancer; had a mammogram in the last 12 months; breast implants Newfoundland and Labrador Begin at age 50 For women aged biennial recall 74 (age 74+ only if previously enrolled in the program) Previous breast cancer; breast implants This age group may change to 50-74; currently pending institutional approval Slide reproduced from: Canadian Partnership Against Cancer. Breast Cancer Screening in Canada: Environmental Scan [Internet]. Toronto (ON): Canadian Partnership Against Cancer; 2017 [cited ( )]. Available from: ( 85

86 Breast Cancer Screening Case 1 Joan is 47 years old. She s come into the office with questions about mammograms. Some of her friends have said mammograms are useless, while others underwent mammograms starting at the age of 40 so is she late? What should we tell Joan?
87 Effectiveness of Mammography Are Mammograms Useless? In Nelson et al most recent review - mammography screening is associated with lower breast cancer mortality in women International Agency for Research on Cancer (IARC) reaffirmed - mammographic screening reduces mortality in women and in shows substantial reduction in risk of death from breast cancer In Canada the breast screening programs using mammography are associated with a 40 % decrease in mortality from breast cancer 87
88 So Should Joan proceed to a mammogram? For women between 40 and 49 years of age: Among women who do not screen, the risk of dying from breast cancer is: 1 in 313 With regular screening your risk of dying of breast cancer is: 1 in 370 However, with regular screening: your risk of having a false positive mammogram requiring further screening is: 1 in 3 you risk of having a biopsy is: 1 in 28 your risk of having part or all of a breast removed unnecessarily is: 1 in
89 CTFPHC Recommendation: Mammography (40-49 years) For women aged years we recommend not routinely screening with mammography (Weak recommendation; moderate quality evidence) Slide reproduced from: CTFPHC Breast Cancer Screening Recommendations
90 Findings and Implications: years Significant reduction in RR, but: Screening in women aged decreased the absolute risk of dying from breast cancer by 0.05% CTFPHC judgment: Most women should not receive screening but many could receive it o Less favourable balance of benefit vs. harm, compared to older women o Risk of FP higher, compared to older women o Clinicians must consider patient preferences and values Slide reproduced from: CTFPHC Breast Cancer Screening 90 Recommendations 2011
 Menses before age 15 On oral contraceptives What is your breast cancer screening recommendation for Jane?")
91 Breast Cancer Screening Case 2 Jane 35 years old, pre-menopausal No personal history of cancer Positive family history of breast cancer (her mother and sister) Not received any genetic testing and is unaware of any carriers within her family G1, P1 (no breastfeeding) Menses before age 15 On oral contraceptives What is your breast cancer screening recommendation for Jane? 91

92 Breast Cancer Screening Case 2: Risk Assessment 92

93 High risk breast cancer screening 93
94 Breast Cancer Screening Case 2: Risk Assessment Ontario Breast Screening Program (OBSP): Who Is Eligible? Women ages 30 to 69 are eligible for screening mammography and screening breast magnetic resonance imaging (MRI) (or, if MRI is not medically appropriate, screening breast ultrasound) every year at High Risk OBSP sites Must be at high risk for breast cancer as identified through Category A OR Category B on the Requisition for High Risk Screening Category A: eligible for direct entry into the High Risk OBSP based on personal and family history Category B: genetic assessment required to determine eligibility for the High Risk OBSP Women with bilateral mastectomies are not eligible for the High Risk OBSP 94
95 High Risk OBSP The High Risk OBSP includes the following features: A navigator for specialized support to women at high risk for breast cancer. Organizes genetic assessment and screening tests. Provides counseling regarding the screening and assessment process Facilitation of genetic assessment (i.e., counselling and/or testing) for women who may be at high risk for breast cancer (i.e., fall under Category B) Annual screening for women through the High Risk OBSP with mammography and MRI (or ultrasound if MRI is contraindicated) No self-referrals women at high risk for breast cancer must be referred to the High Risk OBSP by a physician For further information, visit cancercare.on.ca/obsphighrisk.
96 Management of High Risk* by Screening Program Nunavut** Does your program screen women who are identified at high risk (Yes; No) If yes, what is the screening protocol administered by the program Screening modality used (e.g. MRI) Interval (e.g. annual) Start and stop age *High risk = women who are at a greater lifetime risk of developing breast cancer and/or developing more aggressive breast cancers at an earlier age **No organized screening program available in Nunavut ---- No information was provided at the time the data was collected N/A = Not applicable Additional information Northwest Territories Guidelines currently under review Yukon No N/A N/A N/A No current program policies for high risk British Columbia Yes Mammography Annual Women under age 40 are accepted with a physician referral Annual breast MRI is available outside the screening program by physician referral for women with BRCA1/2 gene mutations or very strong family history of breast cancer Alberta No N/A N/A N/A ---- Saskatchewan No N/A N/A N/A ---- Manitoba Yes Mammography Annual Women can access genetic counselling and MRI through physician Ages accepted to mobile unit with physician referral; age 75+ accepted by selfreferral but not actively recruited or recalled Slide reproduced from: Canadian Partnership Against Cancer. Breast Cancer Screening in Canada: Environmental Scan [Internet]. Toronto (ON): Canadian Partnership Against Cancer; 2017 [cited ( )]. Available from: ( 96
97 Management of High Risk* by Screening Program Does your program screen women who are identified at high risk (Yes; No) If yes, what is the screening protocol administered by the program Screening modality used (e.g. MRI) Interval (e.g. annual) Start and stop age Additional information Ontario Québec Yes MRI (or ultrasound if MRI is contraindicated) and mammogram Annual Women who are 70 years and above are screened annually with mammogram only Yes Mammography Biennial Women at high risk are not excluded from the program at this time, they are invited in the same way as women at moderate risk, and the additional investigation is the responsibility of the primary care provider New Brunswick No N/A N/A N/A ---- Nova Scotia Yes Mammography Annual NSBSP is in the process of standardizing the management of high risk women in the breast screening program. Women over the age of 69 are not sent a reminder postcard to book their next screen, but are accepted into the program should they choose to screen Prince Edward Island Newfoundland and Labrador Yes Mammography Annual Ultrasound & MRI are not used as screening modalities No N/A N/A N/A ---- *High risk = women who are at a greater lifetime risk of developing breast cancer and/or developing more aggressive breast cancers at an earlier age ---- No information was provided at the time the data was collected N/A = Not applicable Slide reproduced from: Canadian Partnership Against Cancer. Breast Cancer Screening in Canada: Environmental Scan [Internet]. Toronto (ON): Canadian Partnership Against Cancer; 2017 [cited ( )]. Available from: ( 97
98 Referral for High Risk* Nunavut** Managed by screening program Surveillance/High risk program Diagnostic centre OR referred to: Referral back to primary physician Other (please specify) Northwest Territoriesᶲ No Yukon No N/A N/A N/A N/A British Columbia No (MRI where available in BC) Alberta No (high risk clinics) High risk clinics 2 Genetics clinics Saskatchewan No ---- Centre of Care Manitoba N/A N/A N/A Women identified as high risk may be managed by BreastCheck or by their family physician. They may attend BreastCheck to access screening or a Diagnostic Centre. There are plans to review these guidelines, but currently this work has not yet started *High risk = women who are at a greater lifetime risk of developing breast cancer and/or developing more aggressive breast cancers at an earlier age **No organized screening program available in Nunavut ᶲ Guidelines currently under review ---- No information was provided at the time the data was collected N/A = Not applicable Slide reproduced from: Canadian Partnership Against Cancer. Breast Cancer Screening in Canada: Environmental Scan [Internet]. Toronto (ON): Canadian Partnership Against Cancer; 2017 [cited ( )]. Available from: ( 98
99 Referral for High Risk* Managed by screening program Surveillance/High risk program Diagnostic centre OR referred to: Referral back to primary physician Other (please specify) Ontario No N/A N/A N/A Québec No New Brunswick No** N/A N/A N/A ---- Nova Scotia φ N/A N/A N/A ---- Prince Edward Island N/A N/A N/A N/A Newfoundland and Labrador No *High risk = women who are at a greater lifetime risk of developing breast cancer and/or developing more aggressive breast cancers at an earlier age **The Screening Program only has guidelines for average risk individuals; there is no formal process to identify and manage women at high risk Φ Women under 40 are imaged in a diagnostic centre; they are not part of the screening program Currently standardizing the practice of radiological screening of women at high lifetime risk of breast cancer ---- No information was provided at the time the data was collected N/A = Not applicable Slide reproduced from: Canadian Partnership Against Cancer. Breast Cancer Screening in Canada: Environmental Scan [Internet]. Toronto (ON): Canadian Partnership Against Cancer; 2017 [cited ( )]. Available from: ( 99
100 Breast Cancer Screening: Case 3 The resident you are supervising comes in to ask you to chaperone a clinical breast exam at Sara s (age 52) health visit. Sara, who recently underwent mammography as part of breast screening program, is also inquiring if she should be performing routine breast self examinations. Sara s personal and family history is negative for breast cancer. What do you tell your resident about clinical breast exams? What about breast self examinations?
101 CTFPHC Recommendation: Clinical Breast Exam (CBE) We recommend not routinely performing CBE alone or in conjunction with mammography to screen for breast cancer. (Weak recommendation; low quality evidence) Slide reproduced from: CTFPHC Breast Cancer Screening Recommendations
102 Effectiveness & Harm: Clinical Breast Exam (CBE) Effectiveness of CBE has not been established Harm of CBE: o For each additional cancer detected with CBE per 10,000 women, there would be an additional 55 false-positives (Chiarelli et al, 2009) Slide reproduced from: CTFPHC Breast Cancer Screening 102 Recommendations 2011
103 CTFPHC Recommendation: Breast Self Exam (BSE) We recommend not advising women to routinely practice BSE (Weak recommendation; moderate quality evidence) Slide reproduced from: CTFPHC Breast Cancer Screening Recommendations
104 Effectiveness: Breast Self Exam (BSE) Outcomes Illustrative Comparative Risks* (95% CI) Relative Assumed Risk Corresponding Risk Effect per million per million (range) (95% CI) Control BSE No of Participants (Studies) Quality of the Evidence (GRADE) Breast Cancer Mortality Follow-up: mean 5 years 1,540 1,509 (1,278 to 1,771) RR 0.98 (0.83 to 1.15) 387,359 (2 studies) Moderate 1,2,3 *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). 1 blinding and concealment were not clear 2 no heterogeneity exists. P-value for testing heterogeneity is and I 2 =0%. 3 the question addressed is the same for the evidence regarding the population, comparator and outcome. Slide reproduced from: CTFPHC Breast Cancer Screening Recommendations

105 Breast Cancer Screening: Case 3 Sara asks you if she should also undergo a breast MRI or a breast ultrasound as part of her routine breast cancer screening. What should we tell Sara?
106 CTFPHC Recommendation: Magnetic Resonance Imaging (MRI) We recommend not routinely screening with MRI (Weak recommendation; no evidence) Slide reproduced from: CTFPHC Breast Cancer Screening Recommendations
107 Screening with Breast Ultrasound Mammography is the only primary imaging technique that has been licensed by Health Canada for breast cancer screening for the general population, and is the only screening test that is recommended by evidencebased clinical practice guidelines. The use of MRI as an adjunct for women at very high risk is known and in these women ultrasound has been used but only when MRI is not possible. 107
108 Screening with Breast Ultrasound No evidence to support using bilateral breast ultrasound as a screening tool Has shown to find a few occult cancers on mammography in some studies, but in all studies it has also shown a very large number of false positives resulting in unacceptable numbers of women undergoing unnecessary procedures. 108
109 Estimates of Adverse Outcomes To save one life from breast cancer over 11 years Screening every 2 3 years Unnecessary breast biopsy False positive mammogram Women aged years Women aged years Women aged years 2100 women 75 women 690 women 720 women 26 women 204 women 450 women 11 women 96 women Slide reproduced from: CTFPHC Breast Cancer Screening Recommendations
110 Canadian Task Force of Preventative Health Care: Breast Cancer Screening Recommendations For women aged years we recommend not routinely screening with mammography (Weak recommendation; moderate quality evidence) For women aged years we recommend routinely screening with mammography every 2 to 3 years (Weak recommendation; moderate quality evidence) For women aged years we recommend routinely screening with mammography every 2 to 3 years (Weak recommendation; low quality evidence) Slide reproduced from: CTFPHC Breast Cancer Screening Recommendations
111 Useful Resources 111


112 Canadian Task Force Preventive Health


113 Michael Evans Reframe Health Lab
114 CCO Screening Mobile App/ Web-site App decommissioned February 23th 2018 Removed from app stores No longer up to date CCO launched new responsive website Designed to provide optimal viewing for all devices including mobile phones, tablets, desktops Bookmark pages from cancercareontario.ca website to your favourites 114

115
Updates In Cancer Screening: Navigating a Changing Landscape
 Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Page 1. Selected Controversies. Cancer Screening! Selected Controversies. Breast Cancer Screening. ! Using Best Evidence to Guide Practice!
 Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Breast Cancer Screening in Canada: ENVIRONMENTAL SCAN
 Breast Cancer Screening in Canada: ENVIRONMENTAL SCAN Data collected in 2018 Acknowledgements Production of this environmental scan has been made possible through financial support from Health Canada through
Breast Cancer Screening in Canada: ENVIRONMENTAL SCAN Data collected in 2018 Acknowledgements Production of this environmental scan has been made possible through financial support from Health Canada through
Cancer Screening I have no conflicts of interest. Principles of screening. Cancer in the World Page 1. Letting Evidence Be Our Guide
 Cancer Screening 2012 Letting Evidence Be Our Guide Jeffrey A. Tice, MD Division of General Internal Medicine University of California, San Francisco I have no conflicts of interest Principles of screening
Cancer Screening 2012 Letting Evidence Be Our Guide Jeffrey A. Tice, MD Division of General Internal Medicine University of California, San Francisco I have no conflicts of interest Principles of screening
CANCER SCREENING. Er Chaozer Department of General Medicine, Tan Tock Seng Hospital
 CANCER SCREENING Er Chaozer Department of General Medicine, Tan Tock Seng Hospital Introduction Screening average risk patients Benefits and harms from screening Early cancer detection early treatment
CANCER SCREENING Er Chaozer Department of General Medicine, Tan Tock Seng Hospital Introduction Screening average risk patients Benefits and harms from screening Early cancer detection early treatment
Nicolaus Copernicus University in Torun Medical College in Bydgoszcz Family Doctor Department CANCER PREVENTION IN GENERAL PRACTICE
 Nicolaus Copernicus University in Torun Medical College in Bydgoszcz Family Doctor Department CANCER PREVENTION IN GENERAL PRACTICE A key mission for family medicine is preserving health and maximizing
Nicolaus Copernicus University in Torun Medical College in Bydgoszcz Family Doctor Department CANCER PREVENTION IN GENERAL PRACTICE A key mission for family medicine is preserving health and maximizing
Guidelines for Breast, Cervical and Colorectal Cancer Screening
 Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
SCREENING. Highlights. Introduction HEALTH STATUS REPORT CHAPTER 9: SEPTEMBER 2016
 HEALTH STATUS REPORT SCREENING CHAPTER 9: SEPTEMBER 2016 Highlights Screening represents an effective secondary prevention strategy to reduce the burden of disease, such as cancer. Not having a Pap test
HEALTH STATUS REPORT SCREENING CHAPTER 9: SEPTEMBER 2016 Highlights Screening represents an effective secondary prevention strategy to reduce the burden of disease, such as cancer. Not having a Pap test
Page 1. Cancer Screening for Women I have no conflicts of interest. Overview. Breast, Colon, and Lung Cancer. Jeffrey A.
 Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Selected Controversies. Cancer Screening. Breast Cancer Screening. Selected Controversies. Page 1. Using Best Evidence to Guide Practice
 Cancer Screening Using Best Evidence to Guide Practice Judith M.E. Walsh, MD, MH Division of General Internal Medicine Women s Health Center of Excellence University of California, San Francisco Selected
Cancer Screening Using Best Evidence to Guide Practice Judith M.E. Walsh, MD, MH Division of General Internal Medicine Women s Health Center of Excellence University of California, San Francisco Selected
Cancer Screenings and Early Diagnostics
 Cancer Screenings and Early Diagnostics Ankur R. Parikh, D.O. Medical Director, Center for Advanced Individual Medicine Hematologist/Medical Oncologist Atlantic Regional Osteopathic Convention April 6
Cancer Screenings and Early Diagnostics Ankur R. Parikh, D.O. Medical Director, Center for Advanced Individual Medicine Hematologist/Medical Oncologist Atlantic Regional Osteopathic Convention April 6
Guidelines for the Early Detection of Cancer
 Guidelines for the Early Detection of Cancer The American Cancer Society recommends these cancer screening guidelines for most adults. Screening tests are used to find cancer before a person has any symptoms.
Guidelines for the Early Detection of Cancer The American Cancer Society recommends these cancer screening guidelines for most adults. Screening tests are used to find cancer before a person has any symptoms.
Organized Breast Cancer Screening Programs in Canada REPORT ON PROGRAM PERFORMANCE IN 2007 AND 2008
 Organized Breast Cancer Screening Programs in Canada REPORT ON PROGRAM PERFORMANCE IN 2007 AND 2008 Organized Breast Cancer Screening Programs in Canada REPORT ON PROGRAM PERFORMANCE IN 2007 AND 2008 TO
Organized Breast Cancer Screening Programs in Canada REPORT ON PROGRAM PERFORMANCE IN 2007 AND 2008 Organized Breast Cancer Screening Programs in Canada REPORT ON PROGRAM PERFORMANCE IN 2007 AND 2008 TO
Page 1. Controversies in Cancer Prevention and Screening. Disclosures. Screening. Principles of Screening. I have no conflicts of interest
 Controversies in Cancer Prevention and Screening Disclosures Using the Best Evidence in 2015 I have no conflicts of interest Judith M.E. Walsh, MD, MPH Division of General Internal Medicine Women s Health
Controversies in Cancer Prevention and Screening Disclosures Using the Best Evidence in 2015 I have no conflicts of interest Judith M.E. Walsh, MD, MPH Division of General Internal Medicine Women s Health
Cervical Cancer Screening in Canada: ENVIRONMENTAL SCAN
 Cervical Cancer Screening in Canada: ENVIRONMENTAL SCAN Data collected in 2018 Acknowledgements Production of this environmental scan has been made possible through financial support from Health Canada
Cervical Cancer Screening in Canada: ENVIRONMENTAL SCAN Data collected in 2018 Acknowledgements Production of this environmental scan has been made possible through financial support from Health Canada
Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS RESULTS REPORT
 Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS RESULTS REPORT JANUARY 2011 DECEMBER 2012 Acknowledgments The Canadian Partnership Against Cancer would like to gratefully
Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS RESULTS REPORT JANUARY 2011 DECEMBER 2012 Acknowledgments The Canadian Partnership Against Cancer would like to gratefully
CANCER SCREENING USPSTF AND BEYOND. DeAnn Cummings, MD March 3, 2018
 CANCER SCREENING USPSTF AND BEYOND DeAnn Cummings, MD March 3, 2018 OBJECTIVES Review and discuss cancer screening guidelines for: Colorectal CA Prostate CA Breast CA Ovarian CA Secondary prevention, NOT
CANCER SCREENING USPSTF AND BEYOND DeAnn Cummings, MD March 3, 2018 OBJECTIVES Review and discuss cancer screening guidelines for: Colorectal CA Prostate CA Breast CA Ovarian CA Secondary prevention, NOT
Recommendations on Screening for Colorectal Cancer 2016
 Recommendations on Screening for Colorectal Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude
Recommendations on Screening for Colorectal Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude
Decoding the USPSTF. By: Dr Vikram Arora Heritage Valley Health System
 Decoding the USPSTF By: Dr Vikram Arora Heritage Valley Health System Objectives O Gain insight into function of USPSTF O Review grading system O Critically appraise key current recommendations of the
Decoding the USPSTF By: Dr Vikram Arora Heritage Valley Health System Objectives O Gain insight into function of USPSTF O Review grading system O Critically appraise key current recommendations of the
Lung Cancer Screening in Canada: ENVIRONMENTAL SCAN
 Lung Cancer Screening in Canada: ENVIRONMENTAL SCAN Data collected in 2018 Acknowledgements Production of this environmental scan has been made possible through financial support from Health Canada through
Lung Cancer Screening in Canada: ENVIRONMENTAL SCAN Data collected in 2018 Acknowledgements Production of this environmental scan has been made possible through financial support from Health Canada through
Evidence-based Cancer Screening & Surveillance
 Oncology for Scientists Spring 2014 Evidence-based Cancer Screening & Surveillance Martin C. Mahoney, MD, PhD, FAAFP Departments of Medicine & Health Behavior /Oncology_Feb 2014.ppt 1 Objectives: Principles
Oncology for Scientists Spring 2014 Evidence-based Cancer Screening & Surveillance Martin C. Mahoney, MD, PhD, FAAFP Departments of Medicine & Health Behavior /Oncology_Feb 2014.ppt 1 Objectives: Principles
Cancer Facts for Women
 Cancer Facts for Women Some of the cancers that most often affect women are breast, colorectal, endometrial, lung, cervical, skin, and ovarian cancers. Knowing about these cancers and what you can do to
Cancer Facts for Women Some of the cancers that most often affect women are breast, colorectal, endometrial, lung, cervical, skin, and ovarian cancers. Knowing about these cancers and what you can do to
Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program
 Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program A B C D USPSTF recommends the service. There is high certainty that Offer or provide
Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program A B C D USPSTF recommends the service. There is high certainty that Offer or provide
A senior s guide for preventative healthcare services Ynolde F. Smith D.O.
 A senior s guide for preventative healthcare services Ynolde F. Smith D.O. What can we do to prevent disease? Exercise Eating Well Keep a healthy weight Injury prevention Mental Health Social issues (care
A senior s guide for preventative healthcare services Ynolde F. Smith D.O. What can we do to prevent disease? Exercise Eating Well Keep a healthy weight Injury prevention Mental Health Social issues (care
Screening tests. When you need them and when you don t
 Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
Screening tests When you need them and when you don t S creening tests help doctors look for diseases when you don t have symptoms. The tests can Screenings find problems early, when they are easier to
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer
 Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
Recent Changes in Cervical Cancer Screening in Canada
 Recent Changes in Cervical Cancer Screening in Canada Meg McLachlin, MD, FRCPC Program Head, Pathology Senior Medical Director, Diagnostic Services Recent Changes in Cervical Cancer Screening in Canada
Recent Changes in Cervical Cancer Screening in Canada Meg McLachlin, MD, FRCPC Program Head, Pathology Senior Medical Director, Diagnostic Services Recent Changes in Cervical Cancer Screening in Canada
Canadian Task Force on Preventive Health Care
 Screening for Cervical Cancer: Recommendations 2013 Canadian Task Force on Preventive Health Care Presentation for free use to disseminate Guidelines. Feb 2013 Putting Prevention into Practice Canadian
Screening for Cervical Cancer: Recommendations 2013 Canadian Task Force on Preventive Health Care Presentation for free use to disseminate Guidelines. Feb 2013 Putting Prevention into Practice Canadian
Preventive Health Guidelines
 Preventive Health Guidelines Guide to Clinical Preventive Services Adult LifeWise has adopted the United States Preventive Services Task Force (USPSTF) Guide to Clinical Preventive Services. The guideline
Preventive Health Guidelines Guide to Clinical Preventive Services Adult LifeWise has adopted the United States Preventive Services Task Force (USPSTF) Guide to Clinical Preventive Services. The guideline
GUIDELINES FOR MONITORING BREAST CANCER SCREENING PROGRAM PERFORMANCE THIRD EDITION
 Report from the Evaluation Indicators Working Group GUIDELINES FOR MONITORING BREAST CANCER SCREENING PROGRAM PERFORMANCE THIRD EDITION Public Health Agency of Canada Acknowledgments We would like to acknowledge
Report from the Evaluation Indicators Working Group GUIDELINES FOR MONITORING BREAST CANCER SCREENING PROGRAM PERFORMANCE THIRD EDITION Public Health Agency of Canada Acknowledgments We would like to acknowledge
Colorectal Cancer Screening in Canada: ENVIRONMENTAL SCAN
 Colorectal Cancer Screening in Canada: ENVIRONMENTAL SCAN Data collected in 2018 Acknowledgements Production of this environmental scan has been made possible through financial support from Health Canada
Colorectal Cancer Screening in Canada: ENVIRONMENTAL SCAN Data collected in 2018 Acknowledgements Production of this environmental scan has been made possible through financial support from Health Canada
Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS
 Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS RESULTS REPORT JANUARY 2013 DECEMBER 2014 Acknowledgements The Canadian Partnership Against Cancer (the Partnership)
Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS RESULTS REPORT JANUARY 2013 DECEMBER 2014 Acknowledgements The Canadian Partnership Against Cancer (the Partnership)
Cancer Screening 2009: New Tests, New Choices
 Objectives Cancer Screening 2009: New Tests, New Choices UCSF Annual Review in Family Medicine April 21, 2009 Michael B. Potter, MD Professor, Clinical Family and Community Medicine UCSF School of Medicine
Objectives Cancer Screening 2009: New Tests, New Choices UCSF Annual Review in Family Medicine April 21, 2009 Michael B. Potter, MD Professor, Clinical Family and Community Medicine UCSF School of Medicine
Information for trans people
 NHS Screening Programmes Public Health England leads the NHS Screening Programmes About this leaflet This leaflet is for trans (transgender) and non-binary people in England. It tells you about the adult
NHS Screening Programmes Public Health England leads the NHS Screening Programmes About this leaflet This leaflet is for trans (transgender) and non-binary people in England. It tells you about the adult
Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow
 Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow Debra A. Walz, RN, MS, AOCNP, WHNP-BC, RNFA Advanced Oncology & Women s Health Nurse Practitioner Oneida
Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow Debra A. Walz, RN, MS, AOCNP, WHNP-BC, RNFA Advanced Oncology & Women s Health Nurse Practitioner Oneida
Cancer in Women. Lung cancer. Breast cancer
 Cancer in Women You can get cancer at any age, but it is more likely as you get older. The types of cancer people get and the risk of dying from cancer are not the same for all ethnic groups. Here are
Cancer in Women You can get cancer at any age, but it is more likely as you get older. The types of cancer people get and the risk of dying from cancer are not the same for all ethnic groups. Here are
10/25/2011 OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screenin
 OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screening Kathy Gray, DNP, CRNP, FNP-BC Cancer Screenings and Guidelines
OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screening Kathy Gray, DNP, CRNP, FNP-BC Cancer Screenings and Guidelines
CANCER SCREENING USPSTF AND BEYOND. DeAnn Cummings, MD March 9, 2019
 CANCER SCREENING USPSTF AND BEYOND DeAnn Cummings, MD March 9, 2019 OBJECTIVES Review and discuss cancer screening guidelines for: Colorectal CA Prostate CA Breast CA Ovarian CA Secondary prevention, NOT
CANCER SCREENING USPSTF AND BEYOND DeAnn Cummings, MD March 9, 2019 OBJECTIVES Review and discuss cancer screening guidelines for: Colorectal CA Prostate CA Breast CA Ovarian CA Secondary prevention, NOT
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA
 Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Transition to Fecal Immunochemical Testing (FIT)
") Transition to Fecal Immunochemical Testing (FIT) Frequently Asked Questions for Primary Care Providers October 2017 Version 1.1 Overview Ontario will be transitioning from the guaiac fecal occult blood
Transition to Fecal Immunochemical Testing (FIT) Frequently Asked Questions for Primary Care Providers October 2017 Version 1.1 Overview Ontario will be transitioning from the guaiac fecal occult blood
A patient s guide to understanding. Cancer. Screening
 A patient s guide to understanding Cancer Screening Contents 04 06 10 12 Cancer Screening Who Should Go For Cancer Screening 05 Nasopharyngeal Carcinoma Colorectal Cancer 08 Lung Cancer Liver Cancer Breast
A patient s guide to understanding Cancer Screening Contents 04 06 10 12 Cancer Screening Who Should Go For Cancer Screening 05 Nasopharyngeal Carcinoma Colorectal Cancer 08 Lung Cancer Liver Cancer Breast
PREVENTION CARE IN ADULTS
 PREVENTION CARE IN ADULTS Hong Xiao, M.D. Department of Family & Community Medicine Weight and BMI Abdominal Aortic Aneurysm (AAA) Blood Pressure Breast Exam Breast Cancer Mammogram Breast Cancer BRCA
PREVENTION CARE IN ADULTS Hong Xiao, M.D. Department of Family & Community Medicine Weight and BMI Abdominal Aortic Aneurysm (AAA) Blood Pressure Breast Exam Breast Cancer Mammogram Breast Cancer BRCA
I have no financial interests in any product I will discuss today.
 Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Breast Cancer Screening
 Breast Cancer Screening Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Breast Cancer Screening Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Preventive Services Explained
 Preventive Services Explained Medicare covers many preventive care services without charge. Most of these services have been recommended by the U.S. Preventive Services Task Force. However, which beneficiaries
Preventive Services Explained Medicare covers many preventive care services without charge. Most of these services have been recommended by the U.S. Preventive Services Task Force. However, which beneficiaries
Organized Breast Cancer Screening Programs in Canada
 Public Health Agency of Canada Agence de santé publique du Canada Organized Breast Cancer Screening Programs in Canada Yukon Mammography Program Government of the Northwest Territories Government of Nunavut
Public Health Agency of Canada Agence de santé publique du Canada Organized Breast Cancer Screening Programs in Canada Yukon Mammography Program Government of the Northwest Territories Government of Nunavut
Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE
 Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE DEBATE Presenters PRESENTATION MODERATOR Dr. Praveen Bansal -MD, CCFP FCFP Regional Primary Care Lead, Integrated Cancer Screening,
Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE DEBATE Presenters PRESENTATION MODERATOR Dr. Praveen Bansal -MD, CCFP FCFP Regional Primary Care Lead, Integrated Cancer Screening,
Health Interventions in Ambulatory Cancer Care Centres
 ENVIRONMENTAL SCAN Health Interventions in Ambulatory Cancer Care Centres Context Cancer a complex, chronic condition will affect an estimated two in five Canadians in their lifetime. 1 Cancer requires
ENVIRONMENTAL SCAN Health Interventions in Ambulatory Cancer Care Centres Context Cancer a complex, chronic condition will affect an estimated two in five Canadians in their lifetime. 1 Cancer requires
Objectives. I have no financial interests in any product I will discuss today. Cervical Cancer Screening Guidelines: Updates and Controversies
 Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Optima Health. Adult Health Maintenance Guidelines. Guideline History. Original Approve Date 04/93
 Optima Health Adult Health Maintenance Guidelines Guideline History Original Approve Date 04/93 Review/ Revise Dates 8/94, 8/96, 6/97, 7/97, 10/98, 10/99, 5/00, 2/01,6/03, 06/05, 12/07,01/09, 1/10, 1/11,
Optima Health Adult Health Maintenance Guidelines Guideline History Original Approve Date 04/93 Review/ Revise Dates 8/94, 8/96, 6/97, 7/97, 10/98, 10/99, 5/00, 2/01,6/03, 06/05, 12/07,01/09, 1/10, 1/11,
Screening for Genes for Hereditary Breast and Ovarian Cancer in Jewish Women
 Screening for Genes for Hereditary Breast and Ovarian Cancer in Jewish Women Background About 5% of women in Canada with breast cancer and about 12% of women with ovarian cancer, are born with an inherited
Screening for Genes for Hereditary Breast and Ovarian Cancer in Jewish Women Background About 5% of women in Canada with breast cancer and about 12% of women with ovarian cancer, are born with an inherited
Program Guidelines Clinical Guidelines Patient Enrollment Resource Documents Eligibility Guidelines... 2
 BREAST AND CERVICAL CANCER TABLE OF CONTENTS Program Guidelines... 1 Clinical Guidelines... 1 Patient Enrollment... 1 Resource Documents... 1 Eligibility Guidelines... 2 Breast Screening Guidelines and
BREAST AND CERVICAL CANCER TABLE OF CONTENTS Program Guidelines... 1 Clinical Guidelines... 1 Patient Enrollment... 1 Resource Documents... 1 Eligibility Guidelines... 2 Breast Screening Guidelines and
Screening and Detection in Cancer Survivors. Jose W. Avitia, MD Oncology/Hematology
 Screening and Detection in Cancer Survivors Jose W. Avitia, MD Oncology/Hematology Breast Cancer Summary of 2012 ASCO guideline recommendations for surveillance after breast cancer treatment History/physical
Screening and Detection in Cancer Survivors Jose W. Avitia, MD Oncology/Hematology Breast Cancer Summary of 2012 ASCO guideline recommendations for surveillance after breast cancer treatment History/physical
Cancer Control in the Workplace: A Corporate Standard
 Healthy Outcomes Conference, Whistler, BC March 31 April 2, 2009 Cancer Control in the Workplace: A Corporate Standard Dr. Alain Sotto, Hon.BSc, MD, CCFP(EM), FCBOM Chief Physician, Ontario Power Generation
Healthy Outcomes Conference, Whistler, BC March 31 April 2, 2009 Cancer Control in the Workplace: A Corporate Standard Dr. Alain Sotto, Hon.BSc, MD, CCFP(EM), FCBOM Chief Physician, Ontario Power Generation
Cancer Screening & Prevention. Dr. Jamey Burton, MD, FAAFP
 Cancer Screening & Prevention Dr. Jamey Burton, MD, FAAFP Cervical Cancer Breast Cancer Colon Cancer Prostate Cancer Lung Cancer How common is cervical cancer? What causes it? What screening is needed?
Cancer Screening & Prevention Dr. Jamey Burton, MD, FAAFP Cervical Cancer Breast Cancer Colon Cancer Prostate Cancer Lung Cancer How common is cervical cancer? What causes it? What screening is needed?
Screening for Breast Cancer
 Understanding Task Force Recommendations Screening for Breast Cancer U.S. Preventive Services Task Force (Task Force) has issued a final recommendation statement on Screening for Breast Cancer. se final
Understanding Task Force Recommendations Screening for Breast Cancer U.S. Preventive Services Task Force (Task Force) has issued a final recommendation statement on Screening for Breast Cancer. se final
Health Interventions in Ambulatory Cancer Care Centres DRAFT. Objectives. Methods
 ENVIRONMENTAL SCAN Health Interventions in Ambulatory Cancer Care Centres Context Cancer, a complex, chronic condition, will affect an estimated two in five Canadians in their lifetime. 1 Cancer requires
ENVIRONMENTAL SCAN Health Interventions in Ambulatory Cancer Care Centres Context Cancer, a complex, chronic condition, will affect an estimated two in five Canadians in their lifetime. 1 Cancer requires
CVIM s Cancer Screening Practices
 12-13-17 Professional Practice Minutes CVIM s Cancer Screening Practices At CVIM, preventative health care is very important! In these minutes you will find a review of our recommendations for cancer screening
12-13-17 Professional Practice Minutes CVIM s Cancer Screening Practices At CVIM, preventative health care is very important! In these minutes you will find a review of our recommendations for cancer screening
Physiotherapists in Canada, 2011 National and Jurisdictional Highlights
 pic pic pic Physiotherapists in Canada, 2011 National and Jurisdictional Highlights Spending and Health Workforce Our Vision Better data. Better decisions. Healthier Canadians. Our Mandate To lead the
pic pic pic Physiotherapists in Canada, 2011 National and Jurisdictional Highlights Spending and Health Workforce Our Vision Better data. Better decisions. Healthier Canadians. Our Mandate To lead the
Current Strategies in the Detection of Breast Cancer. Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF
 Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Protect & Detect: What Women should Know about cancer. The American College of Obstetricians and Gynecologists
 Protect & Detect: What Women should Know about cancer The American College of Obstetricians and Gynecologists A Message From ACOG President Kenneth L. Noller, MD Dr. Noller is the Louis E. Phaneuf professor
Protect & Detect: What Women should Know about cancer The American College of Obstetricians and Gynecologists A Message From ACOG President Kenneth L. Noller, MD Dr. Noller is the Louis E. Phaneuf professor
Breast Cancer Screening Clinical Practice Guideline. Kaiser Permanente National Breast Cancer Screening Guideline Development Team
 NATIONAL CLINICAL PRACTICE GUIDELINE Breast Cancer Screening Clinical Practice Guideline Kaiser Permanente National Breast Cancer Screening Guideline Development Team This guideline is informational only.
NATIONAL CLINICAL PRACTICE GUIDELINE Breast Cancer Screening Clinical Practice Guideline Kaiser Permanente National Breast Cancer Screening Guideline Development Team This guideline is informational only.
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Recommendations on Screening for Lung Cancer 2016
 Recommendations on Screening for Lung Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude canadien
Recommendations on Screening for Lung Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude canadien
BREAST CANCER & CERVICAL CANCER SCREENING
 BREAST CANCER & CERVICAL CANCER 1 BREAST Cancer WHAT IS BREAST CANCER? Breast cancer starts when cells in the breast begin to grow in an uncontrolled way and build up to form a lump (also known as a tumour).
BREAST CANCER & CERVICAL CANCER 1 BREAST Cancer WHAT IS BREAST CANCER? Breast cancer starts when cells in the breast begin to grow in an uncontrolled way and build up to form a lump (also known as a tumour).
Information leaflet for women with an increased lifetime risk of breast and ovarian cancer. Hereditary Breast and Ovarian Cancer (HBOC)
") Information leaflet for women with an increased lifetime risk of breast and ovarian cancer Hereditary Breast and Ovarian Cancer (HBOC) What is Hereditary Breast and Ovarian Cancer (HBOC)? Hereditary Breast
Information leaflet for women with an increased lifetime risk of breast and ovarian cancer Hereditary Breast and Ovarian Cancer (HBOC) What is Hereditary Breast and Ovarian Cancer (HBOC)? Hereditary Breast
Pap Smears Pelvic Examinations Well Woman Examinations. When should you have them performed???
 Pap Smears Pelvic Examinations Well Woman Examinations. When should you have them performed??? Arlene Evans-DeBeverly, PA-C Copyright 2012 There are always ongoing changes in gynecology, including the
Pap Smears Pelvic Examinations Well Woman Examinations. When should you have them performed??? Arlene Evans-DeBeverly, PA-C Copyright 2012 There are always ongoing changes in gynecology, including the
This information explains the advice about familial breast cancer (breast cancer in the family) that is set out in NICE guideline CG164.
 that is set out in NICE guideline CG164.") Familial breast cancer (breast cancer in the family) Information for the public Published: 1 June 2013 nice.org.uk About this information NICE guidelines provide advice on the care and support that should
Familial breast cancer (breast cancer in the family) Information for the public Published: 1 June 2013 nice.org.uk About this information NICE guidelines provide advice on the care and support that should
Member Newsletter Vol. 1, What cancer screenings should I get? AETNA BETTER HEALTH OF MISSOURI. Early detection can lower your risk
 AETNA BETTER HEALTH OF MISSOURI Member Newsletter Vol. 1, 2016 What cancer screenings should I get? Early detection can lower your risk Cancer screenings can help detect cancer in the early stages. Early
AETNA BETTER HEALTH OF MISSOURI Member Newsletter Vol. 1, 2016 What cancer screenings should I get? Early detection can lower your risk Cancer screenings can help detect cancer in the early stages. Early
Cancer Facts for People Over 50
 National Institute on Aging AgePage Cancer Facts for People Over 50 Cancer strikes people of all ages, but you are more likely to get cancer as you get older, even if no one in your family has ever had
National Institute on Aging AgePage Cancer Facts for People Over 50 Cancer strikes people of all ages, but you are more likely to get cancer as you get older, even if no one in your family has ever had
Optima Health. Adult Health Maintenance Guidelines. Guideline History Original Approve Date 04/93
 Optima Health Adult Health Maintenance Guidelines Guideline History Original Approve Date 04/93 Review/ Revise Dates 8/94, 8/96, 6/97, 7/97, 10/98, 10/99, 5/00, 2/01,6/03, 06/05, 12/07,01/09, 1/10, 1/11,
Optima Health Adult Health Maintenance Guidelines Guideline History Original Approve Date 04/93 Review/ Revise Dates 8/94, 8/96, 6/97, 7/97, 10/98, 10/99, 5/00, 2/01,6/03, 06/05, 12/07,01/09, 1/10, 1/11,
Debate: General surveillance/screening for colon cancer in a resource constrained environment is imperative
 Debate: General surveillance/screening for colon cancer in a resource constrained environment is imperative Dr. Meryl Oyomno Department of surgery, University of Pretoria INTRODUCTION Screening is the
Debate: General surveillance/screening for colon cancer in a resource constrained environment is imperative Dr. Meryl Oyomno Department of surgery, University of Pretoria INTRODUCTION Screening is the
LDCT Screening. Steven Kirtland, MD. Virginia Mason Medical Center February 27, 2015
 LDCT Screening Steven Kirtland, MD Virginia Mason Medical Center February 27, 2015 2 Disclosures 4 5 Cancer Screening Mrs H 64yo 50 pk year smoker Lung Cancer Epidemiology Leading Cause of Cancer Death
LDCT Screening Steven Kirtland, MD Virginia Mason Medical Center February 27, 2015 2 Disclosures 4 5 Cancer Screening Mrs H 64yo 50 pk year smoker Lung Cancer Epidemiology Leading Cause of Cancer Death
Let s look a minute at the evidence supporting current cancer screening recommendations.
 I m Dr. Therese Bevers, Medical Director of the Cancer Prevention Center and Professor of Clinical Cancer Prevention at The University of Texas MD Anderson Cancer Center. Today s lecture is on screening
I m Dr. Therese Bevers, Medical Director of the Cancer Prevention Center and Professor of Clinical Cancer Prevention at The University of Texas MD Anderson Cancer Center. Today s lecture is on screening
CANCER Hafsa Raheel, MD, FCPS (Com med), MCPS (Fam med)
, MCPS (Fam med)") CANCER Hafsa Raheel, MD, FCPS (Com med), MCPS (Fam med) Acknowledgement Dr. Haytham AlSaif OBJECTIVES 1. Appreciate the Global impact of cancer. 2. Identify the most prevalent cancers worldwide, in the
CANCER Hafsa Raheel, MD, FCPS (Com med), MCPS (Fam med) Acknowledgement Dr. Haytham AlSaif OBJECTIVES 1. Appreciate the Global impact of cancer. 2. Identify the most prevalent cancers worldwide, in the
VERSION STUDENT. Cases in Population-Oriented Prevention (C-POP)-based teaching cases. A Critical Look at Prevention: Colorectal Cancer Screening
-based teaching cases. A Critical Look at Prevention: Colorectal Cancer Screening") STUDENT VERSION This project has the objective to develop preventive medicine teaching cases that will motivate medical students, residents and faculty to improve clinical preventive competencies complemented
STUDENT VERSION This project has the objective to develop preventive medicine teaching cases that will motivate medical students, residents and faculty to improve clinical preventive competencies complemented
Manitoba EMR Data Extract Specifications
 MANITOBA HEALTH, HEALTHY LIVING AND SENIORS Manitoba Data Specifications Version 2 Updated: September 11, 2015 1 Introduction The purpose of this document is to describe the data to be included in the
MANITOBA HEALTH, HEALTHY LIVING AND SENIORS Manitoba Data Specifications Version 2 Updated: September 11, 2015 1 Introduction The purpose of this document is to describe the data to be included in the
Disclosures. Overview. Selection the most accurate statement: Updates in Lung Cancer Screening 5/26/17. No Financial Disclosures
 Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Breast Cancer Screening September 21, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Breast Cancer Screening September 21, 2017 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer Screening American
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Breast Cancer Screening September 21, 2017 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer Screening American
Summary of Cancer Prevention and Screening Benefits of the Affordable Care Act (ACA) in Kentucky (includes kynect)
 in Kentucky (includes kynect)") Summary of Cancer Prevention and Screening Benefits of the Talk with patients about ü Potential benefits, harms, and uncertainties of cancer screening ü Identify family history ü Cancer prevention, early
Summary of Cancer Prevention and Screening Benefits of the Talk with patients about ü Potential benefits, harms, and uncertainties of cancer screening ü Identify family history ü Cancer prevention, early
Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over
 Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over 1. BMI - Documented in patients medical record on an annual basis up to age 74. Screen for obesity and offer counseling to encourage
Preventive Care Guideline for Asymptomatic Elderly Patients Age 65 and Over 1. BMI - Documented in patients medical record on an annual basis up to age 74. Screen for obesity and offer counseling to encourage
Shared Decision Making in Breast and Prostate Cancer Screening. An Update and a Patient-Centered Approach. Sharon K. Hull, MD, MPH July, 2017
 Shared Decision Making in Breast and Prostate Cancer Screening An Update and a Patient-Centered Approach Sharon K. Hull, MD, MPH July, 2017 Overview Epidemiology of Breast and Prostate Cancer Controversies
Shared Decision Making in Breast and Prostate Cancer Screening An Update and a Patient-Centered Approach Sharon K. Hull, MD, MPH July, 2017 Overview Epidemiology of Breast and Prostate Cancer Controversies
Dealing with uncertainty CANCER IN GENERAL PRACTICE SCREENING AND EARLY DIAGNOSIS FRJ SEPT 12
 Dealing with uncertainty CANCER IN GENERAL PRACTICE SCREENING AND EARLY DIAGNOSIS FRJ SEPT 12 The 21 st century GP dilemma The attempt to prevent illnesses has led to labelling of an ever increasing proportion
Dealing with uncertainty CANCER IN GENERAL PRACTICE SCREENING AND EARLY DIAGNOSIS FRJ SEPT 12 The 21 st century GP dilemma The attempt to prevent illnesses has led to labelling of an ever increasing proportion
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
The 2012 SAGE Wait Time Program: Survey of Access to GastroEnterology in Canada Can J Gastroenterol 2013;27:83-9.
 The 2012 SAGE Wait Time Program: Survey of Access to GastroEnterology in Canada Can J Gastroenterol 2013;27:83-9. Desmond Leddin MB, David Armstrong MD, Mark Borgaonkar MD, Ronald J Bridges MD, Carlo A
The 2012 SAGE Wait Time Program: Survey of Access to GastroEnterology in Canada Can J Gastroenterol 2013;27:83-9. Desmond Leddin MB, David Armstrong MD, Mark Borgaonkar MD, Ronald J Bridges MD, Carlo A
Optimizing implementation of fecal immunochemical testing in Ontario: A randomized controlled trial
 Optimizing implementation of fecal immunochemical testing in Ontario: A randomized controlled trial J. Tinmouth, N.N. Baxter, L.F. Paszat, E. Randell, M. Serenity, R. Sutradhar, L. Rabeneck Conflicts of
Optimizing implementation of fecal immunochemical testing in Ontario: A randomized controlled trial J. Tinmouth, N.N. Baxter, L.F. Paszat, E. Randell, M. Serenity, R. Sutradhar, L. Rabeneck Conflicts of
West Nile virus and Other Mosquito borne Diseases National Surveillance Report English Edition
 and Other Mosquito borne Diseases National Surveillance Report English Edition July to July 8, 17 (Week 7) West Nile Virus Canada Humans As of surveillance week 7, ending on July 8, 17, the Public Health
and Other Mosquito borne Diseases National Surveillance Report English Edition July to July 8, 17 (Week 7) West Nile Virus Canada Humans As of surveillance week 7, ending on July 8, 17, the Public Health
Screening Mammograms: Questions and Answers
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Screening Mammograms:
The Big Three Screening for breast, cervical & colon cancer; the where, when and how Areview of the latest guidelines and local resources
 The Big Three Screening for breast, cervical & colon cancer; the where, when and how Areview of the latest guidelines and local resources Why Screen? Screen for Life Cancer screening sees what you can
The Big Three Screening for breast, cervical & colon cancer; the where, when and how Areview of the latest guidelines and local resources Why Screen? Screen for Life Cancer screening sees what you can
Melissa Hartman, DO Women s Health Orlando VA Medical Center
 Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Follow-up for Cervical Cancer
, Cancer Care Ontario (CCO) Follow-up for Cervical Cancer") Guideline 4-16 Version 2 A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Follow-up for Cervical Cancer L. Elit, E.B. Kennedy, A. Fyles, U. Metser, and the PEBC
Guideline 4-16 Version 2 A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Follow-up for Cervical Cancer L. Elit, E.B. Kennedy, A. Fyles, U. Metser, and the PEBC
Foundational funding sources allow BCCHP to screen and diagnose women outside of the CDC guidelines under specific circumstances in Washington State.
 Program Description The Breast, Cervical and Colon Health Program (BCCHP) screens qualifying clients for breast cancer. The program is funded through a grant from the Centers for Disease Control and Prevention
Program Description The Breast, Cervical and Colon Health Program (BCCHP) screens qualifying clients for breast cancer. The program is funded through a grant from the Centers for Disease Control and Prevention
OSCAR EMR Cancer Screening Guidelines
 OSCAR EMR Cancer Screening Guidelines Version 2.3 November 2018 Cancer Care Ontario Primary Care Lead (HNHB LHIN) Table of Contents OSCAR EMR Cancer Screening Guidelines 1. INTRODUCTION GETTING READY...
OSCAR EMR Cancer Screening Guidelines Version 2.3 November 2018 Cancer Care Ontario Primary Care Lead (HNHB LHIN) Table of Contents OSCAR EMR Cancer Screening Guidelines 1. INTRODUCTION GETTING READY...
Breast Cancer Screening
 Breast Cancer Screening Claire Frost, MD R3 Talks 1 Objective 1. Understand risks and benefits of screening by reviewing current literature 2. Evaluate major society recommendations on breast cancer screening
Breast Cancer Screening Claire Frost, MD R3 Talks 1 Objective 1. Understand risks and benefits of screening by reviewing current literature 2. Evaluate major society recommendations on breast cancer screening
Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D
 Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D Menopause and Cancer How does menopause affect a woman s cancer risk? Ø Menopause does not cause cancer.but risk of developing
Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D Menopause and Cancer How does menopause affect a woman s cancer risk? Ø Menopause does not cause cancer.but risk of developing
vaccination in Canada Bernard Duval, md, mph, frcpc Institut National de Santé Publique du Québec Québec, Canada Sevilla,
 Follow-up of hepatitis B vaccination in Canada Bernard Duval, md, mph, frcpc Institut National de Santé Publique du Québec Québec, Canada Sevilla, 2004-03 03-11 HB in Canada Low endemicity: HBsAg+ : 0.5%
Follow-up of hepatitis B vaccination in Canada Bernard Duval, md, mph, frcpc Institut National de Santé Publique du Québec Québec, Canada Sevilla, 2004-03 03-11 HB in Canada Low endemicity: HBsAg+ : 0.5%
Report from the National Diabetes Surveillance System:
 Report from the National Diabetes Surveillance System: Diabetes in Canada, 28 To promote and protect the health of Canadians through leadership, partnership, innovation and action in public health. Public
Report from the National Diabetes Surveillance System: Diabetes in Canada, 28 To promote and protect the health of Canadians through leadership, partnership, innovation and action in public health. Public
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
ABOUT FMC MEMBERSHIP:
 ABOUT FMC MEMBERSHIP: FMC and your provincial/territorial association are a part of a network of interdisciplinary professionals made up of private and court connected mediators, lawyers, social workers,
ABOUT FMC MEMBERSHIP: FMC and your provincial/territorial association are a part of a network of interdisciplinary professionals made up of private and court connected mediators, lawyers, social workers,
Ovarian Cancer. What you should know. making cancer less frightening by enlightening
 Ovarian Cancer What you should know making cancer less frightening by enlightening ovarian cancer the facts Over 360 cases are diagnosed in Ireland annually It is the 6th most common cancer in women 4
Ovarian Cancer What you should know making cancer less frightening by enlightening ovarian cancer the facts Over 360 cases are diagnosed in Ireland annually It is the 6th most common cancer in women 4