Histotechnological problems in dermatopathology and their possible consequences
|
|
|
- Lauren Simmons
- 5 years ago
- Views:
Transcription
1 Histotechnological problems in dermatopathology and their possible consequences Zsolt B. Argenyi, M.D. Professor of Pathology & Dermatology Director of Dermatopathology University of Washington, Seattle, WA, USA
2 What a timely topic! Election year Major health care reform Technological explosions Global economic changes Patient privacy issues
3 Dermatopathologists are also under the microscope Provide High Quality Health Care Correct Diagnosis Safety Timelines Effectiveness Efficiency Equivity Patient centeredness (per Institute of Medicine)
4 How to avoid error by a) Increase accuracy correct diagnosis b) Increase precision consistency for reproducibility Think Global Act Specific
5 Raab, S.S., Quality in Cancer Diagnosis, CA Cancer J Clin 2010;60:
6 Percentages of errors in the various phases of TAT Preanalytic phase;32-75% Analytic phase;13-32% Postanalytic phase;9-31% Raab, S.S., Quality in Cancer Diagnosis, CA Cancer J Clin 2010;60:
7 Error Root Cause Analysis Worksteps activities connections pathways steps preanalytic analytic postanalytic
8 SUBSTEP Accessioning steps Specimen receipt in laboratory (transport hand-off) Identification check Assignment of unique laboratory identifier Gross Examination steps Identification check Gross examination of specimen Sectioning of specimen Processing steps (for histologic examination) Tissues processed Identification check Tissues embedded in paraffin Tissues thinly sectioned Slides stained Slides cover-slipped Slides transported to pathologists Interpretation steps Identification check Pathologists examine slides microscopically Pathologists prepare a report Reporting steps Reports sent to clinical providers Examples of Substeps DESCRIPTION Hospital/transport/courier personnel hand of specimens to laboratory personnel. Laboratory personnel check that specimen containers and requisition contain appropriate matching identifiers. Specimens are assigned unique identifiers in laboratory information systems. Laboratory personnel check that issues and accompanying information match. Laboratory personnel visually examine specimens in terms of volume and other characteristics (color, lesions, etc). Descriptions are included in pathology reports. For larger specimens, laboratory personnel may use a variety of cutting instruments to examine further the internal specimen characteristics. Tissues are placed in one of several types of processors that dehydrate the tissues. Laboratory personnel visually match tissue cassettes received with records and evaluate cassette integrity following processing. Laboratory personnel embed tissue in paraffin to create tissue blocks. Laboratory personnel use microtomes to thinly section the paraffin blocks. The thin sections are placed on glass slides. Hematoxylin and eosin is the preferred stain for most histologic tissue sections. A thin layer of glass or plastic is placed on top of the slide. Slides from the same patient (case) are assembled and brought to the pathologist for interpretation. Pathologists match the tissue slides and requisition information. Pathologists place slides under light microscopes and examine the tissues. Diagnostic interpretations are made using histologically observed criteria. Pathologists may choose to order ancillary tests, such as immunohistochemical tests. Reports contain an interpretation based on findings from microscopic and gross examinations. Reports are sent in a variety of ways including mail, facsimile, and the internet. Raab, S.S., Quality in Cancer Diagnosis, CA Cancer J Clin 2010;60:
9 Interpretation steps Misinterpretation Cognitive problems Upstream or system failure Poor quality specimen Individual issues Skills Fatigue Lack of 2 nd opinion Over dx Under dx ERROR SCALE
10 Key Elements of Systemic Quality Control Improvement 1. Effective test ordering 2. Clinical information 3. Procurement of high quality tissue 4. Appropriate tissue handling 5. Quality tissue interpretation 6. Timely follow-up 7. Effective Communication 8. Secondary review

11 Procurement of the highest tissue quality Sampling related Interpretation related False Quality Negative Positive
12 This is the No Blame Box. The slides of 40 false-negative cytology errors were evaluated by a pathologist, assessed in terms of specimen quality and amount of tumor. Each oval represents the assessment of specimen quality and amount of tumor present for each of the 40 cases. The pathologist classified the majority of specimens to be of poor quality. Source: Raab SS, Stone CH, Wojcik EM, et al. Use of a new method in reaching consensus on the cause of cytologic-histologic correlation discrepancy. Am J Clin Pathol. 2006;126:

13 Tissue grossing steps
14 Dermatopathology related technical issues 1. Which are the most common ones? 2. What consequences do they have? 3. How can we avoid them?
15
16 Real life scenarios Problem Possible Causes Actions 1. Tissue is present, but no apparent lesion Incorrect clinical sampling Lesion lost in processing True lost Psuedo lost Suboptimal processing Call physician Correlate with clinical info, photos, diagram. Reprocess 2. Tissue is present, but lesion is inconsistent with clinical information Incorrect clinical sampling Lesion is not sectioned properly Not deep enough Malorientation Correlate with clinical info, photos, diagram. Reorient; step sections. 3. Tissue is present but lesion is suboptimal to evaluate Clinically incorrectly sampled Technically not sufficiently sampled Maloriented Margin is not present Over/under stained Poorly fixed Contaminated Communicate with physician Reprocess and deeper sections
17 Virtual tissue loss resulting incorrect diagnosis
18
19 Incorrect Diagnosis due to inadequate Sampling
20
21
22 Ref. Haupt, et al.
23 The perennial question of deeper sectioning Goal Most accurate diagnosis Lowest costs
24 What can we do to make it better? Retroactive 1.Step sections 2.Reprocessing Proactive 1. Optimal clinical information 2. Utilization of clinical images 3. Diagrams 4. Guided sectioning 5. Prospective step sections Inefficient Tissue consuming Costly Cost effective Turn around time Better diagnostic accuracy
25 Deeper sections; Few facts 1. No standard techniques for deeper sectionings 2. Variable recut rate per institutions 1. Volume 2. Technologist skill 3. Referral pattern 4. Biopsy technique 5. Geographic location 6. Pathologist expertise level 3. Only few studies addressed the issue 1. General concept 2. Lesion specific approach
26
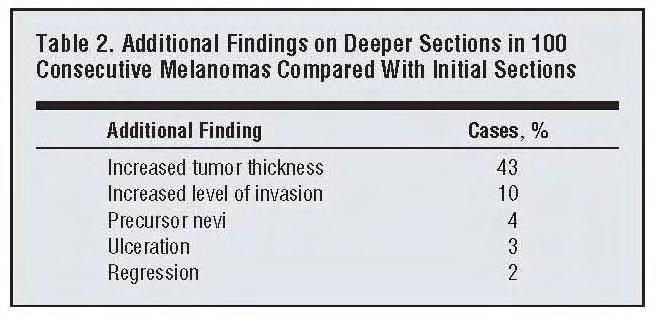
27 Table 1. Utility of additional sections Additional sections No. % 95% Confidence Interval Did not provide additional information (54, 72) Helped make a more accurate diagnosis (16, 32) Help find a benign skin neoplasm not seen on (4, 13) the original sections Help diagnose a malignant skin neoplasm not (1, 8) seen on the original sections Help diagnose a scabies infection by demonstrating a mite not present in original sections (-1, 3) Total Table 2. Reasons for additional sections Reason for additional sections No. % 95% Confidence Interval Initial findings were non-diagnostic (25, 42) Reassurance (25, 41) Superficial biopsy (16, 31) Poor sections (large tips, poor orientation) (3, 12) Attempts to find focal pathology (small (0, 5) lesion, wrong area biopsied, rule out folliculitis) Totals Table 3. Type of case on which levels were ordered Type of case No. % 95% Confidence Interval Neoplasm of the skin (66, 82) Benign (53, 71) Malignant (7, 19) Inflammatory process of the skin (18, 35) Total Table 4. Utility of additional sections in the diagnosis of all cases Additional cuts No. % 95% Confidence Interval Provided additional information (28, 46) Helped make a more accurate diagnosis (16, 32) Helped establish a diagnosis that could (7, 20) not be made on original cuts Total no. of cases that required additional cuts Table 6. Utility of additional sections in the diagnosis of neoplasms of the skin Additional cuts No. % 95% Confidence Interval Helped provide additional information (32, 54) about the diagnosis of a skin neoplasm Helped provide a more accurate (16, 35) diagnosis of a skin neoplasm Helped establish the diagnosis of a skin (9, 26) neoplasm not seen on original cuts Helped establish the diagnosis of a (4, 18) benign skin neoplasm not seen on original cuts Helped establish the diagnosis of a (1, 11) malignant skin neoplasm not seen on original cuts Total no. of neoplasm cases Ref. Maingi, et al.
28
29 Diagnostic yield of step sections of initially diagnosed as actinic keratosis 69 cases with 10 step sections (50 µm intervals) 33% new diagnosis 13% CIS 4% BCC 3% SCC Ref. Carag, et al.
30 Issue of cost effectiveness Example (figures from 2000 from an academic institution) 10 additional sections $ steps $2, Cost effectiveness = new dx yield = total costs/# new dx 1. New dx = $ Cancer dx = $ Intuitive ca dx = $ Ref. Carag, et al.
31 Issue of cost effectiveness Conclusion 1.No generally accepted standards 2.Utilization of additional information to make the decision on the needs of recuts; which correlates with higher yield; 1. Ulceration on first level 2. Clinical diagnosis of skin cancer 3. Pathologic diagnosis of skin cancer 3.Decision remains difficult to make a compromise
32
33
34 Conclusions 1. Step sectioning results in more accurate diagnosis and prognostic parameters 2. Unable to offer standard recommendations 3. Should be a compromise for 1. Extra costs 2. Time 3. Labor 4. Exhaustion of tissue for future use

35 New Approach
36 500 cases Utilization of prospective sectioning 3 slides with a ribbon of 6 sections in 50 µm intervals 12% non diagnostic on level 1 7% changed the diagnosis
37
38
39 Conclusion 1. Step sections were required in about 30% of the cases 2. Improved turnaround time 9% - 45% 3. Cost effectiveness or cost neutral
40 Additional methods to decrease errors and increase diagnostic accuracy 1. Insistence of appropriate clinical information 2. Utilization of clinical photography at grossing the specimen and at the sign-out 3. Systemic use of grossing diagram for correlation 4. Application of ex-vivo dermoscopy at grossing 5. Utilization of dermoscopic image at the grossing and at the sign-out 6. Grossing protocol relevant for biopsy type
41 Key Elements of Systemic Quality Control Improvement 1. Effective test ordering 2. Clinical information 3. Procurement of high quality tissue 4. Appropriate tissue handling 5. Quality tissue interpretation 6. Timely follow-up 7. Effective Communication 8. Secondary review
42 Relevance of Pertinent Clinical Information Clinical information 1. More accurate diagnosis 2. Narrowed differential diagnosis 3. Reduced costs Turn around time Resource utilization
43
44
45
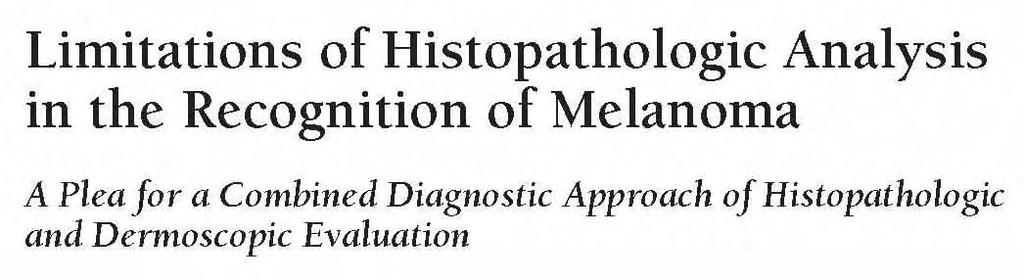
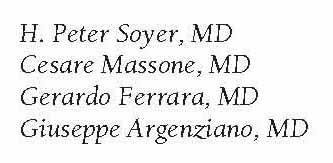
46 Material and Methods I 99 equivocal melanocytic lesions including all melanomas excised from Jan 04 to Dec 05 5 diagnostic scenarios D1 (no information), D2 (age, sex, location), D3 (clinical diagnosis), D4 (clinical image), D5 (dermoscopic image) Dx options: malignant, benign, I am not sure After Dr.Soyer, Queensland Institute of Dermatology
47 Material and Methods II Level of diagnostic confidence (1 5) LDC 1: No diagnostic certainty: no diagnosis can be made. LDC 2: Low diagnostic certainty: a diagnosis is felt as slightly more likely. LDC 3: Moderate diagnostic certainty: a diagnosis is favoured, but with some elements of doubt. LDC 4: High diagnostic certainty: a diagnosis is strongly favoured. LDC 5: Absolute diagnostic certainty: no other diagnosis is possible. After Dr.Soyer, Queensland Institute of Dermatology 47
48 Increase of Level of Diagnostic Confidence After Dr.Soyer, Queensland Institute of Dermatology 48
49 Melan-A-Positive Pseudomelanocytic Nests : A Pitfall in the Histopathologic and Immunohistochemical Diagnosis of Pigmented Lesions on Sun-Damaged Skin. Helmut Beltraminelli, MD Laila El Shabrawi-Caelen, MD Helmut Kerl, MD Lorenzo Cerroni, MD Am J Dermatopathol 2009; 31:305-8
50
51 Key Elements of Systemic Quality Control Improvement 1. Effective test ordering 2. Clinical information 3. Procurement of high quality tissue 4. Appropriate tissue handling 5. Quality tissue interpretation 6. Timely follow-up 7. Effective Communication 8. Secondary review

52 When Dermoscopy is the Pathologist s Friend
53
54

55
56
57 Measurement A
58
59 Measurement B
60
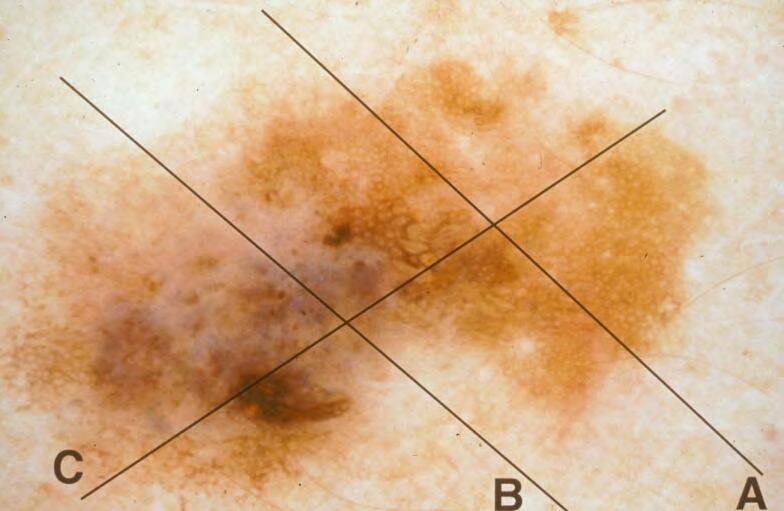
61 Measurement C
62
63 The importance of guided sectioning of melanocytic lesions 1). More control on margin evaluation 2). Better assessment of prognostic parameters 3). Implication on sentinel lymph node dissection and further therapy.
64 Conclusions 1. Errors related to the various phases of the total testing process are abundant in dermatopathology 2. Only a few studies addressed these problems without establishing standards 3. In addition to having impact on patient management it also effects; 1. Costs 2. Laboratory efficiency 3. Reimbursement 4. Legal matters 4. The pathologist overfocused on the analytic phase of the work should pay equal attention to the pre- and post-analytical steps to improve diagnostic accuracy and more efficient laboratory management 5. Dermatopathology is a unique field where cost-effectiveness and higher diagnostic accuracy can be further improved by numerous, relatively simple, and effective methods
Tracking skin cancers and melanoma at the microscopic level
 Tracking skin cancers and melanoma at the microscopic level Rosalie Elenitsas, M.D. Professor of Dermatology Director of Dermatopathology Hospital of the University of Pennsylvania May 12, 2017 Outline
Tracking skin cancers and melanoma at the microscopic level Rosalie Elenitsas, M.D. Professor of Dermatology Director of Dermatopathology Hospital of the University of Pennsylvania May 12, 2017 Outline
Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice
 Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice Dr. Gregory Flynn CEO, Institute for Quality Management in Healthcare Managing Director, Quality Management
Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice Dr. Gregory Flynn CEO, Institute for Quality Management in Healthcare Managing Director, Quality Management
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
What in the world is Histotechnology? Karen Stiffler, MA, HTL Program Director for Histotechnology
 What in the world is Histotechnology? Karen Stiffler, MA, HTL Program Director for Histotechnology The Basics of Histology Histology: the study of body tissues "histo" is from the Greek "histos" meaning
What in the world is Histotechnology? Karen Stiffler, MA, HTL Program Director for Histotechnology The Basics of Histology Histology: the study of body tissues "histo" is from the Greek "histos" meaning
Addendum report coding for the National Quality Improvement Programme in Histopathology: a multi-institutional audit
 Addendum report coding for the National Quality Improvement Programme in Histopathology: a multi-institutional audit S. Mahon 1,3, D. Catargiu 2, S. Phelan 2, S. Crowther 3, N. Swan 1. St. Vincent s University
Addendum report coding for the National Quality Improvement Programme in Histopathology: a multi-institutional audit S. Mahon 1,3, D. Catargiu 2, S. Phelan 2, S. Crowther 3, N. Swan 1. St. Vincent s University
HISTOPATHOLOGY. Introduction
 HISTOPATHOLOGY Introduction Contacts Services offered Pathology tissue request Laboratory hours Special instructions Histopathology reports List of specimens Introduction The Histopathology section of
HISTOPATHOLOGY Introduction Contacts Services offered Pathology tissue request Laboratory hours Special instructions Histopathology reports List of specimens Introduction The Histopathology section of
ANATOMICAL PATHOLOGY TARIFF
 ANATOMICAL PATHOLOGY TARIFF A GUIDE TO UTILISATION. The following guidelines have been agreed by consensus of Anatomical Pathologists who are members of the Anatomical Pathologist s Group, or the National
ANATOMICAL PATHOLOGY TARIFF A GUIDE TO UTILISATION. The following guidelines have been agreed by consensus of Anatomical Pathologists who are members of the Anatomical Pathologist s Group, or the National
Dermatopathology Training Standards
 Dermatopathology Training Standards Tammie Ferringer, MD Section Head and Fellowship Director Dermatopathology Depts of Dermatology and Pathology tferringer@geisinger.edu I do not have any relevant relationships
Dermatopathology Training Standards Tammie Ferringer, MD Section Head and Fellowship Director Dermatopathology Depts of Dermatology and Pathology tferringer@geisinger.edu I do not have any relevant relationships
GOALS AND OBJECTIVES BREAST PATHOLOGY
 GOALS AND OBJECTIVES BREAST PATHOLOGY LEVEL: PGY2, PGY3, PGY5 A number of these rotations are introductory in nature, as they are major subspecialties, and are followed by two more blocks in PGY-3, during
GOALS AND OBJECTIVES BREAST PATHOLOGY LEVEL: PGY2, PGY3, PGY5 A number of these rotations are introductory in nature, as they are major subspecialties, and are followed by two more blocks in PGY-3, during
Quality assurance and quality control in pathology in breast disease centers
 Quality assurance and quality control in pathology in breast disease centers Judith Sandbank M.D. Pathology Assaf-Harofeh Medical Center ISRAEL jsandbank@asaf.health.gov.il 1 st IBDC, 28 th January, 2011
Quality assurance and quality control in pathology in breast disease centers Judith Sandbank M.D. Pathology Assaf-Harofeh Medical Center ISRAEL jsandbank@asaf.health.gov.il 1 st IBDC, 28 th January, 2011
Diagnostics Assessment Programme
 Diagnostics Assessment Programme Diagnostics Consultation Document: VivaScope 1500 and 3000 imaging systems for detecting and monitoring skin cancer lesions Evaluation Report NATIONAL INSTITUTE FOR HEALTH
Diagnostics Assessment Programme Diagnostics Consultation Document: VivaScope 1500 and 3000 imaging systems for detecting and monitoring skin cancer lesions Evaluation Report NATIONAL INSTITUTE FOR HEALTH
117 Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice. Gregory Flynn MD
 117 Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice Gregory Flynn MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe,
117 Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice Gregory Flynn MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe,
CAP Companion Meeting at USCAP Quality and Patient Safety in Anatomic Pathology: Practical Solutions. Surgical Pathology
 CAP Companion Meeting at USCAP 2010 Quality and Patient Safety in Anatomic Pathology: Practical Solutions Directed Peer Review in Surgical Pathology Stephen S. Raab, MD University of Colorado Denver 2010
CAP Companion Meeting at USCAP 2010 Quality and Patient Safety in Anatomic Pathology: Practical Solutions Directed Peer Review in Surgical Pathology Stephen S. Raab, MD University of Colorado Denver 2010
Melanoma. Consultation on draft guideline - stakeholder comments. Comments to be submitted before 5pm on Friday 13 March 2015
 Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
NPQR Quality Payment Program (QPP) Measures 21_18247_LS.
 Measures 21_18247_LS.") NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
NPQR Quality Payment Program (QPP) Measures 21_18247_LS MEASURE ID: QPP 99 MEASURE TITLE: Breast Cancer Resection Pathology Reporting pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes)
4. Monitoring of PAP test with Cervical Biopsy Correlations
 Page 1 of 6 1. For cases of an HSIL Pap test with a discordant biopsy report where only the biopsy report is available, what action do you take? (check all that apply) Paper correlation without review
Page 1 of 6 1. For cases of an HSIL Pap test with a discordant biopsy report where only the biopsy report is available, what action do you take? (check all that apply) Paper correlation without review
Regression 2/3/18. Histologically regression is characterized: melanosis fibrosis combination of both. Distribution: partial or focal!
 Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Diagnostic Detectives: Medical Laboratory Professionals A Closer Look at Careers in Histology
 Diagnostic Detectives: Medical Laboratory Professionals A Closer Look at Careers in Histology When your doctor orders lab tests do you know.. Who prepares, embeds, cuts, and stains tissue samples and biopsies
Diagnostic Detectives: Medical Laboratory Professionals A Closer Look at Careers in Histology When your doctor orders lab tests do you know.. Who prepares, embeds, cuts, and stains tissue samples and biopsies
SURGICAL PATHOLOGY - HISTOLOGY
 SURGICAL PATHOLOGY - HISTOLOGY Request Forms The following information is required on the Anatomic Pathology Request form in General Information in all instances: Patient s full name Room number Medical
SURGICAL PATHOLOGY - HISTOLOGY Request Forms The following information is required on the Anatomic Pathology Request form in General Information in all instances: Patient s full name Room number Medical
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
For additional information on meeting the criteria for Mohs, see Appendix 2.
 Position Statement on Appropriate Uses of Paraffin Sections in Association (Approved by the Board of Directors: August 1, 2011; Revised November 5, 2011; Revised August 9, 2014) According to AMA/CPT, Mohs
Position Statement on Appropriate Uses of Paraffin Sections in Association (Approved by the Board of Directors: August 1, 2011; Revised November 5, 2011; Revised August 9, 2014) According to AMA/CPT, Mohs
Skin biopsy. Sophia Otto SA Pathology
 Skin biopsy Sophia Otto SA Pathology RCPA (Royal College of Pathologists of Australasia) The RCPA is the leading organisation representing pathologists in Australasia. Its mission is to train and support
Skin biopsy Sophia Otto SA Pathology RCPA (Royal College of Pathologists of Australasia) The RCPA is the leading organisation representing pathologists in Australasia. Its mission is to train and support
Dermatology pilots. Ram Patel GPwSI Dermatology Gateway lead for Dermatology.
 Dermatology pilots Ram Patel GPwSI Dermatology Gateway lead for Dermatology Assessing needs Extent of skin disease: Study of 1500 people age 15 years and over 54% reported a skin condition 14% seek advice
Dermatology pilots Ram Patel GPwSI Dermatology Gateway lead for Dermatology Assessing needs Extent of skin disease: Study of 1500 people age 15 years and over 54% reported a skin condition 14% seek advice
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Malignant non-melanocytic lesions
 Malignant non-melanocytic lesions Course C023: Fundamentals of Dermoscopy March 4, 2019, 11:20 AM - 11:50 PM Room: 146B Jason B. Lee, MD Professor & Vice Chair Director of Dermatopathology & Pigmented
Malignant non-melanocytic lesions Course C023: Fundamentals of Dermoscopy March 4, 2019, 11:20 AM - 11:50 PM Room: 146B Jason B. Lee, MD Professor & Vice Chair Director of Dermatopathology & Pigmented
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
What is melanoma? Melanoma dealing with the diagnosis. What is melanoma?
 Melanoma is a form of cancer which develops from that part of the skin which produces its colour. It grows from the cell which produces the brown pigment in our skin: the melanocyte. Often the melanoma
Melanoma is a form of cancer which develops from that part of the skin which produces its colour. It grows from the cell which produces the brown pigment in our skin: the melanocyte. Often the melanoma
Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19
 VivaScope 1500 and 3000 imaging systems for detecting skin cancer lesions Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19 NICE 2018. All rights reserved. Subject to Notice of
VivaScope 1500 and 3000 imaging systems for detecting skin cancer lesions Diagnostics guidance Published: 11 November 2015 nice.org.uk/guidance/dg19 NICE 2018. All rights reserved. Subject to Notice of
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT
 BREAST CANCER - PATHOLOGY ASSESSMENT") PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT Author: Dr Sally Ann Hales On behalf of the Breast and pathology CNGs Written: March 2005 Reviewed by CNG: June 2009 &
PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT Author: Dr Sally Ann Hales On behalf of the Breast and pathology CNGs Written: March 2005 Reviewed by CNG: June 2009 &
Pathology Student Interest Group. Sponsored by the College of American Pathologists
 Pathology Student Interest Group Sponsored by the College of American Pathologists Pathology Right Now, A Pathologist Somewhere Is. Evaluating Surgical Specimens Diagnosis and Staging of Cancer Adequacy
Pathology Student Interest Group Sponsored by the College of American Pathologists Pathology Right Now, A Pathologist Somewhere Is. Evaluating Surgical Specimens Diagnosis and Staging of Cancer Adequacy
Contributions to Anatomic Pathology, over the years
 Contributions to Anatomic Pathology, over the years Anatomic Pathology, part 1 G.B. Morgagni Xavier Bichat Rudolf Wirchow Anatomic Pathology, part 1 Anatomic pathology materials: morphological samples
Contributions to Anatomic Pathology, over the years Anatomic Pathology, part 1 G.B. Morgagni Xavier Bichat Rudolf Wirchow Anatomic Pathology, part 1 Anatomic pathology materials: morphological samples
ALL THINGS DERMATOLOGY
 ALL THINGS DERMATOLOGY Dr Aravind Chandran Dermatologist Auckland District Health Board and Skin Specialist Centre Honorary Lecturer University of Auckland ALL THINGS DERMATOLOGY PITFALLS & PRACTICAL TIPS
ALL THINGS DERMATOLOGY Dr Aravind Chandran Dermatologist Auckland District Health Board and Skin Specialist Centre Honorary Lecturer University of Auckland ALL THINGS DERMATOLOGY PITFALLS & PRACTICAL TIPS
Lessons learned in the use of digital imaging at Memorial Sloan Kettering Cancer Center
 Lessons learned in the use of digital imaging at Memorial Sloan Kettering Cancer Center Executive War College May 3, 2018 Victor E. Reuter, M.D. Vice-Chair, Department of Pathology Medical Director, Warren
Lessons learned in the use of digital imaging at Memorial Sloan Kettering Cancer Center Executive War College May 3, 2018 Victor E. Reuter, M.D. Vice-Chair, Department of Pathology Medical Director, Warren
Virtual Microscopy: Express Surgical Pathology Consultation. Mercè Jordà, University of Miami, Florida
 Virtual Microscopy: Express Surgical Pathology Consultation Mercè Jordà, University of Miami, Florida Telepathology versus Virtual microscopy (Digital Pathology) Telepathology Use of telecommunications
Virtual Microscopy: Express Surgical Pathology Consultation Mercè Jordà, University of Miami, Florida Telepathology versus Virtual microscopy (Digital Pathology) Telepathology Use of telecommunications
Histopathology National Quality Improvement Programme Data Report 2015 Edition 3 created July 2016
 Histopathology National Quality Improvement Programme Data Report 2015 Edition 3 created July 2016 Authors Histopathology National Quality Improvement Programme Working Group, RCPI Programme Team Contributors
Histopathology National Quality Improvement Programme Data Report 2015 Edition 3 created July 2016 Authors Histopathology National Quality Improvement Programme Working Group, RCPI Programme Team Contributors
PATHOPHYSIOLOGY. DEFINED Involves the study of function that results from disease processes.
 DEFINED Involves the study of function that results from disease processes. What is pathology? Pathology is the branch of medical sciences that treats the essential nature of disease, especially the changes
DEFINED Involves the study of function that results from disease processes. What is pathology? Pathology is the branch of medical sciences that treats the essential nature of disease, especially the changes
Policy #: 127 Latest Review Date: June 2011
 Name of Policy: Mohs Micrographic Surgery Policy #: 127 Latest Review Date: June 2011 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates. Background/Definitions:
Name of Policy: Mohs Micrographic Surgery Policy #: 127 Latest Review Date: June 2011 Category: Surgery Policy Grade: Active Policy but no longer scheduled for regular literature reviews and updates. Background/Definitions:
Page 1 of 3. We suggest the following changes:
 Page 1 of 3 Loren E. Clarke, M.D. Myriad Genetic Laboratories, Inc. 320 Wakara Way, Salt Lake City, UT 84108 Phone: 801.883.3470 Email: lclarke@myriad.com Date of Request: June 2017 NCCN Guidelines Panel:
Page 1 of 3 Loren E. Clarke, M.D. Myriad Genetic Laboratories, Inc. 320 Wakara Way, Salt Lake City, UT 84108 Phone: 801.883.3470 Email: lclarke@myriad.com Date of Request: June 2017 NCCN Guidelines Panel:
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Cleveland Clinic Laboratories. Anatomic Pathology
 Cleveland Clinic Laboratories Anatomic Pathology OUR MISSION Cleveland Clinic Laboratories contributes to excellent patient care by providing high-quality, comprehensive laboratory testing and patient-focused
Cleveland Clinic Laboratories Anatomic Pathology OUR MISSION Cleveland Clinic Laboratories contributes to excellent patient care by providing high-quality, comprehensive laboratory testing and patient-focused
Mapping Basal Cell and Squamous Carcinoma By 10 Min CK5 Direct Immunohistochemistry on Frozen Section Skin Tissues during Mohs Micrographic Surgery
 Mapping Basal Cell and Squamous Carcinoma By 10 Min CK5 Direct Immunohistochemistry on Frozen Section Skin Tissues during Mohs Micrographic Surgery Robert Glinert, MD and Song Q. Zhao, MD, Ph.D., MPH Department
Mapping Basal Cell and Squamous Carcinoma By 10 Min CK5 Direct Immunohistochemistry on Frozen Section Skin Tissues during Mohs Micrographic Surgery Robert Glinert, MD and Song Q. Zhao, MD, Ph.D., MPH Department
Tips on getting the most from your alopecia pathology reports. D irector, H a ir C linic, Boston Medical C e n ter
 Tips on getting the most from your alopecia pathology reports Lynne J. Goldberg, MD J a g Bhawan Professor o f Dermatology a n d Pathology & Laboratory Medicine Boston U n iversity School of Medicine D
Tips on getting the most from your alopecia pathology reports Lynne J. Goldberg, MD J a g Bhawan Professor o f Dermatology a n d Pathology & Laboratory Medicine Boston U n iversity School of Medicine D
How to decipher a pathology report for alopecia
 How to decipher a pathology report for alopecia DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Lynne J. Goldberg, MD S063-Hair Disorders Made Easier DISCLOSURES I do not have any relationships with industry
How to decipher a pathology report for alopecia DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Lynne J. Goldberg, MD S063-Hair Disorders Made Easier DISCLOSURES I do not have any relationships with industry
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Associate Clinical Professor of Dermatology MUSC
 Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Handout for Dr Allison s Lectures on Grossing Breast Specimens:
 Handout for Dr Allison s Lectures on Grossing Breast Specimens: Dr. Kimberly H. Allison Director of Breast Pathology and Breast Pathology Fellowship Director of Residency Training in Pathology Stanford
Handout for Dr Allison s Lectures on Grossing Breast Specimens: Dr. Kimberly H. Allison Director of Breast Pathology and Breast Pathology Fellowship Director of Residency Training in Pathology Stanford
Multispectral Digital Skin Lesion Analysis. Summary
 Subject: Multispectral Digital Skin Lesion Analysis Page: 1 of 8 Last Review Status/Date: March 2016 Multispectral Digital Skin Lesion Analysis Summary There is interest in noninvasive devices that will
Subject: Multispectral Digital Skin Lesion Analysis Page: 1 of 8 Last Review Status/Date: March 2016 Multispectral Digital Skin Lesion Analysis Summary There is interest in noninvasive devices that will
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
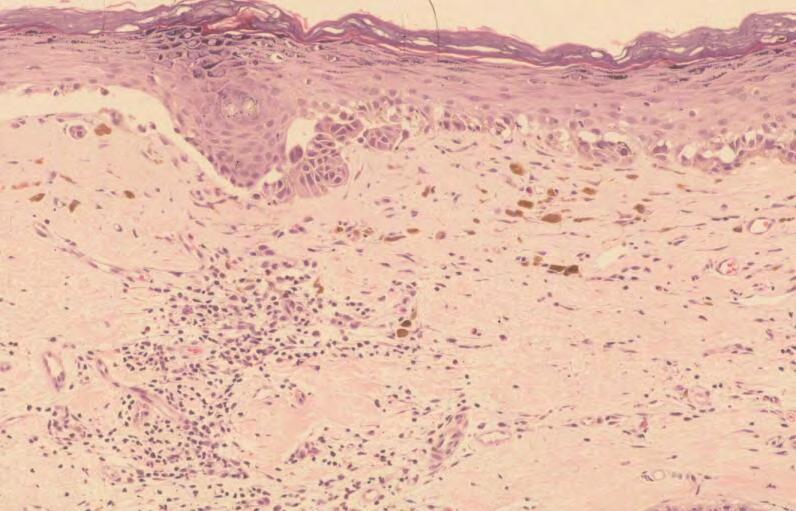
Melanocytes in nonlesional sun-exposed skin: A multicenter comparative study
 Melanocytes in nonlesional sun-exposed skin: A multicenter comparative study AliHendi,MD, a,b David A. Wada, MD, d M. Amanda Jacobs, MD, e JuliaE.Crook,PhD, c Kimberly R. Kortuem, MD, d Brent R. Weed,
Melanocytes in nonlesional sun-exposed skin: A multicenter comparative study AliHendi,MD, a,b David A. Wada, MD, d M. Amanda Jacobs, MD, e JuliaE.Crook,PhD, c Kimberly R. Kortuem, MD, d Brent R. Weed,
Diagnosis of Lentigo Maligna Melanoma. Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ
 Diagnosis of Lentigo Maligna Melanoma Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ Conflict of Interest: None Topics Epidemiology and Natural History Clinical and Histologic
Diagnosis of Lentigo Maligna Melanoma Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ Conflict of Interest: None Topics Epidemiology and Natural History Clinical and Histologic
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Clinicopathologic Self- Assessment S003 AAD 2017
 Clinicopathologic Self- Assessment S003 AAD 2017 Clay J. Cockerell, M.D. Director, Cockerell Dermatopathology Director, Division of Dermatopathology UT Southwestern Medical Center July 2017 No relevant
Clinicopathologic Self- Assessment S003 AAD 2017 Clay J. Cockerell, M.D. Director, Cockerell Dermatopathology Director, Division of Dermatopathology UT Southwestern Medical Center July 2017 No relevant
The role of Electron Microscopy in the study of cytologic specimens. Elba A. Turbat-Herrera, MD
 The role of Electron Microscopy in the study of cytologic specimens. Elba A. Turbat-Herrera, MD Louisiana State University Health Sciences Center Shreveport, LA, USA Introduction The field of Cytology
The role of Electron Microscopy in the study of cytologic specimens. Elba A. Turbat-Herrera, MD Louisiana State University Health Sciences Center Shreveport, LA, USA Introduction The field of Cytology
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Mole mapping and monitoring. Dr Stephen Hayes. Associate Specialist in Dermatology, University Hospital Southampton
 Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
VDx: Unlocking Complex Diagnostics
 VDx: Unlocking Complex Diagnostics VDx now offers PARR testing in-house on formalin-fixed tissue Complicated Case? Is this cat s chronic lymphocytic enteritis really chronic IBD or is this early small
VDx: Unlocking Complex Diagnostics VDx now offers PARR testing in-house on formalin-fixed tissue Complicated Case? Is this cat s chronic lymphocytic enteritis really chronic IBD or is this early small
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Among the benign intraepithelial melanocytic proliferations, Inflamed Conjunctival Nevi. Histopathological Criteria. Resident Short Reviews
 Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Resident Short Reviews Inflamed conjunctival nevi (ICN) may suggest malignancy because of their rapid growth and atypical histology. The objective of this study was to characterize the diagnostic features
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons
 Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons Ben J. Friedman, MD Senior Staff Physician Department of Dermatology Department of Pathology and Laboratory Medicine Henry
Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons Ben J. Friedman, MD Senior Staff Physician Department of Dermatology Department of Pathology and Laboratory Medicine Henry
Cytological evaluation of effusion fluid with cell block technique and cytology smears among Sudanese patients
 EUROPEAN ACADEMIC RESEARCH Vol. IV, Issue 3/ June 2016 ISSN 2286-4822 www.euacademic.org Impact Factor: 3.4546 (UIF) DRJI Value: 5.9 (B+) Cytological evaluation of effusion fluid with cell block technique
EUROPEAN ACADEMIC RESEARCH Vol. IV, Issue 3/ June 2016 ISSN 2286-4822 www.euacademic.org Impact Factor: 3.4546 (UIF) DRJI Value: 5.9 (B+) Cytological evaluation of effusion fluid with cell block technique
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision
 Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Differentiation of Tumors with Specific Red Cell Adherence (SRCA) test
 test") 753 Differentiation of Tumors with Specific Red Cell Adherence (SRCA) test Dr. Abhishek A Mangaonkar *, Dr. A G Valand 1 Intern, Grant Medical College and Sir J.J. Group of Hospitals, Mumbai, India 2 Professor,
753 Differentiation of Tumors with Specific Red Cell Adherence (SRCA) test Dr. Abhishek A Mangaonkar *, Dr. A G Valand 1 Intern, Grant Medical College and Sir J.J. Group of Hospitals, Mumbai, India 2 Professor,
Mohs. Micrographic Surgery. For Treating Skin Cancer
 Mohs Micrographic Surgery For Treating Skin Cancer Skin Cancer Basics Skin cancer is common. Over the past three decades, more people have had skin cancer than all other cancers combined. Each year in
Mohs Micrographic Surgery For Treating Skin Cancer Skin Cancer Basics Skin cancer is common. Over the past three decades, more people have had skin cancer than all other cancers combined. Each year in
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
") What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology,
UW Medicine Neuropathology
 Neuropathology in Patient Care Surgical Neuropathology is that subspecialty of pathology that provides diagnoses on biopsies from the brain, spinal cord, skeletal muscle, peripheral nerve, and eye. In
Neuropathology in Patient Care Surgical Neuropathology is that subspecialty of pathology that provides diagnoses on biopsies from the brain, spinal cord, skeletal muscle, peripheral nerve, and eye. In
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Abstract. Introduction. Salah Abobaker Ali
 Sensitivity and specificity of combined fine needle aspiration cytology and cell block biopsy versus needle core biopsy in the diagnosis of sonographically detected abdominal masses Salah Abobaker Ali
Sensitivity and specificity of combined fine needle aspiration cytology and cell block biopsy versus needle core biopsy in the diagnosis of sonographically detected abdominal masses Salah Abobaker Ali
FNA thyroid. Thyroid FNA accuracy. Thyroid FNA And Cytopathology. Variability in FNA sampling via palpation
 Thyroid FNA And Cytopathology University of California, San Francisco FNA thyroid Wide range of accuracy- causes Overview of tools and sampling Preparation techniques Impact of US guidance Impact of training
Thyroid FNA And Cytopathology University of California, San Francisco FNA thyroid Wide range of accuracy- causes Overview of tools and sampling Preparation techniques Impact of US guidance Impact of training
Skin Cancer A Personal Approach. Dr Matthew Strack Dunedin New Zealand
 Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
EXAM OF THE FUTURE CORE EXAM STUDY GUIDE
 The CORE modules build upon the knowledge and abilities tested in the BASIC exam. Some material in the BASIC content outline may also be covered in the CORE modules. Presented herein are examples of the
The CORE modules build upon the knowledge and abilities tested in the BASIC exam. Some material in the BASIC content outline may also be covered in the CORE modules. Presented herein are examples of the
Anatomic Pathology / MICROWAVE PROCESSING OF SURGICAL SPECIMENS
 Anatomic Pathology / MICROWAVE PROCESSING OF SURGICAL SPECIMENS A Comparison of Routine and Rapid Microwave Tissue Processing in a Surgical Pathology Laboratory Quality of Histologic Sections and Advantages
Anatomic Pathology / MICROWAVE PROCESSING OF SURGICAL SPECIMENS A Comparison of Routine and Rapid Microwave Tissue Processing in a Surgical Pathology Laboratory Quality of Histologic Sections and Advantages
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation. Dermatopathology Specialists Needed. Changing Trends
 Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Phoebe Rich MD Adjunct Professor OHSU Portland, Oregon
 Nail Tips for Diagnosis and Management of Nail Disorders Winter Clinical Dermatology Conference 2017 Hawaii Phoebe Rich MD Adjunct Professor OHSU Portland, Oregon Objectives diagnostic clues for benign
Nail Tips for Diagnosis and Management of Nail Disorders Winter Clinical Dermatology Conference 2017 Hawaii Phoebe Rich MD Adjunct Professor OHSU Portland, Oregon Objectives diagnostic clues for benign
Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor
 Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Case Reports in Medicine Volume 2015, Article ID 742920, 4 pages http://dx.doi.org/10.1155/2015/742920 Case Report A Rare Cutaneous Adnexal Tumor: Malignant Proliferating Trichilemmal Tumor Omer Alici,
Skin lesions suspicious for melanoma: New Zealand excision margin guidelines in practice
 Skin lesions suspicious for melanoma: excision margin guidelines in practice Tess Brian MBBS; 1 Michael B. Jameson MBChB, FRACP, FRCP, PhD 2,3 1 Department of Plastic and Reconstructive Surgery, Waikato
Skin lesions suspicious for melanoma: excision margin guidelines in practice Tess Brian MBBS; 1 Michael B. Jameson MBChB, FRACP, FRCP, PhD 2,3 1 Department of Plastic and Reconstructive Surgery, Waikato
Providence Medford Medical Center Pathology Department
 Providence Medford Medical Center Pathology Department Anatomic pathology services including histology, cytology and autopsies are offered through Providence Medford Medical Center Pathology Department.
Providence Medford Medical Center Pathology Department Anatomic pathology services including histology, cytology and autopsies are offered through Providence Medford Medical Center Pathology Department.
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is:
 Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
ORAL MELANOMA Definition Epidemiology Clinical Presentation
 ORAL MELANOMA Definition Melanoma is a highly malignant neoplasia, arising from melanocytes, the cells that produce the brownish pigment melanin. Melanin is the determinant in skin colour and protects
ORAL MELANOMA Definition Melanoma is a highly malignant neoplasia, arising from melanocytes, the cells that produce the brownish pigment melanin. Melanin is the determinant in skin colour and protects
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
The role of the cytologist in breast cancer screening
 The role of the cytologist in breast cancer screening I.Seili-Bekafigo, MD, PhD Clinical cytologist KBC Rijeka Croatian Society for Clinical Cytology Fine needle aspiration (FNA, FNAB, FNAC) Fine needle
The role of the cytologist in breast cancer screening I.Seili-Bekafigo, MD, PhD Clinical cytologist KBC Rijeka Croatian Society for Clinical Cytology Fine needle aspiration (FNA, FNAB, FNAC) Fine needle
Carol Davila University of Medicine and Pharmacy, Bucharest, Romania b
 Mædica - a Journal of Clinical Medicine MAEDICA a Journal of Clinical Medicine 2015; 10(3): 226-230 ORIGINAL PAPERS Improving Melanoma Path Reports: the Importance of Histopathological Parameters in Diagnosis
Mædica - a Journal of Clinical Medicine MAEDICA a Journal of Clinical Medicine 2015; 10(3): 226-230 ORIGINAL PAPERS Improving Melanoma Path Reports: the Importance of Histopathological Parameters in Diagnosis
Apps and Telemedicine H. Peter Soyer Dermatology Research Centre
 Apps and Telemedicine H. Peter Soyer Dermatology Research Centre p.soyer@uq.edu.au https://twitter.com/hpsoyer William Gibson The future is already here it's just not very evenly distributed Vision 3D
Apps and Telemedicine H. Peter Soyer Dermatology Research Centre p.soyer@uq.edu.au https://twitter.com/hpsoyer William Gibson The future is already here it's just not very evenly distributed Vision 3D
Management of Atypical Pigmented Lesions
 Management of Atypical Pigmented Lesions Jennifer A. Stein MD, PhD Associate Director, Pigmented Lesion Section Ronald O. Perelman Department of Dermatology NYU Langone Medical Center July 29, 2017 1-4
Management of Atypical Pigmented Lesions Jennifer A. Stein MD, PhD Associate Director, Pigmented Lesion Section Ronald O. Perelman Department of Dermatology NYU Langone Medical Center July 29, 2017 1-4