Advances in Imaging Technology In The Management of Colorectal Cancer
|
|
|
- Liliana Ward
- 5 years ago
- Views:
Transcription

1 Advances in Imaging Technology In The Management of Colorectal Cancer Dushyant Sahani, M.D Director of CT Associate Professor Department of Radiology Massachusetts General Hospital Harvard Medical School


2 CRC Detection >150,000 patients diagnosed each year with CRC > 55, 000 deaths in from CRC
3 Colorectal Cancer Screening Multiple studies demonstrated that 80% CRC originate from a precursor lesion Risk of Cancer very low in polyps < 1 cm Adenomatous polyp Early detection and removal of these lesions can be preventative of colon cancer Muto T et.al. Cancer 1975 Winawer SJ. Am J Med 1999 Aldridge AJ et. al. Eur J Surg 2001
4 CRC: Pattern of Spread Mucosa Sub mucosa Serosa Modified Duke TNM 5 year survival A % 1 B % C % D 4 0-5%


5 Management of Colon and Rectal Cancer: Different Landscapes Higher local failure in locally advanced rectal ca (T3/T4 and/or N disease) 1. Lack of serosal layer 2. Complex anatomy (levator, pelvic sidewall)

 Node involvement")
6 Prognostic Indicators in Rectal Cancer Tumor Level of tumor invasion Depth of extramural spread Mesorectal fascia involvement (CRM) Node involvement Distant Metastasis
7 Role of Imaging in CRC Staging (TNM)- Influences management Tumor stage- Rectal wall invasion and local spread Rectum T1/T2: Local resection T3 and beyond: ChemoXRT Nodes: Regional vs Distant Metastases- Hepatic vs. Extrahepatic

8 MDCT: CRC Survey Exam


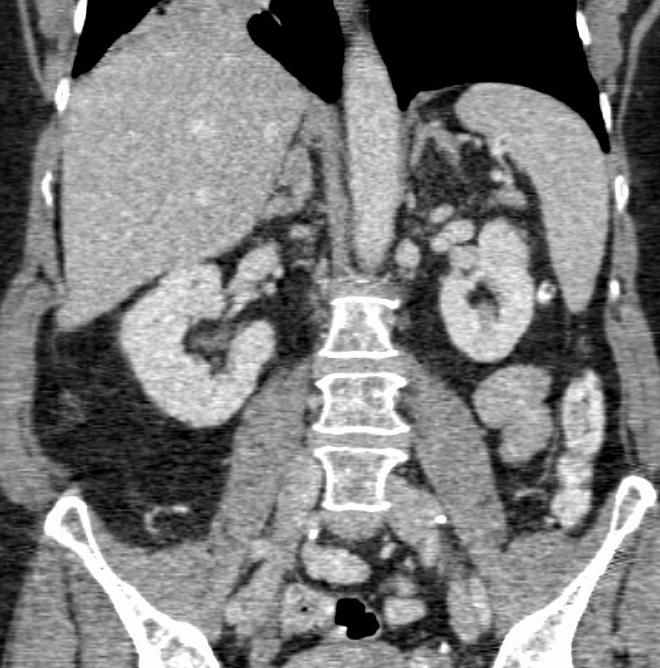
9 MDCT: CRC Survey Exam




10 Sahani et al. AJR 2002 MDCT for Liver Resection Planning IVC MHV





11 MDCT: Mapping Hepatic Vascular Anatomy Sahani et al. AJR 2002; Kapoor et al AJR 2005; Sahani et al. JCAT 2005




12 MDCT: CRC Staging CT Accuracy Overall: 48-74% Liver: 78% Extrahepatic: 71% Lymph nodes: 23-73%


13 CT: Limitations T2 or T3-T4?Nodal disease?metastases


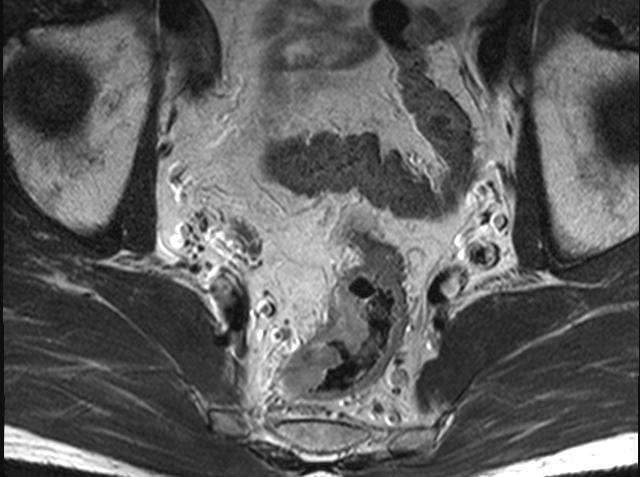
14 Rectal Cancer: Local staging


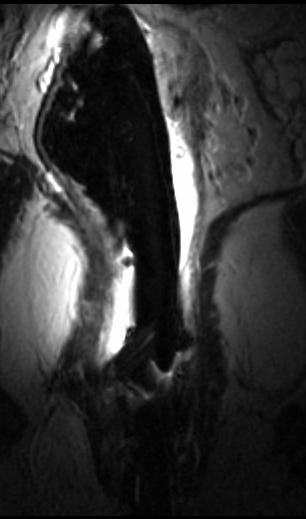
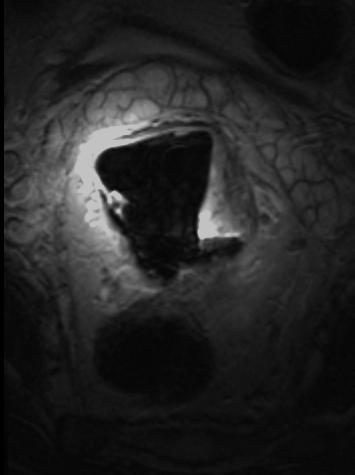
15 T-stage: Endorectal Coil MR Superior SNR and resolution Permits visualization of layers of rectum Enables differentiation of T1-T2 from T3-T4 disease Visulaization of mesorectal fascia and anal sphincter T2 T3
16 T-stage Accuracy of MRI (64-90%) Study EUS MRI Zagoria et al % 80% Kim % 81% Hunerbein % 91% Fuschsjager % 64%
17 Optimal Endorectal Coil Positioning

18 High Rectal Lesions


19 T-stage: MR vs. EUS T-staging accuracy* MR 84.6 % EUS 76.9 % MR less operator dependent Preferred by surgeons Tumor penetration of the rectal wall** Sensitivity Specificity MR 86 % 65 % EUS 89 % 33 % *Gualdi GF et al. Dis Col Rect 2000; ***Bloomquist L et al Eur Radiol 2000
* Nodal disease is better predicted ** Patient compliance *Brown G et al, Radiology 1999; **Brown G et al, Radiology 2003.")
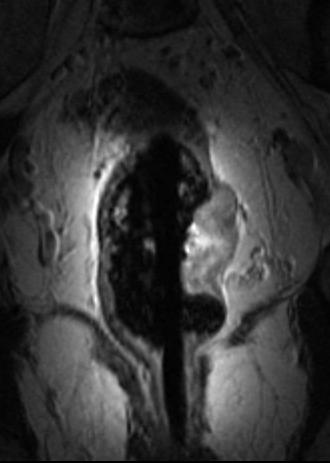
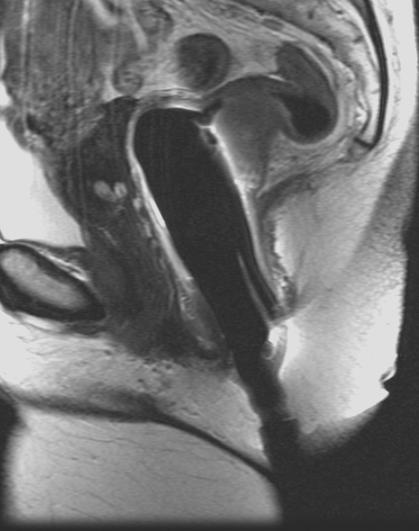
20 T-stage: Phased Array Surface Coil MR High-resolution technique comparable to Endo-MR for T-stage (T3-T4) Superior display of tumor & mesorectal fascia (MRF)* Nodal disease is better predicted ** Patient compliance *Brown G et al, Radiology 1999; **Brown G et al, Radiology *Brown G et al, Br J Surg 2003.
21 MR Technique Combined pelvic phased array and endorectal coils No bowel prep First endo-rect coil inserted Lidocaine gel Pelvic phased array coil is then placed
22 MRI Technique Multiplanar T2-FSE with no FS TR/TE: /102ms ETL: 16 FOV: MATRIX: 256X 256 Axial T1 SE TR/TE: 600/11 FOV: 14 Matrix 256 x 256 Axial/cor/sag post Gd- T1-SPGR FS 2d/3D TR/TE: 240/4.2 FA: 75
23 T-stage Accuracy: Endo-MR Vs Phased MR (70-85% Vs %) Study Endo-MRI Phased-MRI 2005 Oberholzer K. JMRI. Bianchi PP. J Gastrointest Surg Akin O. Clin Imaging. Bipat S. Radiology. 70% 71-89% 85% 75%


24 Endo-MR T2 vs. T3 Disease? T3 T3



25 T-stage: Phased Array Surface Coil MR N=99 TME with detailed histo-path evaluation MRI 94 % agreement for T-stage with pathology Extra-mural venous invasion 15/18 *Brown G et al, Br J Surg 2003.
 Positive")


26 Circumferential Resection Margin (CRM) Positive tumor/node < 1mm of MRF Predicts local recurrence MRI predicted CRM with 92% agreement with histopathology* *Brown G et al, Br J Surg 2003.
27 T-stage Accuracy of MRI (52-97%) Study EUS MRI 2007 MERCURY Study. Radiology Hancock L. Colorectal Dis Chu. Am J Roentgenol. Tatli S. JMRI Kim JC. Am J Surg 52-92% 88-97% 78-97%


28 Rectal CA-3T MR Improved SNR


29 N-stage: MR Node +ve: adverse prognosis Nodes near MRF can threatens CRM Node size unreliable for characterization 3-6 mm indeterminate > 6 mm suspicious > 8 mm malignant Signal or contour abnormality are better predictors 85 % agreement with pathology *Brown G et al, Br J Surg 2003.
30 N-stage Accuracy of MRI and EUS (60-75%) Study EUS MRI 2007 Hancock L. Colorectal Dis Siddiqui AA. Int Semin Surg Oncol. Tatli S. JMRI Kim JC. Am J Surg 2005 Oberholzer K. JMRI. Bianchi PP. J Gastrointest Surg. Koh DM. Eur Radiol. 60% 60-74% 65-75% 64-76% 62%

31 N Stage -DWI for Lymph node characterization


32 N-Stage: Pre USPIO Post USPIO Courtesy: A.Padhani UK


33 Courtesy: A.Padhani UK N-Stage: Pre USPIO Post USPIO Malignant
34 M-Stage : Liver Metastases 60% pts of CRC develop liver metastasis Untreated: Median survival 6-12 mts, no survivors at 5 yrs Surgery: 66% 2 yr and 33% 5 year survival Homsi J, Garrett CR. Cancer Control 2006;13:42-47 Cohen AD, Keneny NE. Oncologist 2003;6:553-66
35 Liver Surgery: Considerations Poor prognostic factors Tumor > 7 cm Multiple lesions Tumors involving > 2 segments Requiring major hepatectomy Homsi J, Garrett CR. Cancer Control 2006;13:42-47 Cohen AD, Keneny NE. Oncologist 2003;6: Marrero JA. Current opinion in Gastroenterology 2006;22:

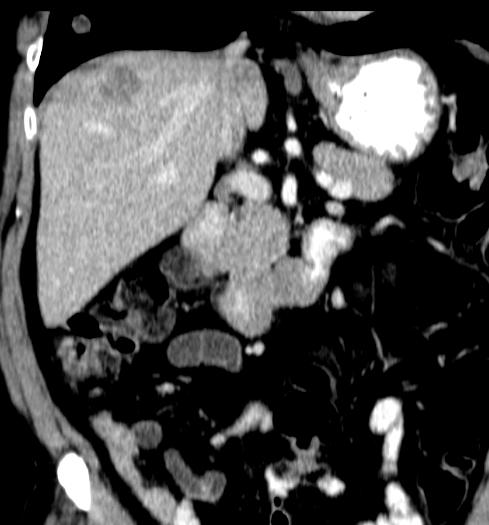
36 CRC Metastases: Right Hepatectomy

37 CRC Metastasis 4 mts chemo Hepatic Resection Possible

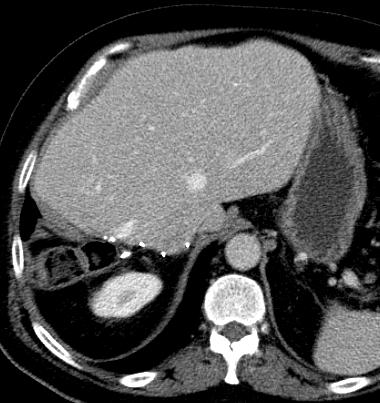
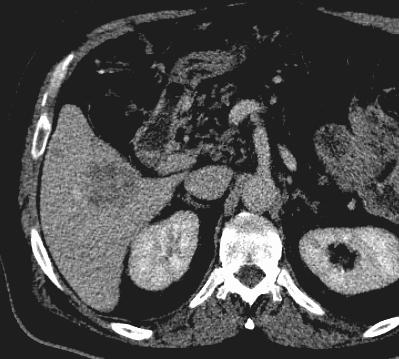
38 Lesion Is Too Small To Characterize CECT Vs. MRI Lesions > 1.5 cm can be routinely characterized on a dual MDCT


39 Small Lesion Detection: CT Vs. MR CT MR CT can confidently detect > 80% of lesions > 1.5 cm. In fatty liver, hypovascular lesions are less conspicuous on CT


40 M-Stage: CT and MR CECT MR
41 M-Stage: MR Studies Assessment Accuracy < 1cm lesions Bartolozzi et al. (2004) CRC Unenhanced MR Mn-DPDP MR CT 92/128 (72%) 115/128 (90%) 91/128 (71%) 24/47 (51%) 39/47 (83%) 17/47 (38%) Kim MJ et al. (2004) MnDPDP MR SPIO-enhanced. 92/121 (76%) 105/121 (87%) 76% 87% Ward J et al. (2003) CRC PC-T2W-FSE CE-MR Unenhanced MR 83/101 (81%) 92/101 (92%) 80/101 (79%) 22/27 (82%) 24/27 (92%) 21/27 (81%)




42 M-stage: MR vs. FDG-PET FDG-PET Metastases: 65 Lesions <1cm: 12 MRI Metastases: 88 Lesions <1cm 33 Sahani DV et al. AJR 2005



43 M-Stage: Role DWI imaging T2 WI DWI-MR Post -Gd T1 FS



44 Role of PET/PET-CT in CRC Restaging recurrent disease Johnson et al Dis Col Rectum 2001 Before surgery with curative intent Park et al, Ann Surg, 2001 Increased CEA with inconclusive conventional workup Zervoset al, Surgery 2002 Evaluation of equivocal findings on other imaging

45 Colorectal Recurrence Equivocal CT findings 55yo M s/p APR presacral soft tissue abnormality post op vs recurrence?


46 Rising CEA Inconclusive CT 60 yo M s/p APR with chemo and XRT with rising CEA
47 Data obtained from meta-analysis of 11 studies Huebner. J Nuc Med 2000 Role of CT and PET in CRC Care path in CRC CT Accuracy PET Accuracy Sensitivity Specificity Sensitivity Specificity Pre-operative staging 48 to 77% 83 to 95% Recurrent CRC 46 to 69% 96% 79 to 93% 96% Liver Metastases 38 to 79% 97% 78 to 88% 100% Lymph Node Metastases 22 to 73% 96% 29 to 45% 96%
48 Newer Treatments: Neoadjuvant options with therapies targeting neoangiogensis Conventional methods of monitoring treatment response is less effective or inaccurate 4 mts chemo

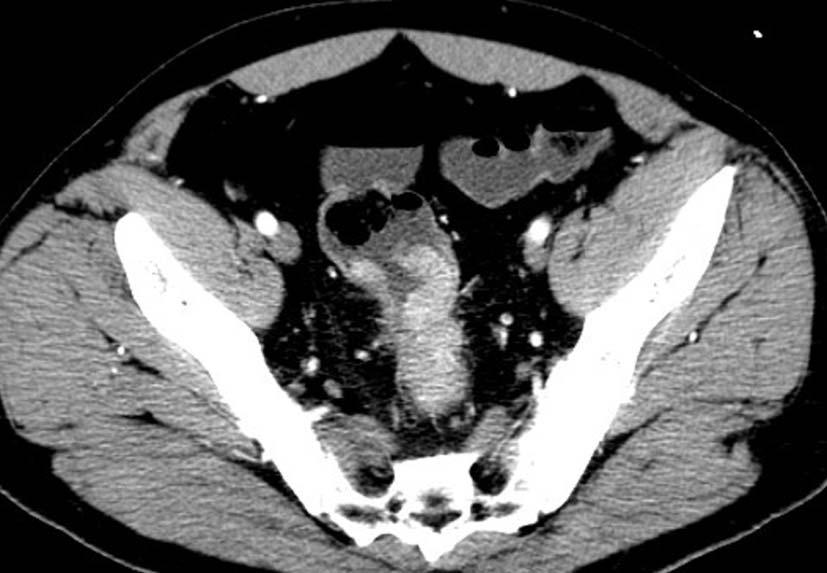
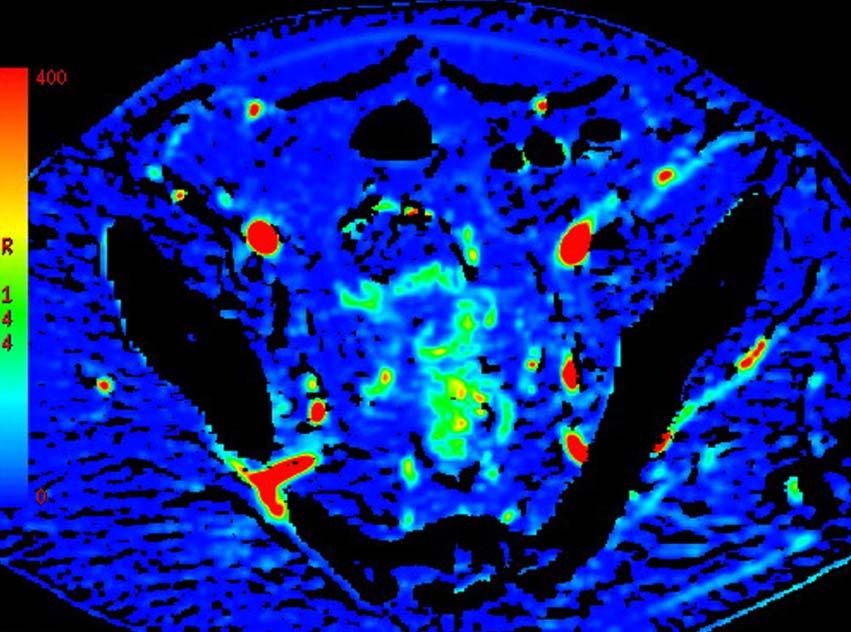
49 CTp Technique
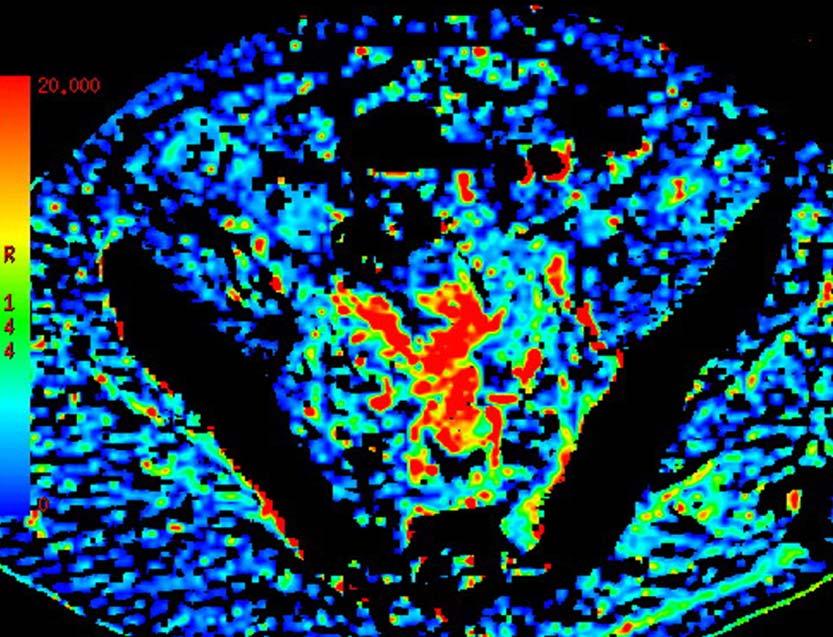
50 Monitoring Antiangiogenic (Avastin) Response in Rectal Cancer Changes in blood flow Baseline BF BF after Avastin Average blood flow reduction of 36% Willett CG et al. Nat Med Feb;10(2):145-7
 Response in")



51 Monitoring Antiangiogenic (Avastin) Response in Rectal Cancer baseline 90 ml/100gm/min 2 weeks following therapy 40 ml/100gm/min ENDOSCOPY PET BLOOD FLOW Willett CG et al. Nat Med Feb;10(2):145-7
52 Rectal Cancer: CTp changes following Treatment BF BV MTT 10 0 Baseline Post Avastin post CRT Sahani. SCBT/MR 2007
53 Sahani. SCBT/MR 2007 Predicting Response: Baseline CTp Response : Downstage of T-stage on pathology from pre treatment Perfusion Parameter Responders 10/16 Non-responders 6/16 P value BF 67.5 ± ± MTT 9.1 ± ±
54 Perfusion CT: Response to Therapy CXRT Mean BF Mean BF Mean BV Mean BV Mean MTT Mean MTT Mean PS Mean PS Before Chemoradiation CRT responders (n=12) CRT nonresponders (n=3) After Chemoradiation Sahani DV et. al. Radiology Mar;234(3):785-92
55 Initial CRC staging Summary CT: Survey MR: T-N staging, liver PET/CT is a combination of two powerful, complementary modalities Tumor recurrence/metastases Monitoring Angiogenesis is feasible with CT/MR
56 Summary High-resolution MRI is highly accurate for preoperative staging Allows identification of critical prognostic risk factors Impacts selection of appropriate management protocol and surgical planning Accurate assessment of nodal disease remains a challenge DWI and Lymphotropic MR contrast agent appear promising for lymph node characterization
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
Esophageal Cancer. What is the value of performing PET scan routinely for staging of esophageal cancers
 Esophageal Cancer What is the value of performing PET scan routinely for staging of esophageal cancers What is the sensitivity and specificity of PET scan for metastatic lesions When should PET scan be
Esophageal Cancer What is the value of performing PET scan routinely for staging of esophageal cancers What is the sensitivity and specificity of PET scan for metastatic lesions When should PET scan be
Colorectal Cancer and FDG PET/CT
 Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014
 Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
Preoperative Staging MRI in Rectal Cancer: Where Are We Going in the Pelvis? Dr. Anat Ravid Surgical Oncology Lead Erie St. Clair Regional Cancer Program May 1, 2014 Objectives: How are we looking? Who
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Acknowledgements. Update of Focal Liver Lesions Goals. Focal Liver Lesions. Imaging Choices For Liver Lesions. Focal Liver Lesions
 Acknowledgements Update of Focal Liver Lesions 2012 Giles Boland Massachusetts General Hospital Harvard Medical School No disclosures Dushyant Sahani Mukesh Harisinghani Goals Focal liver lesions Imaging
Acknowledgements Update of Focal Liver Lesions 2012 Giles Boland Massachusetts General Hospital Harvard Medical School No disclosures Dushyant Sahani Mukesh Harisinghani Goals Focal liver lesions Imaging
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management
 Curr. Treat. Options in Oncol. (2016) 17: 32 DOI 10.1007/s11864-016-0403-7 Lower Gastrointestinal Cancers (AB Benson, Section Editor) Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management
Curr. Treat. Options in Oncol. (2016) 17: 32 DOI 10.1007/s11864-016-0403-7 Lower Gastrointestinal Cancers (AB Benson, Section Editor) Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY
 PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
Imaging techniques in the diagnosis, staging and follow up of GI cancers. Moderators: Banke Agarwal, MD and Paul Schultz, MD
 Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Behandeling van colorectale levermetastasen. Rol van beeldvorming van de lever bij colorectaal carcinoom
 Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
All along the colon: multimodality imaging and staging
 Satellite Symposium ESGAR 2011 All along the colon: multimodality imaging and staging Chairman: Prof. T. Lauenstein (Essen Germany) Invitation Sunday, May 22 nd, 2011 13:00-14:00 Venice Convention Centre,
Satellite Symposium ESGAR 2011 All along the colon: multimodality imaging and staging Chairman: Prof. T. Lauenstein (Essen Germany) Invitation Sunday, May 22 nd, 2011 13:00-14:00 Venice Convention Centre,
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
Local staging of colon cancer: the current role of CT
 Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
PET/CT in Gynaecological Cancers. Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp
 PET/CT in Gynaecological Cancers Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp Cervix cancer Outline of this talk Initial staging Treatment monitoring/guidance
PET/CT in Gynaecological Cancers Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp Cervix cancer Outline of this talk Initial staging Treatment monitoring/guidance
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
Follow up The way ahead. John Griffith
 Follow up The way ahead John Griffith Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring
Follow up The way ahead John Griffith Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
11/09/2014. Update Management of Rectal Cancer. Outline. I have no disclosures
 Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer
 Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer Park JH, Powell AG, Roxburgh CSD, Richards CH, Horgan PG, McMillan DC, Edwards J James Park Clinical
Mismatch repair status, inflammation and outcome in patients with primary operable colorectal cancer Park JH, Powell AG, Roxburgh CSD, Richards CH, Horgan PG, McMillan DC, Edwards J James Park Clinical
FDG-PET/CT in Colo-rectal Cancer & Gastrointestinal Cancer
 Sarajevo (Bosnia & Hercegovina) Tuesday, June 17, 2014 FDG-PET/CT in Colo-rectal Cancer & Gastrointestinal Cancer FDG PET/CT virtual colonoscopy Preoperative staging (A) CT-based virtual colonoscopy showing
Sarajevo (Bosnia & Hercegovina) Tuesday, June 17, 2014 FDG-PET/CT in Colo-rectal Cancer & Gastrointestinal Cancer FDG PET/CT virtual colonoscopy Preoperative staging (A) CT-based virtual colonoscopy showing
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive. Lloyd A. Mack September 19, 2015
 Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
Advanced Pelvic Malignancy: Defining Resectability Be Aggressive Lloyd A. Mack September 19, 2015 CONFLICT OF INTEREST DECLARATION I have no conflicts of interest Advanced Pelvic Malignancies Locally Advanced
RESEARCH ARTICLE. Value of FDG PET/Contrast-Enhanced CT in Initial Staging of Colorectal Cancer - Comparison with Contrast-Enhanced CT
 0.446/apjcp.206.26/APJCP.206.7.8.407 RESEARCH ARTICLE Value of FDG PET/ContrastEnhanced CT in Initial Staging of Colorectal Cancer Comparison with ContrastEnhanced CT Anchisa Kunawudhi, Karun Sereeborwornthanasak
0.446/apjcp.206.26/APJCP.206.7.8.407 RESEARCH ARTICLE Value of FDG PET/ContrastEnhanced CT in Initial Staging of Colorectal Cancer Comparison with ContrastEnhanced CT Anchisa Kunawudhi, Karun Sereeborwornthanasak
Restaging after neoadjuvant chemoradiation in rectal cancers: is histology the key in patient selection?
 Original Article Restaging after neoadjuvant chemoradiation in rectal cancers: is histology the key in patient selection? Nitin Singhal 1, Karthik Vallam 1, Reena Engineer 2, Vikas Ostwal 3, Supreeta Arya
Original Article Restaging after neoadjuvant chemoradiation in rectal cancers: is histology the key in patient selection? Nitin Singhal 1, Karthik Vallam 1, Reena Engineer 2, Vikas Ostwal 3, Supreeta Arya
Title: What is the role of pre-operative PET/PET-CT in the management of patients with
 Title: What is the role of pre-operative PET/PET-CT in the management of patients with potentially resectable colorectal cancer liver metastasis? Pablo E. Serrano, Julian F. Daza, Natalie M. Solis June
Title: What is the role of pre-operative PET/PET-CT in the management of patients with potentially resectable colorectal cancer liver metastasis? Pablo E. Serrano, Julian F. Daza, Natalie M. Solis June
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer
 Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
Introduction. Approximately 40,000 patients are diagnosed with rectal. Original Article
 Original Article Does a fine line exist between regional and metastatic pelvic lymph nodes in rectal cancer striking discordance between national guidelines and treatment recommendations by US radiation
Original Article Does a fine line exist between regional and metastatic pelvic lymph nodes in rectal cancer striking discordance between national guidelines and treatment recommendations by US radiation
Disclosures. Diffusion and Perfusion Imaging in the Head and Neck. Learning objectives ???
 Disclosures No relevant financial disclosures Diffusion and Perfusion Imaging in the Head and Neck Ashok Srinivasan, MD Associate Professor Director of Neuroradiology University of Michigan Health System
Disclosures No relevant financial disclosures Diffusion and Perfusion Imaging in the Head and Neck Ashok Srinivasan, MD Associate Professor Director of Neuroradiology University of Michigan Health System
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Role of DE-CT in Oncology
 Role of DE-CT in Oncology Dushyant Sahani, M.D Director of CT Associate Professor of Radiology Massachusetts General Hospital Harvard Medical School Email-dsahani@partners.org Disclosure Research Grant
Role of DE-CT in Oncology Dushyant Sahani, M.D Director of CT Associate Professor of Radiology Massachusetts General Hospital Harvard Medical School Email-dsahani@partners.org Disclosure Research Grant
AJCC Cancer Staging 8 th Edition
 AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
BC CRC Update Unusual Colorectal Tumors
 BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER
 IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER") THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER Arpana Shrestha, Fu Tian and Jin-jian Xiang Department
THE ROLE OF HIGH RESOLUTION MAGNETIC RESONANCE IMAGING (MRI) IN DETECTING CIRCUMFERENTIAL RESECTION MARGIN (CRM) FOR THE PROGNOSIS OF RECTAL CANCER Arpana Shrestha, Fu Tian and Jin-jian Xiang Department
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
Essentials of Clinical MR, 2 nd edition. 73. Urinary Bladder and Male Pelvis
 73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Oncology Review article High-Resolution MRI in Rectal Cancer
 Oncology Review article High-Resolution MRI in Rectal Cancer Adriana Dieguez Department Of Magnetic Resonance And Computed Tomography In Oncologic Diseases, Diagnóstico Médico Junín 1023, C1113AAE. Buenos
Oncology Review article High-Resolution MRI in Rectal Cancer Adriana Dieguez Department Of Magnetic Resonance And Computed Tomography In Oncologic Diseases, Diagnóstico Médico Junín 1023, C1113AAE. Buenos
MRI and metastases of PCa
 MRI and metastases of PCa François CORNUD Céline COUVIDAT David EISS Arnaud LEFEVRE IRM Paris 16, France, Paris, France Université Paris Descartes, Paris, France When imaging should be considered for detection
MRI and metastases of PCa François CORNUD Céline COUVIDAT David EISS Arnaud LEFEVRE IRM Paris 16, France, Paris, France Université Paris Descartes, Paris, France When imaging should be considered for detection
Contrast-enhanced Breast MRI RSSA 2013
 Contrast-enhanced Breast MRI RSSA 2013 Prof. dr. Maurice van den Bosch University Medical Center Utrecht, the Netherlands Index 1) Breast cancer 2) Why MRI of the breast 3) Technique 4) Interpretation
Contrast-enhanced Breast MRI RSSA 2013 Prof. dr. Maurice van den Bosch University Medical Center Utrecht, the Netherlands Index 1) Breast cancer 2) Why MRI of the breast 3) Technique 4) Interpretation
MRI in staging of rectal carcinoma
 MRI in staging of rectal carcinoma Poster No.: C-0152 Congress: ECR 2015 Type: Scientific Exhibit Authors: J. R. Ramos Rodriguez, M. Atencia Ballesteros, M. D. M. Muñoz Ruiz, A. J. Márquez Moreno, M. D.
MRI in staging of rectal carcinoma Poster No.: C-0152 Congress: ECR 2015 Type: Scientific Exhibit Authors: J. R. Ramos Rodriguez, M. Atencia Ballesteros, M. D. M. Muñoz Ruiz, A. J. Márquez Moreno, M. D.
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
11/10/2015. Prostate cancer in the U.S. Multi-parametric MRI of Prostate Diagnosis and Treatment Planning. NIH estimates for 2015.
 Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER?
 CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
The Surgical Management of Colorectal Metastases
 11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
Stephen McManus, MD David Levi, MD
 Stephen McManus, MD David Levi, MD Prostate MRI Indications INITIAL DETECTION, STAGING, RECURRENT TUMOR LOCALIZATION, RADIATION THERAPY PLANNING INITIAL DETECTION Clinically suspected prostate cancer before
Stephen McManus, MD David Levi, MD Prostate MRI Indications INITIAL DETECTION, STAGING, RECURRENT TUMOR LOCALIZATION, RADIATION THERAPY PLANNING INITIAL DETECTION Clinically suspected prostate cancer before
Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological Response
 Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer. Rectal Cancer: The CCF perspective 16/11/2017. Meagan Costedio, MD, FACS, FASCRS. 38,220 new cases estimated in
 Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
Rectal cancer with synchroneous liver mets: A challenging clinical case
 ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
Dr Sneha Shah Tata Memorial Hospital, Mumbai.
 Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Colorectal Liver Metastases Metachronous
 Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Imaging: When to get MRI, CT or PET-CT?
 Imaging: When to get MRI, CT or PET-CT? Alina Uzelac, D.O. Assistant Clinical Professor Neuroradiology UCSF Department of Radiology and Biomedical Imaging San Francisco General Hospital Overview CT MRI
Imaging: When to get MRI, CT or PET-CT? Alina Uzelac, D.O. Assistant Clinical Professor Neuroradiology UCSF Department of Radiology and Biomedical Imaging San Francisco General Hospital Overview CT MRI
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Low risk. Objectives. Case-based question 1. Evidence-based utilization of imaging in prostate cancer
 Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
CREATE Trial Proposal: Survey of current practice and potential trial participation
 CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Transanal Excision of Rectal Cancer : What Next?
 Transanal Excision of Rectal Cancer : What Next? November 10 th 2017 Meagan Costedio MD FACS FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division
Transanal Excision of Rectal Cancer : What Next? November 10 th 2017 Meagan Costedio MD FACS FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD
 Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures No relevant
Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures No relevant
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment