Rob Glynne-Jones Mount Vernon Cancer Centre
|
|
|
- Sheryl Booker
- 5 years ago
- Views:
Transcription


1 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre
2 My Disclosures: last 5 years Speaker: Roche, Merck Serono, Sanofi Aventis, Pfizer, AIS Advisory Boards: Roche, Merck Serono, Sanofi Aventis, Astra Zeneca, Amgen, Servier, Eisai, BMS Funding to attend meetings: Roche, Merck Serono, Sanofi Aventis, Research funding: Roche, Merck Serono, Sanofi Aventis
3 My Inherent Bias
4 Bias Radiotherapy to the pelvis causes substantial permanent late morbidity and functional problems
5 You need The optimal management of localized rectal cancer: High quality Magnetic Resonance Imaging (MRI). ] 5
 patients who underwent primary")


6 Measuring depth of extramural spread MERCURY Radiology 2007, 243: /311 (95 %) patients who underwent primary surgery. The mean difference between MRI and histopathology assessment of tumor EMD was mm, SD = 3.85 mm, the 95 % CI was to mm. MRI and histopathology assessment of tumor spread are considered equivalent to within 0.5 mm ( R).

7 Extramural vascular invasion

8 EMVI and threatened CRM

9 % Relapse-free MRI-EMVI score & Outcome n=135. Median follow-up=3 12 ( ) years. 100 MRI-EMVI score= 0-2 MRI-EMVI score= % 32% p = Time since operation (Years)
10 You need The optimal management of localized rectal cancer: High quality Magnetic Resonance Imaging (MRI). Surgeons who perform high quality TME ] 10
11 You need The optimal management of localized rectal cancer: High quality Magnetic Resonance Imaging (MRI). Surgeons who perform high quality TME Pathologists who photograph and score the specimen and can confirm high quality and feed back ] 11




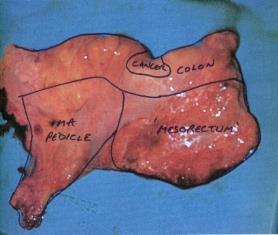
12 We can judge the quality of the Surgery
13 Scoring the Quality of the mesorectum Mesorectum Defects Coning MRF Complete Intact, smooth Not deeper than 5 mm None Smooth, regular Nearly complete Moderate bulk, irregular No visible muscularis propria Moderate Irregular Incomplete Little bulk Down to muscularis propria Moderate marked Irregular Both the specimen as a whole (fresh) and cross sectional slices (fixed) are examined in order to make an adequate interpretation
14 You need The optimal management of localized rectal cancer: High quality Magnetic Resonance Imaging (MRI). Surgeons who perform high quality TME Pathologists who photograph and score the specimen and can confirm high quality and feed back A functional MDT with a good chair ] 14
15 You need The optimal management of localized rectal cancer: High quality Magnetic Resonance Imaging (MRI). Surgeons who perform high quality TME Pathologists who photograph and score the specimen and can confirm high quality and feed back A functional MDT with a good chair To listen to your patient ] 15
16 You need The optimal management of localized rectal cancer: High quality Magnetic Resonance Imaging (MRI). Surgeons who perform high quality TME Pathologists who photograph and score the specimen and can confirm high quality and feed back A functional MDT with a good chair To listen to your patient And maybe in future immunoscore ] 16
17 CD3 infiltration - immunoscore The yptnm downstaging and TRG were used as endpoints to evaluate response to pcrt 72% of the biopsies with high infiltration of CD3 + cells responders to CRT (complete or partial response) 63% of the biopsies with a low infiltration of CD3 + cells were non-responders to CRT (P = 0.015). Anitei M-G Clin Cancer Res 2014;20:1891
18 Pre- vs post-operative chemoradiation CAO/ARO/AIO Locoregional Recurrences P=0.006 Acute G3/4 adverse events 27% vs 40% (p=0.001) Post Pre Months 13% 6% Long-term G3/4 adverse events 14% vs 24% (p=0.01) There is a standard for chemoradiation Sauer R. et al., N Engl J Med 2004;351:
19 Different standards In different countries
20 Glimelius Radiother Oncol 2017

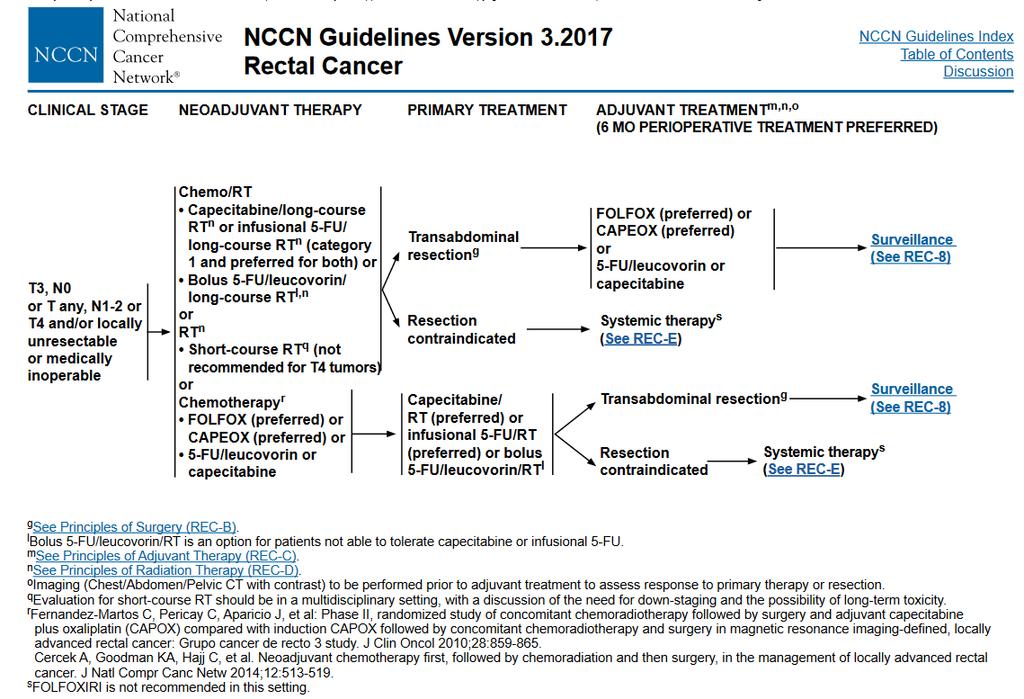
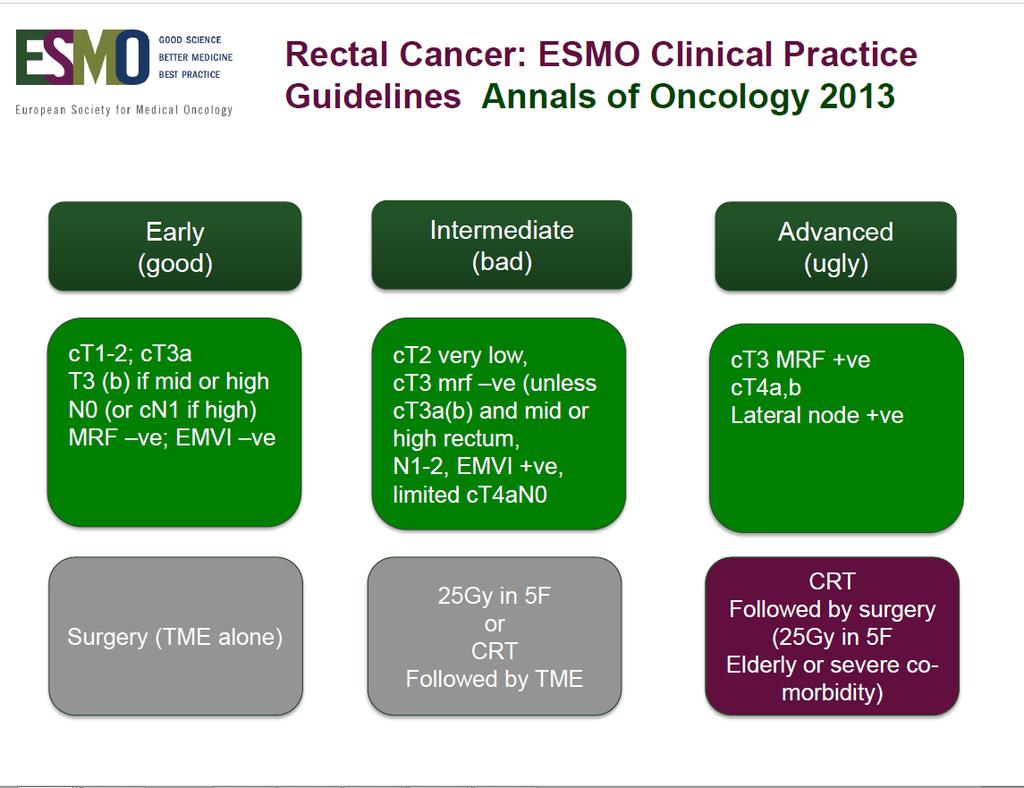
21 ESMO Rectal Cancer Guidelines
22

23 Major Milestones in rectal cancer management
24 Preoperative Options to influence outcomes in rectal cancer Radiotherapy (5 x 5Gy) Chemoradiation (with fluoropyrimidine) Neoadjuvant chemotherapy +/- Biologicals (now Immunotherapy) Different combinations and sequences of the above (4 x 3 x 2 x 1= 24) (Post-op CRT as adjuvant)
25 5 Options for chemotherapy in locally advanced rectal cancer Induction - pre RT (Shortcourse(SCPRT) or chemoradiation (CRT) Concurrent - With RT (CRT) Consolidation - post CRT or SCPRT if waiting 6 12 weeks before surgery Neoadjuvant alone without RT Post-op adjuvant
26 2013 ESMO Guidelines An important aim is to treat so that the risk of residual disease in the pelvis, frequently causing a disabling local recurrence, is very low. This risk should preferably be less than about 5% in the population in whom curative treatment is intended Bengt Glimelius
27 What is the risk of metastatic disease for ct3n1?
28
29 The optimal management of localized rectal cancer Could you select on a more individual basis? ie is preventing local recurrence your only objective?
30 Glimelius Radiother Oncol 2017
31 Pre- vs post-operative chemoradiation CAO/ARO/AIO-94 03/01/13
32 Dutch TME trial Kapiteijn NEJM 2001 At two years, overall survival was 82.0 percent in the group assigned to radiotherapy and surgery and 81.8 percent in the group assigned to surgery alone (P=0.84).
33 SCPRT versus CRT : no difference in local control 14.4% vs 18.6% P= % vs 4.4% P = 0.24). Polish Trial (Bujko 2006) TROG-01 Trial (Ngan 2012)
34 SCPRT versus CRT : Equivalence in overall survival
35 Short course (5x5 Gy) and immediate Surgery Short course (5x5 Gy) and wait 6-8 weeks (or even longer)
36 STOCKHOLM III Resectable Rectal AdenoCa R A N D O M I S E 25 Gy in 5 F 25 Gy in 5 F 50 Gy in 25 F Surgery Surgery (delayed) Surgery (delayed) Primary endpoint: sphincter preservation rate Pettersson et al BJS 2010/ Erlandsson 2017
37 Stockholm III trial :Overall Survival
38 Stockholm III trial :Recurrence Free Survival
39 RT selected on the basis of Involved LN
40 Fokas 2014 Updated Results of the CAO/ARO/AIO-94 Trial for CRT Preop N category No at risk 10-Year Cumulative Incidence of Local Recurrence (%) No at risk 10-Year Cumulative Incidence of Distant Mets (%) No at risk 10-Year DFS (%) Overall cn cn unknown In German trial defining LN status on ultrasound did not predict DFS or OS or LR!
41 Clinical Lymph node staging Parameters of clinical lymph node staging in %. Colon cancer without neoadjuvant treatment Rectal cancer without neoadjuvant treatment Rectal cancer with 5x5 Gy RT (n=21,629) (n=2,178) (n=3,401) Sensitivity Specificity PPV NPV Brouwe NPM, Brouwer M, Stijns RCH, et al., Clinical lymph node staging by imaging in colorectal cancer: A flip of the coin? J Clin Oncol 35, 2017 (suppl; abstr e15160) 41

42 The Mercury Study Patel U et al J Clin Oncol 2011 Magnetic Resonance Imaging Detected Tumor Response for Even Locally Advanced Gina Rectal Brown Cancer Predicts Survival did Outcomes: not find MERCURY that Experience defining LN status on MRI predicted DFS or OS or LR!
43 Local Recurrence rates in CRO7 according the plane of surgery Quirke P et al Lancet Mar 7; 373(9666): Plane of Surgery TNM stage Muscularis propria Intramesorectal Mesorectal I 8% 2% 0% II 6% 2% 5% III 20% 14% 6%
: 821 828 Plane of Surgery TNM stage Muscularis propria Intramesorectal Mesorectal I 8% 2%")
44 Local Recurrence rates in CRO7 according the plane of surgery Quirke P et al Lancet Mar 7; 373(9666): Plane of Surgery TNM stage Muscularis propria Intramesorectal Mesorectal I 8% 2% 0% II 6% 2% 5% III 20% 14% 6%
: 821 828 Plane of Surgery TNM stage Muscularis propria Intramesorectal Mesorectal I 8% 2%")
45 Local Recurrence rates in CRO7 according the plane of surgery Quirke P et al Lancet Mar 7; 373(9666): Plane of Surgery TNM stage Muscularis propria Intramesorectal Mesorectal I 8% 2% 0% II 6% 2% 5% III 20% 14% 6%
46 Pathologically defined Lymph nodes only affect your local recurrence rate if you leave them inside the patient!
47 Novel Options
48 NSABP R04 (5FU vs Capecitabine- +/- oxaliplatin) 1608 patients PVI 5FU 225 mg/m 2, 5 days per week Capecitabine 825 mg/m 2 BID 7 days per week pcr 138/777 (17.8%) 161/779 (20.7%) G3-5 diarrhoea 11.7% 11.7% 3 three-year localregional event rates 11.2% 11.8% 5 Year DFS 66.4% 67.7% 5 year OS 79.9% 80.8%
49 Endpoint STAR-01 ACCORD 12/0405 CAO/ARO/ AIO-04 NSABP R-04 PETACC-6 PCR 16% both arms 14% vs 19% 12.8% vs 16.5% (p=0.038) 19% vs 21% 11.5% vs 13% CRM 4% vs 7% 8% vs 13% 5% vs 6% No data 2% vs 2% Node + (stage III) 29% vs 26% 30% vs 26% 27% vs 26% Not stated 27% vs 26% Oxaliplatin Phase III trials: Control arm in red
50 Phase III Chemoradiotherapy trials with or without Oxaliplatin Trial CAO/ARO/AIO-04 Rodel Lancet Oncology 2015 NSABP R-04 JNCI 2016 ACCORD 12 updated 2016 GI ASCO STAR-01 WGICC 2016 No of patients Regimens DFS Difference 1236 CRT + Ox 60mg Plus OX adjuvant 71.2% vs 75.9% +4.7% (HR 0.79) 1606 CRT + Ox 60mg 64.2% vs 69.2% +5% 598 CRT + Ox 60mg + RT 50Gy 67.9% v 72.7% +4.3% 747 CRT + Ox 60mg 5 year 66.3% vs 69.2 % +2.9% (HR 0.89) PETTAC CRT + Ox 60mg Plus OX adjuvant 75% vs 74% (lowest pcr) -0.6% outlier Chinese Trial Jiao year DFS 69.9% vs 80.6% (P>0.05) 208 CRT + Ox 60mg All received adjuvant ESMO FOLFOX PRECEPTORSHIP 6 8 cycles PROGRAM +10.6%
51 Adjuvant trials in colon cancer using oxaliplatin in the novel arm. Trial Patient No Path Stage Treatment arms Median Age Compliance to planned cycles 5 year DFS MOSAIC (Andre 2004 updated 2015 NSABP C07 (Kuebler 2007) updated 2011 NO16968 (Haller 2011) 2246 II, III LV5FU2 FOLFOX % 74.7% 2407 II, III FULV 59 Not stated FLOX 59 Not stated 1886 III FULV 61 83% XELOX 62 69% 67.5% vs 73.2% +5.7% 64.2% vs 69.4% +5.2% 3-year DFS 70.9% vs 66.5% +4.4%

52 US Intergroup phase III trial ACOSOG, Z9062, CALGB, E81001 LARC stage II/III MRI: CRM -ve R 5FU CRT FOLFOX #6 PR/ SD? PD? T M E R0? R1/2? FOLFOX #8 FOLFOX #6 5FU CRT 5FU CRT N planned: > endpoint: 3y DFS 2 toxicity, local failures, OS,
53 Prospect Selective use of chemoradiation in patients with ct2n1 and ct3n0-1 rectal cancer undergoing sphincter-sparing low anterior resection.
54 Prospect Selective use of chemoradiation in patients with ct2n1 and ct3n0-1 rectal cancer undergoing sphincter-sparing low anterior resection. The 3-year DFS and freedom from LR for PROSPECT-eligible patients were 79.1% and 97.4% BOSSE D et al. Clin Colorectal cancer 2016 Sep;15(3):243-9
55 RAPIDO Trial N = 885 patients T4 EMVI + N2 CRM + R A N D O M I Z A T I O N SCPRT GY 5X5 Standard CRT CapOx + 6 Capecitabine: 825 mg/m2 Oxaliplatin: 130 mg/m2 T M E Primary endpoint 3 year DFS
56 RAPIDO Results: Pathology TNM5 Operated patients (n=792) TNM5 Operated patients (n=796) ypt0 yptis ypt1 ypt2 ypt3 ypt % 0.6% 4.2% 20.3% 44.2% 7.4% ypn0 ypn1 ypn % 19.7% 9.0% 56 ECCO congress, AMSTERDAM - G.A.P. Hospers 28-Jan- 2017
57 Polish-2: study design 6 weeks 6 weeks N = 540, randomized 1:1 ct4 or fixed at DRE ct3 M0 ECOG 0-2 Treatment length and total oxaliplatin dose were balanced.
58 Primary end-point [n=515] R0 resection rates (surgery performed & pathologic R0 status): 77% for SCPRT with 3 cycles of chemotherapy 71% for CRT (control arm) (p=0.081) Overall acute toxicity Grade III/IV toxicities Secondary end-points SCRPT + FOLFOX4 CRTx P value 75% 83% p= % 21% NS pcr rate 16% 12% p= 0.17
59 Polish-2: Secondary end-points Overall survival Disease-free survival p=0.046 p=0.85 chemoradiation short-course radiotherapy with consolidating chemotherapy [median follow-up: 36 months]
60 Conclusions CRT with capecitabine is a standard QA is essential We probably should be more selective for RT We need oncological outcomes/results of RAPIDO? Better paradigm We may need to consider immune markers
61 Thank you
62 Transcriptomic classification of four consensus molecular subtypes CMS1, called MSI-like, contains most microsatellite instable (MSI) tumors and enriched for tumors with a CpG-island methylator phenotype (CIMP) and mutations in the BRAF oncogene (14%). CMS2, called canonical, with high chromosomal instability (CIN) and activation of the Wnt and MYC pathways (37%). CMS3, called metabolic - enriched in KRAS mutations and shows a disruption of metabolic pathways (13%). CMS4, called mesenchymal, has a mesenchymal phenotype and frequent CIMP phenotype (23%) stratifies CRC into intrinsic subtypes with different prognosis Guinney J et al. The consensus molecular subtypes of colorectal cancer. Nat Med 2015;21:

63 or SCPRT + chemo
64 The FOWARC trial Design MdG/RT MdG X1 CRT Gy MdG 2-4 MdG X1 TME Post-op MdG R* FOLFOX/RT FOLFOX x 1 CRT Gy FOLFOX 2-4 FOLFOX TME Post-op FOLFOX FOLFOX Alone FOLFOX x 4-6 Cycles TME Post-op FOLFOX Deng, J Clin Oncol 2016 Endpoints Primary endpoint: 3 yr DFS *Patients recruited from 15 Chinese Centres
65
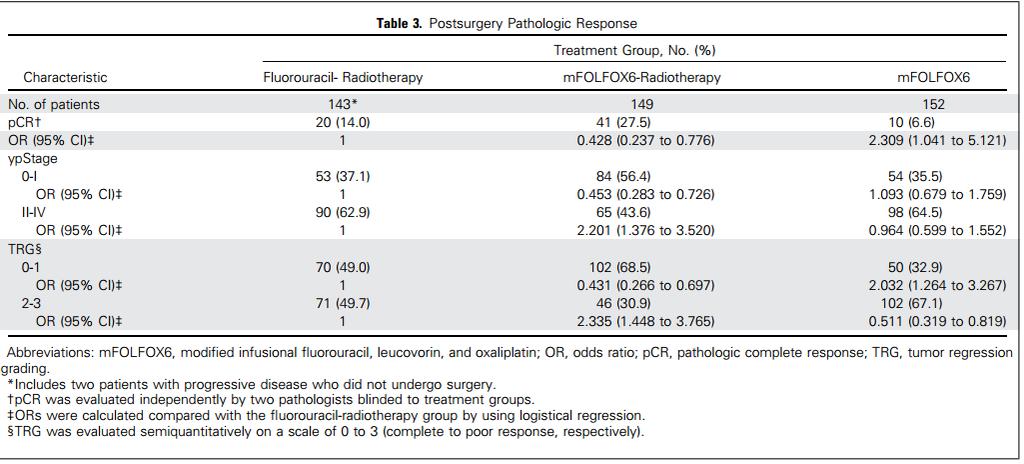
66 Regimens Number of patients G3/G4 toxicity Diarrhea Interval to surgery (median in days) ypn+ pcr TRG0-1 De Gramont RT Gy FOLFOX RT Gy % % 14% 49% % % 27.5% 68.5% FOLFOX alone % Not stated Not stated 6.6% 32.9%
67 FOWARC Regimens Number of patients MRI staging Good quality TME G3/G4 toxicity diarrhea Interval to surgery (median in days) pcr TRG0-1 De Gramont RT Gy % 53 14% 49% FOLFOX RT Gy % 80% 14.5% % 68.5% FOLFOX alone % Not stated 6.6% 32.9%
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Management of early rectal cancer: Any role for adjuvant chemotherapy
 Management of early rectal cancer: Any role for adjuvant chemotherapy Andrés Cervantes Professor of Medicine CURRENTS CONCEPTS IN RECTAL CANCER DIAGNOSIS AND THERAPY TME surgery Optimal staging by MRI
Management of early rectal cancer: Any role for adjuvant chemotherapy Andrés Cervantes Professor of Medicine CURRENTS CONCEPTS IN RECTAL CANCER DIAGNOSIS AND THERAPY TME surgery Optimal staging by MRI
ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER
 ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
State of the art: Standard(s) of radio/chemotherapy for rectal cancer
 of radio/chemotherapy for rectal cancer") State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
Neoadjuvant treatment Evolution and Current Status
 Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
ESMO Preceptorship Programme, Colorectal Cancer, Vienna
 State of the art multimodal treatment of anal cancer ESMO Preceptorship Programme, Colorectal Cancer, Vienna Rob Glynne-Jones Mount Vernon Centre for Cancer Treatment Disclosures: last 5 years Speaker:
State of the art multimodal treatment of anal cancer ESMO Preceptorship Programme, Colorectal Cancer, Vienna Rob Glynne-Jones Mount Vernon Centre for Cancer Treatment Disclosures: last 5 years Speaker:
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Adjuvant treatment for stage III colon cancer
 ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Adjuvant treatment for stage III colon cancer Andrés Cervantes Disclosures Consulting and advisory services, speaking or writing engagements,
ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Adjuvant treatment for stage III colon cancer Andrés Cervantes Disclosures Consulting and advisory services, speaking or writing engagements,
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
CREATE Trial Proposal: Survey of current practice and potential trial participation
 CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Neues zur neoadjuvanten Vorbehandlung beim Rektumkarzinom
 Neues zur neoadjuvanten Vorbehandlung beim Rektumkarzinom Prof. Dr. med. R. Fietkau Strahlenklinik Disclosure I have the following potential confilct(s) of interest to report: Type of affiliation/ financial
Neues zur neoadjuvanten Vorbehandlung beim Rektumkarzinom Prof. Dr. med. R. Fietkau Strahlenklinik Disclosure I have the following potential confilct(s) of interest to report: Type of affiliation/ financial
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Terapia neoadyuvante en cáncer de recto Estado del arte Mauricio Lema Medina MD Clínica de Oncología Astorga / Clínica SOMA - Medellín, Colombia
 Terapia neoadyuvante en cáncer de recto Estado del arte Mauricio Lema Medina MD Clínica de Oncología Astorga / Clínica SOMA - Medellín, Colombia Temario Generalidades Adyuvancia en colon y recto FU / Capecitabina
Terapia neoadyuvante en cáncer de recto Estado del arte Mauricio Lema Medina MD Clínica de Oncología Astorga / Clínica SOMA - Medellín, Colombia Temario Generalidades Adyuvancia en colon y recto FU / Capecitabina
Disclosures. Clinical and molecular features to guide adjuvant therapy. Personalized Medicine - Decision Tools -
 Disclosures Clinical and molecular features to guide adjuvant therapy Daniel Sargent Professor of Biostatistics & Oncology Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis
Disclosures Clinical and molecular features to guide adjuvant therapy Daniel Sargent Professor of Biostatistics & Oncology Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Adjuvant treatment Colon Cancer
 ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
Perioperative versus adjuvant management of gastric cancer, update 2013
 Perioperative versus adjuvant management of gastric cancer, update 2013 Cornelis J.H. van de Velde, MD, PhD,FRCPS and FACS,Hon. Professor of Surgery President ECCO - the European Cancer Organization Past-President
Perioperative versus adjuvant management of gastric cancer, update 2013 Cornelis J.H. van de Velde, MD, PhD,FRCPS and FACS,Hon. Professor of Surgery President ECCO - the European Cancer Organization Past-President
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT
 Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Rectal cancer: Poster Session Review
 AIOM PostASCO GI Roma, 5-6 febbraio 2016 Rectal cancer: Poster Session Review Sara Lonardi SS Trattamento Multidisciplinare Tumori Colorettali - UOC Oncologia Medica 1 Dipartimento di Oncologia Clinica
AIOM PostASCO GI Roma, 5-6 febbraio 2016 Rectal cancer: Poster Session Review Sara Lonardi SS Trattamento Multidisciplinare Tumori Colorettali - UOC Oncologia Medica 1 Dipartimento di Oncologia Clinica
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Rectal cancer with synchroneous liver mets: A challenging clinical case
 ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO
 Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Congresso AIOM Giovani Perugia, 9 luglio 2016 NOVITA IN TEMA DI TERAPIA DEL CARCINOMA DEL COLON-RETTO Carlotta Antoniotti Polo Oncologico Azienda Ospedaliero-Universitaria Pisana Università di Pisa What
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Is There a New Standard of Care for Adjuvant Therapy in Colon Cancer? When is 3 Months Enough?
 Is There a New Standard of Care for Adjuvant Therapy in Colon Cancer? When is 3 Months Enough? Jeffrey Meyerhardt, MD, MPH Dana-Farber Cancer Institute Boston, MA 1 Disclosure Ad Board: Genentech Honorarium:
Is There a New Standard of Care for Adjuvant Therapy in Colon Cancer? When is 3 Months Enough? Jeffrey Meyerhardt, MD, MPH Dana-Farber Cancer Institute Boston, MA 1 Disclosure Ad Board: Genentech Honorarium:
American College of Surgeons Clinical Research Program Surgical Investigators Webinar. November 17, Moderator: Y. Nancy You, M.D.
 American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director American College of Surgeons Clinical Research Program Surgical Investigators Webinar November 17, 2017 Moderator:
American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director American College of Surgeons Clinical Research Program Surgical Investigators Webinar November 17, 2017 Moderator:
Adjuvant therapies for large bowel cancer Wasantha Rathnayake, MD
 LEADING ARTICLE Adjuvant therapies for large bowel cancer Wasantha Rathnayake, MD Consultant Clinical Oncologist, National Cancer Institute, Maharagama, Sri Lanka. Key words: Large bowel; Cancer; Adjuvant
LEADING ARTICLE Adjuvant therapies for large bowel cancer Wasantha Rathnayake, MD Consultant Clinical Oncologist, National Cancer Institute, Maharagama, Sri Lanka. Key words: Large bowel; Cancer; Adjuvant
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Anal Cancer Valencia May 2018 Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker: Roche, Merck Serono,
ESMO Preceptorship Programme Anal Cancer Valencia May 2018 Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker: Roche, Merck Serono,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
Progress and Challenges in the Adjuvant Treatment of Stage II & III Colon Cancer
 Progress and Challenges in the Adjuvant Treatment of Stage II & III Colon Cancer Professor Eva Segelov Monash Health and Monash University (with thanks to A/P Jeremy Shapiro) Melbourne, Australia Apr 2017
Progress and Challenges in the Adjuvant Treatment of Stage II & III Colon Cancer Professor Eva Segelov Monash Health and Monash University (with thanks to A/P Jeremy Shapiro) Melbourne, Australia Apr 2017
S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m B a y e r
 EXPERTS KNOWLEDGE SHARE with Prof. Köhne, Dr. Modest and Dr. Vecchione Madrid (Spain) Sunday September 10 th 2017 S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m
EXPERTS KNOWLEDGE SHARE with Prof. Köhne, Dr. Modest and Dr. Vecchione Madrid (Spain) Sunday September 10 th 2017 S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m
MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany
 MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory boards for AMGEN, ROCHE I Speaker
MSI and other molecular markers: how useful are they? Daniela E. Aust, Institute for Pathology, University Hospital Dresden, Germany Disclosure slide I Member of advisory boards for AMGEN, ROCHE I Speaker
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer
 Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer") Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016
 Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016 Disclosures Consultant for Johnson and Johnson (Ethicon Inc) Encompasses
Where are we at with organ preservation for rectal cancer? Simon Bach Queen Elizabeth Hospital Birmingham ACPGBI Edinburgh 2016 Disclosures Consultant for Johnson and Johnson (Ethicon Inc) Encompasses
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
THE BEST OF ESMO 2016
 THE BEST OF ESMO 2016 Colorectal cancer Pr Julien TAIEB, Sorbonne Paris Cité and Paris Descartes University Georges Pompidou European Hospital Paris, FRANCE esmo.org DISCLOSURES JT has received research
THE BEST OF ESMO 2016 Colorectal cancer Pr Julien TAIEB, Sorbonne Paris Cité and Paris Descartes University Georges Pompidou European Hospital Paris, FRANCE esmo.org DISCLOSURES JT has received research
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
American College of Surgeons Clinical Research Program Surgical Investigators Webinar. October 5, Moderator: Y. Nancy You, M.D.
 American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director American College of Surgeons Clinical Research Program Surgical Investigators Webinar October 5, 2018 Moderator:
American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director American College of Surgeons Clinical Research Program Surgical Investigators Webinar October 5, 2018 Moderator:
The Role Of The Post-CRT MRI In Assessing Response
 Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer -
 International Society of Geriatric Oncology Lisbon October 23 rd 25t h 2014 Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer - Claus-Henning Köhne Klinik für Onkologie
International Society of Geriatric Oncology Lisbon October 23 rd 25t h 2014 Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer - Claus-Henning Köhne Klinik für Onkologie
Biomarkers to optimize treatment selection in colorectal cancer Edwin Pun HUI, MBChB, MD, FRCP (Lond & Edin)
") Recent advances in the management of CRC II 2017/12/17 (Sun.) 10:10-11:00 Biomarkers to optimize treatment selection in colorectal cancer Edwin Pun HUI, MBChB, MD, FRCP (Lond & Edin) Department of Clinical
Recent advances in the management of CRC II 2017/12/17 (Sun.) 10:10-11:00 Biomarkers to optimize treatment selection in colorectal cancer Edwin Pun HUI, MBChB, MD, FRCP (Lond & Edin) Department of Clinical
Long Term Outcomes of Preoperative versus
 RESEARCH ARTICLE Long Term Outcomes of Preoperative versus Postoperative Concurrent Chemoradiation for Locally Advanced Rectal Cancer: Experience from Ramathibodi Medical School in Thailand Pichayada Darunikorn
RESEARCH ARTICLE Long Term Outcomes of Preoperative versus Postoperative Concurrent Chemoradiation for Locally Advanced Rectal Cancer: Experience from Ramathibodi Medical School in Thailand Pichayada Darunikorn
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
RECTAL CANCER: Adjuvant Therapy. Maury Rosenstein, MD Montefiore Medical Center December 2012
 RECTAL CANCER: Adjuvant Therapy Maury Rosenstein, MD Montefiore Medical Center December 2012 Overview Indications for adjuvant therapy Preoperative Postoperative New Advances Epidemiology Approximately
RECTAL CANCER: Adjuvant Therapy Maury Rosenstein, MD Montefiore Medical Center December 2012 Overview Indications for adjuvant therapy Preoperative Postoperative New Advances Epidemiology Approximately
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Pancreatic Adenocarcinoma
 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
COLORECTAL CANCER. Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program
 COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
COLORECTAL CANCER Bert H. O Neil, MD Jackie and Joseph Cusick Professor of Oncology Director, GI Malignancies and Phase I Program Rectal Cancer Adjuvant therapy No single study specific to rectal cancer
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Neoadjuvant Therapy for Rectal Cancer is Overrated. Joon H. Lee, Research Resident University of Colorado 8/31/2009
 Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
The International Duration Evaluation of Adjuvant Chemotherapy study: implications for clinical practice
 Editorial The International Duration Evaluation of Adjuvant Chemotherapy study: implications for clinical practice Marwan Fakih Department of Medical Oncology and Therapeutics Research, City of Hope Comprehensive
Editorial The International Duration Evaluation of Adjuvant Chemotherapy study: implications for clinical practice Marwan Fakih Department of Medical Oncology and Therapeutics Research, City of Hope Comprehensive
2015 EUROPEAN CANCER CONGRESS
 2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Preoperative or Postoperative Therapy for the Management of Patients with Stage II or III Rectal Cancer
 Evidence-Based Series 2-4 Version 2 A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Preoperative or Postoperative Therapy for the Management of Patients with
Evidence-Based Series 2-4 Version 2 A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Preoperative or Postoperative Therapy for the Management of Patients with
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Contemporary management of locally advanced rectal cancer: Resolving issues, controversies and shifting paradigms
 Review Article Contemporary management of locally advanced rectal cancer: Resolving issues, controversies and shifting paradigms Aeris Jane D. Nacion 1, Youn Young Park 2, Nam Kyu Kim 2 1 Department of
Review Article Contemporary management of locally advanced rectal cancer: Resolving issues, controversies and shifting paradigms Aeris Jane D. Nacion 1, Youn Young Park 2, Nam Kyu Kim 2 1 Department of
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
12/7/2011. The reporting of colorectal cancer pathology: recent advances. Colorectal cancer resection specimens
 The reporting of colorectal cancer pathology: recent advances Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 Colorectal cancer resection specimens
The reporting of colorectal cancer pathology: recent advances Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 Colorectal cancer resection specimens
Ning Li, Jing Jin, Jing Yu, Shuai Li, Yuan Tang, Hua Ren, Wenyang Liu, Shulian Wang, Yueping Liu, Yongwen Song, Hui Fang, Zihao Yu, Yexiong Li
 Original Article Down-staging depth score to predict outcomes in locally advanced rectal cancer achieving ypi stage after neoadjuvant chemo-radiotherapy versus de novo stage pi cohort: A propensity score-matched
Original Article Down-staging depth score to predict outcomes in locally advanced rectal cancer achieving ypi stage after neoadjuvant chemo-radiotherapy versus de novo stage pi cohort: A propensity score-matched
Evaluation of the Efficacy of Modified De Gramont and Modified FOLFOX4 Regimens for Adjuvant Therapy of Locally Advanced Rectal Cancer
 Efficacy of Modified De Gramont and FOLFOX4 Regimens for Locally Advanced Rectal Cancer RESEARCH COMMUNICATION Evaluation of the Efficacy of Modified De Gramont and Modified FOLFOX4 Regimens for Adjuvant
Efficacy of Modified De Gramont and FOLFOX4 Regimens for Locally Advanced Rectal Cancer RESEARCH COMMUNICATION Evaluation of the Efficacy of Modified De Gramont and Modified FOLFOX4 Regimens for Adjuvant
JY Douillard MD, PhD Professor of Medical Oncology
 Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
Advances in Chemotherapy of Colorectal Cancer
 Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Meta analysis in Rectal Cancer
 Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
The left versus right colon cancer story What is the truth?
 The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
The left versus right colon cancer story What is the truth? Prof. V. Heinemann CCC LMU, Klinikum Grosshadern Ludwig-Maximilian-University of Munich, Germany Three stages of truth (Schopenhauer) Ridicule
JY Douillard MD, PhD Professor of Medical Oncology
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
Short-Course Radiation Versus Long-Course Chemoradiation for Rectal Cancer
 Original Article 1223 Short-Course Radiation Versus Long-Course Chemoradiation for Rectal Cancer Bruce D. Minsky, MD a ; Claus Rödel, MD b ; and Vincenzo Valentini, MD c Abstract The 2 broad approaches
Original Article 1223 Short-Course Radiation Versus Long-Course Chemoradiation for Rectal Cancer Bruce D. Minsky, MD a ; Claus Rödel, MD b ; and Vincenzo Valentini, MD c Abstract The 2 broad approaches
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
Colorectal Cancer in 2017: From Biology to the Clinics. Rodrigo Dienstmann
 Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
Colorectal Cancer in 2017: From Biology to the Clinics Rodrigo Dienstmann MOLECULAR CLASSIFICATION Tumor cell Immune cell Tumor microenvironment Stromal cell MOLECULAR CLASSIFICATION Biomarker Tumor cell
BRAF Testing In The Elderly: Same As in Younger Patients?
 EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer