Case presentation. Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016
|
|
|
- Bethany Short
- 5 years ago
- Views:
Transcription
1 Case presentation Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016
2 60 y/o man with long standing UC+PSC. Last 10 years on clinical and endoscopic remission. Med: Asacol 4.8 gr/d +Ursodiol 750mg/d

3 Colonoscopy 2010 Colonoscopy 2010 Pathology: Negative for dysplasia Inflammatory polyp
4 Colonoscopy 2011 Negative for dysplasia

5 Colonoscopy 2013 Pathology: Negative for dysplasia

6 Colonoscopy April 2014 Flat lesions rectum- from 10 cm. Pathology- Low grade dysplasia
7 60 y/o, UC+PSC What next? Colonoscopy 2010 No dysplasia Colonoscopy 2013 No dysplasia April 2014 Low grade dysplasia Rectum (10CM)

8 Colonoscopy Sep Biopsy from 50 cm- indefinite for dysplasia cm -Low grade Dysplasia -
9 60 y/o, UC+PSC What next? Colonoscopy 2010 No dysplasia Colonoscopy 2013 No dysplasia April 2014 Low grade dysplasia Rectum (10CM) Colonoscopy Sep 2014 Sep 2014 Indefinite dysplasia Bx from 50 cm Low grade dysplasia from Bx 10 cm
10 Colonoscopy Nov lesion in the ascending colon.(distorted TUBULAR ARCHITECTURE) 2.lesion in the splenic flexure.(tubulovillous ADENOMATOUS CHANGE ) 3.lesion in the rectum.(low grade dysplasia)
11 60 y/o, UC+PSC What next? Multifocal lesions Colonoscopy 2010 No dysplasia Colonoscopy 2013 No dysplasia April 2014 Low grade dysplasia Rectum (10CM) Sep 2014 Indefinite dysplasia from 50 cm Low grade dysplasia from 10 cm. Nov 2014 RT colon Lesion. Splenic flexure lesions Rectum lesions

12 Case 2 Dysplasia associated lesion or mass Adenoma like Mass
13 Case 2
14 Case 2
15 Background
16
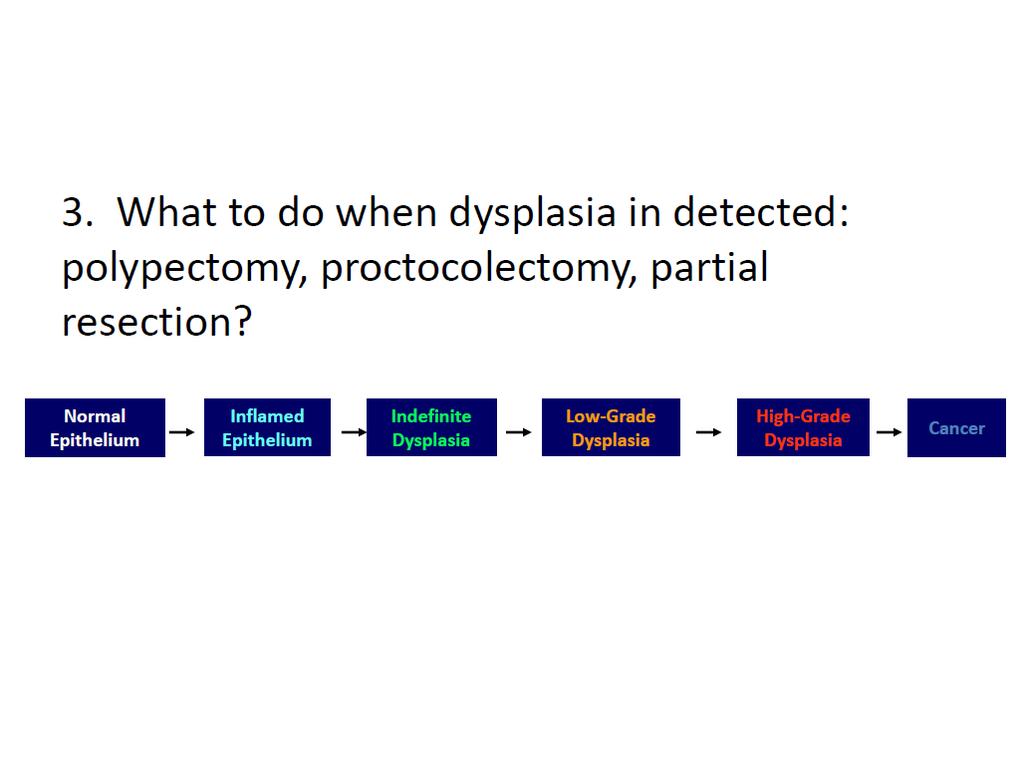
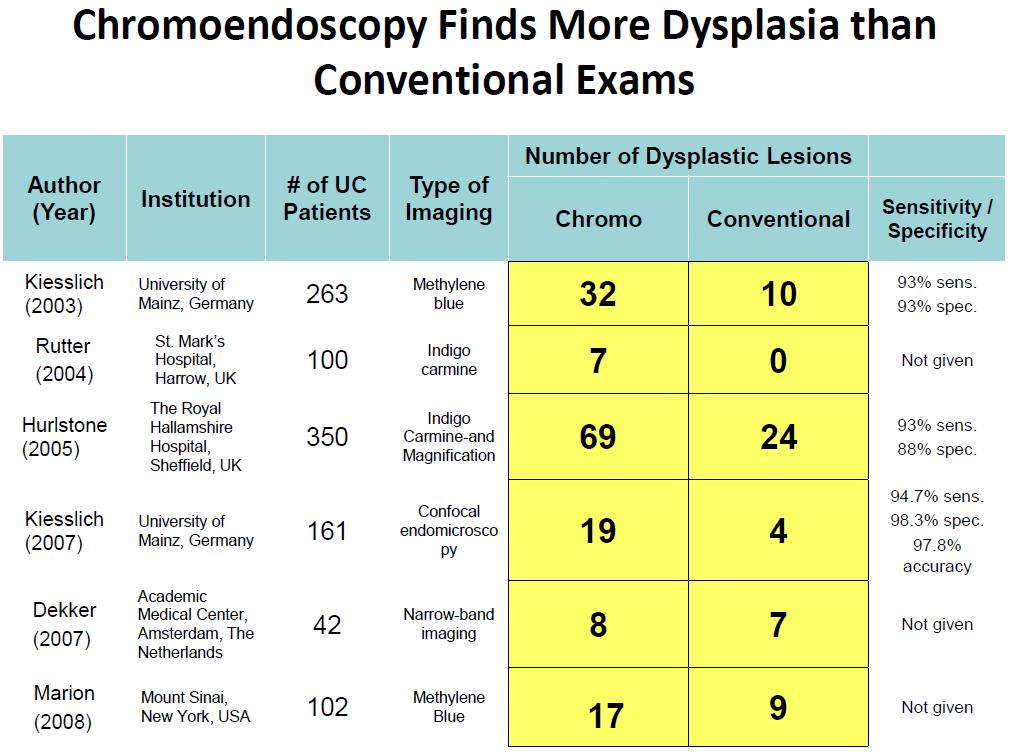
17 Performance of surveillance and role of chromoendoscopy: what is standard of care?
18
19
20

21
22
23
24
25
26
27
28 So what is the right answer?
29

30 Discuss it with your patients
31 Thanks Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. Feb 2016
32
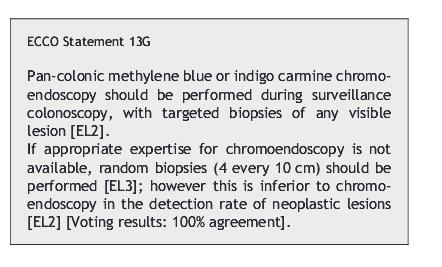
33 ECCO 2013
34 Final pathology Case 1 Specimen: COLON RIGHT Gross Description: The specimen container is labeled with the patient's identification and as "right hemicolectomy" and contains a right hemicolectomy specimen comprised of terminal ileum, ileocecal valve, appendix, cecum, ascending colon and adjacent pericolonic adipose tissue. The terminal ileum measures 8.2 cm in length 6.5 cm in lumenal circumference. Ileocecal valve measures 6.6 cm in circumference. The appendix measures 4.6 cm in length x 1.3 cm in diameter. The colonic component of the specimen measures 25.2 cm in length by up to 11.4 cm in the middle circumference. Both the proximal and distal margins of the specimen are received opened. Pericolonic adipose tissue is present to a maximum of 8.6 cm. Within the ascending colon there is a circumferential, broad-based and constricting lesion measuring 3.5 cm from proximal to distal thigh 4.8 cm in lumenal circumference. The lumen narrows to a minimum of 2.6 cm. This lesion is present 14.5 cm from the proximal margin and 10.4 cm from the distal margin. This lesion causes puckering of the serosal surface. Serial cuts of the lesion demonstrated chalky white and gray appearance with obliteration of the muscularis propria, extension into the adjacent adipose tissue. This lesion extends to within 0.1 cm of the closest peritonealized surface, and is present 1.4 cm from the closest pericolonic margin of resection. The mucosa of the terminal ileum has a finely granular tan and gray appearance. There is a single focus of nodularity noted measuring 2.1 x 2.3 cm, and is present 2.5 cm from the proximal margin. Serial cuts through this focus show slightly thickened mucosa. The ileocecal valve has a slight flattened and otherwise unremarkable appearance. The serosal aspect of the appendix is pink-tan, smooth and glistening. Serial cuts show a patent unremarkable lumen. The mucosa of the cecum has a thickened, nodular tan and pink appearance however is unremarkable on sectioning. The remaining serosal aspect of the specimen is pink-tan glistening appearance. The bowel wall ranges in thickness from 0.4 to 0.6 cm. Palpation of the adjacent pericolonic adipose tissue reveals multiple well-circumscribed ovoid nodules, consistent with lymph nodes that measure up to 1.4 cm in greatest dimension.
35 Staging information is based on the AJCC 7th edition Case 1 Ancillary Testing: The tumour has been examined for the mismatch repair genes products MLH1, MSH2, MSH6 and PMS2 because of the patients age (< 60). MLH1: Normal nuclear staining. MSH2: Normal nuclear staining. MSH6: Normal nuclear staining. PMS2: Normal nuclear staining. Immunohistochemcial analysis showed normal nuclear staining for MLH1, MSH2, MSH6 and PMS2. This finding is highly correlated with tumours that are microsatellite stable (MSS). This testing does not preclude referral to a genetic counsellor if there is a strong family history or if there is concern that this patient has a risk for hereditary cancer. Additional Information (added November 29, 2011): Review of the specimen with the additional endoscopic findings shows deep plasma cells and eosinophils with mild architectural distortion consistent with an underlying chronic colitis. The disease is most severe in the distal part of the specimen and would be consistent with ulcerative colitis. The distal margin shows focal nuclear atypia and findings which would be considered indefinite for dysplasia in the setting of colitis.
36 Colonoscopy pathology report Case 1 1. The specimen container is labelled with the patient's identification and contains 3 pieces of tan to pink tissue ranging up to 0.1 to 0.2 cm in greatest dimension. - 1 tissue submitted in toto. 2. The specimen container is labelled with the patient's identification and contains 2 pieces of pink-tan tissue measuring 0.1 and 0.2 cm in greatest dimension. - 1 tissue submitted in toto. Microscopic Description: Both biopsies show active colitis with regenerative mucosa consistent with an active chronic colitis. Mucosal ulceration with ulcer base material is noted in the rectal biopsy. In addition, both biopsies show areas of increased nuclear atypia and gland crowding consistent with a low-grade tubular adenoma or focal low-grade dysplasia. Endoscopic correlation is required to separate discrete adenomas vs. areas of low-grade dysplasia. DIAGNOSIS: 1, 2. Colon (25cm, rectum), biopsies: - Active chronic colitis with focal low-grade dysplasia (see description)
37 Stage grouping Once a person's T, N, and M categories have been determined, usually after surgery, this information is combined in a process called stage grouping. The stage is expressed in Roman numerals from stage I (the least advanced) to stage IV (the most advanced). Some stages are subdivided with letters. Stage 0 Tis, N0, M0: The cancer is in the earliest stage. It has not grown beyond the inner layer (mucosa) of the colon or rectum. This stage is also known as carcinoma in situ or intramucosal carcinoma. Stage I T1-T2, N0, M0: The cancer has grown through the muscularis mucosa into the submucosa (T1) or it may also have grown into the muscularis propria (T2). It has not spread to nearby lymph nodes or distant sites. Stage IIA T3, N0, M0: The cancer has grown into the outermost layers of the colon or rectum but has not gone through them (T3). It has not reached nearby organs. It has not yet spread to the nearby lymph nodes or distant sites. Stage IIB T4a, N0, M0: The cancer has grown through the wall of the colon or rectum but has not grown into other nearby tissues or organs (T4a). It has not yet spread to the nearby lymph nodes or distant sites. Stage IIC T4b, N0, M0: The cancer has grown through the wall of the colon or rectum and is attached to or has grown into other nearby tissues or organs (T4b). It has not yet spread to the nearby lymph nodes or distant sites. Stage IIIA One of the following applies. T1-T2, N1, M0: The cancer has grown through the mucosa into the submucosa (T1) and it may also have grown into the muscularis propria (T2). It has spread to 1 to 3 nearby lymph nodes (N1a/N1b) or into areas of fat near the lymph nodes but not the nodes themselves (N1c). It has not spread to distant sites. T1, N2a, M0: The cancer has grown through the mucosa into the submucosa (T1). It has spread to 4 to 6 nearby lymph nodes (N2a). It has not spread to distant sites. Stage IIIB One of the following applies. T3-T4a, N1, M0: The cancer has grown into the outermost layers of the colon or rectum (T3) or through the visceral peritoneum (T4a) but has not reached nearby organs. It has spread to 1 to 3 nearby lymph nodes (N1a/N1b) or into areas of fat near the lymph nodes but not the nodes themselves (N1c). It has not spread to distant sites. T2-T3, N2a, M0: The cancer has grown into the muscularis propria (T2) or into the outermost layers of the colon or rectum (T3). It has spread to 4 to 6 nearby lymph nodes (N2a). It has not spread to distant sites. T1-T2, N2b, M0: The cancer has grown through the mucosa into the submucosa (T1) or it may also have grown into the muscularis propria (T2). It has spread to 7 or more nearby lymph nodes (N2b). It has not spread to distant sites. Stage IIIC One of the following applies. T4a, N2a, M0: The cancer has grown through the wall of the colon or rectum (including the visceral peritoneum) but has not reached nearby organs (T4a). It has spread to 4 to 6 nearby lymph nodes (N2a). It has not spread to distant sites. T3-T4a, N2b, M0: The cancer has grown into the outermost layers of the colon or rectum (T3) or through the visceral peritoneum (T4a) but has not reached nearby organs. It has spread to 7 or more nearby lymph nodes (N2b). It has not spread to distant sites. T4b, N1-N2, M0: The cancer has grown through the wall of the colon or rectum and is attached to or has grown into other nearby tissues or organs (T4b). It has spread to at least one nearby lymph node or into areas of fat near the lymph nodes (N1 or N2). It has not spread to distant sites. Stage IVA Any T, Any N, M1a: The cancer may or may not have grown through the wall of the colon or rectum, and it may or may not have spread to nearby lymph nodes. It has spread to 1 distant organ (such as the liver or lung) or set of lymph nodes (M1a). Stage IVB Any T, Any N, M1b: The cancer may or may not have grown through the wall of the colon or rectum, and it may or may not have spread to nearby lymph nodes. It has spread to more than 1 distant organ (such as the liver or lung) or set of lymph nodes, or it has spread to distant parts of the peritoneum (the lining of the abdominal cavity) (M1b). If you have any questions about your stage, please ask your doctor to explain the extent of your disease.
38 Stage grouping Once a person's T, N, and M categories have been determined, usually after surgery, this information is combined in a process called stage grouping. The stage is expressed in Roman numerals from stage I (the least advanced) to stage IV (the most advanced). Some stages are subdivided with letters. Stage 0 Tis, N0, M0: The cancer is in the earliest stage. It has not grown beyond the inner layer (mucosa) of the colon or rectum. This stage is also known as carcinoma in situ or intramucosal carcinoma. Stage I T1-T2, N0, M0: The cancer has grown through the muscularis mucosa into the submucosa (T1) or it may also have grown into the muscularis propria (T2). It has not spread to nearby lymph nodes or distant sites. Stage IIA T3, N0, M0: The cancer has grown into the outermost layers of the colon or rectum but has not gone through them (T3). It has not reached nearby organs. It has not yet spread to the nearby lymph nodes or distant sites. Stage IIB T4a, N0, M0: The cancer has grown through the wall of the colon or rectum but has not grown into other nearby tissues or organs (T4a). It has not yet spread to the nearby lymph nodes or distant sites. Stage IIC T4b, N0, M0: The cancer has grown through the wall of the colon or rectum and is attached to or has grown into other nearby tissues or organs (T4b). It has not yet spread to the nearby lymph nodes or distant sites. Stage IIIA One of the following applies. T1-T2, N1, M0: The cancer has grown through the mucosa into the submucosa (T1) and it may also have grown into the muscularis propria (T2). It has spread to 1 to 3 nearby lymph nodes (N1a/N1b) or into areas of fat near the lymph nodes but not the nodes themselves (N1c). It has not spread to distant sites. T1, N2a, M0: The cancer has grown through the mucosa into the submucosa (T1). It has spread to 4 to 6 nearby lymph nodes (N2a). It has not spread to distant sites. Stage IIIB One of the following applies. T3-T4a, N1, M0: The cancer has grown into the outermost layers of the colon or rectum (T3) or through the visceral peritoneum (T4a) but has not reached nearby organs. It has spread to 1 to 3 nearby lymph nodes (N1a/N1b) or into areas of fat near the lymph nodes but not the nodes themselves (N1c). It has not spread to distant sites. T2-T3, N2a, M0: The cancer has grown into the muscularis propria (T2) or into the outermost layers of the colon or rectum (T3). It has spread to 4 to 6 nearby lymph nodes (N2a). It has not spread to distant sites. T1-T2, N2b, M0: The cancer has grown through the mucosa into the submucosa (T1) or it may also have grown into the muscularis propria (T2). It has spread to 7 or more nearby lymph nodes (N2b). It has not spread to distant sites. Stage IIIC One of the following applies. T4a, N2a, M0: The cancer has grown through the wall of the colon or rectum (including the visceral peritoneum) but has not reached nearby organs (T4a). It has spread to 4 to 6 nearby lymph nodes (N2a). It has not spread to distant sites. T3-T4a, N2b, M0: The cancer has grown into the outermost layers of the colon or rectum (T3) or through the visceral peritoneum (T4a) but has not reached nearby organs. It has spread to 7 or more nearby lymph nodes (N2b). It has not spread to distant sites. T4b, N1-N2, M0: The cancer has grown through the wall of the colon or rectum and is attached to or has grown into other nearby tissues or organs (T4b). It has spread to at least one nearby lymph node or into areas of fat near the lymph nodes (N1 or N2). It has not spread to distant sites. Stage IVA Any T, Any N, M1a: The cancer may or may not have grown through the wall of the colon or rectum, and it may or may not have spread to nearby lymph nodes. It has spread to 1 distant organ (such as the liver or lung) or set of lymph nodes (M1a). Stage IVB Any T, Any N, M1b: The cancer may or may not have grown through the wall of the colon or rectum, and it may or may not have spread to nearby lymph nodes. It has spread to more than 1 distant organ (such as the liver or lung) or set of lymph nodes, or it has spread to distant parts of the peritoneum (the lining of the abdominal cavity) (M1b). If you have any questions about your stage, please ask your doctor to explain the extent of your disease.
39 Colonoscopy 2012 Case 1 The video colonoscope was introduced into the rectum and advanced to the anastomosis on the right side. The neoterminal ileum was seen and was entirely normal.. Random biopsy was taken. The anastomosis itself looked well-healed except for some small puckering of the skin. There was no obvious area of concern. On withdrawing the scope, the remainder of the colonic mucosa with the preparation looked normal without any obvious signs of inflammation. In the sigmoid around 30 cm, there was a little bit of inflammation with small aphthous ulcers. This was biopsied The rectum itself appeared relatively normal. Retroflexion views were normal in the rectal junction. IMPRESSION: Normal-looking colon. Rule out recurrence of dysplasia, and rule out microscopic signs of inflammation.
40 Pathology from Colonoscopy 2012 Case 1 DIAGNOSIS: 1. Terminal ileum, biopsy: - Without significant abnormality 2. Anastomosis site, biopsy: - Without significant abnormality 3+4. Colon, 80 cm and 60 cm, biopsies: - Chronic colitis, inactive - Negative for dysplasia 5. Colon, 30 cm, biopsy: - Chronic colitis, inactive - Focal low grade dysplasia 6. Colon, rectum, biopsy: - Chronic colitis, inactive - Focal epithelial changes indefinite for dysplasia
41 Last colonoscopy 12/2014 Case 1 Procedure Note: Following informed consent and the usual bowel preparation, the patient was sedated with midazolam 4 mg and fentanyl 25 mcg IV. Digital rectal exam was performed, which was normal. The pediatric colonoscope was inserted per rectum and advanced to the anastomosis, where the neoterminal ileum was intubated. The neoterminal ileum was normal as was the anastomosis. The right colon was also normal. Between 40 and 50 cm around the splenic flexure there was no active inflammation, but there was chronic change with scarring. In the distal 30 cm of the colon there was colitis Mayo score 1 with erythema, and mild reduction in submucosal vascular pattern. Biopsies were taken every 10 cm throughout the colon to assess for any dysplasia. Pathology: DIAGNOSIS: 1-7. Colon, 70 cm, 60 cm, 50 cm, 40 cm, 30 cm, 20 cm and rectum, biopsies: - Features consistent with quiescent ulcerative colitis - Low grade dysplasia at 30 cm - Epithelial changes indefinite for dysplasia at 60 cm and rectum
42 Case 1 M.D. is a 31 year old male who presented with a three month history of right sided abdominal pain on Jan/2011. Weight loss, denied any melena or hematochezia. Subsequently developed constipation, obstructive symptoms.

43 Case 1 CT-scan showed an apple core obstruction in the ascending colon with severe proximal dilatation.
44 Case 1 Urgent OR with Dr. Cohen for a right hemicolectomy on January 27, Surgery report: An hard mass at the hepatic flexure and no obvious masses had seen in the remainder of his colon. Pathology:?????
45 Pathology : Case 1 5 cm diameter tumor, 6/51 positive lymph nodes. Low-grade colonic adenocarcinoma, pt4a pn2a (Stage IIIc); In addition Features of chronic colitis with focal changes indefinite for dysplasia at the distal margin (see additional information)
46 Surgery Pathology specimen chronic colitis with focal changes indefinite for dysplasia at the distal margin (see additional information) Low grade Adenocarcinoma. Mayo1 Mayo 0 Mayo 1
47 Colonoscopy Sep/2011 Mild inflammation distal to the anastomosis region Mayo1 With some atypia. Mayo 0 Mild Inflammation rectosigma with low grade dysplasia. Mayo 1
48 Case 1 Oncology stand point: completed adjuvant Chemotherapy with FOLFOX on the 17th of August FOLOFOX: 5-FU, leucovorin, and oxaliplatin No Metastatic disease per CT.
49 Case 1 RT. Hemicolectomy Carcinoma (Distal margin with chronic colitis +) Stage IIIc=T4a N2a Jan/2011 Mild Colitis Transverse, and recto sigma with Low grade dysplasia Colonoscopy Sep/2011 completed FOLFOX chemotherapy. 09/2011
50 What next? 27 y/o, who had been diagnosed with UC just post to RT hemicolectomy d/t advanced tumor. Residual colon with mild active disease and with low grade dysplasia at least in the rectum. Post chemotherapy.(folfox) What Next.Total proctocolectomy IPAA?
51 Case 1 RT.Hemicolectomy Carcinoma (Distal margin+) Stage IIIc=T4a N2a Jan/2011 Mild Colitis Transverse, and recto sigma with Low grade dysplasia Colonoscopy Sep/2011 completed FOLFOX chemotherapy. 09/2011 Colonoscopy 2012 Inactive disease with focal low grade dysplasia recrum Colonoscopy 12/2014 Inactive disease with focal low grade dysplasia in the rectum
52 What next? 31 y/o, who had been diagnosed with UC just post to RT hemicolectomy d/t advanced tumor 4 years ago. Residual colon with mild active disease and with low grade dysplasia at least in the rectum. Post chemotherapy.(folfox) Last colonoscopy- Inactive disease, Low grade dysplasia in the rectum What Next.Total proctocolectomy IPAA?
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Seventh Edition Staging 2017 Colorectum. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects
 Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects Patient Group Macroscopic examination Ileum Histology Colon/rectum Histology 1 INR Normal Acute and chronic
Supplemental Digital Content 1. Endoscopic and histolological findings in INR and FR study subjects Patient Group Macroscopic examination Ileum Histology Colon/rectum Histology 1 INR Normal Acute and chronic
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
AJCC Cancer Staging 8 th Edition
 AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
Small Intestine Cancer Early Detection, Diagnosis, and Staging
 Small Intestine Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
Small Intestine Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Colon and Rectum 5/1/14
 Collecting Cancer Data: Colon and Rectum 2013 2014 NAACCR Webinar Series May 1, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Colon and Rectum 2013 2014 NAACCR Webinar Series May 1, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה
 ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Preoperative Data Colorectal Cancer Database
 Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels.
 Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Listed below are some of the words that you might come across concerning diseases and conditions of the bowels. Abscess A localised collection of pus in a cavity that is formed by the decay of diseased
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]](/thumbs/82/86264030.jpg "Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]") Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
CELLULAR PATHOLOGY TURNAROUND TIMES
 Title: - Summary CELLULAR PATHOLOGY TURNAROUND TIMES These are average figures for some key specimens in days for the month of November 2016. The times include weekends when the laboratory is closed. The
Title: - Summary CELLULAR PATHOLOGY TURNAROUND TIMES These are average figures for some key specimens in days for the month of November 2016. The times include weekends when the laboratory is closed. The
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Polyps Adenomas Lipomas
 30 Chapter 2 CT Colonography Chapter 2 Polyps Adenomas Lipomas Case 8 Case 9 Case 10 Case 11 Case 12 Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Pseudopolyp Polyp after intravenous administration of
30 Chapter 2 CT Colonography Chapter 2 Polyps Adenomas Lipomas Case 8 Case 9 Case 10 Case 11 Case 12 Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Pseudopolyp Polyp after intravenous administration of
Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay
 1 Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay Abstract: The estate of a 60 year old male alleged negligence against a gastroenterologist in failing to properly evaluate
1 Physician s Cognitive and Communication Failures Result in Cancer Treatment Delay Abstract: The estate of a 60 year old male alleged negligence against a gastroenterologist in failing to properly evaluate
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING
 SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Outline. Colon and Rectal Cancers. Overview. Overview. Anatomic Distribution. Incidence and Mortality 12/12/2013
 Colon and Rectal Cancers FCDS 2013-2014 Educational Webcast Series December 12, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff 1 Outline Overview Incidence/Mortality/Survival Risk
Colon and Rectal Cancers FCDS 2013-2014 Educational Webcast Series December 12, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff 1 Outline Overview Incidence/Mortality/Survival Risk
Colon and Rectal Cancers. Outline. Overview 12/12/2013. FCDS Educational Webcast Series December 12, 2013
 Colon and Rectal Cancers FCDS 2013-2014 Educational Webcast Series December 12, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff 1 Outline Overview Incidence/Mortality/Survival Risk
Colon and Rectal Cancers FCDS 2013-2014 Educational Webcast Series December 12, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff 1 Outline Overview Incidence/Mortality/Survival Risk
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
THE INS & OUTS OF COLONOSCOPY
 THE INS & OUTS OF COLONOSCOPY INSERTION TIPS & FEATURES OF HIGH-QUALITY WITHDRAWAL C A M E R O N B E L L R O Y A L N O R T H S H O R E H O S P I T A L C H A I R, N E T I N A T I O N A L T C T L E A D WHY
THE INS & OUTS OF COLONOSCOPY INSERTION TIPS & FEATURES OF HIGH-QUALITY WITHDRAWAL C A M E R O N B E L L R O Y A L N O R T H S H O R E H O S P I T A L C H A I R, N E T I N A T I O N A L T C T L E A D WHY
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
Anaplastic A term used to describe cancer cells that divide rapidly and have little or no resemblance to normal cells.
 Oncology Terminology A Adenocarcinoma A cancerous tumor that arises in or resembles glandular tissue. Adjunct agent In cancer therapy, a drug or substance used in addition to the primary therapy. Adjuvant
Oncology Terminology A Adenocarcinoma A cancerous tumor that arises in or resembles glandular tissue. Adjunct agent In cancer therapy, a drug or substance used in addition to the primary therapy. Adjuvant
Overview. Collecting Cancer Data: Colon 11/5/2009. Collecting Cancer Data: NAACCR Webinar Series 1. Agenda NAACCR WEBINAR SERIES
 Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist
 ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
Caring for a Patient with Colorectal Cancer. Objectives. Poll question. UNC Cancer Network Presented on 10/15/18. For Educational Use Only 1
 Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN
 Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
Neoplasms of the Colon and of the Rectum
 Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Department of Surgery, Aizu Central Hospital, Fukushima
 Case Reports Resection of Asynchronous Quadruple Advanced Colonic Carcinomas Followed by Reconstruction with Ileal Interposition between the Transverse Colon and Rectum Sho Mineta 1, Kimiyoshi Shimanuki
Case Reports Resection of Asynchronous Quadruple Advanced Colonic Carcinomas Followed by Reconstruction with Ileal Interposition between the Transverse Colon and Rectum Sho Mineta 1, Kimiyoshi Shimanuki
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin
 The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
The Pathologist s Role in the Diagnosis and Management of Neoplasia in Barrett s Oesophagus Cian Muldoon, St. James s Hospital, Dublin 24.06.15 Norman Barrett Smiles [A brief digression - Chair becoming
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Colorectal cancer starts in the colon or rectum.
 The content of this booklet was adapted from content originally published by the National Cancer Institute. Colon Cancer Treatment (PDQ ) Patient Version. Updated December 7, 2017. https://www.cancer.gov/types/colorectal/patient/colon-treatment-pdq
The content of this booklet was adapted from content originally published by the National Cancer Institute. Colon Cancer Treatment (PDQ ) Patient Version. Updated December 7, 2017. https://www.cancer.gov/types/colorectal/patient/colon-treatment-pdq
Gastric (Stomach) Cancer
 Cancer") Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
High risk stage II colon cancer
 High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
High risk stage II colon cancer Joel Gingerich, MD, FRCPC Assistant Professor Medical Oncologist University of Manitoba CancerCare Manitoba Disclaimer No conflict of interests 16 October 2010 Overview
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Radiology of the abdomen Lecture -1-
 Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Radiology of the abdomen Lecture -1- Objectives To know radiology modalities used in abdomen imaging mainly GI tract. To know advantages and disadvantages of each modality. To know indications and contraindications
Stomach Cancer Early Detection, Diagnosis, and Staging
 Stomach Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
Stomach Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be
Stage: The Language of Cancer
 Stage: The Language of Cancer American Joint Committee on Cancer American College of Surgeons Chicago, IL Validating science. Improving patient care. No materials in this presentation may be repurposed
Stage: The Language of Cancer American Joint Committee on Cancer American College of Surgeons Chicago, IL Validating science. Improving patient care. No materials in this presentation may be repurposed
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Colorectal cancer Chapelle, J Clin Oncol, 2010
 Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Unexpected Findings at Endoscopy
 The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Rodger C. Haggitt Memorial Lecture
 The Rodger C. Haggitt Memorial Lecture I got an email on 4/22/14 from Hala El Zamaity inviting me to give this lecture and giving me this topic: The ever changing TNM classification and its implication
The Rodger C. Haggitt Memorial Lecture I got an email on 4/22/14 from Hala El Zamaity inviting me to give this lecture and giving me this topic: The ever changing TNM classification and its implication
Colon Cancer , The Patient Education Institute, Inc. oc Last reviewed: 05/17/2017 1
 Colon Cancer Introduction Colon cancer is fairly common. About 1 in 15 people develop colon cancer. Colon cancer can be a life threatening condition that affects the large intestine. However, if it is
Colon Cancer Introduction Colon cancer is fairly common. About 1 in 15 people develop colon cancer. Colon cancer can be a life threatening condition that affects the large intestine. However, if it is
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right?
 Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Guide to Colorectal Cancer
 Guide to Colorectal Cancer Comprehensive, oncologist-approved cancer information from the American Society of Clinical Oncology (ASCO) www.cancer.net Made available through: ABOUT ASCO The American Society
Guide to Colorectal Cancer Comprehensive, oncologist-approved cancer information from the American Society of Clinical Oncology (ASCO) www.cancer.net Made available through: ABOUT ASCO The American Society
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Terumitsu; Nagayasu, Takeshi
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation A rare case of segmental ulcerative Tominaga, Tetsuro; Nonaka, Takashi; Shuichi; Kunizaki, Masaki; Sumida, Terumitsu; Nagayasu, Takeshi Acta medica
NAOSITE: Nagasaki University's Ac Title Author(s) Citation A rare case of segmental ulcerative Tominaga, Tetsuro; Nonaka, Takashi; Shuichi; Kunizaki, Masaki; Sumida, Terumitsu; Nagayasu, Takeshi Acta medica
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia