What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you)
|
|
|
- Dylan Owens
- 5 years ago
- Views:
Transcription
1 What Every Pathologist Wants the GI Nurse to Know (and how you can help us help you) Jonathan N. Glickman MD PhD Director, GI Pathology, Caris Diagnostics, Newton, MA Associate Professor of Pathology, Harvard Medical School
2 Introduction OUTLINE Overview of Anatomic Pathology Workflow Procedures (i.e., what do pathologists do anyway?) Pathologist- Clinical Group Interactions Clinical and Endoscopic Information- the More the Better! Sample Pathology Cases
 Pathology residency GI pathology fellowship Staff pathologist, BWH")
3 A little about myself.. Washington University Medical School, MD PhD 1995 Brigham and Women s Hospital (BWH) Pathology residency GI pathology fellowship Staff pathologist, BWH and Children s Hospital Associate Professor of Pathology, Harvard Medical School Director of GI Pathology, Caris Diagnostics, Newton, MA
4 Caris Pathology Who are we? Three closely collaborating full-service laboratories (Irving, TX; Newton, MA; Phoenix, AZ) 16 GI pathology fellowship-trained physicians 13 additional pathologists with GI expertise and fellowship training in surgical pathology, cytopathology, or hematopathology. Over 20 institutions represented: University of Washington, Baylor College of Medicine, Beth Israel Deaconess Medical Center, Brigham and Women s Hospital, Cleveland Clinic, Dallas VA Medical School, Duke University, Georgetown University, Harvard Medical School, Indiana University, Johns Hopkins University, Mayo Clinic, M.D. Anderson Cancer Center, Memorial Sloan-Kettering Cancer Center, University of Cincinnati, University of Iowa, University of Kansas, University of Kentucky, University of Michigan, University of Nebraska Medical Center, University of Pittsburgh, University of Southern California, University of Texas
5 Pathology Practice Two basic venues for anatomic pathology practices Hospital based Non-hospital based (private lab/outpatient) Key differences Pathologist activities Types of specimens Nature of pathologist-clinician interactions Access to clinical and endoscopic information
6 Anatomic Pathology Laboratory- Workflow 1. Receipt and Accessioning - Patient identification - Documentation of clinical history and endoscopic findings 2. Gross examination and description of tissue 3. Tissue processing and embedding in paraffin 4. Sectioning/slide preparation and staining 5. Microscopic examination of slides 6. Preparation and release of pathology report

7 Review received paperwork Verify that specimens received match paperwork Verify patient info Correlate with preaccessioned cases Log into information system Accessioning

")
8 Gross Description and Tissue Submission Trained Pathology Assistant Review of paperwork, submitted clinical information Dictation Tissue sectioning (if necessary) Placement in cassettes


9 Tissue Processing/Embedding/Sectioning Good tissue processing and sectioning is paramount to a good consultation report Proper processing Additional fixation in formalin Progressive dehydration to allow paraffin permeation Tissue is embedded in paraffin blocks Paraffin saturation enables thin sections Acts a support medium Sectioned at 4-6 microns onto glass slides Technique matters!


10 Slide preparation and staining Taken through deparaffinization, rehydration, and drying steps Once rehydrated, slides are stained
11 Tissue Sectioning
12 Tissue Sectioning
13 Tissue Sectioning

14 Tissue Sectioning


15 Integration of all supplied information Formulation of diagnosis Microscopic examination
16 Quality Control Patient identification errors Accurate clinical information Specimen loss Specimen mix-up

17 Specimen labeling Please label clearly! Printed labels are even better!

18 What should a good GI biopsy pathology report do?
19 Final Diagnosis A summary medical interpretation based on the gross and microscopic findings Incorporates supplied clinical history and endoscopic information, results of prior pathology, etc. Standard terminology Classification systems Necessary for clear communication Must state all pertinent positive and negative findings relevant to diagnosis
20 Comment A narrative prominently placed in the pathology consultation report that addresses clinical/pathologic correlations, pertinent supportive evidence, prognostic information, references Answer the clinical question posed to the best of our ability Place histologic findings in clinical and endoscopic context Differential diagnosis, with preference if appropriate. Sufficient information to make meaningful treatment decisions Polyps- margins, high grade dysplasia Need for more tissue?
21 An Informative Pathology Report Differentiates normal from abnormal Willing to call a biopsy normal! Provides all pertinent positives/negatives H. pylori, granulomas, dysplasia Makes as specific a diagnosis as possible (etiologic/with attention to current disease classifications and terminology) Establishes a correlation between clinical and pathologic findings Doesn t leave the clinician hanging!
22 The more information, the better!
23 Endoscopic findings may (and often do) influence pathologic evaluation Availability of endoscopy report (even better, with images) Examples Polyp vs. flat mucosa Barrett's mucosa in esophagus Appearance of duodenum (normal vs. abnormal, for celiac disease) Severity and distribution of colitis

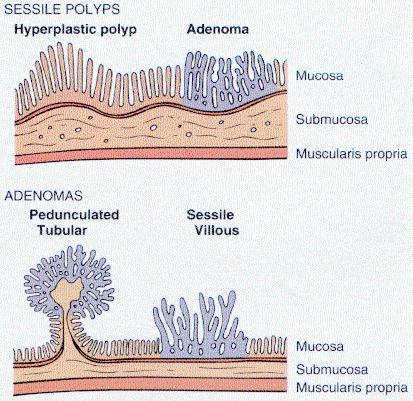
24 Colonic polyps Hyperplastic polyp Robbins & Cotran, 2005 Adenoma


25 Polyp mimics Polyp vs. flat mucosal biopsy Mucosal folds Submucosal lesions Lymphoid aggregates Deeper levels for small lesions


26 Polyp - additional levels Small polyp identified endoscopically Tubular adenoma only on deeper levels Altered surveillance interval Original Deeper

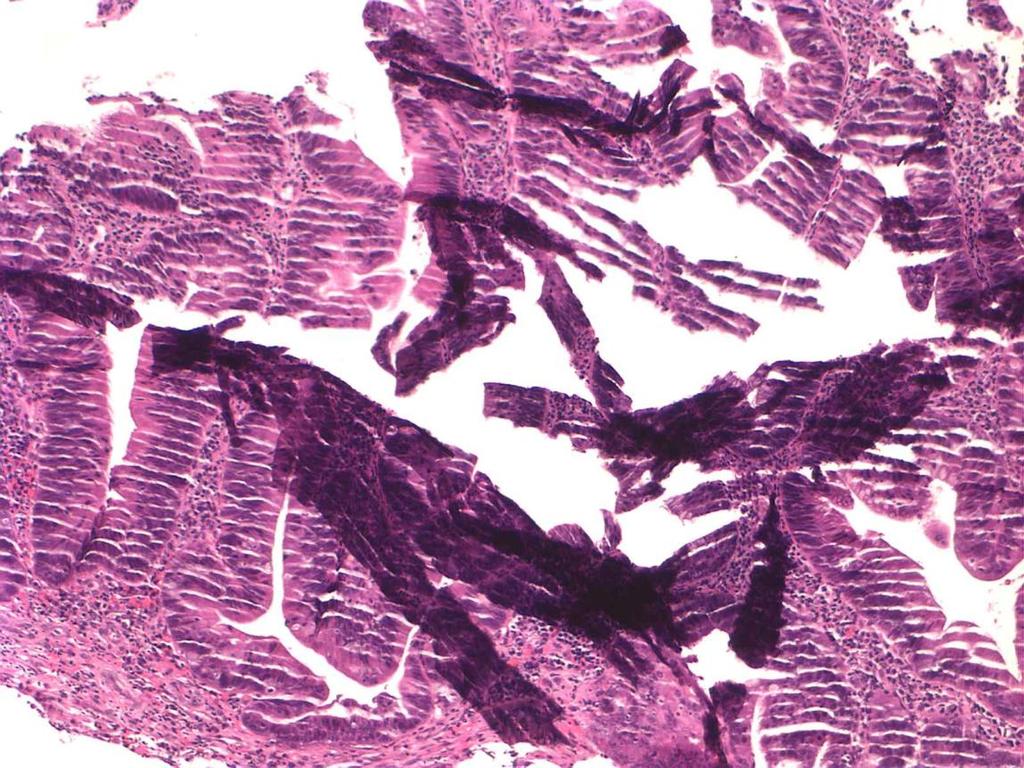
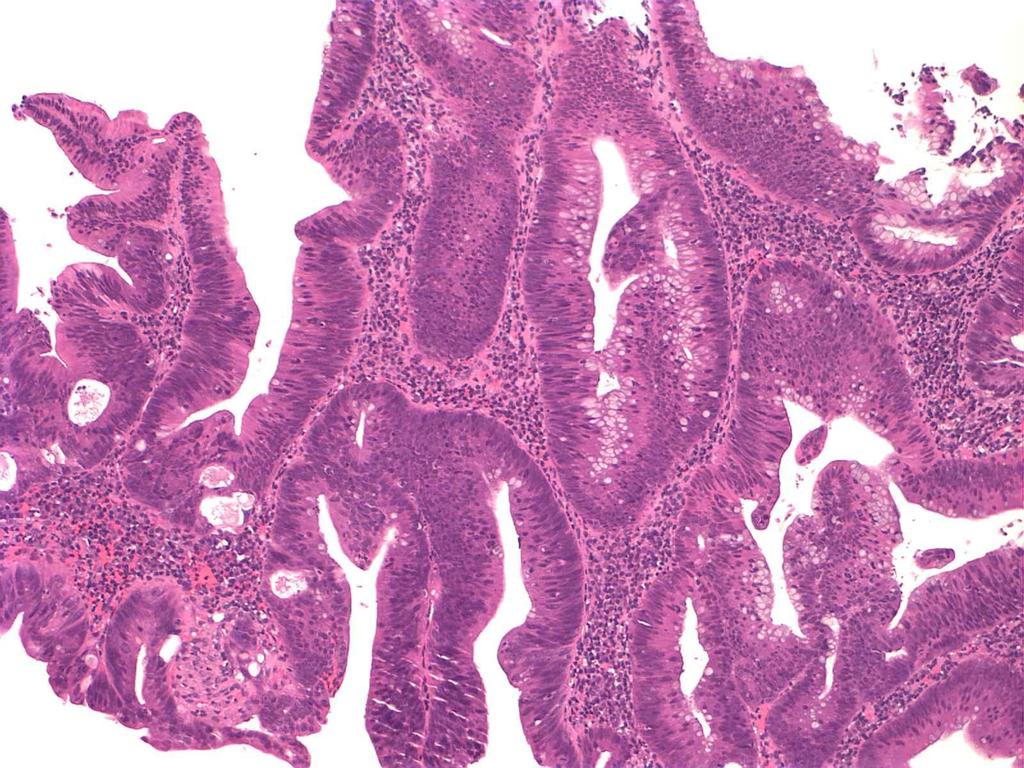
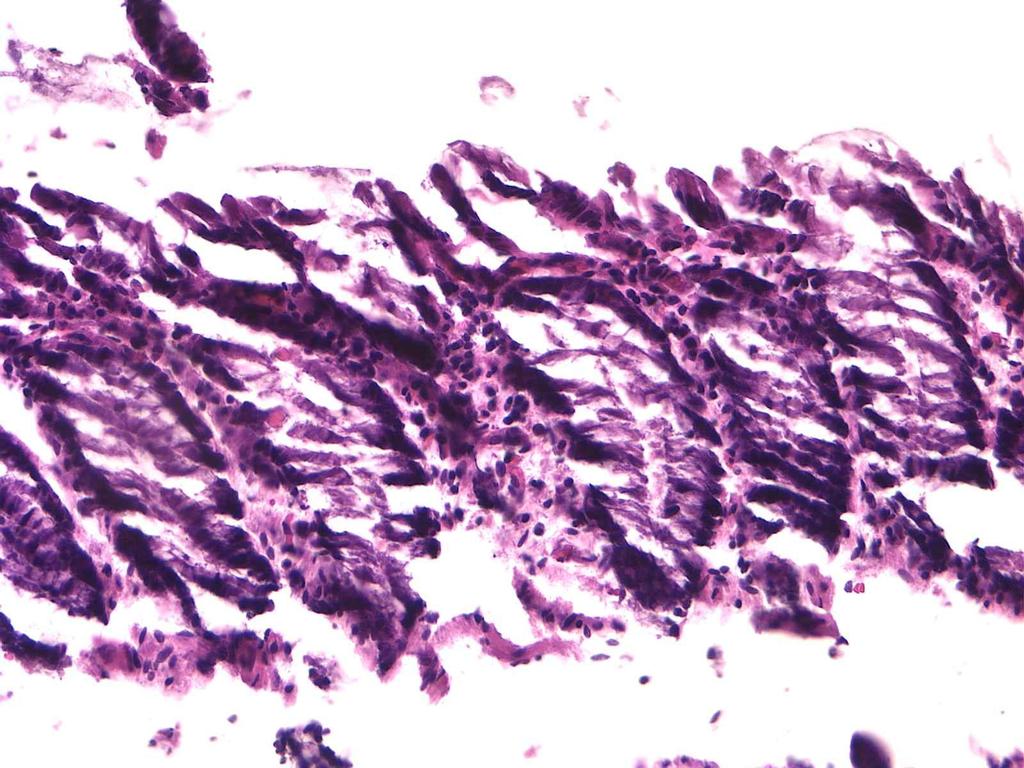
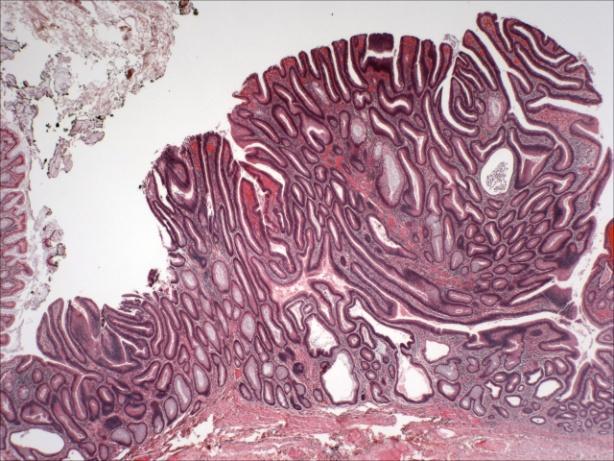
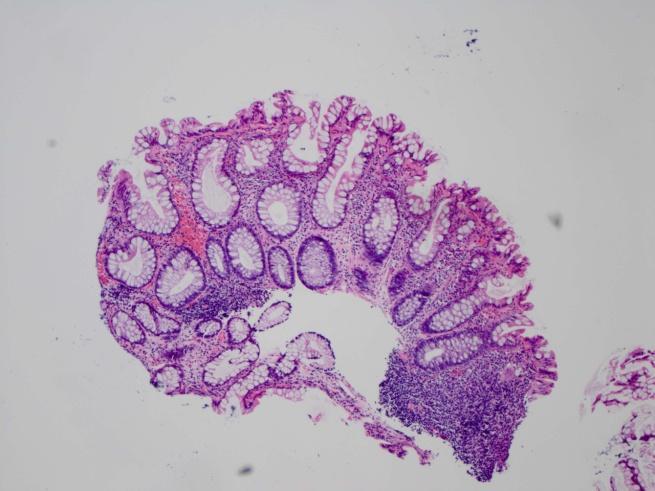
27 50 year-old woman with a 1.2 cm polyp in the right colon

28 Compared to hyperplastic polyps: Larger Sessile Right sided Endoscopically subtle: thickened fold Molecular abnormalities in DNA mismatch repair: microsatellite instability Sessile serrated adenoma
29 Newer polyp entities Many bland polyps previously thought to be hyperplastic polyps are actually pre-malignant lesions. Histologic difference between: large hyperplastic polyps traumatized hyperplastic polyps mixed hyperplastic-adenomatous polyps traditional serrated adenomas sessile serrated adenomas sessile serrated adenomas with dysplasia or carcinoma

")
")
30 Polyp Margins Cold (forceps) Hot (snare) Pedunculated Sessile



31 Distal esophagus biopsy Barrett s mucosa? Squamocolumnar mucosa with intestinal metaplasia? Comment: If this biopsy is derived from endoscopically abnormal mucosa in the tubular esophagus, then the presence of intestinal metaplasia fulfills the American College of Gastroenterology diagnostic criteria of Barrett s esophagus.



32 Barrett s esophagus- additional levels Patient history of heartburn Tongues of columnar mucosa Intestinal metaplasia only on deeper levels Patient now gets appropriate surveillance for Barrett s esophagus

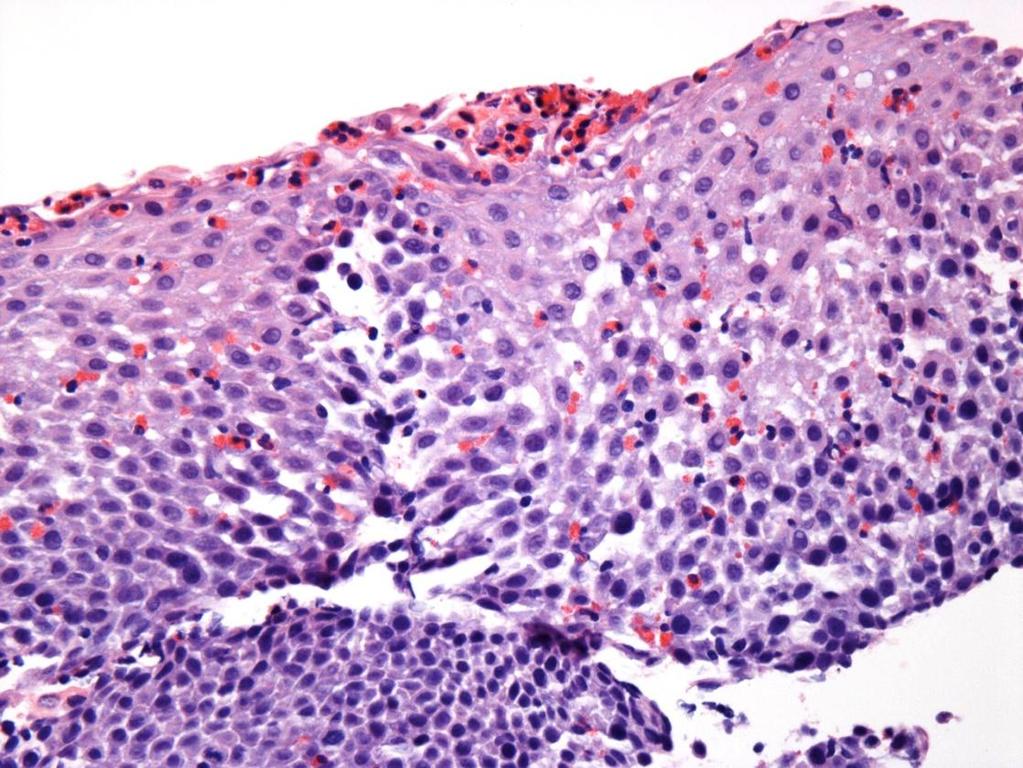
33 Barrett s esophagus no dysplasia


34 Barrett s esophagus Low grade dysplasia Barrett s esophagus High grade dysplasia
35 Location of Biopsies GI tract disorders in which distribution of disease is key to recognition IBD Esophagitis (reflux vs. eosinophilic) Barrett s esophagus Atrophic gastritis Knowing the location of biopsy is a key part of pathologic evaluation Avoid pooling biopsies in one jar!
36 Optimal/preferred endoscopic sampling IBD surveillance: Every 10 cm of involved colon, plus gross lesions. Duodenum (for celiac): Multiple (at least 2-3 fragments) Stomach: Antrum and corpus Esophagus: Distal third and middle third (to exclude eosinophilic esophagitis) Barrett s esophagus: every 2 cm
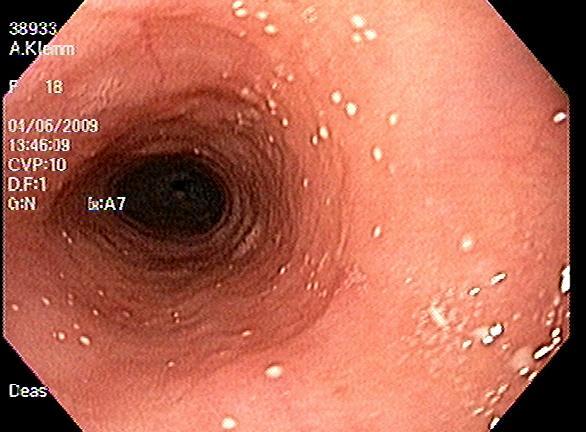

37 Eosinophilic esophagitis
38 Diagnosis and classification of IBD Often not possible based on histologic examination alone. Clinical context is critical Distinction from mimics. Confounding effects of prior medical therapy, surgery. Prior of prior biopsies and/or resections may be helpful.

39 Crohn s disease vs. UC Organ involvement Distribution Layers involved Microscopic

40 Subclassification of IBD Attempt to subclassify IBD whenever possible Clinical and endoscopic information always helpful Communication with gastroenterologist Sigmoid colon: chronic colitis
41 Recognition of histologic mimics; clinical history can distinguish 74 year-old woman presented with rectal bleeding Colonoscopy revealed rectal erythema and mucosal granularity
42 H Ulcerative colitis Patient G


43 Ulcerative colitis- key histologic features Architectural distortion Branching Irregularity Crypt atrophy Lymphoplasmacytic infiltrate Neutrophilic activity Normal

44 Diagnosis Benign Anorectal Mucosa with Evidence of Trauma/Prolapse

45 Some innocuous processes that can mimic IBD Mimics: Prolapse changes Healing ulcers Anastomotic site changes Chronic medication effect (e.g. NSAIDs) Chronic ischemia Patient was not labeled with a chronic colitis/proctitis or neoplasm Inappropriate treatment with immunosuppressive agents was avoided


46 Diverticular disease associated colitis
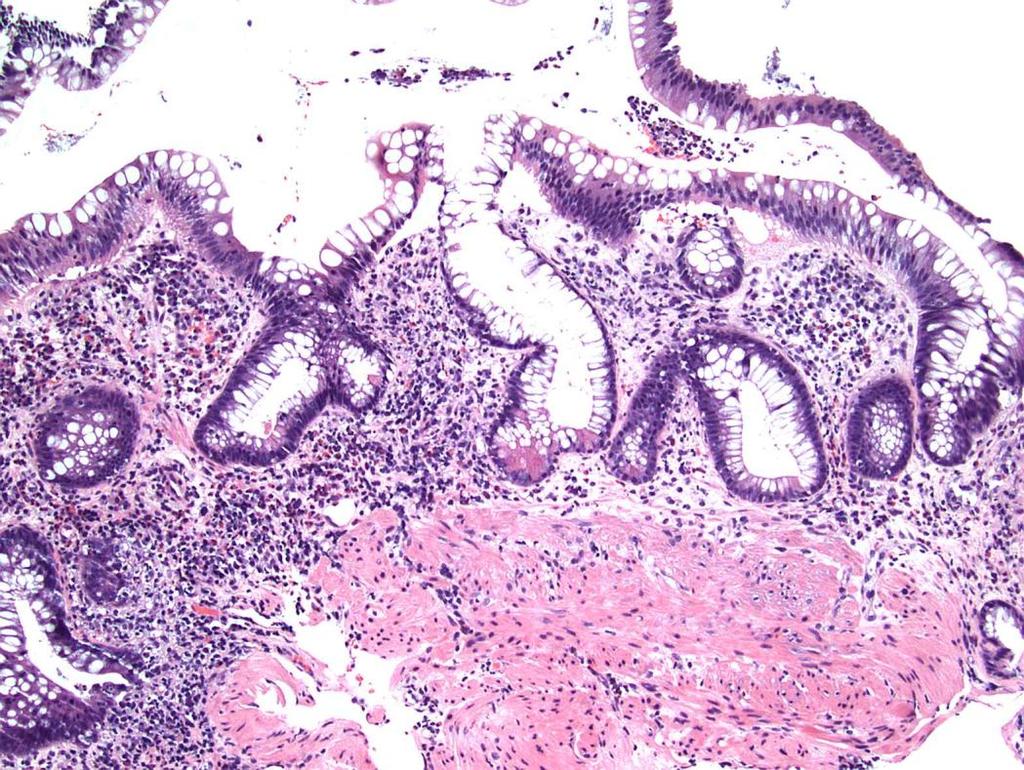
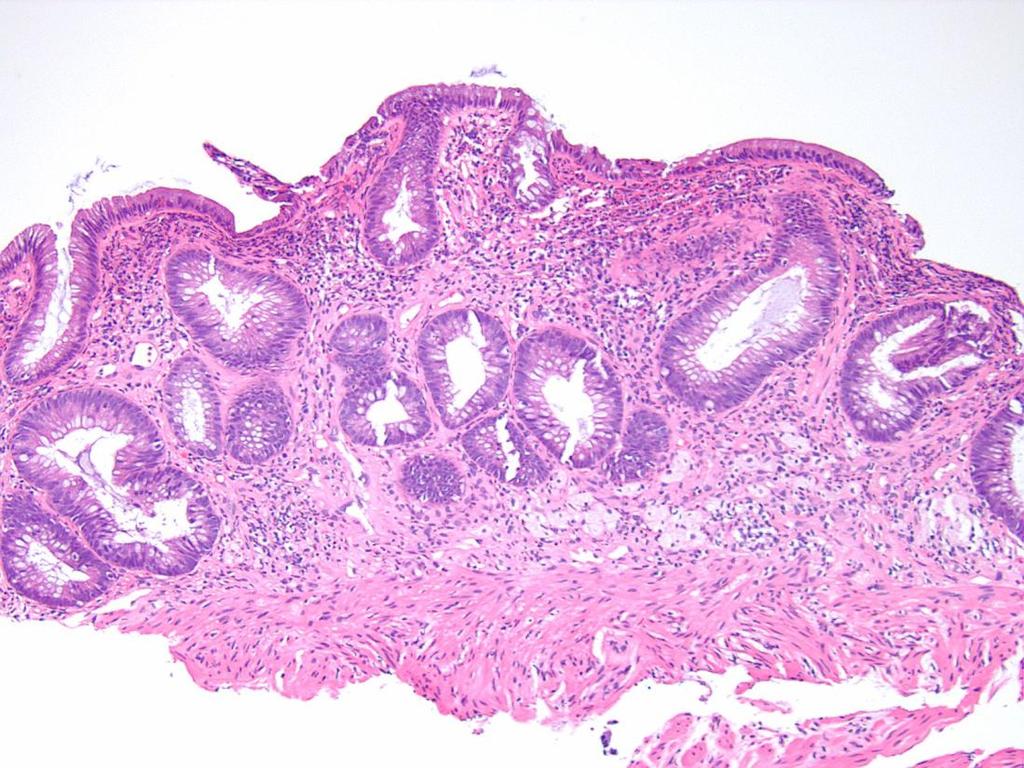
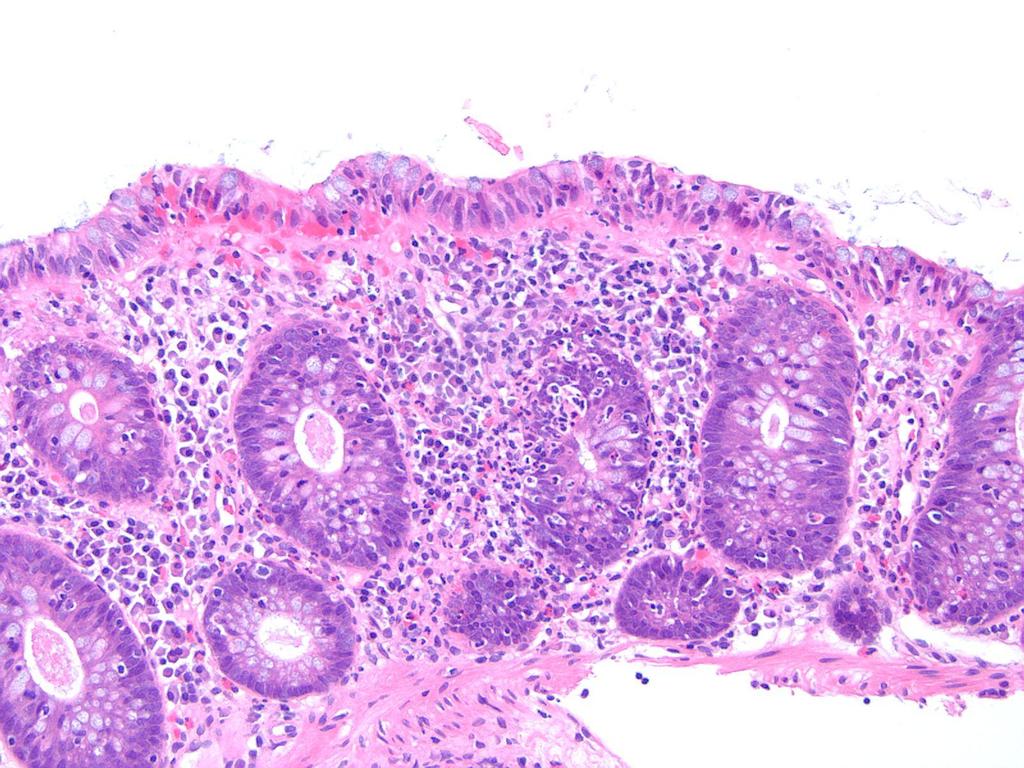
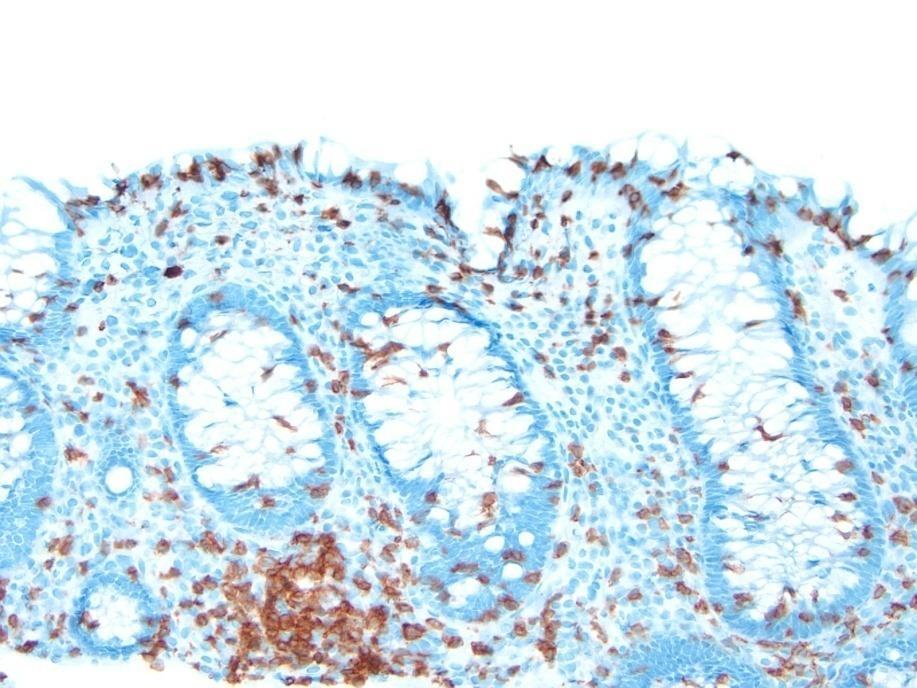
47 Missed diagnoses 18 year-old woman with a clinical history of ulcerative colitis Patient presents with diarrhea
48

49 Our diagnosis Lymphocytic Colitis Patient avoids potent immunosuppressive therapy, and does not require lifetime endoscopic surveillance
50 Conclusions Pathologic diagnosis does not occur in a vacuum High quality diagnosis (accurate and beneficial to patient care) results from a team-oriented approach. The more we know, the better!
51 THANK YOU
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Pitfalls in the Diagnosis of Inflammatory Bowel Disease
 Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Pitfalls in the Diagnosis of Inflammatory Bowel Disease Robert H Riddell MD Mt Sinai Hospital Toronto Prof of Lab. Medicine and Pathobiology University of Toronto Atypical gross / endoscopic distribution
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care
: Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
Quality ID #249 (NQF 1854): Barrett s Esophagus National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Transfer of Health Information and Interoperability 2019 COLLECTION TYPE:
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT.
 PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
PATHOLOGY OF NON NEOPLASTIC LESIONS OF THE UPPER GASTROINTESTINAL TRACT. OESOPHAGEAL LESIONS OESOPHAGITIS AND OTHER NON NEOPLASTIC DISORDERS Corrosive Gastroesophageal reflux (GERD), Pills, Acid intake,
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Kids Like to Break the Rules: Gastrointestinal Pathology in Children
 Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
Kids Like to Break the Rules: Gastrointestinal Pathology in Children Jeffrey Goldsmith MD Director of Surgical Pathology, Beth Israel Deaconess Medical Center; Consultant in Gastrointestinal Pathology,
IBD. Crohn s. Outline. Ulcerative colitis versus Crohn s disease: is biopsy useful? UC vs. Crohn s? Is it easy? Biopsy settings 21/07/2017 IBD
 Outline Ulcerative colitis versus Crohn s disease: is biopsy useful? Roger Feakins Colorectal biopsies Ileal and upper GI biopsies Special situations New techniques Summary Inflammatory bowel disease (IBD)
Outline Ulcerative colitis versus Crohn s disease: is biopsy useful? Roger Feakins Colorectal biopsies Ileal and upper GI biopsies Special situations New techniques Summary Inflammatory bowel disease (IBD)
EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018
 EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018 Please respond to the following items on a scale from 5 (highest) to 1 (lowest). The
EVALUATION FORM WSGNA 2018 Fall Conference Endoscopy for Malignant and Premalignant Lesions of the GI Tract 10/27/2018 Please respond to the following items on a scale from 5 (highest) to 1 (lowest). The
Oncologist-induced Disease of the GI tract: New Developments
 Oncologist-induced Disease of the GI tract: New Developments Jeffrey D Goldsmith, MD Children s Hospital Boston, Beth Israel Deaconess Medical Center, Harvard Medical School Boston, MA Everyone s on drugs
Oncologist-induced Disease of the GI tract: New Developments Jeffrey D Goldsmith, MD Children s Hospital Boston, Beth Israel Deaconess Medical Center, Harvard Medical School Boston, MA Everyone s on drugs
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions
 Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Barrett s Esophagus: Review of Diagnostic Issues and Pre- Neoplastic Lesions Robert Odze, MD, FRCPC Chief, Gastrointestinal Pathology Associate Professor of Pathology Brigham and Women s Hospital Harvard
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y.
 Digestive Endoscopy (2007) 19(s1):S145-S149. Auto-Fluorescence Imaging is useful to assess the activity of ulcerative colitis Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y. Auto-Fluorescence Imaging
Digestive Endoscopy (2007) 19(s1):S145-S149. Auto-Fluorescence Imaging is useful to assess the activity of ulcerative colitis Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y. Auto-Fluorescence Imaging
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
1. Esophageal diverticulum located above the upper esophageal sphincter is called
 Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
Test Bank for Robbins Basic Pathology 9th Edition by Kumar Link full download: http://testbankair.com/download/test-bank-for-robbins-basic-pathology-9thedition-by-kumar/ Chapter 14: Oral Cavity and Gastrointestinal
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST QUESTIONS. Ver. #
 SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
SAMs Guidelines DEVELOPING SELF-ASSESSMENT MODULES TEST Ver. #5-02.12.17 GUIDELINES FOR DEVELOPING SELF-ASSESSMENT MODULES TEST The USCAP is accredited by the American Board of Pathology (ABP) to offer
Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract
 Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract Alina M.Boeriu 1, Daniela E.Dobru 1, Simona Mocan 2 1) Department of Gastroenterology, University of Medicine and Pharmacy;
Magnifying Endoscopy and Chromoendoscopy of the Upper Gastrointestinal Tract Alina M.Boeriu 1, Daniela E.Dobru 1, Simona Mocan 2 1) Department of Gastroenterology, University of Medicine and Pharmacy;
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
What is your diagnosis? a. Lymphocytic colitis. b. Collagenous colitis. c. Common variable immunodeficiency (CVID) associated colitis
 associated colitis") Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Case History A 24 year old male presented with fatigue, fever, watery diarrhea, and a cough with sputum production for the past three weeks. His past medical history was significant for recurrent bouts
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Outcome High Priority
 MEASURE TYPE: Outcome High Priority") Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Preventive Care 2019 COLLECTION TYPE: MIPS CLINICAL QUALITY
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Preventive Care 2019 COLLECTION TYPE: MIPS CLINICAL QUALITY
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
SAM PROVIDER TOOLKIT
 THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
THE AMERICAN BOARD OF PATHOLOGY Maintenance of Certification (MOC) Program SAM PROVIDER TOOLKIT Developing Self-Assessment Modules (SAMs) www.abpath.org The American Board of Pathology (ABP) approves educational
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations
 Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
Common Inflammatory Gastrointestinal Disorders: Endoscopic and Pathologic Correlations Nicole C. Panarelli, M.D. Attending Pathologist Montefiore Medical Center Associate Professor of Pathology - Albert
하부위장관비종양성질환의 감별진단 주미인제의대일산백병원
 하부위장관비종양성질환의 감별진단 주미인제의대일산백병원 Solutions for diagnostic problems in Colitis : Please ask yourself five questions Normal or Inflamed? Acute or Chronic? IBD or Other chronic colitis? Ulcerative colitis or
하부위장관비종양성질환의 감별진단 주미인제의대일산백병원 Solutions for diagnostic problems in Colitis : Please ask yourself five questions Normal or Inflamed? Acute or Chronic? IBD or Other chronic colitis? Ulcerative colitis or
Small Bowel Cases. Introduction. Introduction, Continued 12/7/2011. Lesions Found on endoscopic biopsies Just Like Signing Out
 Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Information Technology Solutions
 2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה
 ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
ד"ר דוד ירדני המכון לגסטרואנטרולוגיה ומחלות כבד מרכז רפואי סורוקה Presentaion: S.A is 38 years old. Referred for rectal bleeding investigation. Describes several occasions of bleeding and abdominal pain.
Gastric atrophy: use of OLGA staging system in practice
 Gastroenterology and Hepatology From Bed to Bench. 2016 RIGLD, Research Institute for Gastroenterology and Liver Diseases ORIGINAL ARTICLE Gastric atrophy: use of OLGA staging system in practice Mahsa
Gastroenterology and Hepatology From Bed to Bench. 2016 RIGLD, Research Institute for Gastroenterology and Liver Diseases ORIGINAL ARTICLE Gastric atrophy: use of OLGA staging system in practice Mahsa
SAGES 2019 Flexible Endoscopy Course for Fellows
 Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus
 New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
New Developments in the Endoscopic Diagnosis and Management of Barrett s Esophagus Prateek Sharma, MD Key Clinical Management Points: Endoscopic recognition of a columnar lined distal esophagus is crucial
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Billing Guideline. Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16
 Effective Date: 1/1/14 Last revision effective 4/16") Billing Guideline Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16 Florida Hospital Care Advantage plans include full coverage of in-network
Billing Guideline Subject: Colorectal Cancer Screening Exams (Invasive Procedures) Effective Date: 1/1/14 Last revision effective 4/16 Florida Hospital Care Advantage plans include full coverage of in-network
Chapter 12: Training in Pathology. DDSEP Chapter 13: Question 19
 DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
DDSEP Chapter 13: Question 19 A 70 year-old male with a history of celiac disease diagnosed in his forties reports abdominal pain, dark stools, and 20-pound weight loss. He reports complete compliance
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
FINAL HISTOLOGICAL DIAGNOSIS: Villo-adenomatous polyp with in-situ-carcinomatous foci (involving both adenomatous and villous component).
.") SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
Vital staining and Barrett s esophagus
 Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Marcia Irene Canto, MD, MHS Baltimore, Maryland Vital staining or chromoendoscopy refers to staining of endoscopic tissue or topical application of chemical stains or pigments to alter tissue appearances
Patho Basic Chronic Inflammatory Bowel Diseases. Jürg Vosbeck Pathology
 Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Patho Basic Chronic Inflammatory Bowel Diseases Jürg Vosbeck Pathology General Group of chronic relapsing diseases with chronic bloody or watery diarrhea Usually ulcerative colitis (UC) or Crohn s disease
Barrett s Esophagus Burn, Resect, Freeze, or Just Watch Strategies for Evaluation and Surveillance of Barrett s Amitabh Chak, MD OBJECTIVES: NOTES:
 Speaker 1 Barrett s Esophagus Burn, Resect, Freeze, or Just Watch Strategies for Evaluation and Surveillance of Barrett s Amitabh Chak, MD 1. List the epidemiology of Barrett s esophagus. 2. Review the
Speaker 1 Barrett s Esophagus Burn, Resect, Freeze, or Just Watch Strategies for Evaluation and Surveillance of Barrett s Amitabh Chak, MD 1. List the epidemiology of Barrett s esophagus. 2. Review the
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Barrett s Esophagus. lining of the lower esophagus that bears his name (i.e., Barrett's esophagus). We now
. We now") Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Shamika Johnson Anatomy & Physiology 206 April 20, 2010 Barrett s Esophagus What is Barrett s Esophagus? Norman Barrett was a pathologist. In 1950, he described an abnormality in the lining of the lower
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD)
 & Endoscopic Submucosal Dissection (ESD)") Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Relative risk of dysplasia for patients with intestinal metaplasia in the distal oesophagus and in the gastric cardia
 Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Gut 2000;46:9 13 9 PAPERS Division of Gastroenterology, University of Kansas, VA Medical Center, Kansas City, Missouri, USA P Sharma A P Weston Department of Pathology, VA Medical Center, Kansas M Topalovski
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Clinicopathological Characteristics of Superficial Type
 Diagnostic and Therapeutic Endoscopy, 1995, Vol. 2, pp. 99-105 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
Diagnostic and Therapeutic Endoscopy, 1995, Vol. 2, pp. 99-105 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
Gastroenterology Fellowship Program
 Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
Gastroenterology Fellowship Program Outpatient Clinical Rotations I. Overview A. Three Year Continuity Clinic Experience All gastroenterology fellows will be required to have a ½ day continuity clinic
Sessile Serrated Polyps
 Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Lymphocytic and Collagenous Colitis: Epidemiologic Differences and Similarities
 Dig Dis Sci (2013) 58:2970 2975 DOI 10.1007/s10620-013-2718-6 ORIGINAL ARTICLE Lymphocytic and Collagenous Colitis: Epidemiologic Differences and Similarities Amnon Sonnenberg Robert M. Genta Received:
Dig Dis Sci (2013) 58:2970 2975 DOI 10.1007/s10620-013-2718-6 ORIGINAL ARTICLE Lymphocytic and Collagenous Colitis: Epidemiologic Differences and Similarities Amnon Sonnenberg Robert M. Genta Received:
Colonoscopy MM /01/2010. PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
 of Service: Outpatient") Colonoscopy Policy Number: Original Effective Date: MM.12.003 12/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
Colonoscopy Policy Number: Original Effective Date: MM.12.003 12/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Duodenal adenomas Management. Dr Stratis Alexandridis Consultant Gastroenterologist BRI
 Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy
 Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy M. Perdiki 2, G. Bamias 1, D. Pouloudi 2, H. Gogas 3, I. Delladetsima 2 1 Academic Dpt. of Gastroenterology,
Histological and immunological characteristics of colitis associated with anti-ctla 4 antibody therapy M. Perdiki 2, G. Bamias 1, D. Pouloudi 2, H. Gogas 3, I. Delladetsima 2 1 Academic Dpt. of Gastroenterology,
ACG Clinical Guideline: Colorectal Cancer Screening
 ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
HISTOPATHOLOGICAL STUDY OF ENDOSCOPIC BIOPSIES OF STOMACH
 HISTOPATHOLOGICAL STUDY OF ENDOSCOPIC BIOPSIES OF STOMACH Pages with reference to book, From 177 To 179 Javed Iqbal Kazi, Syed Mahmood Alam ( Departments of Pathology, Jinnah Postgraduate Medical Centre,
HISTOPATHOLOGICAL STUDY OF ENDOSCOPIC BIOPSIES OF STOMACH Pages with reference to book, From 177 To 179 Javed Iqbal Kazi, Syed Mahmood Alam ( Departments of Pathology, Jinnah Postgraduate Medical Centre,
Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum
 Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful in characterizing esophageal location
 Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
Diseases of the Esophagus (2005) 18, 87 92 2005 ISDE Blackwell Publishing, Ltd. Original article Gland ducts and multilayered epithelium in mucosal biopsies from gastroesophageal-junction region are useful
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of the distal esophagus, gastroesophageal junction and gastric cardia?
 Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Diseases of the Esophagus (2007) 20, 36 41 DOI: 10.1111/j.1442-2050.2007.00638.x Blackwell Publishing Asia Original article Is intestinal metaplasia a necessary precursor lesion for adenocarcinomas of
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
What do we need for diagnosis of IBD
 What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
What do we need for diagnosis of IBD Kaichun Wu Dept. of Gastroenterology, Xijing Hospital Fourth Military Medical University Xi an an,, China In China UC 11.6/10 5,CD 1.4/10 5 Major cause of chronic diarrhea
11/1/2017. Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota. Cerilli & Greenson
 Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota Acute infectious (self-limited) colitis Focal active colitis Pseudomembranous colitis Ischemic colitis Collagenous
Tetyana Mettler, MD Department of Laboratory Medicine and Pathology University of Minnesota Acute infectious (self-limited) colitis Focal active colitis Pseudomembranous colitis Ischemic colitis Collagenous
A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue
 A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue UCSF Liver and Gastrointestinal Pathology Update Sept. 4, 2009 How to Go Wrong When Evaluating Small Bowel Biopsies, Based on
A Practical Approach to Small Bowel Biopsies: All that flattens is not sprue UCSF Liver and Gastrointestinal Pathology Update Sept. 4, 2009 How to Go Wrong When Evaluating Small Bowel Biopsies, Based on
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Do any benign polyps require an operation?
 Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday