Treatment strategy of metastatic rectal cancer
|
|
|
- Geoffrey Charles
- 5 years ago
- Views:
Transcription

1 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014
2 Colorectal cancer is the third most frequent cancer in the western world 25% of patients have liver metastases at the time of diagnosis 25% will develop liver metastases during the course of the disease Two thirds of patients with liver metastases will die of their liver metastases
3 Only 15 years ago A patient suffering from a colorectal cancer with synchronous liver metastases would have a resection of the primary tumour followed by chemotherapy with 5- Fu / leucovorine and in case of good response (16%) a resection of the liver metastases
4 What is new? New chemotherapeutic agents with a high response rate Effective pelvic radiochemotherapy Better MRI, CT scan and echoendoscopy Precise rectal surgery with mesorectal excision Safe R0 liver surgery Portal vein embolisation and radiofrequency ablation However, with all these new tools.. How to use them and to choose the best strategy for a given patient?
5 Three approaches may be applied The classical staged The simultaneous approach.but The liver-first approach or reverse strategy We want to increase the number of patients treated with a curative intent è the aim is the long-term survival!
6 Primary first when Threat of large bowel occlusion The patient is unable to withstand a strong chemotherapy (side effects++) A large rectal tumour with little metastatic disease in the liver A probably perforated primary (e.g. fistula into the small bowel) with fever


7 54 year-old man T4 symptomatic rectal cancer with small amount of liver cancer è Best treated by pelvic radiotherapy followed by rectal surgery
8 New thinking For the 25% of the patients who have synchronous liver metastases è systemic disease at diagnosis Complete synchronous resection (primary and liver metastases rarely possible) Goat-cabbage-wolf situation: While taking care of the colon the liver disease will progress neo-adjuvant rectal radiochemotherapy is ineffective on the liver Optimal liver chemotherapy too radio-sensitizing
9 Our approach: liver first
10 Our approach: Liver-oriented chemotherapy- first Team work!
11 Liver (oriented chemo-) first For whom? 1. No occlusion 2. Fit enough to support side effects of chemotherapy 3. R0 resection(s) at all sites whatever the number of surgical procedures used to reach the goal
12 How did this approach become ethically possible? New agents used in new chemotherapy combinations è response rate from 16% to 80% è liver surgery has become a low risk procedure
13 Only possible with new chemotherapeutic agents! First Line Chemotherapy in Metastatic CRC: evolution of response rate and median survival BSC FU/FA mayo Seium Y et al. Ann Oncology 2005; 16: Bevacizumab (Avastin) Cetuximab (Erbitux) FU/LOHP FOLFIRI Folfox+Ab Oxaliplatin and Irinotecan
14 Influence of preoperative chemotherapy on the risk associated to major hepatectomy for CRLM Influence of the number of cycles of chemotherapy on the percentage of postoperative morbidity Karoui M. et al. Ann Surg 2006; 243: 1-7
15 Implications for clinical practice I Patients should be evaluated by experienced colorectal and liver surgeons and oncologists before starting therapy to avoid unduly prolonged treatment. Radiological imaging of the highest quality should be obtained at the beginning and at the latest after 3 cycles of chemo, as well as the CEA levels.




16 With this level of sophistication, traditional CT imaging is insufficient! After chemotherapy rely on MRI with hepato-specific contrast
17 Implications for clinical practice II Go to surgery as soon as the CRLM are resectable with a decrease of the CEA (usually 3 cycles of chemo are enough!). Do not give Avastin in the last 6 weeks before surgery (cave: perforation or poor cicatrization)

18 Mrs Y.R. 38 year-old, low rectal cancer T3 N1, CEA 525, one pulmonary nodule: CT

19 OCX chemo: CT after OCX 01/2004 liver firstè pelvic Rxthè LARè Lung surgery

20 Last CT scan: she died of recurrence after 7 years.after 7 surgical procedures. IV I
21 The «ideal concept» of the reverse strategy Very efficient neoadjuvant chemotherapy è short and strong! Followed 3 weeks later by a RO resection of the liver metastases And 4 weeks later by colorectal surgery or first pelvic radiochemotherapy when needed Adjuvant chemotherapy
22 Chemotherapy first in resectable disease Is it just a waste of time? Are we decreasing the chance for a patient with resectable disease to be cured?
23 Overall survival after resection of multiple liver metastases (>4) according to chemotherapy response (%) % Responding : % Stabilization : 39 Progression : % Log Rank: p< % 44% 12% 37% 30% 8% Years Update: Adam R et al. Ann Surg 2004; 240:
24 Pathological response to preoperative chemotherapy: a new outcome end point after resection of hepatic colorectal metastases. 305 patients 25 with complete histological response (8.1%) 5-year overall survival 75% Blazer DG et al., JCO 2008
25 Liver surgery has become a low risk procedure at some conditions!

26 Contribution of «pro-generative» strategies Multi Unilobar Multi Bilobar Multi Bilobar Remnant Liver<30% 3 nod. 30 mm >3 nod >30 mm chemo +++ <40% Portal Embolization Portal embolization + Percutaneous RxF By courtesy of René Adam 2-Stage Hepatectomy

27 Use of transplantation techniques in liver resections for cancer In situ split Reverse in situ split for extended right resections, without liver clamping nor blood transfusions
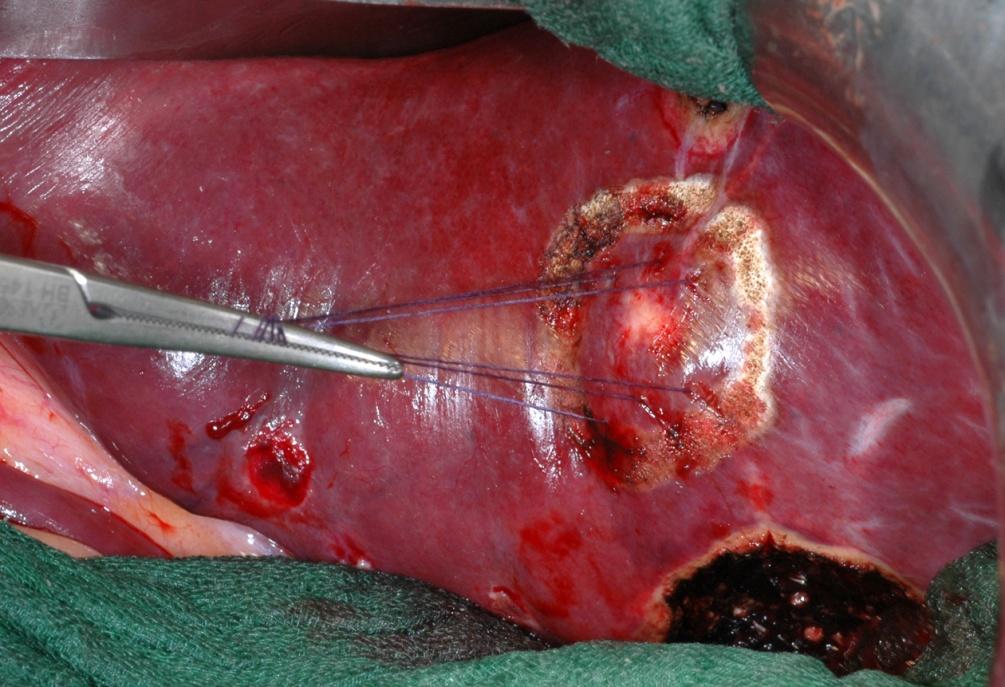
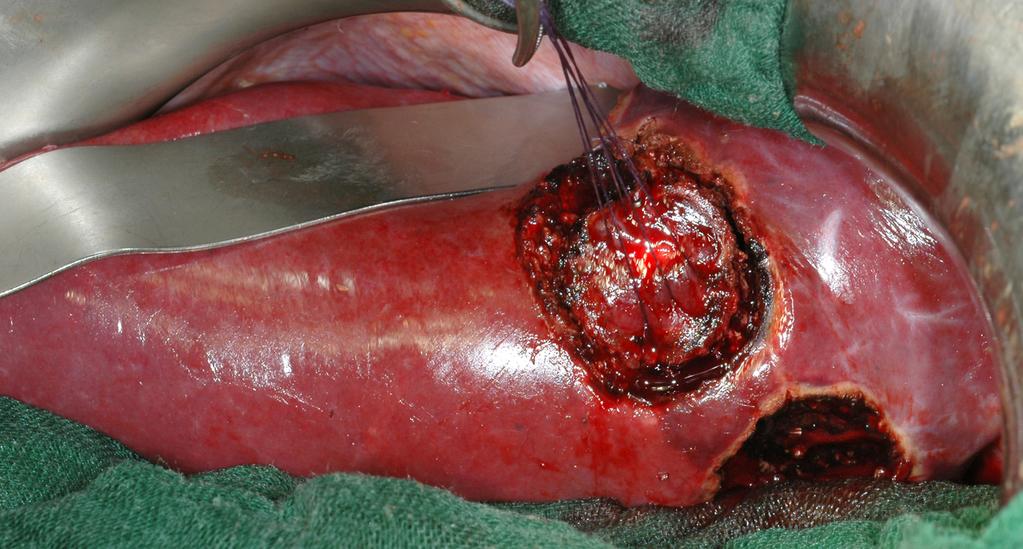

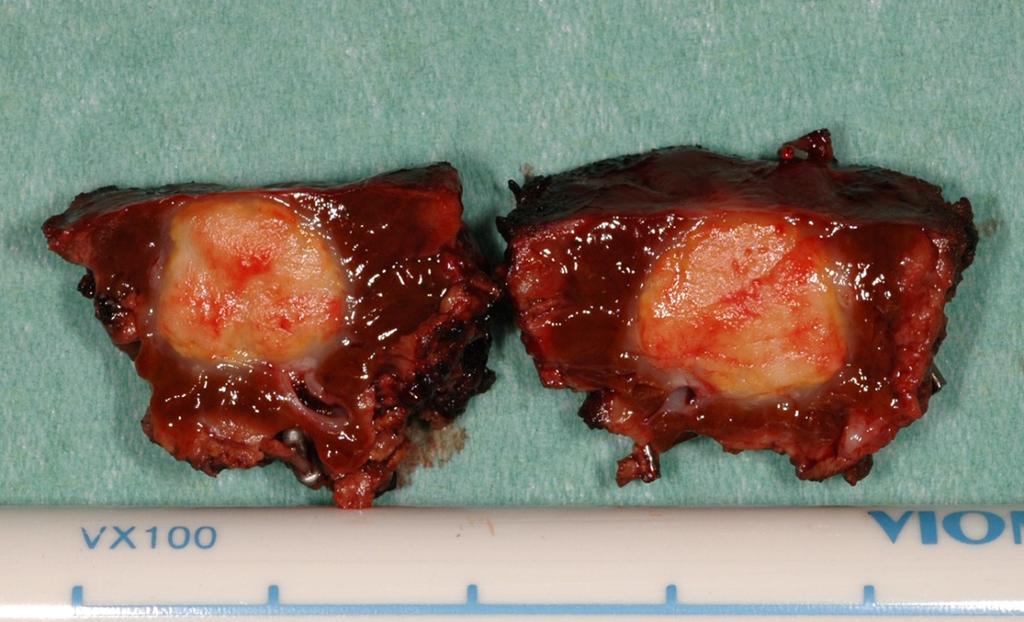
28 Conservative radical metastasectomy: the sling technique

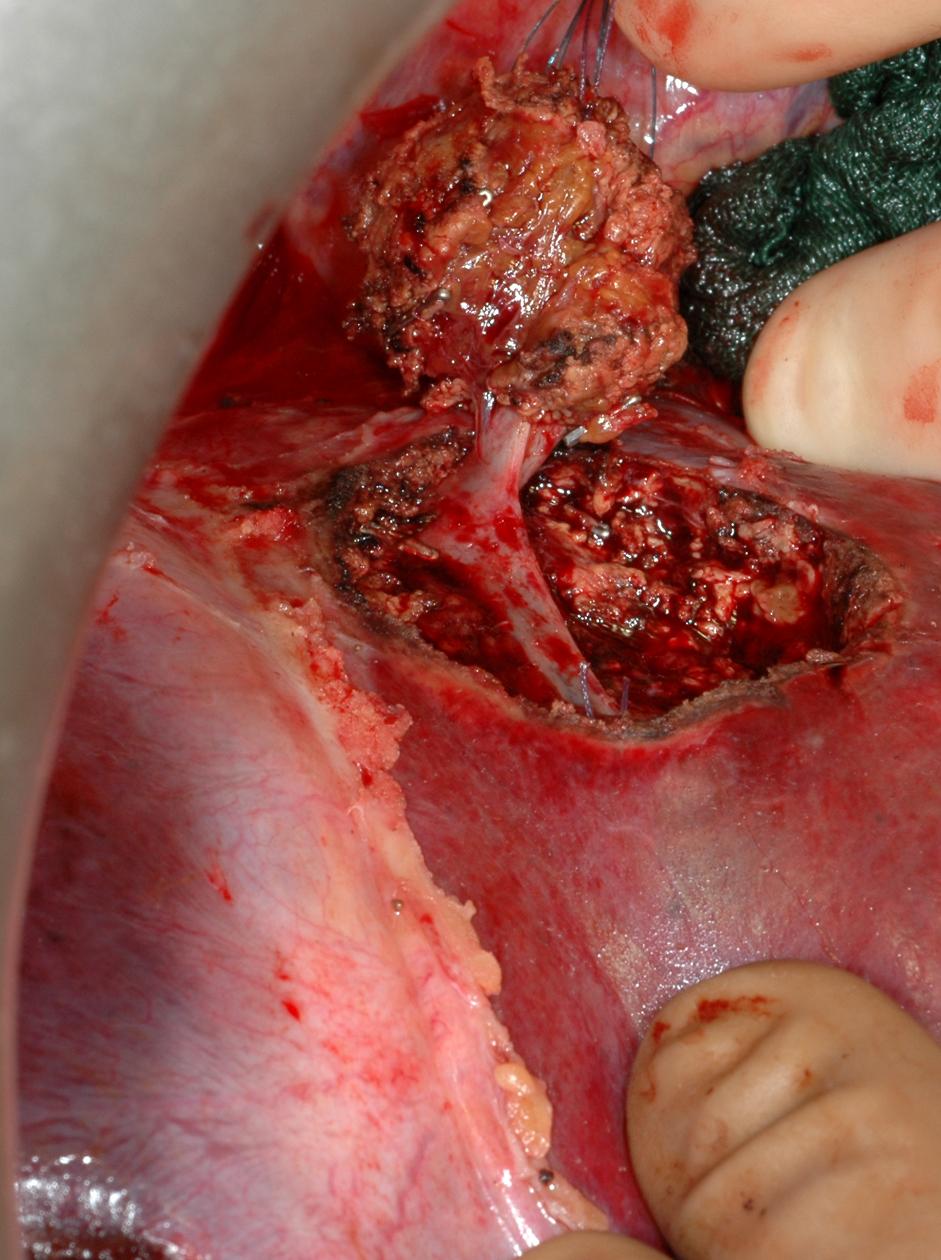
29 Depth control by US
30 Liver surgery: a low risk procedure Since 1991, liver surgery at the University Hospitals of Geneva (prospective database). 8 deaths out of 1012 hepatectomies è mortality of 0,8% 450 hepatectomies were major (45%) 65% of hepatectomies without blood transfusion Kooby DA et al. Influence of transfusions on perioperative and long-term outcome in patients following hepatic resection for colorectal metastases. Ann Surg 2003; 237:
31 Rationale of the reverse approach Colorectal surgery in real life
32 Morbidity and anastomotic leakage of colorectal surgery Authors Journal and year of p. Patients Mortality Morbidity Anastomotic leak G.Mantion Y. Panis Survey AFC Low rectum = % 2.5% 38.3% 43% 5% colon 11% rectum Matthiessen P. Colorectal disease rectum 2.1%? 12% Lipska MG ANZ J Surg colon and rectum 3.7%? 6.5% Chiappa A J Surg Oncol rectum 0% 39.4% 12% Tran CL Am J Surg patients rectum 0% 52% 17% abcess and fistula

33 Ann Surg 2011; 254:
34
35 Preoperative versus postoperative chemoradiotherapy for rectal cancer 843 patients randomly assigned to receive: preoperative RxChemotherapy n = 421 patients Postoperative complications 36% postoperative RxChemotherapy n = 402 patients Postoperative complications 34% Received full dose of radiotherapy N = 380 patients (92%) Received full dose of chemotherapy N = 369 patients (89%) Received full dose of radiotherapy N = 206 patients (54%) Received full dose of chemotherapy N = 193 patients (50%) Local relapse 6% Local relapse 13% Sauer R. et German Rectal Cancer Study Group NEJM 2004; 351:
36 Neoadjuvant chemotherapy Increases the resectability rate Allows to spare liver parenchyma May select responders versus non responders Probably (?) increases the long-term survival after CRLM resection Provided that the patient can have it!
37 Illustration of the reverse approach by our first case
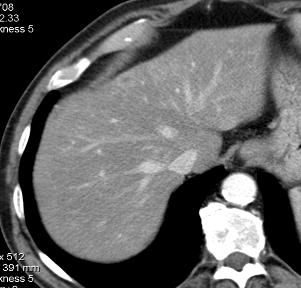
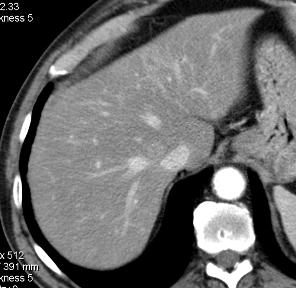
38 Reverse management of CRLM Case 1 Mrs R. 54 year-old Consultation for diarrhea Colonoscopy: adenocarcinoma at 8 cm from the anal margin, (T3 echoendoscopy) CEA 247 CTscan : 3 liver metastases CRS: 4



39 Reverse management of CRLM Case 1 Mrs R. 54 year-old before chemotherapy CT scan



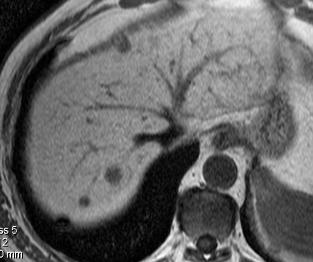
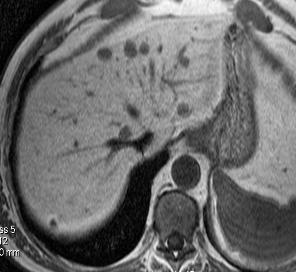
40 Reverse management of CRLM Case 1 Mrs R. 54 year-old After OCFL chemotherapy è Almost no tumour, è No rectal symptoms
41 Reverse management of CRLM Case 1 Mrs R. 54 year-old è OCFL 4 months left lobectomy, resection of segment IVa, atypical resection segments VI- VII Pelvic radiotherapy from to 4.08 (39Gy) Low anterior abdominal resection
 Rectum Ulcerated scar lesion with")

42 Histology Liver metastases mostly scar tissue with viable tumor cells in the periphery (1/3) Rectum Ulcerated scar lesion with microscopic island of residual adenocarcinoma and one focus of perineural invasion Follow up No evidence of recurrence after > 13 years
43 Results of reverse strategy using chemotherapy first, liver resection second primary tumor resection third 58 patients with non obstructive CRC, 50% rectal tumor, 50% initially non resectable Median number of CRM was 6 (mean 7.2) (2-21) Median size 6 cm (1-14) Bilobar in 70%, 11% had lung metastases Fong clinical risk score 3 to 5 (mean 3.7) Mentha G. et al. Brit J. Surg 2006; 93:
44 Clinical risk score = a scale with 5 criteria Positive lymph node of the primary Disease-free interval < 12 months (primary to CRM) Number of CRM > 1 Preoperative CEA level > 200 ng/ml Size of the largest CRM > 5 cm Fong Y. Ann Surg 1999; 230: 309 (1001 resected patients) With CRS of 3 or more 40% Mala T et al. World J Surg 2002; 26:
 had no resection è 6 deaths < 12")
45 50 patients (86%) who completed the programme 62% 48% 13 lived > 5 years 8 out of 50 patients (14%) had no resection è 6 deaths < 12 months
46 The «liver first approach» High-impact chemotherapy followed by resection of liver metastases before removal of the primary tumour seems to be associated with an increased rate of curative resection and improved long-term survival without detrimental effect on the evolution of the primary when a precise schedule is respected. Mentha G. et al Br J Surg 2006; 93: Mentha G. et al Dig Surg 2008; 25:
47 Lessons we have learned Some patients are more suitable than others and this you will see on the colorectal disease These patients are very sick and disease is likely to recur. Thing about it from the beginning (conservative radical hepatectomies) If you have a chance to cure, it depends on «perfection» for all the steps (chemotherapy, liver surgery, colorectal surgery).
48 Conclusions This new strategy for patients with advanced synchronous liver metastases allowed: to downstage the CRM in 80% of the cases, to select patients with responding disease avoiding unnecessary surgery to deliver state of the art preoperative rectal radiotherapy without the fear that liver metastases will meanwhile progress beyond the possibility of cure Mentha G. et al. Brit J. Surg 2006; 93:
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
The Surgical Management of Colorectal Metastases
 11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Trattamento chirurgico delle lesioni epatiche secondarie difficili. Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica
 Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Colorectal Liver Metastases Metachronous
 Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Aintree University Hospital
 Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers
 Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
How to deal with synchronous primary and liver metastases
 How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
Primary tumor with synchronous metastases
 Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Management of Stage IV Colorectal Cancer: Expanding the Horizon
 Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: diagnosis and management of colorectal cancer 1.1 Short title Colorectal cancer 2 The remit The Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: diagnosis and management of colorectal cancer 1.1 Short title Colorectal cancer 2 The remit The Department
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Rectal cancer with synchroneous liver mets: A challenging clinical case
 ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
ESMO Preceptorship Programme Rectal cancer Singapur November 2017 Rectal cancer with synchroneous liver mets: A challenging clinical case Andrés Cervantes Disclosures Consulting and advisory services,
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Introduction. Case Report
 Case Report A patient who showed a pathologically complete response after undergoing treatment with XELOX plus bevacizumab for synchronous liver metastasis of grade H2 from sigmoid colon cancer Yasuhito
Case Report A patient who showed a pathologically complete response after undergoing treatment with XELOX plus bevacizumab for synchronous liver metastasis of grade H2 from sigmoid colon cancer Yasuhito
Behandeling van colorectale levermetastasen. Rol van beeldvorming van de lever bij colorectaal carcinoom
 Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer
 Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Liver surgery for colorectal liver metastases. Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham
 Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
COLORECTAL CANCER 44
 COLORECTAL CANCER 44 Colorectal Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by Stuart M. Lichtman, MD Memorial Sloan-Kettering Cancer Center Commack,
COLORECTAL CANCER 44 Colorectal Cancer Highlights from the 2009 Annual Meeting of the American Society of Clinical Oncology Edited by Stuart M. Lichtman, MD Memorial Sloan-Kettering Cancer Center Commack,
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Complete pathological response (ypt0n0m0) after preoperative chemotherapy alone for stage IV rectal cancer
 after preoperative chemotherapy alone for stage IV rectal cancer") CASE REPORT Open Access Complete pathological response (ypt0n0m0) after preoperative chemotherapy alone for stage IV rectal cancer Surennaidoo P Naiken 1*, Christian Toso 1, Laura Rubbia-Brandt 2, Theodoros
CASE REPORT Open Access Complete pathological response (ypt0n0m0) after preoperative chemotherapy alone for stage IV rectal cancer Surennaidoo P Naiken 1*, Christian Toso 1, Laura Rubbia-Brandt 2, Theodoros
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age. Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010
 Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Audit Report. Colorectal Cancer Quality Performance Indicators. Patients diagnosed April 2016 March Published: March 2018
 Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: March 2018 Mr Michael Walker NOSCAN MCN Clinical
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Patient Presentation. 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201
 Patient Presentation 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201 CT shows: Thickening of the right hemidiaphragm CT shows: Fluid in the right paracolic sulcus CT shows: Large
Patient Presentation 32 y.o. female complains of lower abdominal mass CEA = 433, CA125 = 201 CT shows: Thickening of the right hemidiaphragm CT shows: Fluid in the right paracolic sulcus CT shows: Large
RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY
 AFTER LONG COURSE CHEMORADIOTHERAPY") COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
INTERACTIVE SESSION 2
 INTERACTIVE SESSION 2 2 patients with lung metastases, with complete response after oncologic treatment - Clinical Case Presentation: Dr. Esther Casado Dr. Sergi Call - Expert Opinion: Dr. Raúl Embún Dr.
INTERACTIVE SESSION 2 2 patients with lung metastases, with complete response after oncologic treatment - Clinical Case Presentation: Dr. Esther Casado Dr. Sergi Call - Expert Opinion: Dr. Raúl Embún Dr.
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study
 Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
Colon, or Colorectal, Cancer Information
 Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS
 TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES. Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí
 INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
LIVER SURGERY 2. Case 1. Med 5 Refresher Course (Surgery) 2013/14. Dr Sunny Cheung
 2013/14. Dr Sunny Cheung") LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
Colorectal Cancer Quality Performance Indicators
 Publication Report Colorectal Cancer Quality Performance Indicators Patients diagnosed between April 2013 and March 2016 Publication date 27th June 2017 An Official Statistics Publication for Scotland
Publication Report Colorectal Cancer Quality Performance Indicators Patients diagnosed between April 2013 and March 2016 Publication date 27th June 2017 An Official Statistics Publication for Scotland
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
How to integrate surgery in the treatment of patients with liver-only metastatic disease
 How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
A clinical study of metastasized rectal cancer treatment: assessing a multimodal approach
 Med Oncol (2014) 31:839 DOI 10.1007/s12032-014-0839-1 ORIGINAL PAPER A clinical study of metastasized rectal cancer treatment: assessing a multimodal approach Michaela Jung Annica Holmqvist Xiao-Feng Sun
Med Oncol (2014) 31:839 DOI 10.1007/s12032-014-0839-1 ORIGINAL PAPER A clinical study of metastasized rectal cancer treatment: assessing a multimodal approach Michaela Jung Annica Holmqvist Xiao-Feng Sun
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma
 Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness
Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness
Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131
 Colorectal cancer: diagnosis and management Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Colorectal cancer: diagnosis and management Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Follow up The way ahead. John Griffith
 Follow up The way ahead John Griffith Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring
Follow up The way ahead John Griffith Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring
Transanal endoscopic microsurgery for early rectal cancer: single center experience
 Original paper Videosurgery Transanal endoscopic microsurgery for early rectal cancer: single center experience Narimantas Samalavicius 1,2, Marijus Ambrazevicius 1, Alfredas Kilius 1, Kestutis Petrulis
Original paper Videosurgery Transanal endoscopic microsurgery for early rectal cancer: single center experience Narimantas Samalavicius 1,2, Marijus Ambrazevicius 1, Alfredas Kilius 1, Kestutis Petrulis
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Dr Adam Bartlett. General Surgeon Senior Lecturer University of Auckland Auckland City Hospital
 Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Colorectal Cancer Comparative Audit Report
 SOUTH EAST SCOTLAND CANCER NETWORK (SCAN) PROSPECTIVE CANCER AUDIT Colorectal Cancer 2014 2015 Comparative Audit Report Mr B.J. Mander, NHS Lothian, Lead Colorectal Cancer Clinician, SCAN Group Chair Mr
SOUTH EAST SCOTLAND CANCER NETWORK (SCAN) PROSPECTIVE CANCER AUDIT Colorectal Cancer 2014 2015 Comparative Audit Report Mr B.J. Mander, NHS Lothian, Lead Colorectal Cancer Clinician, SCAN Group Chair Mr
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Colorectal Cancer and FDG PET/CT
 Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
Hybrid imaging in colorectal & esophageal cancer Emmanuel Deshayes IAEA WorkShop, November 2017 Colorectal Cancer and FDG PET/CT 1 Clinical background Cancer of the colon and rectum is one of the most
CREATE Trial Proposal: Survey of current practice and potential trial participation
 CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
Risk factors for cancer recurrence or death within 6 months after liver resection in patients with colorectal cancer liver metastasis
 ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
Audit Report. Colorectal Cancer Quality Performance Indicators. Patients diagnosed April 2014 March Published: July 2016
 NORTH OF SCOTLAND PLANNING GROUP Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2014 March 2015 Published: July 2016 Mr
NORTH OF SCOTLAND PLANNING GROUP Colorectal Cancer Managed Clinical Network Audit Report Colorectal Cancer Quality Performance Indicators Patients diagnosed April 2014 March 2015 Published: July 2016 Mr
Ghosts in the Machine: Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand
 Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies
 Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name