Hester Cheung Memorial Lecture
|
|
|
- Muriel Little
- 5 years ago
- Views:
Transcription


1 Hester Cheung Memorial Lecture STEVEN D WEXNER, MD, PHD (HON),FACS, FRCS, FRCS(ED) Director, Digestive Disease Center; Chairman, Department of Colorectal Surgery; Cleveland Clinic Florida Professor of Surgery, Florida Atlantic University College of Medicine Professor of Surgery, Florida International University College of Medicine Professor of Surgery University of South Florida College of Medicine Professor of Surgery, Ohio State University
2 Education and training Primary School: Canossa School, Hong Kong Secondary School: Belilios Public School, Hong Kong, University: The Chinese University of Hong Kong, Bachelor of Medicine & Bachelor of Surgery (M.B.,Ch.B.), Clinical attachment: Department of Surgery, Westmead Hospital, University of Sydney, Australia. (Supervisor Professor J Fletcher), May June, 1997
3 Professional qualifications Year Degree Institution 1998 M.B. Ch.B. The Chinese University of Hong Kong 2002 MRCS Edin The Royal College of Surgeons of Edinburgh 2007 FRACS The Royal Australasian College of Surgeons 2007 FCSHK The Collage of Surgeons of Hong Kong 2007 FHKAM Surgery Hong Kong Academy of Medicine
4 Appointments Consultant in lower GI team of Surgical Department in Pamela Youde Nethersole Eastern Hospital from Jan 2012 to March 2016 Consultant Surgeon in Hong Kong Adventist Hospital (Tsuen Wan) after April 2016 Honorary Clinical Assistant Professor, University of Hong Kong Li Ka Shing, Faculty of Medicine Honorary Clinical Assistant Professor, Chinese University, Faculty of Medicine
5 Administrative posts Department Level Co-ordinator and Mentor, Joint Hospital Surgical Grand Round (2009 to 2012) Co-ordinator and Mentor, Joint Hospital Higher Surgical Trainee Assessment (2009 to 2012) Hospital Level Co-ordinator Cluster Quality & Risk Management Committee, PYNEH since 2012 till 2014 Sub-committee for Medical Equipment/ Technology Planning Vice-chairman of Cluster Cancer Services Co-ordination Committee since Nov 2013 Chairman of Cluster Medical Records Policies & Procedures Subcommittee since Nov 2013
6 Overseas training Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, USA. Colon and Rectal Surgery Program, Department of Surgery, New York-Presbyterian Hospital, Cornell University, New York, USA. Department of Gastroenterology and Digestive Endoscopy Unit, Toranomon Hospital, Tokyo, Japan.
7 Honors / Awards (highlights) 11 awards for best paper or paper presentation Pamela Youde Nethersole Eastern Hospital Most Appreciated Staff Award 2003 Outstanding Performance Award 2005, Best Chair Award 2010
8 Writings and meetings 62 Peer-reviewed publications 12 Book chapters 37 Abstracts 43 Invited lectures 44 Conference/meeting presentations 43 Courses/workshops as organizer or faculty


9
10 Minimizing Surgical / Procedural Trauma ABDOMINAL SURGERY RECTAL SURGERY ANORECTAL OPEN OPEN HEMORRHOIDECTOMY HALS HARMONIC SCALPEL LAP LAP STAPLED ENDOLUMINAL STENTING NOTES DEARTERIALIZATION SILS ROBOTIC NOTES CO2 COLONOSCOPY
 30 min after colonoscopy (P = 0.")
11 RCT to assess the effect of CO2 insufflation on pain during and after colonoscopy. 96 patients randomized to undergo colonoscopy with CO2 or Air insufflation Patients in the CO2 group had less pain: During colonoscopy (P < 0.01) 30 min after colonoscopy (P = 0.02) More patients reported the examination as painless (45% vs 14%, P < 0.01) and 30 min after (70 vs 51%, P = 0.04).
12 RCT
13 Median follow-up : months No difference in disease recurrence Similar 5-year survival rates

14 Comparative cohort study - Rectal cancer patients - Compare the perioperative and short-term outcomes of 52 Patients Neoadjuvant Chemoradiotherapy + Lap proctectomy 138 Patients Chemoradiotherapy Lap proctectomy without Neoadjuvant
15 Median operating time - significantly longer in the neoadjuvant group (155 versus 135 minutes, p = 0.09) No significant difference was observed in terms of blood loss conversion rates postoperative morbidity Length of hospital stay sphincter preservation rates Overall 5- year survival rates
16 Prospective, 10 year evaluation of the long-term oncological outcome after laparoscopic sphincter-preserving TME with a median follow up of ~ 4 years. 177 Patients ( ) 38 received Neoadjuvant Chemoradiotherapy Conversion rate 1% (+) Resection margins 5%
17 Median follow-up - 49 months: Local recurrence - 5.1% Overall metastatic recurrence rate - 22%. Overall 5-year survival - 74% 5-year disease-free survival - 71%
18 Retrospective review of prospectively collected data : 146 patients with T4 rectal cancer underwent laparoscopic proctectomy. Median operative time Median blood loss Conversion rate 16% Anastomotic leakage 4.1% 125 (46 285) min 50 (0 1800) ml Lymph Node harvest 13 (2 40)
19 Recurrence rates Stage II - 41% Stage III - 53% Local recurrence - 3.9% Median follow up 18 (1 118)months Overall survival Conclusions: 25 months Stage II 63M, Stage III 36M, Stage IV 12M Laparoscopic colectomy in histologically T4 cancer is safe. Oncological outcomes remain satisfactory.
20 10 year period Octogenarians, median age 83 (range 80-95) years Median operative time 110 (60 245) min Median blood loss 50 (0 1,000) ml Conversion rate 1% Leakage rate 3.3 percent Overall morbidity rate 17% Operative mortality rate 3% Median follow-up 24 (0 102m) months Recurrence - 22% Five-year survival 51%
21 15-year period: 579 Lap proctectomies 316 Lap proctectomy for rectosigmoid and upper rectal cancer 152 Laparoscopic sphincter-saving TME 92 Lap APR 17 Lap Hartman for rectal cancer 2 Lap proctocolectomy
22 Median follow-up - 56 (range, 8 288) months. Port-site recurrence - 2 patients. Locoregional recurrence - 7.4% Overall 5- and 10-year survivals for rectal cancer were 70% and 45.5% Cancer-specific 5- and 10- year survival was 76% and 56% Conclusions: laparoscopic resection for rectal cancer is safe with good long-term oncological outcomes.
23 Retrospective comparison over 12 year period Laparoscopic Hartmann s reversal 47 Patients Open Hartmann s reversal 35 Patients Conversion rate - 28% in the laparoscopic group. No difference in: operation time blood loss Laparoscopic approach: Shorter median length of stay (12 vs 14 days, P=0.002) Less post-operative paralytic ileus (2 vs 17%, P=0.038). Less incisional hernia (0 vs 14%, P=0.012).

24 Retrospective comparison over 12 year period Laparoscopic Hartmann s reversal 47 Patients Open Hartmann s reversal 35 Patients Conversion rate - 28% in the laparoscopic group.
25
: 53 12 3 Emergency stenting for acute obstruction Palliative for endoscopically obstructing tumors pre-emptive stenting - locally advanced tumor,")
26 Institutional experience with Self-expanding metallic stent for colorectal tumors distal to the splenic flexure. 68 Patients ( ): Emergency stenting for acute obstruction Palliative for endoscopically obstructing tumors pre-emptive stenting - locally advanced tumor, before neoadjuvant Chemoradiation Median follow-up 11 months
27 Institutional experience with Self-expanding metallic stents for colorectal tumors distal to the splenic flexure. 68 Patients ( ). Median follow-up 11 months
28 Overall technical success rate 81% Clinical success rate 65% Complications: stent-related perforations 4 (5.9%) distal migrations 7 (10.3%) Post stenting laparoscopic tumor resection: intestinal obstruction group 27 (51%) neoadjuvant chemoradiation group 3 (100%)
29 Complications: stent-related perforations 4 (5.9%) distal migrations 7 (10.3%) Post stenting LAP resection: intestinal obstruction group 27 (51%) neoadjuvant CRX group 3 (100%)

30 24 - endoluminal stenting followed by laparoscopic resection 24 - emergency open surgery.
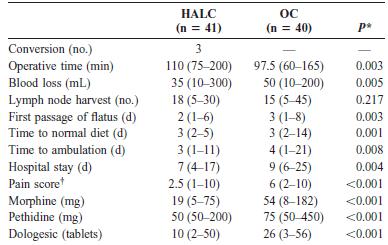
31 Endolaparoscopic Open. Blood loss 50ml 200ml p LN harvested p Pain scores 4 5 p Anastomotic leaks 0 2 p Wound infections 2 8 p 0.04 One-Stage operations 16/24 9/24 p 0.04 Permanent stoma 0/24 6/24 p 0.03
 Endo-lap : 65 Open : 32 no")

32 Long term follow up on the 48 patients from the RCT. Median follow-up (months) Endo-lap : 65 Open : 32 no statistically significant differences in: Disease recurrence rate 5-year overall survival rate 5-year disease-free survival rate
 Median operative time Median blood loss Median hospital stay Median distance of anastomosis from AV 155 (155-165) minutes 50 (20-100) ml 10 (8 29) days 2.")
33 5 patients with T2/T3 low rectal cancer, two post neoadjuvant CRX Combined laparoscopic abdominal and transanal excision with transanal extraction. Median BMI 26 (21-28) Median operative time Median blood loss Median hospital stay Median distance of anastomosis from AV 155 ( ) minutes 50 (20-100) ml 10 (8 29) days 2.5 (2 4) cm Clear radial and distal margins were obtained in all five patients
34 Hybrid NOTES left sided colonic tumors Case series 10 patients Laparoscopic Lt colectomy with transanal NOSE: Lap mobilization and devascularization of Lt colon sigmoid upper rectum Division of upper rectum 5cm distal to tumor Opening of rectal staple line and introduction of Anvil Anvil introduced via a colotomy proximal to the tumor and spike passed through the antimesenteric bowel wall. Division of bowel between the colotomy site and Anvil. Extraction of the sigmoid transanally. Closure of rectal stump EEA anastomosis End to Side.

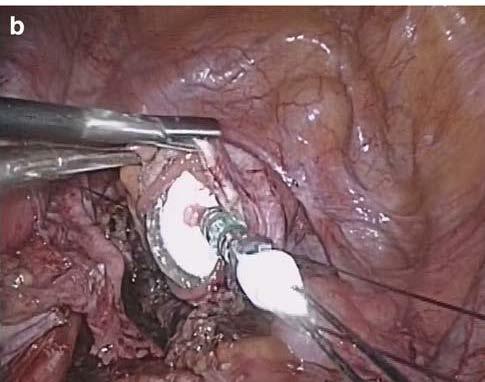
35 Introduction of Anvil

36 Devision of colon between Anvil and Colotomy, proximal to Tumor
37 Hybrid NOTES left sided colonic tumors : Laparoscopic lt colectomy with transanal NOSE 12/ / Patients, 4 Male BMI Tumor location 5 rectosigmoid, 4 sigmoid, 1 descending Median - 30cm from anal verge Median operating time 127 minutes No post-operative complications
38 Median length of stay 7 days (Range 4-18) Median post-op pain score 2 (Range 2-3) Median Lymph Nodes harvested 11 (Range 7-17) Clear resection margin in all patients. (Median proximal 7cm, distal 3cm) Path 8 carcinomas, 2 Tublovillous adenoma with dysplasia.
39 Technical report of a case of combined SILS sigmoidectomy with transrectal specimen extraction. Sessile polyp in distal sigmoid. SILS mobilization and devascularization of sigmoid Division of rectosigmoid junction Opening of rectal staple line and introduction of Anvil Anvil introduced via a colotomy proximal to the polyp and spike passed through the bowel wall.



40 Division of bowel between the colotomy site and Anvil. Extraction of the sigmoid transanally. Closure of rectal stump EEA anastomosis End to Side. First report of combined SILS with NOSE. No operative op post-operative complication D/C at POD 6
41 Randomized prospective trial - Lap colectomy vs Hybrid NOTES colectomy for Lt sided colonic tumors. 3 year period 35 patients in each group.
42
43 Similar : Operative time (105 vs. 100 min, p = 0.851) Blood loss (30 vs. 30 ml,p = 0.954) Length of hospital stay (5 vs. 5 days, p = 0.990) Hybrid NOTES: Significantly lower pain score during the first week (1 vs 2, p = 0.017) Lower wound infection rates (0 vs 4, p = 0.005)

44 Multimedia case reports

45 Prospective assessment of preoperative and postoperative sexual and urinary function of male patients undergoing robot-assisted laparoscopic TME for rectal cancer. 34 month period: 33 patients baseline 3 months postoperative IPSS score NS IIEF-5 score NS A trend towards worsening erectile function after surgery. Robot-assisted technique does not confer additional benefits in the preservation of urogenital function when compared to conventional laparoscopic technique

46 Randomized trial over 20 months : 88 patients. Similar: Operative time Blood loss Day of first bowel movement after surgery Complication rates Analgesic requirements continence outcomes stapled group: Significantly better pain score (P = 0.002) Shorter length of stay (P = 0.02) Earlier return to work (6.7 vs. 15.6, P =0.002) Significantly better satisfaction scores at 6 month f/u (P = 0.001)
47 PPH THD Comparison of short term outcome and efficacy between THD and PPH. 40 patients THD - prospectively collected 37 patients PPH - medical records database. Median f/u 8 (THD) vs 36 (PPH) months
48 THD and PPH similar in Operative time Blood loss Length of stay Time to first BM Early complication rates THD had significant improvement in hemorrhoid symptoms (bleeding and prolapse)
49 THD - Better pain scores (0-10 scale) 1.7 vs 5 p Earlier return to normal daily activity 3.1d vs 6.8d p Long-term THD and PPH had similar Satisfaction scores Complication rate Recurrence rate
50 Minimizing Surgical / Procedural Trauma ABDOMINAL SURGERY RECTAL SURGERY ANORECTAL OPEN OPEN HEMORRHOIDECTOMY HALS HARMONIC SCALPEL LAP LAP STAPLED NOTES ENDOLUMINAL STENTING SILS ROBOTIC NOTES DEARTERIALIZATION CO2 COLONOSCOPY

51 In memoriam
Innovations in rectal cancer surgery TAMIS and transanal TME
 Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Karen Lok Man Tung, Michael Ka Wah Li. Introduction
 Original Article Page 1 of 5 Hybrid natural orifice transluminal endoscopic surgery colectomy versus conventional laparoscopic colectomy for left-sided colonic tumors: intermediate follow up of a randomized
Original Article Page 1 of 5 Hybrid natural orifice transluminal endoscopic surgery colectomy versus conventional laparoscopic colectomy for left-sided colonic tumors: intermediate follow up of a randomized
LONG TERM OUTCOME OF ELECTIVE SURGERY
 LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
LONG TERM OUTCOME OF ELECTIVE SURGERY Roberto Persiani Associate Professor Mini-invasive Oncological Surgery Unit Institute of Surgical Pathology (Dir. prof. D. D Ugo) Dis Colon Rectum, March 2000 Dis
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better!
 Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Laparoscopic vs Robotic Rectal Cancer Surgery: Making it better! Francis Seow- Choen Medical Director Seow-Choen Colorectal Centre Singapore In all situations: We have to use the right tool for the job
Henrique Prata Director General
 PROGRAM ADVANCED COURSE IIN COLORECTAL SURGERY SEPTEMBER 12 TT HH TO 14 TT HH,, 2019 CHAIRMAN Henrique Prata Director General Hospital de Amor - Barretos PRESIDENT DIRECTOR COURSE DIRECTOR Jacques Marescaux
PROGRAM ADVANCED COURSE IIN COLORECTAL SURGERY SEPTEMBER 12 TT HH TO 14 TT HH,, 2019 CHAIRMAN Henrique Prata Director General Hospital de Amor - Barretos PRESIDENT DIRECTOR COURSE DIRECTOR Jacques Marescaux
The Binational Colorectal Cancer Audit. A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017
 The Binational Colorectal Cancer Audit A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017 Binational Colorectal Cancer Database 2010 First Patient 2011 Contract between CMUDS and
The Binational Colorectal Cancer Audit A/Prof Paul McMurrick Head, Cabrini Monash University Dept of Surgery 2017 Binational Colorectal Cancer Database 2010 First Patient 2011 Contract between CMUDS and
Laparoscopic Surgery for Rectal Carcinoma An Experience of 20 Cases in a Government
 Laparoscopic Sugery World for Rectal Journal Carcinoma An of Laparoscopic Experience Surgery, of September-December 20 Cases in a Government 2008;1(3):53-57 Sector Hospital Laparoscopic Surgery for Rectal
Laparoscopic Sugery World for Rectal Journal Carcinoma An of Laparoscopic Experience Surgery, of September-December 20 Cases in a Government 2008;1(3):53-57 Sector Hospital Laparoscopic Surgery for Rectal
Motility Disorders. Pelvic Floor. Colorectal Center for Functional Bowel Disorders (N = 701) January 2010 November 2011
 January 2010 November 2011") Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Motility Disorders Pelvic Floor Colorectal Center for Functional Bowel Disorders (N = 71) January 21 November 211 New Patients 35 3 25 2 15 1 5 Constipation Fecal Incontinence Rectal Prolapse Digestive-Genital
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Transanal Surgery for Large Rectal Polyps and Early Rectal Cancer
 Transanal Surgery for Large Rectal Polyps and Early Rectal Cancer AB Harikrishnan Consultant Colorectal Surgeon, Sheffield Honorary Clinical Senior Lecturer, Sheffield University Associate TPD General
Transanal Surgery for Large Rectal Polyps and Early Rectal Cancer AB Harikrishnan Consultant Colorectal Surgeon, Sheffield Honorary Clinical Senior Lecturer, Sheffield University Associate TPD General
DIVERTICULAR DISEASE. Dr. Irina Murray Casanova PGY IV
 DIVERTICULAR DISEASE Dr. Irina Murray Casanova PGY IV Diverticular Disease Colonoscopy Abdpelvic CT Scan Surgical Indications Overall, approximately 20% of patients with diverticulitis require surgical
DIVERTICULAR DISEASE Dr. Irina Murray Casanova PGY IV Diverticular Disease Colonoscopy Abdpelvic CT Scan Surgical Indications Overall, approximately 20% of patients with diverticulitis require surgical
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Citation for published version (APA): Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects
: Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects") UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Laparoscopic Colorectal Surgery
 Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Laparoscopic Colorectal Surgery 20 th November 2015 Dr Adam Cichowitz General Surgeon Laparoscopic Colorectal Surgery Introduced in early 1990s Uptake slow Steep learning curve Requirement for equipment
Transanal Endoscopic Microsurgery
 Transanal Endoscopic Microsurgery Dana R. Sands, MD, FACS, FASCRS Director, Colorectal Physiology Center Staff Surgeon Department of Colorectal Surgery Cleveland Clinic Florida What is TEM? Minimally invasive
Transanal Endoscopic Microsurgery Dana R. Sands, MD, FACS, FASCRS Director, Colorectal Physiology Center Staff Surgeon Department of Colorectal Surgery Cleveland Clinic Florida What is TEM? Minimally invasive
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Outcomes Following Surgery for Distal Rectal Cancers: A Comparison between Laparoscopic and Open Abdomino- Perineal Resection
 ORIGINAL ARTICLE Outcomes Following Surgery for Distal Rectal Cancers: A Comparison between Laparoscopic and Open Abdomino- Perineal Resection K K Tan, FRCS (Edin), C S Chong, MRCS (Edin), C B Tsang, FRCS
ORIGINAL ARTICLE Outcomes Following Surgery for Distal Rectal Cancers: A Comparison between Laparoscopic and Open Abdomino- Perineal Resection K K Tan, FRCS (Edin), C S Chong, MRCS (Edin), C B Tsang, FRCS
WJOLS /jp-journals
 10.5005/jp-journals-10007-1203 REVIEW ARTICLE Sachin Shashikant Ingle ABSTRACT Background: Worldwide about 782,000 people are diagnosed with colorectal cancer each year. Colorectal cancer is the third
10.5005/jp-journals-10007-1203 REVIEW ARTICLE Sachin Shashikant Ingle ABSTRACT Background: Worldwide about 782,000 people are diagnosed with colorectal cancer each year. Colorectal cancer is the third
Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond
 Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch
Innovative Surgical Management in the Treatment of Rectal Cancer: MIS, Robotic, and Beyond Jonathan E. Efron, MD, FACS, FASCRS The Mark M Ravitch, MD Endowed Professorship in Surgery Chief of the Ravitch
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
SINGLE INCISION LAPAROSCOPIC SURGERY
 SINGLE INCISION LAPAROSCOPIC SURGERY DR ADEWALE ADISA CONSULTANT MINIMAL ACCESS SURGEON & SENIOR LECTURER DEPARTMENT OF SURGERY, OBAFEMI AWOLOWO UNIVERSITY, & OBAFEMI AWOLOWO UNIVERSITY TEACHING HOSPITALS
SINGLE INCISION LAPAROSCOPIC SURGERY DR ADEWALE ADISA CONSULTANT MINIMAL ACCESS SURGEON & SENIOR LECTURER DEPARTMENT OF SURGERY, OBAFEMI AWOLOWO UNIVERSITY, & OBAFEMI AWOLOWO UNIVERSITY TEACHING HOSPITALS
Current innovations in colorectal surgery
 Current innovations in colorectal surgery KS Chapple Consultant Colorectal Surgeon Sheffield Teaching Hospitals NHS Trust Do we need more innovations? What innovations are there and are they worthwhile?
Current innovations in colorectal surgery KS Chapple Consultant Colorectal Surgeon Sheffield Teaching Hospitals NHS Trust Do we need more innovations? What innovations are there and are they worthwhile?
SINGLE INCISION ENDOSCOPIC SURGERY (SIES)
") EAES CONSENSUS CONFERENCE SINGLE INCISION ENDOSCOPIC SURGERY (SIES) STATEMENTS AND RECOMMENDATIONS EAES appreciates your input! Please give your opinion on the below statements and recommendations of the
EAES CONSENSUS CONFERENCE SINGLE INCISION ENDOSCOPIC SURGERY (SIES) STATEMENTS AND RECOMMENDATIONS EAES appreciates your input! Please give your opinion on the below statements and recommendations of the
Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society
 Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society 1.Intuitive Surgical 2.C-Sats 3.Virtual Incision Study comparing
Can Robotics be useful to a General Surgeon Performing Colorectal Surgery? Curtis L. Peery MD April 27 th 2018 Throckmorton Surgical Society 1.Intuitive Surgical 2.C-Sats 3.Virtual Incision Study comparing
Surgery for Ulcerative Colitis 11/14/10. Colectomy for Ulcerative Colitis: What your patient should know. Surgery for Ulcerative Colitis
 Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
Colectomy for Ulcerative Colitis: What your patient should know Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Surgery for Ulcerative
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients in a Single Institution
 Minimally Invasive Surgery, Article ID 530314, 6 pages http://dx.doi.org/10.1155/2014/530314 Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients
Minimally Invasive Surgery, Article ID 530314, 6 pages http://dx.doi.org/10.1155/2014/530314 Clinical Study Laparoscopic versus Open Surgery for Colorectal Cancer: A Retrospective Analysis of 163 Patients
Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic Surgery for Colorectal Disease
 ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
ORIGINAL ARTICLE pissn 2234-778X eissn 2234-5248 J Minim Invasive Surg 2018;21(1):38-42 Journal of Minimally Invasive Surgery Repeat Single Incision Laparoscopic Surgery after Primary Single Incision Laparoscopic
Corporate Medical Policy Transanal Endoscopic Microsurgery (TEMS)
") Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: transanal_endoscopic_microsurgery_(tems) 6/2008 11/2018 11/2019 11/2018 Description of Procedure or Service
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: transanal_endoscopic_microsurgery_(tems) 6/2008 11/2018 11/2019 11/2018 Description of Procedure or Service
Acute Diverticulitis. Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh
 Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
Acute Diverticulitis Andrew B. Peitzman, MD Mark M. Ravitch Professor of Surgery University of Pittsburgh Focus today: when to operate n Recurrent, uncomplicated diverticulitis; after how many episodes?
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN
 LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
LARGE BOWEL OBSTRUCTION MARCUS BURNSTEIN MCQ A 78 yr. old man (HT, DM, 2 coronary stents) has 3 mos. of irregular bowel habits and 72 hrs. of LBO. Distended, non-tender. Normal blood work. Plain xray,
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Laparoscopic reversal of Hartmann's procedure
 J Korean Surg Soc 2012;82:256-260 http://dx.doi.org/10.4174/jkss.2012.82.4.256 CASE REPORT JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Laparoscopic reversal of Hartmann's
J Korean Surg Soc 2012;82:256-260 http://dx.doi.org/10.4174/jkss.2012.82.4.256 CASE REPORT JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Laparoscopic reversal of Hartmann's
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
Transanal endoscopic microsurgery for early rectal cancer: single center experience
 Original paper Videosurgery Transanal endoscopic microsurgery for early rectal cancer: single center experience Narimantas Samalavicius 1,2, Marijus Ambrazevicius 1, Alfredas Kilius 1, Kestutis Petrulis
Original paper Videosurgery Transanal endoscopic microsurgery for early rectal cancer: single center experience Narimantas Samalavicius 1,2, Marijus Ambrazevicius 1, Alfredas Kilius 1, Kestutis Petrulis
Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts Correspondence to
 East and Central African Journal of Surgery http://www.bioline.org.br/js 9 Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts
East and Central African Journal of Surgery http://www.bioline.org.br/js 9 Outcomes of Colostomy Reversal Procedures in Two Teaching Hospitals in Addis Ababa, Ethiopia A. Bekele, B. Kotisso, H. Biluts
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Kurumboor Prakash, N P Kamalesh, K Pramil, I S Vipin, A Sylesh, Manoj Jacob
 Original Article Does case selection and outcome following laparoscopic colorectal resection change after initial learning curve? Analysis of 235 consecutive elective laparoscopic colorectal resections
Original Article Does case selection and outcome following laparoscopic colorectal resection change after initial learning curve? Analysis of 235 consecutive elective laparoscopic colorectal resections
Operational Efficiency in Colon Surgery Enhanced Recovery Pathways: 23 hour laparoscopic colectomy
 Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
Enhanced Recovery Pathways: 23 hour laparoscopic colectomy Conor P. Delaney MD MCh PhD Chairman, Digestive Disease Institute Professor of Surgery, Cleveland, Ohio Disclosure Slide Conor Delaney MD PhD
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,800 116,000 120M Open access books available International authors and editors Downloads Our
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal Laparoscopic Standards and Coding Protocols July 2015 v2.0
 Laparoscopic Standards and Coding Protocols July 2015 v2.0 COLORECTAL LAPAROSCOPIC STANDARDS AND CODING PROTOCOLS Contents 1 Context... 3 2 Laparoscopic Standards... 3 3 Coding Protocols... 3 Appendix
Laparoscopic Standards and Coding Protocols July 2015 v2.0 COLORECTAL LAPAROSCOPIC STANDARDS AND CODING PROTOCOLS Contents 1 Context... 3 2 Laparoscopic Standards... 3 3 Coding Protocols... 3 Appendix
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Preoperative Data Colorectal Cancer Database
 Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Preoperative Data Please place patient label here Patient Information Patient s Last Name First Middle Initial UR MH MP Birth Date Sex Post Code / / M F ECOG (see codes below) Date of Diagnosis Consultant
Incidence of Colorectal Cancers- Australia. Anterior Resection 5/23/2018. What spurs us to investigate?
 Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Incidence of Colorectal Cancers- Australia 17,000 Colorectal cancers in 2018 20% of Colorectal cancers are in the Rectum 12.3% of all new cancers Anterior Resection Syndrome (ARS) Lisa Wilson. Colorectal
Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf?
 Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf? Dieter Hahnloser Klinik für Viszeral- und Transplantationschirurgie UniverstätsSpital Zürich Low Rectal Resection
Ein Leben nach tiefer Rektumresektion: Was erwartet unsere Patienten im Langzeitverlauf? Dieter Hahnloser Klinik für Viszeral- und Transplantationschirurgie UniverstätsSpital Zürich Low Rectal Resection
7/11/17. The Surgeon s Operative Report: Tools and Tips to Enhance Abstraction. Stopwoundinfection.com. Impact to Healthcare
 1. Scott, R. Douglas. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. March 2009. http://www.cdc.gov/hai/pdfs/hai/scott_costpaper.pdf. 2.
1. Scott, R. Douglas. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. March 2009. http://www.cdc.gov/hai/pdfs/hai/scott_costpaper.pdf. 2.
Laparoscopic Colorectal Surgery. Advanced Course. November 19 & Directors of the course: Jacques MARESCAUX
 Laparoscopic Colorectal Surgery November 19 & 20-2010 Directors of the course: Jacques MARESCAUX Richard John HEALD United Kingdom Joël LEROY Faculty : Patrick AMBROSETTI Switzerland Richard BARTHELEMY
Laparoscopic Colorectal Surgery November 19 & 20-2010 Directors of the course: Jacques MARESCAUX Richard John HEALD United Kingdom Joël LEROY Faculty : Patrick AMBROSETTI Switzerland Richard BARTHELEMY
Quality of life after minimally invasive surgery for rectal cancer
 Chen et al. Mini-invasive Surg 2018;2:42 DOI: 10.20517/2574-1225.2018.59 Mini-invasive Surgery Review Open Access Quality of life after minimally invasive surgery for rectal cancer Jason H. Chen 1, Jennifer
Chen et al. Mini-invasive Surg 2018;2:42 DOI: 10.20517/2574-1225.2018.59 Mini-invasive Surgery Review Open Access Quality of life after minimally invasive surgery for rectal cancer Jason H. Chen 1, Jennifer
Disclosures. Personalized Approaches to Gastrointestinal Cancers. Objectives. What is personalized cancer care. Go through some genomic studies
 Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Transanal total mesorectal excision of the rectum This procedure is used for patients who need to have their whole
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Transanal total mesorectal excision of the rectum This procedure is used for patients who need to have their whole
The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer
 The Open Colorectal Cancer Journal, 2011, 4, 13-17 13 Open Access The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer Alexander Lebedyev 1, Damien Urban 2, Danny Rosin 1, Amram Ayalon
The Open Colorectal Cancer Journal, 2011, 4, 13-17 13 Open Access The Laparoscopic Approach in the Treatment of Distal Colorectal Cancer Alexander Lebedyev 1, Damien Urban 2, Danny Rosin 1, Amram Ayalon
Clinical Study Three Ports Laparoscopic Resection for Colorectal Cancer: A Step on Refining of Reduced Port Surgery
 ISRN Surgery, Article ID 781549, 5 pages http://dx.doi.org/10.1155/2014/781549 Clinical Study Three Ports Laparoscopic Resection for Colorectal Cancer: A Step on Refining of Reduced Port Surgery Anwar
ISRN Surgery, Article ID 781549, 5 pages http://dx.doi.org/10.1155/2014/781549 Clinical Study Three Ports Laparoscopic Resection for Colorectal Cancer: A Step on Refining of Reduced Port Surgery Anwar
Case Study Review #2!
 1 Case Study Review #2! Based on your feedback for more SCQR-specific education, we are offering this common case scenario with frequently asked SCQR questions and misinterpreted variables. The case study
1 Case Study Review #2! Based on your feedback for more SCQR-specific education, we are offering this common case scenario with frequently asked SCQR questions and misinterpreted variables. The case study
University of Groningen. Colorectal Anastomoses Bakker, Ilsalien
 University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
University of Groningen Colorectal Anastomoses Bakker, Ilsalien IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document
Our Colorectal Surgery Team
 Our Colorectal Surgery Team At the Singapore General Hospital, our dedicated team of Colorectal surgeons offer comprehensive consultations on all colorectal services. This includes pelvic floor disorders,
Our Colorectal Surgery Team At the Singapore General Hospital, our dedicated team of Colorectal surgeons offer comprehensive consultations on all colorectal services. This includes pelvic floor disorders,
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
19th Annual International Colorectal Disease Symposium An International Exchange of Medical and Surgical Concepts
 Wednesday, February 13, 2008 7-9:00p Early Check-In / Registration (Grand Ballroom Foyer) Thursday, February 14, 2008 6:45 AM Breakfast (Caribbean Ballroom and Foyer) 7:00 AM Registration (Grand Ballroom
Wednesday, February 13, 2008 7-9:00p Early Check-In / Registration (Grand Ballroom Foyer) Thursday, February 14, 2008 6:45 AM Breakfast (Caribbean Ballroom and Foyer) 7:00 AM Registration (Grand Ballroom
Incidence and risk factors of anastomotic leaks. By: khaled Said Assistant professor of colorectal surgery Alexandria
 Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Incidence and risk factors of anastomotic leaks By: khaled Said Assistant professor of colorectal surgery Alexandria Anastomotic leakage after colorectal surgery is a major and potentially life-threatening
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Original Policy Date
 MP 7.01.92 Transanal Endoscopic Microsurgery Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical
MP 7.01.92 Transanal Endoscopic Microsurgery Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical
Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer
 Journal of the Egyptian Nat. Cancer Inst., Vol. 16, No. 4, December: 210-215, 2004 Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer EL-SAYED ASHRAF KHALIL, M.D.FRCS; MOHAMAD
Journal of the Egyptian Nat. Cancer Inst., Vol. 16, No. 4, December: 210-215, 2004 Sphincter Sparing Procedures: Is it a standard for Management of Low Rectal Cancer EL-SAYED ASHRAF KHALIL, M.D.FRCS; MOHAMAD
Initial experience of reduced port surgery using a two-surgeon technique for colorectal cancer
 Tashiro et al. BMC Surgery (2015) 15:91 DOI 10.1186/s12893-015-0078-1 TECHNICAL ADVANCE Open Access Initial experience of reduced port surgery using a two-surgeon technique for colorectal cancer Jo Tashiro
Tashiro et al. BMC Surgery (2015) 15:91 DOI 10.1186/s12893-015-0078-1 TECHNICAL ADVANCE Open Access Initial experience of reduced port surgery using a two-surgeon technique for colorectal cancer Jo Tashiro
PROCARE FINAL FEEDBACK Definitions
 1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
Surgery for Inflammatory Bowel Disease
 Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Surgery for Inflammatory Bowel Disease Emily Steinhagen, MD Assistant Professor Department of Surgery, Division of Colorectal Surgery University Hospitals Cleveland Medical Center Common Questions Why
Follow up The way ahead. John Griffith
 Follow up The way ahead John Griffith Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring
Follow up The way ahead John Griffith Key Emerging Principles Risk stratified pathways of care Personalised care plan and treatment summary with a hand held record Information and education Remote monitoring
How much colon should be resected?
 Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Index. Note: Page numbers of article title are in boldface type.
 Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Index Note: Page numbers of article title are in boldface type. A Abscess(es) in Crohn s disease, 168 169 IPAA and, 110 114 as unexpected finding in colorectal surgery, 46 Adhesion(s) trocars-related laparoscopy
Lynda Sue Dougherty MD FACS FASCRS (703)
") Lynda Sue Dougherty MD FACS FASCRS www.fairfaxcolorectal.com (703) 280-2841 PRACTICE Fairfax Colon & Rectal Surgery, PC 2710 Prosperity Ave, Suite 200 Fairfax, VA 22031 Fairfax Colon and Rectal Surgery
Lynda Sue Dougherty MD FACS FASCRS www.fairfaxcolorectal.com (703) 280-2841 PRACTICE Fairfax Colon & Rectal Surgery, PC 2710 Prosperity Ave, Suite 200 Fairfax, VA 22031 Fairfax Colon and Rectal Surgery
Vincent James Obias, MD MS
 Vincent James Obias, MD MS Education Undergraduate B.S., James Madison University, 1989-1993 Graduate/Medical Education Masters of Science, Medical College of Virginia/Virginia Commonwealth University,
Vincent James Obias, MD MS Education Undergraduate B.S., James Madison University, 1989-1993 Graduate/Medical Education Masters of Science, Medical College of Virginia/Virginia Commonwealth University,
Henrique Prata. Director General Hospital de Cancer de Barretos. University of Strasbourg, France
 PROGRAM ADVANCED COURSE IIN COLORECTAL SURGERY DECEMBER 12 & 13,, 2014 C HH AA I RRM AAN Henrique Prata Director General Hospital de Cancer de Barretos O BB J EE CC TT I VV EE SS PP RR EE SS II IDD EE
PROGRAM ADVANCED COURSE IIN COLORECTAL SURGERY DECEMBER 12 & 13,, 2014 C HH AA I RRM AAN Henrique Prata Director General Hospital de Cancer de Barretos O BB J EE CC TT I VV EE SS PP RR EE SS II IDD EE
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Colorectal Cancer. Nimalan Pathma-Nathan
 Colorectal Cancer Nimalan Pathma-Nathan Introduction Rooms at HSS and Westmead Private Outpatients at Westmead Multidisciplinary clinic Westmead Surgery and scopes HSS Westmead Public, Private and Children
Colorectal Cancer Nimalan Pathma-Nathan Introduction Rooms at HSS and Westmead Private Outpatients at Westmead Multidisciplinary clinic Westmead Surgery and scopes HSS Westmead Public, Private and Children
Rectal Cancer. About the Colon and Rectum. Symptoms. Colorectal Cancer Screening
 Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Patient information regarding care and surgery associated with RECTAL CANCER by Robert K. Cleary, M.D., John C. Eggenberger, M.D., Amalia J. Stefanou., M.D. location: Michigan Heart and Vascular Institute,
Cover Page. The following handle holds various files of this Leiden University dissertation:
 Cover Page The following handle holds various files of this Leiden University dissertation: http://hdl.handle.net/1887/6119 Author: Spruit, E.N. Title: Increasing the efficiency of laparoscopic surgical
Cover Page The following handle holds various files of this Leiden University dissertation: http://hdl.handle.net/1887/6119 Author: Spruit, E.N. Title: Increasing the efficiency of laparoscopic surgical
Acute Care Surgery: Diverticulitis
 Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
Acute Care Surgery: Diverticulitis Madhulika G. Varma, MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment of Diverticular Disease Increasing
COLORECTAL CANCER COMPARATIVE AUDIT REPORT SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT. Mr B.J. Mander SCAN Group Chair
 SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT COLORECTAL CANCER 2013-2014 COMPARATIVE AUDIT REPORT Mr B.J. Mander SCAN Group Chair Mr K Pal, NHS Borders Mr S Whitelaw, NHS Dumfries & Galloway
SOUTH EAST SCOTLAND CANCER NETWORK PROSPECTIVE CANCER AUDIT COLORECTAL CANCER 2013-2014 COMPARATIVE AUDIT REPORT Mr B.J. Mander SCAN Group Chair Mr K Pal, NHS Borders Mr S Whitelaw, NHS Dumfries & Galloway
The effect of rectal washout on local recurrence following rectal cancer surgery
 COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
Laparoscopy assisted versus open surgery for multiple colorectal cancers with two anastomoses: a cohort study
 DOI 10.1186/s40064-016-1948-4 RESEARCH Open Access Laparoscopy assisted versus open surgery for multiple colorectal cancers with two anastomoses: a cohort study Hiroaki Nozawa *, Soichiro Ishihara, Koji
DOI 10.1186/s40064-016-1948-4 RESEARCH Open Access Laparoscopy assisted versus open surgery for multiple colorectal cancers with two anastomoses: a cohort study Hiroaki Nozawa *, Soichiro Ishihara, Koji
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery
 Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery Disclosure M ADHULIKA G. V ARMA M D PROFESSOR AND CHIEF S E CTION O F COLORECTAL S U R G ERY U N I V ERS ITY O F CALIFORNIA,
Pelvic Organ Functions: Urinary, Sexual and Bowel Dysfunction after Rectal Surgery Disclosure M ADHULIKA G. V ARMA M D PROFESSOR AND CHIEF S E CTION O F COLORECTAL S U R G ERY U N I V ERS ITY O F CALIFORNIA,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian