Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
|
|
|
- Barry Stephens
- 5 years ago
- Views:
Transcription
1 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG)
2 Disclosures Recently began offering and implanting SpaceOAR in my clinic - No financial obligations to or income received from Augmenix
3 Outline Screening ProtecT Trial RadBio of Prostate AdenoCA EBRT + brachytherapy boost Hypofractionated EBRT SBRT Immobilization and OAR sparing

4 Screening: Myth Busters DRE PSA?

5 PSA screening trials Andrioleet al.,, JNCI 2012; Schroder et al., Lancet 2014; Hugossonet al., Lancet 2010
6 PSA Screening USPSTF: - Previously recommended against screening (2012) - New draft DOES NOT recommend against screening in men AUA (2013) yo: No screening recommended unless higher risk (ex: family hx, AA) yo: Risk/Benefit discussion with shared decision making based on a man s values and preferences yo: No screening recommended, some in excellent health may benefit

7
8 ProtecT: RP vs RT vs AS UK PCP centers Age: years (median = 62) Eligibility: Stage: ct1c (76%) - ct2 (23%) Gleason: 6 (77%) - 7 (20%) (3%) PSA: 3 20 ( in 90%) Hamdy, et al. & Donovan, et al. NEJM 2016.
 bpfs 58% low, 40% intermediate, 2% high risk patients Median f/u 10")

9 ProtecT: RP vs RT vs AS 1643 patients randomized: AS: 545 pts (482) RT: 545 pts (391) RP: 553 pts (405) bpfs 58% low, 40% intermediate, 2% high risk patients Median f/u 10 years Primary outcome: Prostate-cancer-related mortality Secondary outcomes: OS - DM - Clinical progression - Primary tx failure - QoL Hamdy, et al. & Donovan, et al. NEJM 2016.
10 ProtecT: RP vs RT vs AS AS: PSA Q3m x1yr Q6-12m All rises assessed, but > 50% increases in 1yr prompted formal review RT: Neoadj & concurrent ADT for 3-6 months 3DCRT: 74 Gy in 37 fractions PSA rise of at least 2.0 above nadir prompted formal review RP: Postoperative PSA Q3m x1yr Q6m x 2yrs Q1yr Adjuvant RT discussed with +SM, ECE, or postop PSA >= 0.2 Tx failure = PSA of 0.2 or higher at 3 months postop Hamdy, et al. & Donovan, et al. NEJM 2016.
11 Results AS: 55% required intervention by Nov % RP - 42% EBRT - 8% brachy - 1% HIFU RT: 14% had PSA rise >2 above nadir 5% RP - 25% ADT - 2% HIFU RP: 2% had PSA >0.2 between 31 to 183 days postop 2% underwent adjuvant RT for pt3 or +SM (29/24% total) 4 of 280 with PLND had pn+ disease Prostate-cancer-related mortality: ~ 1% in all three arms with 10 yr median f/u (p=0.48) Hamdy, et al. & Donovan, et al. NEJM 2016.
12 Numbers needed to treat RT: 33 AS pts to avoid one DM 9 AS pts to avoid one clinical progression RP: 27 pts to avoid one DM 9 AS pts to avoid one clinical progression Hamdy, et al. & Donovan, et al. NEJM 2016.

13 Hamdy, et al. & Donovan, et al. NEJM 2016.
14 Patient-reported survey outcomes AS: Sexual and urinary function gradually declined RT: Negative effect on sexual function was greatest at 6 months, but then recovered somewhat and remained stable Minimal effect on urinary continence Bowel function negatively impacted at 6 months, but recovered (except for increasing frequency of bloody stools) Urinary voiding and nocturia worse than other groups at 6 months, but mostly recovered to similar at 12 months RP: Greatest negative effect on sexual function and urinary incontinence Some recovery seen, but remained SS lower than other tx groups Hamdy, et al. & Donovan, et al. NEJM 2016.
15 Active Surveillence Within 6 months, can get mpmri, repeat bx, or do MRI-bx if <10 cores or other concerns (i.e. +MRI, low free PSA, PSADT, age, race, FamHx) PSA no more often then every 6 months DRE no more often than every 12 months Repeat biopsy if: - PSA rises Observation: < 10 yr life expectancy - DRE changes - Preferred for low risk patients - Suspicious MRI - Option for intermediate risk patients

16 Active Surveillance NCCN 2018
17 When it s time to treat Why surgery? - Physically tolerable - Convenient - Low risk of GI toxicity - RT as salvage Why not? - Open urethra risks - Neurologic ED - Operative risks Why RT? - Medically inoperable/risky - Non-invasive - Continence - Vascular ED Why not? - Narrowed urethra risks - GI toxicity - Salvage difficult - Contraindicated
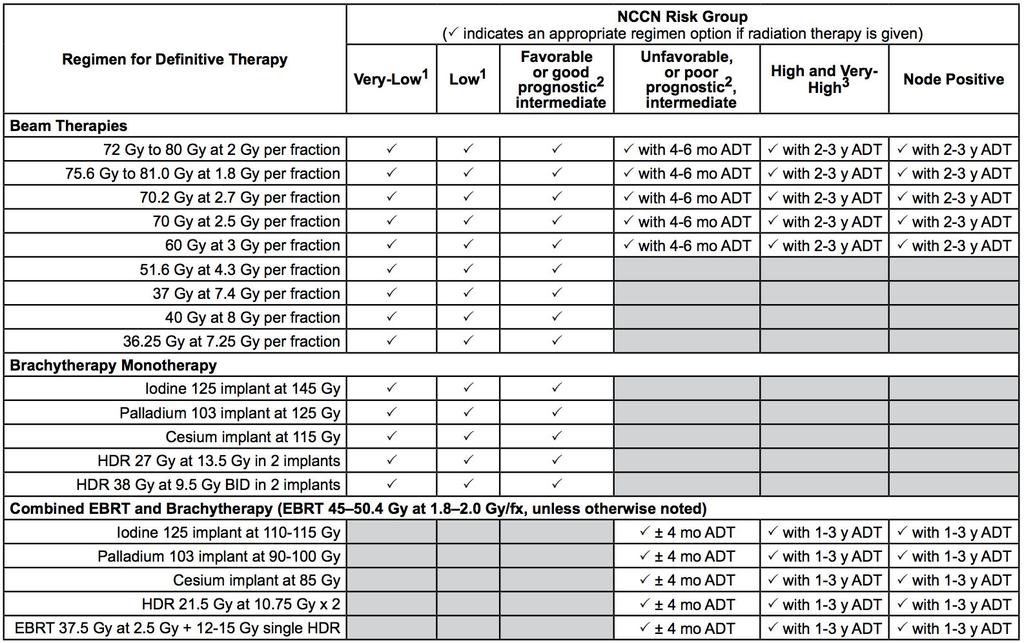
18 Standard RT options pre-2015-ish Dose-escalated EBRT: ~ Gy/fxn weeks of daily RT Monotherapy Brachytherapy: LDR or HDR EBRT + LDR/HDR Brachy BOOST
19
20
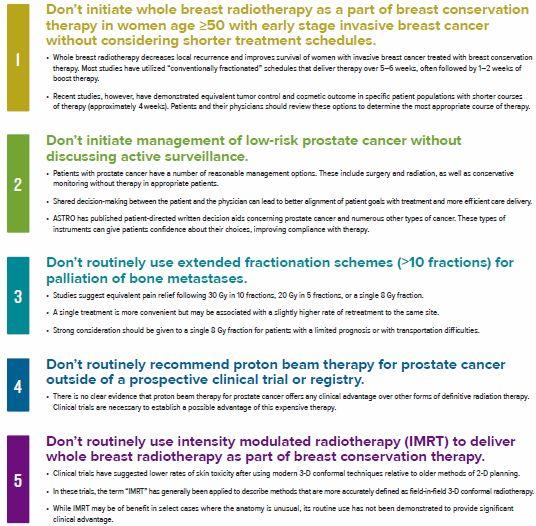
21 RadBio: α/β ratio Historically: - Tumors = HIGH α/β ratios - Fractionation spares LOW α/β ratio cells & late effects Modern: - Prostate AdenoCA = LOW α/β ratio - Highly conformal treatments sparing OAR s

22 A. Loblow, Univ or Toronto. ASTRO 2017.

23 A. Loblow, Univ or Toronto. ASTRO 2017.
24 RadBio: α/β ratio Historically: - Tumors = HIGH α/β ratios - Fractionation spares LOW α/β ratio cells & late effects Modern: - Prostate AdenoCA = LOW α/β ratio - Highly conformal treatments sparing OAR s
25 Hypotheses on hypofractionation: Biologically more effective Slows rate of progression Makes prostate cancer cells less likely to metastasize
26 Brachytherapy Grimm, et al. BJU 2012; Morris et al., IJROBP 2017; T Mitin, 2018 ASTRO Refresher
27 EBRT vs EBRT+HDR
28 ASCENDE-RT EBRT vs combination EBRT+HDR ~400 pts with unfav-int or high risk disease -1 year of ADT -Pelvic IMRT to 46 Gy (2 Gy/fxn) --> 1) IMRT BOOST of 32 Gy (78 Gy total) 2) I-125 LDR BOOST of 115 Gy

29 Morris et al., IJROBP 2017; T Mitin, 2018 ASTRO Refresher
30 ASCENDE-RT EBRT+HDR BOOST increased rates of grade 3 GU toxicity: > 19% (SS) No difference in GI toxicity > 9% (NSS) Rodda et al., IJROBP 2017
31
32 Prostate EBRT Hypofractionation Becoming the new standard of care for many cases Widely available technology advances allowing more conformality ~ Gy per fraction 4 randomized trials showing equal efficacy w/o major toxicity
33
34
35
36
37
38 Prostate SBRT Ultimate dose escalation and hypofractionation Caters to suspected LOW α/β ratio Gland immobilization and motion tracking Typically 5 fxn tx courses
39
40 Dose escalation trial: MSKCC (Zelefsky, et al.) Phase I 6.5Gy x 5 = 32.5Gy 7.0Gy x 5 = 35.0Gy 7.5Gy x 5 = 37.5Gy 8.0Gy x 5 = 40.0Gy Treatment delivery every other day PTV = prostate and SV with a 5mm circ margins and 3mm posteriorly Ferromagentic beacons for intra-fraction motion tracking
41 Dose escalation trial: MSKCC Low and intermediate risk PCa KPS 80 Prostate volume 60cc No ADT allowed IPSS 15 Exclusion: Prior TURP/stricture/prostatitis Radiographic evidence of T3-4 or N1 Zelefsky, et al. MSKCC
 Late rectal bleeding: Zelefsky, et al.")
42 Dose escalation trial: MSKCC (Zelefsky, et al.) Late rectal bleeding: Zelefsky, et al. MSKCC
43 Dose escalation trial: MSKCC (Zelefsky, et al.) Zelefsky, et al.

 Zelefsky, et al.")
44 Dose escalation trial: MSKCC (Zelefsky, et al.) Zelefsky, et al. MSKCC
45 PROCARS: LDR vs SBRT vs EBRT Low risk patients only ~5-6 yrs of f/u Loblaw A, et al. Clin Oncol. Mar 2017; 29(3):
46 PROCARS: LDR vs SBRT vs EBRT Urinary toxicity Sexual toxicity Bowel toxicity Loblaw A, et al. Clin Oncol. Mar 2017; 29(3):
47

48 Ongoing Prostate SBRT Trials Zelefsky, et al. MSKCC
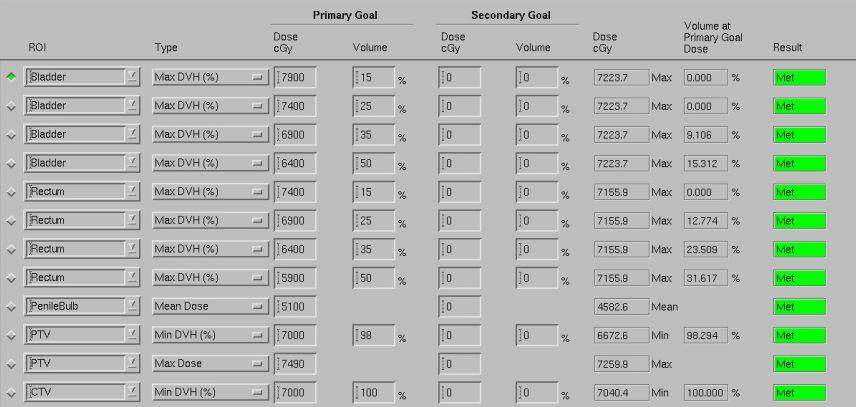
49 Published dose constraints
50

51 Cyberknife vs LINAC SBRT
52 Cyberknife vs LINAC SBRT M Cao, Ph.D. UCLA. AAPM 2014.
53 Beam selection

54 Standard protocol example M Cao, Ph.D. UCLA. AAPM 2014.

55 M Cao, Ph.D. UCLA. AAPM 2014.
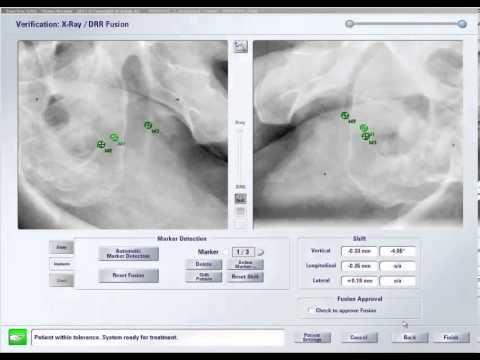
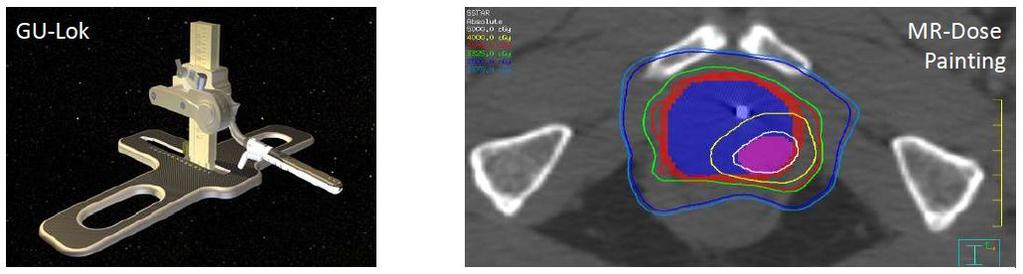
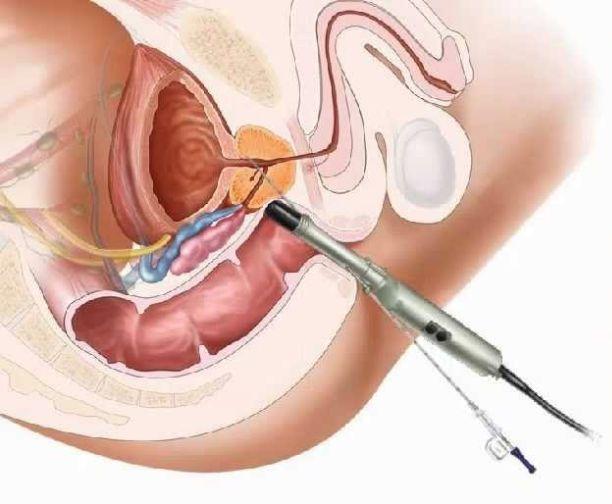
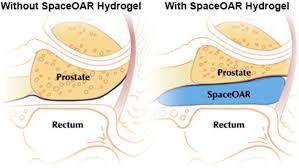
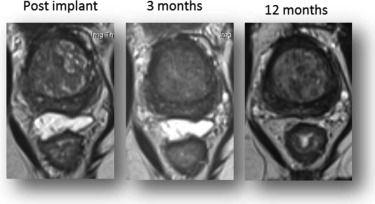
56 Immobilization and OAR sparing techniques VacLoc Fiducial markers - Calypso Daily IGRT Bladder filling Rectal gas reduction - Gasex/Beano - Rectal tube Rectal Balloon Intrafraction KV imaging - ExacTrac Real-time IGRT - Clarity SpaceOAR Hydrogel
57


58 Intrafraction IGRT, tracking, and gating
59

60
61

62 Tumor Location Identification Imaging

63 Gold Fiducial Markers

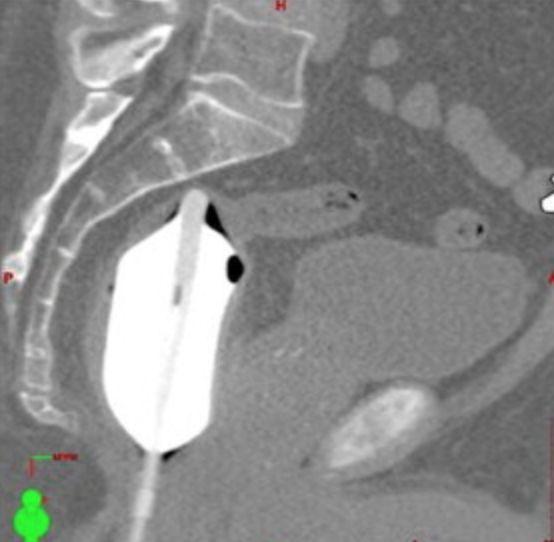
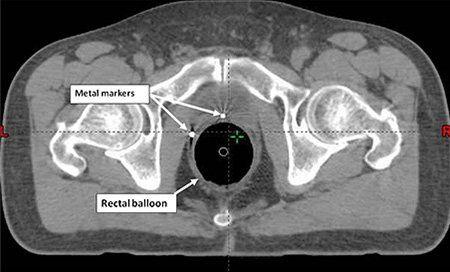
64 Rectal Balloons
65
66

67
 33% circumference: 35.1 vs 38 Gy (SS) Jones, et al. MDACC.")
68 SBRT - 45 Gy in 5 fractions Max rectal dose: 46.2 vs 42.3 Gy (SS) Rectal V45: 1.7 vs 0.3 cc (SS) 33% circumference: 35.1 vs 38 Gy (SS) Jones, et al. MDACC. Medical Dosimetry
69 Conclusions Hypofractionation via EBRT +/- Brachytherapy is becoming a new standard in many cases SBRT dose ranging from 32.5 Gy-40 Gy in 5 fx were well tolerated without significant urinary or rectal toxicities. Important and impressive technology exists for inter/intrafraction prostate gland motion to improve targeting and OAR sparing

70 THANK YOU!!!
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
2018 ASTRO Refresher Course: Prostate Cancer. Timur Mitin, MD PhD Oregon Health and Science University
 2018 ASTRO Refresher Course: Prostate Cancer Timur Mitin, MD PhD Oregon Health and Science University Disclosures UpToDate Chapter author, royalties Oregon Health and Science University Practicing Radiation
2018 ASTRO Refresher Course: Prostate Cancer Timur Mitin, MD PhD Oregon Health and Science University Disclosures UpToDate Chapter author, royalties Oregon Health and Science University Practicing Radiation
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Stereotactic ablative body radiation for prostate cancer SABR
 Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Stereotactic ablative body radiation for prostate cancer SABR John Armstrong. Sinead Callinan. Luke Rock. Beacon Hospital, Dublin, Ireland Low- Intermediate Risk Prostate Comparing treatment choices IMRT
Prostate Cancer. 3DCRT vs IMRT : Hasan Murshed
 Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT
 Donald B. Fuller, M.D. 1, John Naitoh, M.D. 2, Mark Reilly, M.D. 3, Chad Lee, Ph.D 1. 1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT Typically,
Donald B. Fuller, M.D. 1, John Naitoh, M.D. 2, Mark Reilly, M.D. 3, Chad Lee, Ph.D 1. 1. CyberKnife Centers of San Diego, CA 2. Coast Urology La Jolla, CA 3. Sletten Cancer Center Great Falls, MT Typically,
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery
 Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
Linac Based SBRT for Low-intermediate Risk Prostate Cancer in 5 Fractions: Preliminary Report of a Phase II Study with FFF Delivery FILIPPO ALONGI MD Radiation Oncology & Radiosurgery Istituto Clinico
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
LDR Monotherapy vs. HDR Monotherapy
 Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
Abstract No. 1234 LDR Monotherapy vs. HDR Monotherapy Is it time for LDR to retire? Gerard Morton 2 LDR Seed Brachytherapy First 2000 LDR patients from BCCA Low and Intermediate Risk LDR Implant Morris
FOCAL THERAPY PROSTATE SEED BRACHYTHERAPY
 FOCAL THERAPY PROSTATE SEED BRACHYTHERAPY DR. JOSEPH BUCCI MBBS,FRACP,FRANZCR ST. GEORGE CANCER CARE CENTRE PATIENT 47 2005 66 year old Recently remarried - old childhood sweetheart PSA 6.2, ct1c, Gleason
FOCAL THERAPY PROSTATE SEED BRACHYTHERAPY DR. JOSEPH BUCCI MBBS,FRACP,FRANZCR ST. GEORGE CANCER CARE CENTRE PATIENT 47 2005 66 year old Recently remarried - old childhood sweetheart PSA 6.2, ct1c, Gleason
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
The benefit of a preplanning procedure - view from oncologist. Dorota Kazberuk November, 2014 Otwock
 The benefit of a preplanning procedure - view from oncologist Dorota Kazberuk 21-22 November, 2014 Otwock Brachytherapy is supreme tool in prostate cancer management with a wide range of options in every
The benefit of a preplanning procedure - view from oncologist Dorota Kazberuk 21-22 November, 2014 Otwock Brachytherapy is supreme tool in prostate cancer management with a wide range of options in every
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica
 Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica 2014 HYPOFRACTIONATION & PROSTATE CANCER HYPOFRACTIONATION & PROSTATE CANCER: TECHNOLOGY: HIGH CONFORMAL DOSE & IMAGING
Innovazioni tecnologiche in Radioterapia" Sergio Fersino Radioterapia Oncologica 2014 HYPOFRACTIONATION & PROSTATE CANCER HYPOFRACTIONATION & PROSTATE CANCER: TECHNOLOGY: HIGH CONFORMAL DOSE & IMAGING
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
Embracing Technology & Timing of Salvage Hormones
 Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Disclosures. Proton therapy advantages. Why are comparing therapies difficult? Proton Therapy for Low Risk Prostate Cancer
 Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Proton Therapy for Low Risk Prostate Cancer Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments Andrew K. Lee, MD, MPH Associate Professor
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
Prostate Cancer Treatments. Hasan Murshed, MD., DABR Radiation Oncology Residency, UAB Fellowship, MDACC Board Certified, ABR
 Prostate Cancer Treatments Hasan Murshed, MD., DABR Radiation Oncology Residency, UAB Fellowship, MDACC Board Certified, ABR A Brief History of Radiation Wilhelm Roentgen discovered X- rays on November
Prostate Cancer Treatments Hasan Murshed, MD., DABR Radiation Oncology Residency, UAB Fellowship, MDACC Board Certified, ABR A Brief History of Radiation Wilhelm Roentgen discovered X- rays on November
Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division
 IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
IMRT / Tomo / VMAT / Cyberknife / HDR Brachytherapy: Jean Pouliot, PhD Professor and Vice Chair, Department of Radiation Oncology, Director of Physics Division Should Choices be Based on Dosimetric and
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Management. Localized Prostate Cancer. Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center
 Management of Localized Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center Disclosure Information Ad Andrew K. KLee Dr. Lee has indicated no financial relationships,
Management of Localized Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor M.D. Anderson Cancer Center Disclosure Information Ad Andrew K. KLee Dr. Lee has indicated no financial relationships,
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE
 CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
Comparing Current Options in Radiation Therapy. Howard M. Sandler, MD Ronald H. Bloom Family Chair in Cancer Therapeutics Cedars-Sinai Medical Center
 Comparing Current Options in Radiation Therapy Howard M. Sandler, MD Ronald H. Bloom Family Chair in Cancer Therapeutics Cedars-Sinai Medical Center Time Trends for Radiotherapy (and other treatments)
Comparing Current Options in Radiation Therapy Howard M. Sandler, MD Ronald H. Bloom Family Chair in Cancer Therapeutics Cedars-Sinai Medical Center Time Trends for Radiotherapy (and other treatments)
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
How to deal with patients who fail intracavitary treatment
 How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Navigating the Stream: Prostate Cancer and Early Detection. Ifeanyi Ani, M.D. TPMG Urology Newport News
 Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
IMRT RTOG Definitive IMRT for Low Risk Prostate Cancer. All about dose and dose matters, probably Although hormones may matter
 Definitive for Low Risk Prostate Cancer Howard Sandler, MD, MS Bloom Family Chair in Cancer Therapeutics Cedar-Sinai Medical Center All about dose and dose matters, probably Although hormones may matter
Definitive for Low Risk Prostate Cancer Howard Sandler, MD, MS Bloom Family Chair in Cancer Therapeutics Cedar-Sinai Medical Center All about dose and dose matters, probably Although hormones may matter
Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center
 Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center Seungtaek Choi, MD Assistant Professor Department tof fradiation
Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Associate Professor Department tof fradiation Oncology M.D. Anderson Cancer Center Seungtaek Choi, MD Assistant Professor Department tof fradiation
Neoplasie prostatiche Radioterapia: le nuove strategie
 Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
Brachytherapy for Prostate Cancer
 Brachytherapy for Prostate Cancer Who should be thinking about this and why... Juanita Crook Professor Radiation Oncology University of Toronto Princess Margaret Hospital Many options watchful waiting?
Brachytherapy for Prostate Cancer Who should be thinking about this and why... Juanita Crook Professor Radiation Oncology University of Toronto Princess Margaret Hospital Many options watchful waiting?
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER
 PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments
 Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Feasibility of 4D IMRT Delivery for Hypofractionated High Dose Partial Prostate Treatments R.A. Price Jr., Ph.D., J. Li, Ph.D., A. Pollack, M.D., Ph.D.*, L. Jin, Ph.D., E. Horwitz, M.D., M. Buyyounouski,
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
Future Directions in Prostate Cancer: The Case for Protons. John J. Coen, MD Helen & Harry Gray Cancer Center
 Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER
 CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER Klinikum Offenbach Nucletron April 27 th 28 th, 2014 History HDR Protocols for Boost and Monotherapy, Results, Logistics and Practical
CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER Klinikum Offenbach Nucletron April 27 th 28 th, 2014 History HDR Protocols for Boost and Monotherapy, Results, Logistics and Practical
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer
 Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
Phase II study of FFF-SBRT in 5 fractions for low and intermediate risk prostate cancer Ciro Franzese, G D Agostino, E Clerici, E Villa, A Tozzi, T Comito, C Iftode, AM Ascolese, F De Rose, S Pentimalli,
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy. Dr. Matt Andrews Supervisor: Dr. David Bowes
 The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Radical Prostatectomy:
 Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Proton Therapy for Prostate Cancer. Andrew K. Lee, MD, MPH Director Proton Therapy Center
 Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Director Proton Therapy Center Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments
Proton Therapy for Prostate Cancer Andrew K. Lee, MD, MPH Director Proton Therapy Center Disclosures No relevant financial disclosures This presentation will not discuss off-label or investigational treatments
10th anniversary of 1st validated CaPspecific
 Quality of Life after Treatment of Localised Prostate Cancer Dr Jeremy Grummet Clinical Uro-Oncology Fellow May 28, 2008 1 Why? This is important May be viewed as soft science Until we know which treatment
Quality of Life after Treatment of Localised Prostate Cancer Dr Jeremy Grummet Clinical Uro-Oncology Fellow May 28, 2008 1 Why? This is important May be viewed as soft science Until we know which treatment
D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy combined HDR + EBRT 574 HDR monotherapy Total Patients
 Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD
 Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
BRACHYTHERAPY FOR PROSTATE CANCER. Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital
, FRANZCR Radiation Oncologist, The Canberra Hospital") BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
The role of Radiation Oncologist: Hi-tech treatments for liver metastases
 The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate cancer: Update from the BCCA
 Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing
Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing
Partial Breast Irradiation using adaptive MRgRT
 Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Partial Breast Irradiation using adaptive MRgRT Shyama Tetar, radiation-oncologist VUmc Amsterdam 15-12-2017 5 th Vumc SBRT symposium 2017 Current practice Breast conserving treatment (BCT) Breast conserving
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Intensity Modulated Radiotherapy (IMRT) of the Prostate
 of the Prostate") Medical Policy Manual Medicine, Policy No. 137 Intensity Modulated Radiotherapy (IMRT) of the Prostate Next Review: August 2018 Last Review: November 2017 Effective: December 1, 2017 IMPORTANT REMINDER
Medical Policy Manual Medicine, Policy No. 137 Intensity Modulated Radiotherapy (IMRT) of the Prostate Next Review: August 2018 Last Review: November 2017 Effective: December 1, 2017 IMPORTANT REMINDER
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
PROSTATE CANCER TREATMENT
 PROSTATE CANCER TREATMENT INFORMATION GUIDE Several effective treatment options exist today for men diagnosed with prostate cancer. Each man s particular cancer, overall health, age, and lifestyle will
PROSTATE CANCER TREATMENT INFORMATION GUIDE Several effective treatment options exist today for men diagnosed with prostate cancer. Each man s particular cancer, overall health, age, and lifestyle will
Radiotherapy Advances
 Radiotherapy Advances Not Radiotherapy Principles IMRT IGRT Image Fusion Planning Introduction IMRT = Intensity Modulated RadioTherapy Restriction: IMRT with photon beams IMRT: Highly conformal technique
Radiotherapy Advances Not Radiotherapy Principles IMRT IGRT Image Fusion Planning Introduction IMRT = Intensity Modulated RadioTherapy Restriction: IMRT with photon beams IMRT: Highly conformal technique
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
How can we Personalize RT as part of Breast-Conserving Therapy?
 How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update
 Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update DONALD B. FULLER, M.D. RADIATION ONCOLOGIST GENESIS HEALTHCARE Disclosure & Disclaimer The
Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update DONALD B. FULLER, M.D. RADIATION ONCOLOGIST GENESIS HEALTHCARE Disclosure & Disclaimer The
Stereotactic Ablative Radiotherapy for Prostate Cancer
 Stereotactic Ablative Radiotherapy for Prostate Cancer Laurie Cuttino, MD Associate Professor of Radiation Oncology VCU Massey Cancer Center Director of Radiation Oncology Sarah Cannon Cancer Center at
Stereotactic Ablative Radiotherapy for Prostate Cancer Laurie Cuttino, MD Associate Professor of Radiation Oncology VCU Massey Cancer Center Director of Radiation Oncology Sarah Cannon Cancer Center at
3/6/2018 PROSTATE CANCER IN 2018 OBJECTIVE WHAT IS THE PROSTATE? WHAT DOES IT DO? Rahul Mehan, MD
 PROSTATE CANCER IN 2018 Rahul Mehan, MD East Valley Urology Center 6116 E Arbor Ave, Bldg 2, Suite 108 Mesa, AZ 85206 rmehan@evucenter.com www.evucenter.com Snapchat: Dr.NoodleKing OBJECTIVE Offer interactive
PROSTATE CANCER IN 2018 Rahul Mehan, MD East Valley Urology Center 6116 E Arbor Ave, Bldg 2, Suite 108 Mesa, AZ 85206 rmehan@evucenter.com www.evucenter.com Snapchat: Dr.NoodleKing OBJECTIVE Offer interactive
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation. Roberto Alonzi Mount Vernon Cancer Centre
 The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
The Paul Evans Memorial Lecture Functional radiotherapy targeting using focused dose escalation Roberto Alonzi Mount Vernon Cancer Centre Overview Introduction and rationale for focused dose escalation
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
SRO Tutorial: Prostate Cancer Clinics
 SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017
 Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017 Relevant Disclosures Advisory role, ownership interest, previous unrestricted grant
Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017 Relevant Disclosures Advisory role, ownership interest, previous unrestricted grant
Section: Therapy Effective Date: October 15, 2016 Subsection: Therapy Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
MRI Applications in Radiation Oncology:
 MRI Applications in Radiation Oncology: Physician s Perspective Jeff Olsen, MD Department of Radiation Oncology Washington University, St. Louis, MO Disclosures Washington University has research and service
MRI Applications in Radiation Oncology: Physician s Perspective Jeff Olsen, MD Department of Radiation Oncology Washington University, St. Louis, MO Disclosures Washington University has research and service
Intensity-Modulated and Image- Guided Radiation Treatment. Outline. Conformal Radiation Treatment
 Intensity-Modulated and Image- Guided Radiation Treatment J. Daniel Bourland, PhD Professor Departments of Radiation Oncology, Physics, and Biomedical Engineering Wake Forest University School of Medicine
Intensity-Modulated and Image- Guided Radiation Treatment J. Daniel Bourland, PhD Professor Departments of Radiation Oncology, Physics, and Biomedical Engineering Wake Forest University School of Medicine
PROSTATE CANCER SURVEILLANCE
 PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Changing Paradigms in Radiotherapy
 Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
Changing Paradigms in Radiotherapy Marco van Vulpen, MD, PhD Mouldroomdag-2015 Towards the elimination of invasion 1 NIH opinion on the future of oncology Twenty-five years from now,i hope that we won
DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS
 DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS Andrius IVANAUSKAS*, Eduardas ALEKNAVIČIUS*, Arvydas BURNECKIS*, Albert MILLER *Institute of Oncology Vilnius
DOSIMETRIC OPTIONS AND POSSIBILITIES OF PROSTATE LDR BRACHYTHERAPY WITH PERMANENT I-125 IMPLANTS Andrius IVANAUSKAS*, Eduardas ALEKNAVIČIUS*, Arvydas BURNECKIS*, Albert MILLER *Institute of Oncology Vilnius
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
HDR Brachytherapy I: Overview of Clinical Application and QA. Disclosures. Learning Objectives 7/23/2014. Consultant, Varian Medical Systems
 HDR Brachytherapy I: Overview of Clinical Application and QA Timothy Showalter, MD Associate Professor tns3b@virginia.edu Disclosures Consultant, Varian Medical Systems Learning Objectives To understand
HDR Brachytherapy I: Overview of Clinical Application and QA Timothy Showalter, MD Associate Professor tns3b@virginia.edu Disclosures Consultant, Varian Medical Systems Learning Objectives To understand
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Tanaka et al. BMC Cancer (2017) 17:573 DOI /s
 17:573 DOI /s") Tanaka et al. BMC Cancer (2017) 17:573 DOI 10.1186/s12885-017-3565-1 RESEARCH ARTICLE Comparison of PSA value at last follow-up of patients who underwent low-dose rate brachytherapy and intensity-modulated
Tanaka et al. BMC Cancer (2017) 17:573 DOI 10.1186/s12885-017-3565-1 RESEARCH ARTICLE Comparison of PSA value at last follow-up of patients who underwent low-dose rate brachytherapy and intensity-modulated
Rush University Medical Center RUMC XXXX
 Date: 03/10/2016 Rush University Medical Center RUMC XXXX A PROSPECTIVE EVALUATION OF MULTI-PARAMETRIC MAGNETIC RESONANCE IMAGING (mpmri) GUIDED STEREOTACTIC BODY RADIATION TREATMENT FOR LOCALIZED PROSTATE
Date: 03/10/2016 Rush University Medical Center RUMC XXXX A PROSPECTIVE EVALUATION OF MULTI-PARAMETRIC MAGNETIC RESONANCE IMAGING (mpmri) GUIDED STEREOTACTIC BODY RADIATION TREATMENT FOR LOCALIZED PROSTATE
Newer Aspects of Prostate Cancer Underwriting
 Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
PACE Study. Hypofractionation 17/12/2014. Traditional Model of Fractionation 200 Response. What s the fraction sensitivity of prostate cancer?
 0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO
 LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO BARD 20 NOVEMBRE 2010 DI MUZIO NADIA H. S. RAFFAELE MILANO PHASE I-II STUDY OF HYPOFRACTIONATED SIMULTANEOUS INTEGRATED BOOST WITH TOMOTHERAPY FOR PROSTATE
LA TOMOTERAPIA IN ITALIA: ESPERIENZE A CONFRONTO BARD 20 NOVEMBRE 2010 DI MUZIO NADIA H. S. RAFFAELE MILANO PHASE I-II STUDY OF HYPOFRACTIONATED SIMULTANEOUS INTEGRATED BOOST WITH TOMOTHERAPY FOR PROSTATE