New treatments in melanoma
|
|
|
- Cynthia Norman
- 6 years ago
- Views:
Transcription
1 New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy
2 Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine progression-free and overall survival benchmarks for future Phase II trials This metanalysis summarises the outcome of advanced melanoma patients before 2011 Median survival time 6.2 months Alive at 1 year 25.5% Median PFS 1.7 months Progression free at 6 months 14.5% Korn E, et al. J Clin Oncol 2008;26: Reprinted with permission 2008, American Society of Clinical Oncology. All rights reserved
3 Treatment for advanced melanoma approved by EMA after ipilimumab 2012 vemurafenib 2013 dabrafenib 2014 trametinib 2015 nivolumab pembrolizumab combo dabrafenib-trametinib combo vemurafenib-cobimetinib talimogene laherparepvec pending combo ipilimumabnivolumab Agent Company Indication Nivolumab BMS Unresectable or metastatic melanoma Ipilimumab BMS Unresectable or metastatic melanoma Vemurafenib Roche/Genentech Unresectable or metastatic melanoma with BRAF V600E mutation Dabrafenib Novartis Unresectable or metastatic melanoma with BRAF V600E mutation Trametinib Novartis Unresectable or metastatic melanoma with BRAF V600E/K mutation Talimogene laherparepvec Amgen Unresectable melanoma that is regionally or distantly metastatic (Stage IIIB, IIIC, and IVM1a) with no bone, brain, lung, or other visceral disease. Hodi FS, et al. N Engl J Med 2010;363:711 23; Chapman PB, et al. J Clin Oncol 2012;30(suppl; abstr 8502). Hauschild A, et al. Lancet 2012;380:358 65; Flaherty KT, et al. N Engl J Med 2012;367:107 14; Flaherty KT, et al. N Engl J Med 2012;367: ; Robert C, et al. N Engl J Med 2015;372:320 30; Andtbacka R, et al. J Clin Oncol Sep 1;33(25):
 Slow")
 Quick action, rapid metabolic")

4 Two different drugs... Two different concepts Ipilimumab (immunotherapy) Slow action, but it is able to make the disease chronic BRAF inhibitors (target therapy) Quick action, rapid metabolic shutdown, unfortunately resistance after a median of 6-8 months Oct-2010 Jun-2011 Day 0 Day 15 Courtesy of Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy

5 Advanced melanoma: Different approaches according to mutational status BRAF V600E/K Q61 NRAS c-kit NRAS wt BRAF wt Ascierto PA, et al. J Transl Med. 2012;10:83
6 TARGET THERAPY
7 BRAF inhibitors VEMURAFENIB DABRAFENIB

8 Growth factors RAS RAF pathway MAPK pathway and BRAF inhibitors mechanism of action Oncogenic BRAF signaling Oncogenic BRAF signaling arrested with BRAF inhibitors RTK RAS GTP (activated RAS) Constitutive activation is independent of extracellular factors and does not respond to biochemical signals that would normally regulate activity Normal activation of RAS via extracellular factors at the inner cell membrane via RTK PP PP BRAF MEK ERK BRAF V600 PP MEK PP ERK BRAF V600 MEK ERK BRAF inhibitors Selective binding of oncogenic BRAF kinase by vemurafenib, blocks the constitutively activated pathway and downstream activity Normal cell proliferation and survival cell proliferation and survival cell proliferation and survival Ascierto PA, et al. J Trans Med 2012;10:85. This work is licensed under a Creative Commons Attribution 4.0 International License
9 Vemurafenib and dabrafenib: Data from the BRIM-3 and BREAK-3 studies BRIM-3 Randomised Phase III open label vemurafenib vs. dacarbazine Primary endpoint: OS Cross-over: no Patients enrolled: 675 (337 vemurafenib; 338 dacarbazine) Median follow-up: 12.5 mo Median OS: 13.6 mo vemurafenib vs. 9.7 mo dacarbazine HR = 0.70 (95% CI ); p= ORR: 57% vemurafenib vs. 9% dacarbazine PFS: median PFS was 5.9 months for vemurafenib and 1.7 mo for dacarbazine (HR 0.30, 95% CI ; p<0.0001) BREAK-3 Randomised Phase III open label dabrafenib vs. dacarbazine Primary endpoint: PFS Cross-over: Yes Patients enrolled: 250 (187 dabrafenib; 63 dacarbazine) Median follow-up time: 16.9 mo Median OS: 20 mo dabrafenib vs.15.6 mo dacarbazine HR = 0.77 (95% CI ); p=not significant ORR: 50% dabrafenib vs. 6% dacarbazine PFS: median PFS was 6.9 mo for dabrafenib versus 2.7 mo for dacarbazine (HR = 0.37, 95% CI ; p<0.0001) 9,7 13,6 McArthur G, et al. Lancet Oncol 2014;15: Reprinted from The Lancet 2014, with permission from Elsevier Hauschild A, et al. Lancet 2012;380:358 65; Hauschild A, et al. J Clin Oncol 2013 ASCO Annual Meeting Abstracts;31 suppl May:9013; By permission of Hauschild A, et al. ESMO Poster 1092
10 AE (%) BRAF inhibitors*: AEs (grade 2 in 5% patients) Vemurafenib (n=336) Dabrafenib (n=187) Grade 2 Grade 3 Grade 2 Grade 3 Arthralgia <1 Rash 10 8 NR NR Fatigue cuscc/keratoacanthoma Nausea 7 1 NR NR Alopecia 8 NR NR Pruritus 6 1 NR NR Hyperkeratosis a Diarrhoea 5 <1 NR NR Headache 4 <1 5 Pyrexia NR NR 8 3 PPE/palmar-plantar hyperkeratosis NR NR 6 2 *Data from BRIM-3 and BREAK-3 trials a Includes 1 (<1%) patient with grade 4 event AEs = adverse events; cuscc = cutaneous squamous-cell carcinoma; NR = not reported; PPE = palmar-plantar Chapman erythrodysaesthesia PB, et al. N Engl J Med 2011;364: ; Hauschild A, et al. Lancet 2012;380: Adapted from Ascierto PA, et al. Am J Ther. 2015; 22:44-53
11 The paradoxical effect of BRAF inhibitors Hatzivassiliou et al., Heidorn et al. and Poulikakos et al. described how RAF inhibitors can drive downstream ERK signaling in the absence of BRAF mutations, contributing to resistance in tumours treated with these drugs BRAF inhibitors reduce ERK activation with subsequent tumour regression. In case of lacking BRAF mutation but in presence of a mutant form of a RAS protein, activated RAS binds and stimulates BRAF-CRAF or CRAF-CRAF dimers to switch on the ERK pathway This promotes tumour growth in NRAS-mutant melanoma or can induce a premalignant lesion in other tissues. On treatment with BRAF inhibitors, binding of the drug to one RAF subunit transactivates the other, in cooperation with RAS interaction, resulting in paradoxical ERK activation and tumour progression Hatzivassiliou G, et al. Nature 2010;464:431 5; Heidorn SJ, et al. Cell 2010;140:209 1; Poulikakos PI, et al. Nature 2010; 464:427 30; Reprinted by permission from Macmillan Publishers Ltd: Downward J, et al. Nature Med 2011;17:286 8, 2011

![21,6 months [95% CI 17 5 not reached] Reprinted from Larkin J, et](/docs-images/71/65975277/images/12-2.jpg "al. Lancet Oncol 2014;15:436 44.")
12 Factors significantly associated with longer median PFS and OS: LDH level PFS Median PFS 7,6 months [95% CI ] OS Median OS 21,6 months [95% CI 17 5 not reached] Reprinted from Larkin J, et al. Lancet Oncol 2014;15: , with permission from Elsevier
13 Proportion alive Factors significantly associated with longer median PFS and OS: LDH level (cont d) OS extended follow-up in V600E-mutant positive patients enrolled 1.0 in BREAK-2 study V600E: 0.7 Median OS 13.1 months 0.6 (95% CI: ) Time since first dose, months Number 76 at risk Median follow-up of 13 months In the BRAF V600E group, 21 patients (28%) were alive beyond 30 months All these patients had a baseline normal LDH As of 9 December 2013, 8 (9%) patients continued on dabrafenib without disease progression (median exposure of 37 months) Data cut off: December 2013 Ascierto PA, et al. J Clin Oncol 2014;32:5s(suppl; abstr 9034). Poster presented at ASCO 2014
 Long-term survival with vemurafenib can be achieved in patients with low baseline tumour burden Baseline targets, PFS & OS TARGETS <11.5 cm TARGETS 11.")
14 Factors significantly associated with longer median PFS and OS: Tumour burden Prolonged responses to vemurafenib in patients with BRAFV600-mutant melanoma with low tumour burden at baseline: data from the phase I study (BRIM-1) Long-term survival with vemurafenib can be achieved in patients with low baseline tumour burden Baseline targets, PFS & OS TARGETS <11.5 cm TARGETS 11.5 cm Median PFS Median OS BREAK-3 Long-term responders on dabrafenib were observed to have smaller lesions at baseline vs. patients that experienced disease progression. Indeed, 10% of patients continued to receive dabrafenib without disease progression at data cut-off. The 72% of them had a low tumour burden With permission from Amaravadi R, SMR-P3, presented at SMR Congress Tampa, Florida November 2011 Hauschild A, et al. Poster presented at ESMO 2014, Poster 1092PD, Abstract 5785.







15 Effect of BRAF inhibitors on the immune system BRAF inhibition is associated with increased melanoma antigen expression in tumours of patients with metastatic melanoma CD4+ and CD8+ increase in responder lesion and decrease in lesions which progressed Antitumour activity of combined BRAFi+MEKi plus anti-pd-1 3 MHC and melanoma antigen expression 3 BRAF inhibition is associated with increased CD8+ T-cell infiltrate in tumours of patients with metastatic melanoma Wilmott JS, et al. Clin Cancer Res 2011;18: , Reprinted from Clinical Cancer Research 2012, with permission from AACR Frederick DT, et al. Clin Cancer Res 2013;19: , Reprinted from Clinical Cancer Research 2013, with permission from AACR From Hu-Lieskovan S, et al. Sci Transl Med 2015;7:279ra41., Reprinted with permission from AAAS






16 Resistance BRAF-mutant melanomas acquire BRAF inhibitor resistance via upregulation of both MAPK and PI3K AKT pathways. However, MAPK reactivation is the major pathway of acquired BRAF inhibitor resistance in melanoma. Among MAPK-reactivating mechanisms associated with acquired BRAF inhibitor resistance the most frequents are NRAS mutations, mutant BRAF amplification and alternative splice variants, MAP2K1 and CDKN2A mutations Shi H, et al. Cancer Discovery 2014; 4:80-93 Courtesy of Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Day 0 Day 7 Day 15 Day 30
17 BRAF plus MEK inhibitors DABRAFENIB + TRAMETINIB VEMURAFENIB + COBIMETINIB ENCORAFENIB + BINIMETINIB
 5 improved response rates and PFS in BRAF")
18 Rationale for the combination of BRAF and MEK inhibitors Rationale Most common mechanism of acquired resistance to vemurafenib is MAPK reactivation through MEK 1,2 MEK + BRAF inhibition prevents the development of acquired resistance in preclinical models 3 MEK + BRAF inhibition (dabrafenib + trametinib 4 phase 3 and vemurafenib + cobimetinib phase 1/2) 5 improved response rates and PFS in BRAF inhibitor naive melanoma patients Reduced incidence of hyperproliferative lesions by blocking paradoxical activation of the MAPK pathway from RAF inhibition 6 BRAF inhibitors vemurafenib dabrafenib encorafenib MEK inhibitors trametinib cobimetinib binimetinib 1. Shi H, et al. Cancer Discov Trunzer K, et al. J Clin Oncol Paraiso K, et al. Br J Cancer Long GV, et al. J Clin Oncol Ribas A, et al. Lancet Oncol Su F, et al. New Engl J Med Gowrishankar et al.; licensee InTech. ISBN: , DOI: / Available from: Open access article distributed under the terms of the Creative Commons Attribution License 3.0
19 Estimated Survival Function Results from the fase I/II dabrafenib/ trametinib Cohort 150/2 Median: 25 mo 12-mo OS rate: 80% 24-mo OS rate: 51% 36-mo OS rate: 38% Cohort Dabrafenib 150 mg BID Dabrafenib 150 mg BID/trametinib 1 mg QD Dabrafenib 150 mg BID/trametinib 2 mg QD 0.0 Patients at Risk Data as of 15 January 2015 Time Since Randomization, months Longer follow-up reveals median OS of 25 months for patients in the 150/2 cohort. Landmark OS results for the 150/2 cohort: 1 year, 80%; 2 year, 51%; 3 year, 38%. Normal LDH and fewer disease sites were associated with prolonged survival. Prior immunotherapy had no effect on OS. No new safety signal observed and no increase in cuscc cases or treatment-emergent malignancies Daud A, et al. ASCO 2015, J Clin Oncol 2015;33 (suppl; abstr 9036) Poster 279 (with permission of Daud A.)
20 Combi-D study: Phase III study which compared dabrafenib/trametinib to dabrafenib monotherapy The combination dabrafenib/trametinib improved PFS and OS: PFS HR was 0,67, and OS HR was 0,71 with 1-year OS rate of 74% and 2-years OS rate of 51%. The median OS was 25,1 months. The treatment was well tolerated and the toxicity was manageable Long G, et al. N Engl J Med 2014; 371: Reprinted from Long G, et al. Lancet 2015;386: , with permission from Elsevier

21 Combi-V study: Phase III study which compared dabrafenib/trametinib to vemurafenib monotherapy PFS OS Median Follow-up: D + T = 11 months and Vem = 10 months Robert C, et al. N Engl J Med 2015; 372:30-9. Copyright 2015 Massachusetts Medical Society.Reprinted with permission from Massachusetts Medical Society,
22 CoBrim study: Phase III study which compared vemurafenib/cobimetinib to vemurafenib monotherapy PFS OS With permission from Larkin J, et al. J Clin Oncol 2015;33(suppl. Abstr 9006). Larkin J, et al. N Engl J Med 2015;373: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
23 Comparison between vemurafenib and dabrafenib/trametinib or vemurafenib/cobimetinib: PFS D+T V+C dabra/trame PFS = 11,4 months vs HR = 0,56 vemu = 7,3 months ORR = 64 % vs. 51% vemu/cobi PFS = 12,3 months vs HR = 0,58 vemu = 7,2 months ORR = 70% vs. 50% Robert C, et al. N Engl J Med 2015; 372:30-9. Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society With permission from Larkin J, et al. J Clin Oncol 2015;33(suppl. Abstr 9006).
24 Comparison between vemurafenib and dabrafenib/trametinib or vemurafenib/cobimetinib: OS D + T HR = 0.69 (95% CI ) P = V + C HR = 0.65 (95% CI ) P = Robert C, el al. N Engl J Med 2015; 372:30-9. Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society Larkin J, et al. N Engl J Med 2015;373: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
25 Overall safety summary for Combi-V and CoBrim studies Combi-V D + T (n=350) CoBrim V + C (n=254) Patients with at least 1 AE, n (%) 343 (98) 250 (98) Grade 3 AE, n (%) 184(54) 165 (65) AEs leading to permanent discontinuation, n (%) 44 (13) 32 (13) Any SAE, n (%) 131 (37) 75 (30) Fatal SAEs, n (%) 3 (< 1) 6 (2) Robert C, et al. N Engl J Med 2015;372:30-9. Larkin J, et al. N Engl J Med 2015;373:23-34.
26 Overall safety summary for Combi-V and CoBrim studies: AEs in > 20% patients D + T (n=350) V + C (n=254) AE (%) All grades Grade 3/4 All grades Grade 3/4 Pyrexia Nausea 35 <1 39 <1 Diarrhoea Fatigue Vomiting Hypertension Arthralgia 24 < Rash Pruritus 9 0 NR NR Hyperkeratosis Photosensitivity Increased LFTs NR NR 16 <1 NR = not reported Robert C, et al. N Engl J Med 2015; 372:30-9. Larkin J, et al. N Engl J Med 2015;373:23-34.
27 Overall safety summary for Combi-V and CoBrim studies: Selected adverse events D + T (n=350) V + C (n=254) AE (%) All grades Grade 3/4 All grades Grade 3/4 Cutaneous small-cell carcinoma and keratoacanthoma 1 0 <1 3 Increased CPK NR NR Retinal detachment NR NR 8 2 Chorioretinopathy <1 NR 12 <1 QT prolongation NR NR 3 <1 Decreased ejection fraction 8 NR 7 1 NR = not reported In the majority of cases asymptomatic and resolved without treatment Robert C, et al. N Engl J Med 2015; 372:30-9. Larkin J, et al. N Engl J Med 2015;373:23-34.
 and PFS (11.3 months) are consistent with other BRAFi/MEKi combinations.")
28 Encorafenib plus binimetinib: A new combination Combination of encorafenib and binimetinib is well tolerated and shows promising activity for BRAFinhibitor naïve, BRAF-mutant melanoma. Response rate (74,5%) and PFS (11.3 months) are consistent with other BRAFi/MEKi combinations. Lower rates of pyrexia and photosensitivity distinguishes this combination from dabrafenib/trametinib and vemurafenib/cobimetinib. Further evaluation of this combination is underway: COLUMBUS (ENCO/BINI vs. ENCO vs. vemurafenib). Sullivan RJ, et al. ASCO 2015, abstract 9007, With permission from Sullivan RJ
29 IMMUNOTHERAPY
30 Anti-CTLA-4 IPILIMUMAB

31 Mechanism of action T-Lymphocyte activation requires two signals Simeone E and Ascierto PA. J Immunotoxicol 2012:9: Reprinted by permission of Taylor & Francis Ltd.
32 The MDX study: Randomised Phase III, double blinded, three arms study which compared ipilimumab + gp100 vs. ipilimumab + placebo vs. gp100 + placebo N=676 pretreated advanced melanoma patients were enrolled. Randomisation was 3:1:1 and the primary endpoint was OS No separation in curves for the first 3 months Separation and survival impact occurs after 3 months (~ 4 months improvement in median OS Near doubling of 1 and 2 years when we start to see durable long-term survivors Median OS ipi + gp100 = 10,0 mos Ipi + placebo = 10,1 mos gp100 + placebo = 6,4 mos Hodi SF, et al. New Engl J Med 2010;363:711-23, Copyright 2010 Massachussetts Medical Society. Reprinted with permission from Massachussetts Medical Society
33 Proportion alive CTLA-4 immune checkpoint pathway inhibition using ipilimumab: Pooled OS data from melanoma patients In a pooled analysis of 12 studies, an OS plateau starts at approximately 3 years with follow-up of up to 10 years in some patients N=1861 Median OS, months (95% CI): 11.4 ( ) a 3-year OS rate, % (95% CI): 22 (20 24) a Ipilimumab CENSORED Months Patients at risk Ipilimumab Schadendorf D, et al. J Clin Oncol 2015;33: Reprinted with permission American Society of Clinical Oncology. All rights reserved
34 Ipilimumab activity is independent by the mutational status Ascierto PA, et al. J Trans Med 2014:12:116. Open Access article distributed under the terms of the Creative Commons Attribution License 4.0
35 No effect in surrogate endpoints Best Overall Response Rate (BORR) ipi + gp100 = 5.7% Ipi + placebo = 10,9% gp100 + placebo = 1.5% Hodi FS, et al. New Engl J Med 2010;363: Copyright 2010 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society


36 The concept of pseudo-progression Reprinted from Ribas A, et al. Clin Cancer Res 2009;15: With permission from AACR
37 Immuno-related response criteria (irrc): Patterns of response to ipilimumab The four response patterns observed in advanced melanoma patients treated with ipilimumab in clinical studies. The new patterns of responses consider response after initial increase in total tumour burden, and response in index and new lesions after the appearance of new lesions Reprinted from Wolchok JD, et al. Clin Cancer Res 2009; 15: , With permission from AACR
38 Evolution of the antitumoural effect One of the characteristics of ipilimumab is the possibility to achieve SD, PR, or CR after a «pseudo» progression of the disease (see immuno-related Response Criteria). In order to catch these responses, it is recommended to perform the first assessment at week 16 (instead of week 12), and, in case of progression, this should be confirmed with another CT scan after 4 weeks Total volume of tumour * 25% 50% 100% Basal SD PR CR * Tumoural volume can include infiltrating lymphocytes and tumoural cells PD SD PR CR Models of response Adapted from Wolchok JD, et al. Clin Cancer Res 2009;15:
39 Safety profile: Most common immunorelated adverse events (grades 3 4) experienced in the MDX study The most common immuno-related adverse events occur in the skin, gastrointestinal apparatus (colitis, diarrhea), liver, and endocrinopathies (thyroiditis and hypophisitis). Ocular, neurological, and renal are less frequent irae (%) Ipi + gp100 (N=380) Patients (%) Ipi + placebo (N=131) Grade 3 Grade 4 Grade 3 Grade 4 Any Dermatologic Gastro-intestinal (colitis, diarrhoea) Endocrinopathies Hepatic Death due to irae Hodi FS, et al. New Engl J Med 2010;363:711-23
40 Safety profile: Real world experience the Italian Expanded Access Programme The safety profile of ipilimumab found in a real world experience (Italian expanded access programme of ipilimumab) was consistent with those found in clinical studies 12:116 12:116 12:116 12:116 Ascierto PA, et al. J Trans Med 2014:12:116

41 Treatment guidelines: Managing iraes early enables completion of 12-week induction cycle Most ipilimumab iraes managed with product-specific treatment guidelines iraes, including grade ¾, generally managed with 3-step approach Ascierto PA, et al. Am J Ther 2015;22:44-53
42 Anti-PD-1 NIVOLUMAB PEMBROLIZUMAB
 and PDL2 in various cell types that can affect anti-tumour immunity Anti-PD-1 antibodies prevent the link")

43 Mechanisms of action of PD1, PDL1 and PDL2 The roles of programmed cell death protein 1 (PD1), programmed cell death protein 1 ligand 1 (PDL1) and PDL2 in various cell types that can affect anti-tumour immunity Anti-PD-1 antibodies prevent the link PD-1/PD-L1 removing the negative signal generated by this interaction Reprinted by permission from Macmillan Publishers Ltd: Nguyen LT, et al. Nat Rev Immunol 2015;15: Copyright 2015 Reprinted from Zang X, et al. Clin Cancer Res 2007;13:5271 9, with permission from AACR
44 Nivolumab: Data from the Phase I study (CA ) The dosage selected for the Phase 3 studies was 3 mg/kg every two weeks on the basis of the higher response rate (41%) reached by this schedule. With this dosage the median PFS and OS was 10 months and 20 months respectively, while the duration of response was 22 months. In all cohorts patients the 1-, 2-, 3-, 4-years OS rate was 63%, 48%, 42%, 32% respectively Topalian S, et al. NEJM 2012; 366: ; Topalian S, et al. J Clin Oncol. 2014;32 (10): Reprinted with permission American Society of Clinical Oncology. All rights reserved Hodi FS, et al. SMR 2014 Congress. Pigment Cell Melanoma Res 2014;27:1199
 Nivolumab ICC In patients with advanced melanoma who have progressed despite anti-ctla-4 therapy, and BRAF inhibitors if BRAF mutated, nivolumab monotherapy")
45 Nivolumab: Data from the randomised Phase III study in ipilimumab pre-treated patients (CA ): Nivolumab vs. investigator chemotherapy choiche (ICC) Nivolumab ICC In patients with advanced melanoma who have progressed despite anti-ctla-4 therapy, and BRAF inhibitors if BRAF mutated, nivolumab monotherapy demonstrated superior efficacy to ICC: Objective response rate of 32% with nivolumab compared to 11% with ICC. Majority (95%) of responses were ongoing in patients who received nivolumab; median DOR not reached. Responses were observed regardless of pre-treatment PD-L1 expression status, BRAF mutation status, and prior anti-ctla-4 benefit Reprinted from Weber J, et al. Lancet Oncol 2015;16:375-84, 2015 with permsssion from Elsevier
, PFS (mpfs 5,1 mos vs.")
46 Nivolumab: Data from the randomised Phase III study in first line in BRAF wt advanced melanoma patients (CA ): Nivolumab vs. dacarbazine In treatment-naïve, BRAF wild-type patients with metastatic melanoma, nivolumab led to significant improvements over dacarbazine in OS (mos NR vs. 10,8 mos; HR 0,42), PFS (mpfs 5,1 mos vs. 2,2 mos; HR 0,43), ORR (40% vs. 13,9%). The survival benefit of nivolumab vs. dacarbazine was observed irrespective of tumour PD-L1 status, and across all pre-defined subgroups From Robert C, et al. N Engl J Med 2015;372:320-30, Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
 there was a 8% of patients")




47 Unconventional responses in patients treated with nivolumab CA CA In both the two randomised phase III studies (CA and CA ) there was a 8% of patients who progressed according with RECIST v1.1 criteria, but achieved or maintained a 30% reduction in the target lesion tumour burden ( immune-related, unconventional response pattern ) For this reason, together the classical RECIST criteria, we must consider immunorelated criteria even for nivolumab treatment By permission of Weber J, Weber J, et al. ESMO 2014 Congress; September 26-30, 2014; Madrid, Spain. Abstract LBA3. Weber J, et al. Lancet Oncol 2015; 16:375-84, Reprinted from The Lancet, Copyright 2015, with permission from Elsevier. From Robert C, et al. N Engl J Med 20145;372: Supplementary material. Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.
48 Nivolumab safety profile: Selected immuno-related adverse events experienced in the Phase I-III trials Select AE organ category patients, n (%) Nivolumab CA n. 107 pts Any Grade Grade 3 4 Nivolumab CA n. 268 pts Any Grade Grade 3 4 Nivolumab CA n. 206 pts Any Grade Grade 3 4 Skin 36 (38) 2 (2) 78 (29) 1 (<1) 77 (37) 3 (2) Gastrointestinal 18 (19) 2 (2) 31 (12) 3 (1) 35 (17) 3 (2) Endocrine 13 (14) 2 (2) 21 (8) 0 (0) 15 (7) 2 (1) Hepatic 7 (7) 1 (1) 12 (5) 2 (1) 15 (7) 2 (1) Pulmonary 4 (4) 0 6 (2) 0 (0) 3 (2) 0 Infusion reaction 6 (6) 0 5 (2) 1 (<1) 9 (4.4) 0 Renal 2 (2) 1 (1) 4 (2) 1 (<1) 4 (2) 1 (1) 1. Topalian S, et al. N Engl J Med 2012; 366: Sznol M, et al. ASCO Weber J, et al. Lancet Oncol 2015; 16: Robert C, et al. N Engl J Med 20145; 372:320-30
49 Pembrolizumab: Data from the Phase I study (Keynote-001) (cont d) PFS In the keynote-001 study the PFS and OS data showed no differences between the two different treatment's schedules used in the study: 2 mg/kg Q3W and 10 mg/kg Q3W OS This data supported the use of the lower dosage of pembrolizumab (2 mg/kg Q3W) for the following studies Hamid O, et al. N Engl J Med Jul 11;369: Reprinted from Robert C, et al. Lancet 2014;384: Copyright 2014, with permission from Elsevier
50 Pembrolizumab: Data from the Phase I study (Keynote-001) All population (n. 655 patients) Long-term follow-up of 655 patients enrolled in the Keynote 001 showed that pembrolizumab is associated with an important antitumour activity: 33% of ORR with 8% of complete response; median duration of response was 28.2 months Only naive patients (n. 152 patients) In the cohort of treatment-naïve patients (n. 152), pembrolizumab showed 45% of ORR with 14% of complete response; ORR in BRAF wt and BRAF mutated patients was 45% and 50% respectively; median duration of response was not reached Daud A, et al. ASCO 2015 J Clin Oncol 2015;33 suppl May 20:abstract 9005 (Permission of Daud A.)
51 Pembrolizumab: Data from the randomised Phase II study in ipilimumab refractory advanced melanoma patients (Keynote-002): Pembrolizumab (2 mg/kg Q3W and 10 mg/kg Q3W) vs. investigator chemotherapy choiche (ICC) Both pembrolizumab doses substantially improved PFS compared with chemotherapy (P < ). Mean PFS up to 12 months of follow-up was approximately 2-fold longer with pembrolizumab. ORR was 21% for pembro 2 mg/kg Q3W, 25% for pembro 10 mg/kg Q3W, and 4% for ICC. Reprinted from Ribas A, et al. Lancet Oncol 2015;16: Copyright 2015, with permission from Elsevier
52 Pembrolizumab: Data from the randomised Phase II study in ipilimumab refractory advanced melanoma patients (Keynote-002): Pembrolizumab (2 mg/kg Q3W and 10 mg/kg Q3W) vs. investigator chemotherapy choiche (ICC) (Cont d) Median duration of response not reached for pembrolizumab, 37 weeks for chemotherapy There was no significant differences in PFS, ORR, or duration of response between pembrolizumab doses Reprinted from Ribas A, et al. Lancet Oncol 2015;16: Copyright 2015, with permission from Elsevier
53 Pembrolizumab: Data from the randomised Phase III study in advanced melanoma patients (Keynote-006): Pembrolizumab (10 mg/kg Q2W and 10 mg/kg Q3W) vs. ipilimumab Both pembrolizumab arms showed a better ORR, PFS, and OS compared to ipilimumab. ORR was 33,7% for pembro 10 mg/kg Q2W, 32,9% for pembro 10 mg/kg Q3W, and 11,9% for ipilimumab Robert C, et al. N Engl J Med 2015;372: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
54 Pembrolizumab: Data from the randomised Phase III study in advanced melanoma patients (Keynote-006): Pembrolizumab (10 mg/kg Q2W and 10 mg/kg Q3W) vs. ipilimumab. (Cont d) Median OS was not reached in all the three arms. 1-year OS rate was 74,1% for pembro 10 mg/kg Q2W, 68,4% for pembro 10 mg/kg Q3W, and 58,2% for ipilimumab. OS HR was 0,63 for pembro 10 mg/kg Q2W vs. ipilimumab, and 0,68 for pembro 10 mg/kg Q3W vs. ipilimumab Robert C, et al. N Engl J Med 2015;372: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
55 Unconventional responses in patients treated with pembrolizumab Immune-related, unconventional response pattern was observed in 6% of the 327 patients treated with pembrolizumab in the Keynoye-001 study For this reason, together the classical RECIST criteria, we must consider immunorelated criteria even for pembrolizumab treatment By permission from Wolchok JD; Wolchok JD, et al. ASCO J Clin Oncol 2015;33(suppl; abstr 3000)
56 Select AE Organ Category Patients, n (%) Pembrolizumab safety profile: Selected immuno-related adverse events experienced in the Phase I-III trials Pembrolizumab Keynote All cohorts n. 655 pts Any Grade Grade 3 4 Pembrolizumab Keynote mg/kg Q3W n. 178 pts N (%) Any Grade Grade 3 4 Pembrolizumab Keynote mg/kg Q3W n. 179 pts N (%) Any Grade Grade 3 4 Skin* NR NR 68 (39) 0 69 (38) 0 Pembrolizumab Keynote mg/kg Q2W n. 278 pts N (%) Any Grade 106 (38,1) Grade Pembrolizumab Keynote mg/kg Q3W n. 277 pts N (%) Any Grade 107 (38,7) Grade 3 4 Gastrointestinal** 11 (1,7) 7 (1.1) 17 (9) 0 20 (11) 4 (2) 52 (18,7) 11 (3,9) 50 (18) 10 (3,6) Endocrine 64 (9,8) 3 (0,5) 19 (11) 1 (<1) 18 (10) 0 47 (17) 2 (0,8) 35 (12,6) 1 (0,4) Hepatic 4 (0,6) 2 (0,3) 2 (1) 1 (<1) 2 (1) 2 (1) 3 (1.1) 3 (1.1) 5 (1.8) 5 (1.8) Pulmonary 18 (2,7) 2 (0,3) 3 (2) 0 3 (2) 2 (1) 1 (0.4) 0 5 (1.8) 1 (0.4) Infusion reaction NR NR (<1) 0 NR NR NR NR Renal 3 (0,5) 2 (0,3) 1 (<1) 0 1 (<1) (0.4) 0 Uveitis 6 (0,9) (1) 1 (<1) 1 (0.4) 0 3 (1.1) 0 * Pruritus, rash, vitiligo **Colitis, diarrhea NR = not reported diarrhea was not reported hypophysitis was not reported 0 1. Daud A, et al. ASCO Ribas A, et al.lancet Oncol 2015 Jun 23. pii: S (15) Robert C, et al. N Engl J Med 2015;372:


 CR/PR 9 (36) 0 9 (21) Nonresponder 16* (64) 17 (100) 33 (79) All patients 25 17 42 NSCLC From Topalian S, et al.")
57 Proportion of patients Tumour PD-L1 expression as candidate predictive biomarker: First evidence in the nivolumab Phase I trial 42 pts include 18 MEL, 10 NSCLC, 7 CRC, 5 RCC, and 2 CRPC 1 17/17 Melanoma /25 16*/25 PD-L1(+) 0/17 PD-L1(-) PD-L1(+) PD-L1(-) analysis not pre-planned and based on subset of subjects'. *2 pts still under evaluation * RCC Association between pretreatment tumour PD-L1 expression and clinical response Response status PD-L1 Positive no. (%) PD-L1 Negative no. (%) Total no. (%) CR/PR 9 (36) 0 9 (21) Nonresponder 16* (64) 17 (100) 33 (79) All patients NSCLC From Topalian S, et al. NEJM 2012;366: Copyright 2012 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
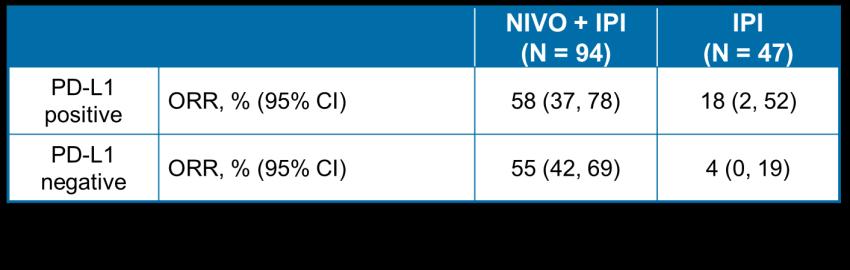
58 Tumour PD-L1 expression as candidate predictive biomarker: Response according to PD-L1 expression in NSCLC and melanoma Subsequent experiences showed that there is a 15-20% of patients PD-L1 negative who respond. Moreover, in the phase I study with the combination ipilimumab/nivolumab, the ORR was similar in both the groups (PD-L1 positive and negative). (Simeone et al. Melanoma Manag. 2015; 2:41 50) Tumour PDL1+ Positive ORR n/n (%) PDL1-Negative ORR n/n (%) MPDL3280A (Hamid ASCO 2013) Melanoma 4/15 (27) 3/15 (20) Nivolumab (Weber ASCO 2013) Melanoma 8/12 (67) 6/32 (19) Nivolumab (Grosso ASCO 2013) Melanoma 7/16 (44) 3/18 (17) Nivolumab (Topalian, N Engl J Med, 2012) NSCLC 9/25 (36) 0/17 (0) Nivolumab (Antonia, WCLC 2013) NSCLC 5/31 (16) 4/32 (13) Pembrolizumab (Garon, WCLC 2013) NSCLC 4/7 (57) 2/22 (9) MPDL3280A3 (Horn, WCLC 2013) NSCLC 8/26 (31) 4/20 (20) Nivolumab/ Ipilimumab (Callahan ASCO 2013) NSCLC 4/10 (40) 8/17 (47) Key questions Variability in tissue collection timing, cell sampling, types of assay, IHC criteria 1. Antonia SJ, et al. Poster presentation at WCLC J Thorac Oncol 2013;8(Suppl 2):abstract: P ; 2. Garon EB, et al. Oral presentation at WCLC J Thorac Oncol 2013;8(Suppl 2):abstract: MO18.02; 3. Horn L, et al. Mini-Oral presentation at WCLC J Thorac Oncol. 2013;8(Suppl 2):abstract: MO Bottom table Presented by: Walter J. Urba, MD, PhD


59 Tumour PD-L1 expression as candidate predictive biomarker: Experience from the randomised Phase III studies with nivolumab (CA ) In the CA study, the patients enrolled were stratified according the PD-L1 expression The ORR according the PD-L1 expression was of 44% in the PD-L1 positive group and 20% in the PD-L1 negative group, confirming that patients PD-L1 negative can respond to anti- PD-1 treatment OS data are not still mature D Angelo S, et al. SMR 2014 Weber J, et al. Lancet Oncol 2015;16:375-84, Reprinted from The Lancet, Copyright 2015, with permission from Elsevier. By permission of Weber J, Weber J et al. ESMO 2014 Congress; September 26-30, 2014; Madrid, Spain. Abstract LBA3.


60 ORR (%, 95% CI) Tumour PD-L1 expression as candidate predictive biomarker: Experience from the randomised Phase III studies with nivolumab - (CA ) Even in the CA study, the patients enrolled were stratified according the PD-L1 expression The ORR according the PD-L1 expression was, in the group of patients treated with nivolumab, 53% in the PD-L1 positive and 33% in the PD-L1 negative % (41 64%) 11% (5 20%) 33% (25 42%) 16% (10 23%) Nivolimumab (n=210) Dacarbazine (n=208) The survival benefit of nivolumab vs. dacarbazine was observed irrespective of tumour PD-L1 status. The 1-year OS rate of the patients treated with nivolumab was 82,1% in the PD-L1 positive group and 67,8% in the PD-L1 negative group 10 0 PD-L1+ PD-L1- From Robert C, et al. N Engl J Med 20145;372: Supplementary material. Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society; Redrawn from Long Y, et al. J Translat Med 2015, 13(Suppl 1):O6
61 Tumour PD-L1 Expression as candidate predictive biomarker: Experience from the randomised Phase III studies with pembrolizumab Ribas A, et al. AACR 2015 From Robert C, et al. N Engl J Med 2015;372: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
62 Tumour PD-L1 expression as candidate predictive biomarker: % of pts PD-L1 positive in the different clinical trials Study NIVOLUMAB: Pts PDL1+ Positive (%) CA (Weber J et al. LO 2015) 49 CA (Robert C et al. NEJM 2014) 35 Ca (Larkin J et al. NEJM 2015) ipi/nivo arm 21.7 Ca (Larkin J et al. NEJM 2015) nivo arm 25.3 PEMBROLIZUMAB: Keynote 006 (Robert C et al. NEJM 2015) pembro every 2 wks 80.6 Keynote 006 (Robert C et al. NEJM 2015) pembro every 3 wks 79.8 Keynote 002 (Puzanov I et al. ASCO 2015) 69 Keynote 001 (Daud A et al. SMR 2014)) 77 Ascierto PA, et al. J Trans Med 2015; 13:213

63 Differences between anti-ctla-4 and anti-pd-1 mechanism of action Rationale for the combination While anti-ctla-4 acts primarily during the early activation of T cells (priming phase) in lymphoid tissue, anti-pd-1 is mostly active during the T-cell effector phase, since its major role is in the tumour microenviroment where the interaction PD-1/PD-L1 represents one of the most important mechanism for the immuno escape From Ribas A, et al. N Engl J Med 2012;366: Copyright 2012 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
, this combo showed 94% and 88% 1- and 2-year OS rate, respectively.")

64 Ipilimumab plus nivolumab: Results from the phase I study (CA ) The combination nivolumab and ipilimumab showed an interesting OS rates of 79% at 2 years. Moreover, in the nivolumab 1 mg/kg + ipilimumab 3 mg/kg cohort (cohort 2), this combo showed 94% and 88% 1- and 2-year OS rate, respectively. The responses were early and durable and the activity was observed regardless of tumour BRAF mutation or PD-L1 expression status. Relatively lower response rate and worse survival with nivolumab 0.3 mg/kg dose, indicating an efficacy threshold between 0.3 and 1 mg/kg By permission from Dr Mario Sznol; Mario Sznol et al. ASCO 2014, Abstract LBA9003^


65 Ipilimumab plus nivolumab: Results Results from the randomised phase II study ipilimumab/nivolumab vs. ipilimumab alone (CA ) From Postow M, et al. N Engl J Med 2015; 372: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society

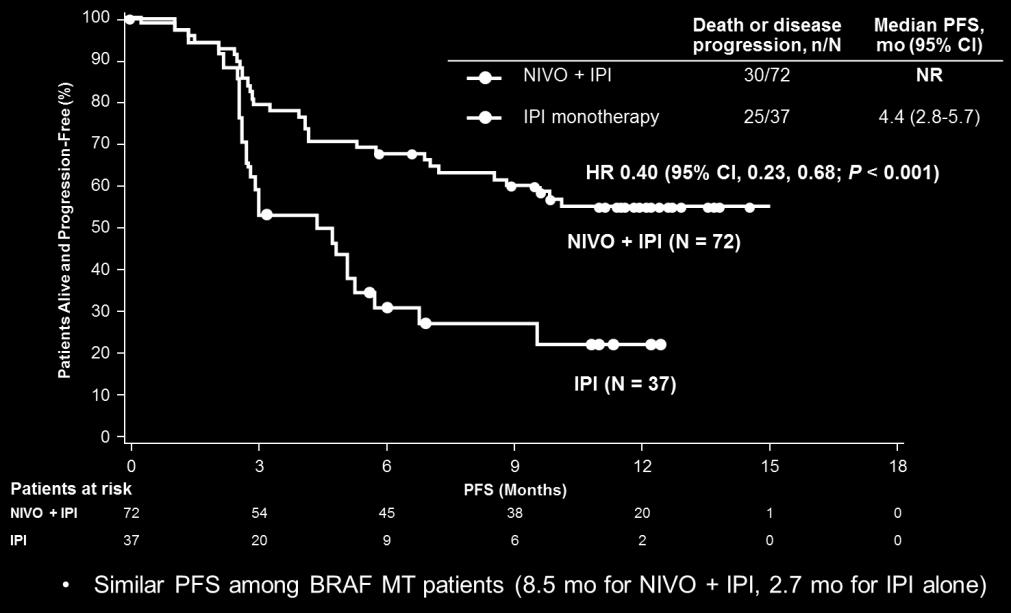
: NIVO + IPI resulted in a longer PFS")

66 Ipilimumab plus nivolumab - Results Results from the three arms randomised phase III study in untreated advanced melanoma patients with ipilimumab/nivolumab or nivolumab alone vs. ipilimumab alone (CA ): NIVO + IPI resulted in a longer PFS From Larkin J et al. N Engl J Med 2015;373: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
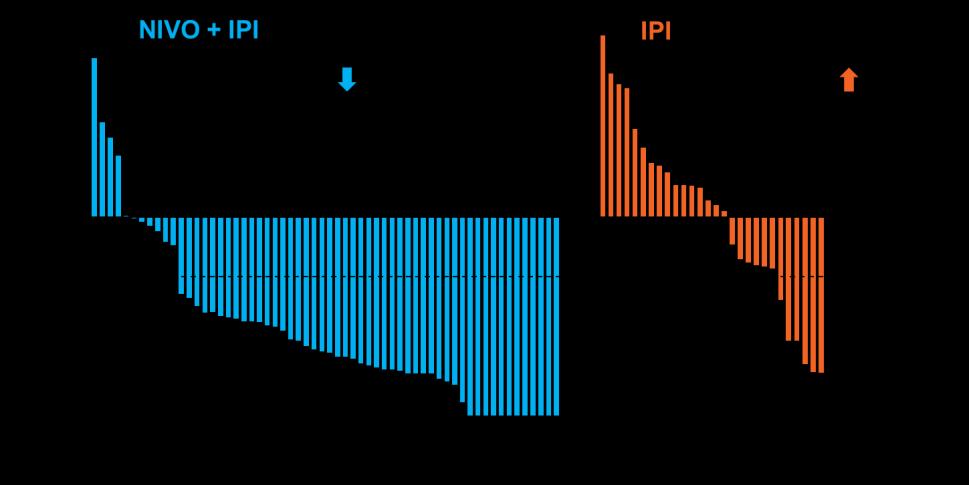
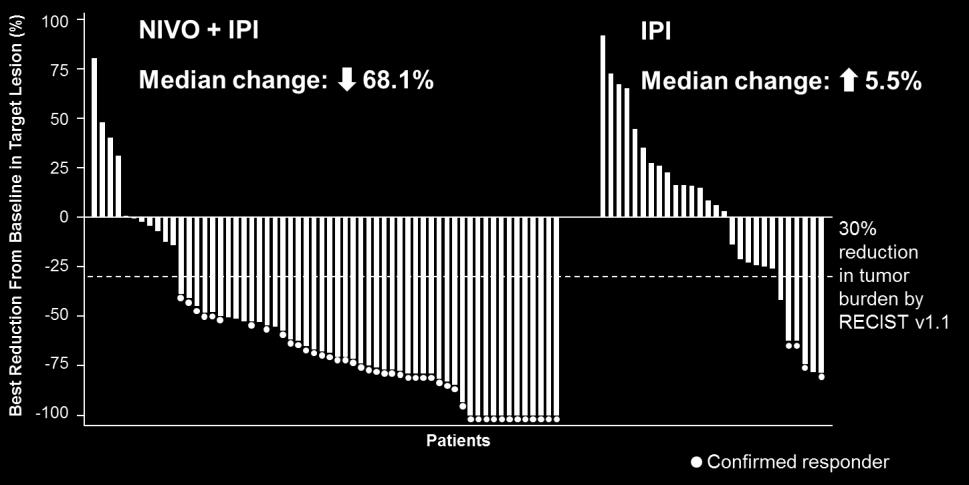
 Baseline reduction from baseline in target lesions (%) Ipilimumab plus nivolumab - Results Results from")


67 Baseline reduction from baseline in target lesions (%) Baseline reduction from baseline in target lesions (%) Baseline reduction from baseline in target lesions (%) Ipilimumab plus nivolumab - Results Results from the three arms randomised Phase III study in untreated advanced melanoma patients with ipilimumab/nivolumab or nivolumab alone vs. ipilimumab alone (CA ): NIVO + IPI resulted in a higher ORR NIVO + IPI Median change: -51.9% IPI Median change: +5.9% NIVO Median change: -34.5% From Larkin J et al. N Engl J Med 2015;373: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society



68 Ipilimumab plus nivolumab (CA ): PFS and ORR by PD-L1 expression level (cut-off 5%) In patients whose tumours have 5% PD-L1 expression, both NIVO alone and NIVO + IPI resulted in a similar prolongation in PFS, although ORR was numerically higher with NIVO + IPI. However we should be cautious when interpreting this data because we should wait the OS data before making any conclusion. From Larkin J, et al. N Engl J Med 2015;373: Copyright 2015 Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society
69 Ipilimumab/nivolumab safety profile: selected immuno-related adverse events experienced in the Phase I, II, and III trials Select AE organ category patients, n (%) Ipi/Nivo CA n. 53 pts (all cohorts) Any Grade Grade 3 4 Ipi/Nivo CA n. 94 pts Any Grade Grade 3 4 Ipi/Nivo CA n. 313 pts Any Grade Grade 3 4 Skin 37 (70) 2 (4) 67 (71) 9 (10) 185 (59,1) 18 (5,8) Gastrointestinal 20 (38) 5 (9) 48 (51) 20 (21) 145 (46,3) 46 (14,7) Endocrine 7 (13) 1 (2) 32 (34) 5 (5) 94 (30,0) 15 (4,8) Hepatic 12 (23) 8 (15) 26 (28) 14 (15) 94 (30,0) 59 (18,8) Pulmonary 3 (6) 1 (2) 11 (12) 3 (2) 22 (7,0) 3 (1,0) Infusion reaction 1 (2) 0 NR NR NR NR Renal 3 (6) 3 (6) 3 (3) 1 (1) 17 (5,4) 6 (2,0) 1. Wolchok J, et al. N Engl J Med 2013; 369: Postow M, et al. N Engl J Med 2015; 372: Larkin J, et al. N Engl J Med 2015;373:23-34 NR = Not reported
70 Conclusions After more than 40 years we got the approval of several compounds effective in the treatment of melanoma (ipilimumab, vemurafenib, dabrafenib, trametenib, cobimetinib, nivolumab, pembrolizumab) These drugs can be split into two important categories with different characteristics and kinetics of action: immunotherapy and target therapy Anti-PD-1s (nivolumab and pembrolizumab) showed to be superior to ipilimumab The combination BRAF + MEK inhibitors is superior to the BRAF inhibitors monotherapy Considering the data coming from the recent phase III trials, anti-pd-1s (nivolumab and pembrolizumab) should be used in first line. However, in case of patients with symptoms and a fast progression of the disease, the combination BRAF plus MEK inhibitors represents a valid opportunity for the treatment in first line At the moment, the combination ipilimumab/nivolumab should be used only in clinical trials
71 Thank you!
LESSONS LEARNT Melanoma Academic Perspective
 LESSONS LEARNT Melanoma Academic Perspective Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosures
LESSONS LEARNT Melanoma Academic Perspective Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosures
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Combination Approaches in Melanoma: A Balancing Act
 Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma
 and Binimetinib (MEK162) in Patients With Metastatic Melanoma") The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma Reinhard Dummer, 1 Keith Flaherty, 2 Richard Kefford, 3 Paolo A. Ascierto, 4 Laure Moutouh-de Parseval,
The Development of Encorafenib (LGX818) and Binimetinib (MEK162) in Patients With Metastatic Melanoma Reinhard Dummer, 1 Keith Flaherty, 2 Richard Kefford, 3 Paolo A. Ascierto, 4 Laure Moutouh-de Parseval,
BRAF Inhibitors in Metastatic disease. Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia
 Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Inhibitors in Metastatic disease Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia Disclosures Research Support Pfizer & Cellgene Consultant Provectus Mortality from Melanoma
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
New Therapeutic Approaches to Malignant Melanoma
 2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
The information in this activity is intended for healthcare professionals based outside of the United States. This activity may contain information
 The information in this activity is intended for healthcare professionals based outside of the United States. This activity may contain information on products outside the approved indications where you
The information in this activity is intended for healthcare professionals based outside of the United States. This activity may contain information on products outside the approved indications where you
What s new in melanoma? Combination!
 DOI 10.1186/s12967-015-0582-1 EDITORIAL Open Access What s new in melanoma? Combination! Paolo A Ascierto 1*, Francesco M Marincola 2 and Michael B Atkins 3 Abstract Melanoma was again a focus of attention
DOI 10.1186/s12967-015-0582-1 EDITORIAL Open Access What s new in melanoma? Combination! Paolo A Ascierto 1*, Francesco M Marincola 2 and Michael B Atkins 3 Abstract Melanoma was again a focus of attention
Immunoterapia e melanoma maligno metastatico: siamo partiti da li. Vanna Chiarion Sileni Istituto Oncologico Veneto
 Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Update on Targeted Therapy in Melanoma
 Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
Update on Targeted Therapy in Melanoma Seville June 2013 James Larkin FRCP PhD London UK Overview What are the targets in melanoma? BRAF / KIT / NRAS / GNAQ / MEK DNA / microtubules CTLA4 / PD1 / PDL1
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib (VEM) or ENCO in BRAF-Mutant Melanoma
 Plus Binimetinib (BINI) vs Vemurafenib (VEM) or ENCO in BRAF-Mutant Melanoma") Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib () or ENCO in BRAF-Mutant Melanoma, Paolo A. Ascierto, Helen J. Gogas, Ana Arance, Mario Mandala,
Overall Survival in COLUMBUS: A Phase 3 Trial of Encorafenib (ENCO) Plus Binimetinib (BINI) vs Vemurafenib () or ENCO in BRAF-Mutant Melanoma, Paolo A. Ascierto, Helen J. Gogas, Ana Arance, Mario Mandala,
Melanoma- Fighting the Dark Side
 Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018
 ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the Private
ASCO / COLUMBUS ENCORE PRESENTATION June 4, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions of the Private
Melanoma in Focus: Update on Novel Therapy, Emerging Agents, and Optimizing Patient Care Presentation 1
 Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Response and resistance to BRAF inhibitors in melanoma
 Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
MELANOMA: THE BEST OF THE YEAR Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone
 MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
Beyond BRAFi/MEKi: Combination and Sequencing Approaches for in Patients with Metastatic BRAF V600 Mutant Melanoma:
 Beyond BRAFi/MEKi: Combination and Sequencing Approaches for in Patients with Metastatic BRAF V600 Mutant Melanoma: Michael B. Atkins, M.D. Deputy Director Georgetown-Lombardi Comprehensive Cancer Center
Beyond BRAFi/MEKi: Combination and Sequencing Approaches for in Patients with Metastatic BRAF V600 Mutant Melanoma: Michael B. Atkins, M.D. Deputy Director Georgetown-Lombardi Comprehensive Cancer Center
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Normal RAS-RAF (MAPK) pathway signaling
 pathway signaling") BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Checkpoint-Inhibitoren beim Lungenkarzinom. Dr. Helge Bischoff Thoraxklinik Heidelberg
 Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Array BioPharma Jefferies 2016 Global Healthcare Conference. June 9, 2016
 Array BioPharma Jefferies 216 Global Healthcare Conference June 9, 216 Safe Harbor Statement 2 Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Array BioPharma Jefferies 216 Global Healthcare Conference June 9, 216 Safe Harbor Statement 2 Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Principles and Application of Immunotherapy for Cancer: Advanced Melanoma
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
BRAF Inhibition in Melanoma
 BRAF Inhibition in Melanoma New York City, Mar 22-23, 2013 Bartosz Chmielowski, MD, PhD Assistant Clinical Professor University of California Los Angeles Disclosures Speaker Bureau: BMS, Genentech, Prometheus
BRAF Inhibition in Melanoma New York City, Mar 22-23, 2013 Bartosz Chmielowski, MD, PhD Assistant Clinical Professor University of California Los Angeles Disclosures Speaker Bureau: BMS, Genentech, Prometheus
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma
 Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
BRAF/MEK inhibitors in the systemic treatment of advanced skin melanoma
 QUALITY OF LIFE IN ONCOLOGY Review article BRAF/MEK inhibitors in the systemic treatment of advanced skin melanoma Maksymilian Kruczała, Aleksandra Grela-Wojewoda, Marek Ziobro Clinic of Systemic and Metastatic
QUALITY OF LIFE IN ONCOLOGY Review article BRAF/MEK inhibitors in the systemic treatment of advanced skin melanoma Maksymilian Kruczała, Aleksandra Grela-Wojewoda, Marek Ziobro Clinic of Systemic and Metastatic
Malignant Melanoma, what s new? Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Malignant Melanoma, what s new? Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Melanoma Epidemiology: Incidence and Mortality Estimated 2012 Global Incidence and Mortality by WHO Region (all
Malignant Melanoma, what s new? Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Melanoma Epidemiology: Incidence and Mortality Estimated 2012 Global Incidence and Mortality by WHO Region (all
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
LA QUARTA ARMA CONTRO IL CANCRO
 LA QUARTA ARMA CONTRO IL CANCRO Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure Employment or
LA QUARTA ARMA CONTRO IL CANCRO Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure Employment or
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management
 Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies
 Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
Update on Melanoma Treatment. Tara C Mitchell, MD
 Update on Melanoma Treatment Tara C Mitchell, MD Overview Immune therapy update Targeted therapy update New concepts in treating melanoma What is the immune system? A complex network of protective cells
Update on Melanoma Treatment Tara C Mitchell, MD Overview Immune therapy update Targeted therapy update New concepts in treating melanoma What is the immune system? A complex network of protective cells
Array BioPharma Second Quarter of F2018 Update FEBRUARY 6, 2018
 Array BioPharma Second Quarter of F2018 Update FEBRUARY 6, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Array BioPharma Second Quarter of F2018 Update FEBRUARY 6, 2018 SAFE HARBOR STATEMENT Forward-looking statements made in the course of this presentation are made pursuant to the safe harbor provisions
Melanoma BRAF mutado y terapias dirigidas. Javier Medina Martínez Hospital Virgen de la Salud, Toledo
 Melanoma BRAF mutado y terapias dirigidas Javier Medina Martínez Hospital Virgen de la Salud, Toledo Enfermedad avanzada: Seguimiento a largo plazo Retratamiento Metástasis cerebrales Adyuvancia November-2017
Melanoma BRAF mutado y terapias dirigidas Javier Medina Martínez Hospital Virgen de la Salud, Toledo Enfermedad avanzada: Seguimiento a largo plazo Retratamiento Metástasis cerebrales Adyuvancia November-2017
Toxicity of Systemic Melanoma Therapies. Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney
 Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon
 The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon Samantha Bowyer Medical Oncologist Rockingham General Hospital Historical perspective
The changing landscape of medical management of stage III and IV melanoma Current treatments and what s on the horizon Samantha Bowyer Medical Oncologist Rockingham General Hospital Historical perspective
Cancer Progress. The State of Play in Immuno-Oncology
 Cancer Progress The State of Play in Immuno-Oncology Axel Hoos, MD, PhD VP, Oncology R&D, Glaxo Smith Kline Co-Director, Cancer Immunotherapy Consortium Key Drivers in Immuno-Oncology Science Methods Combinations
Cancer Progress The State of Play in Immuno-Oncology Axel Hoos, MD, PhD VP, Oncology R&D, Glaxo Smith Kline Co-Director, Cancer Immunotherapy Consortium Key Drivers in Immuno-Oncology Science Methods Combinations
WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example
 WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example YIDOU ZHANG Health Economics and Payer Analytics Director Oncology Payer Evidence and Pricing, AstraZeneca
WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example YIDOU ZHANG Health Economics and Payer Analytics Director Oncology Payer Evidence and Pricing, AstraZeneca
Emerging Trends & Strategies in the Treatment & Management of Metastatic Melanoma. Evan J. Lipson, MD
 Emerging Trends & Strategies in the Treatment & Management of Metastatic Melanoma Evan J. Lipson, MD Johns Hopkins University School of Medicine Sidney Kimmel Comprehensive Cancer Center April 25, 2014
Emerging Trends & Strategies in the Treatment & Management of Metastatic Melanoma Evan J. Lipson, MD Johns Hopkins University School of Medicine Sidney Kimmel Comprehensive Cancer Center April 25, 2014
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Updates in Metastatic Melanoma
 SCSHP 214 Annual Meeting Updates in Metastatic Melanoma LeAnn B. orris, PharmD, BCPS, BCOP Assistant Professor South Carolina College of Pharmacy Background Estimated 76,69 new cases in 213 Increasing
SCSHP 214 Annual Meeting Updates in Metastatic Melanoma LeAnn B. orris, PharmD, BCPS, BCOP Assistant Professor South Carolina College of Pharmacy Background Estimated 76,69 new cases in 213 Increasing
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Treatment of Tumors Resistant to PD-1 inhibitors
 Treatment of Tumors Resistant to PD-1 inhibitors Harriet Kluger, MD Professor of Medicine (Medical Oncology), Yale School of Medicine Deputy Section Chief, Medical Oncology Associate Cancer Center Director
Treatment of Tumors Resistant to PD-1 inhibitors Harriet Kluger, MD Professor of Medicine (Medical Oncology), Yale School of Medicine Deputy Section Chief, Medical Oncology Associate Cancer Center Director
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Ipilimumab ASCO Data Review and Discussion Webcast. Monday, June 2, 2008
 Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD
 Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Immunotherapy Experience in Melanoma Integrating IO into Clinical Practice Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer
Cutaneous melanoma: new developments for 2018
 Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
BRAF Gene Variant Testing To Select Melanoma or Glioma Patients for Targeted Therapy
 BRAF Gene Variant Testing To Select Melanoma or Glioma Patients for Targeted Therapy Policy Number: 2.04.77 Last Review: 12/2018 Origination: 4/2013 Next Review: 12/2019 Policy Blue Cross and Blue Shield
BRAF Gene Variant Testing To Select Melanoma or Glioma Patients for Targeted Therapy Policy Number: 2.04.77 Last Review: 12/2018 Origination: 4/2013 Next Review: 12/2019 Policy Blue Cross and Blue Shield
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy