RFA of Tumors of the Lung: How and Why. Radiofrequency Ablation. Radiofrequency Ablation. RFA of pulmonary metastases. Radiofrequency Ablation of Lung
|
|
|
- Adela Sharyl Foster
- 6 years ago
- Views:
Transcription
1 RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation Heat-ablation of malignancy in a single session A recent development for tx of lung tumors First clinical i l experience: Dupuy, AJR 2000 Supported by successful trials in animals Our first case: 2/28/2000 Potentially curative in NSCLC >5 yr survival of patients with RFA alone: Simon, 2007 Our experience confirms this observation 25% 5-year overall survival with mature follow-up: Radiofrequency Ablation RFA of pulmonary metastases Goal of tx of lung cancer: cure or palliation. Curative intent: Pi Primary lung cancer must be solitary (e.g. stage I), or have limited, potentially controllable metastases. Pulmonary metastases Palliation: control of symptoms Pain caused by chest wall invasion Hypertrophic pulmonary osteoarthropathy Metastatic disease depends on the primary: Sarcoma Epithelial neoplasms, <4 pulmonary lesions Carcinoma Melanoma Germ Cell Tumors Favorable prognostic factors: Longer disease-free interval Fewer pulmonary metastases 1
2 RFA of pulmonary metastases RFA of pulmonary metastases Test of time paradigm Some patients who have lung resection for oligometastatic t ti disease re-present shortly thereafter with many more metastases. If RFA is used instead, QOL may be better and patients have a test of time to see whether additional metastases develop. Surgery would remain an option for patients with unsuccessful ablations. Reference: Livraghi T, et al. Percutaneous RFA of liver metastases t in potential ti candidates for resection: the test of time approach. Cancer 2003; 97: Radiofrequency Ablation RFA Patient Selection, part 1 No evidence demonstrates superiority of RFA over other established modalities of local control: Surgical resection Radiation therapy The clinical experience with RFA is more limited Therefore it would be unethical to advise a patient to undergo RFA unless the patient is not a candidate for either of the other treatment modalities, or has been offered them and refused. Dx of malignancy must be established?ct-guided needle bx and RFA one sitting Tumor size must be suitable for RFA Up to 4 cm Best results <3 cm Local vascular anatomy Risk of bleeding Heat sink phenomenon RFA Patient Selection, part 2 RFA Patient Selection, part 3 Contraindications: Coagulopathy Multifocal disease such as BACC Pacemakers and ICDs Arrangements should be made with the cardiologist to prepare the device before RFA and return it to its pre-existing mode after RFA Notes: Prior pneumonectomy is not necessarily a contraindication ti to RFA in the remaining i lung Tumor location close to the heart does not make cardiac dysrhythmia more likely during RFA RFA may be considered for salvage if NSCLC recurs locally after XRT 2


3 Consultation Visit RFA Procedure, Part 1 Outpatient procedure Single session Does not preclude additional RFA treatments t t if they become necessary Will not interfere with chemotherapy or radiation therapy if the clinical circumstances warrant Moderate sedation or general anesthesia Patient arrives in outpatient unit Antibiotic prophylaxis? Controversial Consent RFA Chest tube placement Sedation or GA RFA Procedure, Part 2 LeVeen Needle-Electrode Phase I: Electrode placement Approach similar to CT-guided needle biopsy Grounding pads Accurate positioning of needle-electrode Confirmation in 3 dimensions Sample Case Medically inoperable NSCLC Pre-procedure CT image Oblique reformatted image after deployment of an expandable multitined needle-electrode, in the plane of the needle shaft. Oblique reformatted image perpendicular to the plane of the needle shaft, showing the tumor enclosed within the expected treatment volume (circle). 3








4 RFA Procedure, Part 3 Sample Case Phase II: Ablation process Power deposition Protocol ldepends d on manufacturer Monitoring Tissue impedence Temperature Maintainence of sedation Medically inoperable NSCLC CT image showing deployment of the needle- electrode. Immediate post-procedure CT image showing ground-glass opacity surrounding the tumor, indicative of thermal injury to the adjacent lung. 4


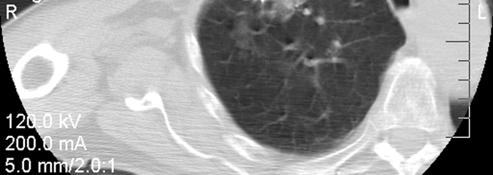
5 Complications ~ Needle Bx Complications Unique to RFA Pneumothorax: Common, reported incidence of 9-63% Air leaks may be prolonged Infection in the lung or pleural space Pulmonary hemorrhage, can be fatal Systemic air embolization, also potentially fatal Tumor seeding of the needle tract is rare Cutaneous burns Thermal injury of adjacent normal tissues Phrenic nerve injury Cerebral microembolization Rarely associated with clinical findings For several days after RFA, patients may have a mild flu-like syndrome attributed to tumor lysis Likelihood proportional to tumor volume Procedural mortality rate of <1% Sample Case Metastatic NSCLC S/p right pneumonectomy 2 years earlier 2 metastases were discovered in the LLL Ablation of the larger, more laterally-located LLL lesion,






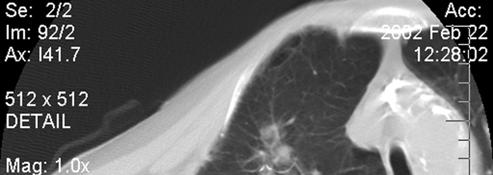
6 Case, continued The patient required chest tube drainage for PTX. He returned two days later for RFA of the second LLL lesion Chest tubes still in place, but no air leak. Note appearance of the site of previous ablation. Note that there is risk of injury to diaphragm. 6








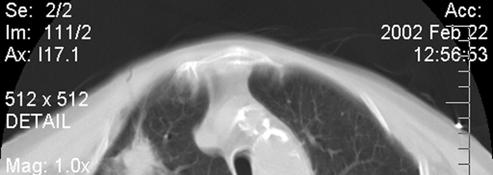
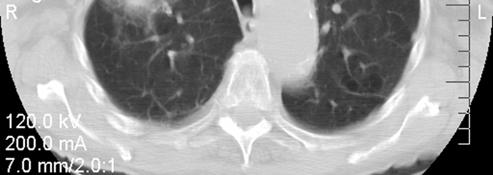
7 Case, continued The following week the patient returned for evaluation of PE, because of hypoxemia. Note that both RFA sites are cavitary. Small fluid collection adjacent to the left crus of the diaphragm, likely the result of thermal injury. Post-RFA Imaging Follow-Up Treatment site monitored to assess response Even when target lesion is coagulated completely, imaging features evolve for one year or more Contrast-enhanced CT At 3, 6 and 12 months after RFA, then annually 3 months: treatment site enlarges, may be cavitary No more than a thin rim of contrast enhancement Thereafter, slow contraction indicating fibrosis 7








8 Sample Case Medically-inoperable NSCLC Diagnostic CT image showing a small tumor, subsequently shown by needle biopsy to be a NSCLC, in the periphery of the right upper lobe. 3 month follow-up CT; the lesion has increased in size, as expected. 3 month follow-up CT, soft tissue window; there is no contrast enhancement. 9 month follow-up CT. The residual opacity at the treatment site is diminishing in size. Post-RFA Imaging Follow-Up PET with FDG Shows uptake early after therapy, <2 months Reactive changes in the lung around the treatment site Degree of uptake should decline subsequently Reported to predict tumor recurrence at 2 months after RFA SUV > 1.8 at the treatment site, or SUV that decreased less than 60% relative to pre-tx baseline Another study of FDG-PET and contrast-enhanced CT in f/u Abolition of FDG uptake was both 100% sensitive and specific for complete response, at both 1 month and 3 months after RFA Dx performance of CT was indistinguishable from PET at 3 months 8








9 Post-RFA Imaging Follow-Up Any unexpected CT or PET findings Needle biopsy Potential for retreatment of incompletely ablated tumors Risk of a second primary lung cancer In general, risk is ~ 2% per year in survivors of NSCLC In our series, 4/9 patients who survived more than 2 years after RFA developed a new primary lung cancer Most of these can be treated with RFA Sample Case Recurrent disease after RFA Pre-procedure CT image. Transverse CT image showing electrode placement. Oblique CT image of electrode. 3 month follow-up CT demonstrating no contrast enhancement. 12 month follow-up CT: definite tumor regrowth and new pleural disease, both of which showed uptake on FDG PET. 9










10 Sample Case Development of new primary lung cancer. Original NSCLC, in RLL, prior to RFA. CT image of electrode placement. CT image of electrode placement. Immediate post-procedure CT image. Diagnostic CT of treatment site at 30 months showing stable scar. No PET uptake at this site. On the same scan, a new mass was found in the upper lobe of the right lung (arrow). Scarring also is visible posteriorly at the site of a previous wedge resection. 10
 Permits assessment of extent of")





11 Efficacy of RFA Two studies: RFA followed by resection of the treated tumor ( ablate and resect ) Permits assessment of extent of RFA-induced id d tumor necrosis One study complete necrosis in 6/9 cases In the other complete absence of viable tumor cells was observed in only 3/10 lesions Complete ablation more likely if tumor <3cm Efficacy of RFA Sample Case Little long-term follow-up data re RFA for NSCLC A series of 36 patients showed median survival of 29 months in a medically-inoperable inoperable population This compares favorably to XRT in a similar population: 3-year overall survival ~ 40% Both treatment modalities are evolving Medically inoperable NSCLC Pre-procedure CT image Immediate post-procedure CT image Post-procedure image at 5 years; residual lesion had been stable with no evidence of recurrence 11






12 RFA and the FDA FDA has not approved RFA for tx of lung cancers Lack of demonstrated efficacy Reported deaths Manufacturers cannot legally promote the use of their RFA devices for this indication Several centers now have >5 years of experience with RFA for NSCLC Multicenter study of RFA in clinical stage I NSCLC ACOSOG protocol Z4033, now underway Future Developments Where does RFA fits into the management of patients who suffer from lung cancer? Competitor to XRT/SBRT? Complementary treatment modality? For tumors that are likely to recur locally after XRT alone, the two modalities can be combined RFA in cases of local failure of XRT, if restaging demonstrates no other sites of disease (salvage tx) Need for clinical trials 12

 Not a")




13 Sample Images Case 1: LUL scar carcinoma (adenocarcinoma) Not a surgical candidate for medical reasons. Not a candidate for XRT previous radiation for sq. cell ca. of neck This patient is our longest survivor Treated 7/00; still alive and well 13



14 Radiofrequency ablation of lung masses Case 2: NSCLC The patient was not a surgical candidate because of marginal pulmonary function 14
15 15
RF Ablation: indication, technique and imaging follow-up
 RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery
 Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Stereotactic Body Radiation Therapy and Radiofrequency Ablation 2014 Masters of Minimally Invasive Surgery Matthew Hartwig, M.D. Duke Cancer Institute Case Presentation I: Patient ER 74 y/o male with A1A
Radiofrequency ablation combined with conventional radiotherapy: a treatment option for patients with medically inoperable lung cancer
 Radiofrequency ablation combined with conventional radiotherapy: a treatment option for patients with medically inoperable lung cancer Poster No.: C-0654 Congress: ECR 2011 Type: Scientific Paper Authors:
Radiofrequency ablation combined with conventional radiotherapy: a treatment option for patients with medically inoperable lung cancer Poster No.: C-0654 Congress: ECR 2011 Type: Scientific Paper Authors:
Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates
 Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates Poster No.: C-2576 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Exhibit
Percutaneous Radiofrequency Ablation of Lung Malignant Tumours: Survival, disease progression and complication rates Poster No.: C-2576 Congress: ECR 2012 Type: Authors: Keywords: DOI: Scientific Exhibit
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Damian Dupuy, MD. Image Guided Intervention (IGI) Studies 10:25 11:05 AM
 Studies 10:25 11:05 AM") Damian Dupuy, MD Image Guided Intervention (IGI) Studies 10:25 11:05 AM Image Guided Intervention (IGI) Studies Damian E. Dupuy, M.D., FACR Professor of Diagnostic Imaging The Warren Alpert Medical School
Damian Dupuy, MD Image Guided Intervention (IGI) Studies 10:25 11:05 AM Image Guided Intervention (IGI) Studies Damian E. Dupuy, M.D., FACR Professor of Diagnostic Imaging The Warren Alpert Medical School
Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases
 Chin J Radiol 2005; 30: 153-158 153 Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases YI-YOU CHIOU YI-HONG CHOU JEN-HUEY CHIANG HSIN-KAI WANG CHENG-YEN CHANG Department
Chin J Radiol 2005; 30: 153-158 153 Percutaneous Ultrasound-guided Radiofrequency Ablation of Colorectal Liver Metastases YI-YOU CHIOU YI-HONG CHOU JEN-HUEY CHIANG HSIN-KAI WANG CHENG-YEN CHANG Department
Radiofrequency Ablation of Lung Cancer at Okayama University Hospital: A Review of 10 Years of Experience. e g
 2011 65 5 287 297 Radiofrequency Ablation of Lung Cancer at Okayama University Hospital: A Review of 10 Years of Experience a* a a b c d e f g h i a a a b c d e g h i 288 65 5 Ⅲ ʼ 2011 289 2 20 10 3 30
2011 65 5 287 297 Radiofrequency Ablation of Lung Cancer at Okayama University Hospital: A Review of 10 Years of Experience a* a a b c d e f g h i a a a b c d e g h i 288 65 5 Ⅲ ʼ 2011 289 2 20 10 3 30
General summary GENERAL SUMMARY
 General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE
 ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE ONCOLOGIC PERCUTANEOUS IMAGE GUIDED TUMOR ABLATION Evolving, growing and increasingly
ONCOLOGIC PERCUTANEOUS INTERVENTION: 2015 UPDATE HANH VU NGHIEM, MD OAKLAND UNIVERSITY WILLIAM BEAUMONT SCHOOL OF MEDICINE ONCOLOGIC PERCUTANEOUS IMAGE GUIDED TUMOR ABLATION Evolving, growing and increasingly
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan
 What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
Complications of percutaneous lung radiofrequency ablation
 Complications of percutaneous lung radiofrequency ablation Poster No.: C-556 Congress: ECR 2009 Type: Educational Exhibit Topic: Interventional Radiology Authors: A. Afaq, S. Khan, U. Patel, E. Leen; London/UK
Complications of percutaneous lung radiofrequency ablation Poster No.: C-556 Congress: ECR 2009 Type: Educational Exhibit Topic: Interventional Radiology Authors: A. Afaq, S. Khan, U. Patel, E. Leen; London/UK
Radiofrequency Ablation (RFA) / Microwave Ablation (MWA) of Lung Tumors
 / Microwave Ablation (MWA) of Lung Tumors") Scan for mobile link. Radiofrequency Ablation (RFA) / Microwave Ablation (MWA) of Lung Tumors Radiofrequency ablation (RFA) and microwave ablation (MWA) are treatments that use image guidance to place
Scan for mobile link. Radiofrequency Ablation (RFA) / Microwave Ablation (MWA) of Lung Tumors Radiofrequency ablation (RFA) and microwave ablation (MWA) are treatments that use image guidance to place
Thoracic Recurrences. Soft tissue recurrence
 Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Navigational Bronchoscopy with Transbronchial Radiofrequency Ablation
 Navigational Bronchoscopy with Transbronchial Radiofrequency Ablation Katie S. Nason, MD MPH AATS Focus on Thoracic: Mastering Surgical Innovation October 28, 2017 No disclosures Radiofrequency ablative
Navigational Bronchoscopy with Transbronchial Radiofrequency Ablation Katie S. Nason, MD MPH AATS Focus on Thoracic: Mastering Surgical Innovation October 28, 2017 No disclosures Radiofrequency ablative
Mahrad Paymani, MD Lake Medical Imaging
 Mahrad Paymani, MD Lake Medical Imaging Background: My name is Mahrad Paymani. I am an Interventional and General Radiologist. I attended four years of college (at UNC Greensboro), four years of medical
Mahrad Paymani, MD Lake Medical Imaging Background: My name is Mahrad Paymani. I am an Interventional and General Radiologist. I attended four years of college (at UNC Greensboro), four years of medical
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation. Basics. What is Percutaneous Ablation? Where are your kidneys?
 Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
ACOSOG Thoracic Committee. Kemp H. Kernstine, MD PhD
 ACOSOG Thoracic Committee Kemp H. Kernstine, MD PhD ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy Govindan, M.D. Carolyn Reed, MD
ACOSOG Thoracic Committee Kemp H. Kernstine, MD PhD ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy Govindan, M.D. Carolyn Reed, MD
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
VATS after induction therapy: Effective and Beneficial Tips on Strategy
 VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY?
 STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY? MICHAEL LANUTI, MD American Association of Thoracic Surgeons Minneapolis, MN 2013 STAGE I INOPERABLE NSCLC RADIOFREQUENCY
STAGE I INOPERABLE NSCLC RADIOFREQUENCY ABLATION OR STEREOTACTIC BODY RADIOTHERAPY? MICHAEL LANUTI, MD American Association of Thoracic Surgeons Minneapolis, MN 2013 STAGE I INOPERABLE NSCLC RADIOFREQUENCY
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
Corporate Medical Policy
 Corporate Medical Policy Radiofrequency Ablation of Miscellaneous Solid Tumors Excluding File Name: Origination: Last CAP Review: Next CAP Review: Last Review: radiofrequency_ablation_of_miscellaneous_solid_tumors
Corporate Medical Policy Radiofrequency Ablation of Miscellaneous Solid Tumors Excluding File Name: Origination: Last CAP Review: Next CAP Review: Last Review: radiofrequency_ablation_of_miscellaneous_solid_tumors
Thoracoscopy for Lung Cancer
 Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Thoracoscopy for Lung Cancer Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your doctor may have recommended an operation to remove your lung cancer. The
Lung Cancer Resection
 Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
THORACIK RICK. Lungs. Outline and objectives Richard A. Malthaner MD MSc FRCSC FACS
 THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
Effect of Electromagnetic Navigation on CT-Guided Percutaneous Thermal Ablation or Biopsy of Lung Tumors
 Effect of Electromagnetic Navigation on CT-Guided Percutaneous Thermal Ablation or Biopsy of Lung Tumors Chaitan K. Narsule 1, Avneesh Gupta 2, Michael I. Ebright 1, Ricardo Sales dos Santos 3, Roberto
Effect of Electromagnetic Navigation on CT-Guided Percutaneous Thermal Ablation or Biopsy of Lung Tumors Chaitan K. Narsule 1, Avneesh Gupta 2, Michael I. Ebright 1, Ricardo Sales dos Santos 3, Roberto
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Despite recent medical advances, the prognosis of metastatic
 BRIEF REPORT A Novel Strategy for Treatment of Metastatic Pulmonary Tumors: Radiofrequency Ablation in Conjunction with Surgery Yoshifumi Sano, MD,* Susumu Kanazawa, MD, Hidefumi Mimura, MD, Hideo Gobara,
BRIEF REPORT A Novel Strategy for Treatment of Metastatic Pulmonary Tumors: Radiofrequency Ablation in Conjunction with Surgery Yoshifumi Sano, MD,* Susumu Kanazawa, MD, Hidefumi Mimura, MD, Hideo Gobara,
Interventional Management of NSCLC. Hiran C Fernando FRCS Professor and Chief, Division Thoracic Surgery Boston Medical Center
 Interventional Management of NSCLC Hiran C Fernando FRCS Professor and Chief, Division Thoracic Surgery Boston Medical Center Comparison of MWA and RFA Qiang Lu et al; AATS 2015 141 patients; 100 with
Interventional Management of NSCLC Hiran C Fernando FRCS Professor and Chief, Division Thoracic Surgery Boston Medical Center Comparison of MWA and RFA Qiang Lu et al; AATS 2015 141 patients; 100 with
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
CT guided thermal ablation of recurrent lung cancer in patients post radiotherapy. A case series review
 CT guided thermal ablation of recurrent lung cancer in patients post radiotherapy. A case series review Poster No.: R-0106 Congress: 2014 CSM Type: Scientific Exhibit Authors: S. Gray; BRISBANE/AU Keywords:
CT guided thermal ablation of recurrent lung cancer in patients post radiotherapy. A case series review Poster No.: R-0106 Congress: 2014 CSM Type: Scientific Exhibit Authors: S. Gray; BRISBANE/AU Keywords:
Horizon Scanning in Surgery: Application to Surgical Education and Practice
 Horizon Scanning in Surgery: Application to Surgical Education and Practice Microwave ablation for lung cancer November 2010 Division of Education Prepared by the Australian Safety and Efficacy Register
Horizon Scanning in Surgery: Application to Surgical Education and Practice Microwave ablation for lung cancer November 2010 Division of Education Prepared by the Australian Safety and Efficacy Register
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD
 Alliance Thoracic Committee Kemp H. Kernstine, MD PhD") ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD 7-12-12 ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy
ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee Kemp H. Kernstine, MD PhD 7-12-12 ACOSOG Thoracic Committee Chair: Bryan Meyers, M.D., MPH Vice Chairs: Malcolm Brock, MD Tom DiPetrillo, M.D. Ramaswamy
Published: Address correspondence to Vidal-Jove Joan:
 Oncothermia Journal 7:111-114 (2013) Complete responses after hyperthermic ablation by ultrasound guided high intensity focused ultrasound (USgHIFU) plus cystemic chemotherapy (SC) for locally advanced
Oncothermia Journal 7:111-114 (2013) Complete responses after hyperthermic ablation by ultrasound guided high intensity focused ultrasound (USgHIFU) plus cystemic chemotherapy (SC) for locally advanced
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Liver Tumors. Patient Education. Treatment options 8 4A. About the Liver. Surgical Specialties
 Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Risk factors for occurrence of local tumor progression after percutaneous radiofrequency ablation for lung neoplasms
 Diagn Interv Radiol 2007; 13:199 203 Turkish Society of Radiology 2007 INTERVENTIONAL RADIOLOGY ORIGINAL ARTICLE Risk factors for occurrence of local tumor progression after percutaneous radiofrequency
Diagn Interv Radiol 2007; 13:199 203 Turkish Society of Radiology 2007 INTERVENTIONAL RADIOLOGY ORIGINAL ARTICLE Risk factors for occurrence of local tumor progression after percutaneous radiofrequency
This booklet has been provided to help answer some of the questions you may have about RFA of liver tumours.
 This booklet has been provided to help answer some of the questions you may have about RFA of liver tumours. RFA of tumours is a minimally invasive procedure used to treat liver tumours (growth or mass
This booklet has been provided to help answer some of the questions you may have about RFA of liver tumours. RFA of tumours is a minimally invasive procedure used to treat liver tumours (growth or mass
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Accomplishes fundamental surgical tenets of R0 resection with systematic nodal staging for NSCLC Equivalent survival for Stage 1A disease
 Segmentectomy Made Simple Matthew J. Schuchert and Rodney J. Landreneau Department of Cardiothoracic Surgery University of Pittsburgh Medical Center Financial Disclosures none Why Consider Anatomic Segmentectomy?
Segmentectomy Made Simple Matthew J. Schuchert and Rodney J. Landreneau Department of Cardiothoracic Surgery University of Pittsburgh Medical Center Financial Disclosures none Why Consider Anatomic Segmentectomy?
VATS Metastasectomy. Inderpal (Netu) S. Sarkaria, MD, FACS
 S. Sarkaria, MD, FACS") VATS Metastasectomy Inderpal (Netu) S. Sarkaria, MD, FACS Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Disclosures Speaking & Education:
VATS Metastasectomy Inderpal (Netu) S. Sarkaria, MD, FACS Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Disclosures Speaking & Education:
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Percutaneous radiofrequency ablation of clinical stage I non small cell lung cancer
 GENERAL THORACIC SURGERY Percutaneous radiofrequency ablation of clinical stage I non small cell lung cancer Takao Hiraki, MD, a Hideo Gobara, MD, a Hidefumi Mimura, MD, a Yusuke Matsui, MD, a Shinichi
GENERAL THORACIC SURGERY Percutaneous radiofrequency ablation of clinical stage I non small cell lung cancer Takao Hiraki, MD, a Hideo Gobara, MD, a Hidefumi Mimura, MD, a Yusuke Matsui, MD, a Shinichi
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Utility of 18 F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer
 Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Thoracostomy: An Update on Imaging Features and Current Surgical Practice
 Thoracostomy: An Update on Imaging Features and Current Surgical Practice Robert D. Ambrosini, MD, PhD, Christopher Gange, MD, Katherine Kaproth-Joslin, MD, PhD, Susan Hobbs, MD, PhD Department of Imaging
Thoracostomy: An Update on Imaging Features and Current Surgical Practice Robert D. Ambrosini, MD, PhD, Christopher Gange, MD, Katherine Kaproth-Joslin, MD, PhD, Susan Hobbs, MD, PhD Department of Imaging
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Gold Anchor enables safe reach to inner organs
 Gold Anchor enables safe reach to inner organs Fine needles for cytology have been used >50 years in all parts of the human body with no to very little harm Gold Anchor comes pre-loaded in needles of the
Gold Anchor enables safe reach to inner organs Fine needles for cytology have been used >50 years in all parts of the human body with no to very little harm Gold Anchor comes pre-loaded in needles of the
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
came from a carcinoma and in 12 from a sarcoma. Ninety lesions were intrapulmonary and the as the chest wall and pleura. Details of the primary
 Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Surgical Management of Pulmonary Metastases. Dr AG Jacobs Principal Specialist Dept Cardiothoracic Surgery Steve Biko Academic Hospital
 Surgical Management of Pulmonary Metastases Dr AG Jacobs Principal Specialist Dept Cardiothoracic Surgery Steve Biko Academic Hospital Introduction Lungs 2 nd most common site of metastatic deposition
Surgical Management of Pulmonary Metastases Dr AG Jacobs Principal Specialist Dept Cardiothoracic Surgery Steve Biko Academic Hospital Introduction Lungs 2 nd most common site of metastatic deposition
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Minimally Invasive Diagnosis. Solid Tumor Percutaneous Core Biopsy. Sheath & spring loaded needle. Specimen submission for solid tumors
 38 th Congress of the International Society of Paediatric Oncology 17-21 September 2006 Minimally Invasive Diagnosis and Treatment of Pediatric Malignancies through Interventional Radiology Minimally Invasive
38 th Congress of the International Society of Paediatric Oncology 17-21 September 2006 Minimally Invasive Diagnosis and Treatment of Pediatric Malignancies through Interventional Radiology Minimally Invasive
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Carcinoma of the Lung
 THE ANNALS OF THORACIC SURGERY Journal of The Society of Thoracic Surgeons and the Southern Thoracic Surgical Association VOLUME 1 I - NUMBER 3 0 MARCH 1971 Carcinoma of the Lung M. L. Dillon, M.D., and
THE ANNALS OF THORACIC SURGERY Journal of The Society of Thoracic Surgeons and the Southern Thoracic Surgical Association VOLUME 1 I - NUMBER 3 0 MARCH 1971 Carcinoma of the Lung M. L. Dillon, M.D., and
Lung cancer is currently the most common cause of cancer-related. Radiofrequency ablation of pulmonary malignant tumors in nonsurgical candidates GTS
 Radiofrequency ablation of pulmonary malignant tumors in nonsurgical candidates Luis J. Herrera, MD a Hiran C. Fernando, MD a Yaron Perry, MD a William E. Gooding, MS b Percival O. Buenaventura, MD a Neil
Radiofrequency ablation of pulmonary malignant tumors in nonsurgical candidates Luis J. Herrera, MD a Hiran C. Fernando, MD a Yaron Perry, MD a William E. Gooding, MS b Percival O. Buenaventura, MD a Neil
Radiofrequency Ablation of Miscellaneous Solid Tumors Excluding Liver Tumors
 Radiofrequency Ablation of Miscellaneous Solid Tumors Excluding Liver Tumors Policy Number: 7.01.95 Last Review: 3/2018 Origination: 3/2006 Next Review: 3/2019 Policy Blue Cross and Blue Shield of Kansas
Radiofrequency Ablation of Miscellaneous Solid Tumors Excluding Liver Tumors Policy Number: 7.01.95 Last Review: 3/2018 Origination: 3/2006 Next Review: 3/2019 Policy Blue Cross and Blue Shield of Kansas
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
An Introduction to PET Imaging in Oncology
 January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
January 2002 An Introduction to PET Imaging in Oncology Janet McLaren, Harvard Medical School Year III Basics of PET Principle of Physiologic Imaging: Allows in vivo visualization of structures by their
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA
 2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
2007 ANNUAL SITE STUDY HODGKIN S LYMPHOMA SUSQUEHANNA HEALTH David B. Nagel, M.D. April 11, 2008 Hodgkin s lymphoma was first described by Thomas Hodgkin in 1832. It remained an incurable malignancy until
I8 COMPLETION INSTRUCTIONS
 The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
C2 COMPLETION INSTRUCTIONS
 The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
RADIOFREQUENCY ABLATION OF MISCELLANEOUS SOLID TUMORS EXCLUDING LIVER TUMORS
 EXCLUDING LIVER TUMORS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
EXCLUDING LIVER TUMORS Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Lung cancer forms in tissues of the lung, usually in the cells lining air passages.
 Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
History of Surgery for Lung Cancer
 Welcome to Master Class for Oncologists Session 1: 7:30 AM - 8:15 AM San Francisco, CA October 23, 2009 Innovations in The Surgical Treatment of Lung Cancer Speaker: Scott J. Swanson, MD 2 Presenter Disclosure
Welcome to Master Class for Oncologists Session 1: 7:30 AM - 8:15 AM San Francisco, CA October 23, 2009 Innovations in The Surgical Treatment of Lung Cancer Speaker: Scott J. Swanson, MD 2 Presenter Disclosure
US-Guided Radiofrequency Ablation of Hepatic Focal Lesions
 US-Guided Radiofrequency Ablation of Hepatic Focal Lesions Poster No.: C-2219 Congress: ECR 2011 Type: Scientific Exhibit Authors: D. Armario Bel, A. PLA, F. TERREL, X. Serres; BARCELONA/ES Keywords: Neoplasia,
US-Guided Radiofrequency Ablation of Hepatic Focal Lesions Poster No.: C-2219 Congress: ECR 2011 Type: Scientific Exhibit Authors: D. Armario Bel, A. PLA, F. TERREL, X. Serres; BARCELONA/ES Keywords: Neoplasia,
Principles of Surgical Oncology. Winnie Achilles Tierklinik Hollabrunn Lastenstrasse Hollabrunn
 Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical