HKIAP FALL SCIENTIFIC MEETING 2014
|
|
|
- Jeremy Stafford
- 6 years ago
- Views:
Transcription

1 HKIAP FALL SCIENTIFIC MEETING 2014 PROF. DAVID DABBS UNIVERSITY OF PITTSBURGH MEDICAL CENTER 15 NOVEMBER 2014 POSTGRADUATE EDUCATION CENTRE PRINCE OF WALES HOSPITAL SHATIN, HONG KONG SAR, CHINA
2 CONTENTS Page The HKIAP Council Guest Speakers in Past Annual Scientific Meetings 3 Meeting Programme of Spring Scientific Meeting 4 Overview of Laboratory Testing for Targeted, Personalized Therapy 5-19 Principles of Molecular Testing: An Example of the Importance of Regulations Ki67 Difficult Practical Issues ASCO Her2 Guideline Changes; Review of Breast and Gastric Her Evolving Role of the Pathologist in Breast Cancer Gene Expression Profiling Notes HKIAP Fall Scientific Meeting 2014 Page 2
3 HKIAP COUNCIL HKIAP Fall Scientific Meeting 2014 Page 3
4 GUEST SPEAKERS IN PAST ANNUAL SCIENTIFIC MEETINGS 1991 Dr Richard L. Kempson and F. Stephen Vogel 1992 Dr Virginia A. LiVolsi, Dr Christopher Fletcher 1993 Dr Juan Rosai and Maria L. Carcangiu 1994 International Congress of IAP 1995 Dr A. Bernard Ackerman 1996 International Liver Pathology Study Group 1997 Dr Thomas V. Colby 1998 Dr Richard L. Kempson 1999 Dr David G. Bostwick 2000 Dr Aileen M. Marty 2001 Challenges and Opportunities in Pathology: Joint International Congress of the Hong Kong College of Pathologists, HKIAP and the Royal College of Pathologists of Australasia 2002 Dr Leon Barnes 2003 Surgical Pathology Update 2003 (co-organized by the Hong Kong Division of International Academy of Pathology and the Department of Pathology, M.D. Anderson Cancer Center, U.S.A) Dr John K.C. Chan 2005 Surgical Pathology Update 2005 (co-organized by the Hong Kong Division of International Academy of Pathology and the Department of Pathology, M.D. Anderson Cancer Center, U.S.A) Dr Parakrama Chandrasoma 2007 Dr Jaime Prat and Dr Bruce Smoller 2008 Surgical Pathology Update 2008 (co-organized by the Hong Kong Division of International Academy of Pathology and the Department of Pathology, M.D. Anderson Cancer Center, U.S.A). Dr Ian Ellis 2009 Dr Christopher DM Fletcher and Dr Steven Silverberg 2010 Dr Stuart Schnitt 2011 Drs Jonathan Epstein and Elizabeth Montgomery (Spring) International Liver Pathology Study Group (Fall) 2012 Dr Jaime Prat (Spring) Dr Elaine S. Jaffe (Fall) 2013 International Society of Urological Pathology (Spring) Prof. Pieter Slootweg (Fall) 2014 Mayo Clinics & Massachusetts General Hospital (Spring) HKIAP Fall Scientific Meeting 2014 Page 4
5 Hong Kong International academy of pathology Fall SCIENTIFIC PROGRAMME Venue: Shaw Auditorium, Postgraduate Education Centre, Prince of Wales Hospital Speaker: Prof. David Dabbs, UPMC 15 November :00 09:30 Registration 09:30 10:15 Overview of Laboratory Testing for Targeted, Personalized Therapy 10:15 11:00 Principles of Molecular Testing: An Example of the Importance of Regulations 11:00 11:30 Coffee break 11:30 12:15 Ki67 Difficult Practical Issues 12:15 12:25 HKIAP AGM 12:25 13:45 Lunch 13:45 14: ASCO Her2 Guideline Changes; Review of Breast and Gastric Her2 14:30 15:15 Evolving Role of the Pathologist in Breast Cancer Gene Expression Profiling HKIAP Fall Scientific Meeting 2014 Page 5


6 Disclosure Statement Overview of Sequencing and Other Molecular Techniques Relevant to Targeted Therapy No financial interests to disclose Acknowledgement: Dr. Jeff Ross-select slides David J Dabbs, MD University of ddabbs@upmc.edu The Evolution of Targeted Therapies for Cancer 1970: ER Testing and Hormonal Therapy for Breast Cancer 1990: Cytogenetics/FISH Testing and Therapy for Heme Malignancies 1998: HER2 Testing in breast cancer for Trastuzumab therapy. 2001: BCR-ABL Testing and Imatinib for CML 2003: EGFR Mutation Testing and Erlotinib for NSCL 2007: KRAS Mutation Testing and Cetuximab/Panitumumab for CRC 2010: EML4-ALK Testing and Crizotinib in NSLC 2011: BRAF Mutation Testing and Vemurafenib in Melanoma 2012: ROS1 and RET Fusion Testing for Crizotinib and RET inhibitors in NSLC 2013: HER2 mutation identification and anti-her2 targeted therapy in NSCLC, breast cancer and micropapillary urothelial cancer 2013: NTRK1 Fusion Testing and crizotinib in NSLC Companion diagnostics are here we are in the era of theranostics-predictive pathology- the next generation of pathology. There Is An Increasing Shift Toward Targeted Therapy Targeted In Cancer Therapy Chemotherapy Anticancer drugs may be highly effective in some, but less effective in others Patients are exposed to the risk of side effects In personalized medicine, clinicians use biomarkers to predict a patient's response to therapy Patients are more likely to get therapies with the greatest impact with fewer side effects 4 CONFIDENTIAL 4 HKIAP Fall Scientific Meeting 2014 Page 6
7 History of DNA sequencing of the human genome 1953: structure of DNA was discovered by Watson&Crick. 1970s: Frederick Sanger developed the Sanger method of rapid DNA sequencing in :Hood introduced the first semi-automated DNA sequencing machine and in 1987 the first fully automated sequencing machine, the ABI 370 was introduced. First publications of the human genome sequence in Diagnostic Challenges in Cancer Genome Testing Cancer genomes are complex, and the number of clinically relevant alterations in a single patient is LOW amongst thousands of total genomic alterations The four types of genomic alterations (Base Substitutions, Insertions/Deletions, Copy Number Alterations and Rearrangements) each are associated with different testing approaches Multiple different tests may consume small amounts of biopsy material Hundreds of clinically relevant cancer genes Number of clinically relevant alterations in a single patient is LOW Number of clinically relevant alterations across a disease spectrum is HIGH Low tumor content in many clinical specimens mandates a test with high accuracy Many clinical cancer specimens are small FFPE specimens. The number of targets and therapies ae increasing the landscape is increasingly complex Limitations of Common Tests Limited number of alterations screened at once Misses some types of mutations DNA Mutation Detected or Missed by Traditional Testing Test Defects Can Miss Consumption of tissue sample Results are specific for the test used: need to know ahead of time what questions to ask IHC Protein expression Any alteration not know of ahead of time FISH Copy number alterations, Indels Rearrangement, Substitutions Hot Spot Panels Substitutions Indels, Copy number alterations, Rearrangements Genomic Alterations in Solid Tumors Widely accepted that the development and progression of cancer is associated with accumulation of alterations in the DNA sequences of the cancer cell genome that include: Base substitutions Short insertions and deletions Homozygous deletions Amplifications Fusions(translocations) Human Genome Project. Our understanding of the genetic underpinnings that initiate or drives malignant progression has set the benchmarks for the development of personalized cancer treatment. HKIAP Fall Scientific Meeting 2014 Page 7
8 Drivers and Passengers Critical so-called driver mutations or copy number alterations that occur in an solid tumors are relatively few. The number of driver alterations contributing to an individual patient s solid tumor is typically low and not predictable, and may change during the life of the tumor. DNA mutations and mutation combinations that exist between different individuals with the same type of malignancy are not predictable..no tumors are alike. Direct sequencing of the tumor cell DNA is required to define the genetic alterations for an individual (personal target analysis). Will this be useful? Cancer Databases The Cancer Genome Atlas of the National Cancer Institute ( Sanger Institute s Cancer Genome Projecthttp:// - map out all the somatic intragenic mutations in cancer. The COSMIC data base is a resource which displays the data generated from these experiments. The Cancer Genome Anatomy Project from National Cancer Institute also has banked information of research on cancer genome, transcriptome, and proteome. The International Cancer Genome Consortium is so far the biggest project to collect human cancer genome data. The data is accessible through the ICGC website. The Other Vital OMICS :Transcriptional Profiling, Epigenomics and microrna Cellular changes NOT associated with changes in the tumor cell DNA sequence. Transcriptomics:Profiles of cancer cell mrna expression, the transcriptome. Epigenomics: Gene expression silencing studied by epigenomic methods including DNA methylation assays. micrornaomics: the study of non-coding RNAs (including microrna novel molecular diagnostic assays designed for early cancer detection or prediction of prognosis. Traditional DNA Sequencing Techniques Primarily focused on germline detection of cancer predisposition. These single gene tests sequence only a select portion of the gene of interest where the greatest likelihood of a sequence abnormality is located. Examples BRCA1, BRCA2, hereditary non-polyposis coli (hmlh1, hmsh2) and other family cancer syndromes. Traditional sequencing has been utilized to genotype germline DNA to determine polymorphisms associated with anti-cancer drug metabolism and toxicity. Traditional HotSpot DNA sequencing of tumor tissue in clinical oncology practice today is focused on a small subset of cancer-related genes. HKIAP Fall Scientific Meeting 2014 Page 8
9 Traditional DNA Sequencing Platforms NGS Sequencing Technologies Method Basic Technique Sensitivity Advantages Disadvantages Sanger Chain Determination Method Pyrosequencing Sequencing by Synthesis Method Allele specific Real time PCR Real time PCR Melting Curve Mass Spectroscopy Based Sequencing (MALDI-TOF) Fluorescent labeled bases, DNA fragments separated by capillary electrophoresis Chemiluminescent DNA polymerase synthesizes complementary DNA to the unknown DNA template strand Primers span codon of interest and probes detect specific mutation Mutated DNA PCR products melt at lower temperatures than wild type DNA Single nucleotide primer extension assays High Higher Higher High Very high for base substitutions Historical Gold Standard Complete sequence More sensitive than Sanger Provides percentage of mutated versus wild type DNA Works well with fragmented DNA from FFPE samples Very high sensitivity Widely used for clinical testing for oncogene mutations in CRC/ NSCLC Very high sensitivity Provides percentage of mutated versus wild type DNA Readily identifies somatic point mutations and germline substitutions Very time consuming Cannot detect large deletions, translocations, copy number changes Short length reads limits technique to hot-spots Limited to hot-spots Does not provide specific abnormalities Limited to hot-spots Demand for more rapid and low-cost sequencing has driven the development of approaches designed to parallelize the sequencing process. These new massively parallel or next generation strategies in comparison with traditional Sanger and other methods, have increased sequencing rates by orders of magnitude and lowered the sequencing cost per base significantly. NGS to characterize the cancer cell genome in depth and further advance the field of personalized oncology. MPS SBS massively parallel sequencing using a proprietary reversible terminator-based method that enables detection of single bases as they are incorporated into growing DNA strands. A fluorescently labeled terminator is imaged as each dntp (deoxyribonucleotide triphosphates: datp, dctp, dgtp, or dttp) is added and then cleaved to allow incorporation of the next base. Since all four reversible terminator-bound dntps are present during each sequencing cycle, natural competition minimizes incorporation bias. The result is base-by-base sequencing that enables highly accurate data for a broad range of applications. NGS Sequencing Platforms Parameter Illumina HiSeq Illumina MiSeq 454 Pyrosequencing Ion Torrent Basic Technique Bead-based Dye Termination Bead-base Dye Termination Oil droplet based pyrosequencing Semiconductor-based Sequencing Major Users SNP Genotyping Clinical Molecular Diagnostics Whole Exome Sequencing Medium sized sequencing CNV Analysis Sequencing Whole Genome Resequencing SNP projects Target and Whole Exome detection Sequencing Whole Genome Resequencing Speed/TAT Immediate Fastest Fastest Fast 1 day to 3 days 5-65 hours <1 day Instrument Cost ~$ K ~$125K for MiSeq $ , ~108K for 454GS Junior ~$50K Length of reads Intermediate 2 X 300 bp Longest Intermediate 2 x 150 bp >300 bases, up to 1000bases Advantages Highest sensitivity for mutation Low cost of instrument Fast Low cost detection Rapid TAT Long reads useful for mapping Lower/ bioinformatics Can detect all classes of genomic expertise required alterations simultaneously (mutation, copy number, rearrangement) Disadvantages High cost Low depth of coverage High reagent costs Generally used as a hotspot Requires substantial operator Lack of sensitivity for low High error rates test and does not cover entire expertise mutant allel frequency tumors exome of selected genes High bioinformatics Lower sensitivity for mutation requirements detection Cannot detect gene amplification or homozygous deletions Cannot detect gene fusions High error rate in homopolymer sequences Nat Rev Genet 2010;11:31-46 HKIAP Fall Scientific Meeting 2014 Page 9
10 Illumina (Solexa) Sequencing Solexa, now part of illumina developed a sequencing technology based on reversible dye terminators. DNA molecules are first attached to primers on a slide and amplified so that local clonal colonies are formed (bridge amplification). Four types of ddntps are added, and nn-incorporated nucleotides are washed away. Unlike pyrosequencing, the DNA can only be extended one nucleotide at a time. A camera takes images of the fluorescently labeled nucleotides; then the dye along with the terminal 3 blocker is chemically removed from the DNA, allowing a next cycle. Hot-Spot Genotyping vs. Target Exome NGS Vs. Whole Genome Analysis Hot Spot Genotyping Target next Generation Sequencing Starting Material FFPE FFPE Fresh/Frozen Can be performed on small samples Mutation Detection Sensitivity Focused on cancerrelated genomic alterations Detects all relevant classes of genomic alterations (copy number, mutation, rearrangement) Requires Matched Normal Tissue Sample Yes Yes Unknown Whole Genome Analysis Varies with technique used, Highest Reduced by low average depth Sanger technique rapidly loses Most uniform depth of of coverage sensitivity when relative coverage percent of tumor DNA drops below 50% Yes Yes No creates the haystack and surrounds the needle No Yes Yes No Not absolutely necessary but it is preferred Yes Flexible to add new genes to test Analysis Complexity and TAT No Yes NA Low Intermediate High Challenges for Delivering NGS Results for Personalized Therapy Selection of NGS Platform. -driven by a variety of factors including system cost, degree of expertise needed to achieve optimum performance and analytic performance in the clinic (sensitivity, specificity, types of alterations detected, etc). Selection of an Appropriate Assay. -the laboratory providing the NGS clinical testing must create its own validated assay that includes all components of the test from initial accessioning, pathology review, DNA extraction, sequencing data analysis, curation and report generation. Cost of the NGS System. More advanced NGS systems have high entry level costs of hardware and high reagent costs per sample processed. This can significantly impede the adoption of NGS technology especially in small less well-capitalized laboratories. Adapted from Simon and Roychowdry, Challenges:Samples Obtaining an Adequate Sample to Sequence. Clinical NGS performed for patients with sold tumors generally uses formalin fixed paraffin embedded material. In general a sample of approximately 15mm with a minimal depth of 40 microns is adequate for NGS. For assay systems that are going to measure gene copy number in addition to searching for mutations, a relative tumor nuclei proportion of the total tissue nuclei present needs to be 20% or greater. When tumor nuclei proportions are below 20%, the risk of missing a copy number alteration or homozygous loss increases rapidly. In general, more samples are rejected as inadequate for NGS testing because they fail to exceed a 20% relative tumor nuclei than due to being too small to extract. If a matched normal blood sample is also sequenced, which is clearly preferable for scientific if not logistical and cost reasons, it may be possible to use computational methods to identify copy number alterations in less pure samples. HKIAP Fall Scientific Meeting 2014 Page 10
11 Challenges:Samples Sample Enrichment. When larger specimens are below the 20% tumor nuclei cut-off, they can often be enriched by simple macrodissection System Validation. Validating the sensitivity and specificity of an NGS One approach to achieve this has been the use of Hapmap cell lines know to have specific genomic alterations that can be diluted down to low mutant allele frequencies (MAF) and run in parallel with clinical samples. The more traditional approach is to obtain sets of samples with known mutations (as defined by another method or another lab) in each of the genes of interest. However, this approach is generally feasible only for the most commonly mutated genes. Sample Turnaround Time: ~two weeks. Challenges: Bioinformatics Requirements Although the selection and proper management of NGS system requires technical expertise in general, the bioinformatics expertise required to perform sensitive and specific therapy impacting NGS is most critical. Statistical analysis of system performance including depth of sequencing coverage and uniformity of coverage is typically performed by the bioinformatics team. The software that drives the decisions as to what alterations are truly present and which ones are clinically significant is rarely ready to go out of the computational box that accompanies the hardware. Local algorithm construction and software modifications are typically needed to allow the system to achieve full performance in sensitivity and specificity. The lack of trained bioinformaticians capable of managing NGS data systems software is a major impediment to the development of NGS testing services in many clinical laboratories. Tumor Genomic heterogeneity A concern when testing both primary and metastatic tumors is the potential for a genomic alteration to be subclonal in the primary tumor or that there may be differences in genomic alterations between the primary and metastatic lesions. Some reports have shown significant variable alterations in a solid tumor such as renal cell carcinoma (Gerlinger M et al NEJM 366(10) 883), others have argued that the driver alterations that are the primary targets of potential therapies are rarely heterogenous unlike the so-called passenger alterations. Similarly, despite concerns about likely differences, published studies comparing the NGS results on primary tumors vs metastatic lesions in the same patient have been notable for the lack of driver alteration heterogeneity. Is NGS the final answer? Probably NOT. Actionable vs Non-actionable Genomic Alterations The term actionable has been applied to somatic cancer genotyping to indicate where the results of sequencing can potentially direct a specific action on the part of the patient s oncologist in response to the sequencing results. There is universal agreement that the alterations in a gene associated with a specific approved therapy in that tumor type is actionable. Most investigators also agree that an alteration indicating a specific approved therapy but in a tumor type that is not approved ( off indication ) is also actionable although it would require the off-label drug use. The most controversial actionability definition has centered around alterations that are directly listed in entry criteria for registered anticancer clinical trials at In some of these genomic alteration targeted therapy trials the association of the sequence result with the drugs mechanism of action or clinical responses is straight forward and well-accepted, in others the alteration and drug link is not as well-established. HKIAP Fall Scientific Meeting 2014 Page 11
12 Correlation of Genomic Alterations with Tumor Diagnosis Given that the FDA continues to approve anti-cancer drugs based on their site of origin, a careful pathology review is required to assign the correct histopathologic diagnosis to the sequence results. Alterations associated with selection of targeted therapies for that cancer type will be considered on-label (e.g. EGFR activating mutation in lung adenocarcinoma) as compared to cases where the same alteration found in another tumor type would generate a recommendation for drug use off-label. Although curation for well-known alterations may be relatively straight forward, as the list of anti-cancer drugs linked to genomic alterations continues to grow, having a skilled curation team capable of searching the current literature and databases is a critical component of the NGS reporting process. The NGS Patient Report The report that is generated from an NGS assay in a solid tumor must be both concise and informative. The report should list the important alterations and associated therapies in an easy format for the oncologist to act on with the details of pathway biology and scientific significance provided separately in the report available for detailed reading. A major advantage for NGS report is when the detected alteration can be used to recommend registered appropriate clinical trials. NGS Regulatory Status Numerous NGS testing providers are now present throughout the United States with CLIA certification Several have also achieved CAP accreditation Recently, a major NGS platform (the Illumina MiSeq) was approved by the FDA although this approval was not for a cancer NGS application Approvals by the FDA for cancer-related NGS testing are anticipated to follow the approval for testing for germline inherited disorders. Should an NGS test become a companion diagnostic and included in a drug label, FDA approval of that NGS assay will be required. Whole Exome and Whole Genome Sequencing? The low and uneven coverage of WGS/WES makes the likelihood of missing actionable alterations in impure specimens unacceptably high. It would be extremely difficult to generate a report that is meaningful to a community oncologist if you don t limit the analysis to genes known to be relevant for human cancer. WES/WGS requires a matched normal DNA sequence to exclude the 100s to 1,000s of rare germine variants not in SNP databases which does easily fit into routine clinical practice. WES/WGS could thus increase the likelihood of an inappropriate decision to target a germline variant of unknown significance with a drug unlikely to benefit the patient. Cost.very high HKIAP Fall Scientific Meeting 2014 Page 12

13 Selected Examples of Cancer Genome Sequencing and Anti-Cancer Drug Selection Genetic Event Disease Drug KRAS Mutation CRC Cetuximab/Panitumumab (contraindicated by KRAS mutation) BRAF Mutation Melanoma Vemurafenib/Dabrafenib EGFR Mutation NSCLC Gefitinib/Erlotinib/Afatinib EMLA, ALK Translocation NSCLC Crizotinib Kit Mutation GIST/melanoma Imatinib/Sunitinib/Regorafenib/ Pazopanib BCR-ABL Translocation CML Imatinib/Dasatinib/ Nilotinib/Bosutinib PML-RARA Translocation (t15;17) HER2 Gene Amplification* APL Breast and Upper GI Cancer ATRA Trastuzumab/Lapatinib ROS1 Fusion NSCLC Cabozantinib (investigational) RET Fusion NSCLC Cabozantinib (investigational) Somatic genome alterations are central to cancer pathogenesis While germ-line mutations can increase the risk of cancer, most cancer causing mutations are somatic Somatic-mutations are present in the cancer DNA but not in the germ-line DNA Somatic alterations can provide a large therapeutic window Genome-targeted treatments can be selective for the genomically altered cancer cell and spare the rest of the body, which is genomically normal Somatic alterations are internally controlled Comparison between germ-line and cancer defines the cancer specific alterations and allows precise diagnosis Progress in Lung Cancer Lung Cancers are among the most genomically deranged of all cancers -mutations and rearrangements Lung Adenocarcinoma AKT1 P1K3CA BRAF HER2 MAP2K1 NRAS ROS1 fusions RET fusions ALK fusions EGFR Unknown KRAS Seidel et al. Sci Transl Med Oct 30, Modified from Pao and Hutchinson, Nature Medicine. 2012; 18: HKIAP Fall Scientific Meeting 2014 Page 13


 Activation loop mutations (L858) Associated with response to erlotinib/gefitinib")
14 Genetic alterations in lung adenocarcinoma Genetic Alterations in SQC (mutations, amplifications) WT ALK KRAS EGFR KRAS EGFR ALK NF1 METexon14 HER2-mut BRAF PI3KCA MET amp AKT MAP2KI ROS1 KIF5B-RET HRAS NRAS WT 33 Courtesy of Dr. Elisabeth Brambilla 34 Gene expression subtypes of SQC EGFR mutants in lung adenocarcinoma Somatic EGFR mutations found in ~30 to 60% of East Asian lung adenocarcinomas, 10-15% of U.S. and European patients Clustered in four areas Nucleotide binding loop (P loop), G719 Exon 19 deletions (ELREA) Exon 20 insertions (C-terminal to alpha helix) Activation loop mutations (L858) Associated with response to erlotinib/gefitinib (except for exon 20 insertion mutants) 35 Nature 2012 HKIAP Fall Scientific Meeting 2014 Page 14
15 Translocations in lung adenocarcinoma ALK Lung adenocarcinoma Crizotinib, investigation agents Soda, 2007;Rikova, 2007 ROS1 Lung adenocarcinoma Crizotinib, investigation agent Rikova, 2007 RET Lung adenocarcinoma Vandetanib, cabozantinib, other Ju, 2011 Kohno, 2012; Lipson, 2012; Takeuchi, 2012 NTRK1 Valshnavi, Capelletti et al. nature Medicine, 2013 CD74-NRG1 fusions (Lynette-Fernandez-Cuesta presentation at WCLC) SND1-BRAF fusions (Jin Jen presentation at WCLC) Lung adenocarcinoma genome analysis conclusions Very high mutation rate with many significant genes yet to be discovered Recurrent mutations in splicing factor genes including U2AF1 and RMB10; mutations in epigenome, genes including ARID1A, SMARCA4 Recurrent splice site mutations in MET leading to skipping of exon 14 containing a Cbl ubiquitination site Not all driver oncogenes in the receptor tryosine kinase/ras/raf pathway are yet known: RIT1 is an additional candidate as are NF1 loss of function mutations and ARAFRAF1 mutations Lung Squamous cell carcinoma: site of knowledge on genomic targets 2010 Lung squamous cell carcinoma causes an estimated 45,000 patient deaths per year in the U.S. so developing new treatments is critical Individual mutated genes are known, but there have been no systematic genomic studies of lung squamous cell carcinoma few known driver oncogenes that may be therapeutic targets Finding molecular targets in lung adenocarcinoma and squamous cell lung cancer genomes Many different therapeutic targets in each cancer type Include mutations, rearrangements and amplifications of many genes Therefore need to analyze multiple genes according to multiple methods or by comprehensive sequencing Lung Adenocarcinoma Lung squamous cell carcinoma Amp Mut Transloc Amp Mut Transloc EGFR EGFR EGFR EGFR EGFR FGR3 ERBB2 ERBB2 ALK ERBB2 PIK3CA MET KRAS ROS1 FGFR1 FGFR2 BRAF RET FGR3 MET NTRK1 DDR2 RIT1 NRG NF1 ARA/R AF1 HKIAP Fall Scientific Meeting 2014 Page 15
16 24 hrs 1-2 working days (except IHC) 10 working days Routine work up of lung adenocarcinomas Tissue collection/fixation Fixation/Tissue Processing Pathologists review and report EGFR mutation testing ALK-FISH Biopsy Pathology Molecular testing Lung cancer genomes and target therapies Novel targetable alterations still being found ROS1, RET, NTRK1 translocations in lung adenocarcinoma RIT1, ARF, RAF1 and MET (splicing) mutations DDR2, FGFR1, FGFR2, FGFR3 in squamous cell lung cancer FGFR1 in small cell lung cancer HLA-A mutations suggest link between genomics and immunotherapy TP53 is most commonly mutated gene across lung and other cancers so if we want to cure cancer, we should look at p53-selective interuption. Final report with tumor histology and mutation results Final report NGS Findings in Breast Cancer Detection of HER2 amplification highly correlates with FISH results on same specimen NGS also detects ERRB2 (HER2) mutations (base substitutions) and fusions not searched for routinely by other methods CDH1 mutated ILC enriches for ERBB2 mutations/fusions ERBB2 mutations in HER2 IHC/FISH tumors can activate ERBB2 signaling and early evidence suggests that they are sensitive to anti HER2 targeted therapies NGS can detect other unexpected targets in relapsed/refractory metastatic breast cancer that are sensitive to target therapies EGFR mutation and TKI response (erlotinib) ESR1 mutation and resistance to Tamoxifen Triple Negative tumors have more alterations than other sub-types including potentially actionable alterations that could lead to non- HER2 based targeted therapies. ESR1 Mutation in Breast Cancer NGS study of 249 breast cancers 12% frequency of ESR1 somatic mutations in relapsed ER+ breast cancer Primary tumors were ESR1 WT Pre-clinical models show ESR1 activation and resistance to endocrine therapy ESR1 mutation testing might explain hormonal therapy resistance and can personalize therapy selection in ER+ metastatic breast cancer Jeselesohn R. Yelensky R, Buchwalter G et al. Emergence of constitutively active estrogen receptor-a mutations in pretreated advanced estrogen receptor positive breast cancer. Clin. Cancer Res 2014 Jan 7. HKIAP Fall Scientific Meeting 2014 Page 16
17 Frequency of ESR1 mutation in recent studies % ( ) 90.00% 00% 80.00% 70.00% 60.00% 50.00% 40.00% 30.00% 20.00% 10.00% 0.00% 0.00% 50.00% 54.55% Li S, Cell reports Robinson DR, Nature genetics 3.28% 17.50% Toy W, Nature genetics 38.46% 1.72% 15.79% Lamin KM, Jeselsohn R,Clin Cancer Research Cancer Res ESR1 mut/pri/er+ ESR1 mut/met/er+ NGS of Residual Disease of TNBC after Neoadjuvant Chemotherapy Identifies Actionable Therapeutic Targets In TNBC patients lacking a pcr neoadjuvant Rx selects a subpopulation of chemotherapy resistant tumor cells. NGS was performed on the residual disease of 74 TNBs with residual disease after neoadjuvant Rx and on 20 matched pretreatment biopsies. Combined NGS and digital RNA expression analysis identified diverse molecular lesions and pathway activation in drug-resistant tumor cells. Ninety percent of the tumors contained a genetic alteration potentially treatable with a currently available target therapy. These data can guide biomarker-driven adjuvant studies targeting micrometastases in chemoresistant TNBC to improve the outcome of patients Thus, because TNBCs that do no achieve a pcr after neoadjuvant Rx are likely to recur as metastatic disease at variable times after surgery, these alterations may guide the selection of targeted therapies immediately after mastectomy before these metastases become evident. Balko JM et al. Molecular Profiling of the Residual Disease of Triple- Negative Breast Cancers after Neoadjuvant Chemotherapy Identifies Actionable Therapeutic Targets. Cancer Disco Jan 23, PMID NGS Findings in Metaplastic Breast Cancer A total of 93 GA were identified, with at least one alteration identified in all cases for an average of 4.65 GA per tumor Nineteen (95%) MPBC cases harbored a total of 36 actionable GA with an average of 1.8 actionable GA per tumor This result is similar to a series of 273 routine breast cancer evaluated by the same assay, where 246 (87%) had actionable GA The most common unactionable GA were alterations in TP53 (80%) MYC (30%) MLL2(25%) and KDM6A (10%) The most common actionable GA were mutations, amplifications and homozygous deletions of PIK3CA (40%), PTEN (25%) and CDKN2A/B (20%), EGFR (10%) and HRAS (10%) with AKT3, BRCA2, CCND1, CCND2, CCNE1, CDK4, FBXW7, FGFR1, NF1, PIK3R1 and SRC altered in a single case The MPC EBB2 (HER2) negative status was identical to IHC/FISH results in 100% of cases. MammoSeq 1) Mutations from primary and metastatic breast cancer 2) Common actionable mutations from other cancers (e.g. B-RAF) 3) Rare actionable mutations (e.g. ErbB2) 4) Copy number amplification and deletions 5) Breast cancer susceptibility genes HKIAP Fall Scientific Meeting 2014 Page 17


 Interrogating gene for both point mutation and CNV changes (with additional amplicons if")
18 MammoSeq ABL1 CDK4* FGFR4* KIT NOTCH1 AKT1 CDKN1B FOXA1 KRAS NRAS AKT3* CDKN2A GATA3 MAP2K4 PAK1* ALK CTNNB1 GRB7* MAP3K1 PDGFRA AR* DNAH14 HIST2H2BE MAP3K4 PIK3CA* ARID1A EGFR* HLA-A MDM2* PIK3R1 ATM ERBB2* HRAS MDM4* PTCH1 AURKA* ERBB3* IDH1 MET* PTEN AURKB* ERBB4 IGF1R* MLL3 RB1 BRAF ESR1* INPP4B* MTOR RET BRCA1 EZH2 INSR* MYC* RPTOR BRCA2 FGF19** JAK2* NCOA3* RUNX1 CCND1* FGFR1* JAK3* NCOR1 SMO CCNE1* FGFR2* JUN NCOR2 STK11 CDH1 FGFR3 KDR NF1 TP53 Gene not previously on PCMP and thus specific to our breast cancer panel * Removed from PCMP - rarely mutated in breast cancer or no obvious therapy APC CSF1R FBXW7 FLT3 GNA11 GNAS GNAQ HNF1A IDH2 MLH1 MPL NPM1 PTPN11 SMAD4 SMARCB1 SRC BRCA1/2 unsure because of potential germline finding and resulting difficulty in interpretation MAP2K4, MAP3K1, MAP3K4 unsure because of typical tumor suppressor mutation phenotype (few recurrent mutations, spread across entire gene, many amplicons) PAK1 two mutations not meeting criteria are being included because we are testing for CNV anyway (design CNV amplicons to overlap with these mutations) Interrogating gene for both point mutation and CNV changes (with additional amplicons if necessary) 50 FoundationOne : Comprehensive NGSbased Genomic Profiling Assay Workflow (14-17 days) 1) Sample preparation: Extensive optimization 2) LC, Hybrid capture: Extensive optimization Pre-Analytic Process (Pre-Sequencing) 3) Analysis pipeline: Advanced computational biology 4) Clinical report: Resource Intensive Post-Analytic Process (Post-Sequencing) Translating research grade NGS to a clinical cancer diagnostic assay requires extensive optimization and investment 51 FoundationOne : Breakthrough breadth and sensitivity: ty: less s time, cost and tissue Ordered by Oncologist Sent by Pathologist Works in routine, real-world setting Requires small amount of routine tissue 236 genes sequenced for all four major classes of alterations: insertions and deletions, copy number alterations, rearrangements, base substitutions Predictors of response or resistance to therapy e.g. ABL1 KRAS MET SRC ALK PDGFRA MTOR AKT1 BRAF RARA PIK3CA AR EGFR FGFR1 PTCH1 KDR ERBB2 FLT3 PTEN NF1 KIT JAK2 RET SMO BCL6 CDH1 CRLF2 EZH2 IKZF1 Indicators of Prognosis JAK1 MSH6 SMAD4 MEN1 MUTYH SOX2 MLH1 PAX5 WT1 MRE11A RB1 MSH2 SMAD2 >99% sensitivity and specificity to call mutant alleles at 5% frequency >95% lab success rate ~ day turn-around from receipt of tissue Results delivered through our Interactive Cancer Explorer FoundationOne TM Solution A fully informative genomic tumor profile Individualized, actionable information leads to treatment options unique to each patient Integrated complex genomic information in an understandable format for partners, physicians, patients >99%* sensitivity at >5% MAF for base substutions 98%* sensitivity at >10% MAF for insertions/deletions Connecting science, medicine and IT for truly personalized treatments and rapid medical discovery This method could save time, money and precious tumor samples while providing highly sensitive and more comprehensive information than what is currently available. - W. Pao, Nature Medicine *Lipson et al. Presented at Advances in Genome Biology & Technology Meeting. 23 February HKIAP Fall Scientific Meeting 2014 Page 18

 For a complete list of the genes assayed, please refer to the Appendix (in another tumor type) Note: Genomic alterations detected may be associated with activity of certain")


19 Diagnosis Patient Name Report Date Lung adenocarcinoma Date of Birth Not Given Client Cancer Center Specimen Received Not Given Gender Female Ordering Physician Doctor, Denise Specimen Site Lymph Node FMI Case # SRF Additional Recipient Not Given Date of Collection Not Given Medical Record # FMI Client # -1 Specimen Type Block Specimen ID Not Given Pathologist Not Given FoundationOne is a next-generation sequencing (NGS) based assay which identifies genomic alterations within hundreds of cancer-related genes. (in patient s tumor type) For a complete list of the genes assayed, please refer to the Appendix (in another tumor type) Note: Genomic alterations detected may be associated with activity of certain FDA approved drugs; however, the agents listed in this report may have varied clinical evidence in the patient s tumor type. Neither the therapeutic agents nor the trials identified are ranked in order of potential or predicted efficacy for this patient, nor are they ranked in order of level of evidence for this patient s tumor type. Electronically Signed by Jeffrey S. Ross M.D., Medical Director CLIA Number: 22D Foundation Medicine, Inc., One Kendall Square Ste B3501, Cambridge MA page 1 of 11 FoundationOne : Comprehensive NGSbased Genomic Profiling Assay Specifications One comprehensive genomic profile for all solid tumors to simultaneously detect all clinically relevant classes of genomic alterations in a single assay Targeted sequencing of 236 known clinically & biologically relevant cancer genes (exons and selected introns) Validated accuracy achieved by high, uniform coverage: >99.5% of exons covered >100X Requires small amounts of tissue from routine FFPE samples, including needle biopsies ( 50ng of DNA) Customized computational biology algorithms validated for high accuracy in clinical samples with high stromal contamination FoundationOne Report: Clear Results On The First Page ABOUT THE TEST: PATIENT RESULTS TUMOR TYPE: LUNG ADENOCARCINOMA 4 genomic alterations Genomic Alterations Identified ALK EML4-ALK fusion 3 therapies associated with potential clinical benefit TSC2 splice site G>A CDKN2A/B loss 0 therapies associated with lack of response TP53 L194R Additional Disease-relevant Genes with No Reportable 6 clinical trials Alterations Detected EGFR KRAS THERAPEUTIC IMPLICATIONS Genomic Alterations FDA Approved Therapies FDA Approved Therapies Potential Clinical Trials Detected ALK Crizotinib None Yes, see clinical trials EML4-ALK fusion section TSC2 None Everolimus Yes, see clinical trials splice site G>A Temsirolimus section CDKN2A/B None None Yes, see clinical trials loss section TP53 None None None L194R Patient and ordering physician information Summary of results and genomic alterations identified Targeted therapies and clinical trials that may be relevant based on genomic alterations identified Report, Inform, And Share Basket Trials 55 Extremely complex molecular information distilled into one easily accessible and discernible report An example of a large basket trial currently enrolling is the NCI Molecular Analysis for Therapy Choice (MATCH) trial. More than 200 actionable mutations/amplifications /translocations are assessed in pretreated solid tumors and lymphomas of varying histology; patients are then matched to investigational drugs directed at the mutation of interest. The objective of the trial is to assess whether the response rate and/or 4-month progression- free survival is improved following treatment with agents chosen based on the presence of specific mutations in patient tumors. Currently, the trial has 20 treatment arms looking at targeted therapy directed toward mutations. HKIAP Fall Scientific Meeting 2014 Page 19
20 Umbrella Trials Whereas in basket studies researchers test the effect of a single drug, on a single mutation in a variety of cancer types, umbrella studies are designed to test the impact of different drugs on different mutations in a single type of cancer. In the BATTLE umbrella trial, for example, researchers recruited non-small cell lung cancer patients, genetically profiled their tumors to determine which mutations they had, and then assigned them to receive a particular drug expected to target their mutations. Basket and umbrella studies represent novel approaches to testing targeted therapeutics. Both types of studies have the potential to accelerate the drug development process so that the right therapies can quickly be delivered to the right patients. Overview of Sequencing and Other Molecular Techniques Relevant to Targeted Therapy David J Dabbs, MD University of ddabbs@upmc.edu HKIAP Fall Scientific Meeting 2014 Page 20

21 PRINCIPLES OF MOLECUAR TESTING: THE IMPORTANCE OF REGULATIONS 52 year old, 1.4 cm IDC, NG 2, ER/PR strong + Her2 (-), Lumpectomy, SLN(-) DAVID J DABBS, M.D PROFESSOR AND CHIEF OF PATHOLOGY MAGEE-WOMEN S HOSPITAL OF UPMC PITTSBURGH, PA Doctor, what will happen to me now? Tumor Size, Grade, Lymph Node Status, ER, PR, Her2 Erb2+ Basal-like Normal breast ER Alpha+ Sorlie, Therese et al. (2001) Proc. Natl. Acad. Sci. USA 98, Copyright 2001 by the National Academy of Sciences HKIAP Fall Scientific Meeting 2014 Page 21
 is a robust, prognostic, with good to excellent reproducibility.")

22 Dendrogram Intrinsic Classification Breast cancer prognostic classification in the molecular era: the role of histological grade *Breast Cancer Res. 2010;12(4):207. doi: /bcr2607. Epub 2010 Jul 30. Review. PMID: Histologic grade (NGS) is a robust, prognostic, with good to excellent reproducibility. The scrutiny applied to histologic grading has only recently been applied to molecular tests. 36% intermediate Histologic Grade; 40% of oncotype dx tests are Intermediate RS. Rare: Grade 1-Grade3. *Rakha EA, Reis-Filho JS, Baehner F, Dabbs DJ, Decker T, Eusebi V, Fox SB, Ichihara S, Jacquemier J, Lakhani SR, Palacios J, Richardson AL, Schnitt SJ, Schmitt FC, Tan PH, Tse GM, Badve S, Ellis IO. Grade and Distant Recurrence Paik S et al. NEJM : Tumor Size and Distant Recurrence Paik S et al. NEJM : HKIAP Fall Scientific Meeting 2014 Page 22
:4273-8. doi: 10.1200/JCO.2010.31.2835. Epub 2011 Oct 11.")
 + PRIHC*(- 0.02925)+(0 for HER2 negative, 0.77681 for equivocal, 11.")
23 Prediction of the Oncotype DX recurrence score: use of pathology-generated equations derived by linear regression analysis Molly E Klein, David J Dabbs, Yongli Shuai, Adam M Brufsky, Rachel Jankowitz, Shannon L Puhalla and Rohit Bhargava ER/PR/Her2 Ki67.. Immunohistochemistry IHC4~Oncotype Dx J Clin Oncol Nov 10;29(32): doi: /JCO Epub 2011 Oct 11. PMID: Magee equations: Mod Pathol 2013 PMID ons.html New Magee equation 1: Recurrence score = Nottingham score* ERIHC*( ) + PRIHC*( )+(0 for HER2 negative, for equivocal, for HER2 positive)+ tumor size* Ki-67 index* New Magee equation 2: Recurrence score = Nottingham score* erihc*( )þ PRIHC*( )+(0 for HER2 negative, for equivocal, for HER2 positive++tumor size* New Magee equation 3: Recurrence score = ERIHC*( ) + PRIHC*( ) + (0 for HER2 negative, for equivocal, for HER2 positive) + Ki-67* HKIAP Fall Scientific Meeting 2014 Page 23
24 MOLECULAR TEST ISSUES Analytical validity; clinical validity; clinical utility. Platform: RT-PCR, Nanostring, cdna microarry Reproducibility: tissue selection, microdissection, dilution, mrna robust? Comparison of tests: half of Oncotype Dx intermediate RS are MammaPrint high risk. The seduction of the black box. Laboratory developed test (LDT) In vitro diagnostic multivariate index assay (IVDMIA) IVDMIA Laboratory developed test (LDT) In vitro diagnostic multivariate index assay (IVDMIA) A laboratory-developed IVDMIA (Oncotype Dx) is a specific subset of LDTs and is not FDA cleared/approved. LDT-laboratory developed test whose performance is determined by the lab. HKIAP Fall Scientific Meeting 2014 Page 24
25 Laboratory developed test (LDT) In vitro diagnostic multivariate index assay (IVDMIA) CLIA CLIA-CLINICAL LABORATORY IMPROVEMENT ACT 1988 Laboratory quality standards Does not assure test accuracy, efficacy or safety of IVDMIAs to this date, does not address molecular testing of IVDMIAs. TAKE HOME MESSAGES-BREAST CANCER MOLECULAR TESTING There are NO gold standards for molecular pathology testing. TAKE HOME MESSAGES-BREAST CANCER MOLECULAR TESTING There are NO gold standards for molecular pathology testing. There are NO CLIA standards.-standards for operating a laboratory. HKIAP Fall Scientific Meeting 2014 Page 25
26 TAKE HOME MESSAGES-BREAST CANCER MOLECULAR TESTING There are NO gold standards for molecular pathology testing. There are NO CLIA standards. There are no quality assessments. TAKE HOME MESSAGES-BREAST CANCER MOLECULAR TESTING There are NO gold standards for molecular pathology testing. There are NO CLIA standards. There are no quality assessments. There is no proficiency testing. TAKE HOME MESSAGES-BREAST CANCER MOLECULAR TESTING There are NO gold standards for molecular pathology testing. There are NO CLIA standards. There are no quality assessments. There is no proficiency testing. There is no proven clinical utility for these tests. (Benefit beyond clinicopathologic data) There are NO gold standards for molecular pathology testing. There are NO CLIA standards. There are no quality assessments. There is no proficiency testing. There is no proven clinical utility for these tests. (Benefit beyond clinical-pathologic data) Benefits and harms are unknown for individual patients. HKIAP Fall Scientific Meeting 2014 Page 26
27 TAKE HOME MESSAGES-BREAST CANCER MOLECULAR TESTING There are NO gold standards for molecular pathology testing. There are NO CLIA standards. There are no quality assessments. There is no proficiency testing. There is no proven clinical utility for these tests. (Benefit beyond clinical-pathologic data) Benefits and harms are unknown for individual patients. FDA clearance/approval is the FIRST STEP to patient safety and clinical transparency. TAKE HOME MESSAGES-BREAST CANCER MOLECULAR TESTING There are NO gold standards for molecular pathology testing. There are NO CLIA standards. There are no quality assessments. There is no proficiency testing. There is no proven clinical utility for these tests. (Benefit beyond clinical-pathologic data) Benefits and harms are unknown for individual patients. FDA clearance/approval is the FIRST STEP to patient safety and clinical transparency. Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group EGAPP, a project developed by the National Office of Public Health Genomics at the CDC to support a rigorous, evidence-based process for evaluating genetic tests and other genomic applications that are in transition from research to clinical and public health practice in the U.S. A key goal of the EWG is to develop conclusions and recommendations regarding clinical genomic applications, and to establish clear linkage to the supporting scientific evidence. Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group Genetics in Medicine Volume 11, Number 1, January 2009 Summary of Findings on Gene Expression Profiling To Predict Risk for Breast Cancer Recurrence..there was not enough evidence to state whether breast cancer GEP should or should not be used for early stage breast cancer treatment decision making. The balance of benefits and harms of using breast cancer GEP could not be determined from the available evidence. HKIAP Fall Scientific Meeting 2014 Page 27
28 EWG Summary no direct or indirect evidence linking tumor gene expression profiling of women with breast cancer to improved health outcomes. further development and evaluation of these technologies encouraged. EWG Summary Does it improve health outcomes? What are the benefits? (reduced adverse events due to low risk women avoiding chemotherapy) The harms? (withholding chemotherapy in patients who need it) IVDMIAs (In Vitro Diagnostic Multivariate Index Assays) Definition (FDA) 1) Combines the values of multiple variables (genes) using an interpretation function to yield a single, patient-specific result (e.g., a classification, score, index, etc.), that is intended for use in the diagnosis of disease or other conditions, or in the cure, mitigation, treatment or prevention of disease, and 2) Provides a result whose derivation is nontransparent and cannot be independently derived or verified by the end user. IVDMIAs are inherently different from other LDTs in that they have Complex unique interpretation functions -LDT IVDMIAs high risk, high impact assays that raise significant issues of safety and effectiveness There is a need for FDA to regulate these devices to ensure that the IVDMIA is safe and effective for its intended use. HKIAP Fall Scientific Meeting 2014 Page 28

 21 genes: 16 known functions 5 reference genes 0 unknown functions NSABP Clinical Trials Overview Protocol B-20")
29 Oncotype DX Selection Process RT-PCR Technology 250 candidate genes derived from the available literature (the knowledge of the year 2000) NSABP Clinical Trials Overview Protocol B /4/82-1/25/88 A Clinical Trial to Assess Tamoxifen in Patients With Primary Breast Cancer and Negative Axillary Nodes Whose Tumors are Positive for Estrogen Receptors 1998-Her2 therapy approved for metastatic breast cancer 2005-Her2 therapy in adjuvant setting (5 clinical trials) 21 genes: 16 known functions 5 reference genes 0 unknown functions NSABP Clinical Trials Overview Protocol B-20 A Clinical Trial to Determine the Worth of Chemotherapy and Tamoxifen over Tamoxifen Alone in the Management of Patients with Primary Invasive Breast Cancer, Negative Axillary Nodes and Estrogen-Receptor-Positive Tumors Tamoxifen vs CMF vs MF Building the Oncotype Test Tamoxifen treated population (?50%) At least 10% Her2+ (unknown at the time). Cohort from 30 years ago 1/3 of patients (~220) premenopausal;2/3 postmenopausal(~450) CMF Chemotherapy Tumor margins HKIAP Fall Scientific Meeting 2014 Page 29

30 PROLIFERATION Ki-67 STK15 Survivin Cyclin B1 MYBL2 INVASION Stromolysin 3 Cathepsin L2 HER2 GRB7 HER2 Oncotype DX: 21 Gene Recurrence Score (RS) Assay Validation set as a Prognostic Test: 668 patients NSABP B-14 Paik et el NEJM : Cancer and 5 Reference Genes From 3 Studies ESTROGEN Coefficient x Expression Level ER PR Bcl2 SCUBE2 The RS recurrence = score x HER2 defined Group as: Score RS= x 4xER HER2 Group Group Score Score x 1.04 ER Group x Proliferation Score eat rat ion ngroup Score x 0.10 Proliferation x Invasion Group Group Score Score x Invasion 05 x CD68 Group Score GSTM1 BAG x CD68 x GSTM x 007x 0.07 GSTM1 7xB BAG1 CD x BAG1 Scaled 0 to 100 Category RS (0 100) REFERENCE Beta-actin GAPDH RPLPO GUS TFRC Low risk Int risk High risk RS < 18 RS 18 and < 31 RS 31 Oncotype dx Recurrence Score Curve Paik S, Tang G, Shak S et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptorpositive breast cancer. J Clin Oncol 2006;24: Ioannidis J. TheOncologist2007;12: Goal-to show magnitude of benefit of chemotherapy from the Recurrence Score: Tamoxifen vs CMF vs MF Used the Tamoxifen arm of B20 as a training set, and in the validation set (!) Mixing training and test datasets: a failed validation presented as a successful validation, with extension of the clinical indications for the test. The development of the 21-gene recurrence score (Oncotype DX ) involved training in data from the patients of the tamoxifen arm of (NSABP)-20 trial. HKIAP Fall Scientific Meeting 2014 Page 30

31 (from Paik S, Tang G, Shak S et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J Clin Oncol 2006;24: Ioannidis J. TheOncologist2007;12: Mixing training and test datasets: a failed validation presented as a successful validation, with extension of the clinical indications for the test. The development of the 21-gene recurrence score (Oncotype DX ) involved training in data from the patients of the tamoxifen arm of (NSABP)-20 trial. NICE NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE n3 (FEBRUARY 2013) Gene expression profiling and expanded immunohistochemistry tests to guide the use of adjuvant chemotherapy in early breast cancer management - MammaPrint, Oncotype DX, IHC4 and Mammostrat: diagnostics consultation 3 NICE The Committee concluded that the evidence implying a predicted differential relative benefit of chemotherapy according to Oncotype DX risk group in LN- patients (Paik et al. 2006) was not robust. The Committee also reviewed evidence implying a predicted differential relative benefit of chemotherapy according to Oncotype DX risk group in LN+ patients (Albain et al. 2010) and data from the neoadjuvant setting. The Committee concluded that these data were not robust enough to support the test s ability to predict the benefit of chemotherapy. HKIAP Fall Scientific Meeting 2014 Page 31


 PPA All 23 equivocal FISH cases NEGATIVE HKIAP Fall Scientific")
32 Published Ahead of Print on October 11, 2011 as /JCO The latest version is at Riverside Methodist Hospital (Mayo Clinic), Cleveland Clinic, UPMC- Magee Take Home Message Of 36 UNEQUIVOCAL POSITIVE IHC/FISH CASES: 14/36 GHI called NEGATIVE(39%) 12/36 GHI called EQUIVOCAL (33%) 10/36 GHI called POSITIVE (28%) PPA All 23 equivocal FISH cases NEGATIVE HKIAP Fall Scientific Meeting 2014 Page 32








33 Take Home Message #2 23 FISH EQUIVOCAL CASES 100% NEGATIVE by Odx Her2 qrt-pcr MWH+/GHI equivocal case 8 Laboratories World-Wide have now documented the Her2 single gene flaw in Oncotype Dx MWH+/GHI case Dvorak L, Dolan M, Fink J, Varghese L, Henriksen J, Gulbahce HE. Correlation Between HER2 Determined by Fluorescence In Situ Hybridization and Reverse Transcription-Polymerase Chain Reaction of the Oncotype DX Test. Appl Immunohistochem Mol Morphol Aug 20. Christgen M, Harbeck N, Gluz O, Nitz U, and Kreipe H. Recognition and handling of discordant negative human epidermal growth factor receptor 2 classification by Oncotype DX in patients with breast cancer.j Clin Oncol 2012 May 29 Epub ahead of print Dabbs DJ, Klein M, Mohsin S, Tubbs R, Shuai Y, Bhargava R. High false-negative rate of HER2 quantitative reverse transcription polymerase chain reaction of the Oncotype DX test: an independent quality assurance study.jco (32): Park MM et al Breast J : HKIAP Fall Scientific Meeting 2014 Page 33
34 21-Gene Assay Profile Limitations Laboratory developed test = no one knows the performance characteristics except Genomic Health. 37% of results are intermediate (Palmer et. al., European Journal of Cancer Supplements 2009) Improper validation x2-not predictive for chemotherapy despite corporate claims. Her 2 gene flaw asco/cap her2 guidelines-no qrtpcr for Her2. >Soon, Dave Dabbs and I have had a multi year running argument about the utility of Oncotype Dx in Her2 positive, ER positive, node negative breast cancer, as you can see below. > Can you shed any light on this issue? Thanks in advance for your time and thoughts. Breast Cancer Res :R46 Soon Paik: All HER2 positive cases were mostly high RS or at least intermediate RS. Therefore I simply do not recommend performing OncotypeDx on HER2 positive tumors. the issue of OncotypeDx being inaccurate about HER2 status - yes it is - since HER2 mrna levels of HER2 positive and negative tumors overlap. Therefore you will have false negative cases if you rely on HER2 mrna levels only (even if you use GRB7 or other genes around HER2, same situation). The only time HER2 mrna levels reported as part of OncotypeDx can be useful is to rule out false negative cases. I guess if the Genomic Health has been marketing otherwise, then they should not do that. Hope this makes sense. Sincerely, Soon Paik HKIAP Fall Scientific Meeting 2014 Page 34
35 Summary FDA clearance is the FIRST STEP to patient safety for these high risk, high impact IVDMIAs (Transparency). EWG-clinical utility, levels of evidence, harms? Thank You. HKIAP Fall Scientific Meeting 2014 Page 35
36 Assessment of Ki67 in Breast Cancer: Recommendations from the International Ki67 and Breast Cancer Working Group. Dowsett M, et al. JNCI September,2011 Proliferation in Breast Cancers Where Are We? Prognosis-intermediate grade tumors David J Dabbs, M.D. Professor and Chief of Pathology Magee-Women s Hospital of UPMC Pittsburgh, PA, USA Assessment of Ki67 in Breast Cancer: Recommendations from the International Ki67 and Breast Cancer Working Group. Dowsett M, et al. JNCI September,2011 Assessment of Ki67 in Breast Cancer: Recommendations from the International Ki67 and Breast Cancer Working Group. Dowsett M, et al. JNCI September,2011 Prognosis-intermediate grade tumors Prediction of responsiveness or resistance to chemotherapy or endocrine therapy Prognosis-intermediate grade tumors Prediction of responsiveness or resistance to chemotherapy or endocrine therapy Estimation of risk in patients on therapy HKIAP Fall Scientific Meeting 2014 Page 36

37 Assessment of Ki67 in Breast Cancer: Recommendations from the International Ki67 and Breast Cancer Working Group. Dowsett M, et al. JNCI September,2011 Established methods of determining proliferation in tissues Prognosis-intermediate grade tumors Prediction of responsiveness or resistance to chemotherapy or endocrine therapy Estimation of risk in patients on therapy Biomarker of treatment efficacy during NAC Mitotic figure counts Thymidine Labeling (Silvestrini et al, 1974) Flow cytometry (Haag, et al 1984) Ki67 antibody (Gerdes, et al 1984) TLI/Ki67 DUAL STAIN..a word about mitotic counts Cell Cycle G0 - resting phase HKIAP Fall Scientific Meeting 2014 Page 37
38 Cell Cycle G0 - resting phase G1 - first gap phase, variable duration, cell prepares for DNA synthesis Cell Cycle G0 - resting phase G1 - first gap phase, variable duration, cell prepares for DNA synthesis S-Phase - DNA synthesis and doubling of the genome take place Cell Cycle G0 - resting phase G1 - first gap phase, variable duration, cell prepares for DNA synthesis S-Phase - DNA synthesis and doubling of the genome take place G2 second gap phase, cell prepares for separation of chromatids Cell Cycle G0 - resting phase G1 - first gap phase, variable duration, cell prepares for DNA synthesis S-Phase - DNA synthesis and doubling of the genome take place G2 second gap phase, cell prepares for separation of chromatids M Phase Mitotic phase after which daughter cell may enter G0 or move into G1 phase HKIAP Fall Scientific Meeting 2014 Page 38
39 Cell Cycle G0 - resting phase G1 - first gap phase, variable duration, cell prepares for DNA synthesis S-Phase - DNA synthesis and doubling of the genome take place G2 second gap phase, cell prepares for separation of chromatids M Phase Mitotic phase after which daughter cell may enter G0 or move into G1 phase Interphase comprised of G1, S and G2, cannot be morphologically recognized PCNA 36 kd nuclear protein associated with DNA - Recognizes a fixed and resistant epitope Little correlation with tumor grade Half life of PCNA is 20 hours and thus may be immunologically detectable in cells that have left the cell cycle. History-Ki67 Pioneers in breast cancer Gerdes J, et al.growth Factors in Malignant Non Hodgkin's Lymphoma Determined in Situ with the Monoclonal Antibody Ki67. Hematology Oncol. 1984: 2:365 Barnard MJ, et al Proliferative Index Carcinoma Determined In Situ by Ki67 Immunostaining and its Relationship to Clinical and Pathological Variables.. J. Pathol; 152:287. Lelle RJ, et al.. The Correlation Of Proliferation With Histological Grading and in Human Mammary Carcinomas. Cancer 59; 1987:83. Ki67 Identified by Gerdes (1983). Mouse monoclonal antibody against nuclear antigen from a Hodgkin s Lymphoma cell line. Nuclear non histone protein named after researcher s location. Ki= University of Kiel, Germany. 67 refers to the number of the clone on the 96 world plate. MIB1 for FFPE, (McCormick et al Histopathology Apr;22(4): ). HKIAP Fall Scientific Meeting 2014 Page 39
40 Proliferative Index in Breast Carcinoma Determined In-Situ by Ki67 Immunostaining and its Relationship to Clinical and Pathological Variables. Barnard NJ, et al. J. Pathology 152: Thymidine Labeling, Flow Cytometry for Breast Cancer Proliferation Rates Ki67: G1, S, G2, M phases 60 unselected cases of breast cases Strong positive correlation between Ki67 and mitotic index. No relation to tumor size, nodal status, estrogen receptor level, menopausal status Ki67 Immunostaining in Primary Breast Cancer: Pathological and Clinical Associations. Bouzubar N, et al. Br. J. Cancer (1989) 50:943 Ki67 performed on 136 primary breast cancers and related to various pathologic features Most often seen in poorly differentiated tumors with high rates of mitotic activity Independent of tumor size, lymph node status and ER expression High Ki67 often associated with early recurrence Ki67 Binding vs. Pathological Features 31% of all differentiated tumors had Ki67 >5% Highly significant association observed between increasing numbers of Ki67 positive cells and increasing histological grade Early recurrence of breast cancer, specifically when Ki67 Immunostaining was >20% Ki67 vs. S Phase Fraction Walker and Camplejohn: comparison of monoclonal antibody Ki67 reactivity with grade and DNA flow cytometry of breast carcinomas. BR J Cancer 1988; 57:281. Viela P, Chevillard S, Mosseri V, et al. Ki67 index and S phase fraction in human breast carcinomas comparison and correlation with prognostic factors. Am J Clin Pathol 1990; 94:681. HKIAP Fall Scientific Meeting 2014 Page 40
41 Effect of Tamoxifen on Ki67 Labeling Index in Human Breast Tumors and its Relationship to Estrogen and Progesterone Receptors Status. Clarke RB, et al. Br J Cancer 1993; 67:606. Ki67 index compared in breast cancer patients randomized to receive either tamoxifen or placebo Ki67 Li before Rx 5.6%, 3.0% after Rx (no significant differences in percent of ER and PR positive staining cells). Placebo group Ki67 Li 5.4% before Rx, 5.75% after Rx. Ki67 Li increased with increasing tumor grade and in tumors that were ER negative compared to ER positive. Quantitative Growth Fraction Evaluation with MIB1 and Ki67 Antibodies in Breast Carcinomas. Barbareschi M, et al. Am J Clin Pathol; 1994;102:171. Sentinel paper describing MIB1, the paraffin antibody recognizing a different epitope compared to Ki67 antibodies (on frozen tissue). Excellent correlation between labeling indices of Ki67 and MIB1. MIB1 Li nearly twice the values of Ki67 Li. Defined values for high and low proliferation activities adjusted. Proliferation and Apoptosis as Markers of Benefit in Neoadjuvant Endocrine Therapy of Breast Cancer. Dowsett M, et al. Clin Cancer Research 2006; 12:1024S Neoadjuvant setting randomized trial, Anastrazole, Anastrazole + Tamoxifen, or Tamoxifen alone. Ki67 measured before and 2 and 12 weeks after treatment. Significant Ki67 decrease at 2 weeks, weakly related to percent tumor shrinkage. Proliferation and Steroid Receptors in Clinical/Pathological Response in Breast Cancer Treated with Letrozol. Miller WR, et al. British Journal of Cancer, 2006; 94:1051 Significant decrease of Ki67 scores two weeks post treatment. Treatment significantly reduced PR expression and Ki67 score, but changes not correlated closely with clinical and pathological responses. HKIAP Fall Scientific Meeting 2014 Page 41
42 Proliferation Measurement in Breast Cancer by Two Different Methods. Martinez-Arribas F, et al. Anticancer Research 2006; 26:199 Comparing S-Phase fraction by flow cytometry and Ki67 index. An expression of Ki67 in 20% or more of tumor cell nuclei correlated highly with histological Grade 3, nuclear Grade 3 and lower absence of ER and PR. Ki67 and Cyclin A as Prognostic Factors in Early Breast Cancer. What are the Optimal Cut Off Values? Ahlin C, et al. Histopathology 2007; 51: invasive carcinomas studied using TMAs. For Ki67, using average scores and maximal scores at the 7 th decile for disease free survival and overall survival. Ki67 values of 15% and 22% respectively. Prognostic Value of Ki67 Expression after Short Term Pre- Surgical Endocrine Therapy for Primary Breast Cancer. Dowsett M, et al. J NCI 2007; 99:167 IMPACT Trial (Immediate Preoperative Anastrozole Tamoxifen or Combined with Tamoxifen) Follow-up demonstrated higher Ki67 expression above baseline after 2 weeks of endocrine therapy was significantly associated with lower RFS. Larger baseline tumor size and lower estrogen receptor level after 2 weeks of treatment was also significantly associated with poor RFS. Lower Ki67 index 2 weeks after endocrine treatment is predictive for a prolonged RFS (prognostic). Ki67 Index, HER2 Status and Prognosis of Patients with Luminal B Breast Cancer. Cheang M, et al. JNCI 2009; 101: 736 Ki67 cut off used to identify luminal A ER positive tumors compared to higher proliferation luminal B ER positive tumors, defined by PAM50. Training set 357 FFPE invasive breast cancers. Validation set 4,046 FFPE invasive breast cancers. Follow-up median time 12.5 years. HKIAP Fall Scientific Meeting 2014 Page 42
43 Definitions of Luminal Types Luminal A: Ki67 low (less than 14%) ER and/or PR positive, Her2 negative Luminal B: Ki 67 greater than 14% Assessment of Ki67 Has Been a Matter of Controversy Ki67@ 10% (at Keshgegian, A. Am J Clin Path 1995; 104:42/Bevilacqua P, et al. Breast Cancer Research Treatment 1996; 37:123) Others use 20% of the cut points (Clahsen PC, et al. European J Surgical Oncology, 1999; 25:356/ Joenseu H, et al. Clin Cancer Research 2003; 9:923.) Strategies for Subtypes Dealing with the Diversity of Breast Cancer: The International Expert Consensus on the Primary Therapy of Early Breast Cancer Annals of Oncology 2011; 22:1736 Immunohistochemical surrogate markers of gene expression profiling viewed similar and adequate to define breast cancers at class types as performed by Cheang et al. Ki67 labeling index is chiefly important in the distinction between luminal A and luminal B subtypes. If reliable Ki67 is not available -histological grade may be used in making the luminal type distinction. Prognostic Impact of Ki67 Overexpression in Subgroups Categorized According to St. Gallen with Early Stage Breast Cancer. Matsubara N, et al. Oncology 2011; 81:345 Using Ki67 cut off of 10%, Ki67 was prognostic only for the intermediate risk group of breast cancer patients. Ki67 was not prognostic for the low or high risk group of patients. The intermediate risk of St. Gallen was used in the year HKIAP Fall Scientific Meeting 2014 Page 43
44 Ki67 as an end of Neoadjuvant Treatment Endpoint IMPACT Study P024 Study Neoadjuvant letrozole vs. tamoxifen Impact Study had a significant degree of Ki67 suppression. Preoperative endocrine prognostic index (PEPI) = predictive of long term outcome PEPI identifies patients with very low risk of recurrence on endocrine therapy alone(lsellis, et al) Ki-67 as prognostic marker in early breast cancer: a meta-analysis of published studies involving patients British Journal of Cancer (2007) 96, Ki-67/MIB-1 positivity is associated with higher probability of relapsein all patients (HR.1.93 (95% confidence interval (CI): ); P<0.001), in node-negative patients (HR.2.31 (95% CI: ); P<0.001) and in node-positive patients (HR.1.59 (95% CI: ); P<0.001). Furthermore, Ki-67/MIB-1 positivity is associated with worse survival in all patients. Cutoffs in studies (5-30%) Assessment of Ki67 in Breast Cancer: Recommendations from the International Ki67 and Breast Cancer Working Group. Dowsett M, et al. JNCI September,2011 Prognosis Prediction of responsiveness or resistance to chemotherapy or endocrine therapy Estimation of risk in patients on therapy Biomarker of treatment efficacy during NAC KI-67 (MIB-1) Issues Variation in analytical practice Cold ischemic time, core biopsy vs. surgical resection, fixative and fixation time, antibody clone, IHC method, cutoff interpretations, method of interpretation (eye vs imaging) Necessity for Ki67 (MIB1) to be processed and interpreted uniformly for meaningful comparisons among clinical trial studies HKIAP Fall Scientific Meeting 2014 Page 44


45 Analytical Validity The original Ki67 antibody applicable only on frozen tissue. MIB1 clone, mouse monoclonal antibody used with HIER in FFPE. SP6 newer rabbit monoclonal antibody. Scoring percent of cells stained divided by the total number of cells scored. HOT SPOT? INTERPRETATION ISSUES INTENSITY? Analytical Validity - Scoring Count at least 3 randomly selected high power field (x40 objective). Two types of heterogeneity: gradient from center to periphery and hotspots. Tumor edge- 3 fields should be scored at the periphery. Hotspots counting is controversial recommended to assess the whole section. Analytical Validity -Scoring Between 500 and 2000 tumor cells have been scored in published studies. 500 cells being the absolute minimum, 1000 cells recommended No published data on Ki67 in TMAs. Most data in the literature are derived from visual scoring of Ki67. HKIAP Fall Scientific Meeting 2014 Page 45
46 Analytical Validity Cut Points Without standardization of methodology, published cut offs have had limited value outside of the studies from which they were derived. Most studies published between 10 and 20% as cutoffs. Greater than 10%, and 14% as cut off are most common. Currently no consensus on the threshold index for determination of prognosis or analytical validity context. Determination of prognosis. Eligibility for NAC HISTOPATHOLOGY Histopathology 2014, 65, DOI: /his.12392hi Immunohistochemical assessment of Ki67 with antibodies SP6 and MIB1 in primary breast cancer: a comparison of prognostic value and reproducibility Maria Ekholm,1,2 Sanda Beglerbegovic,3 Dorthe Grabau,2,4 Kristina L ovgren,2 Per Malmstr om,2,5 Linda Hartman2,6 & Marten Fern o2 1Department of Oncology, Ryhov County Hospital, J onk oping, Sweden, 2Division of Oncology and Pathology, Department of Clinical Sciences Lund, Lund University, Lund, Sweden, 3Division of Pathology, V axj o Central Hospital, V axj o, Sweden, 4Department of Pathology, Skane University Hospital, Lund, Sweden, 5Skane Department of Oncology, Skane University Hospital, Lund, Sweden, and 6Swedish Regional Cancer Centre South, Lund, Sweden Conclusions: SP6 was not superior to MIB1, but the two antibodies were comparable in the assessment of Ki67. Both MIB1 and SP6 could therefore be considered for prognostic use in primary breast cancer. Comparison of the effect of different techniques for measurement of Ki67 proliferation on reproducibility and prognosis prediction accuracy in breast cancer Histopathology 2012, 61, DOI: /j x Conclusion: In node-negative breast cancer without adjuvant systemic treatment, Ki67% by DIA, but not subjective counts, is reproducible and prognostically strong. This casts serious doubt on therapeutic guidelines using subjective counts of Ki67. Preanalytical - Summary Core biopsies and whole sections are acceptable specimens. TMAs are acceptable for clinical trial evaluation. 10% neutral buffered formalin fixation as for steroid receptors. Fresh preparation of tissue sections for IHC staining. HKIAP Fall Scientific Meeting 2014 Page 46
47 Analytical - Summary Known positive and negative controls. Follow recommended antigen retrieval protocols especially if IVD antibody. MIB1 antibody currently endorsed for Ki67. Interpretation and Scoring - Summary Full sections, 3 high power (x40) fields. Invasive edge of tumor should be scored. If hotspots present should be included in overall score of entire tissue. Only nuclear staining is positive. Counting at least 500 tumor cells. Image analysis. Data Handling - Summary Ki67 index expresses percent of positive staining in all total number of tumor cells. Treatment efficacy studies should reflect the percentage suppression of the Ki67 index. Appropriate endpoint for assessing residual risk of recurrence is the Ki67 index. Evidence that MIB1 LI WORKS IN PRACTICE (IHC4) Prognostic value of a combined estrogen receptor, progesterone receptor, Ki67 and human epidermal growth factor receptor 2 Immunohistochemical score in comparison with the Genomic Health recurrence score in early breast cancer. Cuzick J, et al. JCO, 2011, 29:427. Using tissue blocks from the trans ATAC representing multiple sources TMA specimens MIB1 monoclonal antibody HKIAP Fall Scientific Meeting 2014 Page 47
 + Tumor size*0.78677 + KI67 index*0.13269. New Magee Equation 2 (nmse2): RS = 18.8042+ Nottingham score*2.34123 + ERIHC*(-0.03749) + PRIHC*(-0.")
 + (0 for HER2, 1.46495 for equivocal, 12.75525 for HER2 positive) + KI-67*0.18649. J Natl Cancer Inst;2013;105:1897 1906 Mei-Yin C. Polley, Samuel C. Y. Leung, Lisa M.")
48 Magee Study Equations (Mod Pathol. 2008;21: ) New Magee Study Equation 1 (nmse1): RS = Nottingham score* ERIHC*( ) + PRIHC*( ) + (0 for HER2 negative, for equivocal, for HER2 positive) + Tumor size* KI67 index* New Magee Equation 2 (nmse2): RS = Nottingham score* ERIHC*( ) + PRIHC*( ) + (0 for HER2 negative, for equivocal, for HER2 positive) + Tumor size* New Magee Equation 3 (nmse3): RS = ERIHC*( ) + PRIHC*( ) + (0 for HER2, for equivocal, for HER2 positive) + KI-67* J Natl Cancer Inst;2013;105: Mei-Yin C. Polley, Samuel C. Y. Leung, Lisa M. McShane, Dongxia Gao, Judith C. Hugh, Mauro G. Mastropasqua, Giuseppe Viale,Lila A. Zabaglo, Frédérique Penault-Llorca, John M.S. Bartlett, Allen M. Gown, W. Fraser Symmans, Tammy Piper, Erika Mehl,Rebecca A. Enos, Daniel F. Hayes, Mitch Dowsett, Torsten O. Nielsen, on behalf of the International Ki67 in Breast CancerWorking Group of the Breast International Group and North American Breast Cancer Group Conclusions: Substantial variability in Ki67 scoring was observed among some of the world s most experienced laboratories.ki67 values and cutoffs for clinical decision-making cannot be transferred between laboratories without standardizing scoring methodology because analytical validity is limited. 77% of labs achieved sufficient grade MIB-1(77), MM1(83), SP6(60), 30-9(100) NORDIQC nordiqc.org Take Home Message Pre-Analytical: OK Analytical sample, clone, platform, counting,?imaging, reporting. Post-Analytical-QA scheme; clinical outcomes. HKIAP Fall Scientific Meeting 2014 Page 48
49 Back to the Future? Phosphohistone H3 expression has much stronger prognostic value than classical prognosticators in invasive lymph node-negative breast cancer patients less than 55 years of age Ivar Skaland1,3, Emiel AM Janssen1,3, Einar Gudlaugsson1,3, Jan Klos1, Kjell H Kjellevold1, Ha vard Søiland2,3 and Jan PA Baak1,3,4 Modern Pathology (2007) 20, PPH3 correlated(p<0.05) with tumor diameter, estrogen receptor, carcinoma grade, and mitotic activity index. PPH3 values were systematically (80%) higher than the mitotic activity index. Receiver-operating curve analysis objectively showed that PPH3 <13 (n=53; 45% of all cases) vs phosphohistone H3>13 (n=-66; 55% of all cases) was the strongest prognostic threshold, with 20-year recurrence-free survival of distant metastases of 96 and 58%, respectively (P<.0002, HR.9.6) (HR of MAI was 3.9). highly reproducible between observers (R=0.92) and highly consistent with digital image analysis (R=0.96). END HKIAP Fall Scientific Meeting 2014 Page 49

50 Breast Cancer, Gastric Cancer, & HER2: Significant % of patient Demonstrate HER2 alteration Associated with worse prognosis in breast cancer Predicts benefit from targeted therapy for both tumor types HER2 TESTING BREAST & GASTRIC CARCINOMAS DAVID J DABBS MD UNIVERSITY OF PITTSBURGH MAGEE WOMEN S ddabbs@upmc.edu Approximate number of newly diagnosed cases in the US (2010) Rate of HER2-positivity HER2+ disease (determined by IHC and/or FISH testing) Breast Cancer Gastric Cancer 209, ,000 1,* ~ 15-20% (general breast cancer population) Clinical Significance Predictive of response to anti-her2 therapy 2 Associated with poor prognosis 3 ~22%(rates observed in ToGA trial) Clinical Significance Predictive of response to anti-her2 therapy 2,6 ToGA= Trastuzumab for Gastric Cancer *Includes GE Junction. 1. American Cancer Society. Cancer Facts and Figures Atlanta, GA; 2. Herceptin [prescribing information]. South San Francisco, CA: Genetech, Inc. October 29,2010; 3. Ross JS et al. Oncologist. 2009;14: ;4. Slamon DJ et al. Science. 1989;244:;;;;;;;;; ; 5. Slamon DJ et al. Science. 1987;235: ; 6. Bang YJ et al. Lancet. 2010;376(9742): HKIAP Fall Scientific Meeting 2014 Page 50



51 HER2 Status Evaluation and Testing HKIAP Fall Scientific Meeting 2014 Page 51


52 Rationale for HER2 Testing in Every New Breast Cancer Patient at Diagnosis or Recurrence Testing helps identify patients who will be appropriate for HER2-targeted therapy and the most likely to respond HER2 testing has significant implications f or therapeutic decisions Quality assurance & accuracy, high priority to insure optimal patient selection and outcome Ensuring Accurate HER Testing Technical (Pre-analytic, Analytic and Post-analytic), Clinical and Pathologic Considerations Wolff et al. J Clin Oncol. 2007;15:118; Konecny et al. J Natl Cancer Inst. 2003:95:142; Menard et al. J Clin Oncol. 2001;19:329;Konecny et al. J Natl Cancer Inst. 2004;96:1141; Hayes et al. J Clin Oncol.1999;17:2639; Vogel et al. J Clin Oncol. 2002;20:719 HKIAP Fall Scientific Meeting 2014 Page 52

53 HKIAP Fall Scientific Meeting 2014 Page 53

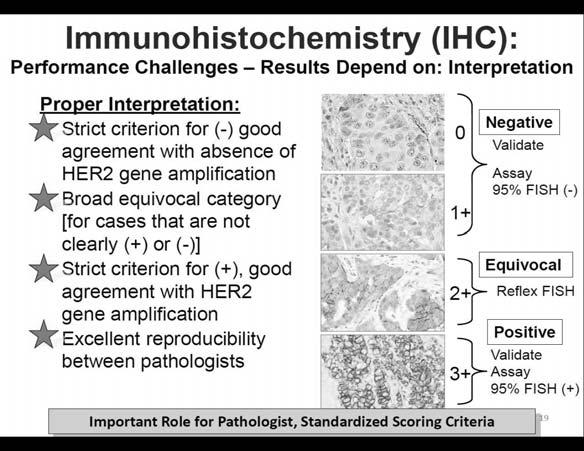
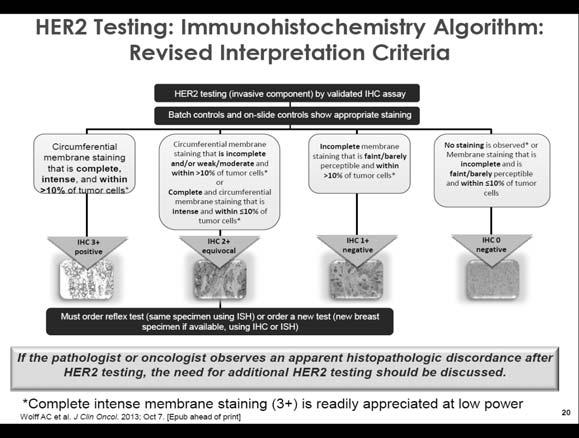
54 EASY Analyzing Slides for HER2 IHC (if all control slides show appropriate staining) Obviously 0 Obviously 3+ Somewhere between 0 and 1+ Challenging Somewhere between 1+ and 2+ Somewhere between 2+ and 3+ Distinction between 1+ and 2+, may make the difference between a patients receiving treatment or not If not entirely clear, consider sending case for HER2 FISH! Correlation of HER2 status with the clinical profile Univariant Correlates HER2 Amplification in Breast Cancer [The Breast (2006) 15:728-35] Variable OR 95%/Cl p=-value Race White/Black Age (years) 10-year increase ER status Negative/positive Nodal Status N1-3/N0 LVI Yes/No SBR Grade II/I III/I <0.001** <0.001* * <0.001* <0.001** <0.001** *P<0.05 is significant [Model based on 1000 patient (HER2 FISH), 192 HER2 gene amplified] **High SBR grade and younger patient age remained highly significant in multivariant analysis Unusual HER2 Genotypes HER2 Biology & HER2 Evaluation In most cases, HER2 protein over-expression results from gene amplification (not all cases) Most discordant gene/protein results are due to technical problems Appropriate trouble shooting, pre-analytic variables, controls, etc. Some uncommon HER2 Genotypes in breast cancer can lead to discordant gene/protein results HER2 genomic heterogeneity Chromosome 17 aneusomy (polysomy & monosomy) HKIAP Fall Scientific Meeting 2014 Page 54


55 HKIAP Fall Scientific Meeting 2014 Page 55


 appear to benefit from treatment with HER2-targeted therapy.")
56 Heterogeneity Intratumoral heterogeneity for HER2 can be seen in breast cancer by IHC With heterogeneity, the fields selected for evaluation will determine whether or not the tumor is reported as ISH amplified. Mean score/ratio depends on the number of amplified cells counted and gene copy # after dilution with non-amplified cells. Can lead to discordant results for HER2 analysis Between IHC and ISH, cores vs excision, between blocks Easier to detect with IHC (can be used to target ISH analysis) Clinical significance of heterogeneity remains unclear however: Patients with HER2 IHC 3+ (10-30%) and ISH ratio (2-2.2) appear to benefit from treatment with HER2-targeted therapy. It is important to carefully review all the pathologic features (grade, proliferative index, ER/PR & HER2 results) for such cases. Hanna, et al., Mod Pathol Jan;27(1):4-18 HKIAP Fall Scientific Meeting 2014 Page 56


57 HER2 Result IHC ISH 2013 HER2 Guideline Updates: Summary of Changes to staining Readily the appreciated Testing at Algorithms low magnification in BC Average HER2 copy Positive >10% of invasive breast tumor cells display HER2/CEP 17 of >2.0, or HER2/CEP17 of <2.0 and number >6 signals/cell Negative IHC 0: No staining observed or membrane staining that is incomplete, faint/barely perceptible and within <10% of the invasive beast tumor cells ICH 1+: Incomplete membrane staining that is faint/barely perceptible and within >10% of the invasive tumor Equivocal 2+ based on circumferential membrane staining, incomplete, weak, or moderate within >10% of the invasive breast tumor cells; or complete & circumferential membrane intense staining within <10% of the invasive breast tumor cells HER2/CEP17 ratio <2.0 and HER2copy number <4 signals/cell HER2/CEP17 ratio <2.0 and a HER2 copy number >4.0 and <6.0 signals/cell Indeterminate Technical issues prevent the assay from being conclusive (eg, issues with controls, specimen handling, artifacts, or analytical failure) Assay must be repeated before diagnosis can be rendered Wolff AC et al. J Clin Oncol. 2013; Oct 7. [Epub ahead of print] Key Points IHC & FISH are important laboratory methodologies for evaluating therapeutic targets in breast cancer These tests are complimentary Technical assay validation is critical Tissue must conform to pre-analytical requirements Continuous monitoring + QA/QC is essential HER2 status should be correlated with clinical profile of the patient HER2+ tumor are more common in younger patients, higher grade tumors, high proliferative index Discordant gene/protein results must be thoroughly investigated before reporting Technical problems with testing, pre-analytic variables, controls Unusual HER2 biology Genomic heterogeneity Aneusomy (polysomy, monosomy) Only one positive result (IHC or FISH) needed to be eligible enrollment in the adjuvant trials HKIAP Fall Scientific Meeting 2014 Page 57

58 ToGA Trastuzumab for Gastric Cancer ToGA Trastuzumab in Gastric Cancer Open label International (Asia, Central & South America, Europe) Phase 3 Randomized controlled trial Inoperable locally advanced, reccurrent or metastatic adenocarcinoma of the stomach or GEJ Compared trastuzumab + chemotherapy to chemotherapy alone Why ToGA? Success of trastuzumab in breast cancer Some upper GI malignancies over-express HER2 Gastric cancer is a tremendous burden worldwide Worldwide Over 900,000 new diagnoses annually 700,000 deaths Third leading cause of cancer mortality In the United States ~21,000 new diagnoses annually >10,000 deaths HKIAP Fall Scientific Meeting 2014 Page 58
59 Hofmann 168 samples 149 stomach 16 GEJ 4 esophagus HER2 IHC and FISH (Hercep Test and pharmdx, Dako) IHC Applied breast cancer scoring Intensity score: absent/faint/moderate/strong Complete vs incomplete membranous reactivity ISH HER2:CEP17>2 = amplified/positive HER2:CEP17,2= not amplified/negative Polysomy = average >3 CEP17 signals/cell Assessed concordance HKIAP Fall Scientific Meeting 2014 Page 59



60 Hofmann IHC3+ IHC2+ IHC1+ IHC 0 FISH FISH TOTAL HKIAP Fall Scientific Meeting 2014 Page 60


61 Hofmann Recommendations IHC Characteristic Score/classification <10% of cells stain 0/negative Faint staining in >10% of cells Weak-moderate basolateral or complete membranous staining in >10% of cells Moderate-strong basolateral or complete membranous staining in >10% of cells Cohesive cluster of cells with moderate to strong basolateral or complete membranous staining in a biopsy 1+/negative 2+/equivocal 3+/positive 3+/positive Ruschoff Validation 547 samples for interobserver variability Identified situations predisposing to disagreement Recommendations to improve concordance Use microscopic magnification to determine intensity of staining Strong staining evident at low power (2.5x, 4x, 5x) Weak-moderate evident at intermediate power (10x, 20x) Faint staining requires high power (40x) Defined cluster as minimum 5 cells ISH should be IHC directed or light-microscopic based Consider FISH for cases with some staining but <10% Lateral and basolateral staining Recommended proficiency testing HKIAP Fall Scientific Meeting 2014 Page 61
 Usually dual probe Ratio of HER2 to CEP17 Positive/amplified if HER2/CEP17 >2 Negative/not amplified if HER2/CEP17 <2 Exploratory Analyses by HER2 Status Using Updated Overall Survival Results `")
62 HER2 ISH Testing Breast (Guideline update 2013 ) Dual probe (ratio HER2/CEP17) Amplified if ratio >2 or if HER2 # >6 Single probe (average HER2 copy) Amplified if HER2 # >6 Gastric (no guidelines yet) Usually dual probe Ratio of HER2 to CEP17 Positive/amplified if HER2/CEP17 >2 Negative/not amplified if HER2/CEP17 <2 Exploratory Analyses by HER2 Status Using Updated Overall Survival Results ` Herceptin+ Chemotherapy Chemotherapy* alone* (n=298) ᵻ (n=296) ŧ FISH+/IHC 0,1+ subgroup (n=133) No. deaths/n (%) 56/62 (90%) 57/71 (80%) Median OS duration, months % CI, months Hazard ratio (95% CI) 1.33 ( ) FISH+/IHC 2+ subgroup (n=160) No. deaths/n (%) 64/80 (80%) 65/80 (81%) Median OS duration, months % CI, months Hazard ratio (95% CI) 0.78 ( ) FISH+/IHC 3+ subgroup (n=294) No. deaths/n (%) 96/151 (64%) 104/143 (73%) Median OS duration, months % CI, months Hazard ratio (95% CI) 0.66 ( ) HKIAP Fall Scientific Meeting 2014 Page 62

63 Caution The study also demonstrated that gene amplification and protein expression (IHC) are not as correlated as with breast cancer, therefore a single method should not be used to determine HER2 status Until we understand the significance of IHC- FISH+ results all gastric cases should be dual tested Key Points Gastric cancer has different biology than breast cancer Gastric cancer cases with basolateral HER2 staining are amplified with ISH IHC scoring criteria modified so that basolateral staining is positive (not just complete) Adenocarcinomas located at the GE junction and those showing intestinal differentiation are more likely to over-express HER2 Key Points Gastric cancer is more heterogeneous than breast cancer Focal HER2 over-expression can be missed on limited endoscopic biopsy Failure to target areas for FISH analysis with the IHC stained slides can lead to discordant results Target FISH enables finding clusters of tumor cells that are amplified In gastric cancer, clusters of five cells is sufficient to call positive on biopsy HKIAP Fall Scientific Meeting 2014 Page 63
64 Key Points Heterogeneity- No current recommendation on how may blocks should be examined ISH should be directed to areas showing HER2 protein over-expression Ruschoff says if <10% of cells are positive, consider ISH Summary Approximately 20% of gastric cancers overexpress HER2 The ToGA trial demonstrated a benefit in patients with advanced gastric cancer treated with trastuzumab + chemotherapy vs chemotherapy alone IHC should be the initial methodology used in gastric cancer; equivocal cases should be assessed with ISH Consider using ISH on negative cases, especially if there are some cells positive ISH should be directed Gastric cancer has different biology than breast cancer, including more frequent heterogeneity, necessitating modifications to HER2 scoring criteria Gastric cancers with basolateral and lateral staining exhibit amplification and should be called positive by IHC A cluster of five positive cells in a biopsy is sufficient to call gastric cancer positive References American Cancer Society. Cancer Facts & Figures Atlanta, GA Herceptin[prescribing, information]. South San Francisco, CA: Genentech, Inc; October 29, 2010 Ross JS et al. Oncologist. 2009;14: Slamon DJ et al. Science. 1989;244: Bang YJ et al. Lancet. 2010; 376(9742): Rowinsky EK. Annu Rev Med. 2004;55: Pegram M et al. Cancer Teat Res. 2000; 103:57 Wolff AC et al. J Clin Oncol. 2007;25(1): Wolff et al. J Clin Oncol. 2007;15:118 Konecny et al. J Natl Cancer Inst. 2003;95:142 Menard et al. J Clin Oncol. 2001; 19:329 Konecny et al J Natl Cancer Inst. 2004;96:1141 Hayes et al. J Clin Oncol. 2006;24:5S. Abstract 510 Slamon et al. N Engl J Med. 2001;344:783 Cobleigh et al. J Clin Oncol. 1999;17:2639 Vogel et al. J Clin Oncol. 2002;20:719 Vanden Bempt I et al. J Clin Oncol. 2008;26(30): Rosenberg CL. J Clin Oncol. 2008;26:1-3 Downs-Kelly E et al. Am J Surg Pathol. 2005;29: Tse et al., J Cl9n Oncol 2011, 29 Bang et al. The Lancet : Hicks, Whitney-Miller. Applied Immunohistochemistry & Molecular Morphology :506-8 Koltz, Hicks and Whitney-Miller. Biotechnic and histochemistry : 40-5 Ruschoff J et al. Virchow Arch. 2010; 457(3): Hofmann M et al. Histopathology. 2008;52: HKIAP Fall Scientific Meeting 2014 Page 64

65 Disclosure The Evolving Role of the Pathologist in Breast Cancer Genomic Profiling No financial interests to disclose. DAVID J DABBS, M.D PROFESSOR AND CHIEF OF PATHOLOGY MAGEE-WOMEN S HOSPITAL OF UPMC PITTSBURGH, PA Heterogeneity of Breast Cancer Gene Expression Profiling to Define Heterogeneity in Breast Cancer Clinicopathologic covariates and receptor status inform treatment decisions However, disease course and treatment outcomes in patients with similar baseline disease covariates vary considerably Advances in molecular understanding suggest underlying heterogeneity Researchers first describe groups of breast tumors with similar gene expression patterns Results revealed groups reflective of variation in growth rates, signaling activity, and cellular makeup Luminal epithelial/er gene cluster Erb-B2 cluster Basal-like 2 gene cluster Basal-like 1 gene cluster 3 Perou CM, et al. Nature. 2000;406(6797): HKIAP Fall Scientific Meeting 2014 Page 65



66 Refining Molecular Classification Expression Profiling Delineates Intrinsic Subtypes Further analysis of the gene expression profile refined the classification of subtypes and the accompanying differences in disease outcome Objective risk/prognostic characterization of breast tumors may guide treatment decisions 1,2 HER2-E Lum B Basal Normal Lum A Dendrogram Intrinsic Classification 1. Figure from Sorlie T, et al. Proc Nat Acad Sci (USA). 2003;100(14): Goldhirsch A, et al. Ann Oncol. 2013;24(9): Defining Heterogeneity in Breast Cancer Predictive Value of Intrinsic Subtypes Early Stage Breast Cancer: The Treatment ent Decision Clinical evidence suggests that intrinsic subtype is predictive of clinical outcomes 1,2 Probability P <.01 Luminal A Luminal B Basal ERBB2+ Treatment risk Adverse events Radiotherapy Endocrine Therapy Treatment benefit Disease free and survival benefit, QoL Chemotherapy Individualized need for disease control Axillary lymph node dissection Time to distant metastasis, months Molecular covariates may better inform which modalities should be incorporated into an individual s treatment plan to balance benefit with risk, as well as cost 1. Wirapati P, et al. Breast Cancer Res. 2008;10(4):R Figure from Sorlie T, et al. Proc Nat Acad Sci (USA). 2003;100(14): QoL, quality of life. 8 HKIAP Fall Scientific Meeting 2014 Page 66
 is a robust, prognostic, with good to excellent reproducibility. The scrutiny applied to histologic grading has only recently been applied to molecular tests.")
67 Tumor Size, Grade, Lymph Node Status, ER, PR, Her2 Tumor Boards-Good actor vs bad actor Breast cancer prognostic classification in the molecular era: the role of histological grade Histologic grade (NGS) is a robust, prognostic, with good to excellent reproducibility. The scrutiny applied to histologic grading has only recently been applied to molecular tests. 36% intermediate Histologic Grade; 40% of oncotype dx tests are Intermediate RS. Rare: Grade 1-Grade3. *Rakha EA, Reis-Filho JS, Baehner F, Dabbs DJ, Decker T, Eusebi V, Fox SB, Ichihara S, Jacquemier J, Lakhani SR, Palacios J, Richardson AL, Schnitt SJ, Schmitt FC, Tan PH, Tse GM, Badve S, Ellis IO. Breast Cancer Res. 2010;12(4):207. doi: /bcr2607. Epub 2010 Jul 30. Review. PMID: Improving Treatment Practice in HR+ Early Breast Cancer Current practice based on tumor size and nodal status has limited utility to identify patients at high risk of late recurrence Algorithms to further refine risk groups have been developed 1,2 Unmet need to further individualize risk assessment beyond current algorithms and improve clinical outcomes Accurate, validated, tumor biomarker tests to identify high-risk patient groups at baseline who may benefit from specific/extended treatment What your Pathologists Know Luminal A: ER +, very high (HS ) PR + Very High (HS ) Ki67: Low 3-14% Grade: 1, few percent grade 2. Luminal B: ER + intermediate-low (HS 1-200) PR: negative or low (HS <100) Grade 2 or 3 Ki67 >15%, often much higher 1. Lee AH, et al. Pathol Oncol Res. 2008;14(2): Cuzick AJ, et al. J Clin Oncol. 2011;29(32): HKIAP Fall Scientific Meeting 2014 Page 67
68 Significant Clinical Impact of Oncotype-MammaPrint Discordance Molecular Subtypes of Cases Discordant Between Risk Classification Assays in ER+ N0-N1 Patients: Shivers et al Miami Breast Conference March, 2014 Table 7: Association of Oncotype Dx and MammaPrint risk groups Oncotype Dx MammaPrint Low Intermediate High Low Risk (10%) Molecular Subtype (MP) LUM A Patients 63 25% Major Discordance Oncotype Dx 47 Low, 12 Int, 4 High High Risk (>10%) Chis-square test of independence: p<0.001 LUM B 51 35% Major discordance 18 Low, 17 Int, 16 High Table 8: Agreement of MammaPrint and collapsed Oncotype Dx risk groups Oncotype Dx MammaPrint RS [0,16] RS (16,100] Low Risk (10%) High Risk (>10%) Kappa estimate=0.26, 95% CI (0.34, 0.42) 14 Breast Cancer GEP Risk assessment profiles are not uniform. Platforms are not uniform. Information is often driven by marketing. Patient results show greater discordance for treatment purposes than the variation that is seen with pathologist grading of tumors. The need for FDA to regulate..july 31, Take Home Message..Why Magee is Offering Prosigna New generation Nanostring platform. Prosigna (PAM50) has superior prognostic information compared to Oncotype.* Intrinsic subtype adds more information to differentiate risk assessment, decreasing intermediate scores by 25%. Low Risk for node negative and positive. 10 year DR prognostic information is unique. A transparent, FDA cleared platform for patient safety. Value-added pathology. *Sestak I et al. Factors Predicting Late Recurrence for ER+ breast Cancer JNCI 2013; 105(19): *Dowsett M et al. Comparison of PAM50 ROR with Oncotype Dx and IHC4 for predicting risk of distant recurrence after endocrine therapy. J Clin Oncol 2013; 31(22): HKIAP Fall Scientific Meeting 2014 Page 68

69 Tumor Biomarker Tests The Burden of Proof 1 Analytical validation Robustness of hypothesis and algorithm Reproducibility of sampling and assay Clinical validation Prospective/retrospective study in the target population 2,a Clinical utility Significant association of biomarker-defined patient subset with treatment outcome Value in guiding treatment decision Economic utility The economic impact of consequent effects on treatment decisions is within accepted regional norms Measuring Nucleic Acids in Clinical Samples Current clinical practice Formaldehyde-fixed, paraffin-embedded (FFPE) samples pose challenges to accurate and reproducible estimation of biomolecules Challenges of expression-profiling FFPE samples FFPE processed samples provide low and variable yields of mrna Analytical need A robust and validated methodology is required to accurately estimate RNA copy number in tumor FFPE samples a Prospective analysis plan sufficient for Level 1 evidence. 1. Hayes DF, et al. Breast. 2013;22(suppl 2):S22-S Simon RM, et al. J Natl Cancer Inst 2009;101(12): Design Advantages of ncounter A Dual Probe Architecture Is the Heart of ncounter Technology Capture Probe Solution Hybridization Reporter Probe Direct detection (no amplification of target) Designed for short sequences (~100 nt) 6 Fluorescent spots are labeled RNA molecules complementary to ssdna backbone ~50 fluorophores/spot generate very bright signal allowing for digital detection 4 colors, no consecutive spots of same color = 972 possible codes Target Barcode-based count eliminates normalization of signal amplitude Capture Probe Reporter Probe Target-Probe Complex Remove Excess Probe Immobilize/Align Wide dynamic range (5 logs) Internal controls to ensure optimal processing Multiplexed B 3 Repeats Target-specific oligos Single-stranded DNA backbone 5 Repeats Digital Count Automated upstream processing Target mrna 6 Fluorescently labeled RNA segments Single molecule fluorescent barcodes, each attached to an individual nucleic acid Geiss GW, et al. Nat Biotechnol. 2008;26(3): HKIAP Fall Scientific Meeting 2014 Page 69
 in patient tumor tissue Ability to detect short chain RNA templates Linearity of measurement over a")
 score Characterizes and integrates intrinsic subtype, proliferation score, and tumor size Distinct thresholds for node-negative and node-positive patient")
 to 161 genes that passed FFPE")

70 ncounter Advantage for Quantitating Nucleic Acids in FFPE Samples Direct measurement minimizes error/bias from enzyme-based processes (reverse transcriptase and polymerase) ncounter-pam50 Gene Expression Profile Expression profile of 46-genes (and 8 house-keeping genes for normalization) in patient tumor tissue Ability to detect short chain RNA templates Linearity of measurement over a wide dynamic range ensures accurate quantitation of both rare and abundant transcripts Facilitated by solution phase hybridization Digital counting design Excess probes Algorithm provides a continuous risk of recurrence (ROR) score Characterizes and integrates intrinsic subtype, proliferation score, and tumor size Distinct thresholds for node-negative and node-positive patient populations Validated for use on the ncounter platform Allows for flexible range of sample input Origins of ncounter-pam50 Gene Signature Deriving the Gene Set and Prognostic Algorithm Determine optimal gene set Hierarchical clustering of 1,906 intrinsic genes defined by previous studies Optimized gene set (qrt-pcr data from 122 breast cancers) to 161 genes that passed FFPE performance criteria Cross-validation (random 10% left out in each of 50 cycles) by N t-test method selected 50 genes ncounter-pam50 Gene Signature gene set Defines Intrinsic Subtype and Proliferation Score Incorporates classification of intrinsic subtype, proliferation score Basal-like HER2-Enriched Luminal A Luminal B Proliferation Develop algorithm Compared reproducibility of classification across 3 centroid-based prediction methods Selected Prediction Analysis of Microarray (PAM) Trained with a multivariable Cox model Risk of recurrence (ROR) score developed for test case using correlation to subtype alone: ROR-S = 0.05*basal *HER2 0.34*LumA * LumB or using subtype correlation plus tumor size: ROR-C= 0.05*basal *HER2 0.23*LumA *LumB * T Parker JS, et al. J Clin Oncol. 2009;27(8): UBE2C PTTG1 MYBL2 CCNB1 BIRC5 HSPC150 TYMS MELK KNTC2 CEP55 CDC6 RRM2 ORC6L ANLN KIF2C EXO1 CENPF CDCA1 CDC20 MKI67 CCNE1 GRB7 TMEM45B ERBB2 BLVRA GPR160 FOXA1 MMP11 NAT1 CXXC5 ESR1 SLC39A6 PGR BAG1 ACTR3B MIA FOXC1 MYC KRT5 SFRP1 KRT17 KRT14 BCL2 PHGDH CDH3 EFGR FGFR4 MDM2 MLPH MAPT HKIAP Fall Scientific Meeting 2014 Page 70

71 ncounter-pam50 Gene Signature Assay Intrinsic Subtypes Have Distinct Clinical Outcomes ncounter-pam50 ROR-Score Discriminates Within Intrinsic Subtype Relapse-Free Survival (probability) Intrinsic subtypes assigned using PAM50 show clear differences in RFS in nodenegative patients who did not receive systemic adjuvant therapy Similar differences in RFS by subtype were seen in the subset of patients with ER + BC Patients who did not receive systemic adjuvant therapy Basal-like 0.2 HER2-enriched Luminal A Luminal B Log-rank P = 2.26e Time, years RFS, relapse-free survival. Parker JS, et al. J Clin Oncol. 2009;27(8): Relapse-Free Survival (probability) Subset of patients with ER + disease Basal-like HER2-enriched Luminal A Luminal B Log-rank P = 1.89e Time, years 25 Risk predictors based on the PAM50 gene set added significant prognostic and predictive value to intrinsic subtype ROR-C (tumor size and subtype model) scores categorize intrinsic subtypes ROR-C Basal-like Parker JS, et al. J Clin Oncol. 2009;27(8): HER2- enriched Luminal A Luminal B 26 ncounter-pam50 Gene Signature Is Robust Validated by TCGA (Independent Dataset, Different Platform) Semi-supervised. hierarchical cluster analysis showed consensus across breast cancer intrinsic subtypes defined in independent datasets using 5 different genomic/ proteomic platforms a These data are independent of ncounter technology a Heat map display of subtypes defined independently by micrornas, DNA methylation, copy number, PAM50 mrna expression, and RPPA expression. The Cancer Genome Atlas Network. Nature. 2012;490(7418): Transitioning qrt-pcr Based PAM50 to ncounter Platform (NanoString) Objective Replace qrt-pcr protocol with an automated, multiplexed assay (ncounter) to assign risk score Endpoints Assess concordance between outputs: Expression measurements of each gene Assignment of intrinsic subtype Proliferation and risk scores Approach Assess concordance with above endpoints Retrain algorithm using ncounter-based measurements 28 HKIAP Fall Scientific Meeting 2014 Page 71




72 New Training as Robust as Published Classifier in the Intended Use Population The recurrence-free curves of the intrinsic subtype cohorts defined by qrt-pcr (left) and ncounter (right) are highly concordant Hands-off Upstream Process Enables Decentralized Testing Minimal HANDS-ON Step 1 12 HOURS or OVERNIGHT Minimal HANDS-ON Step HOURS, AUTOMATED Minimal HANDS-ON Step HOURS, AUTOMATED 1.0 qrt-pcr Subtype 1 ncounter (NanoString) Subtype Probability of Event Her2 4/ LumA 10/54 LumB 22/ Log-rank P =.155 Normal 0/ Probability of Event Her2-enriched 3/13 Luminal A 3/ Log-rank P =.0336 Luminal B 30/ ncounter Prep Station ncounter Digital Analyzer Hybridize 2 Purify 3 Count Simple and fast workflow is well suited for qualified clinical laboratories 1. Nielsen et al. Clin Cancer Res. 2010;16(21): NanoString data on file Internal NanoString data 30 Three Elements of ncoounter-pam50 Gene Signature Breast Cancer Assay ncounter-pam50 Gene Signature Algorithm ROR Score for Individual Patients Hardware: ncounter Analysis System Consumable: Kits Software: Report ROR score integrates intrinsic subtype, proliferation index, and tumor size (in the context of nodal status) to provide an integer score proportional to the risk of recurrence Determine intrinsic subtype through Pearson s correlation to centroids Calculate ROR (Risk of Recurrence Score) Prep Station Digital Analyzer Includes: PAM50 gene-based CodeSet with 8 controls Other consumables required for assay Roche RNA isolation kit sold separately Patient expression profile PAM50 centroids ROR = ar LumA + br LumB + cr Her2e + dr Basal + ep + ft Pearson s correlation to centroids Proliferation score Gross tumor size Product sheet 31 Gnant M, et al. SABCS. 2012; poster P HKIAP Fall Scientific Meeting 2014 Page 72

73 ncounter-pam50 ROR Score Is a Continuous Risk Function ncounter-pam50 Gene Signature Score Categorizes Risk Groups by Nodal Status The probability of distant recurrence within 10 years increases as a function of ROR and nodal status based on data in the tested patient population Nodal Status ROR Range Risk Categorization 0-40 Low Node-negative Intermediate Estimated 10-Year Risk of Distant Recurrence ROR: Node-negatives Node-positives (1-3 positive nodes) ROR Package Insert (US) Node-positive (1-3 nodes) High 0-40 Low High Risk classification groups are provided based on cutoffs related to clinical outcome in the tested patient populations: Low risk: 10-year probability of distant recurrence of < 10% High risk: 10-year probability of distant recurrence of > 20% ROR score discriminates risk groups within patients with node-negative disease 1. Package Insert (US) Gnant M, et al. Ann Oncol. 2014;25(2): ncounter-pam50 Gene Signature Score Categorizes Risk Groups by Nodal Status Analytic Reproducibility of ncounter-pam50 Gene Signature Assay Evaluated in Two Studies Nodal Status ROR Range Risk Categorization 0-40 Low Study 1: Reproducibility from tissue Node-negative Node-positive (1-3 nodes) Intermediate High 0-15 Low Intermediate High Extract RNA from FFPE tumor sample Study 2: Precision from RNA Run on the ncounter Dx Analysis System Risk classification groups are provided based on cutoffs related to clinical outcome in the tested patient populations: Low risk: 10-year probability of distant recurrence of < 10% High risk: 10-year probability of distant recurrence of > 20% ROR score discriminates risk groups within patients with node-negative disease 1. Package Insert (ex-us). Prosigna_Packet_Insert.pdf 2. Gnant M, et al. Ann Oncol. 2014;25(2): ncounter- PAM50 ROR Score 36 HKIAP Fall Scientific Meeting 2014 Page 73
74 L Reproducibility of ncounter-pam50 Gene Signature Assay Concordance in Risk Group Variation in Sample Input Has Minimal Effect on Assignment of Risk Group Reproducibility Study For each tissue sample, macrodissection, RNA extraction, and processing with the assay were performed by a single operator at each site per standard operating procedures 43 tissues across all sites represent a wide range (94 units) of ROR scores and all risk categories Nielsen T, et al. BMC Cancer. 2014;14(1):177. Site 1 Site 2 Site 3 Pathologist 1 Pathologist 2 Pathologist 3 Operator 1 Operator 2 RNA Isolation Kit 1 Duplicate Run with Reagent Lot 1 Samples 1-43 RNA Isolation Kit 1 Duplicate Run with Reagent Lot 1 Operator 3 RNA Isolation Kit 1 Duplicate Run with Reagent Lot 1 37 For intrinsic subtype classifications, the average concordance between sites was 97% ROR Score standard deviation = 2.9 (scale 0 to 100) 100 Basal-like 90 Her2-enriched 80 Luminal A Luminal B ROR Score (Tissue Average) Nielsen T, et al. BMC Cancer. 2014;14(1):177. ROR Score High Intermediate Low Risk category 38 Evaluating Variation in ncounter Gene Expression Estimate Low Variation in Gene Expression Estimate Minimal Effect on ROR Score RNA Precision Study Assessed reproducibility of device, reagents, and operator-specific components using a common template RNA Measured variability between and within assay variables including Testing site (n = 3) Sample type (n = 5) Operator (n = 6) Reagent lot (n = 3) Assay run (n = 18/site) Site 1 Site 2 Site 3 Operator 1 Operator 2 Reagent Lot 1 Reagent Lot 2 Reagent Lot 3 Run 1 Run 2 Run 3 Basal-like HER2-E Lum A Lum B1 Lum B2 X 2 The range of ROR scores for 108 independent measurements was 4 units for each of the 5 sample pools (scale 0 100) 1 ROR Score SD = % concordance was shown between measured and expected subtype result and risk group 1,2 ROR Score Adjusted ROR Score H e Nielsen T, et al. BMC Cancer. 2014;14(1): Nielsen T, et al. BMC Cancer. 2014;14(1): Nielsen TO, et al. Lab Invest. 2013;93(suppl 1):498A Subtype 40 HKIAP Fall Scientific Meeting 2014 Page 74
75 Summary ncounter-pam50 Gene Signature Assay Clinically Validated in Two Studies Representative of the Intended Use Population All aspects of sample processing and measurement were rigorously evaluated Includes site, pathologist, operator, instrument, and reagent lots TransATAC N = 1,007 Study patients (n=1017) Presented at San Antonio Breast Cancer Symposium in December 2011 Published in Journal of Clinical Oncology 1 ABCSG-8 Study (n=1478) Presented at San Antonio Breast Cancer Symposium in December 2012 Published in Annals of Oncology 2 Tested variables had minimal effect on ROR score ncounter-pam50 Gene Signature Assay performed on the ncounter platform is validated for decentralized testing Prospectively defined analysis of two registration-quality databases with 10-yr median follow-up in postmenopausal women with HR+ early stage breast cancer treated with endocrine therapy alone Primary Objective: Validate published observations that the ncounter-pam50 gene signature score provides additional prognostic information over and above standard clinical variables for DRFS at 10 years Primary Analysis: All patients Secondary Analysis: Node-negative, node-positive, and HER2-negative patients Secondary Objective: Validate observations that Luminal A and Luminal B patients have statistically significantly different DRFS at 10 years a 41 a Output of the U.S. version of the ncounter-pam50 gene signature assay FDA cleared for 510(k) does not report intrinsic subtype. 1. Dowsett M, et al. J Clin Oncol. 2013;31(22): Gnant M, et al. Ann Oncol. 2014;25(2): TransATAC: ncounter-pam50 Gene Signature Assay Adds Significant Prognostic Information Beyond CTS TransATAC: ROR Score Discriminates Recurrence Risk Within Nodal Subgroups The study met the predefined primary and secondary objectives of demonstrating significant association of ROR score with distant recurrence in this patient population The ncounter-pam50 Gene Signature Assay adds statistically significant prognostic information in addition to standard clinicopathologic variables ROR score is significantly related to outcome for all populations tested Analyses Population Patients, n P Value Primary All evaluable 1,007 <.0001 Secondary Node-negative 739 <.0001 Node-positive HER2-negative 888 <.0001 Node-Negative Patients Node-Positive Patients (1-3 nodes) Low (n=431) Low (n=6) 0.5 Medium (n=180) 0.5 Medium (n=74) High (n=128) High (n=134) Follow-up Time, years Follow-up Time, years at 10 years Risk Group N (%) Events a at 10 years Risk Group N (%) Events a % Without Recurrence % Without Recurrence Low 431 (58) 17 96% (94%-98%) Low 6 (3) 0 100% (N/A) Intermediate 180 (24) 22 86% (81%-92%) Intermediate 74 (35) 11 84% (76%-93%) High 128 (17) 38 67% (59%-76%) High 134 (63) 38 68% (59%-77%) a Number of events through 10 years. a Number of events through 10 years. 1. Dowsett, M. et al. J Clin Oncol. 2013;31(22): Package Insert (ex-us). Dowsett M, et al. J Clin Oncol. 2013;31(22): Percent Without Distant Recurrence Percent Without Distant Recurrence HKIAP Fall Scientific Meeting 2014 Page 75
76 Patients, % TransATAC: ROR Score Discriminates Recurrence Risk Within Intrinsic Subtypes Node-Negative Patients Luminal A, nodes 0 Luminal B, nodes Follow-up Time, years Node-negative, luminal B patients had a higher risk of RFS events (HR = 4.8 [ ]) Percent Without Distant Recurrence Node-Positive Patients 0.4 Luminal A 1-3 nodes (132) 0.2 Luminal A, 4+ nodes (31) Luminal B, 1-3 nodes (69) Luminal B, 4+ nodes (20) Follow-up Time, years Luminal B patients with 1 to 3 positive nodes had a higher risk of RFS events (HR = 2.0 [ ]) Similar results were seen in patients with 4+ positive nodes (HR = 3.4 [ ]) 1. Dowsett, M. et al. J Clin Oncol. 2013;31(22): Prosigna Package Insert (ex-us). 45 ABCSG-8 Study: Primary and Secondary Objectives Were Met The ncounter-pam50 Gene Signature Assay adds statistically significant prognostic information in addition to standard clinicopathologic variables ROR score is significantly related to outcome for all populations tested Analyses Population Patients, n P Value Primary All evaluable 1,478 <.0001 Secondary Node-negative 1,047 <.0001 Node-positive 431 <.0001 HER2-negative 1,397 <.0001 Gnant M, et al. Ann Oncol. 2014;25(2): ABCSG-8: ROR Score Discriminates Recurrence Risk Within Nodal Subgroups ncounter-pam50 Gene Signature Assay Versus RS: Fewer Intermediate Risk Node-Negative Patients 1.0 Node-Negative Patients 1.0 Node-Positive Patients (1-3 nodes) Risk groups prospectively defined based on predicted probability of 10-year distant recurrence (low < 10%, intermediate 10% to 20%, high > 20%) Clinical and pathologic variables excluded from analysis Percent Without Distant Recurrence Percent Without Distant Recurrence 0.7 Low-Risk 0.7 Low-Risk Intermediate-Risk Intermediate-Risk 0.6 High-Risk 0.6 High-Risk Follow-up Time, years Follow-up Time, years % Without % Without Risk Group Patients, n Events Recurrence at 10 yr Risk Group Patients, n Events Recurrence at 10 yr Low % (94.4%-97.9%) Low % (-) Intermediate % (86.3%-93.3%) Intermediate % (86.9%-97%) High % (78.4 %-88.6%) High % (69.9%-81.2%) 1. Package Insert (US) Gnant M, et al. Ann Oncol. 2014;25(2): Patients in Risk Group Low Intermediate High Follow-Up Time (Years) * Risk groups prospectively defined based on predicted probability of 10-yr distant recurrence (Low <10%, Intermediate 10-20%, High >20%) Dowsett M, et al. J Clin Oncol. 2013;31(22): Prosigna ROR Oncotype RS Percent Without Distance Recurrence ROR, low RS, low ROR, intermediate RS, intermediate ROR, high 60 RS, high 48 HKIAP Fall Scientific Meeting 2014 Page 76

77 Combined Analysis Clinical Validation in More Than 2,400 Patients Conclusions Across Clinical Studies 9,366 enrolled in ATAC 5,880 eligible for TransATAC 2,006 tissue specimen received 1,017 sufficient residual RNA 10 failed QC specs for device 1,007 evaluable RNA specimens 3,901 enrolled in ABCSG-8 3,714 eligible for ABCSG-8 1,620 re-consented or deceased 25 insufficient cancer in specimen 73 insufficient RNA isolated 44 failed QC specs for device 1,478 evaluable tissue specimens Support the clinical validity of ncounter-pam50 Gene Signature Assay ROR score for predicting the risk of late recurrence in postmenopausal women with HR + ESBC ROR score discriminates risk groups within subsets of patients defined by Nodal status (negative versus positive) and Luminal subtype (eg, luminal A and luminal B) ROR score provides clinically actionable information Identifies patients at sufficiently low risk of late-recurrence to be spared extended endocrine therapy Identifies node-positive patients at sufficiently low risk to be spared chemotherapy 2,485 evaluable specimens The results of the TransATAC and ABCSG8 studies provide Level 1 evidence for the clinical validity of the PAM50 test Gnant M, et al. ASCO 2013; Poster Evaluating Prognostic Value of ncounter-pam50 Gene Signature Assay ROR Score Versus Other Tests ROR/ROR* Add Prognostic Information Versus RS (Node-Negative Patients) Several prognostic tools are in use or development to inform treatment decisions in early breast cancer; however, robust characterization of their relative prognostic value is lacking The following analyses compared ROR versus other tests, including CTS, RS, and IHC4 Included 940 samples from TransATAC with the ncounter-pam50 Gene Signature Assay, 21 gene test, and IHC4 assessments or 688 node positive patients from ABCSG-8 Endpoint: Change in likelihood ratio (LR) statistic a RS scores do not significantly change LR after ROR is applied as the first test Order of addition to model Change in LR χ ROR RS ROR* a Likelihood ratios (LR) are used to determine whether a test result usefully changes the probability that a disease condition exists. Dowsett M, et al. SABCS. 2011; Poster S ROR* does not include tumor size Prognostic information from 2 nd test significant Dowsett M, et al. SABCS 2011; Poster S4-5. ROR RS RS ROR ROR* RS RS ROR* NO YES NO YES 52 HKIAP Fall Scientific Meeting 2014 Page 77

 The results of the TransATAC and ABCSG8 studies provide Level")

78 Additional Prognostic Information Beyond CTS in Node-Positive Subgroups N+ (N=331) 2N+ (N=145) 2-3N+ (N=212) LR 2 p-value LR 2 p-value LR 2 p-value ROR < IS ROR-RG < < < For IS, N = 320, 138 and 201 for N1, N2, and N2-3, respectively ROR IS ROR-RG CTS alone Conclusions The ncounter-pam50 Gene Signature Assay has successfully undergone rigorous analytic validation Highly reproducible and suited for decentralized testing The ncounter-pam50 Gene Signature Assay has been clinically validated in 2 large trials of adjuvant endocrine therapy (TransATAC and ABCSG-8) The results of the TransATAC and ABCSG8 studies provide Level 1 evidence for the clinical validity of the PAM50 test. ROR provides more prognostic information in endocrine treated patients than RS, with better differentiation of intermediate and high risk groups. ROR has strong prognostic information in years 5-10, which may help select patients who could benefit most from hormonal therapy beyond 5 years of treatment Additional exploration of the clinical utility of the ncounter-pam50 Gene Signature Assay to inform treatment decisions in the context of adjuvant chemotherapy and radiation therapy is ongoing IS, intrinsic subtype; ROR-RG, risk of recurrence-risk group. Gnant M, et al. ASCO. 2013; Poster Trends in Genome Medicine and Research From Research Discovery Result (2000) to Full Translational Validation (2011/2013) : The Ultimate Goal in Translational Research 2000 Microarray experiments define molecular classification of breast cancer PAM50 gene signature developed and validated 2009 ncounter selected by original PAM50 Medical Researchers as preferred Dx platform for this work 2011 First human study completed (~ 1000 FFPE samples) nd human study (~1500 FFPE samples) completed. Obtained CE Mark for Dx Release in Europe & Israel* 2013 NanoString Technologies received 510(k) clearance from the U.S. Food and Drug Administration (FDA) for its Prosigna Breast Cancer Prognostic Gene Signature Assay sa 55 N = 8102 genes on discovery array 496 intrinsic gene set Perou et al., Molecular Portraits of Human Breast Tumors, Nature, 2000, pp HKIAP Fall Scientific Meeting 2014 Page 78
Clinical Grade Genomic Profiling: The Time Has Come
 Clinical Grade Genomic Profiling: The Time Has Come Gary Palmer, MD, JD, MBA, MPH Senior Vice President, Medical Affairs Foundation Medicine, Inc. Oct. 22, 2013 1 Why We Are Here A Shared Vision At Foundation
Clinical Grade Genomic Profiling: The Time Has Come Gary Palmer, MD, JD, MBA, MPH Senior Vice President, Medical Affairs Foundation Medicine, Inc. Oct. 22, 2013 1 Why We Are Here A Shared Vision At Foundation
Genomic Medicine: What every pathologist needs to know
 Genomic Medicine: What every pathologist needs to know Stephen P. Ethier, Ph.D. Professor, Department of Pathology and Laboratory Medicine, MUSC Director, MUSC Center for Genomic Medicine Genomics and
Genomic Medicine: What every pathologist needs to know Stephen P. Ethier, Ph.D. Professor, Department of Pathology and Laboratory Medicine, MUSC Director, MUSC Center for Genomic Medicine Genomics and
Targeted Agent and Profiling Utilization Registry (TAPUR ) Study. February 2018
 Study. February 2018") Targeted Agent and Profiling Utilization Registry (TAPUR ) Study February 2018 Precision Medicine Therapies designed to target the molecular alteration that aids cancer development 30 TARGET gene alterations
Targeted Agent and Profiling Utilization Registry (TAPUR ) Study February 2018 Precision Medicine Therapies designed to target the molecular alteration that aids cancer development 30 TARGET gene alterations
Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making
 Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making November 20, 2014 Capturing Value in Next Generation Sequencing Symposium Douglas Johnson MD, MSCI Vanderbilt-Ingram
Next Generation Sequencing in Clinical Practice: Impact on Therapeutic Decision Making November 20, 2014 Capturing Value in Next Generation Sequencing Symposium Douglas Johnson MD, MSCI Vanderbilt-Ingram
SureSelect Cancer All-In-One Custom and Catalog NGS Assays
 SureSelect Cancer All-In-One Custom and Catalog NGS Assays Detect all cancer-relevant variants in a single SureSelect assay SNV Indel TL SNV Indel TL Single DNA input Single AIO assay Single data analysis
SureSelect Cancer All-In-One Custom and Catalog NGS Assays Detect all cancer-relevant variants in a single SureSelect assay SNV Indel TL SNV Indel TL Single DNA input Single AIO assay Single data analysis
Transform genomic data into real-life results
 CLINICAL SUMMARY Transform genomic data into real-life results Biomarker testing and targeted therapies can drive improved outcomes in clinical practice New FDA-Approved Broad Companion Diagnostic for
CLINICAL SUMMARY Transform genomic data into real-life results Biomarker testing and targeted therapies can drive improved outcomes in clinical practice New FDA-Approved Broad Companion Diagnostic for
Accel-Amplicon Panels
 Accel-Amplicon Panels Amplicon sequencing has emerged as a reliable, cost-effective method for ultra-deep targeted sequencing. This highly adaptable approach is especially applicable for in-depth interrogation
Accel-Amplicon Panels Amplicon sequencing has emerged as a reliable, cost-effective method for ultra-deep targeted sequencing. This highly adaptable approach is especially applicable for in-depth interrogation
IntelliGENSM. Integrated Oncology is making next generation sequencing faster and more accessible to the oncology community.
 IntelliGENSM Integrated Oncology is making next generation sequencing faster and more accessible to the oncology community. NGS TRANSFORMS GENOMIC TESTING Background Cancers may emerge as a result of somatically
IntelliGENSM Integrated Oncology is making next generation sequencing faster and more accessible to the oncology community. NGS TRANSFORMS GENOMIC TESTING Background Cancers may emerge as a result of somatically
Fluxion Biosciences and Swift Biosciences Somatic variant detection from liquid biopsy samples using targeted NGS
 APPLICATION NOTE Fluxion Biosciences and Swift Biosciences OVERVIEW This application note describes a robust method for detecting somatic mutations from liquid biopsy samples by combining circulating tumor
APPLICATION NOTE Fluxion Biosciences and Swift Biosciences OVERVIEW This application note describes a robust method for detecting somatic mutations from liquid biopsy samples by combining circulating tumor
Personalised cancer care Information for Medical Specialists. A new way to unlock treatment options for your patients
 Personalised cancer care Information for Medical Specialists A new way to unlock treatment options for your patients Contents Optimised for clinical benefit 4 Development history 4 Full FIND IT panel vs
Personalised cancer care Information for Medical Specialists A new way to unlock treatment options for your patients Contents Optimised for clinical benefit 4 Development history 4 Full FIND IT panel vs
The Center for PERSONALIZED DIAGNOSTICS
 The Center for PERSONALIZED DIAGNOSTICS Precision Diagnostics for Personalized Medicine A joint initiative between The Department of Pathology and Laboratory Medicine & The Abramson Cancer Center The (CPD)
The Center for PERSONALIZED DIAGNOSTICS Precision Diagnostics for Personalized Medicine A joint initiative between The Department of Pathology and Laboratory Medicine & The Abramson Cancer Center The (CPD)
5 th July 2016 ACGS Dr Michelle Wood Laboratory Genetics, Cardiff
 5 th July 2016 ACGS Dr Michelle Wood Laboratory Genetics, Cardiff National molecular screening of patients with lung cancer for a national trial of multiple novel agents. 2000 NSCLC patients/year (late
5 th July 2016 ACGS Dr Michelle Wood Laboratory Genetics, Cardiff National molecular screening of patients with lung cancer for a national trial of multiple novel agents. 2000 NSCLC patients/year (late
Dr David Guttery Senior PDRA Dept. of Cancer Studies and CRUK Leicester Centre University of Leicester
 Dr David Guttery Senior PDRA Dept. of Cancer Studies and CRUK Leicester Centre University of Leicester dsg6@le.ac.uk CFDNA/CTDNA Circulating-free AS A LIQUID DNA BIOPSY (cfdna) Tumour Biopsy Liquid Biopsy
Dr David Guttery Senior PDRA Dept. of Cancer Studies and CRUK Leicester Centre University of Leicester dsg6@le.ac.uk CFDNA/CTDNA Circulating-free AS A LIQUID DNA BIOPSY (cfdna) Tumour Biopsy Liquid Biopsy
Next generation histopathological diagnosis for precision medicine in solid cancers
 Next generation histopathological diagnosis for precision medicine in solid cancers from genomics to clinical application Aldo Scarpa ARC-NET Applied Research on Cancer Department of Pathology and Diagnostics
Next generation histopathological diagnosis for precision medicine in solid cancers from genomics to clinical application Aldo Scarpa ARC-NET Applied Research on Cancer Department of Pathology and Diagnostics
Comprehensive Genomic Profiling, in record time. Accurate. Clinically Proven. Fast.
 Comprehensive Genomic Profiling, in record time Accurate. ly Proven. Fast. PCDx advantages Comprehensive genomic profiling, in record time PCDx Comprehensive Genomic Profiling (CGP) provides precise information
Comprehensive Genomic Profiling, in record time Accurate. ly Proven. Fast. PCDx advantages Comprehensive genomic profiling, in record time PCDx Comprehensive Genomic Profiling (CGP) provides precise information
Characterisation of structural variation in breast. cancer genomes using paired-end sequencing on. the Illumina Genome Analyser
 Characterisation of structural variation in breast cancer genomes using paired-end sequencing on the Illumina Genome Analyser Phil Stephens Cancer Genome Project Why is it important to study cancer? Why
Characterisation of structural variation in breast cancer genomes using paired-end sequencing on the Illumina Genome Analyser Phil Stephens Cancer Genome Project Why is it important to study cancer? Why
Evolution of Pathology
 1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
EXAMPLE. - Potentially responsive to PI3K/mTOR and MEK combination therapy or mtor/mek and PKC combination therapy. ratio (%)
") Dr Kate Goodhealth Goodhealth Medical Clinic 123 Address Road SUBURBTOWN NSW 2000 Melanie Citizen Referring Doctor Your ref Address Dr John Medico 123 Main Street, SUBURBTOWN NSW 2000 Phone 02 9999 9999
Dr Kate Goodhealth Goodhealth Medical Clinic 123 Address Road SUBURBTOWN NSW 2000 Melanie Citizen Referring Doctor Your ref Address Dr John Medico 123 Main Street, SUBURBTOWN NSW 2000 Phone 02 9999 9999
Illumina s Cancer Research Portfolio and Dedicated Workflows
 Illumina s Cancer Research Portfolio and Dedicated Workflows Michael Sohn Clinical Sales Specialist Spain&Italy 2017 2017 Illumina, Inc. All rights reserved. Illumina, 24sure, BaseSpace, BeadArray, BlueFish,
Illumina s Cancer Research Portfolio and Dedicated Workflows Michael Sohn Clinical Sales Specialist Spain&Italy 2017 2017 Illumina, Inc. All rights reserved. Illumina, 24sure, BaseSpace, BeadArray, BlueFish,
NeoTYPE Cancer Profiles
 NeoTYPE Cancer Profiles 30+ Multimethod Assays for Hematologic Diseases and Solid Tumors Molecular FISH Anatomic Pathology The next generation of diagnostic, prognostic, and therapeutic assessment What
NeoTYPE Cancer Profiles 30+ Multimethod Assays for Hematologic Diseases and Solid Tumors Molecular FISH Anatomic Pathology The next generation of diagnostic, prognostic, and therapeutic assessment What
NeoTYPE Cancer Profiles
 NeoTYPE Cancer Profiles Multimethod Analysis of 25+ Hematologic Diseases and Solid Tumors Anatomic Pathology FISH Molecular The next generation of diagnostic, prognostic, and therapeutic assessment NeoTYPE
NeoTYPE Cancer Profiles Multimethod Analysis of 25+ Hematologic Diseases and Solid Tumors Anatomic Pathology FISH Molecular The next generation of diagnostic, prognostic, and therapeutic assessment NeoTYPE
What is the status of the technologies of "precision medicine?
 Session 2: What is the status of the technologies of "precision medicine? Gideon Blumenthal, MD, Clinical Team Leader, Thoracic and Head/Neck Oncology, Center for Drug Evaluation and Research (CDER), U.S.
Session 2: What is the status of the technologies of "precision medicine? Gideon Blumenthal, MD, Clinical Team Leader, Thoracic and Head/Neck Oncology, Center for Drug Evaluation and Research (CDER), U.S.
Frequency(%) KRAS G12 KRAS G13 KRAS A146 KRAS Q61 KRAS K117N PIK3CA H1047 PIK3CA E545 PIK3CA E542K PIK3CA Q546. EGFR exon19 NFS-indel EGFR L858R
 KRAS G12 KRAS G13 KRAS A146 KRAS Q61 KRAS K117N PIK3CA H1047 PIK3CA E545 PIK3CA E542K PIK3CA Q546. EGFR exon19 NFS-indel EGFR L858R") Frequency(%) 1 a b ALK FS-indel ALK R1Q HRAS Q61R HRAS G13R IDH R17K IDH R14Q MET exon14 SS-indel KIT D8Y KIT L76P KIT exon11 NFS-indel SMAD4 R361 IDH1 R13 CTNNB1 S37 CTNNB1 S4 AKT1 E17K ERBB D769H ERBB
Frequency(%) 1 a b ALK FS-indel ALK R1Q HRAS Q61R HRAS G13R IDH R17K IDH R14Q MET exon14 SS-indel KIT D8Y KIT L76P KIT exon11 NFS-indel SMAD4 R361 IDH1 R13 CTNNB1 S37 CTNNB1 S4 AKT1 E17K ERBB D769H ERBB
Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities
 Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities Sujana Movva 1, Wenhsiang Wen 2, Wangjuh Chen 2, Sherri Z. Millis 2, Margaret von Mehren 1, Zoran
Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities Sujana Movva 1, Wenhsiang Wen 2, Wangjuh Chen 2, Sherri Z. Millis 2, Margaret von Mehren 1, Zoran
Looking Beyond the Standard-of- Care : The Clinical Trial Option
 1 Looking Beyond the Standard-of- Care : The Clinical Trial Option Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor
1 Looking Beyond the Standard-of- Care : The Clinical Trial Option Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor
Clinical Grade Biomarkers in the Genomic Era Observations & Challenges
 Clinical Grade Biomarkers in the Genomic Era Observations & Challenges IOM Committee on Policy Issues in the Clinical Development & Use of Biomarkers for Molecularly Targeted Therapies March 31-April 1,
Clinical Grade Biomarkers in the Genomic Era Observations & Challenges IOM Committee on Policy Issues in the Clinical Development & Use of Biomarkers for Molecularly Targeted Therapies March 31-April 1,
MET skipping mutation, EGFR
 New NSCLC biomarkers in clinical research: detection of MET skipping mutation, EGFR T790M, and other important biomarkers Fernando López-Ríos Laboratorio de Dianas Terapéuticas Hospital Universitario HM
New NSCLC biomarkers in clinical research: detection of MET skipping mutation, EGFR T790M, and other important biomarkers Fernando López-Ríos Laboratorio de Dianas Terapéuticas Hospital Universitario HM
NGS in tissue and liquid biopsy
 NGS in tissue and liquid biopsy Ana Vivancos, PhD Referencias So, why NGS in the clinics? 2000 Sanger Sequencing (1977-) 2016 NGS (2006-) ABIPrism (Applied Biosystems) Up to 2304 per day (96 sequences
NGS in tissue and liquid biopsy Ana Vivancos, PhD Referencias So, why NGS in the clinics? 2000 Sanger Sequencing (1977-) 2016 NGS (2006-) ABIPrism (Applied Biosystems) Up to 2304 per day (96 sequences
Jennifer Hauenstein Oncology Cytogenetics Emory University Hospital Atlanta, GA
 Comparison of Genomic Coverage using Affymetrix OncoScan Array and Illumina TruSight Tumor 170 NGS Panel for Detection of Copy Number Abnormalities in Clinical GBM Specimens Jennifer Hauenstein Oncology
Comparison of Genomic Coverage using Affymetrix OncoScan Array and Illumina TruSight Tumor 170 NGS Panel for Detection of Copy Number Abnormalities in Clinical GBM Specimens Jennifer Hauenstein Oncology
APPLICATIONS OF NEXT GENERATION SEQUENCING IN SOLID TUMORS - PATHOLOGIST PROSPECTIVE
 AMP COMPANION MEETING SYMPOSIUM AT USCAP 2015 NEXT-GENERATION OF PATHOLOGY: ROLE OF PATHOLOGIST IN NGS-BASED PERSONALIZED MEDICINE APPLICATIONS OF NEXT GENERATION SEQUENCING IN SOLID TUMORS - PATHOLOGIST
AMP COMPANION MEETING SYMPOSIUM AT USCAP 2015 NEXT-GENERATION OF PATHOLOGY: ROLE OF PATHOLOGIST IN NGS-BASED PERSONALIZED MEDICINE APPLICATIONS OF NEXT GENERATION SEQUENCING IN SOLID TUMORS - PATHOLOGIST
Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ
 Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ G E NETIC T E CHNOLOGIST MEDICAL G E NETICS, CARDIFF To Cover Background to the project Choice of panel Validation process Genes on panel, Protocol
Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ G E NETIC T E CHNOLOGIST MEDICAL G E NETICS, CARDIFF To Cover Background to the project Choice of panel Validation process Genes on panel, Protocol
Enabling Personalized
 Molecular Enabling Personalized Diagnostics Medicine- Targeted Sequencing: NGS-based solutions Silvia Dorn Roel Reinders- Andreas Diplas Friday, 19.06.2015 Company Overview Founded in April 2011 Development
Molecular Enabling Personalized Diagnostics Medicine- Targeted Sequencing: NGS-based solutions Silvia Dorn Roel Reinders- Andreas Diplas Friday, 19.06.2015 Company Overview Founded in April 2011 Development
New Drug development and Personalized Therapy in The Era of Molecular Medicine
 New Drug development and Personalized Therapy in The Era of Molecular Medicine Ramesh K. Ramanathan MD Virginia G. Piper Cancer Center Translational Genomics Research Institute Scottsdale, AZ Clinical
New Drug development and Personalized Therapy in The Era of Molecular Medicine Ramesh K. Ramanathan MD Virginia G. Piper Cancer Center Translational Genomics Research Institute Scottsdale, AZ Clinical
FAQs for UK Pathology Departments
 FAQs for UK Pathology Departments This is an educational piece written for Healthcare Professionals FAQs for UK Pathology Departments If you would like to discuss any of the listed FAQs further, or have
FAQs for UK Pathology Departments This is an educational piece written for Healthcare Professionals FAQs for UK Pathology Departments If you would like to discuss any of the listed FAQs further, or have
Targeted Molecular Diagnostics for Targeted Therapies in Hematological Disorders
 Targeted Molecular Diagnostics for Targeted Therapies in Hematological Disorders Richard D. Press, MD, PhD Dept of Pathology Knight Cancer Institute Knight Diagnostic Labs Oregon Health & Science University
Targeted Molecular Diagnostics for Targeted Therapies in Hematological Disorders Richard D. Press, MD, PhD Dept of Pathology Knight Cancer Institute Knight Diagnostic Labs Oregon Health & Science University
Dr Yvonne Wallis Consultant Clinical Scientist West Midlands Regional Genetics Laboratory
 Dr Yvonne Wallis Consultant Clinical Scientist West Midlands Regional Genetics Laboratory Personalised Therapy/Precision Medicine Selection of a therapeutic drug based on the presence or absence of a specific
Dr Yvonne Wallis Consultant Clinical Scientist West Midlands Regional Genetics Laboratory Personalised Therapy/Precision Medicine Selection of a therapeutic drug based on the presence or absence of a specific
Updated Molecular Testing Guideline for the Selection of Lung Cancer Patients for Treatment with Targeted Tyrosine Kinase Inhibitors
 Q: How is the strength of recommendation determined in the new molecular testing guideline? A: The strength of recommendation is determined by the strength of the available data (evidence). Strong Recommendation:
Q: How is the strength of recommendation determined in the new molecular testing guideline? A: The strength of recommendation is determined by the strength of the available data (evidence). Strong Recommendation:
NGS ONCOPANELS: FDA S PERSPECTIVE
 NGS ONCOPANELS: FDA S PERSPECTIVE CBA Workshop: Biomarker and Application in Drug Development August 11, 2018 Rockville, MD You Li, Ph.D. Division of Molecular Genetics and Pathology Food and Drug Administration
NGS ONCOPANELS: FDA S PERSPECTIVE CBA Workshop: Biomarker and Application in Drug Development August 11, 2018 Rockville, MD You Li, Ph.D. Division of Molecular Genetics and Pathology Food and Drug Administration
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Secuenciación masiva: papel en la toma de decisiones
 Secuenciación masiva: papel en la toma de decisiones Cancer is a Genetic Disease Development of cancer is driven by the acquisition of somatic genetic alterations: Nonsynonymous point mutations: missense.
Secuenciación masiva: papel en la toma de decisiones Cancer is a Genetic Disease Development of cancer is driven by the acquisition of somatic genetic alterations: Nonsynonymous point mutations: missense.
1. Q: What has changed from the draft recommendations posted for public comment in November/December 2011?
 Frequently Asked Questions (FAQs) in regard to Molecular Testing Guideline for Selection of Lung Cancer Patients for EGFR and ALK Tyrosine Kinase Inhibitors 1. Q: What has changed from the draft recommendations
Frequently Asked Questions (FAQs) in regard to Molecular Testing Guideline for Selection of Lung Cancer Patients for EGFR and ALK Tyrosine Kinase Inhibitors 1. Q: What has changed from the draft recommendations
Plasma-Seq conducted with blood from male individuals without cancer.
 Supplementary Figures Supplementary Figure 1 Plasma-Seq conducted with blood from male individuals without cancer. Copy number patterns established from plasma samples of male individuals without cancer
Supplementary Figures Supplementary Figure 1 Plasma-Seq conducted with blood from male individuals without cancer. Copy number patterns established from plasma samples of male individuals without cancer
Liquid biopsy: the experience of real life case studies
 Liquid biopsy: the experience of real life case studies 10 th September 2018 Beatriz Bellosillo Servicio de Anatomía Patológica Hospital del Mar, Barcelona Agenda Introduction Experience in colorectal
Liquid biopsy: the experience of real life case studies 10 th September 2018 Beatriz Bellosillo Servicio de Anatomía Patológica Hospital del Mar, Barcelona Agenda Introduction Experience in colorectal
Genomic tests to personalize therapy of metastatic breast cancers. Fabrice ANDRE Gustave Roussy Villejuif, France
 Genomic tests to personalize therapy of metastatic breast cancers Fabrice ANDRE Gustave Roussy Villejuif, France Future application of genomics: Understand the biology at the individual scale Patients
Genomic tests to personalize therapy of metastatic breast cancers Fabrice ANDRE Gustave Roussy Villejuif, France Future application of genomics: Understand the biology at the individual scale Patients
Disclosures Genomic testing in lung cancer
 Disclosures Genomic testing in lung cancer No disclosures Objectives Understand how FISH and NGS provide complementary data for the evaluation of lung cancer Recognize the challenges of performing testing
Disclosures Genomic testing in lung cancer No disclosures Objectives Understand how FISH and NGS provide complementary data for the evaluation of lung cancer Recognize the challenges of performing testing
Identification and clinical detection of genetic alterations of pre-neoplastic lesions Time for the PML ome? David Sidransky MD Johns Hopkins
 Identification and clinical detection of genetic alterations of pre-neoplastic lesions Time for the PML ome? David Sidransky MD Johns Hopkins February 3-5, 2016 Lansdowne Resort, Leesburg, VA Molecular
Identification and clinical detection of genetic alterations of pre-neoplastic lesions Time for the PML ome? David Sidransky MD Johns Hopkins February 3-5, 2016 Lansdowne Resort, Leesburg, VA Molecular
NGS IN ONCOLOGY: FDA S PERSPECTIVE
 NGS IN ONCOLOGY: FDA S PERSPECTIVE ASQ Biomed/Biotech SIG Event April 26, 2018 Gaithersburg, MD You Li, Ph.D. Division of Molecular Genetics and Pathology Food and Drug Administration (FDA) Center for
NGS IN ONCOLOGY: FDA S PERSPECTIVE ASQ Biomed/Biotech SIG Event April 26, 2018 Gaithersburg, MD You Li, Ph.D. Division of Molecular Genetics and Pathology Food and Drug Administration (FDA) Center for
Personalised Healthcare (PHC) with Foundation Medicine (FMI) Fatma Elçin KINIKLI, FMI Turkey, Science Leader
 with Foundation Medicine (FMI) Fatma Elçin KINIKLI, FMI Turkey, Science Leader") Personalised Healthcare (PHC) with Foundation Medicine (FMI) Fatma Elçin KINIKLI, FMI Turkey, Science Leader Agenda PHC Approach Provides Better Patient Outcome FMI offers Comprehensive Genomic Profiling,
Personalised Healthcare (PHC) with Foundation Medicine (FMI) Fatma Elçin KINIKLI, FMI Turkey, Science Leader Agenda PHC Approach Provides Better Patient Outcome FMI offers Comprehensive Genomic Profiling,
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Patricia Aoun MD, MPH Professor and Vice-Chair for Clinical Affairs Medical Director, Clinical Laboratories Department of Pathology City of Hope
 Patricia Aoun MD, MPH Professor and Vice-Chair for Clinical Affairs Medical Director, Clinical Laboratories Department of Pathology City of Hope National Medical Center Disclosures I have no disclosures
Patricia Aoun MD, MPH Professor and Vice-Chair for Clinical Affairs Medical Director, Clinical Laboratories Department of Pathology City of Hope National Medical Center Disclosures I have no disclosures
Detecting Oncogenic Mutations in Whole Blood
 WHITE PAPER Detecting Oncogenic Mutations in Whole Blood Analytical validation of Cynvenio Biosystems LiquidBiopsy circulating tumor cell (CTC) capture and next-generation sequencing (NGS) September 2013
WHITE PAPER Detecting Oncogenic Mutations in Whole Blood Analytical validation of Cynvenio Biosystems LiquidBiopsy circulating tumor cell (CTC) capture and next-generation sequencing (NGS) September 2013
Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San
 Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San Francisco Lung Cancer Classification Pathological Classification
Osamu Tetsu, MD, PhD Associate Professor Department of Otolaryngology-Head and Neck Surgery School of Medicine, University of California, San Francisco Lung Cancer Classification Pathological Classification
Molecular. Oncology & Pathology. Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine. Liquid Biopsy.
 Molecular Oncology & Pathology Hereditary Cancer Somatic Cancer Liquid Biopsy Next-Gen Sequencing qpcr Sanger Sequencing Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine
Molecular Oncology & Pathology Hereditary Cancer Somatic Cancer Liquid Biopsy Next-Gen Sequencing qpcr Sanger Sequencing Diagnostic, Prognostic, Therapeutic, and Predisposition Tests in Precision Medicine
A Day in the Life of a Breast Cancer Doctor: Integrating Omics to Optimize Patient Outcomes. March 17-18, 2015 New York, NY
 A Day in the Life of a Breast Cancer Doctor: Integrating Omics to Optimize Patient Outcomes March 17-18, 2015 New York, NY A Day in the Life of a Breast Cancer Doctor: Integrating Omics to Optimize Patient
A Day in the Life of a Breast Cancer Doctor: Integrating Omics to Optimize Patient Outcomes March 17-18, 2015 New York, NY A Day in the Life of a Breast Cancer Doctor: Integrating Omics to Optimize Patient
Personalized Medicine: Lung Biopsy and Tumor
 Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Elizabeth H. Moore, MD Personalized Medicine: Lung Biopsy and Tumor Mutation Testing Genomic testing has resulted in a paradigm shift in the
Diagnostica Molecolare!
 Diagnostica Molecolare! Aldo Scarpa Unità Diagnostica Molecolare Azienda Ospedaliera Universitaria Integrata di Verona e ARC-NET Centro di Ricerca Applicata sul Cancro PDTA CARCINOMA POLMONARE - IL PAZIENTE
Diagnostica Molecolare! Aldo Scarpa Unità Diagnostica Molecolare Azienda Ospedaliera Universitaria Integrata di Verona e ARC-NET Centro di Ricerca Applicata sul Cancro PDTA CARCINOMA POLMONARE - IL PAZIENTE
AVENIO family of NGS oncology assays ctdna and Tumor Tissue Analysis Kits
 AVENIO family of NGS oncology assays ctdna and Tumor Tissue Analysis Kits Accelerating clinical research Next-generation sequencing (NGS) has the ability to interrogate many different genes and detect
AVENIO family of NGS oncology assays ctdna and Tumor Tissue Analysis Kits Accelerating clinical research Next-generation sequencing (NGS) has the ability to interrogate many different genes and detect
AVENIO ctdna Analysis Kits The complete NGS liquid biopsy solution EMPOWER YOUR LAB
 Analysis Kits The complete NGS liquid biopsy solution EMPOWER YOUR LAB Analysis Kits Next-generation performance in liquid biopsies 2 Accelerating clinical research From liquid biopsy to next-generation
Analysis Kits The complete NGS liquid biopsy solution EMPOWER YOUR LAB Analysis Kits Next-generation performance in liquid biopsies 2 Accelerating clinical research From liquid biopsy to next-generation
MEDICAL POLICY. SUBJECT: MOLECULAR PANEL TESTING OF CANCERS TO IDENTIFY TARGETED THERAPIES (Excluding NSCLC and CRC) EFFECTIVE DATE: 12/21/17
 EFFECTIVE DATE: 12/21/17") MEDICAL POLICY SUBJECT: MOLECULAR PANEL TESTING OF PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
MEDICAL POLICY SUBJECT: MOLECULAR PANEL TESTING OF PAGE: 1 OF: 5 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including
Circulating Tumor DNA in GIST and its Implications on Treatment
 Circulating Tumor DNA in GIST and its Implications on Treatment October 2 nd 2017 Dr. Ciara Kelly Assistant Attending Physician Sarcoma Medical Oncology Service Objectives Background Liquid biopsy & ctdna
Circulating Tumor DNA in GIST and its Implications on Treatment October 2 nd 2017 Dr. Ciara Kelly Assistant Attending Physician Sarcoma Medical Oncology Service Objectives Background Liquid biopsy & ctdna
Next Generation Sequencing in Haematological Malignancy: A European Perspective. Wolfgang Kern, Munich Leukemia Laboratory
 Next Generation Sequencing in Haematological Malignancy: A European Perspective Wolfgang Kern, Munich Leukemia Laboratory Diagnostic Methods Cytomorphology Cytogenetics Immunophenotype Histology FISH Molecular
Next Generation Sequencing in Haematological Malignancy: A European Perspective Wolfgang Kern, Munich Leukemia Laboratory Diagnostic Methods Cytomorphology Cytogenetics Immunophenotype Histology FISH Molecular
Out-Patient Billing CPT Codes
 Out-Patient Billing CPT Codes Updated Date: August 3, 08 Client Billed Molecular Tests HPV DNA Tissue Testing 8764 No Medicare Billed - Molecular Tests NeoARRAY NeoARRAY SNP/Cytogenetic No 89 NeoLAB NeoLAB
Out-Patient Billing CPT Codes Updated Date: August 3, 08 Client Billed Molecular Tests HPV DNA Tissue Testing 8764 No Medicare Billed - Molecular Tests NeoARRAY NeoARRAY SNP/Cytogenetic No 89 NeoLAB NeoLAB
National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2011 Formula Grant
 Foundation Annual Progress Report: 2011 Formula Grant") National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2011 Formula Grant Reporting Period July 1, 2012 June 30, 2013 Formula Grant Overview The NSABP Foundation
National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2011 Formula Grant Reporting Period July 1, 2012 June 30, 2013 Formula Grant Overview The NSABP Foundation
Precision Oncology: Experience at UW
 Precision Oncology: Experience at UW Colin Pritchard MD, PhD University of Washington, Department of Lab Medicine WSMOS Meeting November 1, 2013 Conflict of Interest Disclosures I declare the following,
Precision Oncology: Experience at UW Colin Pritchard MD, PhD University of Washington, Department of Lab Medicine WSMOS Meeting November 1, 2013 Conflict of Interest Disclosures I declare the following,
Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology
 Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology Ugur Ozerdem, M.D. 1 Abstract Background: There is a paradigm shift in breast biopsy philosophy. In
Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology Ugur Ozerdem, M.D. 1 Abstract Background: There is a paradigm shift in breast biopsy philosophy. In
Molecular Testing Updates. Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine
 Molecular Testing Updates Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine Keeping Up with Predictive Molecular Testing in Oncology: Technical
Molecular Testing Updates Karen Rasmussen, PhD, FACMG Clinical Molecular Genetics Spectrum Medical Group, Pathology Division Portland, Maine Keeping Up with Predictive Molecular Testing in Oncology: Technical
Liquid biopsy in lung cancer: The EGFR paradigm
 Liquid biopsy in lung cancer: The EGFR paradigm Lynette M. Sholl, M.D. Brigham and Women s Hospital Dana Farber Cancer Institute Department of Pathology Boston, MA Disclosure of Relevant Financial Relationships
Liquid biopsy in lung cancer: The EGFR paradigm Lynette M. Sholl, M.D. Brigham and Women s Hospital Dana Farber Cancer Institute Department of Pathology Boston, MA Disclosure of Relevant Financial Relationships
Clinically Useful Next Generation Sequencing and Molecular Testing in Gliomas MacLean P. Nasrallah, MD PhD
 Clinically Useful Next Generation Sequencing and Molecular Testing in Gliomas MacLean P. Nasrallah, MD PhD Neuropathology Fellow Division of Neuropathology Center for Personalized Diagnosis (CPD) Glial
Clinically Useful Next Generation Sequencing and Molecular Testing in Gliomas MacLean P. Nasrallah, MD PhD Neuropathology Fellow Division of Neuropathology Center for Personalized Diagnosis (CPD) Glial
Disclosure. Summary. Circulating DNA and NGS technology 3/27/2017. Disclosure of Relevant Financial Relationships. JS Reis-Filho, MD, PhD, FRCPath
 Circulating DNA and NGS technology JS Reis-Filho, MD, PhD, FRCPath Director of Experimental Pathology, Department of Pathology Affiliate Member, Human Oncology and Pathogenesis Program Disclosure of Relevant
Circulating DNA and NGS technology JS Reis-Filho, MD, PhD, FRCPath Director of Experimental Pathology, Department of Pathology Affiliate Member, Human Oncology and Pathogenesis Program Disclosure of Relevant
NGS Gateway Lab Services
 TM NGS Gateway Lab Services Accelerating Precision Medicine Design a Complete Genomic Testing Portfolio with Turnkey Assays About NGS Gateway Lab Services TM Designed to provide a gateway to your own in-house
TM NGS Gateway Lab Services Accelerating Precision Medicine Design a Complete Genomic Testing Portfolio with Turnkey Assays About NGS Gateway Lab Services TM Designed to provide a gateway to your own in-house
StrandAdvantage Tissue-Specific Cancer Genomic Tests. Empowering Crucial First-Line Therapy Decisions for Your Patient
 StrandAdvantage Tissue-Specific Cancer Genomic Tests Empowering Crucial First-Line Therapy Decisions for Your Patient Harness the power of precision medicine with StrandAdvantage Precision medicine in
StrandAdvantage Tissue-Specific Cancer Genomic Tests Empowering Crucial First-Line Therapy Decisions for Your Patient Harness the power of precision medicine with StrandAdvantage Precision medicine in
Molecular Testing in Lung Cancer
 Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Molecular Testing in Lung Cancer Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in lung cancer Source: Khono et al, Trans
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD. Mount Carrigain 2/4/17
 Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
The Role of Pathology/Molecular Diagnostic in Personalized Medicine
 The Role of Pathology/Molecular Diagnostic in Personalized Medicine Ignacio I. Wistuba, M.D. Jay and Lori Eissenberg Professor in Lung Cancer Director of the Thoracic Molecular Pathology Lab Departments
The Role of Pathology/Molecular Diagnostic in Personalized Medicine Ignacio I. Wistuba, M.D. Jay and Lori Eissenberg Professor in Lung Cancer Director of the Thoracic Molecular Pathology Lab Departments
I. Diagnosis of the cancer type in CUP
 Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Individualized Cancer Therapy: Chemotherapy Resistance Testing before Therapy
 Individualized Cancer Therapy: Chemotherapy Resistance Testing before Therapy 1 st st International Oncological Conference Wrocław, October 6 th, 2012 Dr. Frank Kischkel Individualized Cancer Therapy:
Individualized Cancer Therapy: Chemotherapy Resistance Testing before Therapy 1 st st International Oncological Conference Wrocław, October 6 th, 2012 Dr. Frank Kischkel Individualized Cancer Therapy:
Next-generation sequencing based clinical testing for lung cancer in Japan
 Review Article Next-generation sequencing based clinical testing for lung cancer in Japan Masayuki Takeda 1, Kazuko Sakai 2, Kazuhiko Nakagawa 1, Kazuto Nishio 2 1 Department of Medical Oncology, 2 Department
Review Article Next-generation sequencing based clinical testing for lung cancer in Japan Masayuki Takeda 1, Kazuko Sakai 2, Kazuhiko Nakagawa 1, Kazuto Nishio 2 1 Department of Medical Oncology, 2 Department
Next generation diagnostics Bringing high-throughput sequencing into clinical application
 Next generation diagnostics Bringing high-throughput sequencing into clinical application Leonardo A. Meza-Zepeda, PhD Translational Genomics Group Institute for Cancer Research Leonardo.Meza-Zepeda@rr-research.no
Next generation diagnostics Bringing high-throughput sequencing into clinical application Leonardo A. Meza-Zepeda, PhD Translational Genomics Group Institute for Cancer Research Leonardo.Meza-Zepeda@rr-research.no
patients in the era of
 Communicating with cancer patients in the era of personalized medicine September 9 th, 2017 Gerald Prager, M.D. Comprehensive Cancer Center Vienna Medical University of Vienna, Austria Gerald Prager, M.D.
Communicating with cancer patients in the era of personalized medicine September 9 th, 2017 Gerald Prager, M.D. Comprehensive Cancer Center Vienna Medical University of Vienna, Austria Gerald Prager, M.D.
Corporate Medical Policy
 Corporate Medical Policy Molecular Panel Testing of Cancers to Identify Targeted Therapies File Name: Origination: Last CAP Review: Next CAP Review: Last Review: molecular_panel_testing_of_cancers_to_identify_targeted_therapies
Corporate Medical Policy Molecular Panel Testing of Cancers to Identify Targeted Therapies File Name: Origination: Last CAP Review: Next CAP Review: Last Review: molecular_panel_testing_of_cancers_to_identify_targeted_therapies
Computer Science, Biology, and Biomedical Informatics (CoSBBI) Outline. Molecular Biology of Cancer AND. Goals/Expectations. David Boone 7/1/2015
 Outline. Molecular Biology of Cancer AND. Goals/Expectations. David Boone 7/1/2015") Goals/Expectations Computer Science, Biology, and Biomedical (CoSBBI) We want to excite you about the world of computer science, biology, and biomedical informatics. Experience what it is like to be a
Goals/Expectations Computer Science, Biology, and Biomedical (CoSBBI) We want to excite you about the world of computer science, biology, and biomedical informatics. Experience what it is like to be a
NCCN Non-Small Cell Lung Cancer V Meeting June 15, 2018
 Guideline Page and Request Illumina Inc. requesting to replace Testing should be conducted as part of broad molecular profiling with Consider NGS-based assays that include EGFR, ALK, ROS1, and BRAF as
Guideline Page and Request Illumina Inc. requesting to replace Testing should be conducted as part of broad molecular profiling with Consider NGS-based assays that include EGFR, ALK, ROS1, and BRAF as
Oncomine Focus assay panel and Oncomine Knowledgebase Reporter.
 Oncomine Focus assay panel and Oncomine Knowledgebase Reporter. How it can help to identify relevant alteration and early phase trials. Dr Isabelle SOUBEYRAN Dr Emmanuel KHALIFA Molecular Pathology Unit
Oncomine Focus assay panel and Oncomine Knowledgebase Reporter. How it can help to identify relevant alteration and early phase trials. Dr Isabelle SOUBEYRAN Dr Emmanuel KHALIFA Molecular Pathology Unit
High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX
 High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX Test: An Independent Quality Assurance Study DAVID J DABBS, MD Professor and Chief of Pathology
High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX Test: An Independent Quality Assurance Study DAVID J DABBS, MD Professor and Chief of Pathology
Harmesh Naik, MD. Hope Cancer Clinic PERSONALIZED CANCER TREATMENT USING LATEST IN MOLECULAR BIOLOGY
 Harmesh Naik, MD. Hope Cancer Clinic PERSONALIZED CANCER TREATMENT USING LATEST IN MOLECULAR BIOLOGY A NEW GENE A DAY.WHILE YOU ARE ENJOYING MORNING COFFEE From cancer.gov GOALS FOR THE CME TODAY A brief
Harmesh Naik, MD. Hope Cancer Clinic PERSONALIZED CANCER TREATMENT USING LATEST IN MOLECULAR BIOLOGY A NEW GENE A DAY.WHILE YOU ARE ENJOYING MORNING COFFEE From cancer.gov GOALS FOR THE CME TODAY A brief
Non-Profit Startup Paradigm Launches Cancer Panel Based on DNA, RNA Sequencing
 Non-Profit Startup Paradigm Launches Cancer Panel Based on DNA, RNA Sequencing April 11, 2014 By Tony Fong Non-profit diagnostics outfit Paradigm last month joined a growing list of entrants in the clinical
Non-Profit Startup Paradigm Launches Cancer Panel Based on DNA, RNA Sequencing April 11, 2014 By Tony Fong Non-profit diagnostics outfit Paradigm last month joined a growing list of entrants in the clinical
Molecular Markers. Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC
 Molecular Markers Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC Overview Testing methods Rationale for molecular testing
Molecular Markers Marcie Riches, MD, MS Associate Professor University of North Carolina Scientific Director, Infection and Immune Reconstitution WC Overview Testing methods Rationale for molecular testing
Regulatory Landscape for Precision Medicine
 Regulatory Landscape for Precision Medicine Adam C. Berger, Ph.D. Office of In Vitro Diagnostics and Radiological Health, FDA FOCR-Alexandria A Blueprint for Breakthrough Meeting September 13, 2017 1 What
Regulatory Landscape for Precision Medicine Adam C. Berger, Ph.D. Office of In Vitro Diagnostics and Radiological Health, FDA FOCR-Alexandria A Blueprint for Breakthrough Meeting September 13, 2017 1 What
Dr C K Kwan. Associate Consultant, Queen Elizabeth Hospital, HKSAR Honorary member, Targeted Therapy Team, ICR, UK
 HA Convention 2013 Dr C K Kwan MBChB, FRCR, FHKCR, FHKAM, MPM, CPI, MAppMgt(Hlth) Associate Consultant, Queen Elizabeth Hospital, HKSAR Honorary member, Targeted Therapy Team, ICR, UK To personalize cancer
HA Convention 2013 Dr C K Kwan MBChB, FRCR, FHKCR, FHKAM, MPM, CPI, MAppMgt(Hlth) Associate Consultant, Queen Elizabeth Hospital, HKSAR Honorary member, Targeted Therapy Team, ICR, UK To personalize cancer
Importance of Methodology Certification and Accreditations to Perform Assays. Stan Hamilton, MD Head, Pathology and Laboratory Medicine
 Importance of Methodology Certification and Accreditations to Perform Assays Stan Hamilton, MD Head, Pathology and Laboratory Medicine 1 Disclosures No disclosures relevant to this presentation 2 A bad
Importance of Methodology Certification and Accreditations to Perform Assays Stan Hamilton, MD Head, Pathology and Laboratory Medicine 1 Disclosures No disclosures relevant to this presentation 2 A bad
Aliccia Bollig-Fischer, PhD Department of Oncology, Wayne State University Associate Director Genomics Core Molecular Therapeutics Program Karmanos
 Aliccia Bollig-Fischer, PhD Department of Oncology, Wayne State University Associate Director Genomics Core Molecular Therapeutics Program Karmanos Cancer Institute Development of a multiplexed assay to
Aliccia Bollig-Fischer, PhD Department of Oncology, Wayne State University Associate Director Genomics Core Molecular Therapeutics Program Karmanos Cancer Institute Development of a multiplexed assay to
Oncology Drug Development
 Oncology Drug Development Advantages and challenges of using stratified clinical studies Simon J Hollingsworth The 18th Anti-Tumour Drug Development Forum 21 February Japan Stratified Medicine In The Clinic
Oncology Drug Development Advantages and challenges of using stratified clinical studies Simon J Hollingsworth The 18th Anti-Tumour Drug Development Forum 21 February Japan Stratified Medicine In The Clinic
AD (Leave blank) TITLE: Genomic Characterization of Brain Metastasis in Non-Small Cell Lung Cancer Patients
 TITLE: Genomic Characterization of Brain Metastasis in Non-Small Cell Lung Cancer Patients") AD (Leave blank) Award Number: W81XWH-12-1-0444 TITLE: Genomic Characterization of Brain Metastasis in Non-Small Cell Lung Cancer Patients PRINCIPAL INVESTIGATOR: Mark A. Watson, MD PhD CONTRACTING ORGANIZATION:
AD (Leave blank) Award Number: W81XWH-12-1-0444 TITLE: Genomic Characterization of Brain Metastasis in Non-Small Cell Lung Cancer Patients PRINCIPAL INVESTIGATOR: Mark A. Watson, MD PhD CONTRACTING ORGANIZATION:
Integration of Genomics Into Clinical Pathways. Precision Medicine and Decision Support
 Integration of Genomics Into Clinical Pathways Precision Medicine and Decision Support Faculty Andrew Hertler, MD, FACP Chief Medical Officer New Century Health Andrew Hertler, MD, FACP is employed by
Integration of Genomics Into Clinical Pathways Precision Medicine and Decision Support Faculty Andrew Hertler, MD, FACP Chief Medical Officer New Century Health Andrew Hertler, MD, FACP is employed by
Multi-drug, genetic-marker-directed, non-comparative, multi-centre, multi-arm phase II trial in non-small cell lung cancer
 Multi-drug, genetic-marker-directed, non-comparative, multi-centre, multi-arm phase II trial in non-small cell lung cancer Sponsor: University of Birmingham Chief Investigator: Gary Middleton Chief Biostatistician:
Multi-drug, genetic-marker-directed, non-comparative, multi-centre, multi-arm phase II trial in non-small cell lung cancer Sponsor: University of Birmingham Chief Investigator: Gary Middleton Chief Biostatistician:
Supplementary Figure 1. Cytoscape bioinformatics toolset was used to create the network of protein-protein interactions between the product of each
 Supplementary Figure 1. Cytoscape bioinformatics toolset was used to create the network of protein-protein interactions between the product of each mutated gene and the panel of 125 cancer-driving genes
Supplementary Figure 1. Cytoscape bioinformatics toolset was used to create the network of protein-protein interactions between the product of each mutated gene and the panel of 125 cancer-driving genes
Circulating tumour DNA in breast cancer. Kathleen Burke, PhD Bioinformatics Postdoctoral Fellow Laboratory of Dr. Jorge Reis-Filho
 Circulating tumour DNA in breast cancer Kathleen Burke, PhD Bioinformatics Postdoctoral Fellow Laboratory of Dr. Jorge Reis-Filho Conflicts of Interest I have no financial relationships to disclose I will
Circulating tumour DNA in breast cancer Kathleen Burke, PhD Bioinformatics Postdoctoral Fellow Laboratory of Dr. Jorge Reis-Filho Conflicts of Interest I have no financial relationships to disclose I will
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy