Menopause. Pamela S Miles MD Dept. of OB/GYN
|
|
|
- Johnathan Marsh
- 6 years ago
- Views:
Transcription
1 Menopause Pamela S Miles MD Dept. of OB/GYN
2 Defining Menopause Defined as the point in time after 12 consecutive months of amenorrhea with no obvious pathologic cause (avg. 52) Peri-menopause/menopause transition span of time when cycle and endocrine changes occur a few years before and 12 months after final menses resulting from natural menopause Premature menopause is less than or equal to age 40, whether natural or induced; ~1% of women Induced menopause is permanent cessation of menses after BSO or iatrogenic ablation of ovarian function 1/3 of a woman s life

3 STRAW + 10
4 Menopause physiology Loss of follicles, most from atresia, accelerated in our late 30 s Elevated FSH and LH Ovarian estrogen and inhibin production/feedback decreases androgen availability increases with age adrenals decrease DHEA/DHEAS and ovaries decrease androstenedione
5 Midlife Changes Changes in bleeding patterns Vasomotor/hot flushes Sleep disturbances Vulvovaginal dryness and discomfort Urinary changes Sexual/decreased libido Cognition concerns Weight gain Skin and hair changes
6 Routine evaluations
7 Office exam Measured height and weight; BMI or hip/waist ratio BP Pelvic and indicated pap smear Breast exam? Lifestyle concerns
8 Breast Screening ACS - annual mammograms at 40 NCI - annual mammograms at 50, every 1-2 years NAMS - annual mammograms at 40 USPSTF - mammograms every 2 years at 50-74; no SBE WHO - mammograms every 2 years at 50-69; no SBE ACOG 1-2 year interval age and annual after 50 8
9 Breast changes breasts decrease in size due to less estrogen stimulation supportive connective tissue decreases ratio of fat to fibrous tissue increases which makes breasts less firm but easier to evaluate with mammography 9
10 Colon cancer screening Colonoscopy every 10 years beginning at 50 Fecal occult blood testing (FIT, guaiac) yearly Sigmoidoscopy every 5 years; this can be done in combination with FOBT every 5-10 years as an alternative to colonoscopy Barium enema with air contrast every 5 years CT
11 Laboratory screenings to consider Lipids Chemistry/HbA1c TSH Vitamin D STI, HIV and Hep C as indicated
12 Clinical issues
13 Irregular bleeding 90% of women experience 4-8 years of menstrual cycle changes before menopause main cause is irregular ovulation especially in early perimenopause; lack of ovulation in late perimenopause must consider and evaluate for numerous causes, assess risk factors (reproductive tract, systemic, meds) EMB, ultrasound for endometrial thickness, hysteroscopy, labs, STD screening

14

15 Why Flash?? Etiology is unclear but could be related to estrogen withdraw, other diseases and medications; also a more narrow thermoneutral zone Average lasts 1-5 minutes; occurs over months to years especially right before and after the LMP Affects up to 75% of women Varies by ethnicity: AfricanAmerican>Hispanics>Caucasian>Asian Increased in obesity
16
17 Vasomotor symptom treatment Treatment of moderate to severe vasomotor symptoms (VMS) remains the primary indication for systemic hormone therapy Hormone therapy is the most successful treatment (a complete list of products available in the US and Canada is on the NAMS website at menopause.org) 75% successful 50% recurrence with discontinuation Brisdelle 7.5 mg paroxetine approved 2013 for VMS; off label use of other SSRIs Duavee is CE/bazedoxifene approved for VMS
18 Alternative treatments for hot flashes Cooler environment Weight loss/exercise Acupuncture Phytoestrogens/soy/isoflavone black cohash Decrease smoking Vitamin E, omega-3 Progesterone Medications used off-label such as Gabapentin, Lyrica, Clonidine
19 Alternative treatments for hot flashes con t Cognitive behavioral treatment and hypnotherapy have evidence of benefit to decrease bothersome level of symptoms Weight loss and s-equol of soy have evidence of benefit also, though less
20
21 Genitourinary syndrome of menopause (GSM) & VVA Up to 75% of women have atrophic symptoms Lack of estrogen leads to decrease lactobacilli, increased ph, epithelial thinning Ulcerations, petechiae, trauma, pain and dyspareunia can result Rule out other etiologies such as infection and vulvar dystrophy Urinary changes include urgency and increased urinary tract infections
22 Vaginal estrogen therapy Estrogen is the most effective treatment for moderate to severe symptoms of vulvar and vaginal atrophy; topical recommended if this is the only indication for estrogen Up to 90% improve vaginal symptoms Treatment increases blood flow, epithelial maturity, decreases ph, and increases secretions; urethral benefits of decreased UTIs and urgency Progesterone not needed but no safety data beyond one year of treatment; serum estrogen remains in postmenopausal range
23 FDA approved vaginal estrogens: estradiol cream (Estrace) conjugated estrogen cream (Premarin) estradiol ring (Estring) estradiol hemihydrate tablet (Vagifem) All equally effective and choice based on patient preference 23
24 Ospemifene estrogen agonist/antagonist (SERM) FDA approved to treat dyspareunia related to vaginal atrophy 60 mg oral tablet may cause vasomotor symptoms 24
25 Non prescription treatment lubricants - usually water-based and used with sexual activity vaginal moisturizers - used at any time to provide comfort to vaginal tissues sex 25
26 Menopause and sexual function Treatment of moderate to severe vaginal atrophy with systemic HT or local ET can relieve dyspareunia which is a common cause of intercourse avoidance Hormonal therapy not recommended as sole treatment of other sexual function problems (such as decreased libido) Testosterone does not continue to decline at menopause and limited benefit to supplements Flibanserin (Addyi) for treatment of HSDD in premenopausal women
27 Disease Risks
28 Breast Cancer 1 out of 8 risk in US; 2% of women by age 50 Most important risk factors are age and gender SBE, mammogram, MRI, ultrasound, ductal lavage are all screening tools Potential risks include BRCA gene, personal cancer hx, first degree relative with breast cancer, menarche <12, menopause >55, nulliparity or first child after age 30, obesity after menopause, alcohol > 2 drinks/day, lack of exercise, low vitamin D, poor diet, radiation exposure
29 Breast cancer risk reduction Lifestyle changes decrease weight, decrease alcohol Chemoprevention women at increased risk benefit from SERM treatment to prevent primary breast cancer (ex. tamoxifen and raloxifene) Aromatase inhibitors reduce breast cancer recurrence Prophylactic mastectomy
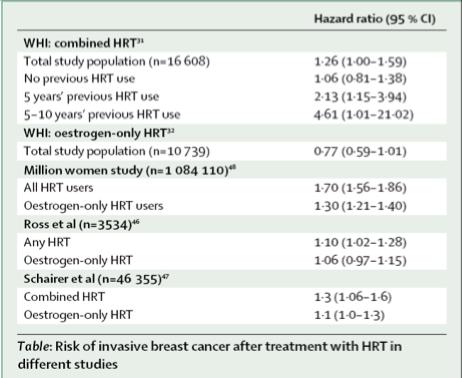
30 HT and Breast cancer Breast cancer risk increases with estrogenprogestin use beyond 3-5 years Estrogen only therapy for up to 7 years had no increase on cancer risk No increased risk if wait for 5 years after menopause to start HRT Unclear if HT risk differs between continuous and sequential progestogen therapy or choice of progestogen; low dose HT has not been evaluated long term
31

32
33 Osteoporosis most common bone disorder affecting humans peak bone mass achieved in third decade 80 % of osteoporosis diagnoses are women 12th leading cause of death in women; average age of hip fracture is 82 with 25% increase mortality in the next year Fragility fracture allows the diagnosis clinically >50 years old - DXA measurements include total hip, femoral neck and posterior-anterior lumbar spine and can define the diagnosis with T-score 2.5 SD below the mean T score is comparison of patient to normal young adult female
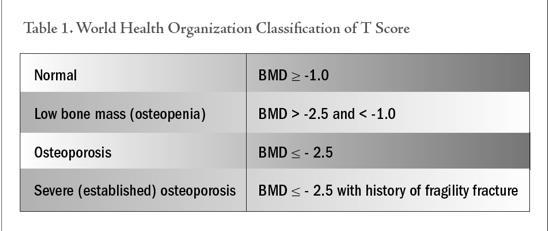
34 T-Score
35 Patients (%) All fractures are Associated With Morbidity Unable to carry out at least one independent activity of daily living 80% Death within one year 20% Permanent disability 30% Unable to walk independently 40% Cooper C, Am J Med, 1997;103(2A):12S-17S
36 Osteoporosis Risks Age increases with age Genetics affects peak bone mass Lifestyle poor nutrition, smoking, alcohol, decreased activity Thinness BMI < 21 Menopausal status decreases 2% per year during perimenopause
37 Bone Mineral Density testing indications: All women > 65 years old postmenopausal with fragility fracture Postmenopausal <65 years old with one or more risk factor: previous fracture after menopause, thinness or BMI <21, parental hip fracture or family hx of osteoporosis, smoker, rheumatoid arthritis, excessive alcohol intake, long term high risk medications

38 Vertebral Fractures Most common fracture type Often silent Insidious, progressive nature Associated with significant morbidity Predict future spine and hip fractures Associated with 2-fold increase in risk of death
39 FRAX Uses risk factors identified by WHO Uses g/cm2 measurement of BMD at femoral neck Calculates 10 year risk of major osteoporotic fracture and risk of hip fracture used to guide appropriate patients for therapy 39

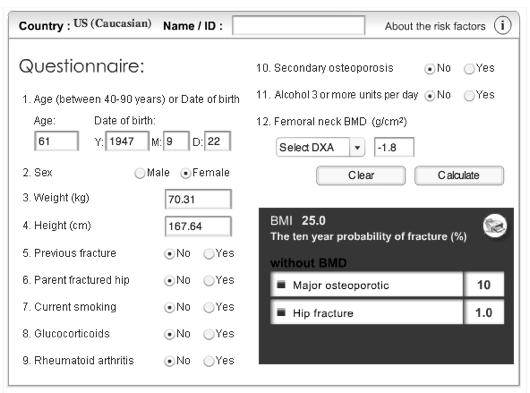
40 FRAX
41 Prescriptive treatment NAMS recommends tx if postmenopausal: -with vertebral or hip fracture -with BMD diagnosis of osteoporosis -with osteopenia and FRAX calculator fracture risk of major osteoporotic fx of at least 20% and hip fx of at least 3%
42 Osteoporosis treatment Rx Systemic estrogen therapy is approved for prevention, not treatment of osteoporosis; this includes Estrogen, E+P regimens and BZA-CE Bisphosphonate medications are approved for prevention and treatment with a diagnosis of osteoporosis Estrogen agonist/antagonist (SERM) raloxifene approved for prevention and treatment Teriparatide (Forteo)- PTH - stimulates osteoblasts; approved for treatment; daily SQ Denosumab-(Prolia) - inhibits osteoclasts; approved for treatment; q 6 month SQ Calcitonin approved for treatment
43 Bisphosphonates first line drugs for treatment reduces risk of vertebral > non-vertebral fractures uncertain if vary in protection from fracture risk Dosing available as oral or intravenous includes alendronate, risedronate, ibandronate and zoledronic acid 43
44 Selective Estrogen-receptor modulators (SERMs) raloxifene (Evista) approved as prevention and treatment reduces vertebral osteoporotic fracture and decreases bone turnover also reduces risk of invasive breast cancer available as oral tablet bazedoxifene+conjugated equine estrogen (Duavee) approved 10/13 for prevention 44
45
46 Calcium Institute of Medicine recommends 1200 mg daily total from food and supplements for women over 50 to maintain bone health absorption affected by estrogen, Vitamin D, foods works with exercise to improve BMD women >60 had decreased hip fractures with calcium/vitamin D when supplement initiated dietary calcium does not appear to increase kidney stones or risk for CVD
47 Vitamin D Approximately 50% of the population is thought to be deficient Active form mediates the absorption of calcium in the intestines must be metabolized to be active so does not have to be taken with calcium Definition of low level not always agreed upon; 20 ng/ml to 50 ng/ml should be adequate; above this does not show continued improvement Recommended dose ~ IU daily for women
48 Vitamin D Risk factors for decreased D levels: *increased age *northern climate *limited sun exposure *obesity *poor dietary intake *dark skin *various medical conditions (poor absorption)
49 Cardiovascular Disease #1 killer of women ET does not increase the risk of CHD when initiated in women recently menopausal (within 10 years) and may even reduce the risk (age 50-59) CVD prevention is not an indication for estrogen treatment menopause related rise in LDL-C occurs Long term HRT use associated with less accumulation of coronary artery calcium and reduced CHD risk and mortality Risk factors (HTN, DM) and lifestyle choices play a role
50 Effect of hormone replacement therapy on cardiovascular events in recently postmenopausal women: randomized trial Conclusion After 10 years of randomized treatment, women receiving hormone replacement therapy early after menopause had a significantly reduced risk of mortality, heart failure, or myocardial infarction, without any apparent increase in risk of cancer, venous thromboembolism, or stroke. Schierbeck et al BMJ 2012;345.
51 Colon cancer associated with other GI diseases (polyps, IBS) and high fat/low fiber diet Decreased risk of colon cancer in E+P treated patients Offer routine screenings GI Diseases Gallbladder disease 2x as frequent in women HRT and OCs increase risk for gallstones with E+P more risk than Estrogen alone and oral HRT has greater risk than transdermal
52 Diabetes Mellitus Glucose metabolism worsens with weight gain and aging Hormonal changes at menopause may contribute to worsening glucose metabolism (relative increase in cortisol) and HT may reduce new onset DM though not approved as prevention More risk of CVD in women with DM; statin tx recommended for age Screening for DM in women age 45 or older (HbA1c, fasting glucose) 52
53 HT and Cognition evidence mixed on effect of HT on cognition at time of menopause but overall no negative effects not recommended at any age for prevention or treatment may increase dementia if begun after age 65 53
54 Hormonal Therapy
55 HRT guidelines Therapeutic goal is lowest effective estrogen dose consistent with individual treatment goals, benefits, and risks plus corresponding low progestogen dose for women with a uterus Lower doses may be better tolerated and have a more favorable benefit-risk ratio than standard doses
56 HT Benefits May reduce total mortality when initiated soon after menopause (<10 years); ET and EPT may reduce mortality by 30% in those <60 Women > 60 who had natural menopause at the median age and never used HT should not start without compelling indication/counseling No clear indication that longer HT duration improves or worsens the benefit-risk ratio in postmenopausal women
57 HT in premature/surgical menopause patients Use of HT or COC s for hormone replacement recommended until median age of menopause women under age 50 likely have smaller risks and greater benefits than women over 50 for same estrogen replacement 57
58 HT and Venous Thromboembolism Oral E+P increases risk 2-5 times and ET up to 1.5 times in postmenopausal women Risk emerges soon after therapy began (1-2 years) and decreases over time Possible lower risk with transdermal than oral and lower doses may be safer but no randomized controlled evidence for either synthetic progestins may increase risk compared to natural progesterone
59 Venous Thromboembolism risk baseline risk increases with age BMI >30 increases risk 3 fold other risk factors include immobilization, CVD, thrombophilic disorders, prothrombotic mutations, etc this is a coagulation event 59
60 Rx Hormone therapy options oral contraceptives estrogen progesterone estrogen/progesterone agonists/antagonists androgens 60
61 E/P Contraceptives safe option for healthy, lean, non-smoking women in midlife include OC s, patch and ring all other usual contraindications apply to patient selection have non-contraceptive benefits which can be important at peri-menopause 61
62 Progesterone contraceptives DepoProvera - may be used to treat irregular bleeding; has concerns for BMD Levonorgestrel IUD s may also be used for contraception, menorrhagia or off label use when taking estrogen Progesterone only oral contraceptive may be used when combined estrogen/progesterone pills are contraindicated 62
63 Estrogen approved treatment for menopause related symptoms estrogen alone appropriate for women with a hysterectomy can be prescribed for those with intolerance to progesterone and still have a uterus with close surveillance all routes of administration equally treat symptoms (pill, patch, topical, vaginal) 63
64 Progesterone Primary menopause related indication for progesterone is endometrial protection from systemic estrogen with multiple regimens approved Cyclic oral progesterone to create regular withdraw cycles or daily for continuous suppression Micronized progesterone may help with symptoms and can benefit sleep Over the counter not adequate for endometrial protection
65 Estrogen/Progestogen Individualization of therapy for each patient is key incorporating quality of life and risk factors (pills and patches) Duration of therapy more limited with EPT (5 years) than ET (7 years) women with premature/early menopause can use until average age of menopause then apply risks/benefits to consider extended therapy ACOG does not recommend routine discontinuation based on age 65
66 Discontinuation of ET/EPT 50% chance of vasomotor symptoms returning when therapy is stopped no difference if stops abruptly or tapers individualize decision 66
67 Estrogen agonists/antagonists raloxifene/evista - prevention and treatment of osteoporosis Conjugated estrogen/bazedoxifene (Duavee) for hot flashes and prevention of bone loss Tamoxifen approved as treatment for breast cancer and prevention of breast cancer in high risk women 67
68 Testosterone Ovaries account for a small portion of circulating testosterone and the post-menopausal ovary continues to produce testosterone The level declines as a function of age and in our 40 s is half of what it was in our 20 s After menopause there is no continued decline from the ovary! Endogenous levels are not directly linked to sexual function; no normal physiologic range or threshold for insufficiency is established in postmenopausal women No recommended testing of levels for treatment guidance
69 Testosterone therapy In post-menopausal women replacement has been shown to improve desire, responsiveness and frequency in those with sexual dysfunction May be considered when patient has sexual concerns not improved with estrogen Only US approved product for women is Estratest (generic); not testosterone alone Injections, compounded topical and subcutaneous implants available for off label use blood levels should be kept in physiologic range for reproductive age women and patient monitored for side effects
70 Bioidentical hormone therapy Defined as compounds that have exactly the same chemical and molecular structure as hormones that are produced in the human body There are prescriptive and compounded bioidenticals There is no data for a difference in safety Compounded not FDA approved No reliable testing of levels (including salivary)
71 Resources - the north american menopause society website has information for providers and patients, including updated position statements on the prominent topics in menopause management - free information and publications information on osteoporosis and link to FRAX calculator (also at ACOG.org
Learning Objectives. Peri menopause. Menopause Overview. Recommendation grading categories
 Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Menopause Symptoms and Management: After Breast Cancer
 Menopause Symptoms and Management: After Breast Cancer An Educational Webinar for Patients and their Caregivers Wen Shen, MD, MPH Division of Gynecologic Specialties July 27, 2018 1 Disclosure I have a
Menopause Symptoms and Management: After Breast Cancer An Educational Webinar for Patients and their Caregivers Wen Shen, MD, MPH Division of Gynecologic Specialties July 27, 2018 1 Disclosure I have a
North American Menopause Society (NAMS)
") North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
A Practitioner s Toolkit for the Management of the Menopause
 Medicine, Nursing and Health Sciences A Practitioner s Toolkit for the Management of the Menopause Developed by the Women s Health Research Program School of Public Health and Preventive Medicine Monash
Medicine, Nursing and Health Sciences A Practitioner s Toolkit for the Management of the Menopause Developed by the Women s Health Research Program School of Public Health and Preventive Medicine Monash
Women s Health: Managing Menopause. Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School
 Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Managing menopause in Primary Care and recent advances in HRT
 Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG Consultant Gynaecologist Heart of England NHS Foundation Trust rajsaha1@yahoo.co.uk Content of today s talk Aims
Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG Consultant Gynaecologist Heart of England NHS Foundation Trust rajsaha1@yahoo.co.uk Content of today s talk Aims
Post-menopausal hormone replacement therapy. Evan Klass, MD May 17, 2018
 Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
SERMS, Hormone Therapy and Calcitonin
 SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK
 2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK WHI the only large, long-term RCT of HT in women aged 50 to 79 years, Drug trail
2017 Position Statement of Hormone Therapy of NAMS: overview SHELAGH LARSON, MS, RNC WHNP, NCMP ACCLAIM, JPS HEALTH NETWORK WHI the only large, long-term RCT of HT in women aged 50 to 79 years, Drug trail
Menopausal Management: What Has Changed?
 Menopausal Management: What Has Changed? Julia V. Johnson, M.D. Professor and Chair, OB/GYN University of Massachusetts Medical School UMass Memorial Medical Center Conflicts of Interest None Learning
Menopausal Management: What Has Changed? Julia V. Johnson, M.D. Professor and Chair, OB/GYN University of Massachusetts Medical School UMass Memorial Medical Center Conflicts of Interest None Learning
OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc.
 OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc. Napa, California IMPORTANT SAFETY INFORMATION ABOUT EVAMIST: WARNING: ENDOMETRIAL CANCER,
OB/GYN Update: Menopausal Management What Does The Evidence Show? Rebecca Levy-Gantt D.O. PremierObGyn Napa Inc. Napa, California IMPORTANT SAFETY INFORMATION ABOUT EVAMIST: WARNING: ENDOMETRIAL CANCER,
HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer
 HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer -- PART 1 -- Definitions HRT hormone replacement therapy HT genome therapy ERT estrogen replacement therapy ET estrogen EPT estrogen progesterone therapy
HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer -- PART 1 -- Definitions HRT hormone replacement therapy HT genome therapy ERT estrogen replacement therapy ET estrogen EPT estrogen progesterone therapy
HRT in Perimenopausal Women. Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College
 HRT in Perimenopausal Women Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College 1 This is the Change But the CHANGE is not a disease 2 Introduction With a marked increase in longevity, women now
HRT in Perimenopausal Women Dr. Rubina Yasmin Asst. Prof. Medicine Dhaka Dental College 1 This is the Change But the CHANGE is not a disease 2 Introduction With a marked increase in longevity, women now
MENOPAUSAL HORMONE THERAPY 2016
 MENOPAUSAL HORMONE THERAPY 2016 Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA NICE provides the National Health Service advice on effective, good value healthcare.
MENOPAUSAL HORMONE THERAPY 2016 Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA NICE provides the National Health Service advice on effective, good value healthcare.
HRT & Menopause Where Do We Stand Now?
 HRT & Menopause Where Do We Stand Now? Mrs. SY Hussain Consultant Gynaecologist The Holly Private Hospital Spire Roding Hospital The Wellington Hospital Discussion Points Discuss Recommendations made by
HRT & Menopause Where Do We Stand Now? Mrs. SY Hussain Consultant Gynaecologist The Holly Private Hospital Spire Roding Hospital The Wellington Hospital Discussion Points Discuss Recommendations made by
GERIATRICS: definitions
 Caring For The Modern Menopausal Woman in 2016: An Update on Women s Health In the Geriatric Population David J Boes, DO, FACOOG MSU-COM May 2016 What defines the geriatric population???? GERIATRICS: definitions
Caring For The Modern Menopausal Woman in 2016: An Update on Women s Health In the Geriatric Population David J Boes, DO, FACOOG MSU-COM May 2016 What defines the geriatric population???? GERIATRICS: definitions
Menopause management NICE Implementation
 Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
Menopause management NICE Implementation Dr Paula Briggs Consultant in Sexual & Reproductive Health Southport and Ormskirk NHS Hospital Trust Why a NICE guideline (NG 23) Media reports about HRT have not
MENOPAUSE. I have no disclosures 10/11/18 OBJECTIVES WHAT S NEW? WHAT S SAFE?
 MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
06-Mar-17. Premature menopause. Menopause. Premature menopause. Menstrual cycle oestradiol. Premature menopause. Prevalence ~1% Higher incidence:
 Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
PERIMENOPAUSE. Objectives. Disclosure. The Perimenopause Perimenopause Menopause. Definitions of Menopausal Transition: STRAW.
 PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
PERIMENOPAUSE Patricia J. Sulak, MD Founder, Living WELL Aware LLC Author, Should I Fire My Doctor? Author, Living WELL Aware: Eleven Essential Elements to Health and Happiness Endowed Professor Texas
UPDATE: Women s Health Issues
 UPDATE: Women s Health Issues Renee B. Alexis, MD, MBA, MPH, FACOG Associate Professor Department of OBGYN Kiran C. Patel College of Osteopathic Medicine Disclosure of Conflicts of Interest I have no financial
UPDATE: Women s Health Issues Renee B. Alexis, MD, MBA, MPH, FACOG Associate Professor Department of OBGYN Kiran C. Patel College of Osteopathic Medicine Disclosure of Conflicts of Interest I have no financial
Managing menopause in Primary Care and recent advances in HRT
 Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG PG Cert. Advanced Gynaecology Endoscopy Consultant Gynaecologist Heart of England NHS Foundation Trust Spire Parkway
Managing menopause in Primary Care and recent advances in HRT Raj Saha, MD, DMRT, FRCOG PG Cert. Advanced Gynaecology Endoscopy Consultant Gynaecologist Heart of England NHS Foundation Trust Spire Parkway
OVERVIEW OF MENOPAUSE
 OVERVIEW OF MENOPAUSE Nicole Budrys, MD, MPH Reproductive Endocrinology Michigan Center for Fertility and Women s Health Presented at SEMCME March 13,2019 Objectives Define menopause Etiology of menopause
OVERVIEW OF MENOPAUSE Nicole Budrys, MD, MPH Reproductive Endocrinology Michigan Center for Fertility and Women s Health Presented at SEMCME March 13,2019 Objectives Define menopause Etiology of menopause
CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology
 CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology A 49-year-old woman complains of irregular menses over the past 6 months, feelings of inadequacy, vaginal dryness, difficulty sleeping, and episodes
CASE 4- Toy et al. CASE FILES: Obstetrics & Gynecology A 49-year-old woman complains of irregular menses over the past 6 months, feelings of inadequacy, vaginal dryness, difficulty sleeping, and episodes
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
What's New in Menopause Management
 Annual Review of Family Medicine December 10, 2015 San Francisco, CA What's New in Menopause Management Michael Policar, MD, MPH Clinical Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine
Annual Review of Family Medicine December 10, 2015 San Francisco, CA What's New in Menopause Management Michael Policar, MD, MPH Clinical Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine
Menopause and HRT. John Smiddy and Alistair Ledsam
 Menopause and HRT John Smiddy and Alistair Ledsam Menopause The cessation of menstruation Diagnosed retrospectively after 1 year of amenorrhoea Average age 51 in the UK Normal physiology - Menstruation
Menopause and HRT John Smiddy and Alistair Ledsam Menopause The cessation of menstruation Diagnosed retrospectively after 1 year of amenorrhoea Average age 51 in the UK Normal physiology - Menstruation
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Topics. Periods Menopause & HRT Contraception Vulva problems
 Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Girls stuff Topics Periods Menopause & HRT Contraception Vulva problems Menorrhagia Excessive menstrual loss occurring with regular or irregular cycles Ovulatory Anovulatory Usual blood loss 30-40ml per
Menopause and Post Gynecological Reproductive Care
 Menopause and Post Gynecological Reproductive Care Nguyet-Cam Vu Lam, MD, FAAFP Associate Program Director St. Luke s Family Medicine Residency 1 Disclosure Dr. Nguyet-Cam Vu Lam has no conflict of interest,
Menopause and Post Gynecological Reproductive Care Nguyet-Cam Vu Lam, MD, FAAFP Associate Program Director St. Luke s Family Medicine Residency 1 Disclosure Dr. Nguyet-Cam Vu Lam has no conflict of interest,
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
Menopausal Symptoms The Who: Hot flashes are reported by as many as 75% of perimenopausal women in the U.S.
 Menopausal Hormone Therapy: The Who, What, Where, When and Why Laurie Birkholz, MD, NCMP Knowledge of Clinical Trials Regarding Hormone Therapy and Likelihood of Prescribing Hormone Objective: The aim
Menopausal Hormone Therapy: The Who, What, Where, When and Why Laurie Birkholz, MD, NCMP Knowledge of Clinical Trials Regarding Hormone Therapy and Likelihood of Prescribing Hormone Objective: The aim
Prior disclosures past 3 years Consultant for Pfizer University of Virginia received Grants/research support from TherapeuticsMD
 Prior disclosures past 3 years Consultant for Pfizer University of Virginia received Grants/research support from TherapeuticsMD JoAnn V. Pinkerton, MD Professor of Obstetrics and Gynecology Director,
Prior disclosures past 3 years Consultant for Pfizer University of Virginia received Grants/research support from TherapeuticsMD JoAnn V. Pinkerton, MD Professor of Obstetrics and Gynecology Director,
Management of Menopausal Symptoms
 Management of Menopausal Symptoms Tammie Koehler DO, FACOG 1 Menopause Permanent cessation of menstruation that occurs after the loss of ovarian activity Determined to have occurred after 1 full year of
Management of Menopausal Symptoms Tammie Koehler DO, FACOG 1 Menopause Permanent cessation of menstruation that occurs after the loss of ovarian activity Determined to have occurred after 1 full year of
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Vol-5 No-1 Jan-Mar 2012
 "Women's Health" is also available at www.squarepharma.com.bd Editorial Board Dr. Omar Akramur Rab MBBS, FCGP, FIAGP Mohammad Hanif M. Pharm, MBA A.H.M. Rashidul Bari M. Pharm, MBA Executive Editor Chowdhury
"Women's Health" is also available at www.squarepharma.com.bd Editorial Board Dr. Omar Akramur Rab MBBS, FCGP, FIAGP Mohammad Hanif M. Pharm, MBA A.H.M. Rashidul Bari M. Pharm, MBA Executive Editor Chowdhury
Appendix: Reference Table of HT Brand Names
 Appendix: Reference Table of HT Brand Names This is a full reference table in alphabetical order, of Brand Name drugs used in HT. It is the basis for prescription advice throughout this handbook. Drug
Appendix: Reference Table of HT Brand Names This is a full reference table in alphabetical order, of Brand Name drugs used in HT. It is the basis for prescription advice throughout this handbook. Drug
Menopause & HRT. Matt McKenna Elliot Davis
 Menopause & HRT Matt McKenna Elliot Davis Menopause Before age 40: Premature Menopause After 12 months clinical diagnosis made Depletion of Ovarian Follicles Oestrogen Progesterone LH FSH Spontaneous Amemorrhoea
Menopause & HRT Matt McKenna Elliot Davis Menopause Before age 40: Premature Menopause After 12 months clinical diagnosis made Depletion of Ovarian Follicles Oestrogen Progesterone LH FSH Spontaneous Amemorrhoea
What in the HRT do we do now? Selecting, managing and maintaining patients on hormone therapy.
 What in the HRT do we do now? Selecting, managing and maintaining patients on hormone therapy. KELLIE FLOOD-SHAFFER, MD, FACOG ASSOCIATE PROFESSOR UNTHSC-DEPARTMENT OF OB/GYN . I have no conflicts of interest
What in the HRT do we do now? Selecting, managing and maintaining patients on hormone therapy. KELLIE FLOOD-SHAFFER, MD, FACOG ASSOCIATE PROFESSOR UNTHSC-DEPARTMENT OF OB/GYN . I have no conflicts of interest
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
Menopause & HRT. Rosie & Alex. Image:
 Menopause & HRT Rosie & Alex Image: http://www.keepcalm-o-matic.co.uk/ Menopause The permanent cessation of menstruation for 12 months When does it happen? Average age 51 Image: Nature Medicine - 12, 612-613
Menopause & HRT Rosie & Alex Image: http://www.keepcalm-o-matic.co.uk/ Menopause The permanent cessation of menstruation for 12 months When does it happen? Average age 51 Image: Nature Medicine - 12, 612-613
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Menopausal Symptoms. Hormone Therapy Products Available in Canada for the Treatment of. Physician Desk Reference - 3rd Edition
 Hormone Therapy Products Available in Canada for the Treatment of Menopausal Symptoms Physician Desk Reference - 3rd Edition A clinical resource provided to you by: The Society of Obstetricians and Gynaecologists
Hormone Therapy Products Available in Canada for the Treatment of Menopausal Symptoms Physician Desk Reference - 3rd Edition A clinical resource provided to you by: The Society of Obstetricians and Gynaecologists
Pearls for Menopause Management: I m ready: now what?
 Pearls for Menopause Management: I m ready: now what? Friday November 13, 2015 Susan Goldstein MD CCFP FCFP NCMP Assistant Professor Department of Family and Community Medicine University of Toronto Menarche
Pearls for Menopause Management: I m ready: now what? Friday November 13, 2015 Susan Goldstein MD CCFP FCFP NCMP Assistant Professor Department of Family and Community Medicine University of Toronto Menarche
Current Topics in Hormone Replacement Therapy
 Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
Current Topics in Hormone Replacement Therapy Corey R. Babb, D.O., FACOOG, IF, NCMP Clinical Assistant Professor of Obstetrics and Gynecology Director of the Oklahoma State University Center for Women
WHI Estrogen--Progestin vs. Placebo (Women with intact uterus)
") HORMONE REPLACEMENT THERAPY In the historical period it was commonly held that estrogen had two principal benefits to postmenopausal women: 1) To alleviate the constitutional symptoms related to the climacteric
HORMONE REPLACEMENT THERAPY In the historical period it was commonly held that estrogen had two principal benefits to postmenopausal women: 1) To alleviate the constitutional symptoms related to the climacteric
Menopause - a summary of management
 Page 1 of 5 Menopause - a summary of management Original article by: May Su Resources Menopause treatment algorithm The Jean Hales Foundation for women's heath. Menopause, a treatment algorithm. (Australian
Page 1 of 5 Menopause - a summary of management Original article by: May Su Resources Menopause treatment algorithm The Jean Hales Foundation for women's heath. Menopause, a treatment algorithm. (Australian
22/09/2014. Menopause Management. Menopause. Menopause symptoms
 Menopause Management Dr Sonia Davison Jean Hailes for Women s Health Menopause Time of last menstrual period - average age 51 Premature Menopause: occurs before age 40 Perimenopause (menopause transition):
Menopause Management Dr Sonia Davison Jean Hailes for Women s Health Menopause Time of last menstrual period - average age 51 Premature Menopause: occurs before age 40 Perimenopause (menopause transition):
This includes bone loss, endometrial cancer, and vasomotor symptoms.
 Hello and welcome. My name is Chad Barnett. I m a Clinical Pharmacy Specialist in the Division of Pharmacy at the University of Texas, MD Anderson Cancer Center and I m very pleased today to be able to
Hello and welcome. My name is Chad Barnett. I m a Clinical Pharmacy Specialist in the Division of Pharmacy at the University of Texas, MD Anderson Cancer Center and I m very pleased today to be able to
Menopause: diagnosis and management NICE guideline NG23. Published November 2015
 Menopause: diagnosis and management NICE guideline NG23 Published November 2015 1 Full title: Menopause : diagnosis and management Available at: http://www.nice.org.uk/guidance/ng23 Guideline published
Menopause: diagnosis and management NICE guideline NG23 Published November 2015 1 Full title: Menopause : diagnosis and management Available at: http://www.nice.org.uk/guidance/ng23 Guideline published
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Case Presentation. Learning Objectives. Case Presentation. Case Presentation
 Learning Objectives To apply up to date information about the natural history of menopause to improve the care of individual women To counsel women about the risks and benefits of systemic hormone therapy
Learning Objectives To apply up to date information about the natural history of menopause to improve the care of individual women To counsel women about the risks and benefits of systemic hormone therapy
By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University
 By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University Cessation of menstruation as a result of the aging process of or surgical removal of the ovaries; change
By J. Jayasutha Lecturer Department of Pharmacy Practice SRM College of Pharmacy SRM University Cessation of menstruation as a result of the aging process of or surgical removal of the ovaries; change
Women s Health: Take Home Messages
 Women s Health: Take Home Messages Caren Solomon, MD Associate Physician, BWH Associate Professor of Medicine, HMS Deputy Editor, NEJM No disclosures Contraception Contraceptive Effectiveness Rates of
Women s Health: Take Home Messages Caren Solomon, MD Associate Physician, BWH Associate Professor of Medicine, HMS Deputy Editor, NEJM No disclosures Contraception Contraceptive Effectiveness Rates of
OSTEOPOROSIS: PREVENTION AND MANAGEMENT
 OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
OSTEOPOROSIS: OVERVIEW OSTEOPOROSIS: PREVENTION AND MANAGEMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Key Risk factors Screening and Monitoring
Benton Franklin County Medical Society 31st Annual CME Seminar
 Management of Current HT/ET and SERM Recommendations Benton Franklin County Medical Society 31st Annual CME Seminar February 21, 2015 Kennewick, Washington Spokane steoporosis Dr. Lynn Kohlmeier Lynn Kohlmeier,
Management of Current HT/ET and SERM Recommendations Benton Franklin County Medical Society 31st Annual CME Seminar February 21, 2015 Kennewick, Washington Spokane steoporosis Dr. Lynn Kohlmeier Lynn Kohlmeier,
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Aromatase Inhibitors & Osteoporosis
 Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
Page 1
 Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Osteoporosis Osteoporosis is a condition characterised by weakened bones that fracture easily. After menopause many women are at risk of developing osteoporosis. Peak bone mass is usually reached during
Englewood Orthopedic Associates 401 South Van Brunt Street Englewood, NJ Tel: Fax: Jessica Fleischer, MD
 Englewood Orthopedic Associates 401 South Van Brunt Street Englewood, NJ 07631 Tel: 201.569.2770 Fax: 201.569.1774 Jessica Fleischer, MD Date: Name: Address: City: State: Zip Code: Age: DOB: / / Gender:
Englewood Orthopedic Associates 401 South Van Brunt Street Englewood, NJ 07631 Tel: 201.569.2770 Fax: 201.569.1774 Jessica Fleischer, MD Date: Name: Address: City: State: Zip Code: Age: DOB: / / Gender:
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
DINE AND LEARN ENDOCRINOLOGY PEARLS. Dr. Priya Manjoo, MD, FRCPC Endocrinology, Victoria, BC
 DINE AND LEARN ENDOCRINOLOGY PEARLS Dr. Priya Manjoo, MD, FRCPC Endocrinology, Victoria, BC OUTLINE HRT and CVD HRT and Breast Cancer Osteoporosis When to treat How long to treat for Bisphosphonates BMD
DINE AND LEARN ENDOCRINOLOGY PEARLS Dr. Priya Manjoo, MD, FRCPC Endocrinology, Victoria, BC OUTLINE HRT and CVD HRT and Breast Cancer Osteoporosis When to treat How long to treat for Bisphosphonates BMD
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
COPING A newsletter from COPN December 23, 2010 Remember: You can live well with osteoporosis!
 COPING A newsletter from COPN December 23, 2010 Remember: You can live well with osteoporosis! SEASONS GREETINGS! This issue of COPING draws to a close our series of articles on the 2010 Clinical Practice
COPING A newsletter from COPN December 23, 2010 Remember: You can live well with osteoporosis! SEASONS GREETINGS! This issue of COPING draws to a close our series of articles on the 2010 Clinical Practice
Abnormal Uterine Bleeding Case Studies
 Case Study 1 Abnormal Uterine Bleeding Case Studies Abigail, a 24 year old female, presents to your office complaining that her menstrual cycles have become a problem. They are now lasting 6 7 days instead
Case Study 1 Abnormal Uterine Bleeding Case Studies Abigail, a 24 year old female, presents to your office complaining that her menstrual cycles have become a problem. They are now lasting 6 7 days instead
The Estrogen Question
 The Estrogen Question Hormone Therapy still offers the best relief for menopausal symptoms. Is it right for you? When 49-year-old Lee Ann Dodson heard the news that the Women's Health Initiative (WHI)
The Estrogen Question Hormone Therapy still offers the best relief for menopausal symptoms. Is it right for you? When 49-year-old Lee Ann Dodson heard the news that the Women's Health Initiative (WHI)
Osteoporosis. Definition
 Osteoporosis Definition Osteoporosis causes bones to become weak and brittle so brittle that a fall or even mild stresses like bending over or coughing can cause a fracture. Osteoporosis-related fractures
Osteoporosis Definition Osteoporosis causes bones to become weak and brittle so brittle that a fall or even mild stresses like bending over or coughing can cause a fracture. Osteoporosis-related fractures
MENOPAUSE. Women in Midlife: Menopause & Osteoporosis. Outline for Menopause. STRAW Stages of the Menopausal Transition-NAMS, /29/2012
 Women in Midlife: Menopause & Osteoporosis Lisa Ward, MD, MScPH, MS UCSF CME Conference March 23rd, 2012 MENOPAUSE Outline for Menopause Definitions Summary of the Evidence Current Guidelines Management
Women in Midlife: Menopause & Osteoporosis Lisa Ward, MD, MScPH, MS UCSF CME Conference March 23rd, 2012 MENOPAUSE Outline for Menopause Definitions Summary of the Evidence Current Guidelines Management
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Update in Women s Health Year In Review
 Update in Women s Health Year In Review Judith Walsh MD, MPH Professor of Medicine Division of General Internal Medicine And Epidemiology and Biostatistics I have no disclosures Disclosures 1 Plan for
Update in Women s Health Year In Review Judith Walsh MD, MPH Professor of Medicine Division of General Internal Medicine And Epidemiology and Biostatistics I have no disclosures Disclosures 1 Plan for
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Beyond the Break. After Breast Cancer: Osteoporosis in Survivorship. Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO
 FCFP Regional Primary Care Lead CCO") Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Ms. Y. Outline. Updates of SERMs and Estrogen
 Ms. Y Updates of SERMs and Estrogen Steven R. Cummings, MD, FACP San Francisco Coordinating Center CPMC Research Institute and UCSF Support from Lilly, Pfizer, Berlex 55 y.o. woman with mild hypertension
Ms. Y Updates of SERMs and Estrogen Steven R. Cummings, MD, FACP San Francisco Coordinating Center CPMC Research Institute and UCSF Support from Lilly, Pfizer, Berlex 55 y.o. woman with mild hypertension
Real life issues & answers: The hormonal patient Defining best practice, 5 key issues & case study
 Real life issues & answers: The hormonal patient Defining best practice, 5 key issues & case study Dr Louise Newson BSc(Hons) MBChB(Hons) MRCP FRCGP www.menopausedoctor.co.uk Case Number 1 - Claire Age
Real life issues & answers: The hormonal patient Defining best practice, 5 key issues & case study Dr Louise Newson BSc(Hons) MBChB(Hons) MRCP FRCGP www.menopausedoctor.co.uk Case Number 1 - Claire Age
Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D
 Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D Menopause and Cancer How does menopause affect a woman s cancer risk? Ø Menopause does not cause cancer.but risk of developing
Menopause and Cancer risk; What to do overcome the risks? Fatih DURMUŞOĞLU,M.D Menopause and Cancer How does menopause affect a woman s cancer risk? Ø Menopause does not cause cancer.but risk of developing
Practical recommendations for hormone replacement therapy in the peri- and postmenopause
 CLIMACTERIC 2004;7:in press Practical recommendations for hormone replacement therapy in the peri- and postmenopause Recommendations from an Expert Workshop, February 2004 Henry Burger, Australia; David
CLIMACTERIC 2004;7:in press Practical recommendations for hormone replacement therapy in the peri- and postmenopause Recommendations from an Expert Workshop, February 2004 Henry Burger, Australia; David
Pharmacology Update: Menopause and Hormone Therapy North American Menopause Society Meeting Disclosure
 Pharmacology Update: Menopause and Hormone Therapy North American Menopause Society Meeting 2015 Disclosure The faculty and planners for this activity, as well as the CME staff, do not have any relevant
Pharmacology Update: Menopause and Hormone Therapy North American Menopause Society Meeting 2015 Disclosure The faculty and planners for this activity, as well as the CME staff, do not have any relevant
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
Proactive Health Management for Women in High Stress Careers April 4, Eirwen M. Miller, MD Division of Gynecologic Oncology
 Proactive Health Management for Women in High Stress Careers April 4, 2018 Eirwen M. Miller, MD Division of Gynecologic Oncology 1 Annual Well-Woman Care Blood pressure Weight Physical exam (including
Proactive Health Management for Women in High Stress Careers April 4, 2018 Eirwen M. Miller, MD Division of Gynecologic Oncology 1 Annual Well-Woman Care Blood pressure Weight Physical exam (including
Long term Sequelae in Natural and Surgical Menopause
 Long term Sequelae in Natural and Surgical Menopause 2 OBJECTIVE Strategies to prevent long term consequences 3 EXPECTED OUTCOME a) Understanding long term problems b) Understanding preventive strategies
Long term Sequelae in Natural and Surgical Menopause 2 OBJECTIVE Strategies to prevent long term consequences 3 EXPECTED OUTCOME a) Understanding long term problems b) Understanding preventive strategies
Before you prescribe
 Initiating hormone replacement therapy (HRT) / menopausal hormone therapy (MHT) Dr Sonia Davison Jean Hailes Consultant Endocrinologist Before you prescribe Ensure there are no contraindications to HRT/MHT
Initiating hormone replacement therapy (HRT) / menopausal hormone therapy (MHT) Dr Sonia Davison Jean Hailes Consultant Endocrinologist Before you prescribe Ensure there are no contraindications to HRT/MHT
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Southern California Center for Sexual Health and Survivorship Medicine Inc, Newport Beach, CA 3
 The WISDOM survey: Physicians Level of Comfort Prescribing Treatment for Vulvar and Vaginal Atrophy (VVA) Symptoms in Women with a Predisposition or History of Breast Cancer Lisa Larkin, MD 1 ; Michael
The WISDOM survey: Physicians Level of Comfort Prescribing Treatment for Vulvar and Vaginal Atrophy (VVA) Symptoms in Women with a Predisposition or History of Breast Cancer Lisa Larkin, MD 1 ; Michael
Guidelines for Menopause Management
 Guidelines for Menopause Management Judith M.E. Walsh, MD, MPH Professor of Medicine UCSF Women s Health Center of Excellence Conflicts of Interest: None Overview Natural history of menopause Hormone therapy:
Guidelines for Menopause Management Judith M.E. Walsh, MD, MPH Professor of Medicine UCSF Women s Health Center of Excellence Conflicts of Interest: None Overview Natural history of menopause Hormone therapy:
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Orals,Transdermals, and Other Estrogens in the Perimenopause
 Orals,Transdermals, and Other Estrogens in the Perimenopause Cases Denise Black, MD, FRCSC Assistant Professor, Obstetrics, Gynecology and Reproductive Sciences University of Manitoba 6/4/18 197 Faculty/Presenter
Orals,Transdermals, and Other Estrogens in the Perimenopause Cases Denise Black, MD, FRCSC Assistant Professor, Obstetrics, Gynecology and Reproductive Sciences University of Manitoba 6/4/18 197 Faculty/Presenter
11/15/2017. Update on HRT. Highgate Private Hospital (Barnet Hospital) Women s Health. Menopause
 Women s Health. Menopause") Update on HRT Miss Moneli Golara Consultant Obstetrician and Gynaecologist MBBS, FRCOG Highgate Private Hospital (Barnet Hospital) E: lauren@medicaladministration.co.uk Women s Health Life expectancy of
Update on HRT Miss Moneli Golara Consultant Obstetrician and Gynaecologist MBBS, FRCOG Highgate Private Hospital (Barnet Hospital) E: lauren@medicaladministration.co.uk Women s Health Life expectancy of
Dr. Mojibian. Menopause
 Dr. Mojibian Menopause I. Introduction - The term menopause is derived from Greek Meno (months) and pause (cessation). The word means cessation of menstruation. - Cliamacteric which is by dictionary definition
Dr. Mojibian Menopause I. Introduction - The term menopause is derived from Greek Meno (months) and pause (cessation). The word means cessation of menstruation. - Cliamacteric which is by dictionary definition
AusPharm CE Hormone therapy 23/09/10. Hormone therapy
 Hormone therapy Learning objectives: Assess options to address quality of life and health concerns of menopausal women Outline indications for hormone therapy Counsel women on the risks and benefits of
Hormone therapy Learning objectives: Assess options to address quality of life and health concerns of menopausal women Outline indications for hormone therapy Counsel women on the risks and benefits of
HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D
 HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D All of the hormones in your body are designed to work together. This is God s plan. Therefore, if one is altered, or deficient, it will affect the actions
HORMONES AND YOUR HEALTH Charlie Tucker Pharm. D All of the hormones in your body are designed to work together. This is God s plan. Therefore, if one is altered, or deficient, it will affect the actions
Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Osteoporosis/Fracture Prevention Clinician Guide SEPTEMBER 2017 Introduction This Clinician Guide was developed to assist Primary Care physicians
Outline. Estrogens and SERMS The forgotten few! How Does Estrogen Work in Bone? Its Complex!!! 6/14/2013
 Outline Estrogens and SERMS The forgotten few! Clifford J Rosen MD rosenc@mmc.org Physiology of Estrogen and estrogen receptors Actions of estrogen on bone BMD, fracture, other off target effects Cohort
Outline Estrogens and SERMS The forgotten few! Clifford J Rosen MD rosenc@mmc.org Physiology of Estrogen and estrogen receptors Actions of estrogen on bone BMD, fracture, other off target effects Cohort
Summary of the risk management plan by product
 Summary of the risk management plan by product 1 Elements for summary tables in the EPAR 1.1 Summary table of Safety concerns Summary of safety concerns Important identified risks Important potential risks
Summary of the risk management plan by product 1 Elements for summary tables in the EPAR 1.1 Summary table of Safety concerns Summary of safety concerns Important identified risks Important potential risks
APPROACH TO THE MENOPAUSAL PATIENT & CURRENT MANAGEMENT of Menopausal Symptoms
 APPROACH TO THE MENOPAUSAL PATIENT & CURRENT MANAGEMENT of Menopausal Symptoms MOA AUTUMN CONFERENCE NOVEMBER 17, 2018 DAVID J BOES, DO, FACOOG BOES@MSU.EDU 1 DISCLOSURES NOTHING TO DISCLOSE RELATIVE TO
APPROACH TO THE MENOPAUSAL PATIENT & CURRENT MANAGEMENT of Menopausal Symptoms MOA AUTUMN CONFERENCE NOVEMBER 17, 2018 DAVID J BOES, DO, FACOOG BOES@MSU.EDU 1 DISCLOSURES NOTHING TO DISCLOSE RELATIVE TO
Because the low bone mass and deterioration
 OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics