ANCO s 2011 San Antonio Breast Cancer Symposium Highlights. Michael Alvarado, M.D. Disclosure
|
|
|
- Vincent Hodge
- 6 years ago
- Views:
Transcription
1 ANCO s 2011 San Antonio Breast Cancer Symposium Highlights Michael Alvarado, M.D. FACS Assistant Professor of Surgery UCSF Michael Alvarado, M.D. Disclosure Advisory Board Member Genomic Health DCIS Study Group 1
2 Selected Topics Contralateral Breast Cancer Risk BRCA Atypical Lesions and Future Risk Molecular Assay and DCIS Recurrence Risk of contralateral breast cancer in BRCA1/2 carriers compared to non BRCA1/2 carriers in a consecutive patient series Alexandra J van den Broek, Marjanka K Schmidt, Rob AEM Tollenaar, Laura J van 't Veer and Flora E van Leeuwen This presentation is the intellectual property of the author/presenter. Contact them at s.vd.broek@nki.nl for permission to reprint and/or distribute. 2
3 Contralateral breast cancer (CBC) risk 30 BRCA carriers 10- year C BC risk (%) General population Adami et al. Cancer 1985;55(3): Harvey et al. Natl Cancer Inst Monogr 1985;68: Liebens et al Eur J Cancer 2006 CBC risk in BRCA carriers: Gaps in knowledge CBC risk estimates in a large unselected population Interaction with non-genetic modifiers It is important to provide precise risk estimates of CBC and identify factors which predict the risk of CBC in this group of high risk women 3
4 Study population: BOSOM Breast cancer Outcome Study Of Mutation carriers Consecutive patient series Invasive breast cancer, n = 7495 Diagnosed < 50 years different hospitals throughout The Netherlands Clinico-pathological data: Medical files, Medical Registries and the Netherlands Cancer Registry n = 5065 with germline DNA Median follow-up time: 9.2 years BRCA mutation analysis Germline DNA: isolated from FFPE tissue blocks BRCA1/2 mutations: Allelic discrimination or Fragment length analyses, sequencing was used to confirm the mutations % of known pathogenic BRCA1/2 mutations in The Netherlands captured with our methods: BRCA1 BRCA2 Overall 78% 51% 70% 4
5 Cumulative risks of CBC Cumulative incidence curve accounting for competing risks KM- curve / Cox regression models overestimate the risk CIC- curves are modeled by Fine and Gray method All models adjusted for age at diagnosis BRCA mutation prevalence BOSOM cohort BRCA mutation status N % No mutation BRCA BRCA
6 CBC risk BRCA carriers * = P < 0.05 ** = P < Non-genetic modifiers which predict the risk of CBC in carriers Is it possible to define subgroups based on characteristics of the first BC? Age at diagnosis (<41 vs 41-50) Triple negative (TN) status (ER- & PR- & HER2- vs ER+ and/or PR+ and/or HER2+) 6
7 CBC risk noncarriers: age at diagnosis 6.6 P = ns 6.1 CBC risk BRCA carriers: age at diagnosis * = P <
8 Non-genetic modifiers which predict the risk of CBC in carriers Is it possible to define subgroups based on characteristics of the first BC? Age at diagnosis (<41 vs 41-50) Triple negative (TN) status (ER- & PR- & HER2- vs ER+ and/or PR+ and/or HER2+) CBC risk noncarriers: TN status P = ns
9 CBC risk BRCA carriers: TN status P = ns CBC risk in subgroups: non-carriers Age diagnosis first BC Receptor status first BC Total N # CBCs Cum 10- year risk 95% CI Non-carriers Non-TN <41 Non-TN TN <41 TN BRCA mutation carriers Non-TN <41 Non-TN TN <41 TN
10 CBC risk in subgroups: BRCA carriers Age diagnosis first BC Receptor status first BC Total N # CBCs Cum 10- year risk 95% CI Non-carriers Non-TN <41 Non-TN TN <41 TN BRCA mutation carriers Non-TN <41 Non-TN TN <41 TN CBC risk dependant on therapy first BC? Chemo- / hormonal therapy Total N # CBCs Cum 10- year risk 95% CI Total N # CBCs Cum 10- year risk 95% CI Non-carriers Carriers No Yes 2091* ** * Of which 632 (22 CBC) were treated with hormonal therapy ** Of which 11 (1 CBC) were treated with hormonal therapy Adjustment for therapy (chemo and/or hormonal) given for the first BC did not materially change the previous results 10
11 Conclusions BRCA carriers 10-year cumulative risk for CBC Non-carriers: 6% BRCA1 carriers: 20% BRCA2 carriers: 11% Subgroups of BRCA carriers: Low risk subgroup Patients with a non-tn first BC diagnosed between ages % Higher risk subgroups Patients with a TN first BC diagnosed between ages % Patients with a first BC diagnosed under age % Discussion / Future research Other adjustments did not change the results: - Year of diagnosis of the first BC - Therapy given for the first BC (Chemo- / hormonal therapy) Similar results as for TN-status are seen for ER-status Similar risk estimates seen in BRCA1 mutation carriers alone 11

12 Clinical relevance Improving personalized surveillance after BC Improving personalized treatment choices Contribution to the understanding of the etiology of BC If confirmed in other studies, age criteria and receptor-status of the first breast tumor may be included in guidelines for prophylactic measures and screening in the follow-up of BRCA1/2 mutation carriers San Antonio Breast Cancer Symposium December 6-10, 2011 Clarifying the Risk of Breast Cancer in Women with Atypical Breast Lesions SB Coopey, E Mazzola, JM Buckley, J Sharko, AK Belli, EMH Kim, F Polufriaginof, G Parmigiani, JE Garber, BL Smith, MA Gadd, MC Specht, AJ Guidi, CA Roche, KS Hughes Division of Surgical Oncology, Massachusetts General Hospital, Boston, MA; Department of Biostatistics & Computational Biology, Dana-Farber Cancer Institute, Boston, MA; Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA; Department of Pathology, Newton- Wellesley Hospital, Newton, MA 12
13 San Antonio Breast Cancer Symposium December 6-10, 2011 Certain pathologic diagnoses significantly increase breast cancer risk Atypical ductal hyperplasia (ADH) Atypical lobular hyperplasia (ALH) Lobular carcinoma in situ (LCIS) Borderline DCIS/Severe ADH Objectives Clarify level of risk by diagnosis Evaluate the efficacy of chemoprevention This presentation is the intellectual property of the author/presenter. Contact at for permission to reprint and/or distribute. Methods San Antonio Breast Cancer Symposium December 6-10, 2011 All electronically available pathology Mass General, Brigham & Women s, Newton Wellesley Natural Language Processing (Clearforest, Waltham, MA) Atypia diagnoses verified by human reader All women diagnosed with ADH, ALH, LCIS, or Borderline DCIS No prior or concurrent breast cancer Intact breasts Trumping order for maximum diagnosis Borderline DCIS > LCIS > ALH > ADH Use of chemoprevention agents identified by chart review Yes, No, Unknown Effect of chemoprevention analyzed from 1999 forward This presentation is the intellectual property of the author/presenter. Contact at for permission to reprint and/or distribute. 13

14 Results San Antonio Breast Cancer Symposium December 6-10, ,333 breast pathology reports 42, 950 individuals 2942 women with atypical breast lesions Mean Age Dx: 53 years (range: 19-93) Mean FU all: 66 months Borderline DCIS 12% ADH 41% LCIS 19% ALH 28% San Antonio Breast Cancer Symposium December 6-10, 2011 Estimated 5 and 10-Year Breast Cancer Risks Based on Atypia Type Atypia Type 5-Year Cancer Risk 10-Year Cancer Risk ADH (n=1199) 4.8% 14.8% Borderline (n=345) 7.1% 14.5% ALH (n=828) 9.4% 20.2% LCIS (n=570) 8.7% 16.3% This presentation is the intellectual property of the author/presenter. Contact at scoopey@partners.org for permission to reprint and/or distribute. 14
15 San Antonio Breast Cancer Symposium December 6-10, 2011 Breast Cancer Risk by Atypia Type No Chemoprevention (All years) Probability of Being Cancer Free 5-Year 10-Year ADH 4.5% 17.3% ALH 10.9% 20.7% LCIS 10.5% 23.7% Borderline 9.7% 26% *ADH at 5 years only significant difference Time from Atypia to Cancer (years) This presentation is the intellectual property of the author/presenter. Contact at scoopey@partners.org for permission to reprint and/or distribute. San Antonio Breast Cancer Symposium December 6-10, 2011 Laterality of Cancer No Chemoprevention (All years) Number of Cancers Ipsilateral Cancer Contralateral Cancer Bilateral Cancer Side Unknown Borderline(n=21) 47.6% 42.8% 4.8% 4.8% LCIS (n=45) 55.6% 37.8% 4.4% 2.2% ADH (n=57) 59.6% 38.6% 1.8% 0% ALH (n=61) 60.7% 37.7% 0% 1.6% Significantly more ipsilateral cancers for all atypia types combined (p<0.005) This presentation is the intellectual property of the author/presenter. Contact at scoopey@partners.org for permission to reprint and/or distribute. 15
16 San Antonio Breast Cancer Symposium December 6-10, 2011 Invasive vs. DCIS No Chemoprevention (All years) Number of Cancers Invasive Cancer Non-Invasive Cancer ADH (n=57) 47.4% 52.6% Borderline (n=21) 57.1% 42.9% ALH (n=61) 68.9% 31.1% LCIS (n=45) 71.1% 28.9% invasive vs non-invasive cancer ADH and Borderline: No significant difference ALH and LCIS: p<0.001 This presentation is the intellectual property of the author/presenter. Contact at for permission to reprint and/or distribute. San Antonio Breast Cancer Symposium December 6-10, 2011 Results: Chemoprevention 2460 patients 1999 and beyond 466 (18.9%) treated» Tamoxifen, raloxifene, and/or exemestane» Any duration 1472 (59.8%) patients not treated 522 (21.2%) patients with data unavailable This presentation is the intellectual property of the author/presenter. Contact at for permission to reprint and/or distribute. 16
17 San Antonio Breast Cancer Symposium December 6-10, 2011 Chemoprevention determined by atypia type 40.75% 33.42% 18.33% 18.45% Borderline LCIS ALH ADH 17 San Antonio Breast Cancer Symposium December 6-10, 2011 Probability of Cancer after Atypia Diagnosis With and Without Chemoprevention, 1999 and Beyond 4.1% Probability of Being Cancer Free 8.3% 7.5% 21.3% Chemoprevention Yes (n=466) No (n=1472) Time from Atypia to Cancer (years) (p<0.05) This presentation is the intellectual property of the author/presenter. Contact at for permission to reprint and/or distribute. 17
18 San Antonio Breast Cancer Symposium December 6-10, 2011 Chemoprevention Decreased Risk for all Atypia Types 1999 and Beyond 8.5% 19.9% 8.5% 18.7% ADH (p<0.05) ALH (p<0.05) 2.1% 10.3% 14.7% 10.3% Borderline (p<0.05) LCIS (p<0.05) 32.4% Conclusions San Antonio Breast Cancer Symposium December 6-10, 2011 ADH, ALH, LCIS, and Borderline DCIS increase a woman s risk of breast cancer to a similar amount Chemoprevention for all atypia types significantly reduces breast cancer risk at 5 and 10 years Increased use of chemoprevention for patients with atypia will significantly decrease cancer risk This data will be used to create a better model of breast cancer risk prediction based on atypia type and use of chemoprevention This presentation is the intellectual property of the author/presenter. Contact at scoopey@partners.org for permission to reprint and/or distribute. 18

19 A QUANTITATIVE MULTIGENE RT-PCR ASSAY FOR PREDICTING RECURRENCE RISK AFTER SURGICAL EXCISION ALONE WITHOUT IRRADIATION FOR DUCTAL CARCINOMA IN SITU (DCIS): A PROSPECTIVE VALIDATION STUDY OF THE DCIS SCORE FROM ECOG E5194 Solin LJ, Gray R, Baehner FL, Butler S, Badve S, Yoshizawa C, Shak S, Hughes L, Sledge G, Davidson N, Perez EA, Ingle J, Sparano J, Wood W Eastern Cooperative Oncology Group (ECOG) North Central Cancer Treatment Group (NCCTG) Genomic Health, Inc (GHI) 2011 San Antonio Breast Cancer Symposium DUCTAL CARCINOMA IN SITU: BACKGROUND 45,000 new cases in 2010 in U.S. (estimated) Most patients (~ 60-70%) eligible for breast conservation surgery (lumpectomy) - Radiation and tamoxifen reduce risk Reliable methods to select treatment with surgery alone have not been established using clinical and pathologic factors NIH State-of-the-Science recommendation: Develop and validate risk stratification models. Allegra, JNCI, 2010 This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. 19

 compared to invasive disease GHI data on file This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute.")
20 NEW DCIS SCORE: DEVELOPMENT A genomic-based score to predict local recurrence, regardless of adjuvant tamoxifen, was desired Based on prior studies, a DCIS Score algorithm was developed - Selected a subset of genes from Oncotype DX Recurrence Score that were prognostic in tamoxifen treated and untreated patients - No thresholding for proliferation gene group for DCIS Score Different from Recurrence Score (thresholded at score 6.5) Proliferation lower in DCIS (92% < 6.5) compared to invasive disease GHI data on file This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. DCIS SCORE DCIS Score (0 100) evaluated 2 ways: - Continuous variable - 3 prespecified risk groups: Low < 39 Intermediate High > 55 This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. 20
21 ECOG E5194 (PARENT STUDY) Prospective multicenter study (n = 670) Cohort 1: Low/intermediate grade, size < 2.5 cm Cohort 2: High grade, size < 1 cm Study treatment - Surgical excision - Minimum 3 mm negative margin width - No radiation - Tamoxifen option beginning May 2000 Reported outcomes at 5 and 7 years (Hughes, JCO, 2009) - Currently 10-year outcomes This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. PRESPECIFIED STUDY OBJECTIVES Primary: To determine whether there is a significant association between the DCIS Score and the risk of an ipsilateral breast event (IBE) Secondary: To determine whether the DCIS Score provides value beyond standard clinical and pathologic factors Conditional (if DCIS Score validated): To evaluate the Recurrence Score as a predictor of risk of an ipsilateral breast event (IBE) This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. 21
22 METHODS FOR DCIS SCORE VALIDATION STUDY - Prospective-retrospective study design Prespecified: Study objectives, population, laboratory assays, endpoints, statistical methods - Oncotype DX assay performed (n = 327; 49%) Standardized methods for 21 gene assay Central pathology review Calculated: DCIS Score and Recurrence Score - Study endpoint: Ipsilateral breast events (IBE) 1 o Endpoint: Any IBE (DCIS or invasive carcinoma) 2 o Endpoints: Invasive IBE DCIS IBE This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. PATIENT AND TUMOR CHARACTERISTICS Characteristic* Patient age Number 61 years (Median) Postmenopausal 248 (76%) Tumor size 7 mm (Median) Tumor size < 10 mm 260 (80%) Negative margins > 5 mm 214 (65%) Tamoxifen use 96 (29%) ER positive (RT-PCR) 318 (97%) Study cohort: Cohort (83%) Cohort 2 54 (17%) *Similar to parent trial for all variables except for tumor size This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. 22
23 PRIMARY ANALYSES OF THE RISK FOR AN IPSILATERAL BREAST EVENT (IBE) Hazard Ratio* (95% CI) P value Primary Analysis DCIS Score 2.34 (1.15, 4.59) 0.02 Tamoxifen use 0.56 (0.24, 1.15) 0.12 Conditional Analysis Recurrence Score 0.70 (0.15, 2.65) 0.62 *Hazard ratio is for a 50 point difference This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. DCIS SCORE: 10-YEAR IPSILATERAL BREAST EVENTS (IBE) BY RISK GROUP ANY IBE This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. 23

 ANY IBE This presentation is the 24")
24 DCIS SCORE: 10-YEAR IPSILATERAL BREAST EVENTS (IBE) BY RISK GROUP ANY IBE INVASIVE IBE This presentation is the intellectual property of the author/presenter. Contact for permission to reprint and/or distribute. DCIS SCORE: 10-YEAR RISK OF AN IPSILATERAL BREAST EVENT (IBE) ANY IBE This presentation is the intellectual property of the author/presenter. Contact for permission to reprint and/or distribute. 24
25 DCIS SCORE: 10-YEAR RISK OF AN IPSILATERAL BREAST EVENT (IBE) ANY IBE INVASIVE IBE This presentation is the intellectual property of the author/presenter. Contact for permission to reprint and/or distribute. MULTIVARIABLE MODELS OF RISK FOR IBE Hazard Ratio (95% CI) P value Excluding the DCIS Score Tumor size 1.54 (1.14, 2.02) 0.01 Postmenopausal 0.49 (0.27, 0.90) 0.02 Including the DCIS Score DCIS Score 2.41 (1.15, 4.89) 0.02 Tumor size 1.52 (1.11, 2.01) 0.01 Postmenopausal 0.49 (0.27, 0.90) 0.02 For study cohort, surgical margins, grade, comedo necrosis, and DCIS pattern, all p >.46. For tamoxifen, p =.09. This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. 25
26 SUMMARY: DCIS SCORE 1. Present study validates the DCIS Score as a predictor of an ipsilateral breast event (IBE) and invasive IBE 2. DCIS Score quantifies 10-year risk of IBE - Continuous variable or 3 risk groups 3. DCIS Score provides independent information on IBE risk beyond clinical and pathologic variables - Including tamoxifen, grade, and negative margin width - Identifies underlying tumor biology 4. DCIS Score provides a new clinical tool to guide treatment selection for patients with newly diagnosed DCIS This presentation is the intellectual property of the author/presenter. Contact solin@einstein.edu for permission to reprint and/or distribute. Poster Discussion SABCS

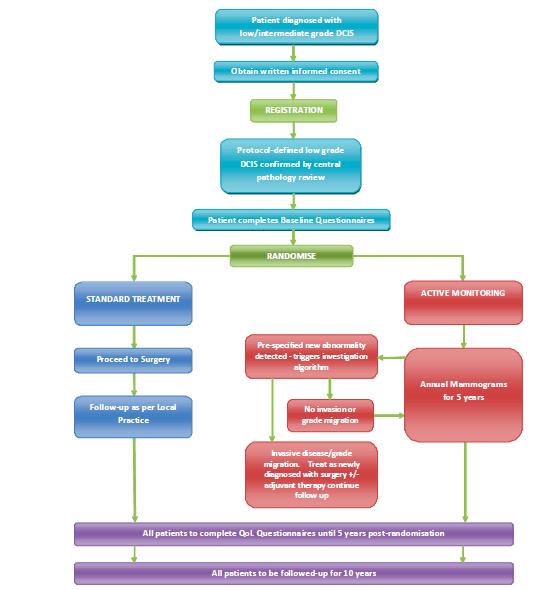
27 STANDARD TREATMENT Proceed to Surgery Follow- up as per Local Prac8ce Pa8ent diagnosed with low/intermediate grade DCIS Obtain wrieen informed consent Protocol- defined low grade DCIS confirmed by central pathology review ACTIVE MONITORING ANDOMISE Pre- specified new abnormality de tected - triggers inves8ga8on algorithm Invasive disease/grade adjuvant therapy con8nue follow up ACTIVE MONITORING Annual Mammograms for 5 years All pa8ents to complete QoL Ques8onnaires un8l 5 years post- randomisa8on All pa8ents to be followed- up for 10 years 1/12/12 Vacuum assisted biopsies of Ductal Carcinoma in situ and concordance with post-operative histology: implications for the Low risk DCIS Trial Soni Soumian, Sue Down, Fozia Roked, Shalini Chaudhri, Adele Francis Department of Surgery, Queen Elizabeth Hospital, Birmingham UK Background Low Risk DCIS Trial Pathway Results Results In the Low grade group, the concordance with final The enormous increase in the diagnosis of Ductal carcinoma in situ (DCIS) by the NHS Breast screening has not lead to an expected decrease in the histology was 74% (17/23). In this group, the diagnosis was upgraded to intermediate grade in 17% (4/23) and invasive incidence of invasive breast cancer. It is not clear if all grades of DCIS progress inexorably to invasive cancer if left untreated. There is recognition that DCIS is overtreated, ie if left alone may not cause harm during the woman s lifetime. In the absence of new clinical trial data, surgery still REGISTRATIO N Background carcinoma in 9% (2/23). Further analysis of the results in the Low grade group that remains the universal treatment. upgraded to invasive cancer (2/23) revealed that one of the Recently a randomized trial called the Low risk DCIS Trial has been proposed which intends to specifically compare the current treatment of low grade DCIS ie surgery with active monitoring using annual mammography. In Pa8ent completes Baseline Ques8onnaires RResults patients had a ultrasound diagnosed mass (7 mm microcalcification within the mass) which would exclude the patient from the Low risk DCIS trial. order to effectively implement this, concordance between diagnostic biopsy and excision histology is vital and therefore vacuum assisted mammotome biopsy (VAB) and a central pathology review of diagnostic biopsy specimens prior to randomization will be mandatory. The other patient on final histology had a 1.3 mm lobular carcinoma (5mm microcalcification on mammogram) within the DCIS. Therefore, in this study, we assessed the concordance between diagnostic biopsies performed by VAB technique and the post operative histology for DCIS in our institution. No invasion or grade migra8on A total of 160 cases were identified out of which 102 (63%) were of high grade, 35 (22%) of intermediate grade and 23 (14%) were of low grade histology. Conclusions Materials & Methods migra8on. Treat as newly diagnosed with surgery +/- Average age was 61 years. More than 4 cores were taken in all cases during VAB Concordance was the highest in the low grade DCIS group procedures. Screening group contributed 76% of DCIS patients. in this series and is to our knowledge the first to be reported using specifically large volume biopsies done using VAB Retrospective data of all diagnostic breast biopsies specifically using the VAB technique with the primary diagnosis of DCIS from year 2001 to 2010 in our institution was collected. Both screening and symptomatic patients were included. Concordance between diagnostic histology and post operative excision Inclusion Criteria In the High grade group, the concordance with final histology was 70% (72/102). In this group, the diagnosis was upgraded to invasive carcinoma in 21% (21/102). 9% (9/102) were downgraded to intermediate or low grade. Exclusion Criteria techniques. These results and concordance audit data from other centres in the UK will be used by trial pathologists to refine protocols for the Low risk DCIS trial. histology was assessed for high, intermediate and low grade DCIS. Demographic details and potential factors influencing concordance includingg number of cores taken and lesion size were also collected for analysis - Low risk DCIS Vaccum assisted Biopsy -Palpable mass with histology confirmed by Central pathology review -Mass lesion on Mammography - Asymptomatic -Mass lesion on Ultrasonography In the Intermediate grade group, the concordance with final histology was 66% (23/35). In this group, the diagnosis was upgraded to invasive carcinoma in 11% (4/35) and to high grade in 17% (6/35). 6% (2/35) were downgraded to low grade. Determine Concordance Core Biopsy and Excision UK Trial to evaluate active monitoring of Low Grade DCIS Retrospective analysis of consecutive Core Biopsy for DCIS compared to surgical excision 27

28 28
29 Thank you 29
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Speaker s Bureau. Travel expenses. Advisory Boards. Stock. Genentech Invuity Medtronic Pacira. Faxitron. Dune TransMed7 Genomic Health.
 Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Disclosures. Premalignant Lesions of the Breast: What Clinicians Want and Why. NY Times: Prone to Error: Earliest Steps to Find Cancer.
 Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Disclosures Premalignant Lesions of the Breast: What Clinicians Want and Why I have nothing to disclose Rick Baehner, MD Assistant Professor, UCSF Pathology NY Times: Prone to Error: Earliest Steps to
Supplementary Online Content
 Supplementary Online Content Giannakeas V, Sopik V, Narod SA. Association of Radiotherapy With Survival in Women Treated for Ductal Carcinoma In Situ With Lumpectomy or Mastectomy. JAMA Netw Open. 2018;1(4):e181100.
Supplementary Online Content Giannakeas V, Sopik V, Narod SA. Association of Radiotherapy With Survival in Women Treated for Ductal Carcinoma In Situ With Lumpectomy or Mastectomy. JAMA Netw Open. 2018;1(4):e181100.
3/27/2017. Disclosure of Relevant Financial Relationships. Papilloma???
 Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Management of Papillary Lesions Diagnosed at Rad Path Concordant Core Biopsy (CNB) Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
Genomic Profiling of Tumors and Loco-Regional Recurrence
 1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Prophylactic Mastectomy State of the Art
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Personalized Treatment of DCIS
 Global Breast Cancer Conference 2016 [The Shilla Hotel, Jeju] Symposium 1 : DCIS - What s New? (14:40-15:50) Personalized Treatment of DCIS 2016. 4. 28. Breast Division, Department of Surgery Sungkyunkwan
Global Breast Cancer Conference 2016 [The Shilla Hotel, Jeju] Symposium 1 : DCIS - What s New? (14:40-15:50) Personalized Treatment of DCIS 2016. 4. 28. Breast Division, Department of Surgery Sungkyunkwan
Ductal Carcinoma in Situ. Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA
 Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Ductal Carcinoma in Situ Laura C. Collins, M.D. Department of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Definition of DCIS WHO 2012 A neoplastic proliferation
Pathology of Lobular & Ductal Preneoplasia. Syed A Hoda, MD Weill-Cornell, New York, NY
 Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Pathology of Lobular & Ductal Preneoplasia Syed A Hoda, MD Weill-Cornell, New York, NY Proliferative Epithelial Changes in Breast A wide range of proliferative epithelial changes occur in the breast There
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon OBE Edinburgh Breast Unit
 10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon OBE Edinburgh Breast Unit 10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon
10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon OBE Edinburgh Breast Unit 10 reasons why it makes sense to rename DCIS to minimise overtreatment? PRO: Mike Dixon
Bruno CUTULI Policlinico Courlancy REIMS. WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ
 Bruno CUTULI Policlinico Courlancy REIMS WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ XXI CONGRESSO AIRO GENOVA 22.11.2011 INTRODUCTION Due to wide diffusion of mammography,
Bruno CUTULI Policlinico Courlancy REIMS WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ XXI CONGRESSO AIRO GENOVA 22.11.2011 INTRODUCTION Due to wide diffusion of mammography,
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Short Term Cancer Risk
 in a Cohort of 2312 Women with High Risk Breast Lesions Kubat E 1, Puligandla B 2, Collins L 3, Jiang SF 4, Callahan M 5, Kutner S 6, Habel L 4, Shim V 1 1 Surgery, Kaiser Permanente, Oakland, CA; 2 Pathology,
in a Cohort of 2312 Women with High Risk Breast Lesions Kubat E 1, Puligandla B 2, Collins L 3, Jiang SF 4, Callahan M 5, Kutner S 6, Habel L 4, Shim V 1 1 Surgery, Kaiser Permanente, Oakland, CA; 2 Pathology,
2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights
 2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights Mylin A. Torres, M.D. Director, Glenn Family Breast Center Associate Professor Department of Radiation Oncology Winship Cancer Institute
2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights Mylin A. Torres, M.D. Director, Glenn Family Breast Center Associate Professor Department of Radiation Oncology Winship Cancer Institute
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
The Oncotype DX Assay A Genomic Approach to Breast Cancer
 The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Chief Investigator Adele Francis University of Birmingham UK. Prof MWR Reed (CoI) University of Sheffield
 University of Sheffield") The LORIS Trial: A multicentre, randomised phase III trial of standard surgery versus active monitoring in women with newly diagnosed low risk ductal carcinoma in situ. Chief Investigator Adele Francis
The LORIS Trial: A multicentre, randomised phase III trial of standard surgery versus active monitoring in women with newly diagnosed low risk ductal carcinoma in situ. Chief Investigator Adele Francis
Evaluation & Management of PowerPoint Cover Title. the High Risk Population. High Risk Clinic
 Evaluation & Management of PowerPoint Cover Title the High Risk Population High Risk Clinic Subtitle Joanna Would Springman, Go Here PA-C Assessment Genetics Known genetic mutation Family history with
Evaluation & Management of PowerPoint Cover Title the High Risk Population High Risk Clinic Subtitle Joanna Would Springman, Go Here PA-C Assessment Genetics Known genetic mutation Family history with
LOBULAR CARCINOMA IN SITU: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE
 : WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
Atypical proliferative lesions diagnosed on core biopsy - 6 year review
 Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
Atypical proliferative lesions diagnosed on core biopsy - 6 year review Dr Angela Harris, Dr Julie Weigner & Dr Ricardo Vilain NSW Health Pathology Pathology North, Hunter Anatomical Pathology & Cytology
Imaging Surveillance in Women with a History of Treated Breast Cancer. Wei Tse Yang, M.D.
 Imaging Surveillance in Women with a History of Treated Breast Cancer Wei Tse Yang, M.D. Breast Cancer 1. Extent 2. Response 3. Recurrence Surveillance Breast Cancer 1. Extent 2. Response Surveillance
Imaging Surveillance in Women with a History of Treated Breast Cancer Wei Tse Yang, M.D. Breast Cancer 1. Extent 2. Response 3. Recurrence Surveillance Breast Cancer 1. Extent 2. Response Surveillance
TRIAL SYNOPSIS LORIS. The Low Risk DCIS Trial. Chief Investigator. Miss Adele Francis
 TRIAL SYNOPSIS LORIS Chief Investigator The Low Risk DCIS Trial Miss Adele Francis ISRCTN No. 27544579 Sponsor University of Birmingham, United Kingdom Trial Design Objectives of Feasibility Study A multi-centre,
TRIAL SYNOPSIS LORIS Chief Investigator The Low Risk DCIS Trial Miss Adele Francis ISRCTN No. 27544579 Sponsor University of Birmingham, United Kingdom Trial Design Objectives of Feasibility Study A multi-centre,
Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer
 Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer Sheryl G.A. Gabram, MD, MBA, FACS Professor of Surgery, Emory University Director, High Risk Assessment Program Winship Cancer
Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer Sheryl G.A. Gabram, MD, MBA, FACS Professor of Surgery, Emory University Director, High Risk Assessment Program Winship Cancer
Surgical Pathology Issues of Practical Importance
 Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
Surgical Pathology Issues of Practical Importance Anne Moore, MD Medical Oncology Syed Hoda, MD Surgical Pathology The pathologist is central to the team approach needed to manage the patient with breast
A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 A DEEPER DIVE INTO DUCTAL CARCINOMA IN SITU: CLINICAL AND PATHOLOGIC CONSIDERATIONS IN 2015
Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008
 Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008 Breast Cancer Most common cancer in American women 180,000 new cases per year Second most common cause of cancer death 44,000
Angela Gilliam, MD University of Colorado Surgical Grand Rounds November 3, 2008 Breast Cancer Most common cancer in American women 180,000 new cases per year Second most common cause of cancer death 44,000
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Ductal Carcinoma in Situ (DCIS)
") Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
So, Who are the appropriate individuals that should consider genetic counseling and genetic testing?
 Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Surgical Excision Without Radiation for Ductal Carcinoma in Situ of the Breast: 12-Year Results From the ECOG-ACRIN E5194 Study
 Surgical Excision Without Radiation for Ductal Carcinoma in Situ of the Breast: 12-Year Results From the ECOG-ACRIN E5194 Study Lawrence J. Solin, Albert Einstein Healthcare Network Robert Gray, Dana-Farber
Surgical Excision Without Radiation for Ductal Carcinoma in Situ of the Breast: 12-Year Results From the ECOG-ACRIN E5194 Study Lawrence J. Solin, Albert Einstein Healthcare Network Robert Gray, Dana-Farber
Breast Cancer: Current Approaches to Diagnosis and Treatment
 Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Mousa. Israa Ayed. Abdullah AlZibdeh. 0 P a g e
 1 Mousa Israa Ayed Abdullah AlZibdeh 0 P a g e Breast pathology The basic histological units of the breast are called lobules, which are composed of glandular epithelial cells (luminal cells) resting on
1 Mousa Israa Ayed Abdullah AlZibdeh 0 P a g e Breast pathology The basic histological units of the breast are called lobules, which are composed of glandular epithelial cells (luminal cells) resting on
04/10/2018 HIGH RISK BREAST LESIONS. Pathology Perspectives of High Risk Breast Lesions ELEVATED RISK OF BREAST CANCER HISTORICAL PERSPECTIVES
 Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
Pathology Perspectives of High Risk Breast Lesions Savitri Krishnamurthy MD Professor of Pathology Deputy Division Head Director of Clinical Trials, Research and Development The University of Texas MD
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer
 The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
Advances in the Diagnosis and Treatment of Breast Cancer. Carol Tweed, M.D. Anne Arundel Medical Center DeCesaris Cancer Institute Annapolis, MD
 Advances in the Diagnosis and Treatment of Breast Cancer Carol Tweed, M.D. Anne Arundel Medical Center DeCesaris Cancer Institute Annapolis, MD Disclosures Genomic Health: Speaker and Consultant AstraZeneca:
Advances in the Diagnosis and Treatment of Breast Cancer Carol Tweed, M.D. Anne Arundel Medical Center DeCesaris Cancer Institute Annapolis, MD Disclosures Genomic Health: Speaker and Consultant AstraZeneca:
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Disclosure. Objectives 03/19/2019. Current Issues in Management of DCIS Radiation Oncology Considerations
 Current Issues in Management of DCIS Radiation Oncology Considerations Fariba Asrari, M.D. Director. Johns Hopkins Breast Center at Green Spring Station Department of Radiation Oncology & Molecular Sciences
Current Issues in Management of DCIS Radiation Oncology Considerations Fariba Asrari, M.D. Director. Johns Hopkins Breast Center at Green Spring Station Department of Radiation Oncology & Molecular Sciences
Risk Assessment, Genetics, and Prevention
 Risk Assessment, Genetics, and Prevention Katherine D. Crew, MD MS Director, Clinical Breast Cancer Prevention Program Columbia University Medical Center 1 Outline Breast cancer risk factors Hereditary
Risk Assessment, Genetics, and Prevention Katherine D. Crew, MD MS Director, Clinical Breast Cancer Prevention Program Columbia University Medical Center 1 Outline Breast cancer risk factors Hereditary
Use of a Protease Activated System for Real-time Breast Cancer Lumpectomy Margin Assessment
 Use of a Protease Activated System for Real-time Breast Cancer Lumpectomy Margin Assessment Barbara L. Smith, MD, PhD Professor of Surgery, Harvard Medical School Division of Surgical Oncology Massachusetts
Use of a Protease Activated System for Real-time Breast Cancer Lumpectomy Margin Assessment Barbara L. Smith, MD, PhD Professor of Surgery, Harvard Medical School Division of Surgical Oncology Massachusetts
4/13/2010. Silverman, Buchanan Breast, 2003
 Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk
Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk
Breast Cancer Pathway Map
 Care Ontario Pathway Map 03.18 Printer Friendly Version Note: print 11x17 landscape for best results, some features and content are only available on web version of pathway map Prevention Screening Diagnosis
Care Ontario Pathway Map 03.18 Printer Friendly Version Note: print 11x17 landscape for best results, some features and content are only available on web version of pathway map Prevention Screening Diagnosis
Reliable Evaluation of Prognostic & Predictive Genomic Tests
 Reliable Evaluation of Prognostic & Predictive Genomic Tests Richard Simon, D.Sc. Chief, Biometric Research Branch National Cancer Institute http://brb.nci.nih.gov Different Kinds of Biomarkers Prognostic
Reliable Evaluation of Prognostic & Predictive Genomic Tests Richard Simon, D.Sc. Chief, Biometric Research Branch National Cancer Institute http://brb.nci.nih.gov Different Kinds of Biomarkers Prognostic
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Promise of a beautiful day
 Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
Promise of a beautiful day Ductal carcinoma in Situ Lobular Carcinoma in Situ Natural History Manosmed Tartous Oct 2009 Gérard ABADJIAN MD Pathology Department Hôtel-Dieu de France. Associate Professor
The Future of Breast MRI Improving Outcomes
 The Future of Breast MRI Improving Outcomes Connie Lehman MD PhD Professor of Radiology Harvard Medical School Director of Breast Imaging Massachusetts General Hospital Opportunities New technology provides
The Future of Breast MRI Improving Outcomes Connie Lehman MD PhD Professor of Radiology Harvard Medical School Director of Breast Imaging Massachusetts General Hospital Opportunities New technology provides
Chemo-endocrine prevention of breast cancer
 Chemo-endocrine prevention of breast cancer Andrea DeCensi, MD Division of Medical Oncology Ospedali Galliera, Genova; Division of Cancer Prevention and Genetics, European Institute of Oncology, Milano;
Chemo-endocrine prevention of breast cancer Andrea DeCensi, MD Division of Medical Oncology Ospedali Galliera, Genova; Division of Cancer Prevention and Genetics, European Institute of Oncology, Milano;
MANAGEMENT OF DENSE BREASTS. Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015
 MANAGEMENT OF DENSE BREASTS Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015 No financial disclosures National Cancer Institute National Cancer Institute Increased Cancer Risk... DENSITY
MANAGEMENT OF DENSE BREASTS Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015 No financial disclosures National Cancer Institute National Cancer Institute Increased Cancer Risk... DENSITY
Learning Objectives. Financial Disclosure. Breast Cancer Quality Improvement Project with Oncotype DX. Nothing to disclose
 Breast Cancer Quality Improvement Project with Oncotype DX Denise Johnson Miller, MD, FACS Medical Director Breast Surgery Hackensack Meridian Health Legacy Meridian (Jersey Shore University Medical Center,
Breast Cancer Quality Improvement Project with Oncotype DX Denise Johnson Miller, MD, FACS Medical Director Breast Surgery Hackensack Meridian Health Legacy Meridian (Jersey Shore University Medical Center,
Ductal Carcinoma-in-Situ: New Concepts and Controversies
 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Breast MRI: Friend or Foe?
 Breast : Friend or Foe? APPLEGATE HAS DOUBLE MASTECTOMY IN CANCER SCARE DIAGNOSED WITH CANCER IN ONE BREAST Comments: 0 ASSOCIATED PRESS 8/19/2008 UCSF Postgraduate Course March 19, 2009 E. Shelley Hwang
Breast : Friend or Foe? APPLEGATE HAS DOUBLE MASTECTOMY IN CANCER SCARE DIAGNOSED WITH CANCER IN ONE BREAST Comments: 0 ASSOCIATED PRESS 8/19/2008 UCSF Postgraduate Course March 19, 2009 E. Shelley Hwang
IJC International Journal of Cancer
 IJC International Journal of Cancer Short Report Oncotype Dx recurrence score among BRCA1/2 germline mutation carriers with hormone receptors positive breast cancer Naama Halpern 1, Amir Sonnenblick 2,
IJC International Journal of Cancer Short Report Oncotype Dx recurrence score among BRCA1/2 germline mutation carriers with hormone receptors positive breast cancer Naama Halpern 1, Amir Sonnenblick 2,
BREAST MRI. Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School
 BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
BREAST MRI Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School BREAST MRI Any assessment of the breast parenchyma requires the administration
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
National Diagnostic Imaging Symposium 2013 SAM - Breast MRI 1
 National Diagnostic Imaging Symposium 2013 December 8-12, 2013 Disney s Yacht Club Resort Lake Buena Vista, Florida Self Assessment Module Questions, Answers and References Day SAM Title - Each SAM title
National Diagnostic Imaging Symposium 2013 December 8-12, 2013 Disney s Yacht Club Resort Lake Buena Vista, Florida Self Assessment Module Questions, Answers and References Day SAM Title - Each SAM title
Prophylactic Mastectomy
 Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO 08/24/2012 Section: Surgery Place(s) of Service: Inpatient I.
Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO 08/24/2012 Section: Surgery Place(s) of Service: Inpatient I.
Targeting Surgery for Known Axillary Disease. Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center
 Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Update from the 29th Annual San Antonio Breast Cancer Symposium
 Update from the 29th Annual San Antonio Breast Cancer Symposium The San Antonio Breast Cancer Symposium is one of the most important breast cancer conferences. Approximately 8,000 physicians, oncologists,
Update from the 29th Annual San Antonio Breast Cancer Symposium The San Antonio Breast Cancer Symposium is one of the most important breast cancer conferences. Approximately 8,000 physicians, oncologists,
She counts on your breast cancer expertise at the most vulnerable time of her life.
 HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
Breast MRI: Friend or Foe?
 Breast MRI: Friend or Foe? UCSF Postgraduate Course May 18, 2013 Cheryl Ewing, MD Clinical Professor of Surgery UCSF Department of Surgery APPLEGATE HAS DOUBLE MASTECTOMY IN CANCER SCARE DIAGNOSED WITH
Breast MRI: Friend or Foe? UCSF Postgraduate Course May 18, 2013 Cheryl Ewing, MD Clinical Professor of Surgery UCSF Department of Surgery APPLEGATE HAS DOUBLE MASTECTOMY IN CANCER SCARE DIAGNOSED WITH
Evaluations & CE Credits
 Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. 1 Breast Density and Breast Cancer
Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. 1 Breast Density and Breast Cancer
Prophylactic Mastectomy
 Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/01/2015 Section: Surgery Place(s) of Service:
Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 09/01/2015 Section: Surgery Place(s) of Service:
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
TMIST: Frequently Asked Questions
 TMIST: Frequently Asked Questions Key Topics for Site Investigators and Staff This document answers frequently asked questions about the Tomosynthesis Mammographic Imaging Screening Trial (TMIST/EA1151);
TMIST: Frequently Asked Questions Key Topics for Site Investigators and Staff This document answers frequently asked questions about the Tomosynthesis Mammographic Imaging Screening Trial (TMIST/EA1151);
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy
 Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy Poster No.: C-2515 Congress: ECR 2015 Type: Authors: Scientific Exhibit Ö. S. Okcu 1, A. Oktay
Excisional biopsy or long term follow-up results in breast high-risk lesions diagnosed at core needle biopsy Poster No.: C-2515 Congress: ECR 2015 Type: Authors: Scientific Exhibit Ö. S. Okcu 1, A. Oktay
The management of B3 lesions with emphasis on lobular neoplasia
 The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential
The management of B3 lesions with emphasis on lobular neoplasia Abeer Shaaban Queen Elizabeth Hospital Birmingham NHSBSP core biopsy categories B1 - Normal B2 - Benign B3 Uncertain malignant potential
Overview of peculiarities and therapeutic options for patients with breast cancer and a BRCA germline mutation
 Overview of peculiarities and therapeutic options for patients with breast cancer and a BRCA germline mutation Dr Niklas Loman PhD MD Consultant oncologist Skåne University Hospital Lund, Suecia Prognosis
Overview of peculiarities and therapeutic options for patients with breast cancer and a BRCA germline mutation Dr Niklas Loman PhD MD Consultant oncologist Skåne University Hospital Lund, Suecia Prognosis
The TAILORx Trial: A review of the data and implications for practice
 The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
Ca in situ e ormonoterapia. Discussant : LORENZA MARINO
 Ca in situ e ormonoterapia Discussant : LORENZA MARINO Ca in situ e ormonoterapia Quali fattori di rischio? Radioterapia? Ormonoterapia? BCS Recurrence rates (FUP 13-20y) Cuzick, Lancet Oncol.2011; 12(1):
Ca in situ e ormonoterapia Discussant : LORENZA MARINO Ca in situ e ormonoterapia Quali fattori di rischio? Radioterapia? Ormonoterapia? BCS Recurrence rates (FUP 13-20y) Cuzick, Lancet Oncol.2011; 12(1):
Recent Update in Surgery for the Management of Breast Cancer
 Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Have you been recently diagnosed with DCIS?
 Have you been recently diagnosed with DCIS? Jen D. A busy mother of two and active community volunteer. Jen D. A busy mother of 2 and active community volunteer. *DCIS = Ductal carcinoma in situ AnAn educational
Have you been recently diagnosed with DCIS? Jen D. A busy mother of two and active community volunteer. Jen D. A busy mother of 2 and active community volunteer. *DCIS = Ductal carcinoma in situ AnAn educational
Morphological and Molecular Typing of breast Cancer
 Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care
 Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Quality ID #263: Preoperative Diagnosis of Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION:
Breast Cancer Screening Clinical Practice Guideline. Kaiser Permanente National Breast Cancer Screening Guideline Development Team
 NATIONAL CLINICAL PRACTICE GUIDELINE Breast Cancer Screening Clinical Practice Guideline Kaiser Permanente National Breast Cancer Screening Guideline Development Team This guideline is informational only.
NATIONAL CLINICAL PRACTICE GUIDELINE Breast Cancer Screening Clinical Practice Guideline Kaiser Permanente National Breast Cancer Screening Guideline Development Team This guideline is informational only.
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond.
 HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy
 Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy Breast Cancer is the most common cancer diagnosed in women in the United
Atypical Ductal Hyperplasia and Papillomas: A Comparison of Ultrasound Guided Breast Biopsy and Stereotactic Guided Breast Biopsy Breast Cancer is the most common cancer diagnosed in women in the United
Rationale For & Design of TAILORx. Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York
 Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
BREAST SURGERY PROGRESS TEST Name:
 General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
General Surgery Residency Program Excellent surgeons BREAST SURGERY PROGRESS TEST Name: Choose the BEST answer for the following questions. 1. All of the following factors are associated with an increased
Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
") Original article Annals of Oncology 14: 450 454, 2003 DOI: 10.1093/annonc/mdh088 Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
Original article Annals of Oncology 14: 450 454, 2003 DOI: 10.1093/annonc/mdh088 Mammographic features and correlation with biopsy findings using 11-gauge stereotactic vacuum-assisted breast biopsy (SVABB)
Recurrence, new primary and bilateral breast cancer. José Palacios Calvo Servicio de Anatomía Patológica
 Recurrence, new primary and bilateral breast cancer José Palacios Calvo Servicio de Anatomía Patológica Ipsilateral Breast Tumor Relapse (IBTR) IBTR can occur in approximately 5 20% of women after breast-conserving
Recurrence, new primary and bilateral breast cancer José Palacios Calvo Servicio de Anatomía Patológica Ipsilateral Breast Tumor Relapse (IBTR) IBTR can occur in approximately 5 20% of women after breast-conserving
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Prophylactic Mastectomy
 Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/01/2013 Section: Surgery Place(s) of Service:
Prophylactic Mastectomy Policy Number: Original Effective Date: MM.06.010 01/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/01/2013 Section: Surgery Place(s) of Service:
Breast Cancer Risk Assessment and Prevention
 Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Histological Type. Morphological and Molecular Typing of breast Cancer. Nottingham Tenovus Primary Breast Cancer Study. Survival (%) Ian Ellis
 Ian Ellis") Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological Type
W3C Life Sciences: Clinical Observations Interoperability: EMR + Clinical Trials Use-case for EMR + Clinical Trials Interoperability
 W3C Life Sciences: Clinical Observations Interoperability: EMR + Clinical Trials Use-case for EMR + Clinical Trials Interoperability Background: The key issue is to investigate whether some of the data
W3C Life Sciences: Clinical Observations Interoperability: EMR + Clinical Trials Use-case for EMR + Clinical Trials Interoperability Background: The key issue is to investigate whether some of the data
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Interpretation of Breast Pathology in the Era of Minimally Invasive Procedures
 Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine Jacksonville Medical Director, UF Health Breast Center Chief of Pathology
Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks
 Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks Grant W. Carlson Wadley R. Glenn Professor of Surgery Divisions of Plastic Surgery & Surgical Oncology Emory
Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks Grant W. Carlson Wadley R. Glenn Professor of Surgery Divisions of Plastic Surgery & Surgical Oncology Emory
IORT What We ve Learned So Far
 IORT What We ve Learned So Far The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation
IORT What We ve Learned So Far The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation
Abstract # 1503: Predisposing germline mutations in high grade ER+ HER2- breast cancer patients diagnosed age < 50
 Abstract # 1503: Predisposing germline mutations in high grade ER+ HER2- breast cancer patients diagnosed age < 50 Garber JE 1, Tung NM 2, Elkin EP 3, Allen BA 3, Singh NA 3, Wenstrup R 3, Hartman AR 3,
Abstract # 1503: Predisposing germline mutations in high grade ER+ HER2- breast cancer patients diagnosed age < 50 Garber JE 1, Tung NM 2, Elkin EP 3, Allen BA 3, Singh NA 3, Wenstrup R 3, Hartman AR 3,