Pulmonary Nodules & Masses
|
|
|
- Eustacia Horn
- 6 years ago
- Views:
Transcription
1 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology
2 Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties and licensing fees from multiple companies for CAD related software through University of Chicago (UCTech) Research support from Philips Healthcare Advisory Board for GE Medical Will not discuss investigational use.

3
4 What is a Pulmonary Nodule?
5 What is a Pulmonary Nodule?

6 What is a Pulmonary Nodule?
7 Pulmonary Nodule A rounded opacity, well or poorly defined, measuring up to 3 cm in diameter

8 28 year-old female with history of marijuana use and chronic cough.

9 Mucinous Adenocarcinoma

10 90% of peripheral cancers visible in retrospect (Muhm 1983)

11 Missed Lung Cancers : JHM Austin et al. Rad 1992;182: Size: cm (mean 1.6) Location : Upper lobes 81% Conspicuity : Overlapping bones in 82%

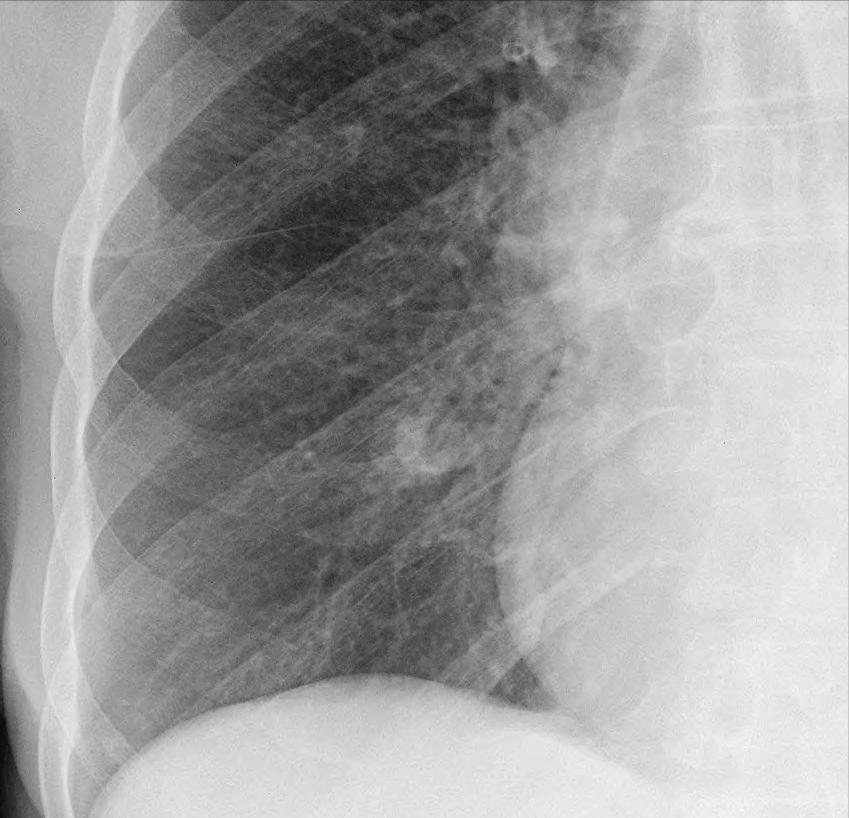
12 74 y/o man with COPD and rales

13 Lung Carcinoma 74 y/o man with COPD and rales

14 Conventional CXR Dual energy soft tissue image

15 Bone Suppression Imaging Standard CXR BSI CXR DES CXR
16 69 y/o female with hx of multiple myeloma

17 69 y/o female with hx of multiple myeloma Standard CXR ST image

18 69 y/o female with hx of multiple myeloma Standard CXR Bone image


19 Standard Thoracic CT Protocol; University of Chicago 2016 Key 1mm 3mm 3mm Cor MIPs MINIPs Sag Source Scout Scout Dose Contrast

20 MIP 1mm thin section

21 MIP 1mm thin section Zoom
22 ? Nodule


23 Axial Coronal Sagittal
24 Diagnostic Features of Nodules Size Morphology Growth rate Calcification

25

26 6mm metastasis
27
28 Percentage of Lung Cancers Detected by CXR According to Size mm 6-10mm 11-20mm 21-45mm Adapted from : Henschke et al. Lancet 1999;
29 Nodule Size and Probability of Malignancy Size ELCAP Mayo Nelson PanCan <3mm 0.1% 2-5mm <1% 0.4% <0.4% 4-7mm 0.7% 6-10mm 24% 8-20mm 18.7% 21-30mm 33.3% 21-45mm 80%
30 Diagnostic Features of Nodules Size Morphology Growth rate Calcification Overall Shape Solid/Non-solid Edge features-spiculated -Lobulated -Smooth
31 Ground Glass Nodule Solid Nodule

32 Smooth
33 Smooth Lobulated
34 Smooth Lobulated Spiculated

35 Smooth Lobulated Spiculated Part-Solid
36 Diagnostic Features of Nodules Size Margins Growth rate Calcification
37 Growth rate of nodules Volume doubling time (VDT): 26% diameter increase = One volume doubling
38 Growth rate of nodules Volume doubling time (VDT): 26% diameter increase = One volume doubling Typical lung ca. VDT = days Range = days
39 Growth rate of Small Cancers (Hasegawa BJR 2000) Parameter Mean VDT (Days) <10mm 536 >20mm 299 Smoker 292 Non-smoker 607 Adenoca 533 Squamous 129 Small cell 97 GGO 813 Mixed Solid

40 ARS #1 Incidental finding in a 58 year old former smoker
41 ARS #1 The MOST likely diagnosis is: (1) Indolent fungal infection. (2) Chronic organizing pneumonia (3) Atypical adenomatous hyperplasia (4) Nodular fibrosis (5) Invasive adenocarcinoma
42 Part-Solid and Non-Solid Nodules in a Screening Program Henschke et al. AJR 2002 ;178: Part-solid: 63% malignant Non-solid: 18% malignant Solid: 7% malignant
43 Persistent Non-Solid nodules 53 NS nodules in 49 pts Persisted or grew for > 1 month 75% were adenoca/ BAC 6% AAH 19% Nodular fibrosis/organizing pna Kim et al. Radiology ,1 p267
44 Lung Cancer: Major cell types Adenocarcinoma (50%)

45 Adenocarcinoma Up to 50% of lung cancers 55% present as peripheral nodule, often sub-solid May grow very slowly over years Some associated with pulmonary fibrosis
46 Lung Cancer: Major cell types Adenocarcinoma (50%) - Bronchioloalveolar (5%)
47 Lung Cancer: Major cell types Adenocarcinoma (50%) - Bronchioloalveolar (5%)
48 Lung Adenocarcinoma Classification AAH :Atypical Adenomatous Hyperplasia AIS : Adenoca in Situ MIA : Minimally Invasive Adenoca LPA : (Invasive) Lepidic Predominant Adenoca International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society International Multidisciplinary Classification of Lung Adenocarcinoma. WD Travis et al. Journal of Thoracic Oncology Volume 6, Number 2, February 2011
49 Lung Adenocarcinoma Classification AAH :Atypical Adenomatous Hyperplasia AIS : Adenoca in Situ MIA : Minimally Invasive Adenoca LPA : (Invasive) Lepidic Predominant Adenoca Non-Mucinous Mucinous International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society International Multidisciplinary Classification of Lung Adenocarcinoma. WD Travis et al. Journal of Thoracic Oncology Volume 6, Number 2, February 2011

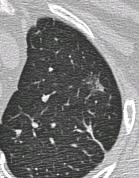
50 Atypical Adenomatous Hyperplasia (AAH) Typically GGO <5mm Precursor of adenoca Found in 20% + of lobes resected for lung ca



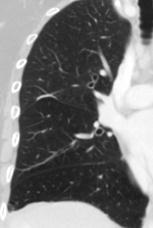
51 Ground Glass Nodule
52 MIA

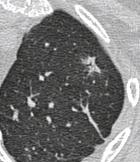
53 MIA -> Invasive lepidic predominant adenoca



54 Spectrum of Sub-solid Nodules GGO Part Solid Part Solid & Cystic

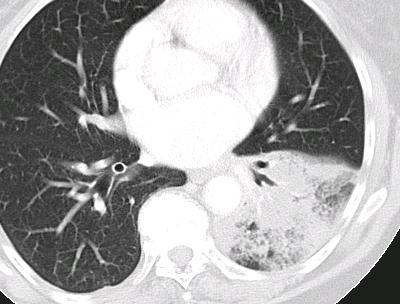
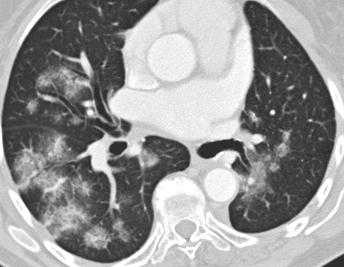

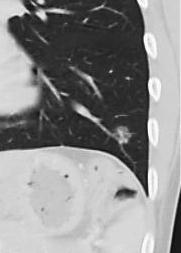
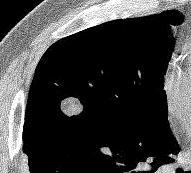
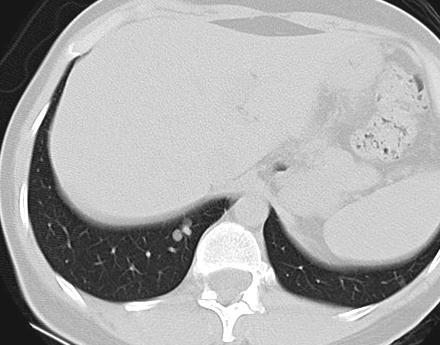
55 Mucinous Adenocarcinoma
56 Lung Cancer: Major cell types Adenocarcinoma (50%) Squamous cell (30%)

57 Squamous Cell Carcinoma 75% arise from segmental or larger bronchi 20% show central necrosis & cavitation 17% present with atelectasis


58 Small Cell Lung Cancer

59 Small-Cell Carcinoma 15-20% of lung cancers Early metastases, mediastinal adenopathy Strongest association with cigarette smoking Ectopic ACTH, inappropriate ADH
60 Lung Cancer: Major cell types Adenocarcinoma (50%) Squamous cell (30%) Small cell Undifferentiated (15%) Large cell Undifferentiated (5%)

61 Large Cell Undifferentiated Carcinoma 2-5%% of lung cancers 50% present as large peripheral mass May show very rapid growth Poor prognosis
62 Diagnostic Features of Nodules Size Margins Growth rate Calcification
63 Regarding calcification in lung nodules, which of the following statements is false: ARS #2 (1) Focal central calcification is reliable evidence of benignancy. (2) Eccentric calcification is highly suggestive of malignancy. (3) Popcorn calcification is associated with hamartomas. (4) Calcification is detectable by CT in about 6-10% of lung cancers. (5) Laminar calcification is associated with healed post infectious granulomas.
64 Patterns of Calcification Central Laminated Eccentric Popcorn Diffuse Stippled
65 Patterns of Calcification Benign Indeterminate Central Laminated Eccentric Popcorn Diffuse Stippled

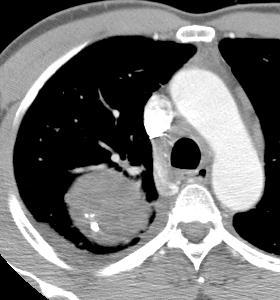
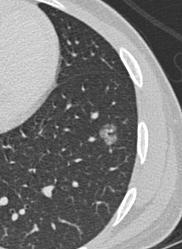
66 Dystrophic Calcification in Lung Cancer
67 Calcified Lung Carcinoma Calcium detectable by CT in 10%
68 Calcified Lung Carcinoma Calcium detectable by CT in 10% Usually 2 dystrophic ca++ or
69 Calcified Lung Carcinoma Calcium detectable by CT in 10% Usually 2 dystrophic ca++ or engulfed granulomatous ca++
70 Calcified Lung Carcinoma Calcium detectable by CT in 10% Usually 2 dystrophic ca++ or engulfed granulomatous ca++ Most calcified carcinomas are 5cm.+
71 Calcified Lung Carcinoma Calcium detectable by CT in 10% Usually 2 dystrophic ca++ or engulfed granulomatous ca++ Most calcified carcinomas are 5cm.+ Diffuse, speckled or irregular
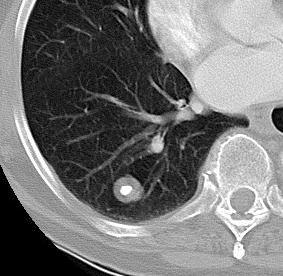
72 Granuloma
73 Granuloma Usually due to TB or Histo. in Midwest Typically diffuse, laminar or central calcs Typically smooth margins

74 Calcified Metastases- Osteosarcoma
75 Criteria for Benignancy Absence of growth over 2+ years* Benign pattern of Ca ++ * Does not apply to sub-solid nodules
76 ARS #3 60 y/o man who had a previous lobectomy for lung cancer.
77 ARS #3 60 y/o man who had a previous lobectomy for lung cancer. 8mm

78 ARS #3 Which of the following would be the most appropriate recommendation : Three to four month CT follow-up One year CT follow-up. PET scan Aspiration needle biopsy Immediate VATs resection 8mm
79 Recommendations for Follow-up and Management of Small Nodules 1 (Radiology NOV 2005) Nodule Low risk patient 3 High risk patient 4 Size 2 < 4 mm No follow-up needed 5 CT follow-up CT at 12 months; if unchanged, no further follow-up 6 >4-6 mm CT follow-up at 12 months; if unchanged, no further follow-up 6 >6-8 mm Initial CT follow-up at 6 to 12 months, then at 18 to 24 months if no change Initial CT follow-up at 6 to 12 months, then at months if no change 6 Initial CT follow-up at 3 to 6 months, then at 12 and 24 months if no change. >8 mm One or more of the following: CT follow-up at 3, 9, 24 months/ Dynamic CT 7 / PET scan / Biopsy
80 Recommendation for Incidental Subsolid Nodules Adapted from Radiology Jan Naidich et al. Nodule Type Pure GGN < 5mm Pure GGN > 5mm Recommendations No CT follow-up CT at 3 mos then annually for 3 yrs Part-solid nodule: SC < 5mm Part-solid nodule: SC > 5mm Multiple GGNs < 5mm Multiple GGNs > 5mm without dominant lesion Dominant nodule(s) with solid component CT at 3 mos then annually for 3 yrs+ CT at 3 mos then bx or resection CT at 2 and 4 yrs CT at 3 mos then annually for 3 yrs CT at 3 mos* then bx or resection especially if SC >5mm GGN:Ground glass nodule SC: Solid component
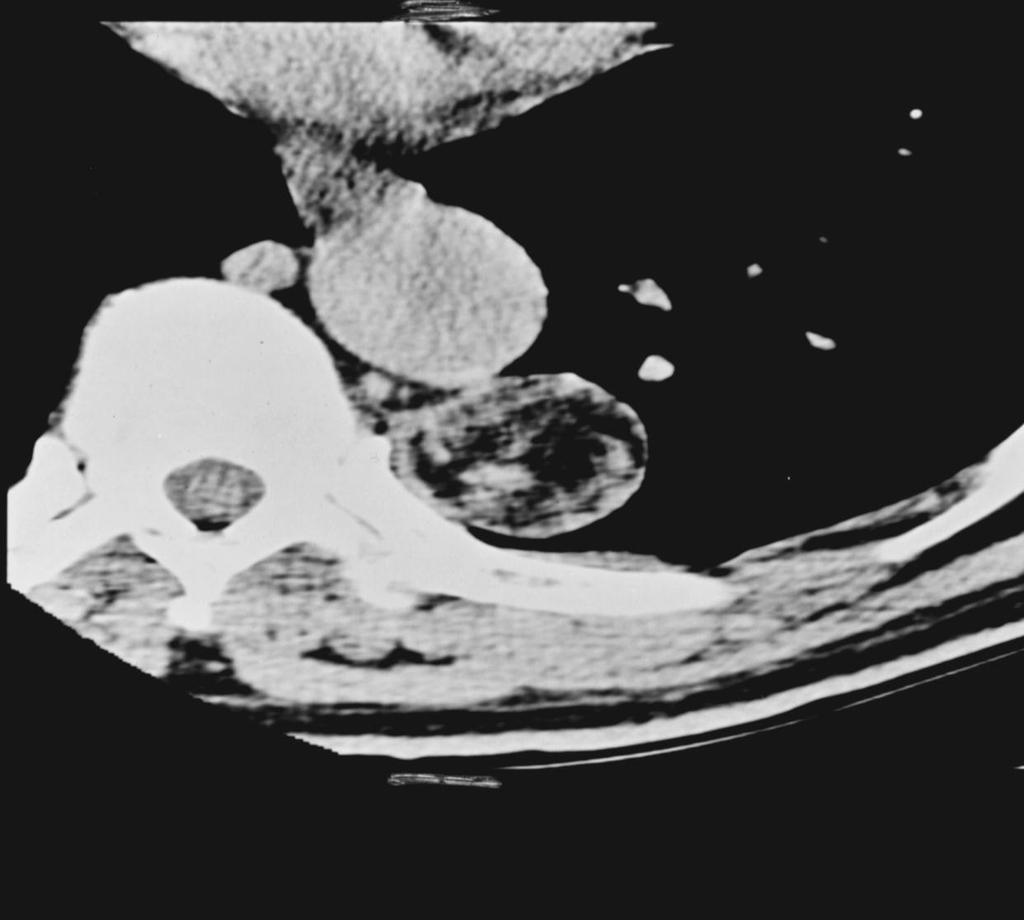
81 27 y/o woman with lung mass
82 Carcinoid Tumor
83 Carcinoid Tumor Neuroendocrine tumors; carcinoid syndrome rare (1-3%)
84 Carcinoid Tumor Neuroendocrine tumors; carcinoid syndrome rare (1-3%) Majority (80%) in main or segmental bronchi; present with atelectasis/obstructive pneumonia
85 Carcinoid Tumor Neuroendocrine tumors; carcinoid syndrome rare (1-3%) Majority (80%) in main or segmental bronchi; present with atelectasis/obstructive pneumonia Calcification in 30%
86 Carcinoid Tumor Neuroendocrine tumors; carcinoid syndrome rare (1-3%) Majority (80%) in main or segmental bronchi; present with atelectasis/obstructive pneumonia Calcification in 30% Atypical carcinoids : 10%
87
88 Hamartoma
89 Hamartoma
90 Hamartoma Most commonly resected benign tumor Peak incidence in sixth decade Endobronchial in 5% Fat and/or calcium on CT in 50%+ Well-defined, slow growing


91 Intrapulmonary Lymph Nodes Touching or within 5mm of pleural surface Typically triangular or oval Thin septal connection Usually in lower lungs
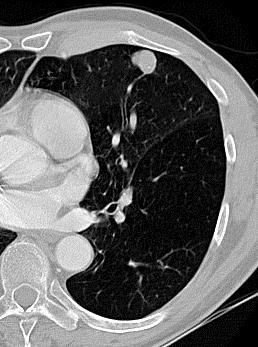
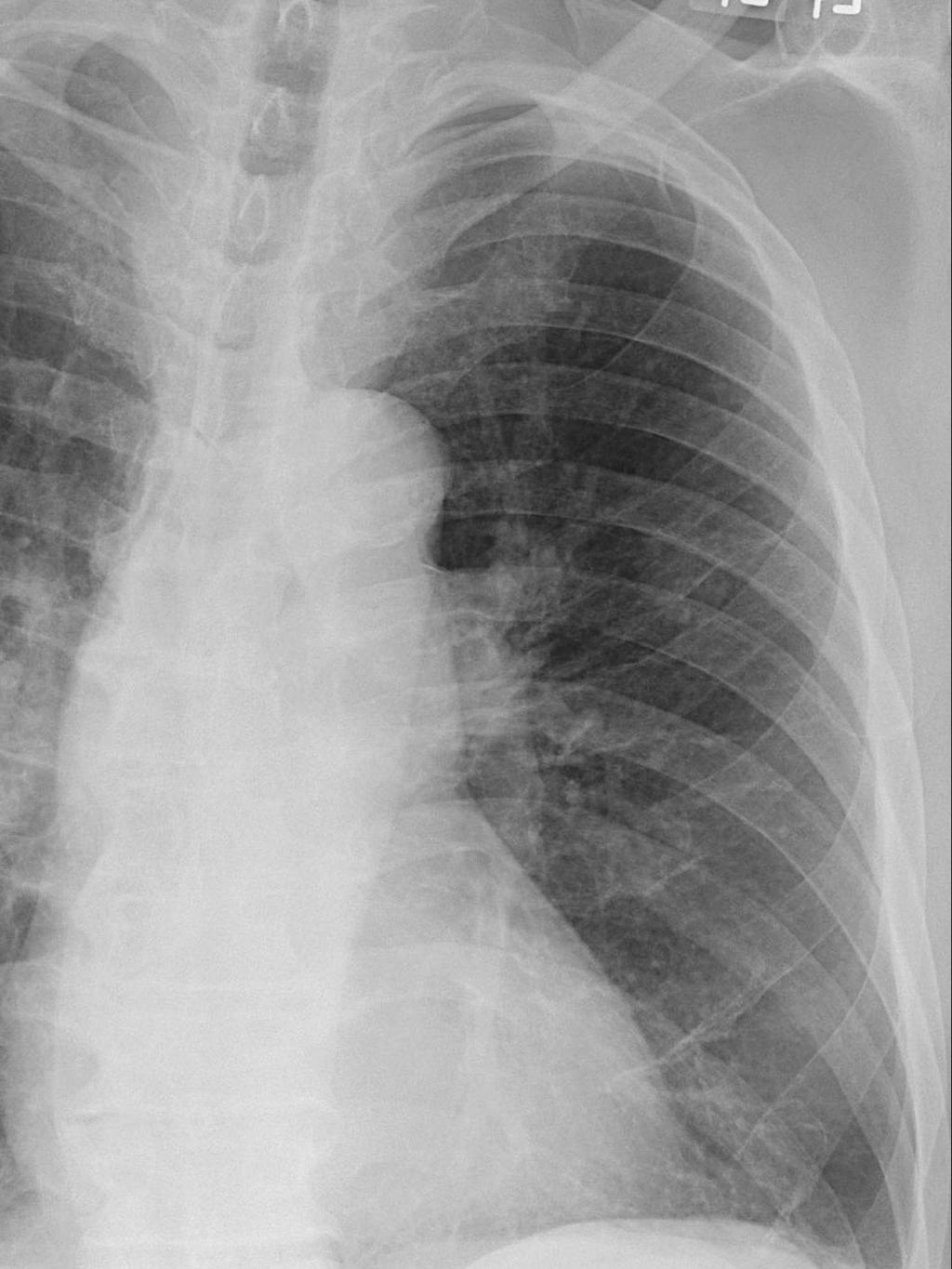
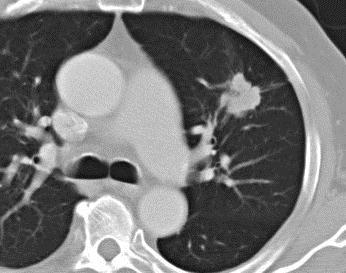
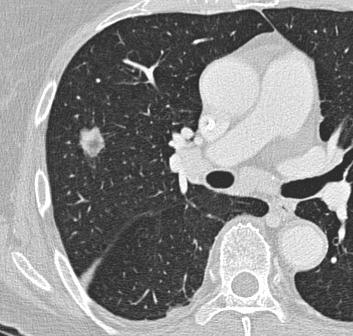
92 Incidental Nodule in 35 year old woman
93 Pulmonary AVM
94 AVM
95 AVM
96 AVM

97 AVM
98 Pulmonary AVM F:M=2:1, all ages Hemoptysis & dyspnea 35% multiple 40% - 65% have HHT (Osler-Weber-Rendu) Mostly lower lobe location
99 Conclusions Use routine thin sections and reformats to characterize small nodules Learn to recognize suspicious morphology Regard persistent non-solid nodules on CT with high suspicion, even if unchanged over long periods Always compare with earliest available scan to determine growth in subsolid nodules

100
101 Mucinous Adenocarcinoma
102 Mucinous Adenocarcinoma
103


104 Adenocarcinoma
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES. https://tinyurl.com/hmpn2018
 PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES
 Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Approach to Pulmonary Nodules
 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
LUNG NODULES: MODERN MANAGEMENT STRATEGIES
 Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
The small subsolid pulmonary nodules. What radiologists need to know.
 The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
Evidence based approach to incidentally detected subsolid pulmonary nodule. DM SEMINAR July 27, 2018 Harshith Rao
 Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
Xiaohuan Pan 1,2 *, Xinguan Yang 1,2 *, Jingxu Li 1,2, Xiao Dong 1,2, Jianxing He 2,3, Yubao Guan 1,2. Original Article
 Original Article Is a 5-mm diameter an appropriate cut-off value for the diagnosis of atypical adenomatous hyperplasia and adenocarcinoma in situ on chest computed tomography and pathological examination?
Original Article Is a 5-mm diameter an appropriate cut-off value for the diagnosis of atypical adenomatous hyperplasia and adenocarcinoma in situ on chest computed tomography and pathological examination?
Lung Cancer Screening: To Screen or Not to Screen?
 Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
SCBT-MR 2015 Incidentaloma on Chest CT
 SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
Lung Cancer Diagnosis for Primary Care
 Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
How to Analyse Difficult Chest CT
 How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
How to Analyse Difficult Chest CT Complex diseases are:- - Large lesion - Unusual or atypical pattern - Multiple discordant findings Diffuse diseases are:- - Numerous findings in both sides 3 basic steps
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI
 Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening
 Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening 1. Introduction In January 2005, the Committee for Preparation of Clinical Practice Guidelines for the Management
Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening 1. Introduction In January 2005, the Committee for Preparation of Clinical Practice Guidelines for the Management
Pulmonary Nodules. Michael Morris, MD
 Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Lung Cancer screening :
 Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach
 The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer
 Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for
Best Medical Practices: Maximizing Skills, Minimizing Risk Lung Cancer Optimal Management of Incidental Pulmonary Nodule Ramin Khorasani, MD, MPH Vice Chair, Department of Radiology Director, Center for
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Chest imaging III: Nodular pulmonary disease. Ádám Domonkos Tárnoki, MD, PhD Assistant professor Department of Radiology, Semmelweis University 1
 Chest imaging III: Nodular pulmonary disease Ádám Domonkos Tárnoki, MD, PhD Assistant professor Department of Radiology, Semmelweis University 1 Pattern 2 Nodular pattern Several round opacity, typically
Chest imaging III: Nodular pulmonary disease Ádám Domonkos Tárnoki, MD, PhD Assistant professor Department of Radiology, Semmelweis University 1 Pattern 2 Nodular pattern Several round opacity, typically
Screening for Lung Cancer: Are We There Yet?
 Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Screening for Lung Cancer: Are We There Yet? Kavita Garg, MD Professor of Radiology University of CO, Denver Mountain States Cancer Conference Nov 6 th 2010 The Epidemiology of Lung Cancer Tobacco is the
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2
 Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer
 November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC)
") CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC) Poster No.: C-2192 Congress: ECR 2014 Type: Educational Exhibit Authors: I. Sandu, A. R. Popita, I.-A. Brumboiu; Cluj-Napoca/RO
CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC) Poster No.: C-2192 Congress: ECR 2014 Type: Educational Exhibit Authors: I. Sandu, A. R. Popita, I.-A. Brumboiu; Cluj-Napoca/RO
CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC)
") CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC) Poster No.: C-2192 Congress: ECR 2014 Type: Educational Exhibit Authors: I. Sandu, A. R. Popita, I.-A. Brumboiu; Cluj-Napoca/RO
CT findings in multifocal or diffuse non-mucinous bronchioloalveolar carcinoma (BAC) Poster No.: C-2192 Congress: ECR 2014 Type: Educational Exhibit Authors: I. Sandu, A. R. Popita, I.-A. Brumboiu; Cluj-Napoca/RO
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art
 SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
Ground Glass Opacities
 Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
The revised lung adenocarcinoma classification an imaging guide
 Review Article The revised lung adenocarcinoma classification an imaging guide Natasha Gardiner 1, Sanjay Jogai 2, Adam Wallis 3 1 Specialty Registrar in Clinical Radiology, Wessex Deanery, UK; 2 Consultant
Review Article The revised lung adenocarcinoma classification an imaging guide Natasha Gardiner 1, Sanjay Jogai 2, Adam Wallis 3 1 Specialty Registrar in Clinical Radiology, Wessex Deanery, UK; 2 Consultant
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University
 LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
Objectives. Why? Why? Background 11/5/ % incurable disease at presentation Locally advanced disease Metastasis. 14% 5 year survival
 Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
Pulmonary Nodules: When to worry, when to chill. Douglas Arenberg Associate Professor Pulmonary & Critical Care
 Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
Pulmonary Nodules: When to worry, when to chill Douglas Arenberg Associate Professor Pulmonary & Critical Care Disclosure MDCH Grant Funds to improve tobacco cessation service in the Michigan Medicine
THE BENEFITS OF BIG DATA
 THE BENEFITS OF BIG DATA Disclosures I am a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell
THE BENEFITS OF BIG DATA Disclosures I am a named inventor on a number of patents and patent applications relating to the evaluation of pulmonary nodules on CT scans of the chest which are owned by Cornell
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Management of Multiple Pure Ground-Glass Opacity Lesions in Patients with Bronchioloalveolar Carcinoma
 ORIGINAL ARTICLE Management of Multiple Pure Ground-Glass Opacity Lesions in Patients with Bronchioloalveolar Carcinoma Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Jhingook Kim, MD, PhD,* Young Mog Shim, MD,
ORIGINAL ARTICLE Management of Multiple Pure Ground-Glass Opacity Lesions in Patients with Bronchioloalveolar Carcinoma Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Jhingook Kim, MD, PhD,* Young Mog Shim, MD,
HRCT features distinguishing minimally invasive adenocarcinomas from invasive adenocarcinomas appearing as mixed ground-glass nodules
 Original Article HRCT features distinguishing minimally invasive adenocarcinomas from invasive adenocarcinomas appearing as mixed ground-glass nodules Wei Yu 1, Zhaoyu Wang 2, Liyong Qian 2, Shanjun Wang
Original Article HRCT features distinguishing minimally invasive adenocarcinomas from invasive adenocarcinomas appearing as mixed ground-glass nodules Wei Yu 1, Zhaoyu Wang 2, Liyong Qian 2, Shanjun Wang
Stage I synchronous multiple primary non-small cell lung cancer: CT findings and the effect of TNM staging with the 7th and 8th editions on prognosis
 Original Article Stage I synchronous multiple primary non-small cell lung cancer: CT findings and the effect of TNM staging with the 7th and 8th editions on prognosis Jingxu Li, Xinguan Yang, Tingting
Original Article Stage I synchronous multiple primary non-small cell lung cancer: CT findings and the effect of TNM staging with the 7th and 8th editions on prognosis Jingxu Li, Xinguan Yang, Tingting
With recent advances in diagnostic imaging technologies,
 ORIGINAL ARTICLE Management of Ground-Glass Opacity Lesions Detected in Patients with Otherwise Operable Non-small Cell Lung Cancer Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Kwhanmien Kim, MD,* Young Mog
ORIGINAL ARTICLE Management of Ground-Glass Opacity Lesions Detected in Patients with Otherwise Operable Non-small Cell Lung Cancer Hong Kwan Kim, MD,* Yong Soo Choi, MD,* Kwhanmien Kim, MD,* Young Mog
SCBT-MR 2015 LungRADS : Basics
 SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
Financial disclosure COMMON DIAGNOSES IN HRCT. High Res Chest HRCT. HRCT Pre test. I have no financial relationships to disclose. Anatomy Nomenclature
 Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Financial disclosure I have no financial relationships to disclose. Douglas Johnson D.O. Cardiothoracic Imaging Gaston Radiology COMMON DIAGNOSES IN HRCT High Res Chest Anatomy Nomenclature HRCT Sampling
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Lung Cancers Manifesting as Part-Solid Nodules in the National Lung Screening Trial
 Cardiopulmonary Imaging Original Research Yip et al. Lung Cancers Manifesting as Part-Solid Nodules Cardiopulmonary Imaging Original Research Rowena Yip 1 Claudia I. Henschke 1 Dong Ming Xu 1 Kunwei Li
Cardiopulmonary Imaging Original Research Yip et al. Lung Cancers Manifesting as Part-Solid Nodules Cardiopulmonary Imaging Original Research Rowena Yip 1 Claudia I. Henschke 1 Dong Ming Xu 1 Kunwei Li
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE?
 PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Correlation in histological subtypes with high resolution computed tomography signatures of early stage lung adenocarcinoma
 Original Article Correlation in histological subtypes with high resolution computed tomography signatures of early stage lung adenocarcinoma Yingying Miao 1,2 *, Jianya Zhang 1,2 *, Jiawei Zou 1,2, Qingqing
Original Article Correlation in histological subtypes with high resolution computed tomography signatures of early stage lung adenocarcinoma Yingying Miao 1,2 *, Jianya Zhang 1,2 *, Jiawei Zou 1,2, Qingqing
Pathology and Prognosis of Persistent Stable Pure Ground-Glass Opacity Nodules After Surgical Resection
 GENERAL THORACIC Pathology and Prognosis of Persistent Stable Pure Ground-Glass Opacity Nodules After Surgical Resection Sukki Cho, MD, HeeChul Yang, MD, Kwhanmien Kim, MD, and Sanghoon Jheon, MD Department
GENERAL THORACIC Pathology and Prognosis of Persistent Stable Pure Ground-Glass Opacity Nodules After Surgical Resection Sukki Cho, MD, HeeChul Yang, MD, Kwhanmien Kim, MD, and Sanghoon Jheon, MD Department
Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society
 This copy is for personal use only. To order printed copies, contact reprints@rsna.org Heber MacMahon, MB, BCh David P. Naidich, MD Jin Mo Goo, MD, PhD Kyung Soo Lee, MD, PhD Ann N. C. Leung, MD John R.
This copy is for personal use only. To order printed copies, contact reprints@rsna.org Heber MacMahon, MB, BCh David P. Naidich, MD Jin Mo Goo, MD, PhD Kyung Soo Lee, MD, PhD Ann N. C. Leung, MD John R.
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The Maine Lung Cancer Coalition. Working Together to Reduce Lung Cancer in Maine
 The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
Uniportal video-assisted thoracoscopic surgery segmentectomy
 Case Report on Thoracic Surgery Page 1 of 5 Uniportal video-assisted thoracoscopic surgery segmentectomy John K. C. Tam 1,2 1 Division of Thoracic Surgery, National University Heart Centre, Singapore;
Case Report on Thoracic Surgery Page 1 of 5 Uniportal video-assisted thoracoscopic surgery segmentectomy John K. C. Tam 1,2 1 Division of Thoracic Surgery, National University Heart Centre, Singapore;
Right infrahilar nodule
 Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
CT Screening for Lung Cancer: Frequency and Significance of Part-Solid and Nonsolid Nodules
 Claudia I. Henschke 1 David F. Yankelevitz 1 Rosna Mirtcheva 1 Georgeann McGuinness 2 Dorothy McCauley 1 0lli S. Miettinen 3 for the ELCAP Group Received June 19, 2001; accepted after revision November
Claudia I. Henschke 1 David F. Yankelevitz 1 Rosna Mirtcheva 1 Georgeann McGuinness 2 Dorothy McCauley 1 0lli S. Miettinen 3 for the ELCAP Group Received June 19, 2001; accepted after revision November
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
Lung tumors & pleural lesions
 Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung Cancer Associated with Cystic Airspaces: Don t Let This Lesion Fool You!
 Lung Cancer Associated with Cystic Airspaces: Don t Let This Lesion Fool You! Annemie Snoeckx Antwerp University Hospital, University of Antwerp, Belgium Head of Department: Prof. dr. Paul M. Parizel June
Lung Cancer Associated with Cystic Airspaces: Don t Let This Lesion Fool You! Annemie Snoeckx Antwerp University Hospital, University of Antwerp, Belgium Head of Department: Prof. dr. Paul M. Parizel June
Lecture Goals. Lung (Bronchogenic) Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic
 Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic") Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Invasive Pulmonary Adenocarcinomas versus Preinvasive Lesions Appearing as Ground-Glass Nodules: Differentiation by Using CT Features 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Sang Min Lee, MD
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Sang Min Lee, MD
C2 COMPLETION INSTRUCTIONS
 The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer?
 CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer? Diagnosis and Management of Lung Cancer, 3rd
CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer? Diagnosis and Management of Lung Cancer, 3rd
The IASLC/ATS/ERS classification of lung adenocarcinoma-a surgical point of view
 Review Article The IASLC/ATS/ERS classification of lung adenocarcinoma-a surgical point of view Wentao Fang 1, Yangwei Xiang 1, Chenxi Zhong 1, Qunhui Chen 2 1 Department of Thoracic Surgery, 2 Department
Review Article The IASLC/ATS/ERS classification of lung adenocarcinoma-a surgical point of view Wentao Fang 1, Yangwei Xiang 1, Chenxi Zhong 1, Qunhui Chen 2 1 Department of Thoracic Surgery, 2 Department
Current Approach to Screening for Lung Cancer. James R Jett M.D.
 Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Characteristics of Subsolid Pulmonary Nodules Showing Growth During Follow-up With CT Scanning
 CHEST Original Research Characteristics of Subsolid Pulmonary Nodules Showing Growth During Follow-up With CT Scanning Haruhisa Matsuguma, MD ; Kiyoshi Mori, MD ; Rie Nakahara, MD ; Haruko Suzuki, MD ;
CHEST Original Research Characteristics of Subsolid Pulmonary Nodules Showing Growth During Follow-up With CT Scanning Haruhisa Matsuguma, MD ; Kiyoshi Mori, MD ; Rie Nakahara, MD ; Haruko Suzuki, MD ;
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan
 What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
What to Do with Small Lung Nodules Hanh Vu Nghiem, MD William Beaumont Hospital Royal Oak, Michigan Small Lung Nodules What to do with small lung nodules? We biopsy them when requested What are our accuracy
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Spectrum of Radiological Findings in Bronchogenic Carcinoma A Retrospective Study
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. VIII January. (2018), PP 43-59 www.iosrjournals.org Spectrum of Radiological Findings
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 01 Ver. VIII January. (2018), PP 43-59 www.iosrjournals.org Spectrum of Radiological Findings
Volume and Mass Doubling Times of Persistent Pulmonary Subsolid Nodules Detected in Patients without Known Malignancy 1
 Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Original Research
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights. Original Research
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times
 Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times Andrea Borghesi, MD Davide Farina, MD Roberto Maroldi, MD Department of Radiology University of Brescia Brescia,
Small Pulmonary Nodules: Our Preliminary Experience in Volumetric Analysis of Doubling Times Andrea Borghesi, MD Davide Farina, MD Roberto Maroldi, MD Department of Radiology University of Brescia Brescia,
THORACIK RICK. Lungs. Outline and objectives Richard A. Malthaner MD MSc FRCSC FACS
 THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
THORACIK RICK Outline and objectives Lungs Management of a solitary lung nodule Mediastinum Management of a mediastinal mass Pleura Management of a pleural fluid & pneumothorax Esophagus & Stomach Management
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!!
 The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
Diagnostic challenge: Sclerosing Hemangioma of the Lung. Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and
 Diagnostic challenge: Sclerosing Hemangioma of the Lung. S. Arias M.D, R. Loganathan M.D, FCCP Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and Mental Health Center/Weill
Diagnostic challenge: Sclerosing Hemangioma of the Lung. S. Arias M.D, R. Loganathan M.D, FCCP Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and Mental Health Center/Weill
Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule
 Original Article Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule Xuan Zhang*, Hong-Hong Yan, Jun-Tao Lin, Ze-Hua Wu, Jia Liu, Xu-Wei Cao, Xue-Ning Yang From
Original Article Comparison of three mathematical prediction models in patients with a solitary pulmonary nodule Xuan Zhang*, Hong-Hong Yan, Jun-Tao Lin, Ze-Hua Wu, Jia Liu, Xu-Wei Cao, Xue-Ning Yang From
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Lung imaging. Sebastian Ley 1,2
 CLINICAL YEAR IN REVIEW LUNG IMAGING Lung imaging Sebastian Ley 1,2 Affiliations: 1 Dept of Diagnostic and Interventional Radiology, Chirurgische Klinik Dr. Rinecker, Munich, Germany. 2 Dept of Clinical
CLINICAL YEAR IN REVIEW LUNG IMAGING Lung imaging Sebastian Ley 1,2 Affiliations: 1 Dept of Diagnostic and Interventional Radiology, Chirurgische Klinik Dr. Rinecker, Munich, Germany. 2 Dept of Clinical
10/17/2016. Nuts and Bolts of Thoracic Radiology. Objectives. Techniques
 Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Nuts and Bolts of Thoracic Radiology October 20, 2016 Carleen Risaliti Objectives Understand the basics of chest radiograph Develop a system for interpreting chest radiographs Correctly identify thoracic
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
MANAGEMENT RECOMMENDATIONS
 1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms
 Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Original Research Article Role of CT imaging to evaluate solitary pulmonary nodule with extrapulmonary neoplasms Anand Vachhani 1, Shashvat Modia 1*, Varun Garasia 1, Deepak Bhimani 1, C. Raychaudhuri
Mediastinal Tumors: Imaging
 Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
I8 COMPLETION INSTRUCTIONS
 The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
Common Blind Spots on Chest CT: Where Are They All Hiding? Part 1 Airways, Lungs, and Pleura
 Residents Section Structured Review Wu et al. Common lind Spots on Chest CT Residents Section Structured Review Carol C. Wu 1 Leila Khorashadi 2 Gerald F. bbott 1 Matthew D. Gilman 1 Wu CC, Khorashadi
Residents Section Structured Review Wu et al. Common lind Spots on Chest CT Residents Section Structured Review Carol C. Wu 1 Leila Khorashadi 2 Gerald F. bbott 1 Matthew D. Gilman 1 Wu CC, Khorashadi
Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D.
 Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D. Lung Cancer 219,440 new cases/year in U.S. (2009) 169,390 deaths/year in U.S. mortality greater than from breast, colon, prostate CA combined
Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D. Lung Cancer 219,440 new cases/year in U.S. (2009) 169,390 deaths/year in U.S. mortality greater than from breast, colon, prostate CA combined
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
A Chronology of Advancements in the Diagnosing of Lung Nodules
 November 17, 2017 A Chronology of Advancements in the Diagnosing of Lung Nodules Presenter: Daniel P. Harley, MD, MSB, FACS Surgical Director of the Angelos Center for Lung Diseases 1 Pulmonary Nodules
November 17, 2017 A Chronology of Advancements in the Diagnosing of Lung Nodules Presenter: Daniel P. Harley, MD, MSB, FACS Surgical Director of the Angelos Center for Lung Diseases 1 Pulmonary Nodules
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory