Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
|
|
|
- Gabriella Waters
- 6 years ago
- Views:
Transcription
1 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
2 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium Routine colonoscopy screening Multiple polyps Pathology Diminutive transverse colon polyp tubular adenoma 2.5 cm sessile sigmoid polyp tubulovillous adenoma with foci of invasive adenocarcinoma Diminutive rectosigmoid polyp, and three 4 mm sigmoid polyps serrated adenoma
3 Despite negative margins, concern for draining lymph node bed Repeat colonoscopy for removal of remaining polyps and tattooing of site of invasive carcinoma for surgery Pathology 4 mm cecal polyp, 4 mm descending colon polyp tubular adenoma Remnant of previous 2.5 cm polyp benign Two flat sigmoid polyps hyperplastic polyps One flat sigmoid polyp sessile
4 Presented to hospital for elective sigmoid resection Operative findings Tattooed area of sigmoid with no palpable mass Large and thick omentum; difficulty in identifying safe plane of dissection at splenic flexure Procedure: laparoscopic converted to open sigmoidectomy with primary end-to-end anastomosis, repair of bladder dome injury EBL=100 ml
5 Postoperatively Extubated POD#1 Flatus on POD#3 and diet started and advanced as tolerated Discharged home on POD#6 with Foley Pathology: no malignancy; 9 LN negative
6 NEOPLASTIC POLYPS Background Risk factors Treatment Screening for colorectal cancer
7 BACKGROUND Adenomas, serrated adenomas Occur in 33% of population by age 50, 50% by age 70 60% adenomatous polyps are distal to splenic flexure Synchronous adenomas in 40%
8 Adenoma-carcinoma causal relationship Almost all colon cancer arises within an adenoma 30% incidence of residual adenomas in specimens Risk of cancer increases with larger and more polyps High incidence of cancer in familial adenomatous polyposis syndrome Risk of cancer is 4% after 5 years and 14% after 10 years
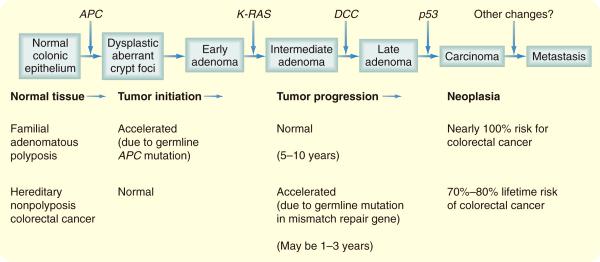
9 Pathways Traditional Begins with APC tumor suppressor gene on chromosome 5q for β-catenin adenoma DCC tumor suppressor gene on chromosome 18 with neural cell adhesion molecule and alteration in apoptosis more advanced adenoma p53 tumor suppressor gene on chromosome 17 for cell cycle arrest or apoptosis for DNA damage carcinoma K-ras oncogene on chromosome 12 for signal transduction, increased replication and exophytic growth
10
11 Serrated pathway Begins with BRAF oncogene mutation in serine-threonine kinase signaling DNA methylation, microsatellite instability Elderly women, smokers Larger, sessile, right colon polyps Mix of hyperplastic and adenomatous features
12 RISK FACTORS Histologic variants Tubular adenoma <5% malignant Tubulovillous adenoma 20-25% malignant Villous adenoma 35-40% malignant
13 Size Diminutive = <6 mm - <0.5% malignant <1 1-2% malignant >2 cm up to 40% malignant
14 Shinya et al. Ann Surg
15 Dysplasia Mild 5.7% malignant Moderate 18% malignant Severe 34.5% malignant 5-7% adenomatous polyps have high-grade dysplasia; 3-5% have invasive carcinoma Have not yet invaded through muscularis mucosa so if completely excised, patient is cured

16 Haggitt level for polypoid lesions Invasion into submucosa with increased risk of carcinoma, lymph node metastasis, cancer-related mortality
17 KiKuchi classification for sessile lesions Sm1 = slight invasion of submucosa, µm Sm2 = intermediate invasion Sm3 = deep submucosal invasion to inner surface of muscularis propria Mayo Clinic series, 23% risk of LN mets
18 Risk for lymph node metastasis is 8-15% in malignant polyps Unfavorable pathologic features: Submucosal invasion, Haggitt level 4 Poor differentiation, high-grade dysplasia Tumor budding - clusters of malignant cells away from main site of submucosal invasion Lymphovascular invasion Resection margin <2 mm
19 TREATMENT Complete colonoscopy with polypectomy
20 National Polyp Study Winawer et al. NEJM 1993
21 National Polyp Study Adenomas progress into invasive adenocarcinoma Search and remove polyps to prevent adenocarcinoma
22 More recently Polypectomy leads to 53% reduction in colorectal cancer mortality Zauber et al. NEJM 2012.
23 Polypectomy technique Biopsy (<5 mm) Snare Piecemeal excision Endoscopic mucosal resection (EMR)

24 EMR Saline injection into submucosal plane, suction cautery attachment, snare polypectomy For small (<1cm), flat / depressed lesions Curative for early cancers without LVI or capable of harboring a focal cancer If large, sessile, villous, then surgical resection
25 Adverse outcomes in polypectomy Risk of death is 1 in Bleeding in 4.8 per 1000 Perforation in up to 1 in 1000 Post-polypectomy syndrome in up to 3 in 1000 Cautery injury with microperforation and bacterial translocation Abdominal pain, fever, leukocytosis
26 Resection margin If negative margin and no unfavorable pathologic feature, 0.8% risk of adverse outcome (residual carcinoma, recurrence, lymph node metastasis, decreased survival) If negative margin but have unfavorable pathologic feature, 18% risk of adverse outcome If +/indeterminate margins, 27% have adverse outcome
27 Contraindications to polypectomy Signs of invasive malignancy (fungating, ulcerated, distorted, necrosis, involves surrounding bowel wall) Relative: bleeding diathesis, acute colitis Indication for colectomy Contraindication to polypectomy High risk pathologic features despite complete polypectomy (margin <3 mm, poor differentiation, LVI, Haggitt level 4)
28 SCREENING Initial screening Fecal occult blood testing (FOBT) Sigmoidoscopy 60 cm; use with FOBT or double barium enema study Every 5 years; if positive, colonoscopy Colonoscopy

29 Double contrast barium enema (DCBE) For polyps >1 cm For those who refuse or unable to have full colonoscopy Paired with flex sigmoidoscopy Every 5 years; if positive, colonoscopy Glick. AJR 2000



30 CT colonography = virtual colonoscopy Air-distended, prepped colon Identified 90% lesions >10 mm Every 5 years; if positive, colonoscopy Johnson et al. NEJM 2008 Yucel et al. AJR 2008
31 Risk Category Average risk, asymptomatic (Age >50, consider >45 for African Americans) 1 st degree relative with CRC, adenomatous polyps at age <60 Two 2 nd degree relatives with CRC Gene carrier or at risk for FAP Gene carrier or at risk for HNPCC Initial Screening FOBT each year Flexible sigmoidoscopy every 5 years Colonoscopy every 5-10 years CT colonography every 5-10 years Same as for average risk but starting at age 40 Colonoscopy every 5 years at age 40, or 10 years younger than age of earliest diagnosis in family Flexible sigmoidoscopy each year, starting at age Colonoscopy every year, starting at age 20-25, or 10 years younger than age of earliest diagnosis in family MD Anderson Surgical Oncology Handbook, 5 th edition, 2012
32 Surveillance screening after polypectomy Current Surgical Therapy, 10 th edition
33 CONCLUSIONS Risk factors for malignancy include histology, size, and depth of invasion Polypectomy reduces incidence and mortality from colorectal cancer Past medical history and family history help direct appropriate screening for polyps
34 QUESTIONS 1. The appropriate screening strategy for a 50 year old man with no family history of colon cancer and a sibling with adenomatous polyps removed at age 50 would be to begin a. Colonoscopy at age 30, repeated every 2 years b. Colonoscopy at age 40, repeated every 5 years c. Sigmoidoscopy and fecal occult testing at age 40, repeated every 5 years d. Colonoscopy at age 50, repeated every 10 years e. Sigmoidoscopy and fecal occult testing at age 50, repeated every 5 years
35 2. Findings at colonoscopy that indicate decreased interval for screening are all except a. Adenomatous polyp >1 cm b. Nonserrated hyperplastic rectal polyp c. >3 adenomatous polyps d. Villous adenoma e. Sessile polyp removed piecemeal
36 3. A 60 year old woman had 2 polyps removed from the left colon during screening colonoscopy. She began having left abdominal pain at night, especially when lying on her left side or coughing. Which is not true? a. Previous abdominal operation is a risk factor b. Symptoms typically occur within 24 hours after colonoscopy c. Abdominal plain film is the radiologic study of choice d. Splenic injury can be managed nonoperatively e. Hypotension suggests a splenic injury
37 That s all, folks! Thank you
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING
 CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Cancer Screening. Layth Al-Jashaami, MD GI Fellow, PGY 4
 Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Historical. Note: The parenthetical numbers in the Clinical Indications section refer to the source documents cited in the References Section below.
 Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Colon Cancer Screening
 July 2005 Colon Cancer Screening Ning Tang, HMS IV Objectives Background on incidence and death rates from colon cancer Present recent patient cases of colon cancer, and the radiographic findings Discuss
July 2005 Colon Cancer Screening Ning Tang, HMS IV Objectives Background on incidence and death rates from colon cancer Present recent patient cases of colon cancer, and the radiographic findings Discuss
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Research Article Endoscopic Management of Nonlifting Colon Polyps
 Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
Clinical UM Guideline
 Subject: Guideline #: Current Effective Date: 06/28/2016 Status: Revised Last Review Date: 05/05/2016 Description This document addresses colonoscopy, an endoscopic procedure which allows direct visual
Subject: Guideline #: Current Effective Date: 06/28/2016 Status: Revised Last Review Date: 05/05/2016 Description This document addresses colonoscopy, an endoscopic procedure which allows direct visual
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
ACG Clinical Guideline: Colorectal Cancer Screening
 ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
AMSER Rad Path Case of the Month: December 2018
 AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
BC CRC Update Malignant Polyp Who Needs Surgery
 BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
Guidelines for Breast, Cervical and Colorectal Cancer Screening
 Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Colorectal Cancer Screening: A Clinical Update
 11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
Colonoscopy MM /01/2010. PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
 of Service: Outpatient") Colonoscopy Policy Number: Original Effective Date: MM.12.003 12/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
Colonoscopy Policy Number: Original Effective Date: MM.12.003 12/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.
: Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.") Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Summary. Cezary ŁozińskiABDF, Witold KyclerABCDEF. Rep Pract Oncol Radiother, 2007; 12(4):
:") Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic. Scott Rieder Dr. Colquhoun
 Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH
 Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Colorectal Cancer Screening. Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital
 Colorectal Cancer Screening Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital March, 2018 CRC Epidemiology 4th most common malignancy in US (136,000 cases/yr) 2nd
Colorectal Cancer Screening Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital March, 2018 CRC Epidemiology 4th most common malignancy in US (136,000 cases/yr) 2nd
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer
 Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
2. Describe pros/cons of screening interventions (including colonoscopy, CT colography, fecal tests)
") Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Colorectal Cancer Screening
 Scan for mobile link. Colorectal Cancer Screening What is colorectal cancer screening? Screening examinations are tests performed to identify disease in individuals who lack any signs or symptoms. The
Scan for mobile link. Colorectal Cancer Screening What is colorectal cancer screening? Screening examinations are tests performed to identify disease in individuals who lack any signs or symptoms. The
Colorectal Cancer Prevention Quantity and Quality Count
 Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
Colorectal Cancer Screening and Surveillance
 Medical Coverage Policy Effective Date...10/15/2017 Next Review Date...10/15/2018 Coverage Policy Number... 0148 Colorectal Cancer Screening and Surveillance Table of Contents Related Coverage Resources
Medical Coverage Policy Effective Date...10/15/2017 Next Review Date...10/15/2018 Coverage Policy Number... 0148 Colorectal Cancer Screening and Surveillance Table of Contents Related Coverage Resources
Colorectal Cancer Screening
 Recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer Colorectal Cancer Screening Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D, Robertson
Recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer Colorectal Cancer Screening Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D, Robertson
Carol A. Burke, MD, FACG
 Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Colonic adenomas-a colonoscopy survey
 Gut, 1979, 20, 240-245 Colonic adenomas-a colonoscopy survey P. E. GILLESPIE, T. J. CHAMBERS, K. W. CHAN, F. DORONZO, B. C. MORSON, AND C. B. WILLIAMS From St Mark's Hospital, City Road, London SUMMARY
Gut, 1979, 20, 240-245 Colonic adenomas-a colonoscopy survey P. E. GILLESPIE, T. J. CHAMBERS, K. W. CHAN, F. DORONZO, B. C. MORSON, AND C. B. WILLIAMS From St Mark's Hospital, City Road, London SUMMARY
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
CRC Risk Factors. U.S. Adherence Rates Cancer Screening. Genetic Model of Colorectal Cancer. Epidemiology and Clinical Consequences of CRC
 10:45 11:45 am Guide to Colorectal Cancer Screening SPEAKER Howard Manten M.D. Presenter Disclosure Information The following relationships exist related to this presentation: Howard Manten MD: No financial
10:45 11:45 am Guide to Colorectal Cancer Screening SPEAKER Howard Manten M.D. Presenter Disclosure Information The following relationships exist related to this presentation: Howard Manten MD: No financial
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
what is the alternative mechanism of histogenesis? Aspects of the morphology of the adenomacarcinoma Morphology of the
 Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Malignant colorectal polyps: venous invasion and
 774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
Colorectal Cancer Screening and Surveillance
 1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
Colorectal Cancer. Mark Chapman. MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist
 21 st March 2018 Consultant Coloproctologist") Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Improving Outcomes in Colorectal Cancer: The Science of Screening. Colorectal Cancer (CRC)
") Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Colorectal Cancer Screening. Dr Kishor Muniyappa 2626 Care Drive, Suite 101 Tallahassee, FL Ph:
 Colorectal Cancer Screening Dr Kishor Muniyappa 2626 Care Drive, Suite 101 Tallahassee, FL 32308 Ph: 850-297-0351 What we ll be talking about How common is colorectal cancer? What is colorectal cancer?
Colorectal Cancer Screening Dr Kishor Muniyappa 2626 Care Drive, Suite 101 Tallahassee, FL 32308 Ph: 850-297-0351 What we ll be talking about How common is colorectal cancer? What is colorectal cancer?
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE RISK OF RESIDUAL CANCER AND LYMPH NODE METASTASIS
 253SJS102210.1177/1457496913482253S. E. Steigen, et al.adenomas with adenocarcinomas and risk factors Scandinavian Journal of Surgery 102: 90 95, 2013 ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE
253SJS102210.1177/1457496913482253S. E. Steigen, et al.adenomas with adenocarcinomas and risk factors Scandinavian Journal of Surgery 102: 90 95, 2013 ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE
Incidence and Multiplicities of Adenomatous Polyps in TNM Stage I Colorectal Cancer in Korea
 Original Article Journal of the Korean Society of J Korean Soc Coloproctol 2012;28(4):213-218 http://dx.doi.org/10.3393/jksc.2012.28.4.213 pissn 2093-7822 eissn 2093-7830 Incidence and Multiplicities of
Original Article Journal of the Korean Society of J Korean Soc Coloproctol 2012;28(4):213-218 http://dx.doi.org/10.3393/jksc.2012.28.4.213 pissn 2093-7822 eissn 2093-7830 Incidence and Multiplicities of
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
Colorectal Cancer: Screening & Surveillance
 Objectives Colorectal Cancer: Screening & Surveillance Chanda K. Ho, MD MPH Advances in Internal Medicine Brief overview epidemiology and pathogenesis of colorectal cancer (CRC) To review screening modalities
Objectives Colorectal Cancer: Screening & Surveillance Chanda K. Ho, MD MPH Advances in Internal Medicine Brief overview epidemiology and pathogenesis of colorectal cancer (CRC) To review screening modalities
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
CRC and Endoscopy. Objectives. Background
 CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
T colonoscopy (Fig. 1) which permits direct
 which permits direct") FLEXIBLE COLONOSCOPY HIROMI SHINYA, MD,* AND WILLIAM WOLFF, MD~ Colonoscopy with fiberoptic instruments has opened new vistas in diagnosis and treatment of colonic disease. Such endoscopy requires skill,
FLEXIBLE COLONOSCOPY HIROMI SHINYA, MD,* AND WILLIAM WOLFF, MD~ Colonoscopy with fiberoptic instruments has opened new vistas in diagnosis and treatment of colonic disease. Such endoscopy requires skill,
Neoplasms of the Colon and of the Rectum
 Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias