MALIGNANT MELANOMA. Dr D. Tenea Department of Dermatology University of Pretoria
|
|
|
- Irma Preston
- 6 years ago
- Views:
Transcription
1 MALIGNANT MELANOMA Dr D. Tenea Department of Dermatology University of Pretoria
2 BACKGROUND History MM. of the skin is a malignant neoplasm of the epidermal melanocytes The incidence rates show considerable variation between the countries: - Australia/New Zealand high incidence (50 cases /100,000inhabit.) - Sweden/ UK/ USA / Netherlands medium incidence (10-20 cases/ per inhabitants ) - Most Western-Eastern European countries 4-10 cases / No. of deaths due to MM. has increased for the past decades and continue to rise in most fair skinned populations throughout the world Mortality rates have not risen as quickly as the incidence of melanoma ( mortality rates in older males ; mortality in middle-aged women & young individuals )
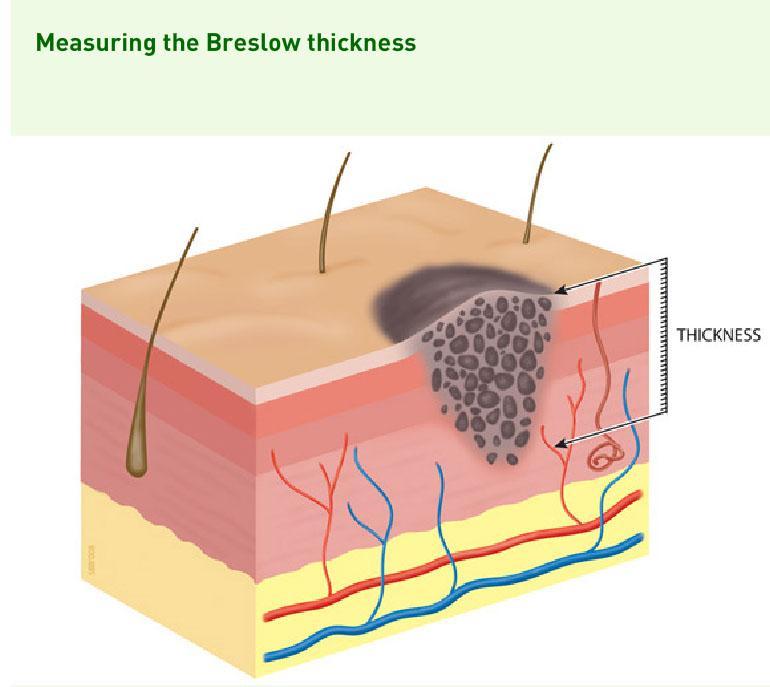
3 Why is early detection of Melanoma worthwhile History? The stage of initial Dx. determines the patient`s chance of survival There is a direct relationship between the depth of tumor ( Breslow thickness ) and the chances of survival Increased knowledge about the early signs and symptoms of MM in the public and in primary health care workers important 20% melanoma patients have recurrence of their disease ( Pts. with thicker melanomas ) Rationale for screening of melanoma identification of high risk population Melanoma writes its message in the skin with its own ink and is there for all to see it
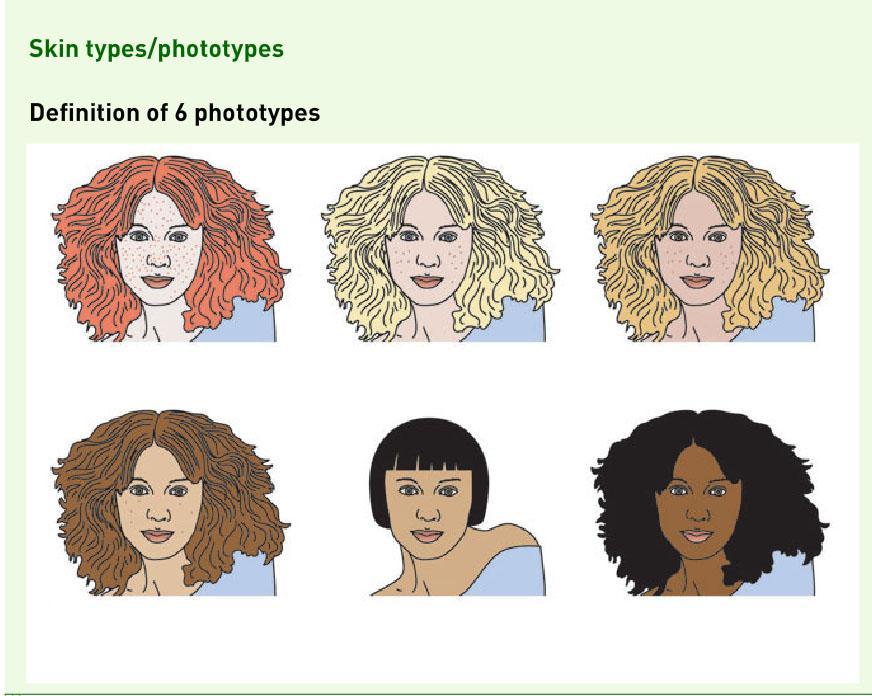
4 RISK FACTORS History There is no single cause of melanoma ( multifactorial ) The development of MM occurs as a result of interaction between the environmental factors and individual ( host ) factors : Environmental factors : sun exposure in childhood - No. of sunburns in childhood / adolescence - Intermittent high exposure during holidays Host factors : Genetic factors ( mutations in CDKNA2 gene ; many variants of MC1R gene detected ) Family History - Genetic diseases : XP, OCA (Albinism) - Skin type / phenotype ( Fitzpatrick scale 6 ) - Many banal melanocytic naevi ( > 50) - Congenital naevi > 5 ; AMN > 5 / DNS
5
6 Risk Factors Ctd. History Handy mnemonic is MM RISK : M : Moles ( multiple atypical moles ) M : Moles ( numerous common moles + moles present at birth ) R : Red hair, fair skin, blue eyes, freckling I : Inability to tan : skin phenotype I II S : Sunburn severe sunburn < age of 15 years K : Kindred family Hx. of MM in first degree relatives Melanoma in children very rare ( Spitz nevus or Juvenile Melanoma) Melanoma diagnosed in Pregnancy poor prognosis?
7 Melanoma Growth Pattern History Majority of MM have a radial growth phase ( in situ / microinvasive) before the development of vertical growth phase Body sites involved ( primaries ): Skin ( 90% ) Ocular ( 2% ) conjunctiva, sclera Other mucosal membranes(1%): anus,oral Visceral < 0.1% (adrenals, lung, esophagus Nail ( subungual) < 1% Unknown primary ( 5%) BANS areas : back, arms, neck, scalp poor prognosis Amelanotic Melanoma (absence of pigment) poorly differentiated state Depigmented haloes Not a diagnostic feature of melanoma
8 CLINICO-PATHOLOGICAL VARIANTS History OF MELANOMA There are 5 classic clinical subtypes of MM each having typical features 1. Superficial spreading MM (70%) develops slowly, from a pre-existing AMN, in people aged years 2. Nodular MM (20%) fast growing (within a few months) often de novo, in people aged yr. 3. Lentigo Maligna Melanoma (5%) develop very slowly from a lentigo maligna on sun damaged skin, in people > 65yr. (elderly) 4. Acrolentiginous Melanoma (5%) most common type in Blacks ; located on hands, feet, nails 5. Mucosal MM (1%) more often seen in Blacks (ocular, anal, vagina, oral mucosa) ; late Dx. ; younger / middle age group
9 UNUSUAL TYPES OF MELANOMA History 1. Amelanotic Melanoma nodular or polypoid, late Dx, poor prognosis ulceration is common 2. Desmoplastic Melanoma sun exposed skin, more often in white men, flat-pigmented patch or an amelanotic papule ; late Dx, poor prognosis ; tendency to local recurrence 3. Malignant Blue Naevus white men > 45yr, scalp, nodule/plaque >2cm 4. Naevus of Ota associated Melanoma (ophthalmo-maxilaris )+ mucosal involvement (ocular, palate, nasal/tympanic mucosa) 5. Subungual Melanoma Blacks : 20-31% over age of 60yr, brown longitudinal nail band, mainly on thumb
10 CLINICAL ASSESSMENT OF MALIGNANT History MELANOMA Assess the skin phenotype and the extend of sun damage Estimate the total No. of moles and presence/absence of AMN Measure the diameter of a changing mole + monitor the colour, borders, presence/absence of Ulceration Check whether a mole is different from other moles (ugly duckling sign) Apply ABCDE rule or 7 point-checklist for early detection of melanoma A asymmetry B borders (irregular) C colour variation D diameter >7 mm E elevation of formerly flat lesion or evolution ( change )
11 CLINICAL ASSESSMENT OF MALIGNANT History MELANOMA Ctd. Recently F was added standing for : Feeling (itching, stinging,burning or for Funny Mole ( ugly Duckling `sign) 7 point-checklist emphasis on changing mole in adulthood : - Major features : change in size (1), shape (2), colour (3) - Minor features : diameter > 7mm (1), inflammation (2),oozing/crusting bleeding (3), changing in sensation (4) 1 Major Criterion or 3 Minor Criteria are fulfilled Melanoma (see Dr. within a few weeks ) What determines how long a melanoma will remain in situ is not clear? (combination of factors)
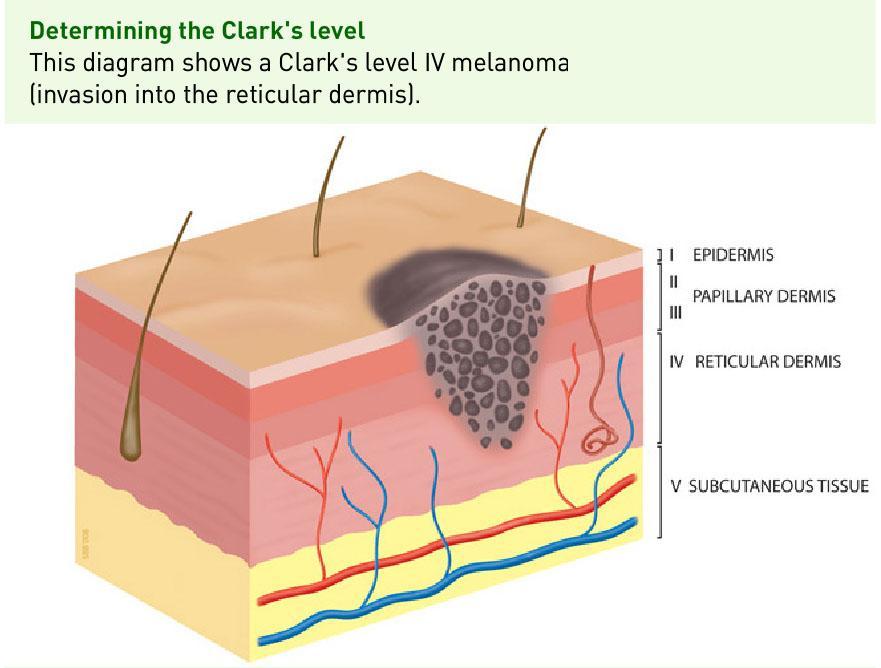
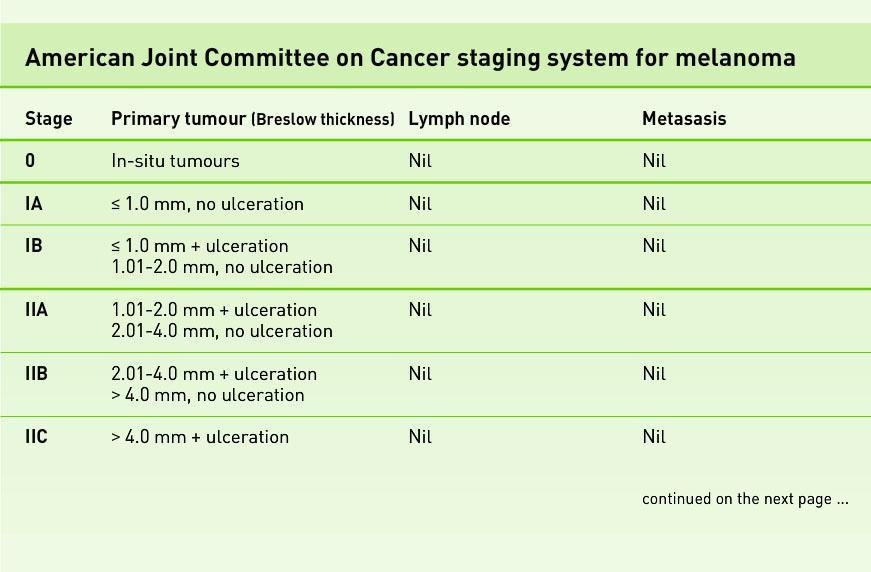
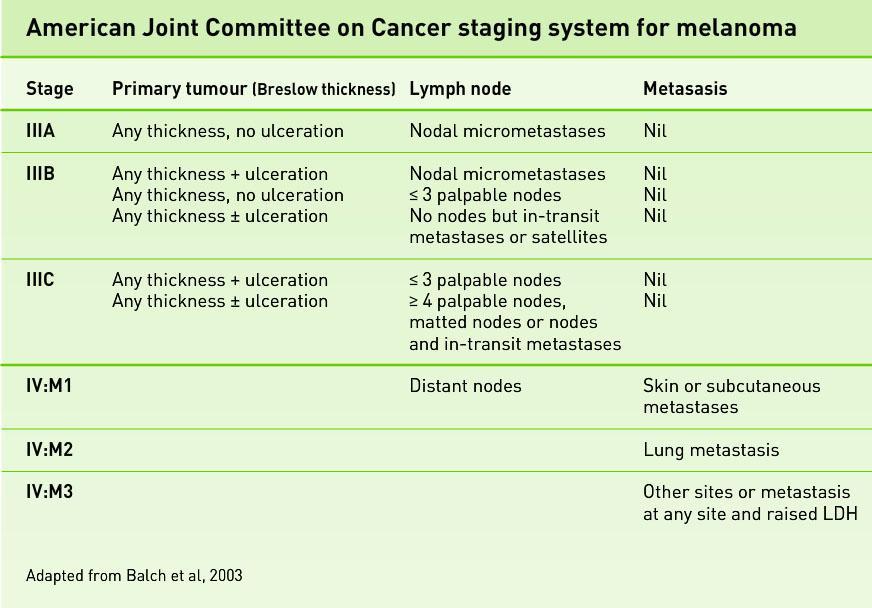
12 STAGING OF MELANOMA History The Breslow depth is the most important prognostic factor in Melanoma, with stratification cutoffs of <1mm, mm, mm, >4mm in the revised 2002 AJCC melanoma staging Ulceration is the next most important adverse prognostic feature (its presence upstages the patient into the next worst prognostic level) The number of LN involved is a powerful predictor of survival Sentinel LN status is the most important prognostic factor for recurrence and predictor of survival Clark`s pathological level of invasion in the skin is useful in staging very thin melanomas
13
14
15 STAGING OF MELANOMA Ctd. History The stage of Melanoma in an individual patient results from Clinical Examination + Histopathology of Tumor specimen + Sentinel LN investig. No further investigations ( X-Rays, CT-scans, MRI scans) Stages I & II There is no consensus of further investigations in advanced stages Serum LDH levels may indicate metastases (low specificity / sensitivity) is useful in TX of stage IV (disseminated) disease Total body CTscans + liver/brain/bone imaging Not useful in detecting occult melanoma metastasis in asymptomatic patients
16
17
18 APPROACH TO THE EARLY DETECTION History OF MELANOMA Educating people about early warning signs and self-examination Screening of selected high-risk individuals (family Hx. of melanoma) Training of Primary Health Care Workers Using ABCDEF rule / 7-point-checklist Setting up dedicated Pigmented Lesion Clinics (PLC) Primary prevention by educating people about risks of UV radiation is essential to reduce the chances of developing Melanoma When should you refer a patient? 1. When there is a high index of suspicion of MM 2. When the lesion is large & complete excision would be disfiguring 3. Patients with multiple AMN/ changing mole/ Family Hx. of MM
19 Characteristics History of Familial Melanomas FAMMM Syndrome = Familial Atypical Multiple Mole Melanoma ( many individuals with atypical moles and melanomas within a family) MM tend to occur at a younger age People are more likely to have multiple melanomas MM usually develop from precursor lesions (AMN) Other cancer types may be associated ( pancreatic cancer ) Familial Melanoma is the most important indicator of melanoma risk for an individual A positive family history of one MM increases the patient`s risk 10X
20 MANAGEMENT History Use of Sunscreens controversial ( protective role vs. risk of MM ) Use of Sunbeds + Sunlamps same adverse effect on skin as solar UV rad. Avoid sun exposure between 11 AM 15 hr. PM (children + adolescents) Planning out-door activities in the mornings/ evenings No prospective data exist regarding appropriate margins for melanomas thicker than 4mm (margins > 2cm have no effect on recurrence/survival) Surgical margins of 5mm melanoma in situ Surgical margins of 1 cm for MM up to 2mm depth Intermediate thickness tumors (1-4mm) 2cm margins Wider margins may be necessary to achieve local control (head/neck, hands/feet melanomas)
21 MANAGEMENT Ctd. History Stage II B, IIC, III melanomas surgical excison with 2cm margins + block dissection of the draining LN and IFN-alfa for 1yr. Post-surgery Stage III and Stage IV are suitable for Chemotherapy combined with Immunotherapy: Dacarbazine, Cisplatin or Texanes( Docetaxel)+ IFN Combination Chemotherapy (CVD) + IFN + IL % response Intra arterial Chemotherapy ( Melphalan) in transit metastases Vaccines are currently being investigated for therapeutic use in patients with Extracutaneous Melanoma( survival advantage with vaccines?)
22 CUTANEOS T-CELL LYMPHOMA ( Mycosis Fungoides ) Misnomer ( coined by Alibert ) Peripheral non-hodgkin T-cell lymphoma Indolent course ( develops slowly over many years ) Unknown aetiology ( controversies about HTLV-1, HIV, HHV-8, occupational exposure ) Urban areas > rural areas Males > Females Age : Mid /late adulthood Blacks > Caucasians Gradual progression from patches plaques - tumours
23 Mycosis Fungoides Ctd. Clinical presentation : unusual forms of eczema / psoriasis ( failure to Tx.) Predilection : photoprotected areas ( trunk, thighs, buttocks ) Very pruritic lesions Prognosis of early stage MF variable Progression means skin involvement + extracutaneous involvement ( LN, hepato-splenomegaly, bone marrow infiltration, peripheral blood atypical Lf. > 5% ) Diagnosis : Skin biopsy + immunohist. stains Treatment : PUVA, Re-PUVA, topical steroids,bexaroten (patch stage ) Localised Radiotherapy / Electron beam radiation (plaque stage) Chemotherapy ( CHOP ) tumour stage
24 TNMB classification for CTCL History T T0 Nondiagnostic (eg. Parapsoriasis ) T1 Limited patch/plaque ( < 10% total skin surface ) T2 Generalized patch/plaque ( > 10% total skin surface) T3 Tumors T4 Erythroderma N N0 Lymph nodes clinically uninvolved N1 Lymph nodes enlarged, histologically uninvolved N2 Lymph nodes clinically uninvolved, histologically involved N3 Lymph nodes enlarged and histologically involved
25 TNMB classification Ctd. History M M0 No visceral involvement M1 Visceral involvement B B0 Circulating atypical / Sezary cells < 5% of lymphocytes B1 Circulating atypical / Sezary cells > 5% of lymphocytes Adverse prognostic factors: - Age > 60 years - Type and extension of skin involvement ( tumor >plaque > patch ) - >5% Sezary cells or atypical lymphocytes in the peripheral blood - Increased serum-ldh levels - Palpable lymphadenopathy ( poor prognostic sign : LN3 and LN4 ) - Bone marrow involvement ( occurs in the advanced stage of disease) - Transformation into a large cell lymphoma
26 CUTANEOUS METASTASES Neoplastic lesion arising from another neoplasm with which is no longer in continuity Skin metastases are uncommon ( 1-2% ) Portend a grave prognosis ( survival 3-6 months ) Mode of spread : -direct invasion, local metastases (contiguous extension ), distant metastases, accidental implantation during surgery Tend to occur near the site of the primary tumour Metastases may occur at radiation site, in surgical scars
27 METASTASES- Ctd. History Differences in localisation + different patterns of cutaneous metas. Age : elderly people ( years ) Sex differences Growth pattern of skin metastases is unpredictable and may not reflect that of primary tumour May occur concurrently with metas. to the other organs or skin involvement may be the presenting finding Cutaneous metastases may simulate other cutaneous disorders High index of suspicion maintained : - non-healing ulcers - persistent indurated erythema - unexplained skin nodules
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
VACAVILLE DERMATOLOGY
 Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Corporate Medical Policy
 Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Subject Index. Dry desquamation, see Skin reactions, radiotherapy
 Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Index. pet.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A C a-aminobutyric acid, carbon-labeled, 94 ABCD(E)s, of melanoma, 2 Acral-lentiginous melanoma, 3 Adrenal glands, metastasis to, structural imaging
Note: Page numbers of article titles are in boldface type. A C a-aminobutyric acid, carbon-labeled, 94 ABCD(E)s, of melanoma, 2 Acral-lentiginous melanoma, 3 Adrenal glands, metastasis to, structural imaging
ORAL MELANOMA Definition Epidemiology Clinical Presentation
 ORAL MELANOMA Definition Melanoma is a highly malignant neoplasia, arising from melanocytes, the cells that produce the brownish pigment melanin. Melanin is the determinant in skin colour and protects
ORAL MELANOMA Definition Melanoma is a highly malignant neoplasia, arising from melanocytes, the cells that produce the brownish pigment melanin. Melanin is the determinant in skin colour and protects
Derm quiz. Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52. bit.ly/2a8asoy. Scan the QR code with your phone
 Dermatology quiz Derm quiz Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52 OR bit.ly/2a8asoy OR Scan the QR code with your phone Contents Childhood rashes Pigmented lesions Sun damage Pityriasis References
Dermatology quiz Derm quiz Go to this link: goo.gl/forms/kchrhmtzl3vfnlv52 OR bit.ly/2a8asoy OR Scan the QR code with your phone Contents Childhood rashes Pigmented lesions Sun damage Pityriasis References
Professor Michael Eccles
 Professor Michael Eccles Developmental Genetics & Pathology Laboratory Pathology Department University of Otago Dunedin 15:00-15:15 Melanoma Metastasis and Treatment Resistance Melanoma metastasis and
Professor Michael Eccles Developmental Genetics & Pathology Laboratory Pathology Department University of Otago Dunedin 15:00-15:15 Melanoma Metastasis and Treatment Resistance Melanoma metastasis and
MELANOMA. Some people are more likely to get a m Melanoma than others:
 MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
Melanoma. Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania
 Melanoma Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania WHAT IS MELANOMA? Melanoma is a type of skin cancer (a serious skin cancer because
Melanoma Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania WHAT IS MELANOMA? Melanoma is a type of skin cancer (a serious skin cancer because
They can develop anywhere on the skin and also inside the mouth. They can develop in normal skin or where there is an existing skin mole.
 What are malignant melanomas? Malignant melanomas are one type of skin cancer. They can develop anywhere on the skin and also inside the mouth. They can develop in normal skin or where there is an existing
What are malignant melanomas? Malignant melanomas are one type of skin cancer. They can develop anywhere on the skin and also inside the mouth. They can develop in normal skin or where there is an existing
Cancer Registry Report. Cancer Focus: Melanoma
 Cancer Registry Report Cancer Focus: Melanoma In 2005, nearly 60,000 patients were diagnosed with melanoma, resulting in about 7800 deaths Fortunately, melanoma is often diagnosed in an early stage when
Cancer Registry Report Cancer Focus: Melanoma In 2005, nearly 60,000 patients were diagnosed with melanoma, resulting in about 7800 deaths Fortunately, melanoma is often diagnosed in an early stage when
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Overview of Cutaneous Lymphomas: Diagnosis and Staging. Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology
 Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Major Topic. Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星
 Major Topic Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星 Patient Data Name: OOO Age: 70 Gender: Male Date of admission: Day 1 Chief Complaint Black skin tumor at the back of the
Major Topic Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星 Patient Data Name: OOO Age: 70 Gender: Male Date of admission: Day 1 Chief Complaint Black skin tumor at the back of the
MELANOMA. 4 Fitzroy Square, London W1T 5HQ Tel: Fax: Registered Charity No.
 MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
 Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Epidemiology. Objectives 8/28/2017
 Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Melanoma. Walt Mudie - Block 5
 Melanoma Walt Mudie - Block 5 Melanoma Graphic Warning Medical names: cutaneous melanoma (melanoma of skin), intraocular melanoma (melanoma of eye) Affects mainly skin, can also affect eye, vagina or anus
Melanoma Walt Mudie - Block 5 Melanoma Graphic Warning Medical names: cutaneous melanoma (melanoma of skin), intraocular melanoma (melanoma of eye) Affects mainly skin, can also affect eye, vagina or anus
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
World Articles of Ear, Nose and Throat Page 1
 World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper:
 This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/127789/ Version: Accepted Version Article: Muinonen-Martin,
This is a repository copy of Easily missed? Amelanotic melanoma. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/127789/ Version: Accepted Version Article: Muinonen-Martin,
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Finding Melanoma. Is not easy!
 Finding Melanoma Is not easy! Finding Melanoma Victoria mean depth at diagnosis is 1.5 mm. Melanoma 1.5mm Has Stage 1B Mortality 10% Melanoma Spotting a killer! Spotting a killer Visual Clues What are
Finding Melanoma Is not easy! Finding Melanoma Victoria mean depth at diagnosis is 1.5 mm. Melanoma 1.5mm Has Stage 1B Mortality 10% Melanoma Spotting a killer! Spotting a killer Visual Clues What are
Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology
 Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology Agenda Overview of cutaneous T and B- cell lymphomas Diagnosis, Staging, Prognosis
Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology Agenda Overview of cutaneous T and B- cell lymphomas Diagnosis, Staging, Prognosis
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Index. Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, Anorectal melanoma RT for, 1035
 Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases
 Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2
 MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2 In the second part of our feature on pigmented skin lesions, dermatology specialist Dr Sweta Rai describes the steps to rational decision-making
MELANOCYTIC LESIONS: EFFECTIVE MANAGEMENT IN PRIMARY CARE: Part 2 In the second part of our feature on pigmented skin lesions, dermatology specialist Dr Sweta Rai describes the steps to rational decision-making
BACK TO TABLE OF CONTENTS FOCUS ON MELANOMA Oncology Annual Report BAPTIST HEALTH LEXINGTON ONCOLOGY ANNUAL REPORT
 FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
SUBUNGUAL MALIGNANT MELANOMA ON THE RIGHT INDEX IN A DENTIST AFTER PROLONGED OCCUPATIONAL EXPOSURE TO X-RAYS
 SUBUNGUAL MALIGNANT MELANOMA ON THE RIGHT INDEX IN A DENTIST AFTER PROLONGED OCCUPATIONAL EXPOSURE TO X-RAYS J. HATZIS*, V. MAKROPOULOS**, N. AGNANTIS*** * Department of Skin and Venereal Diseases, University
SUBUNGUAL MALIGNANT MELANOMA ON THE RIGHT INDEX IN A DENTIST AFTER PROLONGED OCCUPATIONAL EXPOSURE TO X-RAYS J. HATZIS*, V. MAKROPOULOS**, N. AGNANTIS*** * Department of Skin and Venereal Diseases, University
PATHOLOGY OF THE SKIN 2. Tumours of the skin
 PATHOLOGY OF THE SKIN 2. Tumours of the skin Máirín E. McMenamin MB MRCPI FRCPath Dip (Dermatopathol) RCPath St. James s Hospital and University of Dublin, Trinity College Tumour (Neoplasia) Benign or
PATHOLOGY OF THE SKIN 2. Tumours of the skin Máirín E. McMenamin MB MRCPI FRCPath Dip (Dermatopathol) RCPath St. James s Hospital and University of Dublin, Trinity College Tumour (Neoplasia) Benign or
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Pigmented lesions of the Oral cavity
 Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Oral medicine أ.م.د احسان عبد هللا كميل Pigmented lesions of the Oral cavity Pigmented oral lesions are a large group of disorders in which the dark or brown color is the essential clinical characteristic.
Clinicopathologic Self- Assessment S003 AAD 2017
 Clinicopathologic Self- Assessment S003 AAD 2017 Clay J. Cockerell, M.D. Director, Cockerell Dermatopathology Director, Division of Dermatopathology UT Southwestern Medical Center July 2017 No relevant
Clinicopathologic Self- Assessment S003 AAD 2017 Clay J. Cockerell, M.D. Director, Cockerell Dermatopathology Director, Division of Dermatopathology UT Southwestern Medical Center July 2017 No relevant
Directly Coded Summary Stage Melanoma
 Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
Racial differences in six major subtypes of melanoma: descriptive epidemiology
 Wang et al. BMC Cancer (2016) 16:691 DOI 10.1186/s12885-016-2747-6 RESEARCH ARTICLE Racial differences in six major subtypes of melanoma: descriptive epidemiology Yu Wang 1, Yinjun Zhao 2 and Shuangge
Wang et al. BMC Cancer (2016) 16:691 DOI 10.1186/s12885-016-2747-6 RESEARCH ARTICLE Racial differences in six major subtypes of melanoma: descriptive epidemiology Yu Wang 1, Yinjun Zhao 2 and Shuangge
Periocular skin cancer
 Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Questions. Answers. Share your photos and diagnoses with us!
 Illustrated quizzes on problems seen in everyday practice Case 1 An 80-year-old man presented with a slowly growing, asymptomatic, pearly telangiectatic nodule on the chest. He had worked much of his life
Illustrated quizzes on problems seen in everyday practice Case 1 An 80-year-old man presented with a slowly growing, asymptomatic, pearly telangiectatic nodule on the chest. He had worked much of his life
Oral and Maxillofacial Surgery Department
 Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Mole mapping and monitoring. Dr Stephen Hayes. Associate Specialist in Dermatology, University Hospital Southampton
 Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee
 I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest risk.
 Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre
 Malaysian J Pathol 202; (2) : 97 0 ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre Jayalakshmi PAILOOR, Kein-Seong
Malaysian J Pathol 202; (2) : 97 0 ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre Jayalakshmi PAILOOR, Kein-Seong
Management of Cutaneous Melanoma of the Head and Neck and a bit about SCCA/BCC. Irvin Pathak
 Management of Cutaneous Melanoma of the Head and Neck and a bit about SCCA/BCC Irvin Pathak Objectives Risk Factors Biopsy techniques Current surgical treatment Current Status of Adjuvant Therapies Epidemiology
Management of Cutaneous Melanoma of the Head and Neck and a bit about SCCA/BCC Irvin Pathak Objectives Risk Factors Biopsy techniques Current surgical treatment Current Status of Adjuvant Therapies Epidemiology
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Skin Tumors in Children
 AAD San Diego S021 2018 Skin Tumors in Children Jane M. Grant-Kels, MD,FAAD grant@uchc.edu Founding Chair Emeritus, Derm Dept, UCONN Vice Chair Dept of Dermatology Professor of Dermatology, Pathology and
AAD San Diego S021 2018 Skin Tumors in Children Jane M. Grant-Kels, MD,FAAD grant@uchc.edu Founding Chair Emeritus, Derm Dept, UCONN Vice Chair Dept of Dermatology Professor of Dermatology, Pathology and
Melanoma and Mimickers
 Melanoma and Mimickers Kara Walton, MD Assistant Professor of Dermatology and Dermatopathology Medical College of Wisconsin Disclosures No relevant financial disclosures 1 Objectives Recognize common benign
Melanoma and Mimickers Kara Walton, MD Assistant Professor of Dermatology and Dermatopathology Medical College of Wisconsin Disclosures No relevant financial disclosures 1 Objectives Recognize common benign
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Melanoma 10/6/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 Collecting NAACCR Cancer Data: 2015-2016 Melanoma Webinar Series NAACCR 2016-2017 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
Collecting NAACCR Cancer Data: 2015-2016 Melanoma Webinar Series NAACCR 2016-2017 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines
 CLINICAL GUIDANCE The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines Julia Newton Bishop, Veronique Bataille, Alice Gavin, Marko Lens, Jerry Marsden, Tania Mathews
CLINICAL GUIDANCE The prevention, diagnosis, referral and management of melanoma of the skin: concise guidelines Julia Newton Bishop, Veronique Bataille, Alice Gavin, Marko Lens, Jerry Marsden, Tania Mathews