Case histories in Urological cancers
|
|
|
- Rosalyn Morton
- 6 years ago
- Views:
Transcription
1 Case histories in Urological cancers Dr Alison Tree Consultant Clinical oncologist, The Royal Marsden and Institute of Cancer Research
2 2 The Royal Marsden Outline of talk Case histories for: Localised prostate cancer Active surveillance Metastatic disease Bladder cancer
3 3 The Royal Marsden Early diagnosis Difficult in prostate often no symptoms Democracy is the worst form of Government, except for all the rest Winston Churchill Same true for PSA Stick to referral criteria for PSA levels unless obvious cause Think of prostate cancer in LUTS, Bone pain. More common with increasing age, but still possible in 40s and 50s.
4 4 The Royal Marsden Localised prostate cancer
5 5 The Royal Marsden Case history - localised prostate cancer 72 year old man presents with PSA of 12 MRI (always first!) stage T2N0M0 (pelvis) Gleason 3+4 in 7/12 cores (TRUS) Patient otherwise well T1 not visible on MRI T2 confined to prostate T3a Into/beyond prostate capsule T3b Into seminal vesicles T4 into surrounding structures (bladder, rectum, uro-genital diaphragm)

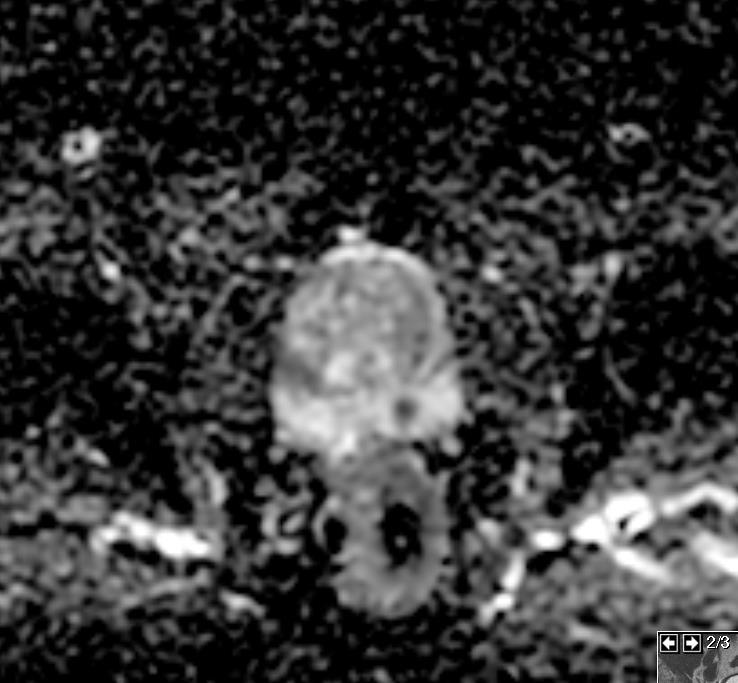
6 6 The Royal Marsden
7 7 The Royal Marsden MDT Every case discussed in local hospital (Epsom, Croydon, Kingston, Georges) Every new radically treatable cancer discussed again in the Central MDT (Marsden/Georges) Review pathology or pathology result, review each scan (radiology and nuclear medicine) Clinicians (Surgeons, Oncologists, specialist nurses) decide on treatment plan or options
8 8 The Royal Marsden MDT discussion Surgery probably not optimal at 72 Options Androgen deprivation therapy plus radiotherapy Brachytherapy Whatever he chooses cure rate around 90%





9 We have made colossal progress in radiotherapy



10 2 D 3 D Bowel side effects 56% 37%

11 33% 13% CHHiP trial vs RT01 trial

12 12
 60 Gy / 20# in 4 weeks 57 Gy / 19# in 3.8 weeks")
13 CHHiP : Phase III Trial of Conventional or Hypofractionated High Dose intensity Modulated Radiotherapy in Prostate Cancer Histologically proven prostate cancer T1b-T3a N0 M0 Estimated risk of seminal vesicle involvement = 30% PSA = < 30ng/ml Due to receive radiotherapy Hormone therapy Randomisation 74 Gy / 37# in 7.4 weeks (standard) 60 Gy / 20# in 4 weeks 57 Gy / 19# in 3.8 weeks
14 14 60 Gy in 20 non-inferior to 74 Gy in 37
15

16 16 Very little toxicity 4% Gd 2+ GI at 2 years
 Refer each to relevant speciality After prostatectomy PSA should be undetectable for life, definitely refer back if reaches 0.")
17 17 The Royal Marsden PSA follow up increasingly Primary care led PSA 6-monthly to 5 years, then annually Side effects rare but may occur many years later GI, GU, ED (ask!) Refer each to relevant speciality After prostatectomy PSA should be undetectable for life, definitely refer back if reaches 0.1 After radiotherapy PSA should be below nadir+2 ng/ml for life, otherwise please refer back

18 So how do we do radiotherapy?

19 Don t worry, I ll leave out the geeky bits Copyright Warner Bros

20 -You don t take any radiotherapy with you -No risk to pregnant family members -No sensation associated -Probably a small risk of seconary cancers (prob <1:250)

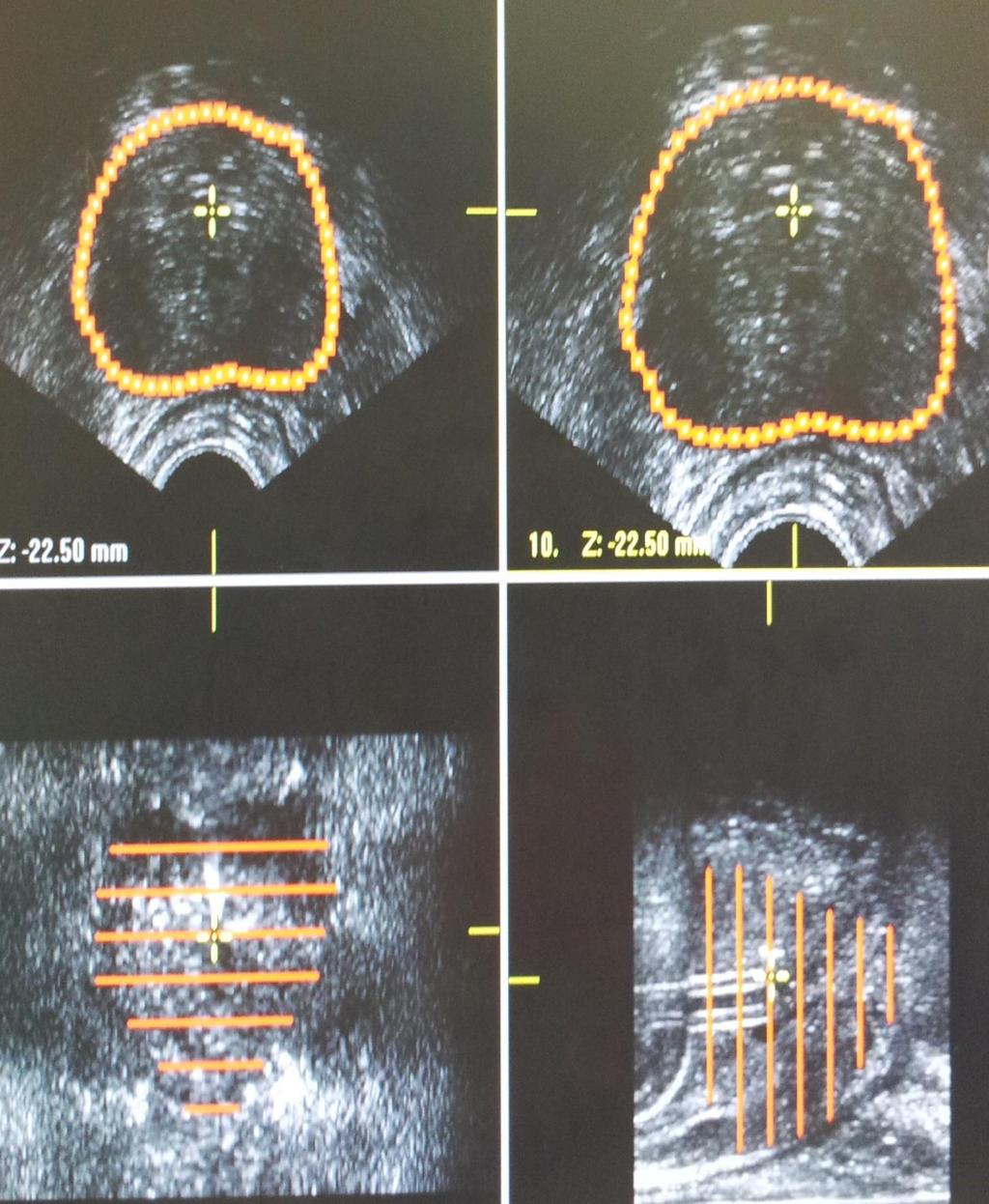
21 21 Fiducial placement under trans-rectal ultrasound guidance outpatient procedure

22 22 A fiducial in situ
23 23 The Royal Marsden Risks Pain Bleeding (GI, GU, Haematospermia) Infection Rectal swab, targeted antibiotics IF FEVER STRAIGHT TO A +E, NEED IV Abx (risk 0.3%)

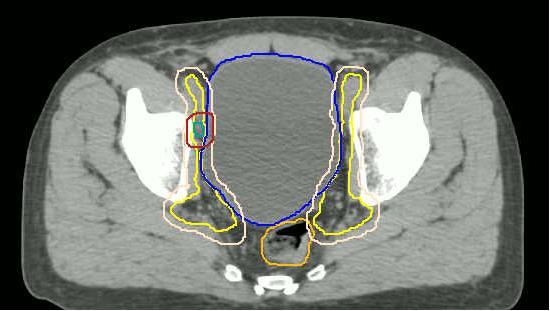
24 24 The Royal Marsden

25 25 The Royal Marsden
26 26 The Royal Marsden So what does the patient experience each day? Empty bladder and take Microlet enema one hour before treatment (enema only first 5-10 treatments to keep rectum empty) Drink 325 mls of water/squash and hold bladder 1 hour Change into gown Lay on treatment couch (hard!) and get moved into the correct position (CT). Radiographers leave the room, so patient is alone, but can be seen and heard Machine moves around patient but doesn t touch. No sensation during treatment
27 27 The Royal Marsden Brachytherapy


28
29

30 30 The Royal Marsden Active surveillance
31 Case history 53 years, PSA 0 Presents to GP with PSA 5.1 Referred to local hospital has TRUS biopsy Gleason 6 (3+3), 2/10 cores positive, ct1c (DRE) MRI T1c or now PIRADS 2
32 What would you do for him? A. Radical prostatectomy 100% B. Radical radiotherapy with Androgen Deprivation Therapy C. Radical radiotherapy alone D. Active surveillance 0% 0% 0% Radical prostatectomy Radical radiotherapy wi.. Radical radiotherapy alone Active surveillance
33 MDT discussion 53 not 73 years old But otherwise very favourable disease Recommend TP biopsy (can be in 6 months) and Active surveillance if no upstaging

 Rx timing")
34 Watchful waiting is not active surveillance Watchful waiting Active surveillance Rx indication Symptoms MRI!! PSA trends (Biopsy results) Rx timing Late/Never Early Rx intent Palliative Curative
35 Royal Marsden Active surveillance cohort 471 men, 81% low risk 70% remain free of treatment at 5 years, 50% at 10 years 0.4% prostate cancer specific mortality at 5 years (5.3% non prostate cancer deaths at 5-years) 35 Selvadurai et al, 2013

36 82,429 men agreed to PSA test 2664 had localised prostate cancer 1643 agreed to be randomised Around 500 in each group
37 FRCR (NICE) AS schedule PSA 3 monthly for 2 years Repeat MR (and biopsy) at months Then repeat MR (and biopsy) 2 years later PSAs 6 monthly years 2-4 Path or MR upgrade - treat
38 Locally advanced prostate cancer
39 Case history Fit 52 year old barrister, PMH of left nephrectomy for oncocytoma in GP had been monitoring PSA: Urologist Dec ng/ml Dec ng/ml Sept ng/ml pt referred to a Trus Bx Gleason 4+5=9 in 10/10 cores, max length 12mm MRI T3b N1 (several suspicious LN up to 14mm in pelvis) Bone scan normal. IPSS =2

40 MRI and biopsy Gleason 4+5=9 (GG5) in 10/10 cores, up to 12mm length, PSA 7.0

41 MRI spine negative Choline PET Several bilateral choline avid pelvic LN - left internal iliac - right and left external iliac - right obturator
42 Commenced ADT with bicalutamide and LHRHa in Nov 2012-Aug 2015 PSA fell from 15 in Oct 2012 to 0.13 by April 2013 Radical EBRT in the IMRT Phase I/II trial with 74Gy in 37# to prostate, 60Gy in 37# to lymph nodes, 5Gy boost to LN
43 12/1/09 3/1/10 6/1/10 9/1/10 12/1/10 3/1/11 6/1/11 9/1/11 12/1/11 3/1/12 6/1/12 9/1/12 12/1/12 3/1/13 6/1/13 9/1/13 12/1/13 3/1/14 6/1/14 9/1/14 12/1/14 3/1/15 6/1/15 9/1/15 12/1/15 3/1/16 6/1/16 9/1/16 PSA (ng/ml) The Royal Marsden PSA Testosterone Date
44 Androgen deprivation therapy Starting treatment Bicalutamide 50mg or 150mg od for 28 days LHRH analogues start 7-14 days after starting Bicalutamide (flare) Usually start monthly Can switch to monthly in those needing >12 months of therapy (T recovery 9months)
45 ADT side effects Fatigue Hot flushes Loss of muscle bulke/weakness Mood swings grumpy/teary/change in personality Almost complete erectile dysfunction/loss of libido (exceptions)?cardiovascular risk Long term Loss of bone density Cardiovascular risk
 of Docetaxel")
46 What about chemo? 6 cycles (=18 weeks) of Docetaxel chemotherapy = 10 months more survival


47
48 Side effects of radiotherapy Bowels diarrhoea, proctitis, bleeding (? Second primary) GU dysuria, LUTS, 1% acute retention Fatigue Rarely see skin reaction now, ED probably takes years to develop.
49 Is radiotherapy curative in node positive disease? James et al, JAMA 2016
50 Metastatic disease
51 Metastatic disease 72 year old man Previously fit and well Presents to A+E with weak legs O/E Power 3/5 left hip flexion and extension, 4/5 right side No dermatomal sensation loss A+E bloods OK, PSA pending.
52 EMERGENCY!
53 Activate the spinal cord compression pathway Ring AOS team Order urgent MRI minutes mean neurons Dex 8mg bd +PPI PSA comes back as 2658 Start Degarelix 240mg sc

54

55 Verteb ral body Spinal cord CSF (whit e on T2)

56 Tumo ur growin g into spinal canal Spinal cord shape distort ed
57 Patient declined for neurosurgery Given emergency radiotherapy 20 Gy in 5 fractions to the spine Staged with a bone scan and CT chest abdomen pelvis Metastases in several bony areas, and widespread metastatic lymphadenopathy
58 How long is his median survival? Median survival of newly diagnosed metastatic prostate cancer 5-6 years at present Currently start with ADT and Docetaxel, then at progression cycle through a range of new generation hormonal therapies (Abi, Enza) and other active agents (Cabazitaxel, Radium) Who knows what is next..





59 59 Metastatic disease LHRH analogues Add antiandrogens Docetaxel Consider Casodex withdrawal, stilboestrol, steroids Radium 223 Abiratero ne Enzalutam ide Cabazitaxe l
60 Bladder cancer
61 Searching for a needle in a haystack?
62 62 year old woman Presents to GP with visible haematuria MSU: E Coli sensitive to Trimethoprim 2 weeks later returns to GP Dysuria and visible haematuria returned MSU no growth
63 You are the GP seeing her in clinic do you? A. Try another course of Trimethoprim and see if it clears up B. Try a different antibiotic C. Send a repeat MSU in 2 weeks D. Refer on a 2 week rule pathway for visible haematuria Try another course of Tr... 0% Try a different antibiotic 3% Send a repeat MSU in % Refer on a 2 week rule... 93%
64 Patient undergoes a Haematuria work up Cystoscopy (flexi, rigid) CT KUB May do urine cytology if no primary in bladder Consider retrograde ureter studies


65 Tumo ur
66 Other things bladder tumours can do Obstruct one ureter (rarely both) Present with sterile dysuria only
67 What next? Biopsy at cystoscopy - TCC into muscle Referred to oncology Patient otherwise well, no comorbidities Advised to have 3 cycles of chemotherapy with Gemcitabine and Cisplatin
68 68 The Royal Marsden The ABC meta-analysis 5% survival advantage
69 Bladder preservation RT TUR BT Chem o Cystosco py Cystecto my
70 What next? Cystoscopy shows complete response Patient elects to have bladder preservation 64 Gy in 32 fractions daily over 6.5 weeks with concomitant chemo MMC 12mg/m2 5FU 500mg/m2/d RT 64 Gy/32 f Weeks
71 The Royal Marsden BC 2001 study CI Robert Huddart Local control 67 % vs 54% Months since randomisation N at risk (events) CT 182 (34) 106 (14) 71 (2) 51 (1) 41 (1) 23 (0) 11 No CT 178 (53) 94 (16) 62 (4) 48 (0) 25 (0) 18 (1) 9
72 3 months post radiotherapy Check cystoscopy no sign of recurrence. Follow up regular CT scans and cystoscopies What to watch out for: Haematuria muscle-invasive or non-muscle invasive recurrence Hydronephrosis Metastases (commonly lymph node, bone, lung)
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
The Royal Marsden. Prostate case study. Presented by Mr Alan Thompson Consultant Urological Surgeon
 Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
PROSTATE CANCER STRATIFIED FOLLOW UP. Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN.
 PROSTATE CANCER STRATIFIED FOLLOW UP Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN. LEARNING OBJECTIVES To refresh your knowledge about prostate cancer. To discuss the purpose and patient benefits
PROSTATE CANCER STRATIFIED FOLLOW UP Hilary Baker Lead CNS for Uro-oncology MSc, BSc, RGN. LEARNING OBJECTIVES To refresh your knowledge about prostate cancer. To discuss the purpose and patient benefits
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
NICE BULLETIN Diagnosis & treatment of prostate cancer
 Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
GUIDELINEs ON PROSTATE CANCER
 GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
PROSTATE CANCER CONTENT CREATED BY. Learn more at
 PROSTATE CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Ask your doctor about screening and treatment options. WHAT IS PROSTATE CANCER? 4 WATCHFUL
PROSTATE CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Ask your doctor about screening and treatment options. WHAT IS PROSTATE CANCER? 4 WATCHFUL
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Prostatectomy as salvage therapy. Cases. Paul Cathcart - Guy s & St Thomas NHS Trust, London
 Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Prostate Cancer Case Study 1. Medical Student Case-Based Learning
 Prostate Cancer Case Study 1 Medical Student Case-Based Learning The Case of Mr. Powers Prostatic Nodule The effervescent Mr. Powers is found by his primary care provider to have a prostatic nodule. You
Prostate Cancer Case Study 1 Medical Student Case-Based Learning The Case of Mr. Powers Prostatic Nodule The effervescent Mr. Powers is found by his primary care provider to have a prostatic nodule. You
BRACHYTHERAPY FOR PROSTATE CANCER. Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital
, FRANZCR Radiation Oncologist, The Canberra Hospital") BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
BRACHYTHERAPY FOR PROSTATE CANCER Dr Brandon Nguyen MBBS(Hons), FRANZCR Radiation Oncologist, The Canberra Hospital PROSTATE BRACHYTHERAPY Why brachytherapy? How do we do it? What are the results? Questions?
One Stop Prostate Biopsy Protocol Author Consultation Date Approved
 One Stop Prostate Biopsy Protocol Author Consultation Date Approved Urology Nurse Practioner PROTOCOL FOR MEN ATTENDING A ONE STOP PROSTATE BIOPSY CLINIC RATIONALE Prostate cancer is the most common cancer
One Stop Prostate Biopsy Protocol Author Consultation Date Approved Urology Nurse Practioner PROTOCOL FOR MEN ATTENDING A ONE STOP PROSTATE BIOPSY CLINIC RATIONALE Prostate cancer is the most common cancer
Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer
 Peterborough City Hospital Department of Urology Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer Hormonal Therapy - How does it work? Prostate Cancer relies on the presence
Peterborough City Hospital Department of Urology Guidelines for the Shared Care of Patients on hormonal therapy for Prostate Cancer Hormonal Therapy - How does it work? Prostate Cancer relies on the presence
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
BLADDER PROSTATE PENIS TESTICLES BE YO ND YO UR CA NC ER
 BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
Guideline Prostate cancer: diagnosis and management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Prostate cancer: diagnosis and management (update) Draft for consultation, December 0 This guideline covers diagnosing and managing prostate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Prostate cancer: diagnosis and management (update) Draft for consultation, December 0 This guideline covers diagnosing and managing prostate
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Information for Patients. Prostate cancer. English
 Information for Patients Prostate cancer English Table of contents What is prostate cancer?... 3 The role of hormones in prostate cancer cell growth... 3 Stages of the disease... 3 Risk factors for prostate
Information for Patients Prostate cancer English Table of contents What is prostate cancer?... 3 The role of hormones in prostate cancer cell growth... 3 Stages of the disease... 3 Risk factors for prostate
17/07/2014. Prostate Cancer Watchful Waiting New Treatments Andrew Williams Urologist and Urological Oncologist ADHB, CMDHB and 161 Gillies Ave, Epsom
 My Biases Prostate Cancer Watchful Waiting New Treatments Andrew Williams Urologist and Urological Oncologist ADHB, CMDHB and 161 Gillies Ave, Epsom I am a member of the specialist group of the Prostate
My Biases Prostate Cancer Watchful Waiting New Treatments Andrew Williams Urologist and Urological Oncologist ADHB, CMDHB and 161 Gillies Ave, Epsom I am a member of the specialist group of the Prostate
When to worry, when to test?
 Focus on CME at the University of Calgary Prostate Cancer: When to worry, when to test? Bryan J. Donnelly, MSc, MCh, FRCSI, FRCSC Presented at a Canadian College of Family Practitioner s conference (October
Focus on CME at the University of Calgary Prostate Cancer: When to worry, when to test? Bryan J. Donnelly, MSc, MCh, FRCSI, FRCSC Presented at a Canadian College of Family Practitioner s conference (October
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Managing clinical outcomes for urological cancers
 Managing clinical outcomes for urological cancers Netty Kinsella Uro-oncology nurse consultant The Royal Marsden Presentation Overview Variation in access to treatment across the LCA Introduce the LCA
Managing clinical outcomes for urological cancers Netty Kinsella Uro-oncology nurse consultant The Royal Marsden Presentation Overview Variation in access to treatment across the LCA Introduce the LCA
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Cancer of Unknown Primary (CUP)
") Cancer of Unknown Primary (CUP) Pathways and Guidelines V1.0 London Cancer September 2013 The following pathways and guidelines document has been compiled by the London Cancer CUP technical subgroup and
Cancer of Unknown Primary (CUP) Pathways and Guidelines V1.0 London Cancer September 2013 The following pathways and guidelines document has been compiled by the London Cancer CUP technical subgroup and
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Locally advanced prostate cancer
 Diagnosis Helpline 0800 074 8383 prostatecanceruk.org 1 Locally advanced prostate cancer In this fact sheet: What is locally advanced prostate cancer? What tests are used to diagnose locally advanced prostate
Diagnosis Helpline 0800 074 8383 prostatecanceruk.org 1 Locally advanced prostate cancer In this fact sheet: What is locally advanced prostate cancer? What tests are used to diagnose locally advanced prostate
To treat or not to treat: When to treat! A case presentation
 To treat or not to treat: When to treat! A case presentation Filip Ameye, MD,Phd Universitary Hospitals Leuven, Belgium Departement of Urology Prostate Center A case presentation Pt. 76 y. Mild LUTS (07/1999)
To treat or not to treat: When to treat! A case presentation Filip Ameye, MD,Phd Universitary Hospitals Leuven, Belgium Departement of Urology Prostate Center A case presentation Pt. 76 y. Mild LUTS (07/1999)
South East Scotland Cancer Network Prostate Cancer Management Protocol.
 South East Scotland Cancer Network Prostate Cancer Management Protocol. INTRODUCTION Prostate cancer is the second most common cancer in men in Scotland, accounting for 17% of all male cancer registrations.
South East Scotland Cancer Network Prostate Cancer Management Protocol. INTRODUCTION Prostate cancer is the second most common cancer in men in Scotland, accounting for 17% of all male cancer registrations.
Prostate cancer. Treatments Side effects and management in the community setting
 Prostate cancer Treatments Side effects and management in the community setting Kristoffer Ohlin CNS Urology Janice Minter Lead Cancer Nurse St George s Hospital Agenda Prostate cancer treatments Radiotherapy
Prostate cancer Treatments Side effects and management in the community setting Kristoffer Ohlin CNS Urology Janice Minter Lead Cancer Nurse St George s Hospital Agenda Prostate cancer treatments Radiotherapy
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Prostate cancer. A guide for men who ve just been diagnosed
 Prostate cancer A guide for men who ve just been diagnosed 2 Prostate cancer A guide for men who ve just been diagnosed About this booklet This booklet is for men who ve recently been diagnosed with prostate
Prostate cancer A guide for men who ve just been diagnosed 2 Prostate cancer A guide for men who ve just been diagnosed About this booklet This booklet is for men who ve recently been diagnosed with prostate
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Deciding on treatment: a step on your journey.
 Deciding on treatment: a step on your journey. One step at a time. After being told that you have prostate cancer, the next step on your journey may be to participate in the decision on which type of treatment
Deciding on treatment: a step on your journey. One step at a time. After being told that you have prostate cancer, the next step on your journey may be to participate in the decision on which type of treatment
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Guidelines for the Management of Bladder Cancer
 Guidelines for the Management of Bladder Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Version 3 and 4 Sections 5.2 and 8 updated Page 1 of 9 1. Scope of
Guidelines for the Management of Bladder Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Version 3 and 4 Sections 5.2 and 8 updated Page 1 of 9 1. Scope of
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
Biodegradable spacer insertion to reduce rectal toxicity during radiotherapy for prostate cancer
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Biodegradable spacer insertion to reduce rectal toxicity during radiotherapy for prostate cancer Radiotherapy
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Biodegradable spacer insertion to reduce rectal toxicity during radiotherapy for prostate cancer Radiotherapy
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
PROSTATE CANCER: A Primer of Diagnosis and Treatment. Jay C. Lee, MD, FRCSC Clinical Associate Professor University of Calgary
 PROSTATE CANCER: A Primer of Diagnosis and Treatment Jay C. Lee, MD, FRCSC Clinical Associate Professor University of Calgary Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
PROSTATE CANCER: A Primer of Diagnosis and Treatment Jay C. Lee, MD, FRCSC Clinical Associate Professor University of Calgary Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
An introduction to advanced prostate cancer
 1 Prostate information An introduction to advanced prostate cancer Introduction Being told by the doctor or specialist nurse that you have advanced prostate cancer, or that your cancer has come back, can
1 Prostate information An introduction to advanced prostate cancer Introduction Being told by the doctor or specialist nurse that you have advanced prostate cancer, or that your cancer has come back, can
Prostate Cancer Case Study 2. Medical Student Case-Based Learning
 Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Biodegradable spacer insertion to reduce rectal toxicity during radiotherapy for prostate cancer
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Biodegradable spacer insertion to reduce rectal toxicity during radiotherapy for prostate cancer Radiotherapy
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Biodegradable spacer insertion to reduce rectal toxicity during radiotherapy for prostate cancer Radiotherapy
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER
 CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER Klinikum Offenbach Nucletron April 27 th 28 th, 2014 History HDR Protocols for Boost and Monotherapy, Results, Logistics and Practical
CLINICAL WORKSHOP IMAGE-GUIDED HDR BRACHYTHERAPY OF PROSTATE CANCER Klinikum Offenbach Nucletron April 27 th 28 th, 2014 History HDR Protocols for Boost and Monotherapy, Results, Logistics and Practical
North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer
 THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
Prostate Biopsy. Prostate Biopsy. We canʼt go backwards: Screening has helped!
 We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA
 Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA ESMO Cape Town 14 Feb 2018 Disclosures Advisory boards/lecturer/consultant-
Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA ESMO Cape Town 14 Feb 2018 Disclosures Advisory boards/lecturer/consultant-
What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen).
.") What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen). It is a very common cancer in men; some cancers grow very slowly,
What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen). It is a very common cancer in men; some cancers grow very slowly,
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Care of bladder cancer patients diagnosed in Northern Ireland 2010 & 2011 (Summary)
") Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Patient: John Doe July 1, CancerOpinions MD: Luke Nordquist, M.D., F.A.C.P Zip Code: 68111
 Cancer Consultation 11404 West Dodge Rd, Ste 650 Omaha, NE 68154 (402) 963-4112 (888)WEB-OPIN (932-6746) Patient: John Doe July 1, 2010 Referral MD: John Smith, MD MRN #
Cancer Consultation 11404 West Dodge Rd, Ste 650 Omaha, NE 68154 (402) 963-4112 (888)WEB-OPIN (932-6746) Patient: John Doe July 1, 2010 Referral MD: John Smith, MD MRN #
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for lymphoma
 Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
The benefit of a preplanning procedure - view from oncologist. Dorota Kazberuk November, 2014 Otwock
 The benefit of a preplanning procedure - view from oncologist Dorota Kazberuk 21-22 November, 2014 Otwock Brachytherapy is supreme tool in prostate cancer management with a wide range of options in every
The benefit of a preplanning procedure - view from oncologist Dorota Kazberuk 21-22 November, 2014 Otwock Brachytherapy is supreme tool in prostate cancer management with a wide range of options in every
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Guidelines for Management of Penile Cancer
 Guidelines for Management of Penile Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Versions 2 and 3 Sections 3, 5, 6 and 16 updated. Page 1 of 10 1. Scope
Guidelines for Management of Penile Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Versions 2 and 3 Sections 3, 5, 6 and 16 updated. Page 1 of 10 1. Scope
Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline
 Treatment Guideline") Mid Essex Locality Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline Contents FlowChart 2 Summary... 3 Key points... 3 Introduction... 3 Pharmacology... 3 Product information... 4 Place
Mid Essex Locality Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline Contents FlowChart 2 Summary... 3 Key points... 3 Introduction... 3 Pharmacology... 3 Product information... 4 Place
Mr Declan Cahill Consultant Urological Surgeon The Royal Marsden
 Diagnosing prostate cancer Mr Declan Cahill Consultant Urological Surgeon 2 Marsden GP Education Day 22 February 2016 Should I have a PSA test? Can I have a PSA test? prostatecanceruk.org 4 83% raised
Diagnosing prostate cancer Mr Declan Cahill Consultant Urological Surgeon 2 Marsden GP Education Day 22 February 2016 Should I have a PSA test? Can I have a PSA test? prostatecanceruk.org 4 83% raised