Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
|
|
|
- Maximilian Brooks
- 6 years ago
- Views:
Transcription









1 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao, MD, FRCPC Ignacio I. Wistuba, MD
2 Modules and Participating Faculty 1. Introducing The New IASLC/ATS/ERS Lung Adenocarcinoma Classification William D. Travis, MD Memorial Sloan Kettering Cancer Center New York, NY Fred R. Hirsch, MD, PhD University of Colorado Aurora, CO Gregory Riely, MD, PhD Memorial Sloan Kettering Cancer Center New York, NY 2. Implications of the New IASLC/ATS/ERS Classification Fred R. Hirsch, MD, PhD University of Colorado Aurora, CO Paul E. Van Schil, MD, PhD University Hospital of Antwerp Edegem (Antwerp), Belgium William D. Travis, MD Memorial Sloan Kettering Cancer Center New York, NY Kavita Garg, MD University of Colorado Aurora, CO 3. Highlights for the Pathologist Ming S. Tsao, MD, FRCPC Princess Margaret Hospital Toronto, Ontario, Canada Ignacio I. Wistuba, MD The University of Texas M.D. Anderson Cancer Center Houston, TX Kim R. Geisinger, MD Piedmont Pathology Associates Hickory, NC 4. Highlights for the Radiologist Kavita Garg, MD University of Colorado Aurora, CO Gregory Riely, MD, PhD Memorial Sloan Kettering Cancer Center New York, NY 5. Case Studies for the Practicing Clinician Gregory Riely, MD, PhD Memorial Sloan Kettering Cancer Center New York, NY William D. Travis, MD Memorial Sloan Kettering Cancer Center New York, NY Fred R. Hirsch, MD, PhD University of Colorado Aurora, CO Paul A. Bunn, Jr., MD University of Colorado Aurora, CO Paul E. Van Schil, MD, PhD University Hospital of Antwerp Edegem (Antwerp), Belgium
3 The New IASLC/ATS/ERS Lung Adenocarcinoma Classification Module 5 Case Studies for the Practicing Clinician
4 Patient # 1 Clinical History Patient is a 70-year-old man who presented with increased cough over 6 months, productive of grey sputum Past medical history: Cholecystectomy, 15 pack-year history of smoking (1ppd x 15 years, quit 40 years ago) Family history: No family history of cancer
5 CT Chest Mass-like consolidated bilateral pulmonary opacities with satellite nodules
6 Initial Evaluation MRI brain no evidence of metastases Bone Scan no evidence of bone metastases Routine Labs normal blood count and chemistries Bronchoscopy performed: brushings for cytology reported as non-small cell carcinoma
7 IASLC/ATS/ERS Adenocarcinoma Classification: Strong Recommendations for Pathologists: Biopsy and Cytology Samples For small biopsies/cytology, NSCLC should be further classified into more specific histologic types (e.g. adenocarcinoma, squamous-cell carcinoma), whenever possible The term NSCLC-NOS be used infrequently and only applied when a more specific diagnosis is NOT possible by morphology/special stains

8 Further Evaluation Available material from bronchoscopy was insufficient for additional pathologic evaluation Patient undergoes CT-guided core needle biopsy Diagnosis: Invasive Adenocarcinoma
9 Diagnostic Algorithm for Small Biopsy and Cytology Specimens Based on morphology and IHC markers NE morphology, NE IHC(+), large cells NSCLC (probably LCNEC) STEP 1. Positive Biopsy (FOB, TBBx, Core, SLBx) or Positive Cytology (effusion, aspirate, washings, brushings) NE morphology, NE IHC(+), small cells, no nucleoli, TTF-1(+/-), CK(+) Keratinization, pearls and/or intercellular bridges Histology: Lepidic, papillary, and/or acinar architecture(s) Cytology: 3-D arrangements, delicate foamy/vacuolated (translucent) cytoplasm, fine nuclear chromatin and often prominent nucleoli, nuclei often eccentrically situated SCLC Classic Morphology: SQCC Classic Morphology: ADC Molecular Analysis: e.g. EGFR mutation ADC: adenocarcinoma; CK: cytokeratin; FOB: fiberoptic bronchoscopy; IHC: immunohistochemistry; LCNEC: large cell neuroendocrine carcinoma; NE: neuroendocrine; NOS: not otherwise specified; NSCLC: non-small cell lung carcinoma; SBx: surgical lung biopsy; SCLC: small cell lung carcinoma; SQCC: squamous cell carcinoma; TBBx: transbronchial biopsy; TTF: thyroid transcription factor;
10 Diagnostic Molecular Pathology Evaluation Diagnostic molecular pathology Positive for EGFR exon 19 deletion, 18bp deletion Negative for ALK rearrangement


11 Treatment Based on histology and molecular pathology evaluation, patient was initially treated with erlotinib Baseline 4 months on erlotinib Radiographic response lasted 16 months
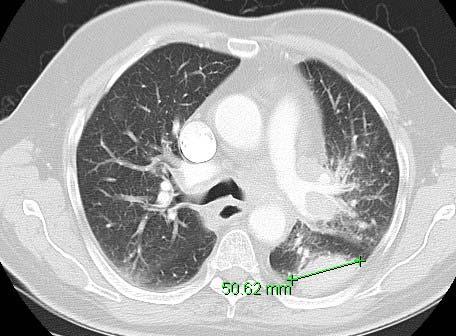
12 Patient # 2 Clinical History 76 year old woman, former 50 pack-year smoker (1 pack per day for 50 years, quit 10 years ago) presents with intermittent, dry cough Past Medical History: COPD, coronary artery disease with prior bypass grafting Family History: no family history of cancer, father and mother died in their 70s of heart disease Abnormal chest X-ray leads to CT scan

13 CT Chest Left lower lobe mass, juxtapleural nodules in left lower and upper lobes, right paratracheal, left tracheobronchial, and left hilar lymphadenopathy.
14 Initial Evaluation MRI Brain unremarkable except for small vessel ischemic changes PET/CT scan showed FDG-avid lung mass, hilar adenopathy, and mediastinal adenopathy Multiple FDG-avid bone lesions on PET with corresponding lesions seen on CT scan
15 Further Evaluation Bronchoscopy showed endobronchial lesions on left with proximal disease Transbronchial biopsy and endobronchial ultrasoundguided biopsy of mediastinal nodes was obtained Initial Pathology Report: Poorly Differentiated Carcinoma
16 IASLC/ATS/ERS Adenocarcinoma Classification: Strong Recommendations for Pathologists: Biopsy and Cytology Samples For small biopsies/cytology, NSCLC should be further classified into more specific histologic types (e.g. adenocarcinoma, squamous), whenever possible The term NSCLC-NOS be used infrequently and only applied when a more specific diagnosis is NOT possible by morphology/special stains
17 Further Classification of NSCLC-NOS (when morphology is indefinite) No clear ADC or SQCC morphology: NSCLC-NOS STEP 2. Apply ancillary panel of one SQCC and one ADC marker +/OR Mucin Non-NE Markers: ADC: TTF1, Napsin-A SQCC: P63, CK5/6, p40 IHC(-) and Mucin(-) ADC-marker(+) or Mucin(+) AND SQCC-marker(+) in different cells ADC-marker(+) and/or Mucin(+) AND SQCC-marker(-) (or weak in same cells) SQCC-marker(+) AND ADC-marker(-) or Mucin(-) NSCLC NOS NSCLC-NOS, possible adenosquamous NSCLC (favor ADC) NSCLC (favor SQCC) STEP 3. Molecular Analysis (e.g. EGFR mutation, ALK rearrangement). If tumor tissue is inadequate for molecular testing, discuss need for further sampling (Back to STEP 1)
18 Further Evaluation Initial Pathology Report: Poorly Differentiated Carcinoma P63 IHC: positive TTF-1 IHC: negative After review of IHC and further light microscopy review: Squamous Cell Carcinoma

19 Treatment Patient is treated with gemcitabine/cisplatin Baseline After 2 cycles
20 Patient # 3 Clinical History 56 year old man, former 60 pack-year smoker (1½ packs per day for 40 years) presents with cough productive of copious amounts of clear sputum Past medical history: COPD, coronary artery disease with placement of coronary stents Family History: mother, who was a smoker, died of lung cancer at the age of 74 Abnormal chest X-ray leads to CT scan

21 CT Chest Consolidation encompassing right lower and right middle lobes
22 Initial Evaluation CT scan brain with IV contrast no metastatic disease, no significant ischemic changes Bone Scan no sites of specific tracer uptake Patient undergoes fluoroscopic core-needle biopsy
23 Pathology Evaluation Invasive Mucinous Adenocarcinoma
24 Diagnostic Molecular Pathology Evaluation Diagnostic molecular pathology Negative for EGFR exon 19 deletion Negative for EGFR exon 21 L858R mutation Positive for KRAS G12C mutation
25 Classification of Lung Adenocarcinomas Term Pathology CT Appearance Adenocarcinoma in situ (AIS) Small ( 3 cm), solitary, noninvasive adenocarcinoma with pure lepidic growth, usually nonmucinous, rarely mucinous Usually pure ground-glass, but may be part-solid, bubble-like, or solid Minimally invasive adenocarcinoma (MIA) Lepidic predominant adenocarcinoma Acinar, papillary, micropapillary, or solid predominant ADC, plus a lepidic component Invasive mucinous adenocarcinoma Small ( 3 cm), solitary adenocarcinoma with predominantly lepidic growth and 5 mm invasion, usually nonmucinous, rarely mucinous Invasive nonmucinous adenocarcinoma that has lepidic growth as its predominant component Invasive adenocarcinoma that is predominantly acinar, papillary, micropapillary, or solid, plus a small proportion of a lepidic component Invasive mucinous adenocarcinoma that has lepidic growth as its predominant component Mainly ground-glass, plus a small (< 5 mm) central solid component** Usually part-solid, including a groundglass component; may be pure groundglass or solid; occasionally bubble-like Solid, but may include a small portion of ground-glass opacity Usually solid or mostly solid, single or multifocal or multilobar, formerly BAC
26 Patient # 4 Clinical History 71 year old woman with 40 pack year history of smoking (1 ppd x 40 years, quit 13 years ago) without symptoms Past Medical History breast cysts Family History unremarkable Patient undergoes a screening CT scan after announcement of NLST data and discussion with physician

27 CT Chest Multilobar ground glass opacities with left lower lobe consolidation
28 Further Evaluation PET/CT scan no FDG-avid lesions PFTs adequate for lobectomy Cardiac stress test no evidence of ischemia After discussion with thoracic surgeon, elects to undergo subsegmental resection as diagnostic procedure


29 Pathology Evaluation Diagnosis: Minimally Invasive Adenocarcinoma
30 IASLC/ATS/ERS Adenocarcinoma Classification: Strong Recommendations for Pathologists The use of term BAC to be discontinued Adenocarcinoma in situ (AIS): Defines small ( 3 cm) solitary ADC with pure lepidic growth Exclude if miliary spread or lobar consolidation 100% disease-free survival (DFS) if completely resected Minimally Invasive Adenocarcinoma (MIA): Defines small ( 3 cm) solitary ADC with pure lepidic growth and small foci of invasion measuring 0.5 cm Near 100% DFS if completely resected
31 Invasive components: MIA (Criteria of Invasion) Histological patterns other than lepidic (e.g. acinar, papillary, micropapillary, solid) Tumor cells infiltrating myofibroblastic stroma MIA excluded with presence of: Lymphatic, blood vessels or pleural invasion Tumor necrosis Microinvasive areas found in one tumor: Multiple foci of MIA invasive areas possible Individual invasive areas measured separately Size of largest invasive area measured in largest dimension 0.5 cm
32 Key Concepts of the IASLC/ATS/ERS Lung Adenocarcinoma Classification Discontinued use of the term BAC, replaced with: Adenocarcinoma in situ Minimally Invasive Adenocarcinoma Lepidic Predominant Adenocarcinoma, Invasive Mucinous Adenocarcinoma Use of the term NSCLC-NOS to describe small biopsies/cytology should be uncommon Immunohistochemistry should be used to further characterize Molecular analysis of lung adenocarcinomas should be routine (e.g. EGFR mutation, ALK rearrangement)
33 Benefits of IASLC Membership Not a member of IASLC? Join today and enjoy the benefits of membership Check for upcoming program and events registration dates, and IASLC member information
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Update on 2015 WHO Classification of Lung Adenocarcinoma 1/3/ Mayo Foundation for Medical Education and Research. All rights reserved.
 1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
1 Our speaker for this program is Dr. Anja Roden, an associate professor of Laboratory Medicine and Pathology at Mayo Clinic as well as consultant in the Anatomic Pathology Laboratory and co-director of
Non-Small Cell Lung Carcinoma - Myers
 Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Role of Routine Histology and Special Testing in Managing Patients with Non- Small Cell Lung Carcinoma Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY
 HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
HOW TO GET THE MOST INFORMATION FROM A TUMOR BIOPSY 7 TH Annual New York Lung Cancer Symposium Saturday, November 10, 2012 William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Disclosure of Relevant Financial Relationships NON-SMALL CELL LUNG CANCER: 70% PRESENT IN ADVANCED STAGE
 MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
MORPHOLOGY AND MOLECULAR TESTING IN NON-SMALL CELL OF LUNG NEW FRONTIEIRS IN CYTOPATHOLOGY PRACTICE American Society for Cytopathology San Antonio, Texas Sunday March 5, 2017 Disclosure of Relevant Financial
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Pulmonary adenocarcinoma Issues, Issues and more issues. Why the headache?
 Issues Pulmonary adenocarcinoma Issues, Issues and more issues. Why the headache? Classification Multiple nodules Invasive size Alain Borczuk, MD Weill Cornell Medicine Chronic headache - Classification
Issues Pulmonary adenocarcinoma Issues, Issues and more issues. Why the headache? Classification Multiple nodules Invasive size Alain Borczuk, MD Weill Cornell Medicine Chronic headache - Classification
Classification of non-small cell lung carcinomas (NSCLC)
") Classification of non-small cell lung carcinomas (NSCLC) 1. NordiQC Conference on Standardization in Applied Immunohistochemistry 4-7 June 2013 Birgit Guldhammer Skov, MD. DMeSci, Dept. Of Pathology, Rigshospitalet,
Classification of non-small cell lung carcinomas (NSCLC) 1. NordiQC Conference on Standardization in Applied Immunohistochemistry 4-7 June 2013 Birgit Guldhammer Skov, MD. DMeSci, Dept. Of Pathology, Rigshospitalet,
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion
 Clinical Case Discussion") Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
Early-stage locally advanced non-small cell lung cancer (NSCLC) Clinical Case Discussion Pieter Postmus The Clatterbridge Cancer Centre Liverpool Heart and Chest Hospital Liverpool, United Kingdom 1 2
8/22/2016. Major risk factors for the development of lung cancer are: Outline
 Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach
 The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
The 2015 World Health Organization Classification for Lung Adenocarcinomas: A Practical Approach Dr. Carol Farver Director, Pulmonary Pathology Pathology and Laboratory Medicine Institute Objectives Discuss
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Ground Glass Opacities
 Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
Ground Glass Opacities A pathologist s perspective Marie-Christine Aubry, M.D. Professor of Pathology Mayo Clinic Objectives Discuss the proposed new pathologic classification of adenocarcinoma with historical
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS
 LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
LUNG CANCER PATHOLOGY: UPDATE ON NEUROENDOCRINE LUNG TUMORS William D. Travis, M.D. Attending Thoracic Pathologist Memorial Sloan Kettering Cancer Center New York, NY PULMONARY NE TUMORS CLASSIFICATION
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center
 The new role of cytology in the diagnosis and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center Outline Role of cytology in the diagnosis of lung cancer Non-small
The new role of cytology in the diagnosis and management of lung cancer Maureen F. Zakowski, M.D. Memorial Sloan-Kettering Cancer Center Outline Role of cytology in the diagnosis of lung cancer Non-small
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Difficult Diagnoses and Controversial Entities in Neoplastic Lung
 Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Difficult Diagnoses and Controversial Entities in Neoplastic Lung Lynette M. Sholl, M.D. Associate Pathologist, Brigham and Women s Hospital Chief, Pulmonary Pathology Service Associate Professor, Harvard
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Lung/Thoracic Neoplasms. Manish Powari
 Lung/Thoracic Neoplasms Manish Powari Biopsy Techniques in Lung cancer diagnosis Decreased cellularity and architecture; thereby influencing subtyping Thoracotomy, resection VATS biopsy/resection L.node
Lung/Thoracic Neoplasms Manish Powari Biopsy Techniques in Lung cancer diagnosis Decreased cellularity and architecture; thereby influencing subtyping Thoracotomy, resection VATS biopsy/resection L.node
International association for the study of lung cancer/american thoracic society/european respiratory
 International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. William Travis, Elisabeth
International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. William Travis, Elisabeth
Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis
 1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE
 25 th IAP-Arab Division Conference 07-09 November 2013, Amman, Jordan MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE Fouad Al Dayel, MD, FRCPA, FRCPath Professor and Chairman Department
25 th IAP-Arab Division Conference 07-09 November 2013, Amman, Jordan MOLECULAR PREDICTIVE MARKERS OF LUNG CARCINOMA: KFSH&RC EXPERIENCE Fouad Al Dayel, MD, FRCPA, FRCPath Professor and Chairman Department
Tumor Board Discussions: Case 1
 Tumor Board Discussions: Case 1 David S. Ettinger, MD The Alex Grass Professor of Oncology Johns Hopkins University School of Medicine Baltimore, Maryland Case #1 50-year-old Asian female, never smoker
Tumor Board Discussions: Case 1 David S. Ettinger, MD The Alex Grass Professor of Oncology Johns Hopkins University School of Medicine Baltimore, Maryland Case #1 50-year-old Asian female, never smoker
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS
 THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS PULMONARY PATHOLOGY SOCIETY USCAP, BALTIMORE, March 2, 2013 William D. Travis, M.D. Dept of Pathology, Memorial Sloan-Kettering Cancer
THE IASLC/ERS/ATS ADENOCARCINOMA CLASSIFICATION RATIONALE AND STRENGTHS PULMONARY PATHOLOGY SOCIETY USCAP, BALTIMORE, March 2, 2013 William D. Travis, M.D. Dept of Pathology, Memorial Sloan-Kettering Cancer
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
YOUR LUNG CANCER PATHOLOGY REPORT
 UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
Histology: Its Influence on Therapeutic Decision Making
 Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
The ABCs of BAC: Bronchioloalveolar Carcinoma
 The ABCs of BAC: Bronchioloalveolar Carcinoma Howard (Jack) West, MD Medical Oncologist Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA March, 2009 President & CEO GRACE
The ABCs of BAC: Bronchioloalveolar Carcinoma Howard (Jack) West, MD Medical Oncologist Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA March, 2009 President & CEO GRACE
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Targeted Therapies in the Management of Non-Small Cell Lung Cancer. A Multi-Disciplinary Approach
 Targeted Therapies in the Management of Non-Small Cell Lung Cancer A Multi-Disciplinary Approach Course Faculty Medical Oncologists: Dr. Barb Melosky British Columbia Cancer Agency, Vancouver, BC Dr. Jeff
Targeted Therapies in the Management of Non-Small Cell Lung Cancer A Multi-Disciplinary Approach Course Faculty Medical Oncologists: Dr. Barb Melosky British Columbia Cancer Agency, Vancouver, BC Dr. Jeff
Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors.
 Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors. o Classify bronchogenic carcinoma. o Discuss etiopathogenesis of bronchogenic ca. o Discuss morphological features of squamous
Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors. o Classify bronchogenic carcinoma. o Discuss etiopathogenesis of bronchogenic ca. o Discuss morphological features of squamous
Expert Round Table with Drs. Anne Tsao and Alex Farivar Part 1: Elderly Man with Indolent Bronchioloalveolar Carcinoma
 Expert Round Table with Drs. Anne Tsao and Alex Farivar Part 1: Elderly Man with Indolent Bronchioloalveolar Carcinoma February 2010 I d like to welcome everyone, thanks for coming out to our lunch with
Expert Round Table with Drs. Anne Tsao and Alex Farivar Part 1: Elderly Man with Indolent Bronchioloalveolar Carcinoma February 2010 I d like to welcome everyone, thanks for coming out to our lunch with
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Lecture Goals. Lung (Bronchogenic) Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic
 Cancer. Causes of Lung Cancer. Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic") Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
Lecture Goals Origin of Lung Cancer Subtypes New Treatment Paradigms in Lung Cancer Overview of Lung Cancer Elizabeth Weihe, MD Assistant Professor of Radiology Director of UCSD RECIST clinic Lung (Bronchogenic)
EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE. Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University
 EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University Objectives Brief overview of EBUS-FNA Strategies to optimize
EBUS-FNAB: HOW TO OPTIMIZE YOUR CYTOLOGY SAMPLES, LHSC EXPERIENCE Dr. Mariamma Joseph Division Head of Cytopathology LHSC and Western University Objectives Brief overview of EBUS-FNA Strategies to optimize
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
EBUS-TBNA Diagnosis and Staging of Lung Cancer
 EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
EBUS-TBNA Diagnosis and Staging of Lung Cancer Nirag Jhala MD, MIAC Professor of Pathology and Lab Med. Director of Anatomic Pathology and Cytopathology Lewis Katz School of Medicine@ Temple University
Neuroendocrine Lung Tumors Myers
 Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
Diagnosis and Classification of Neuroendocrine Lung Tumors Jeffrey L. Myers, M.D. A. James French Professor Director, Anatomic Pathology & MLabs University of Michigan, Ann Arbor, MI myerjeff@umich.edu
The new international multidisciplinary lung adenocarcinoma
 Eur Respir J 2011; 38: 239 243 DOI: 10.1183/09031936.00026711 CopyrightßERS 2011 EDITORIAL Paradigm shifts in lung cancer as defined in the new IASLC/ATS/ERS lung adenocarcinoma classification W.D. Travis*,"",
Eur Respir J 2011; 38: 239 243 DOI: 10.1183/09031936.00026711 CopyrightßERS 2011 EDITORIAL Paradigm shifts in lung cancer as defined in the new IASLC/ATS/ERS lung adenocarcinoma classification W.D. Travis*,"",
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
The lung adenocarcinoma guidelines: what to be considered by surgeons
 Review Article The lung adenocarcinoma guidelines: what to be considered by surgeons Rodrigo A. S. Sardenberg 1, Evandro Sobroza Mello 1, Riad N. Younes 2 1 Hospital Alemão Oswaldo Cruz, São Paulo, Brazil;
Review Article The lung adenocarcinoma guidelines: what to be considered by surgeons Rodrigo A. S. Sardenberg 1, Evandro Sobroza Mello 1, Riad N. Younes 2 1 Hospital Alemão Oswaldo Cruz, São Paulo, Brazil;
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Uniportal video-assisted thoracoscopic surgery segmentectomy
 Case Report on Thoracic Surgery Page 1 of 5 Uniportal video-assisted thoracoscopic surgery segmentectomy John K. C. Tam 1,2 1 Division of Thoracic Surgery, National University Heart Centre, Singapore;
Case Report on Thoracic Surgery Page 1 of 5 Uniportal video-assisted thoracoscopic surgery segmentectomy John K. C. Tam 1,2 1 Division of Thoracic Surgery, National University Heart Centre, Singapore;
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL
 The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
Case Studies. Ravi Salgia, MD, PhD
 Case Studies Ravi Salgia, MD, PhD Professor and Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Associate Director for Clinical Sciences Research City of Hope 04-21-2018 Objectives
Case Studies Ravi Salgia, MD, PhD Professor and Arthur & Rosalie Kaplan Chair Medical Oncology and Therapeutics Research Associate Director for Clinical Sciences Research City of Hope 04-21-2018 Objectives
Lung /4/18. Please submit all questions concerning the webinar content through the Q&A panel.
 Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Fast Facts: Non-Small-Cell Lung Cancer
 Fast Facts Fast Facts: Non-Small-Cell Lung Cancer Mary O Brien MD FRCP Consultant Medical Oncologist The Royal Marsden NHS Foundation Trust London, UK Benjamin Besse MD PhD Thoracic Cancer Unit, Head Department
Fast Facts Fast Facts: Non-Small-Cell Lung Cancer Mary O Brien MD FRCP Consultant Medical Oncologist The Royal Marsden NHS Foundation Trust London, UK Benjamin Besse MD PhD Thoracic Cancer Unit, Head Department
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination
 National Quality Strategy Domain: Communication and Care Coordination") Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE:
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
GROUP 1: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases. Including: Excluding:
 GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Molecular Pathobiology of Lung Cancer. William K. Funkhouser, MD PhD Department of Pathology and Lab Medicine University of North Carolina
 Molecular Pathobiology of Lung Cancer William K. Funkhouser, MD PhD Department of Pathology and Lab Medicine University of North Carolina Outline Lung Anatomy Lung Carcinoma Classification & Morphology
Molecular Pathobiology of Lung Cancer William K. Funkhouser, MD PhD Department of Pathology and Lab Medicine University of North Carolina Outline Lung Anatomy Lung Carcinoma Classification & Morphology
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination
 National Quality Strategy Domain: Communication and Care Coordination") Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE:
Quality ID #395: Lung Cancer Reporting (Biopsy/Cytology Specimens) National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE:
UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER. Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory
 UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER travisw@mskcc.org Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory American Society of Cytopathology Companion
UPDATES IN THE SURGICAL PATHOLOGY OF LUNG CANCER travisw@mskcc.org Four Ps of Pulmonary Cytopathology: Procedural, Predictive, Personalized and Participatory American Society of Cytopathology Companion
Lung cancer is the most common cause of cancer death in
 ORIGINAL ARTICLE Are There Imaging Characteristics Associated with Epidermal Growth Factor Receptor and Mutations in Patients with Adenocarcinoma of the Lung with Bronchioloalveolar Features? Catherine
ORIGINAL ARTICLE Are There Imaging Characteristics Associated with Epidermal Growth Factor Receptor and Mutations in Patients with Adenocarcinoma of the Lung with Bronchioloalveolar Features? Catherine
5/1/2009. Squamous Dysplasia/CIS AAH DIPNECH. Adenocarcinoma
 Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
Pathological Assessment of Diagnostic Specimens Keith Kerr Department of Pathology Aberdeen University Medical School Aberdeen Royal Infirmary Foresterhill, Aberdeen, Scotland, UK Tumours of the Lung:
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Diagnosis of lung cancer. Diagnosis Subtyping. Morphologic features Approach to small samples
 Lung Cytology Lung Cytology Pınar Fırat,MD,MIAC Diagnosis of lung cancer Detection of infections Evaluation of interstitial diseases Morphologic features Approach to small samples Lung Cancer Second most
Lung Cytology Lung Cytology Pınar Fırat,MD,MIAC Diagnosis of lung cancer Detection of infections Evaluation of interstitial diseases Morphologic features Approach to small samples Lung Cancer Second most
Metastatic Renal Cell Carcinoma: The Importance of Immunohistochemistry in Differential Diagnosis
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
The small subsolid pulmonary nodules. What radiologists need to know.
 The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
The small subsolid pulmonary nodules. What radiologists need to know. Poster No.: C-1250 Congress: ECR 2016 Type: Educational Exhibit Authors: L. Fernandez Rodriguez, A. Martín Díaz, A. Linares Beltrán,
September 2014 Imaging Case of the Month. Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Primary enteric adenocarcinoma with predominantly signet ring features of the lung: A case report with clinicopathological and molecular findings
 CASE REPORT Primary enteric adenocarcinoma with predominantly signet ring features of the lung: A case report with clinicopathological and molecular findings Makoto Nagashima 1, Ayako Moriyama 1, Yasuo
CASE REPORT Primary enteric adenocarcinoma with predominantly signet ring features of the lung: A case report with clinicopathological and molecular findings Makoto Nagashima 1, Ayako Moriyama 1, Yasuo
Diagnostic challenge: Sclerosing Hemangioma of the Lung. Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and
 Diagnostic challenge: Sclerosing Hemangioma of the Lung. S. Arias M.D, R. Loganathan M.D, FCCP Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and Mental Health Center/Weill
Diagnostic challenge: Sclerosing Hemangioma of the Lung. S. Arias M.D, R. Loganathan M.D, FCCP Department of Medicine, Division of Pulmonary and Critical Care, Lincoln Medical and Mental Health Center/Weill
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD. Mount Carrigain 2/4/17
 Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Lung Cancer Genetics: Common Mutations and How to Treat Them David J. Kwiatkowski, MD, PhD Mount Carrigain 2/4/17 Histology Adenocarcinoma: Mixed subtype, acinar, papillary, solid, micropapillary, lepidic
Pulmonary adenocarcinoma: implications of the recent advances in molecular biology, treatment and the IASLC/ATS/ERS classification
 Review Article Pulmonary adenocarcinoma: implications of the recent advances in molecular biology, treatment and the IASLC/ATS/ERS classification Swaroop Revannasiddaiah 1, Priyanka Thakur 2, Bhaskar Bhardwaj
Review Article Pulmonary adenocarcinoma: implications of the recent advances in molecular biology, treatment and the IASLC/ATS/ERS classification Swaroop Revannasiddaiah 1, Priyanka Thakur 2, Bhaskar Bhardwaj
RCPath Cancer datasets guiding care for the individual and the wider population. Reporting of lung cancer
 RCPath Cancer datasets guiding care for the individual and the wider population Reporting of lung cancer Thursday 30 th March 2017 Coin Street Conference Centre London Professor Andrew G Nicholson, DM,
RCPath Cancer datasets guiding care for the individual and the wider population Reporting of lung cancer Thursday 30 th March 2017 Coin Street Conference Centre London Professor Andrew G Nicholson, DM,
Lung Cancer Diagnosis for Primary Care
 Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Dr. Andres Wiernik. Lung Cancer
 Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Educational Objectives. Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach.
 Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Primary Pulmonary Colloid Adenocarcinoma: How Can We Obtain a Precise Diagnosis?
 doi: 10.2169/internalmedicine.1153-18 Intern Med 57: 3637-3641, 2018 http://internmed.jp CASE REPORT Primary Pulmonary Colloid Adenocarcinoma: How Can We Obtain a Precise Diagnosis? Shinsuke Ogusu 1, Koichiro
doi: 10.2169/internalmedicine.1153-18 Intern Med 57: 3637-3641, 2018 http://internmed.jp CASE REPORT Primary Pulmonary Colloid Adenocarcinoma: How Can We Obtain a Precise Diagnosis? Shinsuke Ogusu 1, Koichiro
DIAGNOSIS OF LUNG CANCER. Dr. Sayeed ahmed, Assistant prof, MD,DAA.
 DIAGNOSIS OF LUNG CANCER Dr. Sayeed ahmed, Assistant prof, MD,DAA. Diagnosis of lung cancer can be done by 1) Clinical presentation 2) Investigations a) non invasive b) invasive Clinical Presentation Metastatic
DIAGNOSIS OF LUNG CANCER Dr. Sayeed ahmed, Assistant prof, MD,DAA. Diagnosis of lung cancer can be done by 1) Clinical presentation 2) Investigations a) non invasive b) invasive Clinical Presentation Metastatic
Lung Cancer Update. Disclosures. None
 Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
Utility of small biopsies for diagnosis of lung nodules: doing more with less
 & 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 S43 Utility of small biopsies for diagnosis of lung nodules: doing more with less Sanjay Mukhopadhyay Department of Pathology, State University
& 2012 USCAP, Inc. All rights reserved 0893-3952/12 $32.00 S43 Utility of small biopsies for diagnosis of lung nodules: doing more with less Sanjay Mukhopadhyay Department of Pathology, State University
Minimally invasive adenocarcinoma. 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS)
") Minimally invasive adenocarcinoma 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS) 2b lepidic acinar 2c papillary micropapillary solid 2d cribriform
Minimally invasive adenocarcinoma 5mm or less = microinvasion No necrosis No lymphatic or pleural invasion No spread through air-spaces (STAS) 2b lepidic acinar 2c papillary micropapillary solid 2d cribriform