Breast Cancer: Chemotherapy and Novel Agents
|
|
|
- Elvin O’Neal’
- 6 years ago
- Views:
Transcription
1 North Carolina Oncology Association & South Carolina Oncology Society Joint Membership Meeting ~ February 26 27, 2010 The Ballantyne Resort ~ Charlotte, NC Breast Cancer: Chemotherapy and Novel Agents Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center
2 Faculty Disclosure Consultant: sanofi aventis, BiPar, Wyeth, Pfizer, Genentech, BMS, Novartis Research Support: GSK, Boehringer Ingelheim, Genentech, Wyeth, BMS
3 NEW DEVELOPMENTS IN CHEMOTHERAPY DECISION MAKING

4 CAF Benefit in Node positive by Recurrence Score (RS) DFS: RS <18 RS RS prognostic 0.50 for tamoxifen treated patients with positive nodes and predicts significant benefit of CAF in high recurrence score. A low 0.25 recurrence score identifies women who might not benefit from 0.00 p = 0.97 at 10 years HR 1.02 ( ) CAF T (n=91, 26 events) Tamoxifen (n=55, 15 events) p = 0.48 at 10 years HR 0.72 ( ) CAF T (n=46, 22 events) Tamoxifen (n=57, 20 events) p = at 10 years HR 0.59 ( ) anthracycline based chemotherapy, despite positive nodes. CAF T (n=47, 26 events) Tamoxifen (n=71, 28 events) No benefit to CAF over time if low RS Years since registration Interaction p=0.053 Strong benefit if high RS 4 Albain KS, et al. Lancet Oncol CAF=cyclophosphamide, doxorubicin + fluorouracil
5 Clinical Applications of Genomic Profiles Depend On: Identification of a low risk group in whom no further therapy is needed OR Confirmation of accurate prediction of response based on profile Have either of those criteria been met for multigene profiles in N+?
6 Prognostic Profiles Work in HR+ Regardless of Nodal Status. TransATAC 306 of 9366 node positive Endocrine Rx only RS was prognostic in N+: Other prognostic profiles in N+: E2197 (RS, all chemoendocrine) 70 gene profile retrospective study SWOG 8814 (RS) Tam vs CAF Tam Only 1 asks a therapeutic question All (n=1231) Node negative (n=872) Tamoxifen (n=432) Anastrozole (n= 440) Node positive (n=306) Tamoxifen (n=152) Anastrozole (n=154) Adjusted HR (for 50 pt change)* (central grading) Dowsett et al. SABCS 08, Abs 53; Goldstein et al, JCO 08, Mook et al, BCRT 2009; Albain et al, Lancet Oncol 09
7 Genomic Profiles and Absolute Risk: Only Part of the Equation What is the risk of recurrence in N+ postmenopausal women with low Recurrence Score treated with tamoxifen only? SWOG % relapse at 10y ATAC 10% relapse at 10y Selection matters
8 Recurrence Score and Prognosis in Node-positive: SWOG 8814 Tamoxifen-alone Arm RS Group 10-year DFS 10-year OS RS <18 (n=55) 60% 77% RS (n=46) 49% 68% RS 31 (n=47) 43% 51% Prognostic, but there is NO good risk group here Albain KS et al. Lancet Oncol Dec: Epub ahead of print. 8
9 Level of Evidence Re Chemo Benefit? I II III IV V Prospective, high power, designed to test marker) OR Meta-analysis of Level II Prospective clinical trial not designed to test marker. Large study, high % of tissue available. Large but retrospective studies OR Small # of specimens Small retrospective studies, casecontrol studies Pilot studies N=1477 All postmenopausal (Relatively small trial) Concurrent CAF/T N=967 N= 367 Missing tissue Int/High RS: not helpful N=146 low Recurrence Score (the group of interest) 9
10 Recurrence Score and Chemo Benefit at 10 Years Point of inflection RS ~8 B-20 was much higher (benefit not seen until high RS) Effect of concurrent tam? Effect of higher risk = higher benefit? Is there a RS that we know identifies a group with no benefit of chemo, even 3 rd generation? Does this mean that RS=8 is meaningful? This is why there is a TailoRx trial
11 ECOG 1199 By Race and Tumor Subtype 80 Paclitaxel A C N= (8%) African American 175 mg/m 2 35 Docetaxel 100 Sparano J, et al. N Engl J Med Apr 17; 358(16):
, black pts")

12 Race and Outcome in E1199 In E1199 (uniform Rx), black pts had worse DFS and OS than non black. Why? Sparano J, et al. SABCS 2009.

 Sparano J, et al.")
13 Disease-Free and Overall Survival: Triple Negative Disease No difference within triple negative subtype (n~900, 129 black) Sparano J, et al. SABCS 2009.

14 Race and Outcome in Hormone Receptor + HER2- Difference driven by ER positive, HER2 negative subsets.? Heterogeneity of non protocol driven endocrine therapy?? Heterogeneity of luminal subtypes by race? Sparano J, et al. SABCS 2009.
15 Multivariate Model in HR-Pos/HER2-Neg Group: DFS Additional Variables Added to Above Model HR (95% CI) P value Black race only 1.41 (1.00, 2.00) Obesity only 1.26 (1.04, 1.51) Race & Obesity Race Obesity Race-Obesity Interaction Black (Obese) Black (Not Obese) 1.33 (0.93,1.89) 1.23 (1.02, 1.49) 1.09 (0.68, 1.74) 1.80 (1.06, 3.03) Proportional Hazards Model - included Age, Node #, Size, Menopausal Status, Surgery Type. Type of endocrine therapy was excluded because was NS in univariate model. Sparano J, et al. SABCS 2009.
16 Conclusions Black race associated with Younger age and more obesity at presentation Higher rates of triple negative and HER2-pos disease Larger tumor size and less nodal involvement Poorer outcomes in HR-pos/HER2-neg disease Not explained by comorbidities or disparities in care Obesity also appears to be a contributing factor Other confounding variables Findings consistent with some prior reports Clinical trial populations
17 NEW DEVELOPMENTS Biologically Unselected Populations
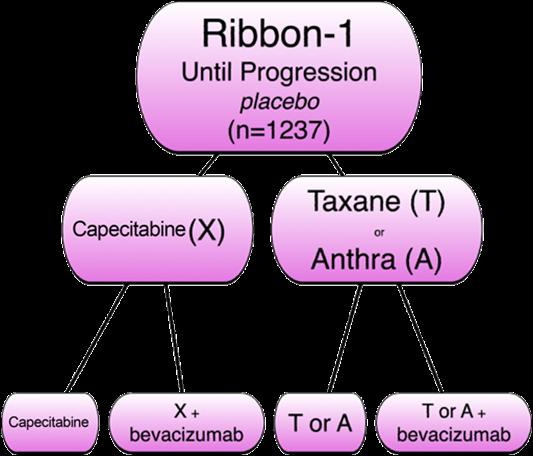
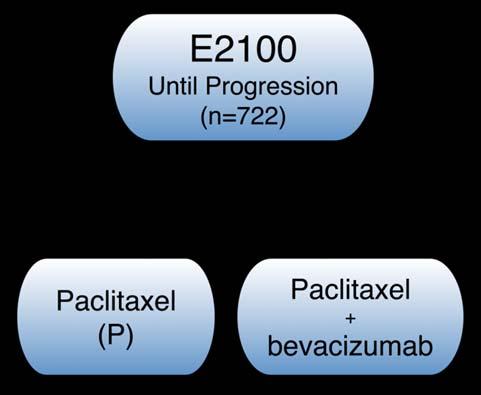
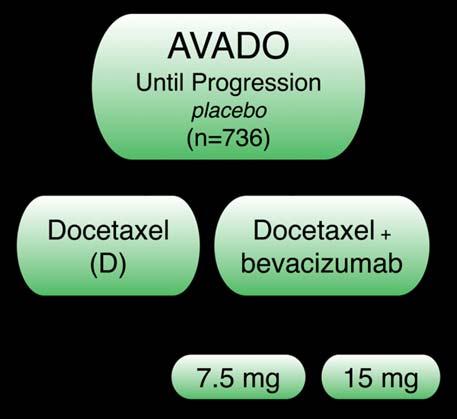
18 First Line Bevacizumab Trials Miller K et al. New England J Med 2007; 357(26): ; Miles D et al, J Clin Oncol 2008;26:50s, Abstract 1036; Robert N et al. J Clin Oncol 2009; 27:18s:, Abstract 1005.
 ORR: 37 vs. 21% (p<0.")
 PFS (primary endpoint) Low: 8.7 vs 8 mos (p=0.03) High: 8.")
 High: 63 vs 44% (p=0.0001) Overall Survival: No sig.")
 A/T: 9.2 vs. 8 mos (p<0.0001) ORR: X: 35 vs 24% (p=0.")
 Overall Survival: Not mature Miller K et al.")
19 Summary Results First Line Bevacizumab PFS (primary endpoint) 12 vs. 6 mos (p<0.001) ORR: 37 vs. 21% (p<0.001) Overall Survival: 27 vs. 25 mos (p=0.16) PFS (primary endpoint) Low: 8.7 vs 8 mos (p=0.03) High: 8.8 vs 8 mos (p=0.0099) ORR: Low: 55 vs 44% (p=0.03) High: 63 vs 44% (p=0.0001) Overall Survival: No sig. difference PFS (primary endpoint) X: 8.7 vs. 5.7 mos (p=0.0002) A/T: 9.2 vs. 8 mos (p<0.0001) ORR: X: 35 vs 24% (p=0.0092) A/T: 51 vs 38% (p=0.0054) Overall Survival: Not mature Miller K et al. New England J Med 2007; 357(26): ; Miles D et al, J Clin Oncol 2008;26:50s, Abstract 1036; Robert N et al. J Clin Oncol 2009; 27:18s:, Abstract 1005.
20 RIBBON 2: Phase III Trial of Second Line Bevacizumab + Chemotherapy Patients with previously treated MBC (HER2 negative or HER2 status unknown) (N = 684) Chemotherapy Regimens* Taxane or Gemcitabine or Capecitabine or Vinorelbine Bevacizumab 15 mg/kg every 3 wks or 10 mg/kg every 2 wks + Chemotherapy (n = 459) Stratified by chemotherapy regimen, time between MBC diagnosis and first PD, and hormone receptor status; randomized 2:1 Placebo + Chemotherapy (n = 225) Treat until disease progression *Dose and schedule of chemotherapy regimens (selected by investigator): Taxane: paclitaxel 90 mg/m 2 /wk for 3 of 4 wks; paclitaxel 175 mg/m 2, nab paclitaxel 260 mg/m 2, or docetaxel mg/m 2 every 3 wks. Gemcitabine 1250 mg/m 2 on Days 1 and 8 every 3 wks. Capecitabine 2000 mg/m 2 on Days 1 14 every 3 wks. Vinorelbine 30 mg/m 2 /wk every 3 wks. Dose of bevacizumab dependent on chemotherapy regimen used. Brufsky A, et al. SABCS Abstract 42. Brufsky A et al. SABCS 2009, Abstract 42.
21 Proportion of Progression Free Patients at Risk, n Chemo/placebo Chemo/bev RIBBON 2: Progression Free Survival Primary Endpoint of PFS, ITT Population Median PFS: 7.2 vs. 5.1 mos HR: 0.78 (P =.0072) Duration of PFS (Mos) Chemo/placebo (n = 225) Chemo/bevacizumab (n = 459) Brufsky A, et al. SABCS Abstract 42. Brufsky A et al. SABCS 2009, Abstract 42.

22 Chemo/Bev Chemo p value PFS (1⁰ endpoint) 7.2m 5.1m ORR 40% 30% 0.02 OS (median) 18m 15m 0.37 Median F/u: 15 mo Drugs: Taxane 44% Gemcitabine 23% Capecitabine 21% Vinorelbine 11% PFS: Chemo/Bev Chemo Taxane 8.0m 5.8m Gem. 6.0m 5.5m Cape 6.9m 4.1m Vin 5.7m 7.0m Brufsky A et al. SABCS 2009, Abstract 42.
23 RIBBON 2: Phase III Trial of Second Line Bevacizumab + Chemotherapy Study met primary endpoint Improved PFS with bevacizumab + standard chemotherapy vs chemotherapy alone for second line treatment of HER2 negative MBC Observed improvement in PFS supported by secondary endpoint of ORR OS data immature Bevacizumab combination chemotherapy regimens well tolerated with no unexpected adverse events Feasible to consider bevacizumab in second line setting Brufsky A, et al. SABCS Abstract 42.
24 SOLTI 0701: Phase IIb Study of Combination Sorafenib + Capecitabine LABC/Stage IV < 1 prior chemo HER2 neg Sorafenib 400 mg PO BID continuously + Capecitabine 100 mg/m 2 PO BID for 14 of 21 days (n = 115) Stratified by visceral vs nonvisceral disease (N = 229) Placebo PO BID continuously + Capecitabine 100 mg/m 2 PO BID for 14 of 21 days (n = 114) Until disease progression or unacceptable toxicity Baselga J, et al. SABCS Abstract 45. Baselga J et al. Eur J Cancer;7 (supp):3

25 Sorafenib (Targets VEGFR, PDGFR, Flt 3, c Kit, MET) Sorafenib Sorafenib Wilhelm SM, et al. Cancer Res Oct 1:64(19):
 P = 0.0006* 42% reduction in the risk of disease progression SOR+CAP 0.00 0.0 1.5 3.0 4.5 6.0 7.5 9.0 10.5 12.0 13.5 15.0 Months PL+CAP *One sided Baselga J et al.")
26 Progression Free Survival: Intent to Treat Population PFS Probability SOR + CAP N=115 PL + CAP N=114 Median PFS, mos HR (95% CI) ( ) P = * 42% reduction in the risk of disease progression SOR+CAP Months PL+CAP *One sided Baselga J et al. Eur J Cancer;7 (supp):3
27 Progression Free Survival: Sensitivity Analyses Analysis Median PFS (mos) SOR PL + +CAP CAP P Value* ITT First-line therapy Second-line therapy Per-protocol NPT as PFS event Favors SOR+CAP Favors PL+CAP NPT not considered *One sided NPT=non protocol anti cancer therapy ; PL=placebo (protocol prohibited new anti cancer treatment or surgery) HR (95% CI) Baselga J et al. Eur J Cancer;7 (supp):3
28 Adverse Event Rates* Overall incidence > 10% and Grade 3/4 2% in either treatment arm Sorafenib + Capecitabine (N=112) Placebo + Capecitabine (N=112) All (%) Grade 3 (%) Grade 4 (%) All (%) Grade 3 (%) Grade 4 (%) HFSR Diarrhea Mucosal inflammation Asthenia Rash Hypertension Fatigue Musculoskeletal pain Dyspnea Neutropenia *Treatment emergent Baselga J et al. Eur J Cancer;7 (supp):3
29 SOLTI 0701: Phase IIb Study of Sorafenib + Capecitabine Sorafenib + capecitabine 42% reduction in risk of disease progression or death PFS benefit observed in subgroup analyses PFS benefit noted in both first line and second line Increased incidence of hand foot syndrome reported in sorafenib/capecitabine arm Phase III registration trial planned for sorafenib/ capecitabine in advanced breast cancer
30 NEW DEVELOPMENTS IN CHEMOTHERAPY HER2 Driven
31 BCIRG 006: Third Analysis (Last one, they promise) AC T 4 x AC 4 x Docetaxel 60/600 mg/m mg/m 2 Her 2+ (Central FISH) N+ or high risk N N=3,222 AC TH TCH 4 x AC 4 x Docetaxel 60/600 mg/m mg/m 2 1 Year Trastuzumab 6 x Docetaxel and Carboplatin 75 mg/m 2 AUC 6 1 Year Trastuzumab Slamon D., SABCS 2009.
 TCH 0.64 (0.41 1.01) No interaction benefit with risk HR 4+ LN 0.66 both H arms Slamon D., SABCS 2009.")
32 BCIRG 006: Disease Free Survival Months from randomization Node negative subset ~ 300 per arm; ~ 100 events ACTH HR 0.47 ( ) TCH 0.64 ( ) No interaction benefit with risk HR 4+ LN 0.66 both H arms Slamon D., SABCS 2009.

33 BCIRG 006: Survival Months from randomization Slamon D., SABCS 2009.
 18m 15m 0.37 Leukemia 0.6% (6) 0.1% (1) 0.")
34 BCIRG 006: Toxicity Median EF over time Months from randomization AC T TCH AC TH CHF 0.7% 0.4% 2.0% Cardiac death OS (median) 18m 15m 0.37 Leukemia 0.6% (6) 0.1% (1) 0.1% (1)
35 BCIRG 006 Adding trastuzumab to chemo works TCH is a reasonable alternative, especially in patients with cardiac issues. Underpowered but inevitable comparisons of TCH vs AC TH suggest higher efficacy but more CHF Stipulating that this is an underpowered analysis : Suggestion that this benefit is largely confined to Topo II nonamplified (which are the majority) in topo II + you can either add H or give anthracycline, and both looked a little better than one.
36 n=3,505 R A N D O M I Z E N9831: Arm B Efficacy Analysis (Finally) Arm A: AC q 3w x 4 Arm B: AC q 3w x 4 Arm C: Cumulative cardiac events: AC q 3w x 4 Paclitaxel qw x 12 Paclitaxel qw x 12 Paclitaxel qw x 12 + H qw x 12 AC TH H AC T H RT and/or hormonal therapy as indicated N9831 H qw x 52 H qw x 40 AC T Perez EA et al, JCO 2008; Perez EA et al, SABCS 2009.
37 Alive and disease free (%) Control (A) vs Sequential (B) Disease Free Survival Logrank p= % 79.7% % 71.9% Years from randomization Perez EA et al, SABCS AC T H (164 events) AC T (222 events) N9831 No. at risk


38 Alive and disease free (%) Sequential (B) vs Concurrent (C) Disease Free Survival Logrank p= % 85.7% AC T+H H ( 138 events) AC T H (174 events) 84.2% 79.8% N Years from randomization No. at risk Perez EA et al, SABCS 2009.
39 Results: Disease Free Survival N9831 Joint Analysis (N9831/B31) ~3 yr median follow up 1 Pairwise comparison AC T vs AC T+H H *Stratified nodal status and receptor status Number of events P value 619 < Adj HR (95%CI) 0.48 ( ) N9831 Analysis (N9831) >5 yr median follow up 2 A B B C Pairwise comparison AC T vs AC T H (n=2,184) AC T H vs AC T+H H (n=1,903)* Number of events Log rank P value Adj HR* (95%CI) ( ) ( ) *Excluding pts on Arm B entered when Arm C was closed 1 Perez EA et al. J Clin Oncol 2007; 2 Perez EA et al. SABCS 2009 #701.
40 Results: Overall Survival N9831 Joint Analysis (N9831/B31) ~3 yr median follow up 1 Pairwise comparison AC T vs AC T+H H Number of events P value Unadj HR (95%CI) 0.65 ( ) N9831 Analysis (N9831) >5 yr median follow up 2 Pairwise comparison Number of events Log rank P value Unadj HR* (95%CI) A B AC T vs AC T H (n=2,184) ( ) B C AC T H vs AC T+H H (n=1,903)* ( ) *Excluding pts on Arm B entered when Arm C was closed 1 Perez EA et al. J Clin Oncol 2007; 2 Perez EA et al. SABCS 2009#701.
41 Conclusions Adjuvant trastuzumab works It is probably better to give adjuvant trastuzumab concurrently with chemotherapy, although cardiac toxicity is higher.
42 Phase II Trial of Her TC in Patients with HER2+ Early BC Accrual: 263 (260 in cardiac safety population) Eligibility T1-2, N0-1 Her2+ (IHC 3+ or FISH+) LVEF 50% by MUGA or ECHO Docetaxel (T) Cyclophosphamide (C) Trastuzumab (H) T = 75mg/m 2 IV q 3 weeks x 4 C = 600mg/m 2 IV q 3 weeks x 4 H = 4mg/Kg Wk 1 2mg/Kg/week Wk mg/Kg q 3 weeks Wk Cardiac events: Sixteen patients (6.1%) LVEF decline to 50% any time during treatment. Nine patients (3.4%) discontinued trastuzumab due to decrease in LVEF. No cases of CHF. 17.5% study discontinuation (patient ~5%, toxicity ~10%) Jones SE, SABCS 2009.
43 Other HER2 Directed Agents

 combinations.")
44 Phase I/II Neratinib Combination Studies (Phase II part) With Paclitaxel >50% 2 nd + line, 15% 1 st line 30% prior H, 15% prior L With Vinorelbine >70% 2 nd + line, 0% 1 st line 100% prior H Diarrhea (any grade) > 90%. This is the issue for neratinib (also lapatinib) combinations. Chow, SABCS 2009, Abs 5081; Awada, SABCS 2009, Abs 5095.
 conjugated to trastuzumab similar to gemtuzumab (Myelotarg) T MCC DM1 Y HER2 mediated")

45 Trastuzumab DM1 (T DM1), a HER2 Antibody Drug Conjugate Maytansine analogue DM1 (antitubule akin to vincas) conjugated to trastuzumab similar to gemtuzumab (Myelotarg) T MCC DM1 Y HER2 mediated internalization Beeram et al. J Clin Oncol Average number DM1 molecules/monoclonal antibody=3.5 T T MCC DM1 Lysine MCC DM1 Lysosomal degradation Active metabolite can t cross plasma membrane (no bystander effect)
 Heavily pretreated (prior A, T, X, H, L required): Krop I et al, SABCS 2009")
46 50% ER+ T DM1 Phase II (n=100) Median time since stage IV diagnosis ~ 40 m (selected population) Heavily pretreated (prior A, T, X, H, L required): Krop I et al, SABCS 2009 #710.

47 T DM1 Efficacy Little cardiotoxicity, well tolerated Coming soon! Combination studies with other biologics in progress Krop I et al, SABCS 2009 #710.
48 Conclusions Genomic prognostic profiles are part of the armamentarium in all ER+ HER2 disease Caution can t ignore anatomy Lots of antiangiogenesis agents and studies largely in combination with chemotherapy. Bevacizumab works, but in whom? Sorafenib promising, but toxicity issues must be considered Studies in HER2+ disease T DM1 and others likely soon to be added to armamentarium!
49 Thank you
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Non-Anthracycline Adjuvant Therapy: When to Use?
 Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Considerations in Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer
 Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER. Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx
 OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
Update in the treatment of Her2- overexpressing breast cancers. Fabrice ANDRE Institut Gustave Roussy Villejuif, France
 Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Postoperative Adjuvant Chemotherapies. Stefan Aebi Luzerner Kantonsspital
 Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Novel Preoperative Therapies for HER2-Positive Breast Cancer. Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center
 Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Nadia Harbeck Breast Center University of Cologne, Germany
 Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
New chemotherapy drugs in metastatic breast cancer. Guy Jerusalem, MD, PhD
 New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA
 Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2017 Relative Risk HER2-positive Breast
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2017 Relative Risk HER2-positive Breast
Novel Chemotherapy Agents for Metastatic Breast Cancer. Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX
 Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Dennis J Slamon, MD, PhD
 I N T E R V I E W Dennis J Slamon, MD, PhD Dr Slamon is Professor of Medicine, Chief of the Division of Hematology/Oncology and Director of Clinical and Translational Research at UCLA s David Geffen School
I N T E R V I E W Dennis J Slamon, MD, PhD Dr Slamon is Professor of Medicine, Chief of the Division of Hematology/Oncology and Director of Clinical and Translational Research at UCLA s David Geffen School
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
NeoadjuvantTreatment In BC When, How, Who?
 NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
HER2-positive Breast Cancer
 HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
BREAST CANCER RISK REDUCTION (PREVENTION)
") BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
Early Stage Disease. Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center
 SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Systemic therapy: HER-2 update. Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven
 Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Treatment of Early-Stage HER2+ Breast Cancer
 Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Edith A. Perez, Ahmad Awada, Joyce O Shaughnessy, Hope Rugo, Chris Twelves, Seock-Ah Im, Carol Zhao, Ute Hoch, Alison L. Hannah, Javier Cortes
 BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot
 Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer
 The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer
 New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives
 Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Metastatic Breast Cancer What is new? Subtypes and variation?
 Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
The TAILORx Trial: A review of the data and implications for practice
 The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
The TAILORx Trial: A review of the data and implications for practice Angela DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology University
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017
 TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
Adjuvant Systemic Therapy in Early Stage Breast Cancer
 Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Dilemmas in Adjuvant Chemotherapy Is adjuvant chemotherapy effective in ER+
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Dilemmas in Adjuvant Chemotherapy Is adjuvant chemotherapy effective in ER+
ASCO and San Antonio Updates
 ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
Adjuvant Chemotherapy + Trastuzumab
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Chemotherapy + Trastuzumab (Optimal Drugs / Dosage / Trastuzumab) Adjuvant Chemotherapy (Optimal Drugs / Optimal Dosage
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Chemotherapy + Trastuzumab (Optimal Drugs / Dosage / Trastuzumab) Adjuvant Chemotherapy (Optimal Drugs / Optimal Dosage
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer
 Node Positive Breast Cancer") Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Adjuvant endocrine therapy (essentials in ER positive early breast cancer)
") Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014
 MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned
 The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY. Dr. Carlos Garbino
 EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
Disease Update: Metastatic Breast Cancer
 Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA
 Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Anthracyclines for Breast Cancer? Are Adjuvant Anthracyclines Dispensible? Needs to be Answered in a Large Prospective Trial
 Anthracyclines for Breast Cancer? Are Adjuvant Anthracyclines Dispensible? Needs to be Answered in a Large Prospective Trial Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Dallas, TX Early Breast Cancer
Anthracyclines for Breast Cancer? Are Adjuvant Anthracyclines Dispensible? Needs to be Answered in a Large Prospective Trial Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Dallas, TX Early Breast Cancer
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Appendix 2. Adjuvant Regimens. AC doxorubin 60 mg/m 2 every 3 weeks x 4 cycles Cyclophosphamide 600 mg/m 2
 Appendix 2 Adjuvant Regimens AC doxorubin 60 mg/m 2 every 3 weeks x 4 cycles Cyclophosphamide 600 mg/m 2 CMF IV cyclophosphamide 600 mg/m 2 days 1 & 8 every 4 weeks methotrexate 40 mg/m 2 for 6 cycles
Appendix 2 Adjuvant Regimens AC doxorubin 60 mg/m 2 every 3 weeks x 4 cycles Cyclophosphamide 600 mg/m 2 CMF IV cyclophosphamide 600 mg/m 2 days 1 & 8 every 4 weeks methotrexate 40 mg/m 2 for 6 cycles
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND!
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
A vision for HER2 future
 School of Medical Oncology Department of Medical and Biological Sciences - University of Udine Department of Oncology - University Hospital of Udine A vision for HER2 future Current therapeutic algorithm
School of Medical Oncology Department of Medical and Biological Sciences - University of Udine Department of Oncology - University Hospital of Udine A vision for HER2 future Current therapeutic algorithm
Advanced HER2+ Breast Cancer: New Options and How to Deploy Them. José Baselga MD, PhD
 Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016
 Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016 Yes! Age disparities vary by tumor subtype Genomic risk prediction data in young women Adjuvant systemic therapy
Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016 Yes! Age disparities vary by tumor subtype Genomic risk prediction data in young women Adjuvant systemic therapy
Emerging Approaches for (Neo)Adjuvant Therapy for ER+ Breast Cancer
Adjuvant Therapy for ER+ Breast Cancer") Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Beyond the Guidelines: Clinical Investigators Provide Their Perspectives on Current Strategies and Ongoing Research in the Management of Breast Cancer
 Beyond the Guidelines: Clinical Investigators Provide Their Perspectives on Current Strategies and Ongoing Research in the Management of Breast Cancer Wednesday, December 11, 2013 7:30 PM 9:30 PM San Antonio,
Beyond the Guidelines: Clinical Investigators Provide Their Perspectives on Current Strategies and Ongoing Research in the Management of Breast Cancer Wednesday, December 11, 2013 7:30 PM 9:30 PM San Antonio,
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones
 ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
National Horizon Scanning Centre. Bevacizumab (Avastin) in combination with non-taxanes for metastatic breast cancer - first line therapy
 in combination with non-taxanes for metastatic breast cancer - first line therapy") Bevacizumab (Avastin) in combination with non-taxanes for metastatic breast cancer - first line therapy December 2007 This technology summary is based on information available at the time of research and
Bevacizumab (Avastin) in combination with non-taxanes for metastatic breast cancer - first line therapy December 2007 This technology summary is based on information available at the time of research and
Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician
 in older individuals: the oncologist s viewpoint for the geriatrician") Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician Hans Wildiers Medical oncologist, Leuven, Belgium Past chairman of the EORTC elderly task force President-elect
Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician Hans Wildiers Medical oncologist, Leuven, Belgium Past chairman of the EORTC elderly task force President-elect
Novel Preoperative Therapies for HER2-Positive Breast Cancer
 Key Findings to Date in the Neoadjuvant Therapy of H2+ Breast Cancer Novel Preoperative Therapies for H2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive
Key Findings to Date in the Neoadjuvant Therapy of H2+ Breast Cancer Novel Preoperative Therapies for H2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive
OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER
 OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER STEPHEN E. JONES, M.D. US ONCOLOGY RESEARCH THE WOODLANDS, TX TOPICS PREMENOPAUSAL BREAST CANCER POSTMENOPAUSAL BREAST CANCER THE FUTURE TOPICS PREMENOPAUSAL
OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER STEPHEN E. JONES, M.D. US ONCOLOGY RESEARCH THE WOODLANDS, TX TOPICS PREMENOPAUSAL BREAST CANCER POSTMENOPAUSAL BREAST CANCER THE FUTURE TOPICS PREMENOPAUSAL
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Role of Primary Resection for Patients with Oligometastatic Disease
 GBCC 2018, April 6, Songdo ConvensiA, Incheon, Korea Panel Discussion 4, How Can We Better Treat Patients with Metastatic Disease? Role of Primary Resection for Patients with Oligometastatic Disease Tadahiko
GBCC 2018, April 6, Songdo ConvensiA, Incheon, Korea Panel Discussion 4, How Can We Better Treat Patients with Metastatic Disease? Role of Primary Resection for Patients with Oligometastatic Disease Tadahiko
Adjuvant chemotherapy in older breast cancer patients: how to decide?
 Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Systemic Therapy Considerations in Inflammatory Breast Cancer
 Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Common disease 175,000 new cases/year 44,000 deaths/year Less than 10% with newly diagnosed at presentation have stage IV disease Chronic disease,
 Chemotherapy for Metastatic Breast Cancer: Recent Results HARMESH R. NAIK, MD. Karmanos Cancer Institute and St. Mary Hospital Metastatic breast cancer (MBC) Common disease 175,000 new cases/year 44,000
Chemotherapy for Metastatic Breast Cancer: Recent Results HARMESH R. NAIK, MD. Karmanos Cancer Institute and St. Mary Hospital Metastatic breast cancer (MBC) Common disease 175,000 new cases/year 44,000
Metronomic chemotherapy for breast cancer
 Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Updates From San Antonio Breast Cancer Symposium 2017
 Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all)
") Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all) 8 November 2014 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky
Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all) 8 November 2014 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky
Chemotherapy for Isolated Locoregional Recurrence
 Chemotherapy for Isolated Locoregional Recurrence Michelle Melisko MD Assistant Clinical Professor UCSF Helen Diller Family Comprehensive Cancer Center MBC and Improved Median Survival with New Therapies
Chemotherapy for Isolated Locoregional Recurrence Michelle Melisko MD Assistant Clinical Professor UCSF Helen Diller Family Comprehensive Cancer Center MBC and Improved Median Survival with New Therapies
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Management of HER2+ MBC SOBO 2012 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for Women s Cancer
Northwestern University Feinberg School of Medicine Management of HER2+ MBC SOBO 2012 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for Women s Cancer
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid
 Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
4, :00 PM 9:00 PM
 Consensus or Controversy? Clinical Investigators Provide Their Perspectives on Practical Issues and Research Questions in the Management of Breast Cancer Robert W Carlson, MD John Crown, MD Charles E Geyer
Consensus or Controversy? Clinical Investigators Provide Their Perspectives on Practical Issues and Research Questions in the Management of Breast Cancer Robert W Carlson, MD John Crown, MD Charles E Geyer
Toxicities of Chemotherapy Regimens used in Early Breast Cancer
 Toxicities of Chemotherapy Regimens used in Early Breast Cancer CERCIT Workshop February 17, 2012 Carlos H Barcenas, M.D., M.S. Fellow Hematology-Oncology MD Anderson Cancer Center CERCIT Scholar Outline
Toxicities of Chemotherapy Regimens used in Early Breast Cancer CERCIT Workshop February 17, 2012 Carlos H Barcenas, M.D., M.S. Fellow Hematology-Oncology MD Anderson Cancer Center CERCIT Scholar Outline
Update on New Perspectives in Endocrine-Sensitive Breast Cancer. James R. Waisman, MD
 Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
XII Michelangelo Foundation Seminar
 XII Michelangelo Foundation Seminar Paradigm shift? The Food and Drug Administration collaborative project P. Cortazar, Silver Spring, USA FDA Perspective: Moving from Adjuvant to Neoadjuvant Trials in
XII Michelangelo Foundation Seminar Paradigm shift? The Food and Drug Administration collaborative project P. Cortazar, Silver Spring, USA FDA Perspective: Moving from Adjuvant to Neoadjuvant Trials in
Adjuvant Endocrine Therapy: How Long is Long Enough?
 Adjuvant Endocrine Therapy: How Long is Long Enough? Harold J. Burstein, MD, PhD Dana-Farber Cancer Institute Harvard Medical School Boston, Massachusetts hburstein@partners.org I have no conflicts to
Adjuvant Endocrine Therapy: How Long is Long Enough? Harold J. Burstein, MD, PhD Dana-Farber Cancer Institute Harvard Medical School Boston, Massachusetts hburstein@partners.org I have no conflicts to
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Herceptin Pivotal Studies
 Herceptin Pivotal Studies Nuhad K Ibrahim, MD, FACP Associate Professor of Medicine Breast Medical Oncology Department MD Anderson Cancer Center Houston, TX, USAE-mail: nibrahim@mdanderson.org Herceptin
Herceptin Pivotal Studies Nuhad K Ibrahim, MD, FACP Associate Professor of Medicine Breast Medical Oncology Department MD Anderson Cancer Center Houston, TX, USAE-mail: nibrahim@mdanderson.org Herceptin