177 LU PSMA THERAPY OF PROSTATE CANCER INITIAL EXPERIENCE. Dr.SHAGOS.G.S. DRM, DNB,MNAMS, FEBNM ASTER MEDCITY.
|
|
|
- Shonda Lang
- 6 years ago
- Views:
Transcription

1 177 LU PSMA THERAPY OF PROSTATE CANCER INITIAL EXPERIENCE Dr.SHAGOS.G.S. DRM, DNB,MNAMS, FEBNM ASTER MEDCITY.
2 PROSTATE CANCER :MAGNITUDE OF PROBLEM ADENOCARCI NOMA PROSTATE:
3 TREATMENT OPTIONS DEPENDS ON STAGING,GLEASONS SCORE. LOCALISED DISEASE, LOW RISK : SURGERY / RADIATION THERAPY. INTERMEDIATE RISK: NEOADJUVANT ADT + SURGERY / R.T (EBRT OR BRACHYTHERAPY). SURGERY POSITIVE SURGICAL MARGINS ADJUVANT R.T
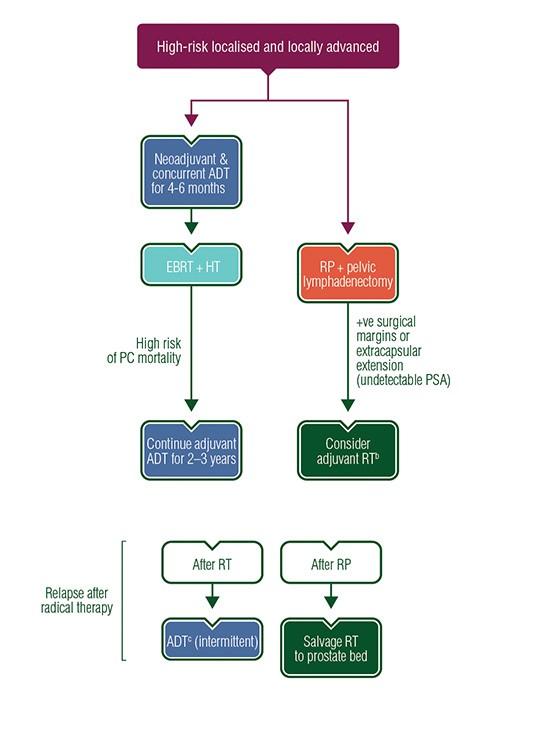
4 HIGH RISK /LOCALLY ADVANCED -NEOADJ ADT + RADICAL R.T + ADJUVANT ADT. - RADICAL PROSTATECTOMY + PELVIC LYMPHADENECTOMY.
5
6
7 INITIAL RESPONSE TO ANDROGEN DEPRIVATION THERAPY IS USUALLY GOOD. DEVELOPMENT OF ANDROGEN RESISTANCE LEADS TO PROGRESSIVE DISEASE MAJOR REASON FOR MORBIDITY AND MORTALITY. METASTATIC DISEASE- ADT, ORCHIECTOMY, CHEMOTHERAPY.
8 CHEMOTHERAPY (DOCETAXEL,ABIRATERONE, ENZALUTAMIDE, CABAZITAXEL), 223 RADIUM CHLORIDE TARGETED RADIONUCLIDE THERAPY
9 Metastatic disease treatment algorithm Published: 22 September Authors:C. Parker1, S. Gillessen2 & A. Horwich3 on behalf of the ESMO Guidelines Committee 1Royal Marsden Hospital, Sutton, UK; 2Department of Oncology/Hematology, Kantonsspital St Gallen, St Gallen, Switzerland; 3The Institute of Cancer Research, London, UK
10 TARGETED RADIONUCLIDE THERAPY METASTATIC CASTRATION RESISTANT PROSTATE CANCER-TARGETS PSMA :TRANSMEMBRANE PROTEIN WITH INCREASED EXPRESSION IN PROSTATE CA. TARGETED DELIVERY OF THERAPEUTIC RADIATION TO ALL METASTATIC SITES, DELIVERS HIGH RADIATION DOSE SPARING NORMAL TISSUES. HIGH ABSORBED TUMOUR DOSES(3.3.mGy/MBq).
11 177 LUTETIUM 177Lu- MEDIUM ENERGY BETA EMITTER, MAX ENERGY 0.5 MeV. MAX TISSUE PENETRATION 2 MM. T1/2 6.7 DAYS. γ-rays: 208 (10%) & 113 kev (6%) ABUNDANCE. SHORTER BETA RANGE-BETTER IRRADIATION OF SMALL
12 PREPARATION Water heater baths switched on for 90 Degrees Transfer 900 micro liter of Buffer Solution to the Eliqort containing 100micor liter of Peptide. Transfer the mixture of Buffer and Peptide to a Syringe. Push this Syringe to the Vial of Lu 177. Pull back the same volume of Air into the syringe Without removing the Syringe from the vial and push air back into the Lu177 Vial. Remove syringe from vial & transfer the vial to the heater bath. Heat the Lu 177 Vial for 25 minutes at 90 Degrees.
13 QUALITY CONTROL of 177Lu-Peptides Chemical purity checked by TLC Put a drop of product on the TLC(silica gel) sheet- sheet placed in a centrifuge tube containing mobile phase(sodium citrate buffer) with activity spot near mobile phase. When mobile phase is close to the end of TLC sheet the sheets are cut into two pieces(in between mobile phase front and drop added) Measure activity- activity at bottom represents labelled product whereas upper part represents impurities as impurities move with mobile phase The purity is ok when A bottom/ (A bottom +A top) 95%
14 PRE THERAPY CHECKLISTS PRETHERAPY IMAGING SHOULD SHOW GOOD LOCALISATION OF GALLIUM PSMA LIGAND IN METASTATIC SITES. DTPA RENOGRAM COMPLETE BLOOD COUNT. BASELINE PSA LEVELS.
15 TECHNIQUE PRE THERAPY HYDRATION, PREMEDICATION, COLD COMPRESS TO PAROTIDS. AMINOVEN 10% IV : 1 BOTTLE PRIOR TO THERAPY, 200 ML/ HR X 3 BOTTLES AFTER THERAPY. IV 177 LUTETIUM PSMA OVER 20 MINUTES.HYDRATION CONTINUED.
16 CASE SCENARIO 1 66 YR OLD,CAD, D.M, DIAGNOSED WITH METASTATIC CA PROSTATE 2003 ( MRI: T4a LESION WITH PARA-AORTIC & LEFT ILIAC NODAL METS). SKELETAL LESIONS IN PELVIS/ FEMUR AND ALL VISUALIZED VERTEBRAE. PSA: 100. B/L ORCHIDECTOMY, switched different hormonal drugs as the PSA trend changed.
17 Bone scan - all vertebrae/ shoulder/ribs/ hip joints, upper 1/3 of both femur R>>L. on Zoledronic acid Q Monthly since SYMPTOMATIC : Pain in right hip joint, severe pain which reduces only with a NSAID (Aceclofenac) PSA is trending upward, Breakthrough disease. GALLIUM PSMA PET CT SKELETAL, HEPATIC, NODAL AND PULMONARY METS.

18 initiated on Inj. Cabazitaxel, Q3WEEKLY with daily Prednisolone. EXTERNAL R.T TO RIGHT HEMIPELVISMINIMAL SYMPTOMATIC RELIEF. RISING PSA LEVELS, INCREASINGLY SYMPTOMATIC. Repeat Gallium PSMA : Increase in number & size of PSMA over expressing lymph nodes,mixed response in skeletal lesions with increase in number of skeletal
19 PRE THERAPY PSA 33.7 ng/ml. DTPA renogram :-No PUJ/VUJ obstruction. Serum Creatinine, CBC -WNL. 1ST SITTING : 7400 MBQ of 177 LU PSMA

20 SERUM PSA INITIAL 33 CAME DOWN TO 2.5 AFTER 1 SITTING. INCREASED TO 37 NG/ML AFTER 2ND SITTING. GA PSMA AFTER 2 SITTINGSMIXED RESPONSE IN SKELETAL, GOOD RESPONSE IN NODAL AND LIVER LESIONS SHOWED PROGRESSION.
21 SYMPTOMATIC RELIEF EXCELLENT WITH RESPECT TO SKELETAL METS-PAIN SCORE 3. NODES RESPONDED WELL. LIVER LESIONS UNRESPONSIVE. RELIEF IN PAIN LASTED FOR 5 MONTHS.SIGNIFICANT IMPROVEMENT IN QOL. AFTER 3RD SITTING DEVELOPED BONE MARROW
22 CASE SCENARIO # 2 MILD RENAL FAILURE 81 yr old gentleman,adenocarcinoma prostate, bilateral orchidectomy in 2006 and was on bicalutamide later on. CHRONIC D.M, POST CABG in TOOK Honvan tablets FOR A WHILE. Abiraterone along with zolendronic acid started in April 2015.

23 Gallium scan :GA PSMA AVID residual prostate CA + multiple supra & Infradiapghramatic lymph nodal, b/l pulmonary, liver and extensive skeletal mets. OLD age,progressive symptomatic disease-- not keen on giving chemotherapy-referred for 177 Lutetium PSMA therapy
 NON RESPONDER TO THERAPY. POST THERAPY: NO DETERIORATION IN RENAL FUNCTION ON FUP FOR 3 MONTHS.")
24 DTPA renogram :PUJ non obstructed LT kidney (FN:79%). Hydronephrotic NON OBSTRUCTED RT kidney(fn:21 %).Total GFR :67 ml/min. S.creat :1.55 mg/dl. S.PSA PRE therapy101.6 ng 170MBQ OF 177 LU PSMA (AMINOVEN GIVEN) NON RESPONDER TO THERAPY. POST THERAPY: NO DETERIORATION IN RENAL FUNCTION ON FUP FOR 3 MONTHS.
25 CASE SCENARIO # 3 73 YR OLD diagnosed with adenocarcinoma prostate in 2014 aug. (S.PSA level of 100 n/ml). Sep 2014, started on Leupride+Tabi: PSA reached nadir at 2ng/ml in Dec,2015. started on Tab abiraterone later on. Serum PSA levels started slowly and serially rising.
26 Gallium PSMA avid primary prostate & multiple avid and non avid skeletal metastases. PSMA non avid hypodense lesion in segment VIII of liver. S.PSA :112 ng/ml MBq of 177 Lu PSMA. requirements for pain killers came down significantly. PAIN SCORE FROM 4 TO 0. s.psa ng/ml

27 2nd sitting : 6290 MBq of 177 Lutetium PSMA after 3 months. POST THERAPY PSA IS 2 NG/ML
28 FOLLOW UP GALLIUM SCAN AFTER 2CYCLES NEAR COMPLETE RESOLUTION OF ALMOST ALL SKELETAL AND NODAL DISEASE-PAIN FREE. NO NEW SKELETAL LESIONS. INCREASE IN SIZE OF NON AVID LIVER LESION SHOWING MILD AVIDITY NOW. AFP 10 BIOPSY : HCC
29 CASE SCENARIO # 4 MARROW METS 73 YR OLD GENTLEMAN. OBSTRUCTIVE LUTS, NO COMORBIDITIES. ELEVATED PSA : 126 ng/dl BONE SCAN EXTENSIVE SKELETAL METS, MARROW INVOLVEMENT.

30 PRE THERAPY BONE SCAN PRE THERAPY GALLIUM SCAN
31 GALLIUM PSMA SCAN: PRIMARY DISEASE + PREDOMINANTLY SKELETAL AND MARROW METS. EXTERNAL R.T TO PELVIC REGION- MILD PAIN RELIEF. LUTETIUM PSMA TAILORED DOWN DOSE : 150 MCI. POST THERAPY : SIGNIFICANT PAIN POST THERAPY,NO POST TREATMENT SCAN.
32 FOLLOW UP MARROW TOXICITY AT 4 WEEKS, REQUIRING MULTIPLE PACKED RBC, PLATELETS TRANSFUSED. NEUTROPAENIC FEVER.GRADUALLY RECOVERING. 8 WEEKS PAIN SCORE: 2. PSA :100- MILD REDUCTION?FIT TO BE TREATED AGAIN
33 LESSONS LEARNT.. MAJOR SIDE EFFECTS NONE SYMPTOMATIC PAIN RELIEF IMPROVED QUALITY OF LIFE ( HAPPY PATIENTS WHO CRAVE FOR MORE LUTETIUM AND NO CHEMO EVER AGAIN PLEASE!!!) SAFE EVEN IN MILD RENAL FAILURE BUT WITH NO OBSTRUCTIVE NEPHROPATHY
34 LESSONS LEARNT.. SKELETAL METASTASES +/ - NODES- RESPONDS WELL. MARROW TOXICITY WELL TOLERATED AT A DOSE OF mci. EXCEPTION- PREDOMINANTLY MARROW METASTASES. MARROW METS: MARROW DEPRESSION AT 4-6 WEEKSREVERSIBLE.
35 LINGERING QUESTIONS EXTENSIVE HEPATIC METASTASES- IS IT WORTH GOING AHEAD?? IF NO RESPONSE AFTER FIRST SITTING, SHOULD WE GO AHEAD WITH NEXT SITTING. THERAPY AT 8 WEEKS INTERVAL OR 12 WEEKS? WHEN DO WE CALL IT A STOP BIOCHEMICAL RESPONSE, SYMPTOMATIC RELIEF OR GALLIUM SCAN
36 LINGERING QUESTIONS. CAN WE STOP ABIRATERONE, ENZALUTAMIDE ETC ONCE PATIENT IS STARTED ON THERAPY. ADDED EFFICACY IF COMBINED WITH DOCETAXEL -? SCIENTIFIC EVIDENCE. IF SO WHAT DOSAGE AND INTERVAL?

37 Searching for answers quest continues.. Thank you!
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
PRO STATE of the art. METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature
 PRO STATE of the art METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature Marcello Tucci, MD Department of Oncology San Luigi Gonzaga Hospital Orbassano, Turin 30 MAY
PRO STATE of the art METASTATIC HORMONE SENSITIVE PROSTATE CANCER Clinical case and evidences from literature Marcello Tucci, MD Department of Oncology San Luigi Gonzaga Hospital Orbassano, Turin 30 MAY
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
GUIDELINEs ON PROSTATE CANCER
 GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
PSMA Targeted radionuclide therapy in Prostate Cancer
 PSMA Targeted radionuclide therapy in Prostate Cancer Tawatchai Chaiwatanarat Division of Nuclear Medicine Department of Radiology Chulalongkorn University Bangkok, Thailand * cell si ze ~20 µm Radionuclide
PSMA Targeted radionuclide therapy in Prostate Cancer Tawatchai Chaiwatanarat Division of Nuclear Medicine Department of Radiology Chulalongkorn University Bangkok, Thailand * cell si ze ~20 µm Radionuclide
Patterns of care for prostate cancer An update
 Patterns of care for prostate cancer An update Daniel Moon Director of Robotic Surgery Epworth Healthcare Honorary Clinical Senior Lecturer University of Melbourne Consultant Urologist Peter MacCallum
Patterns of care for prostate cancer An update Daniel Moon Director of Robotic Surgery Epworth Healthcare Honorary Clinical Senior Lecturer University of Melbourne Consultant Urologist Peter MacCallum
Diagnosis and management of prostate cancer in the
 Diagnosis and management of prostate cancer in the Jeremy Teoh ( 張源津 ) Assistant Professor, Department of Surgery, The Chinese University of Hong Kong. Email: jeremyteoh@surgery.cuhk.edu.hk Estimated age-standardised
Diagnosis and management of prostate cancer in the Jeremy Teoh ( 張源津 ) Assistant Professor, Department of Surgery, The Chinese University of Hong Kong. Email: jeremyteoh@surgery.cuhk.edu.hk Estimated age-standardised
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Community care of Prostate Cancer. Shaun Costello Southern Cancer Network
 Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
Outline. Prostate Cancer. mcrpc Bone Metastases 3/25/2017. Treatment of Prostate Cancer with Radionuclide Based Therapies.
 Treatment of Prostate Cancer with Radionuclide Based Therapies. Homer A. Macapinlac, M.D. Outline Background Prostate Cancer Treatment. Palliation with beta emitters. Improving survival with alpha emitters.
Treatment of Prostate Cancer with Radionuclide Based Therapies. Homer A. Macapinlac, M.D. Outline Background Prostate Cancer Treatment. Palliation with beta emitters. Improving survival with alpha emitters.
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE
 PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE DISCLOSURES/CONFLICTS NONE OBJECTIVES Understand current diagnostic role
PSMA PET SCANNING AND THERANOSTICS IN PROSTATE CANCER KEVIN TRACEY, MD, FRCPC PRECISION DIAGNSOTIC IMAGING REGIONAL PET/CT CENTRE DISCLOSURES/CONFLICTS NONE OBJECTIVES Understand current diagnostic role
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Please consider the following information on ZYTIGA (abiraterone acetate). ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017
. ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017") Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Lutetium-177 PSMA (LuPSMA) Theranostic Phase II trial: Efficacy, safety and QoL in patients
 Theranostic Phase II trial: Efficacy, safety and QoL in patients") Lutetium-177 PSMA (LuPSMA) Theranostic Phase II trial: Efficacy, safety and QoL in patients with castrate-resistant prostate cancer treated with LuPSMA M. S. Hofman, S. Sandhu, P. Eu, P. Jackson, T. Akhurst,
Lutetium-177 PSMA (LuPSMA) Theranostic Phase II trial: Efficacy, safety and QoL in patients with castrate-resistant prostate cancer treated with LuPSMA M. S. Hofman, S. Sandhu, P. Eu, P. Jackson, T. Akhurst,
MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER
 MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER NO RELEVANT FINANCIAL RELATIONSHIPS IN THE PAST TWELVE MONTHS BY PRESENTER OR SPOUSE/PARTNER.
MAMTA PARIKH, MD, MS CHALLENGING CASE #2: GU CANCER & STATE OF THE ART: CASTRATION RESISTANT PROSTATE CANCER NO RELEVANT FINANCIAL RELATIONSHIPS IN THE PAST TWELVE MONTHS BY PRESENTER OR SPOUSE/PARTNER.
STAMPEDE trial (MRC PR08): Arm J overview. Enzalutamide and abiraterone comparison and trial update
: Arm J overview. Enzalutamide and abiraterone comparison and trial update") STAMPEDE trial (MRC PR08): Arm J overview Enzalutamide and abiraterone comparison and trial update Arm J Hypotheses and rationale STAMPEDE: Hypothesis Will addition of enzalutamide and abiraterone to standard-of-care
STAMPEDE trial (MRC PR08): Arm J overview Enzalutamide and abiraterone comparison and trial update Arm J Hypotheses and rationale STAMPEDE: Hypothesis Will addition of enzalutamide and abiraterone to standard-of-care
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Testicular Cancer. Regional Follow-up Guidelines
 Urological Cancers Managed Clinical Network Testicular Cancer Regional Follow-up Guidelines Prepared by Drs J White/ A Waterston, J Salmond, J Wallace, Mr D Hendry, Approved by Urological Cancers MCN and
Urological Cancers Managed Clinical Network Testicular Cancer Regional Follow-up Guidelines Prepared by Drs J White/ A Waterston, J Salmond, J Wallace, Mr D Hendry, Approved by Urological Cancers MCN and
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Alpha-emitting Radionuclides: Ra-223
 Alpha-emitting Radionuclides: Ra-223 prof. dr. K. Goffin Nuclear Medicine and Molecular Imaging Department of Imaging & Pathology UZ Leuven KU Leuven Belgium International Course on Theranostics and Molecular
Alpha-emitting Radionuclides: Ra-223 prof. dr. K. Goffin Nuclear Medicine and Molecular Imaging Department of Imaging & Pathology UZ Leuven KU Leuven Belgium International Course on Theranostics and Molecular
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Prostatectomy as salvage therapy. Cases. Paul Cathcart - Guy s & St Thomas NHS Trust, London
 Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Bone targeted radionuclide therapy. Val Lewington Royal Marsden Hospital, London
 Bone targeted radionuclide therapy Val Lewington Royal Marsden Hospital, London Bone malignancy Primary bone tumours Bone malignancy Primary bone tumours - chemotherapy, surgery & external beam radiotherapy
Bone targeted radionuclide therapy Val Lewington Royal Marsden Hospital, London Bone malignancy Primary bone tumours Bone malignancy Primary bone tumours - chemotherapy, surgery & external beam radiotherapy
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Oligometastasis. Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie?
 Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Prostate Cancer. NCCN Guidelines Version Prostate Cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines )
") NCCN Guidelines Version 1.2016 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 3.2016 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients Continue Version
NCCN Guidelines Version 1.2016 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 3.2016 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients Continue Version
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
STAMPEDE: CRF Completion Guidelines
 : CRF Completion Guidelines V2.0 Randomisation Eligibility checklist Administrative checklist to ensure all screening procedures have been completed Not required to be sent to MRC CTU Randomisation Complete
: CRF Completion Guidelines V2.0 Randomisation Eligibility checklist Administrative checklist to ensure all screening procedures have been completed Not required to be sent to MRC CTU Randomisation Complete
Case histories in Urological cancers
 Case histories in Urological cancers Dr Alison Tree Consultant Clinical oncologist, The Royal Marsden and Institute of Cancer Research 2 The Royal Marsden Outline of talk Case histories for: Localised
Case histories in Urological cancers Dr Alison Tree Consultant Clinical oncologist, The Royal Marsden and Institute of Cancer Research 2 The Royal Marsden Outline of talk Case histories for: Localised
2015 myresearch Science Internship Program: Applied Medicine. Civic Education Office of Government and Community Relations
 2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου
 Η θέση του PET/CT στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου 2014 : the Guidelines year. PRINCIPLES OF IMAGING Imaging is performed for the detection
Η θέση του PET/CT στη σταδιοποίηση του καρκίνου του προστάτη Γ. Αρσος, Γ Εργ. Πυρηνικής Ιατρικής ΑΠΘ, ΓΝΘ Παπαγεωργίου 2014 : the Guidelines year. PRINCIPLES OF IMAGING Imaging is performed for the detection
Prostate Cancer. NCCN Guidelines Version Prostate Cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines )
") NCCN Guidelines Version 1.2016 Prostate NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 2.2017 February 21, 2017 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients
NCCN Guidelines Version 1.2016 Prostate NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 2.2017 February 21, 2017 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Elderly men with prostate cancer + ADT
 Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
INDICATIONS AND USAGE
 1. INDICATIONS AND USAGE a) Axumin is indicated for positron emission tomography (PET) in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following
1. INDICATIONS AND USAGE a) Axumin is indicated for positron emission tomography (PET) in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps?
 Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Prostate Cancer. NCCN Guidelines Version Prostate Cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines )
") NCCN Guidelines Version 1.2016 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 2.2016 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients Continue Version
NCCN Guidelines Version 1.2016 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Version 2.2016 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients Continue Version
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer
 Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer Gleason score Gleason score 2-4: well differentiated (seldom reported now): Low risk
Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer Gleason score Gleason score 2-4: well differentiated (seldom reported now): Low risk
Radioligand imaging & treatment of prostate cancer
 Radioligand imaging & treatment of prostate cancer Christiaan Schiepers, MD, PhD University of California Los Angeles CANM-CAMRT JOINT ANNUAL CONFERENCE MARCH 22-24, 2018 VANCOUVER, B.C. I do not have
Radioligand imaging & treatment of prostate cancer Christiaan Schiepers, MD, PhD University of California Los Angeles CANM-CAMRT JOINT ANNUAL CONFERENCE MARCH 22-24, 2018 VANCOUVER, B.C. I do not have
Prostate Cancer and PSMA:
 Prostate Cancer and PSMA: The Clinical Perspective from Liverpool. Dr. Christopher Mayes. Professor Sobhan Vinjamuri. Department of Nuclear Medicine Royal Liverpool University Hospital (BSUR 2016 Plymouth)
Prostate Cancer and PSMA: The Clinical Perspective from Liverpool. Dr. Christopher Mayes. Professor Sobhan Vinjamuri. Department of Nuclear Medicine Royal Liverpool University Hospital (BSUR 2016 Plymouth)
HOW I DO IT. Introduction. BARKIN J. How I Do It: Managing bone health in patients with prostate cancer. Can J Urol 2014;21(4):
:") HOW I DO IT How I Do It: Managing bone health in patients with prostate cancer Jack Barkin, MD Department of Surgery, University of Toronto, Humber River Hospital, Toronto, Ontario, Canada BARKIN J. How
HOW I DO IT How I Do It: Managing bone health in patients with prostate cancer Jack Barkin, MD Department of Surgery, University of Toronto, Humber River Hospital, Toronto, Ontario, Canada BARKIN J. How
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER
 PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PRECISION IMAGING: QUANTITATIVE, MOLECULAR AND IMAGE-GUIDED TECHNOLOGIES
 PRECISION IMAGING: QUANTITATIVE, MOLECULAR AND IMAGE-GUIDED TECHNOLOGIES Day 3 Authors: Tade, Funmilayo; Akin-Akintayo Oladunni; Schuster, David M. Lab Training Module 1: Introduction to the basics of
PRECISION IMAGING: QUANTITATIVE, MOLECULAR AND IMAGE-GUIDED TECHNOLOGIES Day 3 Authors: Tade, Funmilayo; Akin-Akintayo Oladunni; Schuster, David M. Lab Training Module 1: Introduction to the basics of
STAMPEDE: CRF Completion Guidelines
 : CRF Completion Guidelines V3.0 Randomisation Eligibility checklist Administrative checklist to ensure all screening procedures have been completed Not required to be sent to MRC CTU Randomisation Complete
: CRF Completion Guidelines V3.0 Randomisation Eligibility checklist Administrative checklist to ensure all screening procedures have been completed Not required to be sent to MRC CTU Randomisation Complete
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
RADIONUCLIDE THERAPY FOR PALLIATION OF PAIN FROM BONY METASTASES
 RADIONUCLIDE THERAPY FOR PALLIATION OF PAIN FROM BONY METASTASES Overview and Topics to Be Covered Reviews the use of radionuclide therapy in nuclear medicine for palliation of pain due to bony metastases.
RADIONUCLIDE THERAPY FOR PALLIATION OF PAIN FROM BONY METASTASES Overview and Topics to Be Covered Reviews the use of radionuclide therapy in nuclear medicine for palliation of pain due to bony metastases.
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Case 1: HER2 positive MBC. Sudeep Gupta Tata Memorial Centre
 Case 1: HER2 positive MBC Sudeep Gupta Tata Memorial Centre 54/F, postmenopausal First came to TMC on 3/8/15 Diagnosed in Jan 2015 Right breast mass Bones (L5 & S1), lung, spleen (upfront MBC) IDC grade
Case 1: HER2 positive MBC Sudeep Gupta Tata Memorial Centre 54/F, postmenopausal First came to TMC on 3/8/15 Diagnosed in Jan 2015 Right breast mass Bones (L5 & S1), lung, spleen (upfront MBC) IDC grade
Guideline Prostate cancer: diagnosis and management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Prostate cancer: diagnosis and management (update) Draft for consultation, December 0 This guideline covers diagnosing and managing prostate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline Prostate cancer: diagnosis and management (update) Draft for consultation, December 0 This guideline covers diagnosing and managing prostate