Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
|
|
|
- Lawrence Cummings
- 6 years ago
- Views:
Transcription
1
2 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation.
3 Learning Objectives 1. Identify which patients meet criteria for annual lung cancer screening 2. Identify the four main assessment categories in Lung-RADS reporting
4 Outline Scope of the problem Importance of early detection Low Dose chest CT screening Reporting of screening CT results What do I do with the results?
5 Scope of the problem
6 Lung Cancer Mortality Lung cancer is the leading cause of cancer death in the United States in both men and women Over 200,000 Americans are diagnosed with lung cancer each year An estimated 158,000 Americans were expected to die from lung cancer in 2016, representing 27% of all cancer deaths The number of deaths from lung cancer peaked in 2005 and has since decreased by 2.3% in 2014
7
8
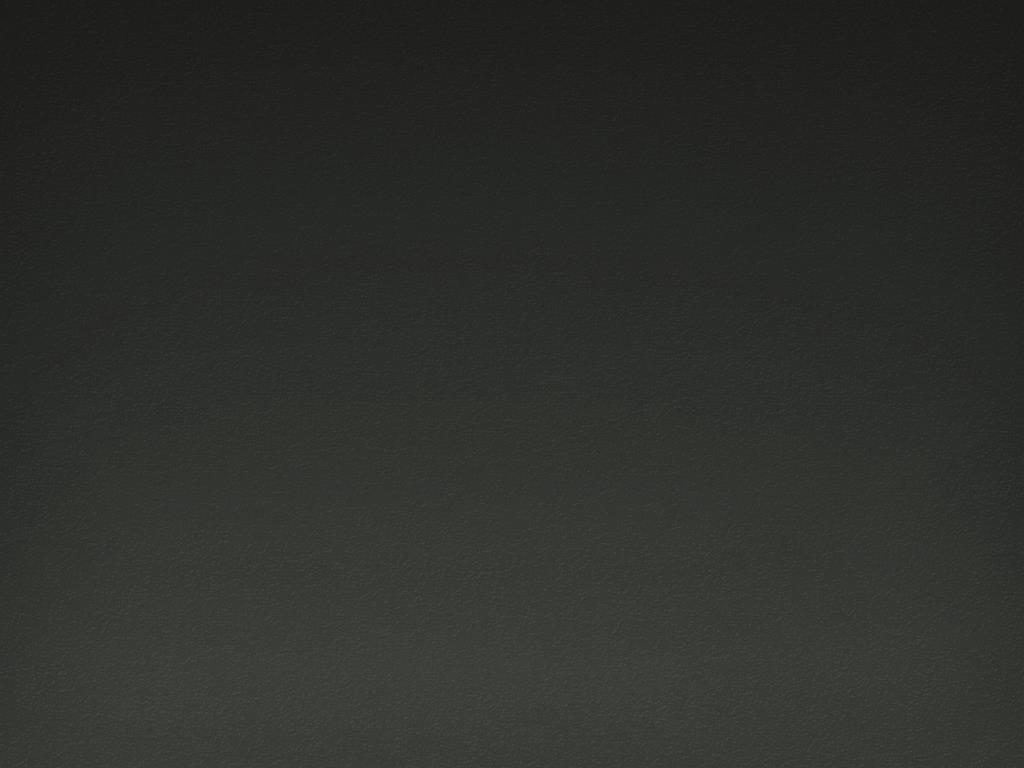
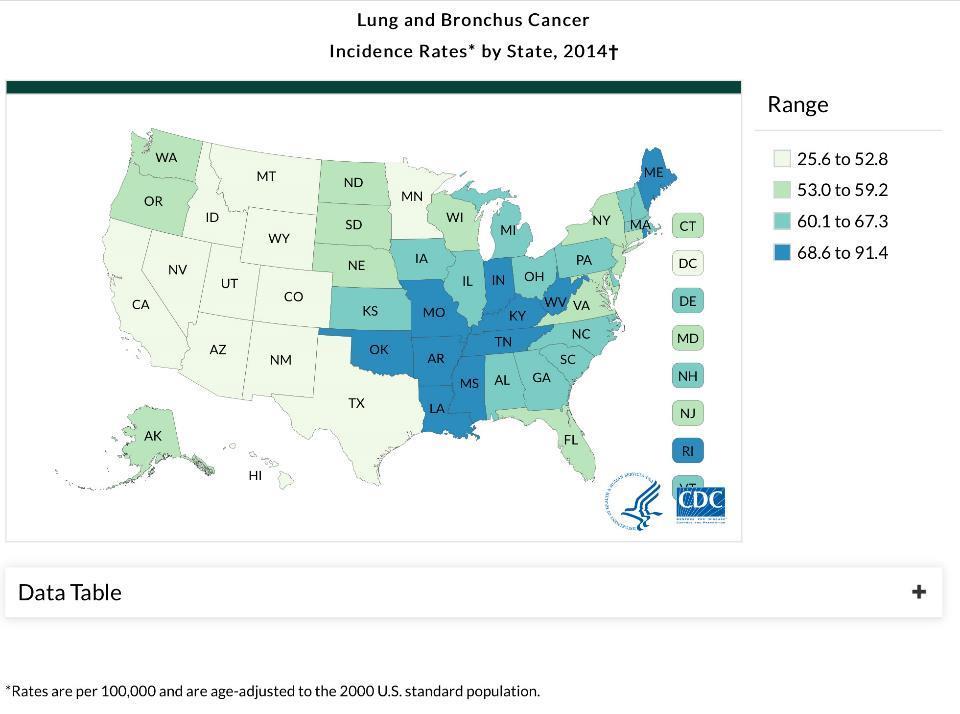
9 Incidence by State Leading Incidence Rates (per 100,000 people) by State, Kentucky West Virginia Arkansas Mississippi Tennessee Maine 72.1
10 Incidence by State Leading Incidence Rates (per 100,000 people) by State, Kentucky West Virginia Arkansas Mississippi Tennessee Maine 72.1
11
12
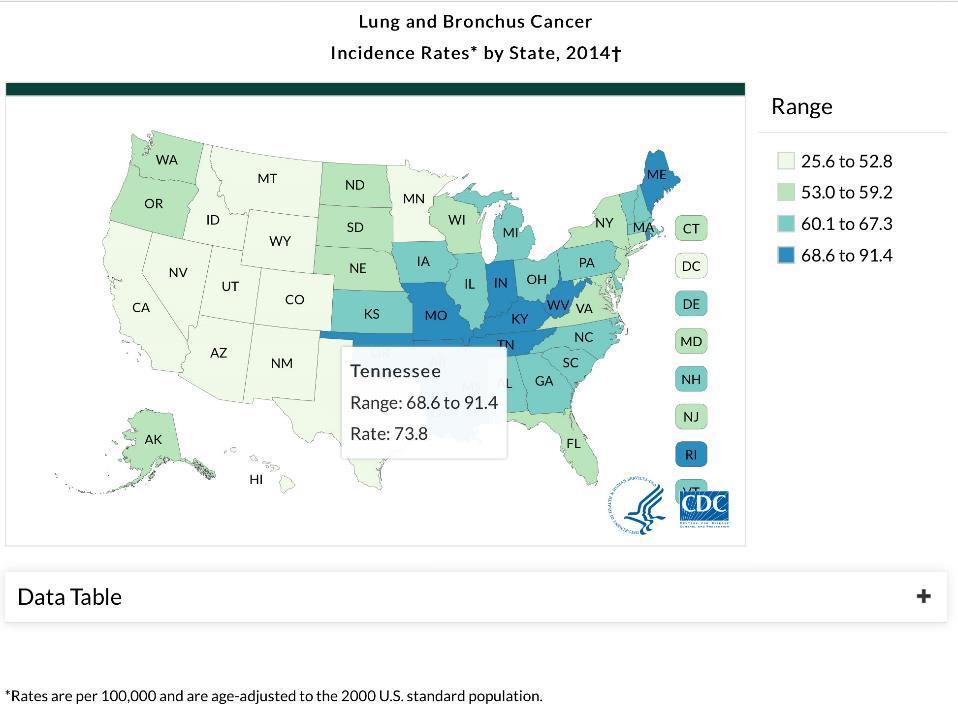
13 Death rate by State Leading Death Rates (per 100,000 people) by State, Kentucky West Virginia t. Tennessee t. Mississippi Arkansas Missouri 53.7

14 Importance of early detection 5 year survival rate of less than 20% in advanced stage lung cancer Screening high risk individuals may dramatically improve survival rates by finding the disease at an earlier, more treatable stage.

15 National Lung Screening Trial, 2011 Low dose chest CT vs CXR >50,000 participants 20% relative mortality decrease Fintelmann et al. The 10 Pillars of Lung Cancer screening. Radiographics volume 35 number 7 pg 1895
16
17

18
19

20
21
22 The fine print on ordering the exam..
 screening for lung cancer in people at high risk for the disease.")
23 Patient and Physician Guide: National Lung Screening Trial (NLST) What is the purpose of this guide? To explain the benefits and harms of low-dose computed tomography (CT) screening for lung cancer in people at high risk for the disease. The NLST showed a reduction in deaths from CT screening compared to chest X-ray screening. The Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial recently showed that chest X-ray screening (compared to no screening) did NOT reduce the chance of dying from lung cancer. Who participated in the NLST? Current or former cigarette smokers within the past 15 years, 55 to 74 years of age, with at least 30 pack-years of smoking [Pack-years = packs per day x number of years smoking]. Participants must have had no symptoms or signs of lung cancer or other serious medical conditions, and be medically fit for surgery. Study Findings: Low-dose CT versus Chest X-ray screening 53,454 current and former smokers were randomly assigned to be screened once a year for 3 years with low-dose CT or chest X-ray. Here s what happened after an average of 6.5 years: Benefit: How did CT scans help compared to chest X-ray, an ineffective screening test? Low-dose CT 26,722 people Chest X-ray 26,732 people 3 in 1,000 fewer died from lung cancer 18 in 1,000 versus 21 in 1,000 5 in 1,000 fewer died from all causes 70 in 1,000 versus 75 in 1,000 Harm: What problems did CT scans cause compared to chest X-ray? 223 in 1,000 more had at least one false alarm 365 in 1,000 versus 142 in 1, in 1,000 more had a false alarm leading to an invasive procedure, such as bronchoscopy, biopsy, or surgery 25 in 1,000 versus 7 in 1,000 2 in 1,000 more had a major complication from Invasive procedures 3 in 1,000 versus 1 in 1,000 Take home messages Lung cancer screening with CT scans is the only screening test shown to lower the chance of dying from lung cancer. The effect of screening may vary depending on how similar you are to the people who participated in the study. The benefit of screening may be bigger if your lung cancer risk is higher. The harm may be bigger if you have more medical problems (like heart or severe lung disease), which could increase problems from biopsies and surgery. For perspective, the reduction in deaths from lung cancer with CT screening is larger than the reduction in deaths from the target cancers of other common screening tests, such as mammograms for breast cancer. There is a tradeoff: CT screening decreases your chance of death but increases your chance of having a false alarm. If you choose to have CT screening, it is important to have it done at a medical center with special expertise in lung cancer screening and treatment. Most important thing you can do DON T SMOKE. Regardless of your screening decision, avoiding cigarettes is the most powerful way to lower your chance of dying overall or suffering or dying from a variety of diseases, such as lung cancer, emphysema, heart or vascular disease. For example, at age sixty-five, 89 in 1,000 male current smokers will die of lung cancer in the next 10 years versus 4 in 1,000 never smokers. For women, the corresponding figures are 55 in 1,000 versus 5 in 1,000. For help quitting, call QUIT-NOW. Cancer.gov Thoracic.org
24 The fine print on ordering the exam.. Find out if the patient has any prior chest CTs
25 Screening & Early Detection Screening high risk individuals with low dose chest CT could reduce lung cancer mortality by 20% compared to chest x-ray. At least 8.6 million Americans qualify as high risk for lung cancer and are recommended to receive annual screening with low dose CT.
26 Low dose chest CT screening
27 Image Acquisition 16 detector row (or more) CT scanner No IV contrast Full chest in field of view 2.5 mm or less section thickness ALARA (as low as reasonably achievable dose less than 3 mgy (absorbed dose, equals 1.5 msv effective dose)

28 Radiation exposure comparison Low dose chest CT equals 6 months of natural background radiation 1 spine x-ray ½ of a calcium score CT RadiologyInfo.org
29 Image Review Interpreting-Physician Criterion Board Certification Training Experience Continuing Education



30 Image Review Goal is two part: 1. Detect signs of early lung cancer such as pulmonary nodules 2. Not to miss potentially important incidental findings (COPD, adenopathy, atherosclerosis, aneurysm, cholelithiasis, & indeterminate thyroid, breast, liver, kidney, adrenal lesions)
31 Image Review Nodule characterization Size matters Size = average of longest and shortest diameter Measured on lung windows in axial plane Density Calcified, solid, part solid, ground glass Margins Circumscribed, irregular, spiculated Change over time Must compare to any available prior (CT neck, chest, abdomen, PET, calcium score CT )
32 Reporting of screening CT results
33 Lung Cancer Screening (LCS) CT report CT scan report should contain: Technique Comparison date Findings description Impression Lung Imaging Reporting and Data System (Lung- RADS) category & specific management recommendations

34 LCS CT report Findings section to contain a description of each nodule including: Location Size Attenuation Morphology Margins Interval change


35 Lung-RADS Structured reporting Quality assurance Reduce confusion Monitor outcomes Version 1.0 released April 2014
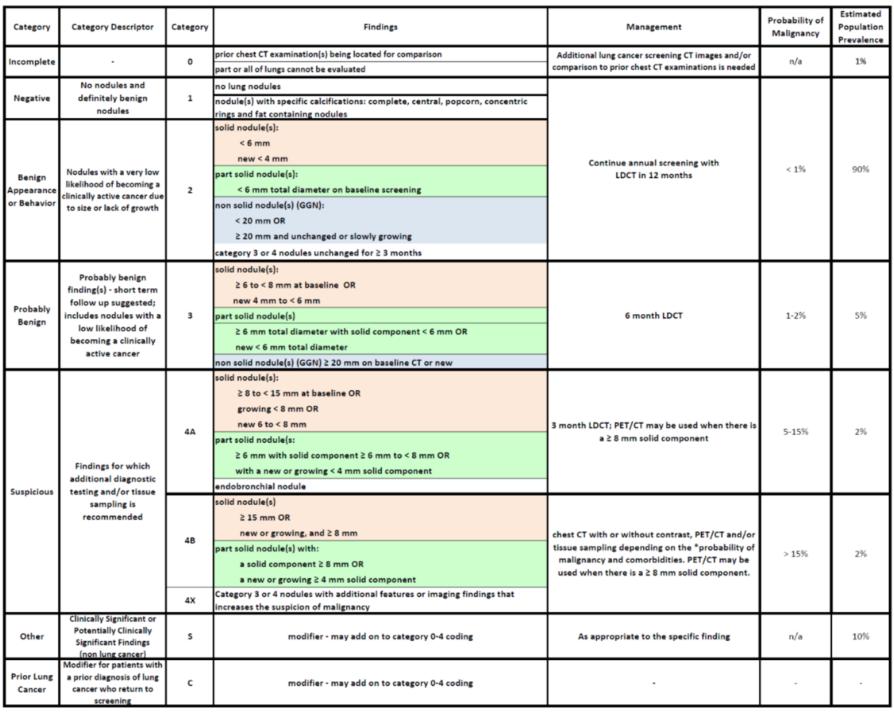
36 Lung RADS Version 1.0 Assessment Categories Release date: April 28, 2014 Category Category Descriptor Category Findings Management prior chest CT examination(s) being located for comparison Additional lung cancer screening CT images and/or Incomplete 0 n/a part or all of lungs cannot be evaluated comparison to prior chest CT examinations is needed Negative Suspicious Other Prior Lung Cancer No nodules and definitely benign nodules Nodules with a very low Benign likelihood of becoming a Appearance clinically active cancer due or Behavior to size or lack of growth Probably benign finding(s) short term follow up suggested; Probably includes nodules with a Benign low likelihood of becoming a clinically active cancer Findings for which additional diagnostic testing and/or tissue sampling is recommended Clinically Significant or Potentially Clinically Significant Findings (non lung cancer) Modifier for patients with a prior diagnosis of lung cancer who return to screening no lung nodules nodule(s) with specific calcifications: complete, central, popcorn, concentric rings and fat containing nodules solid nodule(s): < 6 mm new < 4 mm part solid nodule(s): < 6 mm total diameter on baseline screening non solid nodule(s) (GGN): < 20 mm OR 20 mm and unchanged or slowly growing category 3 or 4 nodules unchanged for 3 months solid nodule(s): 6 to < 8 mm at baseline OR new 4 mm to < 6 mm part solid nodule(s) 6 mm total diameter with solid component < 6 mm OR new < 6 mm total diameter non solid nodule(s) (GGN) 20 mm on baseline CT or new solid nodule(s): 8 to < 15 mm at baseline OR growing < 8 mm OR new 6 to < 8 mm 3 month LDCT; PET/CT may be used when there is 4A 5 15% part solid nodule(s: a 8 mm solid component 4B 4X 6 mm with solid component 6 mm to < 8 mm OR with a new or growing < 4 mm solid component endobronchial nodule solid nodule(s) 15 mm OR new or growing, and 8 mm part solid nodule(s) with: a solid component 8 mm OR a new or growing 4 mm solid component Category 3 or 4 nodules with additional features or imaging findings that increases the suspicion of malignancy Continue annual screening with LDCT in 12 months 6 month LDCT chest CT with or without contrast, PET/CT and/or tissue sampling depending on the *probability of malignancy and comorbidities. PET/CT may be used when there is a 8 mm solid component. Estimated Probability of Population Malignancy Prevalence S modifier may add on to category 0 4 coding As appropriate to the specific finding n/a 10% C modifier may add on to category 0 4 coding < 1% 1% 90% 1 2% 5% 2% > 15% 2% IMPORTANT NOTES FOR USE: 1) Negative screen: does not mean that an individual does not have lung cancer 2) Size: nodules should be measured on lung windows and reported as the average diameter rounded to the nearest whole number; for round nodules only a single diameter measurement is necessary 3) Size Thresholds: apply to nodules at first detection, and that grow and reach a higher size category 4) Growth: an increase in size of > 1.5 mm 5) Exam Category: each exam should be coded 0 4 based on the nodule(s) with the highest degree of suspicion 6) Exam Modifiers: S and C modifiers may be added to the 0 4 category 7) Lung Cancer Diagnosis: Once a patient is diagnosed with lung cancer, further management (including additional imaging such as PET/CT) may be performed for purposes of lung cancer staging; this is no longer screening 8) Practice audit definitions: a negative screen is defined as categories 1 and 2; a positive screen is defined as categories 3 and 4 9) Category 4B Management: this is predicated on the probability of malignancy based on patient evaluation, patient preference and risk of malignancy; radiologists are encouraged to use the McWilliams et al assessment tool when making recommendations 10) Category 4X: nodules with additional imaging findings that increase the suspicion of lung cancer, such as spiculation, GGN that doubles in size in 1 year, enlarged lymph nodes etc 11) Nodules with features of an intrapulmonary lymph node should be managed by mean diameter and the 0 4 numerical category classification 12) Category 3 and 4A nodules that are unchanged on interval CT should be coded as category 2, and individuals returned to screening in 12 months 13) LDCT: low dose chest CT *Link to McWilliams Lung Cancer Risk Calculator Upon request from the authors at: cancer risk calculator At UptoDate solitary pulmonary nodule malignancy risk brock university cancer prediction equation
37
38 Lung-RADS Category 0 Assessment: Incomplete Findings: Prior chest CT exam(s) being located for comparison Part or all of lungs cannot be evaluated Management: Additional lung cancer screening CT images and/or comparison to prior chest CT exam is needed Estimated population prevalence: 1%
: 90% CHI Memorial prevalence: 89% (Cat 1: 72%, Cat 2: 17%)")
39 Lung-RADS Category 1 Assessment: Negative Findings: No lung nodules Nodule(s) with specific calcifications: complete, central, popcorn, concentric rings and fat containing nodules Management: Continue annual screening with low dose chest CT in 12 months Probability of malignancy: < 1% Estimated prevalence (with category 2): 90% CHI Memorial prevalence: 89% (Cat 1: 72%, Cat 2: 17%)
: 90% CHI Memorial prevalence: 89% (Cat 1: 72%, Cat 2:")
40 Lung-RADS Category 2 Assessment: Benign Appearance or Behavior Nodules with a very low likelihood of becoming a clinically active cancer due to size or lack of growth Management: Annual screening in 12 months Findings: Probability of malignancy: <1 % Estimated population prevalence (with category 1): 90% CHI Memorial prevalence: 89% (Cat 1: 72%, Cat 2: 17%)

41 Lung-RADS Category 2

42 Lung-RADS Category 2

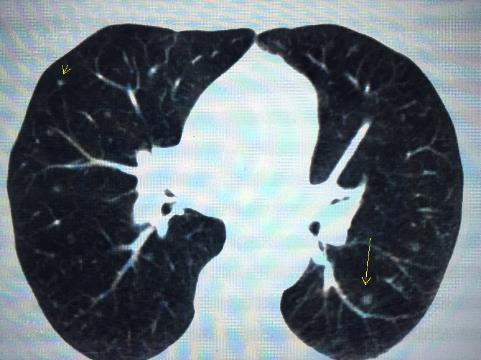
43 Lung-RADS Category 3 Assessment: Probably Benign Findings: Nodules with a low likelihood of becoming a clinically active cancer Management: 6 month follow-up low dose chest CT Probability of malignancy: 1 2% Estimated population prevalence: 5% CHI Memorial prevalence: 6%

44 Lung-RADS Category 3 7 mm irregular nodule Lung-RADS 3 Awaiting 6 month follow up CT

45 Lung-RADS Category 4A Assessment: Suspicious Findings for which additional diagnostic testing and/or tissue sampling is recommended Management: 3 month follow-up LDCT; PET- CT may be used when there is a >= 8 mm solid component Findings: Probability of malignancy: 5 15% CHI Memorial malignancy rate for 4A and 4B combined = 26% Estimated population prevalence: 2% CHI Memorial prevalence 4A & 4B: 5%

46 RLL circumscribed 8 mm Nodule = Lung-RADS 4A At 3 month follow up -> Stable; now category 2 1 cm RLL irregular nodule Lung-RADS 4A Awaiting follow-up; 3 month follow up CT or PET-CT

47 Lung-RADS Category 4B Assessment: Suspicious Findings for which additional diagnostic testing and/or tissue sampling is recommended Management: PET-CT and/or tissue sampling depending on the probability of malignancy & comorbidities. Findings: Probability of malignancy: > 15% CHI Memorial malignancy rate for 4A and 4B combined = 26% Estimated population prevalence: 2% CHI Memorial prevalence 4A & 4B: 5%



48 June 2016 wellness CXR January 2017 screening CT 2.4 x 1.6 cm irregular nodule Lung-RADS category 4B


49 PET-CT showed Stage IA cancer; No evidence of nodal spread of disease or distant metastases CT guided biopsy performed = Poorly differentiated squamous cell carcinoma
50 Lung-RADS Modifiers Category 4X: Category 3 or 4 nodules with additional features or imaging findings that increase the suspicion of malignancy S modifier Added to category 0-4 Clinically significant or potentially clinically significant findings (non lung cancer) C modifier Added to category 0-4 Added to the category for patients with a prior diagnosis of lung cancer who return to screening
51 What do I do with the results?

52 CHI Memorial Experience Cancer detection rate: 1.4% % of cancers that are Stage I: 61.5%
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art
 SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
SCBT-MR 2016 Lung Cancer Screening in Practice: State of the Art Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality
SCBT-MR 2015 LungRADS : Basics
 SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
SCBT-MR 2015 LungRADS : Basics Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report National Lung Cancer Screening Trial 20% lung cancer mortality reduction 6.9% all cause mortality
Approach to Pulmonary Nodules
 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Current Approach to Screening for Lung Cancer. James R Jett M.D.
 Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
Current Approach to Screening for Lung Cancer James R Jett M.D. Potential Conflicts of Interest I am Chief Medical Officer for Oncimmune Ltd (Biomarkers of Cancer) Co-Editor of Lung Cancer Section of UP-TO-DATE
Screening Programs background and clinical implementation. Denise R. Aberle, MD Professor of Radiology and Engineering
 Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Screening Programs background and clinical implementation Denise R. Aberle, MD Professor of Radiology and Engineering disclosures I have no disclosures. I have no conflicts of interest relevant to this
Lung Cancer Screening
 Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
The Maine Lung Cancer Coalition. Working Together to Reduce Lung Cancer in Maine
 The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
The Maine Lung Cancer Coalition Working Together to Reduce Lung Cancer in Maine funding Maine Lung Cancer Coalition (MLCC) Webinar Lung Cancer Screening: Following Up On Abnormal Low Dose CT Scans with
Lung Cancer Screening
 Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
Scan for mobile link. Lung Cancer Screening What is lung cancer screening? Screening examinations are tests performed to find disease before symptoms begin. The goal of screening is to detect disease at
GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES
 Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
Venice 2017 GUIDELINES FOR PULMONARY NODULE MANAGEMENT : RECENT CHANGES AND UPDATES Heber MacMahon MB, BCh Department of Radiology The University of Chicago Disclosures Consultant for Riverain Medical
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES. https://tinyurl.com/hmpn2018
 PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
PULMONARY NODULES AND MASSES : DIAGNOSTIC APPROACH AND NEW MANAGEMENT GUIDELINES Heber MacMahon MB, BCh Department of Radiology The University of Chicago https://tinyurl.com/hmpn2018 Disclosures Consultant
CT Screening for Lung Cancer for High Risk Patients
 CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
CT Screening for Lung Cancer for High Risk Patients The recently published National Lung Cancer Screening Trial (NLST) showed that low-dose CT screening for lung cancer reduces mortality in high-risk patients
SHARED DECISION MAKING AND LUNG CANCER SCREENING
 SHARED DECISION MAKING AND LUNG CANCER SCREENING DISCLOSURES Cathleen E. Morrow, MD None William C. Black, MD No financial disclosure Co-investigator for NLST Member of the ACR Lung-RADS Screening Registry
SHARED DECISION MAKING AND LUNG CANCER SCREENING DISCLOSURES Cathleen E. Morrow, MD None William C. Black, MD No financial disclosure Co-investigator for NLST Member of the ACR Lung-RADS Screening Registry
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE?
 PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
PULMONARY NODULES DETECTED INCIDENTALLY OR BY SCREENING: LOTS OF GUIDELINES BUT WHERE IS THE EVIDENCE? MICHAEL K. GOULD, MD SENIOR RESEARCH SCIENTIST DIRECTOR FOR HEALTH SCIENCES & IMPLEMENTATION SCIENCE
SCBT-MR 2015 Incidentaloma on Chest CT
 SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
Disclosures. Overview. Selection the most accurate statement: Updates in Lung Cancer Screening 5/26/17. No Financial Disclosures
 Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
Pulmonary Nodules. Michael Morris, MD
 Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Pulmonary Nodules Michael Morris, MD Case 45 year old healthy male Smokes socially Normal physical exam Pre-employment screening remote +PPD screening CXR nodular opacity Case 45 year old healthy male
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Lung Cancer Screening: To Screen or Not to Screen?
 Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
Lung Cancer Screening: To Screen or Not to Screen? Lorriana Leard, MD Co-Director of UCSF Lung Cancer Screening Program Vice Chief of Clinical Activities UCSF Pulmonary, Critical Care, Allergy & Sleep
CLINICAL GUIDELINES. Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P.
 CLINICAL GUIDELINES Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P. 3/14/2015 Introduction: The purpose of a lung-cancer screening program is to detect
CLINICAL GUIDELINES Lung-Cancer Screening Program Guidelines Robert Y. Kanterman, M.D. and Thomas J. Gilbert, M.D., M.P.P. 3/14/2015 Introduction: The purpose of a lung-cancer screening program is to detect
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI
 Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Rodney C Richie MD FACP FCCP DBIM Texas Life and EMSI Pulmonary Nodules Well-circumscribed, radiographic opacities measuring 3 cm in diameter Surrounded by aerated lung Not associated with atelectesis
Lung Cancer Screening: To screen or not to screen?
 Lung Cancer Screening: To screen or not to screen? Dan J. Raz, M.D. Co Director, Lung Cancer Screening Program Co Director, LungCancer and Thoracic OncologyProgram Assistant Professor, Thoracic Surgery
Lung Cancer Screening: To screen or not to screen? Dan J. Raz, M.D. Co Director, Lung Cancer Screening Program Co Director, LungCancer and Thoracic OncologyProgram Assistant Professor, Thoracic Surgery
LUNG CANCER SCREENING: LUNG CANCER SCREENING: THE TIME HAS COME LUNG CANCER: A NATIONAL EPIDEMIC
 : THE TIME HAS COME Physician Leader, Lung Cancer Multi-Disciplinary Program Fletcher Allen Health Care Annual Meeting Montpelier, VT - April 25, 2014 Gerald S. Davis, MD Professor of Medicine University
: THE TIME HAS COME Physician Leader, Lung Cancer Multi-Disciplinary Program Fletcher Allen Health Care Annual Meeting Montpelier, VT - April 25, 2014 Gerald S. Davis, MD Professor of Medicine University
Screening for Lung Cancer: New Guidelines, Old Problems
 Screening for Lung Cancer: New Guidelines, Old Problems Robert Schilz DO, PhD Associate Professor of Medicine Interim Chief of the Division of Pulmonary, Critical Care and Sleep Medicine University Hospitals
Screening for Lung Cancer: New Guidelines, Old Problems Robert Schilz DO, PhD Associate Professor of Medicine Interim Chief of the Division of Pulmonary, Critical Care and Sleep Medicine University Hospitals
Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D.
 Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D. Lung Cancer 219,440 new cases/year in U.S. (2009) 169,390 deaths/year in U.S. mortality greater than from breast, colon, prostate CA combined
Role of CT in Lung Cancer Screening: 2010 Stuart S. Sagel, M.D. Lung Cancer 219,440 new cases/year in U.S. (2009) 169,390 deaths/year in U.S. mortality greater than from breast, colon, prostate CA combined
Lung Cancer Screening: Who, What, Why? Myths Dispelled
 Lung Cancer Screening: Who, What, Why? Myths Dispelled Presented By: MaryAnn Tateosian, RT (R), M, MM, CIIP MGH Lung Screening Program Manager December 11, 2018 1 Lung Screening Objectives History of Smoking
Lung Cancer Screening: Who, What, Why? Myths Dispelled Presented By: MaryAnn Tateosian, RT (R), M, MM, CIIP MGH Lung Screening Program Manager December 11, 2018 1 Lung Screening Objectives History of Smoking
CT Low Dose Lung Cancer Screening. Part I. Journey to LDCT LCS Program
 CT Low Dose Lung Cancer Screening Part I Journey to LDCT LCS Program Paul Johnson, M.S., DABHP, DABR Cleveland Clinic September 26, 2015 Lung Caner is No. 1 In Cancer Related Death In The United States
CT Low Dose Lung Cancer Screening Part I Journey to LDCT LCS Program Paul Johnson, M.S., DABHP, DABR Cleveland Clinic September 26, 2015 Lung Caner is No. 1 In Cancer Related Death In The United States
Example of lung screening
 Justification of the use of CT for individual health assessment of asymptomatic people How to obtain evidence for IHA - Example of lung screening Mathias Prokop, MD PhD Professor of Radiology Radboud University
Justification of the use of CT for individual health assessment of asymptomatic people How to obtain evidence for IHA - Example of lung screening Mathias Prokop, MD PhD Professor of Radiology Radboud University
Screening for Lung Cancer. Michael S. Nolledo, MD Deborah Heart and Lung Center
 Screening for Lung Cancer Michael S. Nolledo, MD Deborah Heart and Lung Center 1 1 Outline Ø Introduction Ø Lung Cancer Screening pre-2010 Ø Lung Cancer Screening today 2 2 Lung Cancer 2011 (Siegel et
Screening for Lung Cancer Michael S. Nolledo, MD Deborah Heart and Lung Center 1 1 Outline Ø Introduction Ø Lung Cancer Screening pre-2010 Ø Lung Cancer Screening today 2 2 Lung Cancer 2011 (Siegel et
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
LUNGS? YOU GET THESE YOUR GUIDE TO YEARLY LUNG CANCER SCREENING CHECKED REGULARLY. WHAT ABOUT YOUR. Think. Screen. Know.
 YOU GET THESE CHECKED REGULARLY. WHAT ABOUT YOUR LUNGS? YOUR GUIDE TO YEARLY LUNG CANCER SCREENING WHAT YOU SHOULD KNOW BEFORE, DURING, AND AFTER Think. Screen. Know. Talk to your doctor. TABLE OF CONTENTS
YOU GET THESE CHECKED REGULARLY. WHAT ABOUT YOUR LUNGS? YOUR GUIDE TO YEARLY LUNG CANCER SCREENING WHAT YOU SHOULD KNOW BEFORE, DURING, AND AFTER Think. Screen. Know. Talk to your doctor. TABLE OF CONTENTS
LUNG CANCER: LDCT DISCLOSURES NONE. Erika Swanson, MD Radiation Oncologist Ascension Columbia-St. Mary s February 1, /9/2018
 LUNG CANCER: LDCT Erika Swanson, MD Radiation Oncologist Ascension Columbia-St. Mary s February 1, 2018 DISCLOSURES 2 NONE 1 OBJECTIVES 3 Rationale and evidence for LDCT for lung cancer screening Review
LUNG CANCER: LDCT Erika Swanson, MD Radiation Oncologist Ascension Columbia-St. Mary s February 1, 2018 DISCLOSURES 2 NONE 1 OBJECTIVES 3 Rationale and evidence for LDCT for lung cancer screening Review
Lung Cancer Risk Associated With New Solid Nodules in the National Lung Screening Trial
 Cardiopulmonary Imaging Original Research Pinsky et al. Lung Cancer Risk Associated With New Nodules Cardiopulmonary Imaging Original Research Paul F. Pinsky 1 David S. Gierada 2 P. Hrudaya Nath 3 Reginald
Cardiopulmonary Imaging Original Research Pinsky et al. Lung Cancer Risk Associated With New Nodules Cardiopulmonary Imaging Original Research Paul F. Pinsky 1 David S. Gierada 2 P. Hrudaya Nath 3 Reginald
Lung Cancer Screening:
 Lung Cancer Screening: Maximizing Gain and Dealing with Pandora s Box Mark M. Fuster, MD Division of Pulmonary & Critical Care UCSD Department of Medicine & VA San Diego Healthcare Service San Diego, CA
Lung Cancer Screening: Maximizing Gain and Dealing with Pandora s Box Mark M. Fuster, MD Division of Pulmonary & Critical Care UCSD Department of Medicine & VA San Diego Healthcare Service San Diego, CA
Lung Cancer Screening: Benefits and limitations to its Implementation
 Lung Cancer Screening: Benefits and limitations to its Implementation Rolando Sanchez, MD Clinical Assistant Professor Pulmonary-Critical Care Medicine University of Iowa Lung cancer - Epidemiology Cancer
Lung Cancer Screening: Benefits and limitations to its Implementation Rolando Sanchez, MD Clinical Assistant Professor Pulmonary-Critical Care Medicine University of Iowa Lung cancer - Epidemiology Cancer
Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center
 You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
You Smoke, You Get Lung Cancer, You Die: Can Screening Change this Paradigm? Robert J. McKenna M.D. Chief, Thoracic Surgery Cedars Sinai Medical Center AATS Saturday 4/28/2012 Cancer Screening Cancer
Lung Cancer and CT Screening
 Lung Cancer and CT Screening Samer Kanaan, MD February 17 th, 2012 Goals Understand the Societal impact of Lung Cancer Identify Risk Factors for Lung Cancer List Diagnostic Tests Available for Lung Cancer
Lung Cancer and CT Screening Samer Kanaan, MD February 17 th, 2012 Goals Understand the Societal impact of Lung Cancer Identify Risk Factors for Lung Cancer List Diagnostic Tests Available for Lung Cancer
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
Lung Cancer Diagnosis for Primary Care
 Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Lung Cancer Diagnosis for Primary Care Daniel Nader, DO, FCCP Cancer Treatment Center of America Case 1 In which of the following situations would the U.S. Preventive Services Task Force (USPSTF) recommend
Christine Argento, MD Interventional Pulmonology Emory University
 Christine Argento, MD Interventional Pulmonology Emory University Outline Lung Cancer Statistics Prior Studies for Lung Cancer Screening NLST Studies Following NLST Future Directions Lung Cancer American
Christine Argento, MD Interventional Pulmonology Emory University Outline Lung Cancer Statistics Prior Studies for Lung Cancer Screening NLST Studies Following NLST Future Directions Lung Cancer American
Professor John K Field PhD, FRCPath University of Liverpool Cancer Research Centre, UK.
 Professor John K Field PhD, FRCPath University of Liverpool Cancer Research Centre, UK. J.K.Field@liv.ac.uk 1.8 million new cases in 2012 Bender Nature Outlook 2014 Probability of survival: ALL participants
Professor John K Field PhD, FRCPath University of Liverpool Cancer Research Centre, UK. J.K.Field@liv.ac.uk 1.8 million new cases in 2012 Bender Nature Outlook 2014 Probability of survival: ALL participants
VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening
 VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening ATS San Francisco 2016 James K. Brown MD 1, Kathryn L. Rice, MD 2 (1) San Francisco VA (2) Minneapolis VAMC Disclosures
VHA Demonstration Project for Lung Cancer Screening Using Low-Dose Chest CT Screening ATS San Francisco 2016 James K. Brown MD 1, Kathryn L. Rice, MD 2 (1) San Francisco VA (2) Minneapolis VAMC Disclosures
Goals of Presentation
 Goals of Presentation Review context of lung cancer screening why is it important? Review data from NLST supporting screening with lowdose CT (LDCT) scanning Discuss the pros and cons of LDCT screening
Goals of Presentation Review context of lung cancer screening why is it important? Review data from NLST supporting screening with lowdose CT (LDCT) scanning Discuss the pros and cons of LDCT screening
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD. November 18, 2017
 Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Lung Cancer screening :
 Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
Lung Cancer screening : Pro-Contra SAMO interdisciplinary workshop on chest tumors 27 and 28 january 2017 Prof L.P.Nicod Sevice de pneumologie CHUV-Lausanne -CH Lung Cancer How big is the problem? Epidemiology
SCREENING FOR EARLY LUNG CANCER. Pang Yong Kek
 SCREENING FOR EARLY LUNG CANCER Pang Yong Kek Lecture Outline Why performing screening? How to improve early detection? Benefits and Risks of screening Challenges in screening Conclusion Why Performing
SCREENING FOR EARLY LUNG CANCER Pang Yong Kek Lecture Outline Why performing screening? How to improve early detection? Benefits and Risks of screening Challenges in screening Conclusion Why Performing
I8 COMPLETION INSTRUCTIONS
 The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
Lung Cancer Screening. Ashish Maskey MD Interventional Pulmonology UK Health Care Dec 1 st 2017
 Lung Cancer Screening Ashish Maskey MD Interventional Pulmonology UK Health Care Dec 1 st 2017 Nearly one in six American adults currently smoke cigarettes An estimated 40 million adults in the United
Lung Cancer Screening Ashish Maskey MD Interventional Pulmonology UK Health Care Dec 1 st 2017 Nearly one in six American adults currently smoke cigarettes An estimated 40 million adults in the United
Objectives. Why? Why? Background 11/5/ % incurable disease at presentation Locally advanced disease Metastasis. 14% 5 year survival
 Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
Objectives Appraise lung cancer screening trials results Review screening guidelines Lung Cancer Screening: Past, Present and Future Chi Wan Koo, MD Koo.chiwan@mayo.edu Discuss recommendations essential
GROUP 1: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases. Including: Excluding:
 GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
None
 2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
2014 None rosemary clooney Cancer is one of the most common diseases in the developed world: 1 in 4 deaths are due to cancer 1 in 17 deaths are due to lung cancer Lung cancer is the most common
LUNG NODULES: MODERN MANAGEMENT STRATEGIES
 Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Department of Radiology LUNG NODULES: MODERN MANAGEMENT STRATEGIES Christian J. Herold M.D. Department of Biomedical Imaging and Image-guided Therapy Medical University of Vienna Vienna, Austria Pulmonary
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Imaging in breast cancer. Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since
 Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
Imaging in breast cancer Mammography and Ultrasound Donya Farrokh.MD Radiologist Mashhad University of Medical Since A mammogram report is a key component of the breast cancer diagnostic process. A mammogram
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Evidence based approach to incidentally detected subsolid pulmonary nodule. DM SEMINAR July 27, 2018 Harshith Rao
 Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
Evidence based approach to incidentally detected subsolid pulmonary nodule DM SEMINAR July 27, 2018 Harshith Rao Outline Definitions Etiologies Risk evaluation Clinical features Radiology Approach Modifications:
A Comprehensive Cancer Center Designated by the National Cancer Institute
 N C I C C C A Comprehensive Cancer Center Designated by the National Cancer Institute Screening and Early Detection of Lung Cancer: Ready for Practice? David S. Ettinger, MD, FACP, FCCP Alex Grass Professor
N C I C C C A Comprehensive Cancer Center Designated by the National Cancer Institute Screening and Early Detection of Lung Cancer: Ready for Practice? David S. Ettinger, MD, FACP, FCCP Alex Grass Professor
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
Selected Controversies. Cancer Screening. Breast Cancer Screening. Selected Controversies. Page 1. Using Best Evidence to Guide Practice
 Cancer Screening Using Best Evidence to Guide Practice Judith M.E. Walsh, MD, MH Division of General Internal Medicine Women s Health Center of Excellence University of California, San Francisco Selected
Cancer Screening Using Best Evidence to Guide Practice Judith M.E. Walsh, MD, MH Division of General Internal Medicine Women s Health Center of Excellence University of California, San Francisco Selected
Criteria USPSTF CMS. Frequency Annual screening Annual screening. No signs or symptoms of lung cancer
 Lung Cancer Screening Guidelines with low- dose computed tomography (LDCT): USPSTF and CMS February 6, 2015 Kentucky Cancer Consortium and Kentucky LEADS Component 3 Jennifer Redmond Knight, DrPH, jredknight@kycancerc.org
Lung Cancer Screening Guidelines with low- dose computed tomography (LDCT): USPSTF and CMS February 6, 2015 Kentucky Cancer Consortium and Kentucky LEADS Component 3 Jennifer Redmond Knight, DrPH, jredknight@kycancerc.org
Radiologic assessment of response of tumors to treatment. Copyright 2008 TIMC, Matthew A. Barish M.D. All rights reserved. 1
 Radiologic assessment of response of tumors to treatment Copyright 2008 TIMC, Matthew A. Barish M.D. All rights reserved. 1 Objective response assessment is important to describe the treatment effect of
Radiologic assessment of response of tumors to treatment Copyright 2008 TIMC, Matthew A. Barish M.D. All rights reserved. 1 Objective response assessment is important to describe the treatment effect of
What to know and what to make of it
 Lung Cancer Screening: What to know and what to make of it J. Matthew Reinersman, MD Assistant Professor of Surgery Division of Thoracic and Cardiovascular Surgery Department of Surgery University of Oklahoma
Lung Cancer Screening: What to know and what to make of it J. Matthew Reinersman, MD Assistant Professor of Surgery Division of Thoracic and Cardiovascular Surgery Department of Surgery University of Oklahoma
Lung Cancer Screening: Current Status
 Lung Cancer Screening: Current Status I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of investigational or off-label use of a product
Lung Cancer Screening: Current Status I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of investigational or off-label use of a product
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
Lung Cancer Screening. Eric S. Papierniak, DO NF/SG VHA UF Health
 Lung Cancer Screening Eric S. Papierniak, DO NF/SG VHA UF Health Overview Background Supporting evidence Guidelines Practical considerations Patient selection What to do with abnormal results Billing/coding
Lung Cancer Screening Eric S. Papierniak, DO NF/SG VHA UF Health Overview Background Supporting evidence Guidelines Practical considerations Patient selection What to do with abnormal results Billing/coding
C2 COMPLETION INSTRUCTIONS
 The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
DISCLOSURE. Lung Cancer Screening: The End of the Beginning. Learning Objectives. Relevant Financial Relationship(s) Off Label Usage
 Off Label Usage") Peninsula Regional Medical Center 12 th Annual Lung Cancer Conference March 9, 2017 Lung Cancer Screening: The End of the Beginning David E. Midthun M.D. Professor of Medicine College of Medicine, Mayo
Peninsula Regional Medical Center 12 th Annual Lung Cancer Conference March 9, 2017 Lung Cancer Screening: The End of the Beginning David E. Midthun M.D. Professor of Medicine College of Medicine, Mayo
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2
 Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
Low-dose CT Lung Cancer Screening Guidelines for Pulmonary Nodules Management Version 2 The Committee for Management of CT-screening-detected Pulmonary Nodules 2009-2011 The Japanese Society of CT Screening
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES
 MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
Pulmonologist s Perspective
 Low-dose CT for lung cancer screening Pulmonologist s Perspective Literature Review Kang-Yun Lee, MD PhD Department of Thoracic Medicine Taipei Medical University- Shuang Ho Hospital Taiwan Local vs. Advanced
Low-dose CT for lung cancer screening Pulmonologist s Perspective Literature Review Kang-Yun Lee, MD PhD Department of Thoracic Medicine Taipei Medical University- Shuang Ho Hospital Taiwan Local vs. Advanced
CT Lung Screening Implementation Challenges: State Based Initiatives
 CT Lung Screening Implementation Challenges: State Based Initiatives Andrea McKee, MD Chair Radiation Oncology Lahey Hospital and Medical Center Co-Director Rescue Lung, Rescue Life Program Co-Chair Massachusetts
CT Lung Screening Implementation Challenges: State Based Initiatives Andrea McKee, MD Chair Radiation Oncology Lahey Hospital and Medical Center Co-Director Rescue Lung, Rescue Life Program Co-Chair Massachusetts
MANAGEMENT RECOMMENDATIONS
 1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
1 MANAGEMENT RECOMMENDATIONS 1. Adrenal masses!!!!!!! page 2 2. Liver Masses!!!!!!! page 3 3. Obstetric US Soft Markers for Aneuploidy!! pages 4-6 4. Ovarian and Adnexal Cysts!!!!! pages 7-10 5. Pancreatic
Breast Cancer PET/CT Imaging Protocol
 Breast Cancer PET/CT Imaging Protocol Scanning Protocol: Patients are scanned from the top of the neck through the pelvis. Arms-up position is used to avoid beam-hardening artifact in the chest and abdomen.
Breast Cancer PET/CT Imaging Protocol Scanning Protocol: Patients are scanned from the top of the neck through the pelvis. Arms-up position is used to avoid beam-hardening artifact in the chest and abdomen.
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University
 LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
LUNG CANCER SCREENING WHAT S THE IMPACT? Nitra Piyavisetpat, MD Department of Radiology Chulalongkorn University Objective LDCT lung cancer screening (LCS) Potential Benefits & Harms Recommendation of
Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned
 Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned Jane Kim, MD, MPH Acting Chief Consultant for Preventive Medicine National Center for Health Promotion
Veterans Health Administration Lung Cancer Screening Demonstration Project: Results & Lessons Learned Jane Kim, MD, MPH Acting Chief Consultant for Preventive Medicine National Center for Health Promotion
Page 1. Selected Controversies. Cancer Screening! Selected Controversies. Breast Cancer Screening. ! Using Best Evidence to Guide Practice!
 Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
The Virtual Lung Nodule Clinic
 The Virtual Lung Nodule Clinic Poster No.: C-1023 Congress: ECR 2016 Type: Educational Exhibit Authors: S. Higgins, F. C. Lyall, J. Taylor, J. goldman, S. Rolin, B. 1 2 1 2 2 3 2 2 3 Soar ; Torbay/UK,
The Virtual Lung Nodule Clinic Poster No.: C-1023 Congress: ECR 2016 Type: Educational Exhibit Authors: S. Higgins, F. C. Lyall, J. Taylor, J. goldman, S. Rolin, B. 1 2 1 2 2 3 2 2 3 Soar ; Torbay/UK,
Published Pulmonary Nodule Guidelines A Synthesis
 Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
Published Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj Royal Brompton Hospital London 4/28/2015 1 And very soon to be published Published ^ Pulmonary Nodule Guidelines A Synthesis Dr A Devaraj
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Faculty Disclosure. Objectives. Lung Cancer in Kentucky: Improving Patient Outcomes 10/28/16. Lung Cancer Burden in Kentucky
 Lung Cancer in Kentucky: Improving Patient Outcomes Faculty Disclosure The presenter and members of the development team do not have any conflicts to report. Celeste T. Worth, MCHES Kentucky Collaborative
Lung Cancer in Kentucky: Improving Patient Outcomes Faculty Disclosure The presenter and members of the development team do not have any conflicts to report. Celeste T. Worth, MCHES Kentucky Collaborative
DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS
 DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS December 2018 Page 1 of 18 Document Title: Document Ref. Number: DOH Lung Cancer Screening Service Specifications PH/NCD/LCSC/SR/0.9 Version: 0.9 Approval
DOH LUNG CANCER SCREENING SERVICE SPECIFICATIONS December 2018 Page 1 of 18 Document Title: Document Ref. Number: DOH Lung Cancer Screening Service Specifications PH/NCD/LCSC/SR/0.9 Version: 0.9 Approval
Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer
 November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
Introduction and Background
 CT Lung Cancer Screening and the Medical Physicist: Background, Findings and Participant Dosimetry Summary of the National Lung Screening Trial (NLST) Randell Kruger, PhD, DABR Medical Physics Section
CT Lung Cancer Screening and the Medical Physicist: Background, Findings and Participant Dosimetry Summary of the National Lung Screening Trial (NLST) Randell Kruger, PhD, DABR Medical Physics Section
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
Patient Decision Aid. Summary Guide for Clinicians. Clinician s Checklist
 U.S. Department of Health & Human Services About Us Careers Contact Us Español FAQ Email Updates Effective Health Care Home / Decision Aids / Lung Cancer Screening Tools Patient Decision Aid Summary Guide
U.S. Department of Health & Human Services About Us Careers Contact Us Español FAQ Email Updates Effective Health Care Home / Decision Aids / Lung Cancer Screening Tools Patient Decision Aid Summary Guide
Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening
 Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening 1. Introduction In January 2005, the Committee for Preparation of Clinical Practice Guidelines for the Management
Guidelines for the Management of Pulmonary Nodules Detected by Low-dose CT Lung Cancer Screening 1. Introduction In January 2005, the Committee for Preparation of Clinical Practice Guidelines for the Management
Lung Cancer Screening: Now What?
 Lung Cancer Screening: Now What? Gerold Bepler, M.D., Ph.D. Director, President & CEO Michigan Cancer Consortium, 2013 Annual Meeting, Lansing, MI, 11/20/13 Lung Cancer #1 Cause of Cancer Death for & *
Lung Cancer Screening: Now What? Gerold Bepler, M.D., Ph.D. Director, President & CEO Michigan Cancer Consortium, 2013 Annual Meeting, Lansing, MI, 11/20/13 Lung Cancer #1 Cause of Cancer Death for & *
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Cancer Screenings and Early Diagnostics
 Cancer Screenings and Early Diagnostics Ankur R. Parikh, D.O. Medical Director, Center for Advanced Individual Medicine Hematologist/Medical Oncologist Atlantic Regional Osteopathic Convention April 6
Cancer Screenings and Early Diagnostics Ankur R. Parikh, D.O. Medical Director, Center for Advanced Individual Medicine Hematologist/Medical Oncologist Atlantic Regional Osteopathic Convention April 6
Implementation & optimization of a lung cancer screening CT program. Presented by Izabella Barreto at the 2016 Florida AAPM Chapter Meeting
 Implementation & optimization of a lung cancer screening CT program Presented by Izabella Barreto at the 2016 Florida AAPM Chapter Meeting Izabella Barreto, Nathan Quails, Catherine Carranza, Nathalie
Implementation & optimization of a lung cancer screening CT program Presented by Izabella Barreto at the 2016 Florida AAPM Chapter Meeting Izabella Barreto, Nathan Quails, Catherine Carranza, Nathalie
Amammography report is a key component of the breast
 Review Article Writing a Mammography Report Amammography report is a key component of the breast cancer diagnostic process. Although mammographic findings were not clearly differentiated between benign
Review Article Writing a Mammography Report Amammography report is a key component of the breast cancer diagnostic process. Although mammographic findings were not clearly differentiated between benign
The solitary pulmonary nodule: Assessing the success of predicting malignancy
 The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
The solitary pulmonary nodule: Assessing the success of predicting malignancy Poster No.: C-0829 Congress: ECR 2010 Type: Scientific Exhibit Topic: Chest Authors: R. W. K. Lindsay, J. Foster, K. McManus;
Lung Cancer Update. Disclosures. None
 Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
Lung Cancer Update Ronald J Servi DO FCCP Adjunct Assistant Professor Department of Pulmonary Medicine University of Texas MD Anderson Cancer Center Banner MD Anderson Cancer Center Gilbert, Arizona Disclosures
LDCT Screening. Steven Kirtland, MD. Virginia Mason Medical Center February 27, 2015
 LDCT Screening Steven Kirtland, MD Virginia Mason Medical Center February 27, 2015 2 Disclosures 4 5 Cancer Screening Mrs H 64yo 50 pk year smoker Lung Cancer Epidemiology Leading Cause of Cancer Death
LDCT Screening Steven Kirtland, MD Virginia Mason Medical Center February 27, 2015 2 Disclosures 4 5 Cancer Screening Mrs H 64yo 50 pk year smoker Lung Cancer Epidemiology Leading Cause of Cancer Death
CT screening for lung cancer. Should it be done in the Indian context?
 CT screening for lung cancer Should it be done in the Indian context? Wilson and Jungner screening criteria 1. The condition sought should be an important health problem. 2. There should be an accepted
CT screening for lung cancer Should it be done in the Indian context? Wilson and Jungner screening criteria 1. The condition sought should be an important health problem. 2. There should be an accepted
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
DENOMINATOR: All final reports for CT imaging studies with a finding of an incidental pulmonary nodule for patients aged 35 years and older
 Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Quality ID #364: Optimizing Patient Exposure to Ionizing Radiation: Appropriateness: Follow-up CT Imaging for Incidentally Detected Pulmonary Nodules According to Recommended Guidelines National Quality
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel