Renal Cell Cancer: Present and Future. Bernard Escudier, Gustave Roussy
|
|
|
- Herbert Parrish
- 6 years ago
- Views:
Transcription
1 Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request
2 Disclosures Compensated advisory boards Novartis, Roche, BMS, Pfizer, Exelixis, Ipsen, Acceleron Speaker honoraria Novartis, Bayer, BMS, Pfizer, Ipsen
3 Renal cell carcinoma Accounts for 3.7% of all cancer diagnoses and 2.4% of all cancer deaths worldwide Seventh most common cancer in men Tenth most common cancer in women 1 Incidence highest in the USA, Western Europe and other developed countries 2 Median age at diagnosis is 64 years for kidney and renal pelvis cancer 3 Cancer stage at diagnosis determines treatment options and has a strong influence on the length of survival 5-year relative survival rate: localised = 93% vs metastatic = 12% 3 Median OS ~12 months in metastatic RCC before targeted agents 4 Median OS ~30 months in most recent studies, highly dependent on prognostic factors 5 1. Siegel et al. CA Cancer J Clin 2016; 2. Ferlay et al. Int J Cancer SEER Stat Fact Sheets: Kidney and Renal Pelvis Cancer 4. Soerensen et al. Eur J Cancer 2014; 5. Motzer et al. N Engl J Med 2013
4 The evolving treatment landscape of mrcc IFN-α High-dose IL Cytokines arcc, advanced renal cell carcinoma; FDA, US Food and Drug Administration; IFN-α, interferon α; IL-2, interleukin-2; mtor, mammalian target of rapamycin; VEGF, vascular endothelial growth factor. *Approved by the FDA in RCC. 1. Escudier B, et al. N Engl J Med. 2007;356: ; 2. Motzer RJ, et al. N Engl J Med. 2007;356: ; 3. Hudes G, et al. N Engl J Med. 2007;356: ; 4. Motzer RJ, et al. Lancet. 2008;372: ; 5. Escudier B, et al. Lancet. 2007;370: ; 6. Rini BI, et al. J Clin Oncol. 2008;26: ; 7. Sternberg CN, et al. J Clin Oncol. 2010;28: ; 8. Rini BI, et al. Lancet. 2011;378: ; 9. Motzer RJ, et al. N Engl J Med. 2015;373(19): ; 10. Choueiri TK, et al. N Engl J Med. 2015;373(19): ; 11. Motzer RJ, et al. Lancet Oncol. 2015;16(15):
5 Cytokines have played an important role in mrcc for >20 years DOR in IL-2 responders 1 OS 1 Probability of continuing response mdor = NR (7to >131 months) mdor = 20 months (3 to >126 months) Complete responders Partial responders Probability of survival Time (months) Time (months) IL-2 associated with durable responses: ORR=15% (CR=7% and PR=8%) % of patents alive after 5 10 years of treatment 1 BUT associated with substantial toxicity 2 1. Fisher et al. Cancer J Sci Am McDermott et al. J Clin Oncol 2005
6 Survival with IFN-α in mrcc (by MSKCC risk) Proportion surviving risk factors (n=80) 1 or 2 risk factors (n=269) 3, 4 or 5 risk factors (n=88) Five risk factors associated with worse outcome KPS <80 Time from diagnosis to IFN-α <1 year Low serum haemoglobin High corrected calcium (>2.5mmol/L [10mg/dl]) High LDH (>1.5 ULN) Median survival 30 months 14 months 5 months Time (years) Motzer et al. J Clin Oncol 2002
7 The evolving treatment landscape of mrcc IFN-α High-dose IL-2 Sorafenib 1 Sunitinib 2 Temsirolimus 3 Everolimus 4 Bevacizumab + IFN-α 5,6 Pazopanib 7 Axitinib Cytokines VEGF-TKI, mtor-targeted and IO therapies (based on FDA approval dates) arcc, advanced renal cell carcinoma; FDA, US Food and Drug Administration; IFN-α, interferon α; IL-2, interleukin-2; mtor, mammalian target of rapamycin; VEGF, vascular endothelial growth factor. *Approved by the FDA in RCC. 1. Escudier B, et al. N Engl J Med. 2007;356: ; 2. Motzer RJ, et al. N Engl J Med. 2007;356: ; 3. Hudes G, et al. N Engl J Med. 2007;356: ; 4. Motzer RJ, et al. Lancet. 2008;372: ; 5. Escudier B, et al. Lancet. 2007;370: ; 6. Rini BI, et al. J Clin Oncol. 2008;26: ; 7. Sternberg CN, et al. J Clin Oncol. 2010;28: ; 8. Rini BI, et al. Lancet. 2011;378: ; 9. Motzer RJ, et al. N Engl J Med. 2015;373(19): ; 10. Choueiri TK, et al. N Engl J Med. 2015;373(19): ; 11. Motzer RJ, et al. Lancet Oncol. 2015;16(15):

8 Temsirolimus Everolimus Sunitinib Sorafenib Pazopanib Axitinib Rini BI, Campbel S and Escudier B. Lancet. 2009;373(9669):
9 ...improving OS outcomes Selected phase III studies of targeted therapies in mrcc 30 1L studies 2L studies Median OS (months) vs vs vs vs vs 15.2 Survival plateau ~30 months 20.1 vs vs Bevacizumab + IFN-α vs IFN-α 1,2 Sunitinib vs IFN-α 3,4 Pazopanib vs sunitinib 5 Temsirolimus vs IFN-α 6,* Sorafenib vs placebo 7,8 Axitinib vs sorafenib 9,10 Everolimus vs placebo 11 *Patients with poor prognostic factors 1. Escudier et al. Lancet 2007; 2. Escudier et al. J Clin Oncol 2010; 3. Motzer et al. N Engl J Med 2007; 4. Motzer et al. J Clin Oncol Motzer et al. N Engl J Med 2013; 6. Hudes et al. N Engl J Med 2007; 7. Escudier et al. N Engl J Med Escudier et al. J Clin Oncol 2009; 9. Rini et al. Lancet 2011; 10. Motzer et al. Lancet Oncol 2013; 11. Motzer et al. Cancer 2010
10 ...improving OS outcomes Selected phase III studies of targeted therapies in mrcc 30 1L studies 2L studies Median OS (months) vs vs vs 29.3 Patients with poor prognostic factors 10.9 vs vs 15.2 Survival plateau ~30 months Survival plateau ~20 months 20.1 vs vs Bevacizumab + IFN-α vs IFN-α 1,2 Sunitinib vs IFN-α 3,4 Pazopanib vs sunitinib 5 Temsirolimus vs IFN-α 6,* Sorafenib vs placebo 7,8 Axitinib vs sorafenib 9,10 Everolimus vs placebo 11 *Patients with poor prognostic factors 1. Escudier et al. Lancet 2007; 2. Escudier et al. J Clin Oncol 2010; 3. Motzer et al. N Engl J Med 2007; 4. Motzer et al. J Clin Oncol Motzer et al. N Engl J Med 2013; 6. Hudes et al. N Engl J Med 2007; 7. Escudier et al. N Engl J Med Escudier et al. J Clin Oncol 2009; 9. Rini et al. Lancet 2011; 10. Motzer et al. Lancet Oncol 2013; 11. Motzer et al. Cancer 2010
11 Additional unmet needs of targeted therapies in mrcc Up to 26% of patients refractory to 1L anti-angiogenic agents 1 Complete responses to targeted therapies are rare 2 Bevacizumab + IFN-α TKIs 26% Sunitinib 19% 2.5% 1.6% Sorafenib 5% Bevacizumab 2% Incidence of complete response 1. Heng et al. Ann Oncol Iacovelli et al. Cancer Treat Rev 2014
12 The evolving treatment landscape of mrcc IFN-α High-dose IL-2 Sorafenib 1 Sunitinib 2 Temsirolimus 3 Everolimus 4 Bevacizumab + IFN-α 5,6 Pazopanib 7 Axitinib 8 Cabozantinib 10 Nivolumab 9 * Lenvatinib + Afinitor Cytokines VEGF-TKI, mtor-targeted and IO therapies (based on FDA approval dates) arcc, advanced renal cell carcinoma; FDA, US Food and Drug Administration; IFN-α, interferon α; IL-2, interleukin-2; mtor, mammalian target of rapamycin; VEGF, vascular endothelial growth factor. *Approved by the FDA in RCC. 1. Escudier B, et al. N Engl J Med. 2007;356: ; 2. Motzer RJ, et al. N Engl J Med. 2007;356: ; 3. Hudes G, et al. N Engl J Med. 2007;356: ; 4. Motzer RJ, et al. Lancet. 2008;372: ; 5. Escudier B, et al. Lancet. 2007;370: ; 6. Rini BI, et al. J Clin Oncol. 2008;26: ; 7. Sternberg CN, et al. J Clin Oncol. 2010;28: ; 8. Rini BI, et al. Lancet. 2011;378: ; 9. Motzer RJ, et al. N Engl J Med. 2015;373(19): ; 10. Choueiri TK, et al. N Engl J Med. 2015;373(19): ; 11. Motzer RJ, et al. Lancet Oncol. 2015;16(15):










13 Understanding immune resistance has been key Naive T Cell Activated T Cell Exhausted T Cell Reinvigorated T Cell Positive Signal Negative Signal Positive Signal T-cell clonal expansion Cytokine secretion Effector functions Tumour-directed migration Signal 1 TCR AG MHC CD28 B7 Signal 2 PD-1 PD-L1 PD-1 BMS PD-L1 T-cell clonal expansion Cytokine secretion Effector functions Tumour-directed migration APC or Tumour cell APC or Tumour cell APC or Tumour cell AG, antigen; APC, antigen presenting cell; MHC, major histocompatibility complex; PD-1, programmed death-1; TCR, T-cell receptor. Adapted from Brahmer JR et al. J Clin Oncol. 2010;28: and Keir ME et al. Annu Rev Immunol. 2008;26:
14 PD-L1 expression is a negative prognostic factor in RCC Study or subgroup Log [HR] SE Weight (%) HR IV, random, 95% CI Year HR IV, random, 95% CI Thompson et al [1.39, 6.13] 2004 Thompson et al [1.27, 3.15] 2006 Frigola et al [0.95, 1.76] 2011 Choueiri et al [2.17, 18.88] 2014 Crispin et al [0.77, 3.10] 2014 Choueiri et al [1.04, 1.97] 2015 Total (95% CI) [1.31, 2.50] Favours PD-L1+ 5 Favours PD-L1 20 Heterogeneity: Tau²=0.08; Chi²=12.14, df=5 (p=0.03); I²=59% Test for overall effect: Z=3.63 (p=0.0003) 1. Thompson et al. Proc Natl Acad Sci USA 2004; 2. Thompson et al. Cancer Res 2006; 3. Frigola et al. Clin Cancer Res Choueiri et al. Ann Oncol 2014; 5. Crispin et al. J Clin Oncol 2014; 6. Choueiri et al. Clin Cancer Res 2015 Table adapted from Iacovelli et al. Target Oncol 2015

15 CheckMate 025 phase III Motzer RJ, et al. N Eng J Med. 2015;373(19):
16 CheckMate 025 (phase III): nivolumab associated with longer OS vs everolimus in previously treated mrcc OS estimate Nivolumab (n=410) Everolimus (n=411) HR=0.73 ( ) p= Time (months) Minimum follow-up = 14 months Sharma et al. ECC 2015; Motzer et al. N Engl J Med 2015
17 CheckMate 025: OS benefit of nivolumab irrespective of PD-L1 expression PD-L1 1% (n=24%) PD-L1 <1% (n=76%) 1.0 Nivolumab (n=94) 1.0 Nivolumab (n=279) 0.8 Everolimus (n=87) HR=0.79 ( ) 0.8 Everolimus (n=299) HR=0.77 ( ) OS estimate OS estimate Time (months) Time (months) Sharma et al. ECC 2015; Motzer et al. N Engl J Med 2015
18 CheckMate 025: response outcomes improved with nivolumab Nivolumab (n=410) Everolimus (n=411) ORR, % 25 5 Odds ratio (p-value) Best overall response, % CR PR SD PD Not evaluated 5.98 (p<0.0001) Median time to response (range), months 3.5 ( ) 3.7 ( ) Median DOR (range, months) 12.0 (0 27.6) 12.0 (0 22.2) Ongoing response, % *For patients without progression or death, duration of response is defined as the time from the first response (CR/PR) date to the date of censoring Sharma et al. ECC 2015
19 QoL in CheckMate-025 Mean change from baseline in QoL scores (FKSI-DRS) in the nivolumab group increased over time and differed significantly from the everolimus group at each assessment through week 104 (P <.05) 1 Mean change from baseline Better Worse Nivolumab Everolimus No. of patients at risk Week Nivolumab Everolimus Questionnaire completion rate: 80% during the first year of follow-up. Reprinted with permission from Sharma P, et al. Oral presentation at 2015 ECCO/ESMO; September 25-29, 2015; Vienna, Austria, Abstract 3LBA. 1. Motzer RJ et al. N Engl J Med. 2015;373(19): Supplementary appendix available online:




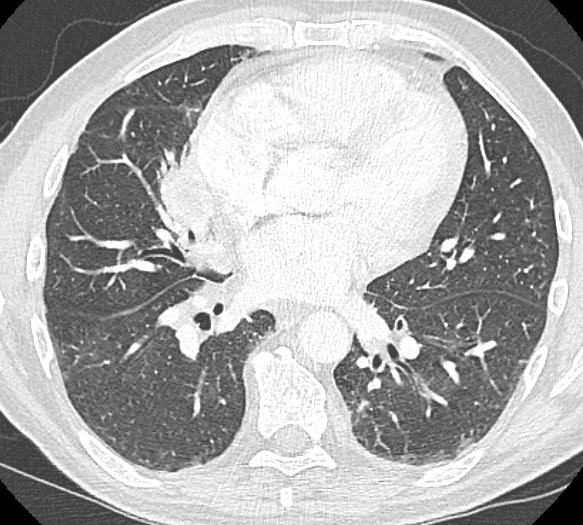
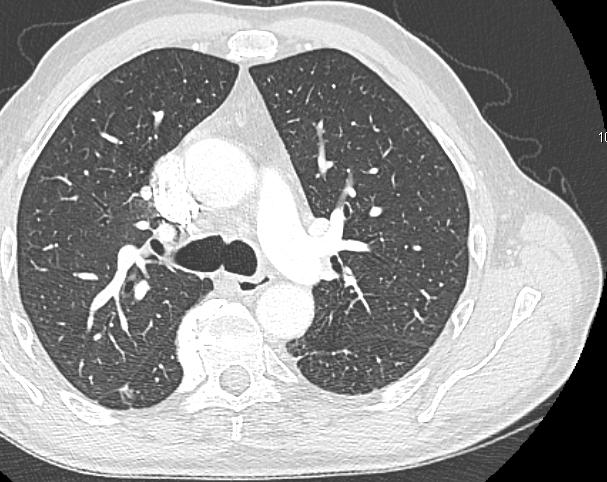
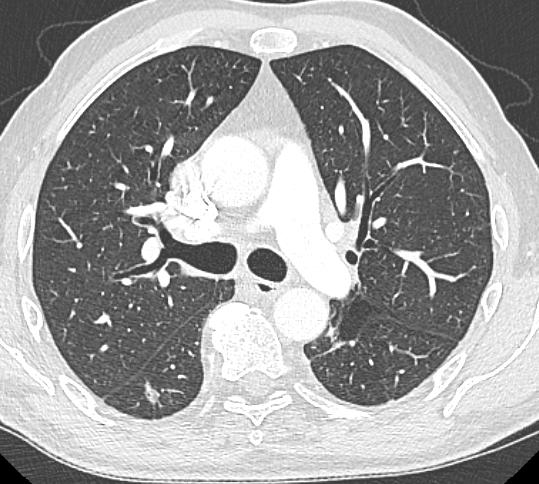
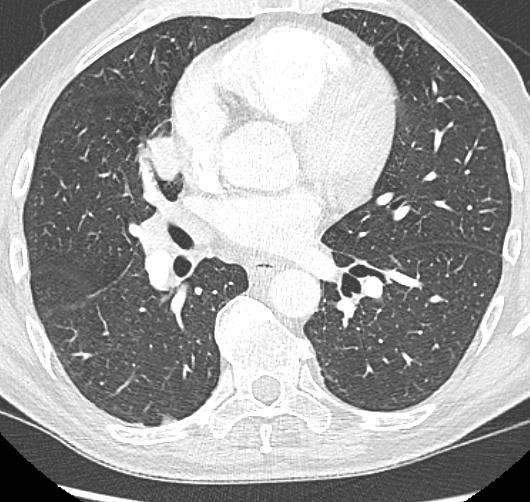
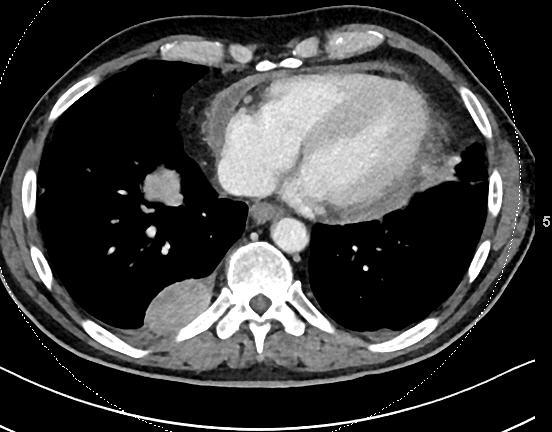
20 Case 1: 4th line therapy, still in CR in May Oct Jan 2016 This patient improved after the first infusion Rapid PR Now in CR after 19 months




21 Case 2: 2nd line therapy, PR ongoing for 12 months Baseline 2 months This patient develop PPR He received steroids Still on Nivolumab with ongoing response


22 Understanding escape mechanisms to VEGF targeted agents has also been very important Adaptive resistance: VEGF-targeted agents fail to produce enduring clinical responses in most patients Intrinsic resistance: No predictive biomarkers available to date Bergers G, Hanahan D. Nat Rev Cancer. 2008;8:




23 Several pathways are involved Early phase: response to anti-vegfr2 treatment No angiogenesis VEGF Hypoxia Cancer cells Late phase: evasion to anti-vegfr2 treatment VEGF Reactivation of angiogenesis FGFs cmet, FGF and others Cancer cells Endothelial cells Endothelial cells FGF2 is expressed by numerous tumor types and exerts its activity by interacting with TK receptors, heparan-sulfate proteoglycans, and integrins expressed on the endothelial cell surface




 Corrected serum calcium ( vs < 10 mg/dl)")
24 Lenvatinib Study Design Key eligibility criteria: Advanced or metastatic RCC Measurable disease Progression on/after 1 prior VEGFtargeted therapy Progression within 9 mos of stopping prior treatment ECOG PS 1 R A N D OM I Z E Lenvatinib 18 mg PO qd + Everolimus 5 mg PO qd Lenvatinib 24 mg PO qd Patients were treated until: Disease progression Unacceptable toxicity Everolimus 10 mg PO qd Stratification factors: Hemoglobin (normal vs low) Corrected serum calcium ( vs < 10 mg/dl) Motzer et al. Lancet Oncol 2016
25 Secondary Endpoint: OS Median, months (95% CI) Lenvatinib/everolimus 25.5 (16.4-NE) Lenvatinib 19.1 ( ) Everolimus 15.4 ( ) 0.6 OS Time, months Lenvatinib/everolimus vs Everolimus HR = 0.51 (95% CI, ); P = Lenvatinib vs everolimus HR = 0.68 (95% CI, ); P = Motzer et al. Lancet Oncol 2016





26 MET and Acquired Resistance to VEGF-targeted Therapies EFGR Plexin B CD44 Α6β4 Integrin Cytoplasm Hypoxia triggers increase in cmet expression and activity: Cell invasion and migration Cell proliferation Cell survival Inhibition of cmet may help overcome acquired resistance to the VEGF pathway Cell proliferation Cell invasion Motility Epithelial-mesenchymal transitions Cell survival Dual inhibitors of cmet and VEGFr2 such as Cabozantinib are active




27 METEOR Study Design Cabozantinib Advanced RCC (N=658) Clear cell component Progression within 6 months of prior VEGFR TKI No limit to the number of prior therapies PD-1 checkpoint inhibitors allowed Treated brain metastases allowed 1:1 60 mg qd PO Stratification MSKCC 1 risk groups: favorable, intermediate, poor Prior VEGFR-TKIs: 1 or 2 Tumor assessment every 8 weeks (RECIST v1.1) Treatment until loss of clinical benefit or intolerable toxicity No crossover allowed Everolimus 10 mg qd PO Choueiri TK, et al. Lancet Oncol 2016;17:917 27
28 Overall Survival Overall Survival (%) No. at Risk Cabozantinib Everolimus 0 Cabozantinib Everolimus No. of Patients Median Overall Survival mo (95% CI) HR = 0.66 (95% CI , P=0.0003) No. of Deaths Cabozantinib (18.7-NE) 140 Everolimus ( ) Months Choueiri TK, et al. Lancet Oncol 2016;17:917 27
29 Updated ESMO guidelines: algorithm for systemic treatment in clear cell mrcc Good or intermediate risk Poor risk 3L 2L 1L Sunitinib Bevacizumab + IFN Pazopanib Temsirolimus Post cytokines Post TKIs Axitinib Sorafenib Pazopanib Nivolumab Cabozantinib Post 2 TKIs Post TKI and mtor Post TKI / nivolumab Post TKI / cabozantinib Nivolumab Cabozantinib Nivolumab Cabozantinib Cabozantinib Nivolumab VEGF TKI VEGF MAb + IFN-α mtor inhibitor PD-1 inhibitor Escudier et al. Ann Oncol 2016

 Non-inflamed KILL CANCER CELLS (tumour) Inflamed CSF1R")
30 How can we further enhance responses? CTLA4 inhibitors Priming and activation of T cells RECRUIT / INFILTRATE (vasculature) Non-inflamed CEA IL-2V* IL-2 ACTIVATE (central) Non-inflamed KILL CANCER CELLS (tumour) Inflamed CSF1R acsf1r* Chen and Mellman. Immunity 2013
31 How can we further enhance responses? VEGF inhibitors Infiltration of T cells into tumours RECRUIT / INFILTRATE (vasculature) Non-inflamed CEA IL-2V* IL-2 ACTIVATE (central) Non-inflamed KILL CANCER CELLS (tumour) inflamed CSF1R acsf1r* Chen and Mellman. Immunity 2013
32 The evolving treatment landscape of mrcc IFN-α High-dose IL-2 Sorafenib 1 Sunitinib 2 Temsirolimus 3 Everolimus 4 Bevacizumab + IFN-α 5,6 Pazopanib 7 Axitinib 8 Nivolumab 9 * Cabozantinib 10 Avelumab + Axitinib? Lenvatinib + Afinitor 11 Nivolumab + Ipilimumab? Atezolizumab + Bevacizumab? Cytokines VEGF-TKI, mtor-targeted and IO therapies (based on FDA approval dates) Investigational therapies arcc, advanced renal cell carcinoma; FDA, US Food and Drug Administration; IFN-α, interferon α; IL-2, interleukin-2; mtor, mammalian target of rapamycin; VEGF, vascular endothelial growth factor. *Approved by the FDA in RCC. 1. Escudier B, et al. N Engl J Med. 2007;356: ; 2. Motzer RJ, et al. N Engl J Med. 2007;356: ; 3. Hudes G, et al. N Engl J Med. 2007;356: ; 4. Motzer RJ, et al. Lancet. 2008;372: ; 5. Escudier B, et al. Lancet. 2007;370: ; 6. Rini BI, et al. J Clin Oncol. 2008;26: ; 7. Sternberg CN, et al. J Clin Oncol. 2010;28: ; 8. Rini BI, et al. Lancet. 2011;378: ; 9. Motzer RJ, et al. N Engl J Med. 2015;373(19): ; 10. Choueiri TK, et al. N Engl J Med. 2015;373(19): ; 11. Motzer RJ, et al. Lancet Oncol. 2015;16(15):

33 First-line trials expected soon PD1 + CTLA4 inhibition PD-L1 + VEGF inhibition Personalized immunotherapy + VEGFR inhibition CheckMate Phase III Immotion Phase III ADAPT 3 Phase III Sunitinib 50 mg/day 4/2 Sunitinib 50 mg/day 4/2 Sunitinib R N = 1071 N = 830 R R N = 450 Nivolumab + ipilimumab 3 mg/kg IV + 1 mg/kg IV every 3 weeks 4 then nivolumab 3 mg/kg IV every 2 weeks Atezolizumab + bevacizumab 1,200 mg IV + 15 mg/kg IV every 3 weeks AGS sunitinib 8 injections in first year followed by quarterly boosters + sunitinib Co-primary endpoint: PFS, OS Co-primary endpoint: PFS, OS Primary endpoint: OS
34 First-line ongoing trials PD-L1 + VEGFR TK inhibition Combination VEGFR + mtor/pd1 inhibition PD1 + VEGFR TK inhibition Javelin renal Phase III Lenvatinib + everolimus or pembrolizumab 3 Phase III KEYNOTE Phase III Sunitinib 50 mg/day 4/2 Sunitinib 50 mg/day 4/2 Sunitinib 50 mg/day 4/2 R N = 583 R N = 735 R N = 840 Avelumab + axitinib 10 mg/kg IV every 2 weeks + 5 mg PO BD Lenvatinib + pembro 20 mg/day mg (IV) every 3 weeks Axitinib + pembro 5 mg BID mg (IV) every 3 weeks Lenvatinib + everolimus 18 mg/day + 5 mg/day Primary endpoint: PFS Primary endpoint: PFS Co-primary endpoint: PFS, OS
35 Multiple targets for checkpoint inhibitor in clinical development for mrcc Activating receptors Inhibitory receptors Anti-CTLA4 Ipilimumab (phase II and III) OX40 GITR CD28 CTLA-4 PD-1 TIM-3 Anti-PD1 Pembrolizumab (phase III) PDR001 (phase I/II) Nivolumab (phase II/III) CD137 CD27 T cell BTLA VISTA Anti-PDL1 Atezolizumab (phase II and III) Avelumab (phase III) HVEM LAG-3 Anti-TIM3 MBG453 (Phase I/II) Anti-LAG3 LAG525 (phase I/II) Agonistic T cell stimulation Blocking Mellman et al. Nature 2011
36 What is the future of immunotherapy in RCC? How best to integrate newer agents into routine clinical practice? Can we predict response? How long should we treat our patients? How to best manage toxicities?
37 What is the future of immunotherapy in RCC? How best to integrate newer agents into routine clinical practice? Can we predict response? How long should we treat our patients? How to best manage toxicities?
38 New response types with immunotherapy Wolchok et al Clin Cancer Res 2009 Immune-Related Response Criteria
39 There is a large evidence that 1. Treatment can be stopped: Especially in case of CR In case of severe toxicity Ongoing discontinuation trials are needed 2. Some patients should be treated beyond progression
40 Should we treat beyond progression? A total of 142 of 153 patients treated with nivolumab beyond progression had tumor measurements pre- and post-progression Of these 142 patients, approximately half had a reduction in tumor burden post-progression and 14% (n = 20) had 30% reduction in tumor burden post-progression Best Reduction From First Progression in Target Lesion (%) Patients Asterisks represent responders before first progression. Square symbol represents % change truncated to 100% Escudier et al. Eur Urol 2017, in press
41 Who should we treat beyond progression? Patients with good safety profile Patients with «clinical benefit» No impairment of general condition No major progression Commonly those with dissociated responses



42 Good patients to treat beyond progression Case 1





43 BL 8w 16w Good patients to treat beyond progression Case 2



44 What is the future of immunotherapy in RCC and melanoma? How best to integrate newer agents into routine clinical practice? Can we predict response? How long should we treat our patients? How to best manage toxicities?
45 Treatment-Related AEs Occurring in 10% of Patients in Either Arm Nivolumab N=406 Everolimus N=397 Event Any Grade Grade 3/4 Any Grade Grade 3/4 Treatment-related AEs, % Fatigue Nausea 14 < Pruritus Diarrhea Decreased appetite 12 < Rash 10 < Cough Anemia Dyspnea <1 Edema, peripheral <1 Pneumonitis Mucosal inflammation Dysgeusia Hyperglycemia Stomatitis Hypertriglyceridemia Motzer RJ et al. N Engl J Med. 2015;373: Epistaxis

 Immune-Mediated Adverse Reaction Management Guide. October 2012. http://www.accessdata.fda.")
46 Toxicity With Immunotherapy Agents Activation of the immune system against tumors can result in a novel spectrum of iraes 1 May be due to cytokine release by activated T cells 1 May be unfamiliar to clinicians Requires a multidisciplinary approach Can be serious 2 Requires prompt recognition and treatment 2 Requires patient and HCP education 3 iraes occur in certain organ systems: 1 Skin Endocrine system Liver Gastrointestinal tract Nervous system Eyes Respiratory system Hematopoietic cells 1. Amos SM et al. Blood. 2011;118: ; 2. YERVOY (ipilimumab) Immune-Mediated Adverse Reaction Management Guide. October _IMMUNE%20MEDIATED%20ADVERSE%20REACTION%20MANAGEMENT%20GUIDE.pdf. March Accessed May 12, 2016; 3. Association of Community Cancer Centers. Advancing Immuno-Oncology in the Community Setting. Accessed May 12, 2016.
47 Months Some key messages Most of the toxicities occur early on Overall 6 >6 12 >12 18 >18 24 >24 30 >30 36 >36
48 Some key messages Most of the toxicities occur early on They are rapidly reversible on steroids (1mg/kg mostly IV) Steroids do not decrease the efficacy, when needed
49 Summary Monotherapy with PD-L1/PD-1 inhibitors has demonstrated activity in mrcc Nivolumab approved as 2L therapy Ongoing investigations using combinations with other compounds Immunotherapy combinations PD-1 + CTLA-4 inhibition Immunotherapy + anti-vegf inhibition PD-1 + TKIs (or bevacizumab) Biomarkers, duration of therapy are still under investigation Management of side effects is important
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea
 Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Integrating novel therapy in advanced renal cell carcinoma
 Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
NEXT GENERATION DRUGS IN KIDNEY CANCER. Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden
 NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Metastatic renal cancer (mrcc): Evidence-based treatment
: Evidence-based treatment") Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Sequencing of therapies in mrcc. Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC
 Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY FOR THE RIGHT PATIENT
 Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game?
 Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Medical Management of Renal Cell Carcinoma
 Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
Linee guida terapeutiche oncologiche. Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona
 Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Targeted and immunotherapy in RCC
 Targeted and immunotherapy in RCC Treatment options Surgery (radical VS partial nephrectomy) Thermal ablation therapy Surveillance Immunotherapy Molecular targeted therapy Molecular targeted therapy Targeted
Targeted and immunotherapy in RCC Treatment options Surgery (radical VS partial nephrectomy) Thermal ablation therapy Surveillance Immunotherapy Molecular targeted therapy Molecular targeted therapy Targeted
Immunotherapy for the Treatment of Kidney and Bladder Cancer
 Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Immunotherapy for the Treatment of Kidney and Bladder Cancer Alan J. Koletsky, MD Genitourinary Cancer Research Program, Lynn Cancer Institute Clinical Asistant Professor of Biomedical Science The Charles
Innovaciones en el tratamiento del ca ncer renal. Enrique Grande
 Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
I Kid(ney) You Not: Updates on Renal Cell Carcinoma
 You Not: Updates on Renal Cell Carcinoma") Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial
: Results of a phase I trial") Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Second - Line Debate: Axitinib
 Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
The Therapeutic Landscape in Advanced Renal Cell Carcinoma
 The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Treatment Algorithm and Therapy Management in mrcc. Manuela Schmidinger Medical University of Vienna Austria
 Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
A Review in the Treatment Options for Renal Cell Cancer
 A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma
 for Metastatic Renal Cell Carcinoma") pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
Renal Cell Carcinoma: Navigating a Maze of Choices
 Renal Cell Carcinoma: Navigating a Maze of Choices Sumanta Kumar Pal, M.D. Associate Professor Department of Medical Oncology & Experimental Therapeutics Co-Director, Kidney Cancer Program City of Hope
Renal Cell Carcinoma: Navigating a Maze of Choices Sumanta Kumar Pal, M.D. Associate Professor Department of Medical Oncology & Experimental Therapeutics Co-Director, Kidney Cancer Program City of Hope
Immunotherapy for the Treatment of Cancer
 Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab.
 CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab. perc noted that patients with brain metastases were excluded from the CheckMate
CheckMate 025, as patients may derive a benefit, based on the opinion of the CGP and the mechanism of action of nivolumab. perc noted that patients with brain metastases were excluded from the CheckMate
New strategies and future of target therapy in advanced kidney cancer
 New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro. Immune checkpoint inhibition in DLBCL
 Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Checkpointinhibitoren in der Uro-Onkologie. Carsten Grüllich
 Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Immunotherapy for Genitourinary Cancers
 Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Sequential Therapy in Renal Cell Carcinoma*
 Sequential Therapy in Renal Cell Carcinoma* Bernard Escudier, MD, Marine Gross Goupil, MD, Christophe Massard, MD, and Karim Fizazi, MD, PhD Because of the recent approval of several drugs for the treatment
Sequential Therapy in Renal Cell Carcinoma* Bernard Escudier, MD, Marine Gross Goupil, MD, Christophe Massard, MD, and Karim Fizazi, MD, PhD Because of the recent approval of several drugs for the treatment
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
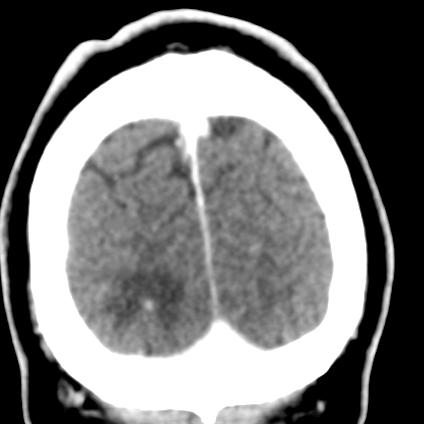
Brain mets under I.O.
 Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016
 for Metastatic Renal Cell Carcinoma September 1, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients
 A Phase II Study of With or Without Bevacizumab vs in Untreated Metastatic Renal Cell Carcinoma Patients David McDermott, 1 Michael Atkins, 2 Robert Motzer, 3 Brian Rini, 4 Bernard Escudier, 5 Lawrence
A Phase II Study of With or Without Bevacizumab vs in Untreated Metastatic Renal Cell Carcinoma Patients David McDermott, 1 Michael Atkins, 2 Robert Motzer, 3 Brian Rini, 4 Bernard Escudier, 5 Lawrence
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care
 vs standard of care") A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce
 in the elderly ( 65y): Position of a SIOG Taskforce") Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce Medical treatment of metastatic RCC in the elderly ( 65y): Members of the SIOG Taskforce
Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce Medical treatment of metastatic RCC in the elderly ( 65y): Members of the SIOG Taskforce
Primary Care Management of the Kidney Cancer Patient
 Primary Care Management of the Kidney Cancer Patient Elaine Lam, MD Mountain States Cancer Conference 2016 November 5, 2016 Learning Objectives 1. Understand the mechanisms of action of currently approved
Primary Care Management of the Kidney Cancer Patient Elaine Lam, MD Mountain States Cancer Conference 2016 November 5, 2016 Learning Objectives 1. Understand the mechanisms of action of currently approved
Media Release. Basel, 6 th February 2018
 Media Release Basel, 6 th February 2018 Phase III IMmotion151 study showed Roche's TECENTRIQ (atezolizumab) and Avastin (bevacizumab) reduced the risk of disease worsening or death by 26 percent in certain
Media Release Basel, 6 th February 2018 Phase III IMmotion151 study showed Roche's TECENTRIQ (atezolizumab) and Avastin (bevacizumab) reduced the risk of disease worsening or death by 26 percent in certain
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents
 in the Era of Targeted Agents") Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Kidney Cancer Session
 New Frontiers in Urologic Oncology September 12 th, 2015 Kidney Cancer Session Moderator: Philippe E. Spiess, M.D. Invited Faculty Members: Wade J. Sexton, MD Jeremiah J. Morrissey, PhD Agenda for Session
New Frontiers in Urologic Oncology September 12 th, 2015 Kidney Cancer Session Moderator: Philippe E. Spiess, M.D. Invited Faculty Members: Wade J. Sexton, MD Jeremiah J. Morrissey, PhD Agenda for Session
Targeted Therapy in Advanced Renal Cell Carcinoma
 Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
Advances in Systemic Therapy Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016
 Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016") Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia
 Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia New target, new agent (James Brugarolas) Atezolizumab + Bevacizumab and PD-L1
Carcinoma renale metastatico: cambia la pratica clinica? Camillo Porta Fondazione I.R.C.C.S. Policlinico San Matteo, Pavia New target, new agent (James Brugarolas) Atezolizumab + Bevacizumab and PD-L1
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Metastatic Renal Cancer Medical Treatment
 Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use
 Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 ipilimumab aligned with patient values. Although few patients had direct experience using this combination agent, patients indicated that side effects associated with nivolumab plus ipilimumab were few
ipilimumab aligned with patient values. Although few patients had direct experience using this combination agent, patients indicated that side effects associated with nivolumab plus ipilimumab were few
Axitinib in renal cell carcinoma: now what do we do?
 Renal Cell Carcinoma Axitinib in renal cell carcinoma: now what do we do? Ian D. Davis Monash University Eastern Health Clinical School, Level 2, Box Hill, Victoria 3128, Australia Correspondence to: Ian
Renal Cell Carcinoma Axitinib in renal cell carcinoma: now what do we do? Ian D. Davis Monash University Eastern Health Clinical School, Level 2, Box Hill, Victoria 3128, Australia Correspondence to: Ian
Clinical Biomarker in Kidney Cancer. Maria Nirvana Formiga, M.D., Ph.D.
 Clinical Biomarker in Kidney Cancer Maria Nirvana Formiga, M.D., Ph.D. Disclosures I am on the Speaker s Bureau with Pfizer and Bayer Clinical trials of BMS and Pfizer Kidney Cancer 70% new cases in developed
Clinical Biomarker in Kidney Cancer Maria Nirvana Formiga, M.D., Ph.D. Disclosures I am on the Speaker s Bureau with Pfizer and Bayer Clinical trials of BMS and Pfizer Kidney Cancer 70% new cases in developed
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain
 New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA. Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA
 UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients
 A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients Viktor Grünwald, 1 David McDermott, 2 Michael Atkins, 3 Robert Motzer, 4
A Phase II Study of Atezolizumab With or Without Bevacizumab vs Sunitinib in Untreated Metastatic Renal Cell Carcinoma Patients Viktor Grünwald, 1 David McDermott, 2 Michael Atkins, 3 Robert Motzer, 4
Pieter de Mulder Lecture
 Pieter de Mulder Lecture From cytokines to targeted therapies to immunotherapy: 30 years of progress in advanced RCC Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome,
Pieter de Mulder Lecture From cytokines to targeted therapies to immunotherapy: 30 years of progress in advanced RCC Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome,
Advances in the Treatment of Renal Cell Carcinoma
 Advances in the Treatment of Renal Cell Carcinoma Developed in collaboration Learning Objectives Upon completion, participants should be able to: Identify patients with metastatic renal cell carcinoma
Advances in the Treatment of Renal Cell Carcinoma Developed in collaboration Learning Objectives Upon completion, participants should be able to: Identify patients with metastatic renal cell carcinoma
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Alternativas de Futuro en Cáncer Renal Enrique Grande
 Alternativas de Futuro en Cáncer Renal Enrique Grande Hospital Ramón y Cajal de Madrid The ncreasingly Challenging Field of mrcc Sorafenib (US 2005, EU 2006) 3,4 Sunitinib (US & EU 2006) 3,4 Early 1940s:
Alternativas de Futuro en Cáncer Renal Enrique Grande Hospital Ramón y Cajal de Madrid The ncreasingly Challenging Field of mrcc Sorafenib (US 2005, EU 2006) 3,4 Sunitinib (US & EU 2006) 3,4 Early 1940s:
CLINICAL POLICY Department: Medical Management Document Name: Inlyta Reference Number: NH.PHAR.100 Effective Date: 05/12
 Page: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Page: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
Sergio Bracarda MD. Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy
 San Donato Hospital Arezzo, Italy") Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies
 Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment
 Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Renal Cell Carcinoma: Status of Medical and Surgical Therapy. Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation
 Renal Cell Carcinoma: Status of Medical and Surgical Therapy Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation Metastatic Renal Cell Carcinoma: Evolution of Current Therapeutic Approaches
Renal Cell Carcinoma: Status of Medical and Surgical Therapy Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation Metastatic Renal Cell Carcinoma: Evolution of Current Therapeutic Approaches
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015
 Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Characterization of Patients with Poor-
 Characterization of Patients with Poor- Risk Metastatic Renal Cell Carcinoma Hamieh L 1 *, McKay RR 1 *, Lin X 2, Simantov R 2, Choueiri TK 1 *Equal contributions 1 Dana-Farber Cancer Institute, Boston,
Characterization of Patients with Poor- Risk Metastatic Renal Cell Carcinoma Hamieh L 1 *, McKay RR 1 *, Lin X 2, Simantov R 2, Choueiri TK 1 *Equal contributions 1 Dana-Farber Cancer Institute, Boston,
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
When to Treat Beyond Progression with Systemic Therapies? Manuela Schmidinger Medical University of Vienna, Austria
 When to Treat Beyond Progression with Systemic Therapies? Manuela Schmidinger Medical University of Vienna, Austria Is Treatment Beyond Progression a Valid Strategy? 1) NO YES? Is Treatment Beyond Progression
When to Treat Beyond Progression with Systemic Therapies? Manuela Schmidinger Medical University of Vienna, Austria Is Treatment Beyond Progression a Valid Strategy? 1) NO YES? Is Treatment Beyond Progression
ONCOS-102 in melanoma Dr. Alexander Shoushtari. 4. ONCOS-102 in mesothelioma 5. Summary & closing
 ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
Immunotherapy for Genitourinary Cancers. Douglas McNeel, MD PhD Professor of Medicine University of Wisconsin Carbone Cancer Center Madison, WI
 Immunotherapy for Genitourinary Cancers Douglas McNeel, MD PhD Professor of Medicine University of Wisconsin Carbone Cancer Center Madison, WI Disclosures Madison Vaccines Inc co-founder, IP, consultant
Immunotherapy for Genitourinary Cancers Douglas McNeel, MD PhD Professor of Medicine University of Wisconsin Carbone Cancer Center Madison, WI Disclosures Madison Vaccines Inc co-founder, IP, consultant
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage