Immunohistochemistry on Limited Tissue Samples: Do s and Don ts
|
|
|
- Walter Quinn
- 6 years ago
- Views:
Transcription

1 Disclosures Immunohistochemistry on Limited Tissue Samples: Do s and Don ts I fretted over this... Andrew M Bellizzi, M.D. Department of Pathology University of Iowa Hospitals and Clinics andrew bellizzi@uiowa.edu Disclosures Last night I was sleepless... in Seattle 1

2 Disclosures Otherwise, I have nothing to disclose Goals To make an accurate, specific diagnosis with as few immunostains as possible To provide (prognostic and) predictive info To avoid less useful immunostains To perform clinically valid immunohistochemistry To triage tissue for other ancillary studies Outline Competing interests: other ancillary studies Technical aspects of immunocytochemistry Enemies of the state: non specific immunos Next generation immunohistochemistry Favorite markers/panels Carcinoma of unknown origin Lung adenocarcinoma vs. squamous cell carcinoma Mesothelioma Solid pancreatic tumors Sarcoma Lymphoma 2

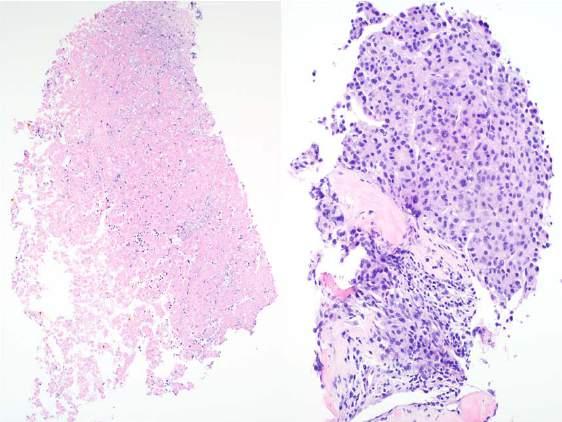
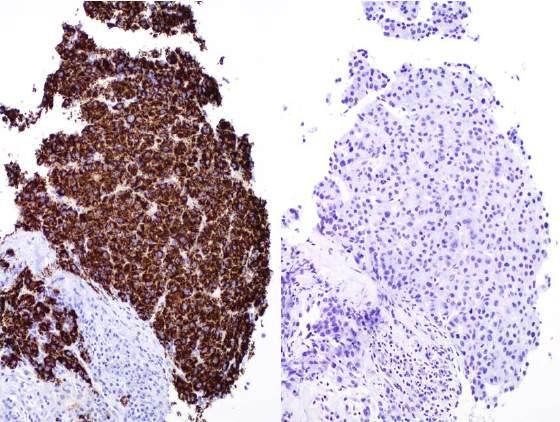
3 63 year old woman with liver, lung, and adrenal masses; presumed lung primary based on FNA of liver lesion 4 months prior; EGFR/ALK/ROS1 wild type; progression on platinumbased chemotherapy; biopsy for cancer mutation profiling TTF 1 3
4 Taher, Thanks for raising this issue in the setting of our increasingly engaging in this era of personalized medicine. This was my case, as staff pathologist. I ordered the TTF 1 because I believed it was necessary to the diagnosis. In fact, in this case, it was negative. I had already ordered it BEFORE your call to the hot seat. So, there was no communication breakdown. I was aware of the prior diagnosis. I read your note while I was evaluating the glass slides. I was aware that the primary driver of this biopsy was to perform NGS. There was actually much more tumor present in the immunostained slide than on the initial H&E, fortunately. I was pessimistic of the prospects for NGS success based on the initial H&E. I was acutely sensitive of the purpose of this biopsy, which is why I limited myself to ONE critical immunostain. Taking one 5 micron section off the tissue block (for IHC) DOES NOT compromise the ability to perform molecular, especially if the sections for molecular are taken simultaneously. The anatomic pathologist is first and foremost responsible that a correct diagnosis is rendered. So, in this case I have to reasonably reassure myself that this is, in fact, metastatic lung adenocarcinoma. In this instance, both purposes should be served. Your note on the consult sheet WAS CRITICAL. If you hadn't made this comment, I would have performed a more extensive immunopanel. As always, communication is key. I would be happy to discuss this issue at greater length or in person. Best, Andrew Tension Between Diagnosis and Predictive Testing is Increasing Use of IHC in pre op lung cytologic specimens Study Period Diagnosis of AdCA IHC Frequency >600% increase in IHC utilization Diagnosis of SCC IHC Frequency % (22/156) 11% (5/46) % (134/156) 89% (41/46) Ocque R, Tochigi N, Ohori P, Dacic S. Am J Clin Pathol 2011;136:81 7. Ancillary Tests in FNA/Small Biopsy Tumor Type Standard Applications Extended Applications Breast Cancer ER, PR, HER2 Esophagus/Gastric AdCA HER2 Oropharygeal SCC and p16 NGS or HPV ISH Head and Neck SCC of Occult Origin Lung Adenocarcinoma EGFR, ALK ROS1, PD L1 RET, MET, LKB1, PTEN Multigene Colon Cancer KRAS, NRAS, BRAF, MSI PIK3CA, PTEN, EGFR CN Mesothelioma p16 FISH Thyroid Aspirate BRAF, KRAS Pancreatic Cyst Aspirate Cyst fluid analysis KRAS, DNA content Panel Melanoma BRAF KIT Sarcoma FISH or RT/PCR (for specific diagnosis) Hematolymphoid Flow cytometry, IgH/TCR gene rearrangements, FISH (for diagnosis or prognosis) 4





5 Aisner DL, Sams SB. Diagn Cytopathol 2012;40: What s Old is New Gailey MP, et al. Cancer Cytopathol ;30 9. Knoepp SM, Roh MH. Cancer Cytopathol : Snow AM, et al. BMC Clin Pathol ;30. Hunt JL, et al. Diagn Cytopathol 1998;18:




6 Lessons Learned Do consider every biopsy of a tumor to be a potential molecular diagnostics specimen Do consider cutting unstained sections up front for molecular testing, if ordering IHC Do communicate with your clinical colleagues about priorities for the specimen Do not give up hope if you ve exhausted a specimen: you may be able to recover DNA from routinely processed material FNA of a Mural Based Gastric Mass Cell block KIT KIT and DOG1 Intensity by FNA Method DOG1 KIT on subsequent resection Cell blocks of 52 GIST, 24 LMS, 10 other No significant difference in number of cells in EUS vs CT cellblocks EUS FNA: FNA collected into CytoLyt (methanol based fixative) CT FNA: FNA collected into RPMI plasma and thrombin added to produce cell block, fixed in 10% formalin, processed for paraffin embedding Hwang DG, et al. Am J Clin Pathol 2011;135:



7 The staining of cytologic preparations with a battery of antibodies to the various cell components or products is very costly and rarely rewarding... The results of ICC vary according to the batch of antibodies and the technical skills of the laboratories, the interpretation of the results is not always easy, and the problem with borderline positive stains is often perplexing. We This Might Be So... Surgical Pathologists order IHC on FFPE tissue Cytopathologists may request IHC on: Direct Smears Air dried Unfixed Post fixed Alcohol fixed Unstained Stained Destained Cytospins Monolayer Preparations Cell Blocks Koss LG. The future of cytology. The Wachtel lecture for Acta Cytol 1990;34:1 9. Cell Block Mandelbaum FS. Diagnosis of malignant tumors by paraffin sections of centrifuged exudates. J Lab Clin Med. 1917; 2:580. Cell Blocks: Advantages and Disadvantages Advantages Processed similarly to surgical pathology material Facilitates multiple sections Easy to store Disadvantages Not amenable to on site adequacy assessment May be pauci/acellular 10.6% of 246 lung/thoracic FNA s (Rafael OC, et al 2014) 57% of 76 consecutive EBUS FNA s (Knoepp, Roh 2013) 7
8 Performance in Other Cytology Specimen Types Potential Sources of Pre Analytic Variation Delay in fixation Type, concentration, ph of fixative Fixation time Tissue Processing Paraffin impregnation (paraffin melting point) Block/slide storage Engel KB, Moore HM. Arch Pathol Lab Med 2011;135: Potential Sources of Analytic Variation Antigen retrieval Yes or no Enzyme or heat induced For heat induced: buffer, ph, heat source Primary antibody dilution Duration of primary antibody incubation Detection chemistry (ABC, polymer based) Optimization and Validation Optimization: determination of provisional assay conditions, which is most often involves staining a single case or small number of cases at varying assay conditions Validation: testing and appropriate tissue set to determine analytic sensitivity and specificity, to reasonably assure that the test performs as expected Goldsmith J. CAP Today Q&A. July 13, Goldsmith J. CAP Today Q&A. July 13, Fitzgibbons PL, et al. Arch Pathol Lab Med 2014;138:
9 Recommendation Tissue should be fixed in 10% neutral ph, phosphate buffered formalin for a minimum of 8 hours. Non formalin based fixatives and or alternative fixation methodologies are strongly discouraged in regard to IHC, in large part because performance data are limited and extrapolation from formalin fixed data is unreliable. Goldstein NS, et al. Appl Immunohistochem Mol Morphol 2007;15: Recommendation Antigen retrieval (AR) is presumed to restore the antigenicity after the formalin fixation. The parameters of an AR protocol must be balanced to match the unique length and type of tissue fixation of the individual laboratory and the characteristics of the individual antibody. Antigen Retrieval Air dried smears theoretically should require (less or) no AR Alcohol fixed smears (coagulation, rather than cross linking, fixation) theoretically should require (less or) no AR Over AR produces high background staining and strong edge staining Under AR produces false negative IHC 9

10 Recommendations Laboratories must validate all IHC tests before placing them into clinical service For initial analytic validation of nonpredictive factor assays, laboratories should test a minimum of 10 positive and 10 negative tissues Fitzgibbons PL, et al. Arch Pathol Lab Med 2014;138: Recommendations If IHC is regularly done on cytologic specimens that are not processed in the same manner as the tissues used for assay validation (eg, alcohol fixed cell blocks, air dried smears, formalin postfixed specimens), laboratories should test a sufficient number of such cases to ensure that assays consistently achieve expected results... The strength of evidence was inadequate to address the criteria and number of samples needed for validation with cytology specimens. If an assay has not been fully validated on cytologic specimens, laboratories may include a disclaimer in their report that results should be interpreted with caution. Controls Unless the laboratory has a large bank of similarly prepared cytology material for positive and negative IC controls (nonformalin fixed cytology specimen by the exact same preparation method as the current sample being tested), then criteria for having proper controls is not met and any interpretation of IC results should be suspect. Fowler LJ, Lachar WA. Arch Pathol Lab Med 2008;132:
 Knoepp SM, Roh MH. Cancer Cytopathol 2013. 121:120 8.")
11 Controls In our experience, unstained direct smears in high quantities can be prepared using centrifuged cellular material for effusion specimens and these can be used for positive control ICC reactions. Multiplexing Double staining, triple staining, etc. Performing a second IHC on a previously IHCstained slide (if negative) Knoepp SM, Roh MH. Cancer Cytopathol : Dabbs DJ, Wang X. Diagn Cytopathol 1998;18: Lessons Learned Do perform ICC on cell blocks, if possible Do examine cell block technique if ICC performing suboptimally Do consider including cytology specimens in clinical IHC validations Do include similarly processed positive controls on ICC runs Do not perform ICC on other cytology specimen types unless the procedure has been specifically optimized for them (esp. antibody dilution, antigen retrieval) 11
 Ovary 98 Endometrium 90 Cervix 53 Pancreas 82 Gallbladder 63 Lung 56 Cholangiocarcinoma 51 Head")
12 Myths CA125 is specific for Müllerian origin CA19 9 is specific for pancreatic origin CK19 is specific for pancreatobiliary origin MOC 31 is an adenocarcinoma marker RCC is specific for renal origin Vimentin is specific for sarcoma CA125 Expression Tumor Site (adenocarcinoma unless otherwise noted) Ovary 98 Endometrium 90 Cervix 53 Pancreas 82 Gallbladder 63 Lung 56 Cholangiocarcinoma 51 Head and Neck (SCC) 40 Thyroid 39 Breast 27 Lung (SCC) 23 Melanoma, lymphoma, sarcoma, 0 neuroendocrine, hepatocellular % Positive (at 10% cells staining with moderate intensity) Gremel G, et al. Histopathology 2014;64: CA19 9 Expression Tumor Site (n) % Positive (adenocarcinoma unless otherwise noted) Pancreas (26) 85 Breast, ductal (119) 48 Breast, lobular (10) 10 Lung (35) 69 Stomach (39) 56 Colon (25) 76 Ovary (29) 41 Kidney (45) 27 Mesothelioma <<1 Kaufmann O, et al. Histopathology 1996;29:
 91")

 41 Mesothelioma (10) 0 Hepatocellular carcinoma (10) 20 Neuroendocrine carcinoma")
 100 Neuroendocrine tumor, pancreas (5) 80 Savage EC, Gailey MP, Bellizzi AM.")
 Hep Par 1 (+)/ MOC 31 ( ) HCC Hep")
13 CK19 Expression Tumor Site (adenocarcinoma unless otherwise noted) Cholangiocarcinoma 100 Pancreas 100 Gallbladder 100 Lung 100 Ovary 98 Breast 98 Colon 98 Stomach 98 Urothelial 95 Cervix 93 Lung (SCC) 91 Melanoma, lymphoma, hepatocellular 0 % Positive (at 10% cells staining with moderate intensity) Gremel G, et al. Histopathology 2014;64: MOC 31 MOC 31 Expression Dx Algorithm: Poorly Differentiated Carcinoma in the Liver Tumor Type (n) % Positive Squamous cell carcinoma (110) 41 Mesothelioma (10) 0 Hepatocellular carcinoma (10) 20 Neuroendocrine carcinoma (5) 60 Lung adenocarcinoma (6) 100 Colon adenocarcinoma (6) 100 Urothelial carcinoma (11) 55 Neuroendocrine tumor, midgut (5) 100 Neuroendocrine tumor, pancreas (5) 80 Savage EC, Gailey MP, Bellizzi AM. Abstract at 2014 USCAP Annual Meeting. HCC vs. ICC vs. Metastasis Perform Hep Par 1, MOC 31 (alternatively Arginase 1, Claudin 4) Hep Par 1 (+)/ MOC 31 ( ) HCC Hep Par 1 ( )/ MOC 31 (+) ICC or Metastasis IHC menu for this application: HCC Markers: Hep Par 1 GPC3 pcea/cd10 (canalicular) Arginase 1 Non HCC Markers: MOC 31 Claudin 4 13
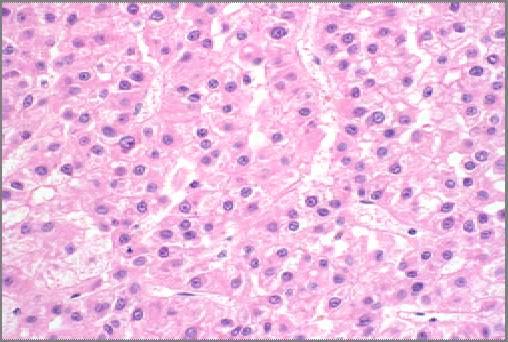
14 Hepatocellular carcinoma 73 year old man with liver lesion, subtotally necrotic Hep Par 1 MOC 31 Large right retroperitoneal tumor 14
 PAX2 (% Positive)")


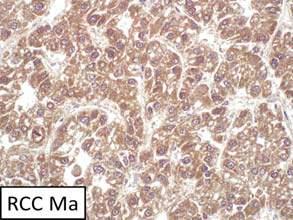
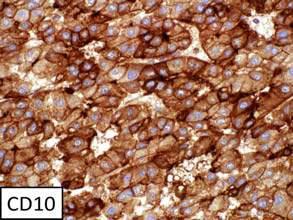
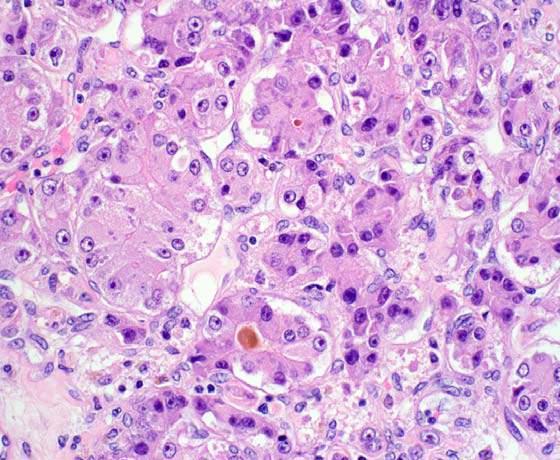
15 13 cm tumor spanning the kidney and adrenal, expresses CD10, melan A, and inhibin PAX8 vs PAX2 Expression Tumor Type PAX8 (% Positive) PAX2 (% Positive) Clear cell Papillary Chromophobe Collecting duct Serous Endometrioid Clear cell Transitional Thyroid 91 0 PAX8 Ozcan A, et al. Am J Surg Pathol 2011;35: Ozcan A, et al. Arch Pathol Lab Med 2012;136: Laury AR, et al. Am J Surg Pathol 2011;35:

 (n=29: p16) Endocervical (n=26: ER, vim,")
 p16 97% (any staining)")
 96% (100% cells stain) McCluggage WG,")



 Do not order CA125, CA19 9, RCC (No")
16 Melanoma Vimentin Burkitt lymphoma Vimentin Endometrioid Endometrial vs. Endocervical AdCA Endometrioid Endometrial (n=30: ER, vim, CEA) (n=29: p16) Endocervical (n=26: ER, vim, CEA) (n=23: p16) ER 93% 38% Vimentin 97% 8% CEA 70% 96% (usually in squamous foci) p16 97% (any staining) 27% ( 50% cells stain) 10% (100% cells stain) 96% (any staining) 96% (100% cells stain) McCluggage WG, et al. Int J Gynecol Pathol Jan;21(1):11 5. McCluggage WG, Jenkins D. Int J Gynecol Pathol Jul;22(3): Results of immunopanel favor endometrial origin Lessons Learned Uterine cervical mass ER, PR Do not extrapolate the results of differentialspecific markers beyond the differential (e.g., CK19, MOC 31) Do not order CA125, CA19 9, RCC (No No Never) Vimentin??? If you must... sparingly... But please don t tell me that you did... Vimentin p16 16




17 Next Generation Immunohistochemistry Gene Expression Profiling Comparing Urothelial, Kidney, and Prostate Cancer Mine developmental biology and molecular genetic literature to find: Lineage restricted transcription factors Markers identified by gene expression profiling Protein correlates of molecular genetic events Bottom line: our markers keep getting better Higgins JPT, et al. Am J Surg Pathol May;31(5): Historically, diagnostic armamentarium geared toward cytoplasmic or membranous differentiation markers; reduced sensitivity in poorly differentiated tumors Primacy of lineage restricted transcription factors Breast cancer Mammaglobin GCDFP 15 GATA 3: highly expressed, regardless of differentiation 17
18 Regional Differential Diagnosis Brain (carcinoma, melanoma, lymphoma, glioma) Lymph node (lymphoma vs. other) Supraclavicular (anything), Periaortic (germ cell tumor) Mediastinum (lung, lung, lung, thymic [KIT,CD5], germ cell) Visceral organ (1 vs metastasis) Lung (AdCA vs SCC vs metastasis) Liver (HCC vs pancreatobiliary vs other) Pleural effusion (AdCA vs mesothelioma) Peritoneum/Ovary (1 surface epithelial vs metastatic GI) Retroperitoneum (well and dedifferentiated liposarcoma) Somatic soft tissue (sarcoma vs. metastasis) Bone (blastic prostate, breast; lytic RCC, thyroid; mixed lung) Diagnosis of Broad Tumor Class Carcinoma (broad spectrum keratins, EMA [aka MUC1]) Melanoma (S 100, SOX10, melan A, HMB 45, MiTF, BRAF) Lymphoma (CD45; CD43, CD79a, MUM1, ALK1, CD30 if LCA ) Sarcoma (CD34, MDM2/CDK4 DDLPS, add l based on morph.) Mesothelioma (WT 1, calretinin, CK5/6, D2 40) Germ cell tumor (SALL4, PLAP) Non epithelial neuroendocrine neoplasm (CG, SYN) Adenocarcinoma (gland forming/ mucin producing) see next algorithm SCC CK7 var. GATA3? Diagnosis of Carcinoma Type UC CK7/CK20+ GATA3+ Squamotransitional (p63, p40, CK5/6+) Carcinoma (cohesive, keratin and/or EMA+) HCC Hep Par 1 + GPC3+ Large polygonal cell (CK7/CK20 ) RCC PAX8+ AdCC Mel A+ Inhibin+ SYN+ SF1+ Neuroendocrine (CG and/or SYN+) NET Ki 67 20% NEC Ki 67 >20% Which Screening Keratin Should I Use? Clone AE1/AE3 X X X X X X X X X X X X OSCAR X X X X MAK 6 X X X X X X MNF116 X X X X CAM5.2 X X KL1 X X X X X X X X X X X 34βE12 X X X X In general, any of these are acceptable It s not the number of keratins, per se, but rather the affinity (e.g., CAM5.2 vs AE1/AE3 in HCC/RCC) Stratified epithelia: K1 6, 9 17 Simple epithelia: 7, 8, 18, 19, Ordóñez NG. Hum Pathol Jul;44(7):
19 Coordinate Expression of CK7/CK20 Site (tumor) CK7 CK20 Prostate, HCC, AdCC, RCC - - Lung, Breast, Müllerian, Pancreatobiliary (PB), Upper GI (UGI) + - Bladder, UGI, PB, Mucinous Ovarian, Colon (esp. Rectum), Occ. Lung + + Colon, Merkel cell, Occ. UGI - + Cancer Epidemiology and Morphology Based Site of Origin Generator Most Common Primary Sites in Men (Rank Order) Prostate (25%) (AdCA) Lung (15%) (AdCA, SCC, NEC) Colorectum (10%) (AdCA) Morphology Characteristic nuclear features regardless of Gleason grade: monomorphous and prominent nucleoli Most Common Primary Sites in Women (Rank Order) Breast (26%) (AdCA) Variable (AdCA) Lung (14%) (AdCA, SCC, NEC) Characteristic cytoarchitectural features: tall, dark, and dirty Colorectum (10%) (AdCA) Morphology Variable Variable (AdCA) Characteristic cytoarchitectural features: tall, dark, and dirty IHC to Assign AdCA Site of Origin: Ranked from Most to Least Ordered (2011) CDX2 (enteric differentiation) TTF 1 (lung, thyroid) ER and PR (breast, Müllerian) PAX8 (kidney, Müllerian, thyroid) Transcription factors in bold p53and WT 1 (serous carcinoma, latter also exp. by mesothelioma) Napsin A (lung, papillary RCC) PSA and PSAP (prostate) GCDFP 15 and mammaglobin (breast) Thyroglobulin (thyroid) GATA 3 (breast; also urothelial) NKX3.1 (prostate) Lung Adenocarcinoma vs Squamous Cell Carcinoma Marker AdCA (% positive) CK TTF p CK5/ SCC (% positive) p63, CK5/6 have a specificity problem TTF 1 has a sensitivity problem Ocque R, Tochigi N, Ohori P, Dacic S. Am J Clin Pathol 2011;136:

20 p40 (ΔNp63) Napsin A Marker AdCA (% positive) SCC (% positive) p p40 3* * Each 1 5% cells staining TTF 1+/p40 AdCA TTF 1 /p40 AdCA Bishop TTF 1 /p40+ JA, et al. Mod Pathol 2012;25: SCC Large Cell Lymphoma (% positive) Marker Lung AdCA (% positive) Napsin A 87 (n=303) SCC (% positive) 3 (n=200) TTF 1 64 (n=94) 2 (n=94) Lower rate of TTF 1+ AdCA than literature (75 85%) Napsin A frequently expressed by RCC (esp. papillary) and clear cell carcinoma Turner BM, et al. Arch Pathol Lab Med 2012;136: Soft Tissue: IHC to Assign Lineage Line of Differentiation Characteristic Historically Useful Immunostains Adipocytic Fatty S 100 Fibroblastic/myofibroblastic Spindled; light pink SMA, CD34, ALK So called fibrohistiocytic Shrinking group (e.g., TSGCT) None especially Smooth muscle Spindled; brightly eosinophilic SMA, desmin Pericytic Spindled; circumferential SMA perivascular growth pattern Skeletal muscle Rhabdomyo(sarco)ma Desmin, myogenin Vascular Vascular channels CD34, CD31, Factor VIII Chondro osseous Cartilage, osteoid S 100 Interstitial cell of Cajal GIST KIT, CD34 Nerve sheath Spindle cell; wavy nuclei S 100, GFAP Uncertain Distinctive tumor types (e.g., synovial sarcoma, epithelioid sarcoma, PEComa) Keratins, EMA, S 100, (TFE3, HMB 45, WT 1) Undifferentiated/unclassified Formerly MFH Diagnosis of exclusion Name Beta catenin Soft Tissue Markers Validated at U of Iowa in Last 3 Years MDM2 and CDK4 (MDM2 FISH) TLE1 MUC4 ERG STAT6 HHV8 Diagnostic Application Desmoid fibromatosis (70%), solid pseudopapillary neoplasm, pancreatoblastoma; hepatoblastoma (50 90%), fetal type lung AdCA, colonic adenoma/adca Well and dedifferentiated liposarcoma Synovial sarcoma; Pitfalls: weaker staining in other sarcomas, frequently positive in carcinomas Low grade fibromyxoid sarcoma, sclerosing epithelioid fibrosarcoma (75%); also broadly expressed by epithelia Vascular tumors,prostate cancer (50%); occ. myeloid leukemias and Ewing sarcoma (10%) Solitary fibrous tumor (NAB2 STAT6 translocation) Kaposi sarcoma, primary effusion lymphoma, multicentric Castleman disease, plasmablastic lymphoma arising in plasmablastic lymphoma 20
, malignant rhabdoid tumors of soft tissue, kidney, CNS (>95%),")
 Burkitt lymphoma DLBCL c Myc c Myc Advantages of ICC over Flow Cytometry Hodgkin lymphoma Burkitt lymphoma vs DLBCL, GC Type BL: c Myc+, Bcl 2 DLBCL: c")
 CD10 Bcl 6 CD5 + CD43 Cyclin D1 Bcl 2 Occ. (30%) Var.")
; keratins to highlight lymphoepithelial lesions Ki 67 proliferation index >40 60% associated with poor prognosis; rarely CD5 or cyclin D1 Follicular")
21 Name Soft Tissue Markers Validated at U of Iowa in Last 3 Years Diagnostic Application SOX10 INI1 Melanoma, MPNST (50%), clear cell sarcoma, myoepithelial differentiation; superior in sensitivity and specificity to S 100 Epithelioid sarcoma (90%), malignant rhabdoid tumors of soft tissue, kidney, CNS (>95%), medullary carcinoma of the kidney, other INI1 deficient tumors (some epithelioid MPNST, myoepithelial CA of soft tissue, extraskeletal myxoid chondrosarc.) Burkitt lymphoma DLBCL c Myc c Myc Advantages of ICC over Flow Cytometry Hodgkin lymphoma Burkitt lymphoma vs DLBCL, GC Type BL: c Myc+, Bcl 2 DLBCL: c Myc, Bcl 2+ or CD20 Tumor Type CD79a PAX5 Tumors composed of small cells Extranodal marginal zone lymphoma of mucosa associated lymphoid tissues (MALT lymphoma) CD10 Bcl 6 CD5 + CD43 Cyclin D1 Bcl 2 Occ. (30%) Var. Mantle cell lymphoma Other Useful Markers/Notes Kappa/lambda light chain restriction (occ.); keratins to highlight lymphoepithelial lesions Ki 67 proliferation index >40 60% associated with poor prognosis; rarely CD5 or cyclin D1 Follicular lymphoma Higher grade tumors more likely to show aberrant IHC (e.g., CD10 or CD43+) Chronic lymphocytic leukemia/small lymphocytic lymphoma CD23+ 21
 Bcl 6+ (60 90%) CD5 CD43 Cyclin D1 Bcl 2 Other Useful Markers/Notes Rare (10%) Occ. (25%) Var.")
22 Tumor Type CD20 CD79a PAX5 CD10 Bcl 6 Tumors composed of intermediate/large cells Diffuse large B cell lymphoma + CD10 Var. (30 60%) Bcl 6+ (60 90%) CD5 CD43 Cyclin D1 Bcl 2 Other Useful Markers/Notes Rare (10%) Occ. (25%) Var. MUM1 (35 65%) Burkitt lymphoma Plasmablastic lymphoma Granulocytic Sarcoma CD20/PAX5 CD79a+ (50 85%) Ki 67 proliferation index approaches 100%; TdT ; c Myc+; Bcl 2 occ. weak + EBV EBER (60 75%); CD45 ; MUM1/CD138/CD38+; EMA/CD30 var.; association with HIV + CD68/KIT/CD99/ CD34/TdT Var. Hematolymphoid Markers Validated at U of Iowa in Last 2 Years Name Tryptase CD163 c MYC SOX11 Diagnostic Application Mast cells Monocyte macrophage lineage marker (more specific than CD68) Burkitt lymphoma and c MYC activated DLBCL Mantle cell lymphoma (w/ emphasis on identifying CycD1 cases) B lymphoblastic lymphoma CD20 Var. (25 50%) CD79a/PAX5+ CD10+ (60%) Bcl 6 + (67%) + TdT (95%), CD34/CD99+; CD13/CD33 Occ. T lymphoblastic lymphoma CD20/ PAX5 CD79a Rare (5 10%) CD10 Var. Bcl 6 Var. + (90%) + TdT (95%), CD3/CD99+; CD4/CD8 double+ (70%); CD1a (67%); CD34 Var.; CD13/CD33 Occ. Lessons Learned Do perform a limited panel of IHC to assign tumor type/site of origin based on clinical and morphologic differential ( big 3 + appropriate next gen markers) Do not equate p63+ with SCC; do consider p40 Do consider using next gen markers to make specific sarcoma and lymphoma diagnoses Thank you!!! 22

23 U of Iowa Development Queue Name Diagnostic Application Androgen receptor Sebaceous CA, salivary duct CA, prostate CA; Pitfall: low specificity Arginase Hepatocellular CA; Pitfall: occ. stains AdCA Claudin 4 Broad spectrum epithelial marker not expressed by hepatocytes/meso s Clusterin Follicular dendritic cell sarcoma, ALCL, tenosynovial GCT, non ileal NET D2 40 Mesothelioma (inc. sarc.), lymphatic endothelium, seminoma, others Glutamine synthetase Focal nodular hyperplasia, BCAT HA, HCC vs. B9 liver: Pitfall: other CAs + Mammaglobin Breast CA;surrogate for ETV6 FISH in mammary analogue secretory CA NKI C3 (CD63) Cellular neurothekeoma; + in many other tumors inc. melanoma NUT NUT midline carcinoma (undifferentiated CA with abrupt keratinization) p40 (ΔNp63) Squamous cell carcinoma (superior spec. to p63); basal cells and myoep s SATB2 Colon AdCA; osteoblastic differentiation; rectal NET SDHB SDHB deficient GIST, paraganglioma/pheochromocytoma, other SMAD4 Pancreatic ductal AdCA (50% demonstrate loss); midgut NET (40%) SF1 Adrenal cortical neoplasms, sex cord stromal tumors Diagnosis of Broad Tumor Class Morphologic Boxes Cohesive, poorly cohesive, dyscohesive Spindle cell (sarcoma, sarcomatoid carcinoma) Pleomorphic (anything) Round cell (lymphoma, sarcoma) Epithelioid (carcinoma, melanoma) Pleomorphic and High Grade are NOT Synonymous Monomorphous or pleomorphic 23



")


 Maxwell")


24 Clear cell sarcoma Melanoma Monomorphous Pleomorphic CDX2 homogenous: LGI CDX2 heterogenous: UGI, mucinous ovarian, PB (20%) NET Site of Origin Algorithm CK20 diffuse, strong: LGI CK20 weak, patchy: UGI, mucinous ovarian, PB ( 40%) Maxwell JE, Sherman SK, Stashek KM, O Dorisio TM, Bellizzi AM, Howe JR. Surgery Dec;156(6):



 Transcription Factor")
 Merkel Cell")
")


 out of 38 examined Czeczok TW,")
:152A. 25")
25 Midgut NETs have a characteristic histologic appearance and nearly always express CDX2 Pancreatic NETs are of diverse histologic appearance and nearly always express ISL1 Merkel cell carcinoma CK20+/TTF 1 ( 90% Merkel cell carcinoma Small cell lung carcinoma TTF 1+/CK20 ( 90% SCLC, 45% visceral NEC) Transcription Factor Infidelity in NEC Frequently Expressed Transcription Factors (%) Merkel Cell Small Cell Extrapulmonary Carcinoma Lung Carcinoma Visceral NEC (n=40) (n=24) (n=19) FLI GATA Islet Myc PAX PLAG SATB SOX TTF NECs expressed a median of 8 TFs (range 0 18) out of 38 examined Czeczok TW, Gailey MP, Hornick JL, Bellizzi AM. Mod Pathol Feb;27(S2):152A. 25

 CAM5.")
:14 24.")
26 76 year old man with past tobacco use and asbestos exposure p/w pleural effusion; at thoracotomy diaphragm encased by nodular fibrous tissue; multiple plaque like areas throughout pleural cavity Pan keratin Calretinin, WT 1, CK5/6, MOC 31, Ber EP4, STAT6 Mesothelioma Marker Expression in Sarcomatoid Mesothelioma AE1/AE3 75% (18/24) CAM5.2 96% (23/24) MNF % (21/21) Calretinin 25% (6/24) WT 1 33% (8/24) D % (24/24) Chirieac LR, et al. Am J Cancer Res. 2011;1(1): All of these were prospectively dx d as pancreatic neuroendocrine tumor... only one of them is 26
 Solid pseudopapillary neoplasm (SPN) Acinar cell carcinoma (ACC)")
 ACC: 14/29 misdiagnosed, 5 as PNET, 5 as ductal AdCA (Sigel et al 13) Immunophenotype")


27 Cellular Epithelioid Neoplasms of the Pancreas Solid neoplasms composed predominantly of neoplastic elements with little stroma Pancreatic neuroendocrine tumor (PNET) Solid pseudopapillary neoplasm (SPN) Acinar cell carcinoma (ACC) Pancreatoblastoma (PB) On cytology: dyshesive, monomorphic SPN: 3 of 6 misdiagnosed as PNET (Bardales et al 04) ACC: 2 of 4 misdiagnosed as PNET (Stelow et al 06) ACC: 14/29 misdiagnosed, 5 as PNET, 5 as ductal AdCA (Sigel et al 13) Immunophenotype of Cellular Epithelioid Neoplasms of the Pancreas Broad Spectrum Keratins PNET SPN ACC PB + 70% + + Synaptophysin 95% 20 70% Rare cells 80% Chromogranin 90% Rare cells 80% Trypsin Rare cells 95% 95% β catenin <5% >95% 10% >90% BCAT Trypsin BCAT Trypsin Core biopsy from a 40 cm retroperitoneal tumor demonstrates undifferentiated neoplasm composed of sheets of epithelioid cells. After performing 17 immunostains a diagnosis of malignant neoplasm indeterminate for sarcoma, carcinoma, or lymphoma was rendered. 27







28 Most consistent with dedifferentiated liposarcoma Resection of similar case Well differentiated component MDM2, CDK4 Abrupt transition Dedifferentiated component Keratin and/or EMA positivity do not assure a diagnosis of carcinoma Potential Pitfall #1 28





29 Leiomyosarcoma Smooth muscle actin, desmin+ Keratin AE1/AE3+: keratin, EMA expression in 30 40% LMS 33 year old woman with 1 year h/o R hip pain; large SQ mass EMA+, AE1/AE3+, GATA 3 focal + p63, CK5/6, ER, PR, TTF 1, WT 1, CD31, S 100, HMB45 all Conclusion: Favor metastatic carcinoma,? breast or urothelial 29


 Conclusion: Favor")
30 INI1: absent expression epithelioid sarcoma, proximal type 63 year old man with increasing hip pain x 1 month; proximal femur lesion with soft tissue extension Undifferentiated Malignant Neoplasm with Osteoclast like Giant Cells Undifferentiated/anaplastic carcinoma Keratin AE1/AE3 CDX2, PAX8, TTF 1 Osteosarcoma SATB2 Leiomyosarcoma Desmin, SMA, caldesmon Keratin AE1/AE3+ (desmin, SMA ) Conclusion: Favor undifferentiated carcinoma 30
 Subsequent femoral head resection for pathologic fracture Abrupt transition from WD chondrosarcoma to undifferentiated neoplasm dedifferentiated chondrosarcoma")
 Epithelioid hemangioma Pseudomyogenic hemangioendothelioma Epithelioid")

31 Musculoskeletal radiologist sug. presence of chondroid matrix (MRI) Subsequent femoral head resection for pathologic fracture Abrupt transition from WD chondrosarcoma to undifferentiated neoplasm dedifferentiated chondrosarcoma Keratin Positive Soft Tissue Tumors EMA Positive Soft Tissue Tumors Chondroid lipoma Pleomorphic liposarcoma Desmoplastic fibroblastoma Solitary fibrous tumor Inflammatory myofibroblastic tumor Myxoinflammatory fibroblastic sarcoma Leiomyosarcoma Rhabdomyosarcoma Schwannoma (cross reactivity with GFAP) Epithelioid hemangioma Pseudomyogenic hemangioendothelioma Epithelioid hemangioendothelioma Angiosarcoma Gastrointestinal stromal tumor Sclerosing perineurioma Dermal nerve sheath myxoma Epithelioid MPNST Ectopic hamartomatous thymoma Ossifying fibromyxoid tumor Myoepithelial tumors of soft tissue Synovial sarcoma Epithelioid sarcoma Desmoplastic small round cell tumor Extrarenal rhabdoid tumor Undifferentiated/unclassified sarcoma Chondroblastoma Dedifferentiated chondrosarcoma Conventional osteosarcoma Ewing sarcoma Chordoma Adamantinoma Osteofibrous dysplasia Pleomorphic liposarcoma Calcifying aponeurotic fibroma Lipofibromatosis Dermatofibrosarcoma protuberans Solitary fibrous tumor Low grade fibromyxoid sarcoma Sclerosing epithelioid fibrosarcoma Leiomyosarcoma Pleomorphic rhabdomyosarcoma Epithelioid hemangioma Epithelioid hemangioendothelioma Angiosarcoma Neurofibroma Perineurioma Dermal nerve sheath myxoma Solitary circumscribed neuroma Meningioma Hybrid nerve sheath tumor Acral fibromyxoma Angiomatoid fibrous histiocytoma Myoepithelial tumors of soft tissue Synovial sarcoma Epithelioid sarcoma Desmoplastic small round cell tumor Extrarenal rhabdoid tumor Undifferentiated/unclassified sarcoma Conventional osteosarcoma Chordoma Epithelioid hemangioma Adamantinoma 31

 75%")
 0% (n=2) Stomach 20% (n=10) 25% (n=8)")
 0% (n=5) Kidney 65% (n=23) 66% (n=3)")
 0% (n=8) Unknown origin 22% (n=9) Total 43%")
:168 76.")
32 Dr. Bellizzi, what kind of S 100 positive carcinoma is this? 78 year old man p/w word finding difficulty: L temporal lobe mass Pan keratin S 100 S 100 Expression in Adenocarcinoma Primary Tumors Metastatic Tumors Salivary gland 80% (n=15) 75% (n=4) Lung 7% (n=27) 12% (n=25) Breast 60% (n=20) 62% (n=8) Esophagus 0% (n=8) 0% (n=2) Stomach 20% (n=10) 25% (n=8) Gallbladder 0% (n=1) 0% (n=1) Colorectum 25% (n=28) 23% (n=13) Pancreas 0% (n=8) 0% (n=5) Kidney 65% (n=23) 66% (n=3) Endometrium 78% (n=36) 64% (n=14) Ovary 84% (n=24) 87% (n=22) Prostate 0% (n=27) 0% (n=8) Unknown origin 22% (n=9) Total 43% (n=228) 39% (n=122) Herrera GA, et al. Am J Clin Pathol Feb;89(2): Melan A (A103) MiTF HMB 45 Conclusion: metastatic melanoma BRAF mutation testing: wild type 32
33 Keratin Positivity in Melanoma Primary cutaneous melanoma (n=62) Vimentin 100% 100% S % 95% NSE 87% 77% HMB45 97% 64% NKI C3 97% 95% Cytokeratin (KL1, CAM5.2, 35βH11) 0% 23% Achilles E, Schröder S. Pathologe Aug;15(4): Recurrent or metastatic melanoma (n=22) Keratin Positivity in Lymphoma Anaplastic large cell lymphoma (5/18; 28%) 1 13/866 (1.5%) hematolymphoid tumors in TMA 2 5/18 (28%) mantle cell lymphomas Otherwise, case reports and small series 1. Gustmann C, et al. Am J Pathol Jun;138(6): Adams H, et al. Pathol Res Pract. 2008;204(8): EMA positivity in Hematolymphoid Neoplasms Anaplastic large cell lymphoma (50 95%) Plasma cell neoplasms (most) Diffuse large B cell lymphoma TC/HR, ALK+, plasmablastic, primary effusion lymphoma T cell lymphoma (20%) Nodular lymphocyte predominant Hodgkin (L&H) Follicular dendritic cell sarcoma (var.) Beware of LCA negative hematolymphoid neoplasms Potential Pitfall #2 33
34 LCA Negative Hematolymphoid Neoplasms Acute megakaryoblastic leukemia B cell acute lymphoblastic leukemia/lymphoma ALK positive large B cell lymphoma EMA+, CK /+; CD20, CD79a Plasmablastic lymphoma (EBER usually +) EMA+/ ; CD20, PAX5 Anaplastic large cell lymphoma, ALK positive (some) Classical Hodgkin lymphoma Follicular dendritic cell sarcoma 34
Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2 on all newly diagnosed cases
 GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2 on all newly diagnosed cases") Adrenal cortical carcinoma Inhibin Synap Melan-A Calretinin Vimentin Chromogr CK7 CK20 Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2
Adrenal cortical carcinoma Inhibin Synap Melan-A Calretinin Vimentin Chromogr CK7 CK20 Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
NEW IHC A n t i b o d i e s
 NEW IHC Antibodies TABLE OF CONTENTS NEW IHC ANTIBODIES from Cell Marque CITED1 (5H6).... 1 Claudin 7 (5D10F3).... 1 GATA1 (4F5).... 1 Transgelin (2A10C2).... 1 NEW IHC ANTIBODIES using RabMAb Technology
NEW IHC Antibodies TABLE OF CONTENTS NEW IHC ANTIBODIES from Cell Marque CITED1 (5H6).... 1 Claudin 7 (5D10F3).... 1 GATA1 (4F5).... 1 Transgelin (2A10C2).... 1 NEW IHC ANTIBODIES using RabMAb Technology
Disclosures. An update on ancillary techniques in the diagnosis of soft tissue tumors. Ancillary techniques. Introduction
 Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Disclosures An update on ancillary techniques in the diagnosis of soft tissue tumors. I have nothing to disclose. Andrew Horvai, MD, PhD Clinical Professor, Pathology Introduction Ancillary techniques
Differential diagnosis of HCC
 Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
The clinically challenging entity of liver metastasis from tumors of unknown primary
 The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
The Panel Approach to Diagnostics. Lauren Hopson International Product Specialist Cell Marque Corporation
 The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center
Carcinoma of Unknown Primary (CUP)
") Metasta c Carcinoma of Unknown Primary: Diagnos c Approach Using Immunohistochemistry James R. Conner, MD, PhD Mount Sinai Hospital Toronto, ON Carcinoma of Unknown Primary (CUP) 3-5% of all new malignant
Metasta c Carcinoma of Unknown Primary: Diagnos c Approach Using Immunohistochemistry James R. Conner, MD, PhD Mount Sinai Hospital Toronto, ON Carcinoma of Unknown Primary (CUP) 3-5% of all new malignant
CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY
 CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY Jason L Hornick, MD, PhD Director of Surgical Pathology Director of Immunohistochemistry Brigham and Women s Hospital Associate
CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY Jason L Hornick, MD, PhD Director of Surgical Pathology Director of Immunohistochemistry Brigham and Women s Hospital Associate
Effective January 1, 2018 ICD O 3 codes, behaviors and terms are site specific
 Effective January 1, 2018 codes, behaviors and terms are site specific /N 8551/3 Acinar adenocarcinoma (C34. _) Lung primaries diagnosed prior to 1/1/2018 use code 8550/3 For prostate (all years) see 8140/3
Effective January 1, 2018 codes, behaviors and terms are site specific /N 8551/3 Acinar adenocarcinoma (C34. _) Lung primaries diagnosed prior to 1/1/2018 use code 8550/3 For prostate (all years) see 8140/3
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
2018 ICD-O-3 Updates in Table Format with Annotation for Reference
 Status Histology Description (this may be preferred term or a synonym) Report Comments New term 8010 3 Urachal carcinoma (C65.9, C66.9, C67._, C68._) New term 8013 3 Combined large cell neuroendocrine
Status Histology Description (this may be preferred term or a synonym) Report Comments New term 8010 3 Urachal carcinoma (C65.9, C66.9, C67._, C68._) New term 8013 3 Combined large cell neuroendocrine
Effective January 1, 2018 ICD O 3 codes, behaviors and terms are site specific
 Effective January 1, 2018 codes, behaviors and terms are site specific Status /N 8010/3 Urachal carcinoma (C65.9, C66.9, C67. _, C68._) 8013/3 Combined large cell neuroendocrine carcinoma (C34. _, C37.9)
Effective January 1, 2018 codes, behaviors and terms are site specific Status /N 8010/3 Urachal carcinoma (C65.9, C66.9, C67. _, C68._) 8013/3 Combined large cell neuroendocrine carcinoma (C34. _, C37.9)
Financial disclosures
 Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Cutaneous Mesenchymal Neoplasms with EWSR1 Rearrangement By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchc Geisel School of
Financial disclosures
 An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
An update on immunohistochemical markers in mesenchymal neoplasms By Konstantinos Linos MD, FCAP, FASDP Assistant Professor of Pathology Geisel School of Medicine at Dartmouth Dartmouth-Hitchcock Medical
Molecular pathology in soft tissue tumors. Sylvia Höller Pathologie
 Molecular pathology in soft tissue tumors Sylvia Höller Pathologie When do we perform molecular testing? Morphology and IHC are not clearly fitting with an entity some translocations are entity specific
Molecular pathology in soft tissue tumors Sylvia Höller Pathologie When do we perform molecular testing? Morphology and IHC are not clearly fitting with an entity some translocations are entity specific
Immunohistochemical classification of the unknown primary tumour (UPT) Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark") Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Technology from Abcam
 CD2 (EP222) CD2 is one of the earliest T-cell lineage restricted antigens to appear during T-cell differentiation and only rare CD2+ cells can be found in the bone marrow. Anti-CD2 is a pan-t-cell antigen
CD2 (EP222) CD2 is one of the earliest T-cell lineage restricted antigens to appear during T-cell differentiation and only rare CD2+ cells can be found in the bone marrow. Anti-CD2 is a pan-t-cell antigen
Histopathological diagnosis of CUP
 Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Contents Part I Introduction 1 General Description 2 Natural History: Importance of Size, Site, Histopathology
 Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
Contents Part I Introduction 1 General Description... 3 1.1 Introduction... 3 1.2 Incidence and Prevalence... 5 1.3 Predisposing and Genetic Factors... 8 References... 16 2 Natural History: Importance
Diagnostic IHC in lung and pleura pathology
 Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
2 Berkeley Street, Suite 403, Toronto, Ontario M5A 2W3 Visit us at: Tel: Fax:
 E-Path A.I. Engine Knowledge Base Enhancements Version 1.0.0.29 April 1, 2018 The major enhancements in the E-Path Knowledge Base from versions 1.0.0.28 through 1.0.0.29 are as follows: 1. Addition/modification
E-Path A.I. Engine Knowledge Base Enhancements Version 1.0.0.29 April 1, 2018 The major enhancements in the E-Path Knowledge Base from versions 1.0.0.28 through 1.0.0.29 are as follows: 1. Addition/modification
ACCME/Disclosures. Diagnosing Mesothelioma in Limited Tissue Samples. Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016
 Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Diagnosing Mesothelioma in Limited Tissue Samples Papanicolaou Society of Cytopathology Companion Meeting March 12 th, 2016 Sanja Dacic, MD, PhD University of Pittsburgh ACCME/Disclosures GENERAL RULES
Ascitic Fluid and Use of Immunocytochemistry. Mercè Jordà, University of Miami
 Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Immunohistochemical classification of lung carcinomas and mesotheliomas. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Immunohistochemistry on Fluid Specimens: Technical Considerations
 Immunohistochemistry on Fluid Specimens: Technical Considerations Blake Gilks Dept of Pathology University of British Columbia, Vancouver, BC, Canada Disclosures None Learning Objectives At the end of
Immunohistochemistry on Fluid Specimens: Technical Considerations Blake Gilks Dept of Pathology University of British Columbia, Vancouver, BC, Canada Disclosures None Learning Objectives At the end of
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
List of Available TMAs in the PRN
 TMA RPCI_BrainCa01 RPCI_BrCa03 RPCI_BrCa04 RPCI_BrCa05 RPCI_BrCa0 RPCI_BrCa07 RPCI_BrCa08 RPCI_BrCa15 RPCI_BrCa1 RPCI_BrCa17 RPCI_BrCa18 RPCI_BrCa19 RPCI_BrCa20 RPCI_BrCa21 RPCI_BrCa24 RPCI_BrCa25 RPCI_BrCa2
TMA RPCI_BrainCa01 RPCI_BrCa03 RPCI_BrCa04 RPCI_BrCa05 RPCI_BrCa0 RPCI_BrCa07 RPCI_BrCa08 RPCI_BrCa15 RPCI_BrCa1 RPCI_BrCa17 RPCI_BrCa18 RPCI_BrCa19 RPCI_BrCa20 RPCI_BrCa21 RPCI_BrCa24 RPCI_BrCa25 RPCI_BrCa2
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Nordic Immunohistochemical Quality Control
 Nordic Immunohistochemical Quality Control Immunohistochemistry in the classifiation of neoplasias of the alimentary tract & External Quality Assurance of Immunohistochemistry for GI cancer markers Mogens
Nordic Immunohistochemical Quality Control Immunohistochemistry in the classifiation of neoplasias of the alimentary tract & External Quality Assurance of Immunohistochemistry for GI cancer markers Mogens
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources
 Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Reporting of carcinoma of unknown primary tumour (CUP)
") Reporting of carcinoma of unknown primary tumour (CUP) Prof John Schofield Kent Oncology Centre with grateful thanks to Dr Karin Oien University of Glasgow Royal College of Pathologists Cancer datasets
Reporting of carcinoma of unknown primary tumour (CUP) Prof John Schofield Kent Oncology Centre with grateful thanks to Dr Karin Oien University of Glasgow Royal College of Pathologists Cancer datasets
Evening Specialty Conference: Cytopathology
 : Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
: Cytopathology N. Paul Ohori, M.D. University of Pittsburgh Medical Center Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships USCAP requires that all planners
I have nothing to disclose
 A 47 year old female with multiple lung nodules Disclosure of Relevant Financial Relationships Tamar Giorgadze, MD, PhD Professor of Pathology Medical College of Wisconsin Milwaukee, Wisconsin USCAP requires
A 47 year old female with multiple lung nodules Disclosure of Relevant Financial Relationships Tamar Giorgadze, MD, PhD Professor of Pathology Medical College of Wisconsin Milwaukee, Wisconsin USCAP requires
3/27/2017. Disclosure of Relevant Financial Relationships
 Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Ophthalmic Pathology Evening Specialty Conference USCAP 2017 5 th March, 2017 Mukul K. Divatia, MD Assistant Professor Department of Pathology & Genomic Medicine Weill Cornell Medical College Houston Methodist
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors
 Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
Review and Updates of Immunohistochemistry in Selected Salivary Gland and Head and Neck Tumors. Monophasic tumors : myoepithelioma, acinic cell carcinoma, and salivary duct carcinoma. Biphasic tumors includes
I. Diagnosis of the cancer type in CUP
 Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia
 Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
Tumores de células pequeñas, redondas y azules: diagnóstico diferencial cuando el tiempo apremia Sílvia Bagué Servei de Patologia Hospital de Sant Pau Barcelona Soft tissue sarcomas Heterogeneous group
What I Learned from 3 Cases and 3 Antibodies
 What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships
What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships
incidence rate x 100,000/year
 Tier R=rare C=common Cancer Entity European crude and age adjusted incidence by cancer, years of diagnosis 2000 and 2007 Analisys based on 83 population-based cancer registries * applying the European
Tier R=rare C=common Cancer Entity European crude and age adjusted incidence by cancer, years of diagnosis 2000 and 2007 Analisys based on 83 population-based cancer registries * applying the European
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities
 Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities Sujana Movva 1, Wenhsiang Wen 2, Wangjuh Chen 2, Sherri Z. Millis 2, Margaret von Mehren 1, Zoran
Predictive biomarker profiling of > 1,900 sarcomas: Identification of potential novel treatment modalities Sujana Movva 1, Wenhsiang Wen 2, Wangjuh Chen 2, Sherri Z. Millis 2, Margaret von Mehren 1, Zoran
Carcinoma of unknown primary origin (CUP) is defined
 is defined") REVIEW ARTICLE Metastatic Carcinoma of Unknown Primary: Diagnostic Approach Using Immunohistochemistry James R. Conner, MD, PhD and Jason L. Hornick, MD, PhD Abstract: Carcinoma of unknown primary origin
REVIEW ARTICLE Metastatic Carcinoma of Unknown Primary: Diagnostic Approach Using Immunohistochemistry James R. Conner, MD, PhD and Jason L. Hornick, MD, PhD Abstract: Carcinoma of unknown primary origin
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Spindle Cell Lesions Of The Breast. Emad Rakha Professor of Breast Pathology and Consultant Pathologist
 Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Spindle Cell Lesions Of The Breast Emad Rakha Professor of Breast Pathology and Consultant Pathologist * SCLs comprise a wide spectrum of diseases, ranging from reactive processes to aggressive malignant
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Classification of the unknown primary tumour: the primary IHC panel
 CIQC/CAP-ACP SEMINAR 2013: DIAGNOSTIC IHC AND MOLECULAR PATHOLOGY Classification of the unknown primary tumour: the primary IHC panel Aalborg University Hospital Denmark Tumours of unknown origin: Histology
CIQC/CAP-ACP SEMINAR 2013: DIAGNOSTIC IHC AND MOLECULAR PATHOLOGY Classification of the unknown primary tumour: the primary IHC panel Aalborg University Hospital Denmark Tumours of unknown origin: Histology
Klinisch belang van chromosomale translocatie detectie in sarcomen
 Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
Translocations in sarcomas Klinisch belang van chromosomale translocatie detectie in sarcomen Judith V.M.G. Bovée, M.D., Ph.D. Department of Pathology Leiden University Medical Center RNA binding DNA binding
Biopsy Interpretation of Spindle cell proliferations of the Serosa
 Biopsy Interpretation of Spindle cell proliferations of the Serosa Richard Attanoos, Cardiff. U.K. Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee)
Biopsy Interpretation of Spindle cell proliferations of the Serosa Richard Attanoos, Cardiff. U.K. Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee)
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP
 What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
What is New in the 2015 WHO Lung Cancer Classification? Zhaolin Xu, MD, FRCPC, FCAP Professor, Dept of Pathology, Dalhousie University, Canada Pulmonary Pathologist and Cytopathologist, QEII HSC Senior
IHC Panels as an Aid in Diagnostic Decision Making
 IHC Antibody Test Selection Using a Panel Approach Steven Westra B.S. Reagent Product Specialist Leica Biosystems IHC Panels as an Aid in Diagnostic Decision Making Diagnostic Use of Tumors Using Algorithms
IHC Antibody Test Selection Using a Panel Approach Steven Westra B.S. Reagent Product Specialist Leica Biosystems IHC Panels as an Aid in Diagnostic Decision Making Diagnostic Use of Tumors Using Algorithms
Schedule of Accreditation issued by United Kingdom Accreditation Service 2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK
 2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK Royal National Orthopaedic Hospital NHS Trust Brockley Hill Stanmore Middlesex HA7 4LP Contact: Professor Adrienne Flanagan Tel: +44 (0)20
2 Pine Trees, Chertsey Lane, Staines-upon-Thames, TW18 3HR, UK Royal National Orthopaedic Hospital NHS Trust Brockley Hill Stanmore Middlesex HA7 4LP Contact: Professor Adrienne Flanagan Tel: +44 (0)20
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
Enterprise Interest Nothing to declare Diagnoses one would not like to miss in soft tissue pathology early in your career Marta Sbaraglia, MD Department of Pathology Hospital of Treviso University of Padua
LOOK-ALIKES IN SPINDLE AND EPITHELIOID TUMORS: Immunohistochemistry. Cytogenetics Flow cytometry Molecular diagnostics
 LOOK-ALIKES IN SPINDLE AND EPITHELIOID TUMORS: Ultrastructural value and pitfalls in diagnosis Guillermo A Herrera Department of Pathology and Translational Pathobiology Louisiana State University Health
LOOK-ALIKES IN SPINDLE AND EPITHELIOID TUMORS: Ultrastructural value and pitfalls in diagnosis Guillermo A Herrera Department of Pathology and Translational Pathobiology Louisiana State University Health
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
FNA Cytology of Metastatic Malignancies of Unknown Primary Site
 FNA Cytology of Metastatic Malignancies of Unknown Primary Site Tarik M. Elsheikh Jan F. Silverman Pathologic Diagnosis of Metastasis Smaller specimens, less invasive techniques FNA cytology is highly
FNA Cytology of Metastatic Malignancies of Unknown Primary Site Tarik M. Elsheikh Jan F. Silverman Pathologic Diagnosis of Metastasis Smaller specimens, less invasive techniques FNA cytology is highly
C.L. Davis Foundation Descriptive Veterinary Pathology Course
 C.L. Davis Foundation 2015 Descriptive Veterinary Pathology Course IHC Resources IHC Identification Targets Antibodies Antibodies 1 Antibodies Specimens Antigen Retrieval Unmasks antigen epitopes Methods
C.L. Davis Foundation 2015 Descriptive Veterinary Pathology Course IHC Resources IHC Identification Targets Antibodies Antibodies 1 Antibodies Specimens Antigen Retrieval Unmasks antigen epitopes Methods
3/27/2017. Pulmonary Pathology Specialty Conference. Disclosure of Relevant Financial Relationships. Clinical History:
 Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Pulmonary Pathology Specialty Conference Saul Suster, M.D. Medical College of Wisconsin Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position
Diagnostic Value of Immunohistochemistry in Soft Tissue Tumors
 Original Article DOI: 10.21276/APALM.1637 Diagnostic Value of Immunohistochemistry in Soft Tissue Tumors Sridevi. V*., Susruthan Muralitharan., and Thanka. J Dept of Pathology, SriMuthukumaran Medical
Original Article DOI: 10.21276/APALM.1637 Diagnostic Value of Immunohistochemistry in Soft Tissue Tumors Sridevi. V*., Susruthan Muralitharan., and Thanka. J Dept of Pathology, SriMuthukumaran Medical
ACCME/Disclosures ALK FUSION-POSITIVE MESENCHYMAL TUMORS. Tumor types with ALK rearrangements. Anaplastic Lymphoma Kinase. Jason L.
 Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Companion Meeting of the International Society of Bone and Soft Tissue Pathology The Evolving Concept of Mesenchymal Tumors ALK FUSION-POSITIVE MESENCHYMAL TUMORS Jason L. Hornick, MD, PhD March 13, 2016
Classification (1) Classification (3) Classification (2) Spindle cell lesions. Spindle cell lesions of bladder (Mills et al.
 Classification (3) Classification (2) Spindle cell lesions. Spindle cell lesions of bladder (Mills et al.") Non-epithelial tumours and nonepithelial tumour-like lesions of the bladder Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Classification (1) Myofibroblastic proliferations and
Non-epithelial tumours and nonepithelial tumour-like lesions of the bladder Dr Jonathan H Shanks The Christie NHS Foundation Trust, Manchester, UK Classification (1) Myofibroblastic proliferations and
S2199 S2200. * Speaker's diagnosis 78
 98 21 2 14 13:30 * Speaker's diagnosis 78 S2199 Meningioma 48 Papillary meningioma * 30 Angiomatous meningioma 15 Ependymoma 12 Papillary ependymoma 6 Anaplastic ependymoma 2 Cellular ependymoma 1 Hemangioblastoma
98 21 2 14 13:30 * Speaker's diagnosis 78 S2199 Meningioma 48 Papillary meningioma * 30 Angiomatous meningioma 15 Ependymoma 12 Papillary ependymoma 6 Anaplastic ependymoma 2 Cellular ependymoma 1 Hemangioblastoma
Update on Cutaneous Mesenchymal Tumors. Thomas Brenn
 Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
Update on Cutaneous Mesenchymal Tumors Thomas Brenn Cutaneous Mesenchymal Tumours Wide morphological and biological spectrum Myofibroblastic, smooth muscle, neural, vascular, apidocytic, undifferentiated;
GUT-C 11/30/2017. Debasmita Das, M.D. PGY-1 Danbury Hospital
 GUT-C 11/30/2017 Debasmita Das, M.D. PGY-1 Danbury Hospital CLINICAL SUMMARY 8/2017 59 year old female Presented to the ED with 1 month history of general malaise, fever and weight loss PMH: Significant
GUT-C 11/30/2017 Debasmita Das, M.D. PGY-1 Danbury Hospital CLINICAL SUMMARY 8/2017 59 year old female Presented to the ED with 1 month history of general malaise, fever and weight loss PMH: Significant
Immunohistochemical Evaluation of Necrotic Malignant Melanomas
 Anatomic Pathology / EVALUATION OF NECROTIC MALIGNANT MELANOMAS Immunohistochemical Evaluation of Necrotic Malignant Melanomas Daisuke Nonaka, MD, Jordan Laser, MD, Rachel Tucker, HTL(ASCP), and Jonathan
Anatomic Pathology / EVALUATION OF NECROTIC MALIGNANT MELANOMAS Immunohistochemical Evaluation of Necrotic Malignant Melanomas Daisuke Nonaka, MD, Jordan Laser, MD, Rachel Tucker, HTL(ASCP), and Jonathan
Outline. Hepatocellular Carcinoma Histologic variants. HCC: Histologic variants
 2018 Park City AP Update Hepatocellular Carcinoma Histologic variants Sanjay Kakar, MD University of California, San Francisco Outline Histologic variants of HCC Morphologic and Immunohistochemical pitfalls
2018 Park City AP Update Hepatocellular Carcinoma Histologic variants Sanjay Kakar, MD University of California, San Francisco Outline Histologic variants of HCC Morphologic and Immunohistochemical pitfalls
Newer soft tissue entities
 Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
Newer soft tissue entities Examples among fibroblastic tumors Turku, May 6, 2010 Markku Miettinen, M.D. AFIP, Washington, DC Fibroblastic neoplasms Solitary fibrous tumor /Hemangiopericytoma Low-grade
INTERPRETATION OF IMMUNOHISTOCHEMICAL STAINS - DIFFICULTIES AND PITFALLS. Gabor Fischer Diagnostic Services Manitoba University of Manitoba
 INTERPRETATION OF IMMUNOHISTOCHEMICAL STAINS - DIFFICULTIES AND PITFALLS Gabor Fischer Diagnostic Services Manitoba University of Manitoba IHC INTERPRETATIONS LOCAL DATA Diagnostic Services Manitoba Number
INTERPRETATION OF IMMUNOHISTOCHEMICAL STAINS - DIFFICULTIES AND PITFALLS Gabor Fischer Diagnostic Services Manitoba University of Manitoba IHC INTERPRETATIONS LOCAL DATA Diagnostic Services Manitoba Number
Case Presentation. Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD. Department of Pathology Jordan University Hospital Amman, Jordan
 Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
Case Presentation Maha Akkawi, MD, Fatima Obeidat, MD, Tariq Aladily, MD Department of Pathology Jordan University Hospital Amman, Jordan The 25th Annual Congress of the ADIAP The 8/11/2013 1 5th International
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
Mesothelioma Pathobasic. Lukas Bubendorf Pathology
 Mesothelioma Pathobasic Lukas Bubendorf Pathology Mechanisms of Asbestos Carcinogenesis in Mesothelioma Asprin High-mobility group protein B1 master switch HMGB1 Initiation/ perpetuation of inflamm. response
Mesothelioma Pathobasic Lukas Bubendorf Pathology Mechanisms of Asbestos Carcinogenesis in Mesothelioma Asprin High-mobility group protein B1 master switch HMGB1 Initiation/ perpetuation of inflamm. response
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Expression of Cytokeratin 5/6 in Epithelial Neoplasms: An Immunohistochemical Study of 509 Cases
 Expression of Cytokeratin 5/6 in Epithelial Neoplasms: An Immunohistochemical Study of 509 Peiguo G. Chu, M.D., Ph.D., Lawrence M. Weiss, M.D. Department of Pathology, City of Hope National Medical Center,
Expression of Cytokeratin 5/6 in Epithelial Neoplasms: An Immunohistochemical Study of 509 Peiguo G. Chu, M.D., Ph.D., Lawrence M. Weiss, M.D. Department of Pathology, City of Hope National Medical Center,
Effusion Cytology: Diagnostic Challenges
 Effusion Cytology: Diagnostic Challenges Tarik M. Elsheikh, MD Professor and Medical Director, Anatomic Pathology Cleveland Clinic Outside Consult Case 45 year old woman, presented with nausea, dyspnea,
Effusion Cytology: Diagnostic Challenges Tarik M. Elsheikh, MD Professor and Medical Director, Anatomic Pathology Cleveland Clinic Outside Consult Case 45 year old woman, presented with nausea, dyspnea,
Role of immunohistochemistry in the differential diagnosis of malignant small round cell tumor: a study of 38 cases
 International Journal of Research in Medical Sciences Patel A et al. Int J Res Med Sci. 2015 Dec;3(12):3833-3839 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20151452
International Journal of Research in Medical Sciences Patel A et al. Int J Res Med Sci. 2015 Dec;3(12):3833-3839 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20151452
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Affiliazione autori0. Riccardo Ricci Journal Club GIPAD, settore GIST Anatomia Patologica, Università Cattolica, Roma
 GIST Manifesting as a Retroperitoneal Tumor: Clinicopathologic Immunohistochemical, and Molecular Genetic Study of 112 Cases American Journal of Surgical Pathology, 2017, 41:577-585 Miettinen M*; Felisiak-Golabek
GIST Manifesting as a Retroperitoneal Tumor: Clinicopathologic Immunohistochemical, and Molecular Genetic Study of 112 Cases American Journal of Surgical Pathology, 2017, 41:577-585 Miettinen M*; Felisiak-Golabek
Evening Specialty Conference Bone and Soft Tissue Pathology. Diagnostic pitfalls in bone and soft tissue pathology
 Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
Evening Specialty Conference Bone and Soft Tissue Pathology. Case 1 Elizabeth G Demicco, MD, PhD Mount Sinai Hospital, New York Disclosure of Relevant Financial Relationships USCAP requires that all planners
DIAGNOSTIC CHALLENGES Pancreas FNAB. Dr. M. Weir Oct 2017
 DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
DIAGNOSTIC CHALLENGES Pancreas FNAB Dr. M. Weir Oct 2017 CONFLICT OF INTEREST DISCLOSURE I have not had in the past 3 years, a financial interest, arrangement or affiliation with one or more organizations
Serous Effusions. Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland
 Serous Effusions Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland Serous membrane Body cavities: Pleural Pericardial Peritoneal Effusion = Excess of fluid 80% Benign 20% Malignant
Serous Effusions Spasenija Savic Prince, MD Pathology, University Hospital Basel, Switzerland Serous membrane Body cavities: Pleural Pericardial Peritoneal Effusion = Excess of fluid 80% Benign 20% Malignant
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, controls and EQA (part II)
") The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents