Targeting the Androgen Receptor in Prostate Cancer. Raoul S. Concepcion, MD,FACS FDUS/Colorado Springs August 2017
|
|
|
- Deirdre Hodges
- 6 years ago
- Views:
Transcription


1 Targeting the Androgen Receptor in Prostate Cancer Raoul S. Concepcion, MD,FACS FDUS/Colorado Springs August 2017
2 Consultant: GHI, CUSP, Tolmar, Integra Connect, Cellay, AZ Speakers Bureau: Dendreon, Astellas, Bayer, Janssen, Pfizer/Medivation, Amgen

3
4


5 Androgens are produced at 3 sites: - Testes - Adrenal gland - Prostate tumor cells
 1970s Steroidal and non-steroidal AAs available Nobel Prize: Andrzej Schally,")

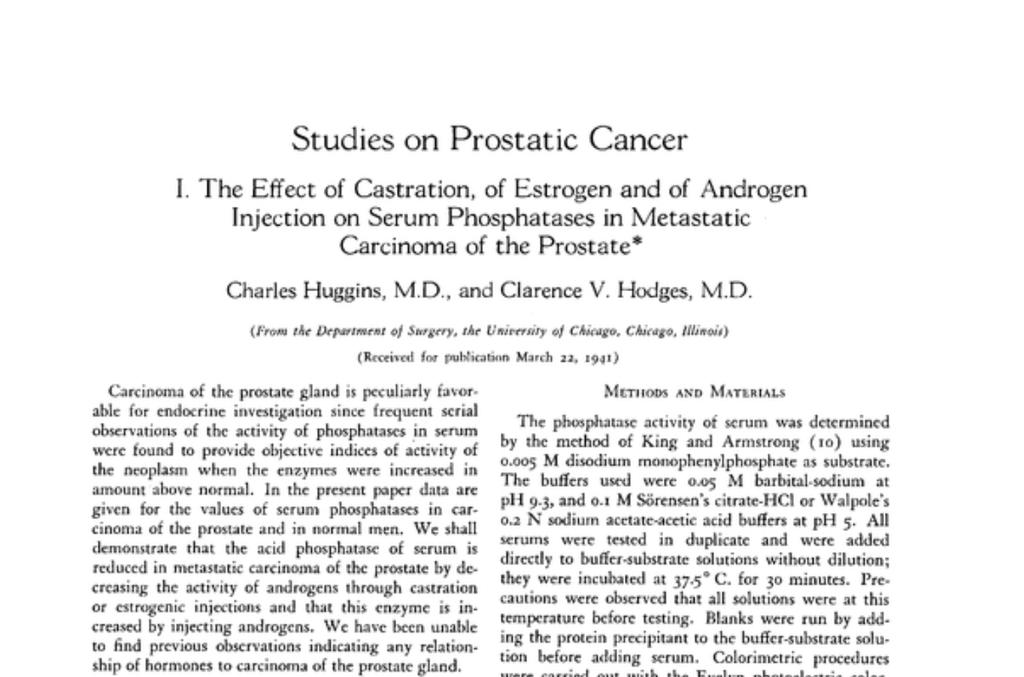
6 Historical Landmarks: 1 st Effective Treatment, 1 st Marker, 2 Nobel Prizes John Hunter 1780-castration 1904 First RP 1938-Acid Phos Huggins -endocrine control Advent of orchiectomy and estrogen treatment (Awarded Nobel Prize for this discovery) 1970s Steroidal and non-steroidal AAs available Nobel Prize: Andrzej Schally, Roger Guillemin 1980s Long-acting synthetic LHRH agonists 2003 First GnRH blocker (abarelix) launched The future New androgen receptor-targeted drugs. AA vaccines, biomarkers, genetic research 1920s RT for PC using radium 1867 First perineal prostatectomy performed 1960s RT established as important treatment for PC 1960s and 70s Synthetic estrogens developed 2004 Docetaxel in combination with prednisone approved 1995 Cryosurgery accepted as a treatment option for recurrent cancer after RT 2008 Degarelix approved in US 2009 ARSI Developed ARSI = Androgen Receptor Signaling Inhibitor; AA = an#androgen; LHRH = luteinizing hormone releasing hormone. Figure courtesy of Dr E. David Crawford
7 Androgen deprivation therapy (ADT) Estrogens (DES) Surgical castration (bilateral orchiectomy) LHRH/GnRH analogs (agonists/antagonists) Antiandrogens/Androgen receptor signaling inhibitors Flutamide, Bicalutamide, Nilutamide Enzalutamide? Apalutamide 17,20 Lyase Inhibitors/Androgen Synthesis inhibitors Ketoconazole Abiraterone Acetate

8 Complications of ADT 1. Hot Flashes 2. Anemia 3. Sexual dysfunction 4. Cognitive dysfunction,? Depression 5. Osteoporosis 6. Metabolic Syndrome n obesity n Insulin resistance n Dyslipidemia n Hypertension Gaztanaga and Cook, JNCCN. 2012;10.

9

10
11

12 Figure 1 Androgen and AR action MH Eileen Tan 1, 2, * et al. Acta Pharmacol Sin 2014; 36: 3 23; doi: /aps Published by 2014 CPS and SIMM

 SHBG Free T Modified from Peter")
13 Target 1: Gonadal/Circulating T LHRH Leuprolide Goserelin Degarelix others Estrogens TESTOSTERONE SHBG GTX758 (ERa agonist) SHBG Free T Modified from Peter Nelson, MD


14 Target 2: Adrenal/Intracrine Ligands AKR1C3 CYP17 DHEA A-dione ADRENAL T DHT Cholesterol -- AKR1C3 CYP17 -- de novo CYP17 ü Ketoconazole ü Abiraterone ü TAK700 ü TOK001 ü VT-464 AKR1C3 ü Indomethacin ü I-analogs 3bHSD ü Abiraterone-HD ü Trilostane Modified from Peter Nelson, MD


15 Target 3: AR Degradation HSP90 Antagonists ü 17AAG ü STA9090 ü AT13387 ü Others Selective AR downregulators or degraders* HSP90 HSP90 AR AR X PROTEASOME Modified from Peter Nelson, MD ü Curcumin ü TOK001 ü AZD3514 ü ASC-J9 ü PPD ü Antisense *many others with low potency

16 Target 4: Androgen Receptor Blockade T 5aReductase DHT Modified from Peter Nelson, MD P AR P AR Ligand Binding AR ü enhanced degradation ü translocation block ü unproductive transcription Competitive Antagonists Flutamide Bicalutamide Nilutamide Enzalutamide ARN509 TOK001
17 Target 5: Prevent AR Nuclear Translocation Microtubule Inhibitors ü Enzalutamide ü Paclitaxel ü Docetaxel ü Cabazitaxel Nuclear Translocation P AR P ARsv P AR P AR Modified from:peter Nelson, MD
18 Target 6: Interfere With AR Enablers P AR P Signaling Pathways ü Her2/3 ü IGF1R ü CDKs ü others Nuclear Translocation ARsv P AR P AR Modified from:peter Nelson, MD

19 Target 7: Block AR DNA/Co-Activator Interaction P AR P AR Androgen-response Elements (ARE) Coactivators TM Important as they may target ARsv Target Gene Expression Non-Competitive Antagonists* EPI-001 D2 Pyrivinium Harmol HCL Others Modified from Peter Nelson, MD *N-C interactions Nuclear translocations AR AF2-LXXLL Interactions Co-factor inhibition





20 Target 8: AR Downstream Effectors PI3K-Pathway Inhibitors P AR P AR TM Target Gene Expression ETS-family Inhibitors Proliferation Survival Metabolism CAMKK2 inhibitor (STO-609) Modified from Peter Nelson, MD

:76-85. 2. DEBES JD, TINDALL DJ. N ENGL J MED.")
:831-838.")
21 The Development of mcrpc Involves Alterations in AR-Signaling Androgen Signaling 1 Pathways to Castration Resistance 1 Aggressive forms of CRPC, such as neuroendocrine, and small-cell carcinomas often lack AR expression 2,3 1. HARRIS WP, ET AL. NAT CLIN PRACT UROL. 2009;6(2): DEBES JD, TINDALL DJ. N ENGL J MED. 2004;351(15): APARICIO A, TZELEPI V. ONCOLOGY (WILLISTON PARK). 2014;28(10): Reprinted by permission from Macmillan Publishers Ltd: Nat Clin Pract Urol, Harris WP, et al. 2009;6(2):
22 Summary of clinical trial outcome Patient setting Control Increase in median, months OS HR p value Docetaxel/P 1 First-line Mitoxantrone/P Cabazitaxel/P 2 Post-docetaxel Mitoxantrone/P < Abiraterone/P 3 Post-docetaxel Placebo/P < Abiraterone/P 4 Chemo-naïve Placebo/P * Enzalutamide 5 Post-docetaxel Placebo <0.001 Enzalutamide 6 Chemo-naïve Placebo < Radium Bone metastases, Pre- and post docetaxel Placebo <0.001 *OS did not reach the prespecified efficacy boundary (p=0.0035) 1. Berthold DR, et al. J Clin Oncol 2008;26:242 5; 2. de Bono JS, et al. Lancet 2010;76: ; 3. Fizazi K, et al. Lancet Oncol 2012;13:983 92; 4. Rathkopf DE, et al. J Clin Oncol 2013;31(suppl. 6): abstract 5; 5. Scher HI, et al. N Engl J Med 2012;367: ; Beer et al., J Clin Oncol 32, 2014 (suppl 4; abstr LBA1^); 7. Parker C, et al. N Engl J Med 2013;369: These studies are different (in type, population, inclusion/exclusion criteria, design and method, primary objectives) and therefore a comparison cannot be made.

23 Biologic Mechanisms Driving CRPC Antonarakis and Armstrong, Clin Oncol News 2011
24 AR Splice Variants Guo Z and Qiu Y. Int J Biol Sci. 2011;7:
25 AR splice variants are associated with poor prognosis and Treatment resistance The translation of splice variants results in proteins with altered activity and regulation 1 AR Splice Variants Exons 4-8 of AR are not required for transcriptional activity and splice variants lacking this region may be constitutively active 2 In one study, expression of AR variants lacking the ligand-binding domain in CRPC bone metastases was associated with poor prognosis 2 Detection of AR-V7 in tumor cells is associated with treatment resistance 3,4 Full-length AR Ligand-binding domain Amino acid AR-V Thadani-Mulero M, et al. Cancer Res. 2014;74(8): American Association for Cancer Research
26 Lack of Response Associated with AR-V7 (Johns Hopkins University) Prospective study of M1 CRPC patients eligible for abiraterone (N=31) and enzalutamide (N=31) treatment; AR-V7 identified in CTC samples pretreatment None (0/18) of the AR-V7 positive patients achieved a PSA50 Only 1 AR-V7 positive patient showed any PSA reduction (enzalutamide) AR-V7 prevalence increased post additional treatments Response Treatment 1 Baseline AR-V7+ Abiraterone 19% (N=31) (6/31) Enzalutamide (N=31) 39% (12/31) AR-V7 status PSA50 P- value rpfs P- value OS (95% CI) P value + 0% (0/6) 2.3 mos 10.6 mos (8.5 NR).004 < % (17/25) >6.3 mos >11.9 mos (11.9 NR) + 0% (0/12) 2.1 mos 5.5 mos (3.9 NR).004 < % (10/19) 6.1 mos NR (NR NR) Patient Treatment Status 2 Before enzalutamide or abiraterone Post enzalutamide Post abiraterone Post abiraterone & enzalutamide AR-V7 Prevalence 12% 25% 51% 67% CRPC=castration-resistant prostate cancer; CTC=circulating tumor cell; M1=metastatic disease; NR=not reached; OS=overall survival; PSA=prostate specific antigen; rpfs=radiographic progression-free survival. 1. Antonarakis ES et al. NEJM /NEJMoa Antonarakis ES et al. ASCO
27

28 Mutation in 3BHSD1 Facilitates Conversion of Precursors to DHT
29
 ECOG PS")
 Key Secondary endpoints: Safety Proportion of patients with negative")
 Proportion of patients with secondary rise in PSA at 1 year and 2 years Quality of life by BFI, SF-12, EPIC, MAX-PC *low")

.")
30 ENACT: Enzalutamide in Patients with Localized Prostate Cancer Undergoing Active Surveillance Recruiting N=230 Key Eligibility Criteria: Clinically localized, histologically proven adenocarcinoma of prostate Not received any treatment for prostate cancer ever and has chosen active surveillance (low/ intermediate risk) ECOG PS < 2 R 1:1 Enzalutamide 160mg QD x 1 year then active surveillance for year 2 Active Surveillance x 2 years Stratification factors: - low vs intermediate risk - mpmri biopsy vs non mpmri biopsy Primary endpoint: Time to progression (pathological or therapeutic) Key Secondary endpoints: Safety Proportion of patients with negative biopsy for PC at 1 and 2 years Percent of cancer positive cores at 1 year and 2 years Time to PSA progression (secondary rise in serum PSA>25% above baseline or >25% above nadir or absolute increase > 2 ng/ ml) Proportion of patients with secondary rise in PSA at 1 year and 2 years Quality of life by BFI, SF-12, EPIC, MAX-PC *low risk = T1c-T2a, PSA<10, N0, M0, GS 6 ; intermediate risk = T2b-T2c, PSA<20, N0, M0, GS 7 (3+4 pattern only). PC progression defined as either pathologic or therapeutic progression. Pathologic progression: increase in primary or secondary Gleason pattern by 1 or higher proportion of cancer positive cores ( 15% increase). Therapeutic progression: the earliest occurrence of primary therapy for PC (prostatectomy/ radiation/focal therapy/systemic therapy). EPIC = Expanded PC Index Composite questionnaire urinary, sexual and hormonal domains; MAX-PC = Memorial Anxiety scale for PC questionnaire; SF-12 = Medical outcomes study 12-item short form survey. (NCT ) 30



31 EMBARK: A Study of Enzalutamide in Patients With High-Risk Nonmetastatic Prostate Cancer Progressing After Definitive Therapy Recruiting Patients with high-risk nonmetastatic prostate cancer progressing after definitive therapy* N = 1860 R *Additional inclusion criteria include: PSA doubling time 9 months; PSA 2.0 ng/ml for patients who had radical prostatectomy as primary treatment or 5.0 ng/ml and greater than or equal to the nadir + 2 ng/ml for patients who had radiotherapy as primary treatment; serum testosterone 150 ng/dl 1:1:1 Randomization stratification Enzalutamide 160 mg qd Enzalutamide 160 mg qd + Leuprolide q12wk Placebo qd + Leuprolide q12wk Objectives Primary Endpoint: Metastasis-free survival Key Secondary Endpoints: Overall survival Proportion of patients treatment-free 2 years after treatment suspension at week 37 due to undetectable PSA Time to castration resistance # Safety Phase 3 multinational randomized study # Time from randomization to first PSA increase that is 25% and 2 µg/l above the nadir or screening value, whichever is lower, and that is confirmed by a second consecutive value obtained at least 3 weeks later Composite measure of incidence and severity of adverse events, serious adverse events, incidence of treatment discontinuation due to adverse events, and incidence of new clinically significant changes in clinical laboratory values and vital signs PSA = prostate-specific antigen; R = randomization (NCT ).

 (Prostate Cancer Clinical")
 ORR Time to pain progression Safety *High-volume disease = metastases involving viscera or 4 bone lesions with at least 1 of which in a bony structure beyond the vertebral column & pelvic")
32 ARCHES: Multinational, Phase 3, Randomized, Double-blind, Placebocontrolled Efficacy and Safety Study of Enzalutamide +ADT vs Placebo + ADT in HSPC Patients Ongoing N= Patients with mhspc - ECOG PS Stratified by: volume of disease Low vs. high prior docetaxel therapy for prostate cancer No prior 1-5 cycles 6 cycles R 1:1 Enzalutamide + ADT 160 mg/d Placebo daily + ADT Primary Endpoint rpfs (based on central review) Key Secondary Endpoints OS Time to first SSE Time to castration resistance Time to deterioration of QoL Time to initiation of new antineoplastic therapy Time to PSA progression ( 2 ng/ml) (Prostate Cancer Clinical Trials Working Group 2 criteria) PSA undetectable rate (< 0.2 ng/ml) ORR Time to pain progression Safety *High-volume disease = metastases involving viscera or 4 bone lesions with at least 1 of which in a bony structure beyond the vertebral column & pelvic bone ADT = androgen deprivation therapy; BPI-SF = Brief Pain Inventory-Short Form; ECOG PS = Eastern Cooperative Oncology Group performance status; EQ-5D-5L = European Quality of life-5 Dimensions-5 Levels; FACT-P = Functional Assessment of Cancer Therapy-Prostate; GnRHa = gonadotropin releasing hormone analogue (agonist or antagonist) or prior bilateral orchiectomy (medical or surgical castration); mhspc = metastatic hormone sensitive prostate cancer; PC = prostate cancer; PSA = prostate-specific antigen; QLQ-PR25 = Quality of Life Questionnaire-Prostate 25; R = randomization; rpfs = radiographic progression-free survival (NCT ) 32


33 TITAN: Hormone Sensitive M1 Study Design Patients mhspc <6 mos of ADT Prior Rx for localized disease allowed Prior docetaxel allowed Metastatic disease documented by 1 bone lesion a Visceral metastasis permitted with bone metastases ECOG of 0-1 Est. N=1000 1:1 ADT + Apalutam ide ADT + placebo a Subjects with 1 bone lesion on scan must have CT / MRI confirmation. Primary Endpoints rpfs, OS Secondary Endpoint Time to symptomatic progression (pain progression or SRE) Time to chronic opioid use Time to initiation of chemotherapy Time to PSA progression Patient Reported Outcomes BPI-SF, BFI, FACT-P, EQ-5D-5L mhspc, metastatic hormone sensitive prostate cancer; SRE, skeletalrelated events. NCT Confidential and Proprietary Stratifications: Gleason Score at Diagnosis ( 7, >7) Geographic Regions (NA, EU, Other countries)




34 SPARTAN: High-Risk nmcrpc Phase 3 Study Design Patients 2:1 Apaluta mide + ADT Primary Endpoint Metastasis-free survival Nonmetastatic CRPC PSADT 10 mos Est. N=1200 On-Study Requirement: Continue LHRHa if no orchiectomy LHRHa, luteinizing hormone-releasing hormone agonist. Placebo + ADT Secondary Endpoint Overall survival Time to symptomatic progression Time to initiation of cytotoxic chemotherapy Radiographic progressionfree survival Time to metastasis
 Bicalutamide 50 mg/day (n = 198) Primary Endpoint Progression-free survival (PFS): Radiographic progression or PSA progression or Death")
:2098-2106. ClinicalTrials.")
35 STRIVE: Study Design Patient Population 396 men with progressive CRPC - M0 or M1 Asymptomatic/ mildly symptomatic Chemotherapy-naïve Ongoing ADT No prior progression on bicalutamide R A N D O M I Z E D 1:1 Enzalutamide 160 mg/day (n = 198) Bicalutamide 50 mg/day (n = 198) Primary Endpoint Progression-free survival (PFS): Radiographic progression or PSA progression or Death Key secondary endpoints: - Time to PSA progression - PSA response - rpfs (M1 population only) ADT = androgen deprivation therapy; CRPC = castration-resistant prostate cancer; M0 = nonmetastatic; M1 = metastatic; PSA = prostate-specific antigen; rpfs = radiographic PFS.. Penson DF, et al. J Clin Oncol Jun 20;34(18): ClinicalTrials.gov identifier: NCT

36 TERRAIN: A Phase 2 Efficacy and Safety Study of Enzalutamide vs Bicalutamide in mcrpc: Study Design 1 Patient population 375 men with progressive mcrpc Asymptomatic/ mildly symptomatic Chemotherapy-naïve Ongoing ADT No requirement for steroids Statistical design Final analysis planned at 220 progression events with 85% power to detect a target hazard ratio of 0.67 (assuming a median PFS of 9 months versus 6 months 2 ) Data cutoff date was 19 October 2014 with 240 events for the primary efficacy endpoint R A N D O M I Z E D 1:1 Enzalutamide 160 mg/day n = 184 Bicalutamide 50 mg/day n = 191 Primary endpoint Progression-free survival (PFS), defined as time from randomization to (whichever occurs first): Radiographic progression SRE Initiation of new antineoplastic therapy Death Secondary endpoints PSA response Time to PSA progression Safety mcrpc = metastatic castration-resistant prostate cancer; PSA = prostate-specific antigen; SRE = skeletal-related event 1. Shore ND, et al. Lancet Oncol. 2016;17: Kucuk O, et al. Urology. 2001;58:53-58.








37 ACIS: Chemo-Naive mcrpc Study Design Patients mcrpc ECOG 0 or 1 Testosteron e levels of <50 ng/dl (by GnRHa or surgical castration) Pain score 3 (BPI-SF Q3) Est. N=960 1:1 AAP + Apaluta mide AAP + Place bo Test PSA90 AAP+ Apaluta mide vs AAP (N~200) PSA 90 posit ive YES: Contin ue to N~960 NO: Stop study Stratification factors: Baseline ECOG 0 vs 1 Region (NA, EU, ROW) Presence / absence of visceral disease Primary Endpoint rpfs Secondary Endpoint Overall survival Time to pain progression Time to opiate use Time to chemothera py Time to ECOG deterioratio n AAP, abiraterone acetate plus prednisone; BPI-SF Q3, patient reported outcome survey for pain; ECOG, Eastern Cooperative Oncology Group; EU, European Union; GnRHa, gonadotropin releasing-hormone agonist; NA, North America; PSA90, PSA response defined as 90% reduction; rpfs, time from randomization to first evidence of radiographic disease progression or death from any cause; altrials.gov. ROW, rest NCT of NCT world.

38 FUTURE Novel and Multi Modal Therapy Radium-223 Saad et al., Urol Oncol. 2014;32(2):70-9.
39 Conclusions The AR continues to be a major driver in the growth and survival of prostate CA cells, even in the CRPC patient As urologists, we need to understand the nuances of resistance mechanisms and genomic alterations Despite all the recent advances, there remains multiple challenges and opportunities for researchers to better understand the disease and possible development of novel targeted agents Thank you rsconcepcion@me.com
40 Blue Earth Imaging -> Blue Earth County MN Blue Tooth Technology ->?????
41
Targeting the Androgen Receptor in Castration Resistant Prostate Cancer. Raoul S. Concepcion, MD,FACS IPCU January 2017
 Targeting the Androgen Receptor in Castration Resistant Prostate Cancer Raoul S. Concepcion, MD,FACS IPCU January 2017 Consultant: Myriad, CUSP, Tolmar, Integra Cloud, Cellay Speakers Bureau: Dendreon,
Targeting the Androgen Receptor in Castration Resistant Prostate Cancer Raoul S. Concepcion, MD,FACS IPCU January 2017 Consultant: Myriad, CUSP, Tolmar, Integra Cloud, Cellay Speakers Bureau: Dendreon,
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Risk of renal side effects with ADT. E. David Crawford University of Colorado, Aurora, CO, USA
 Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer?
 Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Perspective on endocrine and chemotherapy agents. Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
What will change for men with advanced prostate cancer in the next 24 months? ESO Observatory: Perspective on endocrine and chemotherapy agents
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Anti-Androgen Therapies for Prostate Cancer: A Focused Review
 Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Until 2004, CRPC was consistently a rapidly lethal disease.
 Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC
 Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC
 Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Hormonal Manipulations in CRPC. NW Clarke Professor of Urological Oncology Manchester UK
 Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Evolution or revolution in the treatment of prostate cancer
 Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Treatment of Advanced Prostate Cancer
 Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Patients Living Longer: The Promise of Newer Therapies
 Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS
 UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
UPDATE ON RECENT CUTTING-EDGE TRIALS: TREATMENTS NOW AVAILABLE FOR NEWLY DIAGNOSED mhspc PATIENTS Dr. Neal Shore, Carolina Urologic Research Centre, USA Assoc. Prof. Neeraj Agarwal, Huntsman Cancer Institute,
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Group Sequential Design: Uses and Abuses
 Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Apalutamide in the treatment of castrate-resistant prostate cancer: evidence from clinical trials
 811450TAU0010.1177/1756287218811450Therapeutic Advances in UrologyVS Koshkin and EJ Small review-article2018 Therapeutic Advances in Urology Review Apalutamide in the treatment of castrate-resistant prostate
811450TAU0010.1177/1756287218811450Therapeutic Advances in UrologyVS Koshkin and EJ Small review-article2018 Therapeutic Advances in Urology Review Apalutamide in the treatment of castrate-resistant prostate
8/31/ ) Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases
 Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases") Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Please consider the following information on ZYTIGA (abiraterone acetate). ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017
. ZYTIGA - Compendia Communication - NCCN LATITUDE and STAMPEDE June 2017") Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
Page 1 of 2 Janssen Scientific Affairs, LLC 1125 Trenton-Harbourton Road PO Box 200 Titusville, NJ 08560 800.526.7736 tel 609.730.3138 fax June 08, 2017 Joan McClure 275 Commerce Drive #300 Fort Washington,
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Present and Future Perspectives in Treatment of mcrpc Patients
 Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
Present and Future Perspectives in Treatment of mcrpc Patients Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com Disclosures Astellas, Takeda, Janssen, Bouchara Recordati,
Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering
 > Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
> Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Developmental Therapeutics for Genitourinary Malignancies
 Developmental Therapeutics for Genitourinary Malignancies Russell Szmulewitz, MD April 2018 Disclosure Information 23 rd Annual Developmental Therapeutics Symposium Name of Speaker I have the following
Developmental Therapeutics for Genitourinary Malignancies Russell Szmulewitz, MD April 2018 Disclosure Information 23 rd Annual Developmental Therapeutics Symposium Name of Speaker I have the following
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Non metastatic castrate-resistant prostate cancer (M0 CRPC) Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France") Non metastatic castrate-resistant prostate cancer (M0 CRPC) Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium for: Amgen, Astellas,
Non metastatic castrate-resistant prostate cancer (M0 CRPC) Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards/honorarium for: Amgen, Astellas,
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy).
.") Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
Advanced Prostate Cancer. Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options
 Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
New Treatment Options for Prostate Cancer
 New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
Con$nuing Care for Your Pa$ents with Metasta$c CRPC
 27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
January Abiraterone pre-docetaxel for patients with asymptomatic or minimally symptomatic metastatic castration resistant prostate cancer
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone pre-docetaxel for asymptomatic/minimally symptomatic metastatic castration resistant prostate cancer Abiraterone pre-docetaxel for patients with asymptomatic
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone pre-docetaxel for asymptomatic/minimally symptomatic metastatic castration resistant prostate cancer Abiraterone pre-docetaxel for patients with asymptomatic
SIMPOSIO. Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico
 SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE
 NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE S.S. Oncologia Medica Genitourinaria Outline 1. Clinical case 2. Chemotherapy
NOVITÀ IN TEMA DI NEOPLASIA DELLA PROSTATA L ALGORITMO TERAPEUTICO NEL CARCINOMA DELLA PROSTATA METASTATICO SENSIBILE ALLA CASTRAZIONE S.S. Oncologia Medica Genitourinaria Outline 1. Clinical case 2. Chemotherapy
Navigating Prostate Cancer Therapy. Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA
 Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Castrate resistant prostate cancer: the future of anti-androgens.
 Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc
 SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey
 Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi?
 ADT e Terapia ormonale: quando e a chi?") Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi? Paolo Andrea Zucali Dipartimento di Oncologia HUMANITAS CANCER CENTER Rozzano - Milano AGENDA Literature
Focus sulla malattia metastatica ormonosensibile (mhspc) ADT e Terapia ormonale: quando e a chi? Paolo Andrea Zucali Dipartimento di Oncologia HUMANITAS CANCER CENTER Rozzano - Milano AGENDA Literature
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223
 SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer?
 Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Management of castrate resistant disease; after first line hormone therapy fails
 Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
 Prostata: Oral Communications Emerging strategies and controversial topics in advanced prostate cancer Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
Prostata: Oral Communications Emerging strategies and controversial topics in advanced prostate cancer Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi
Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer. Michal Mego
 National Cancer Institute, Slovakia Translational Research Unit Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer Michal Mego 2 nd Department of Oncology, Faculty
National Cancer Institute, Slovakia Translational Research Unit Circulating tumor cells as biomarker for hormonal treatment in breast and prostate cancer Michal Mego 2 nd Department of Oncology, Faculty
Board Review 2017: Prostate Cancer. Dana Rathkopf, MD Associate Attending
 Board Review 2017: Prostate Cancer Dana Rathkopf, MD Associate Attending www.mskcc.org The Paradox of Prostate Cancer High prevalence in the general population: over diagnosis of clinically insignificant
Board Review 2017: Prostate Cancer Dana Rathkopf, MD Associate Attending www.mskcc.org The Paradox of Prostate Cancer High prevalence in the general population: over diagnosis of clinically insignificant
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
- La Terapia Farmacologica -
 XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
SUPPLEMENTARY APPENDIX. COU-AA-301 enrolled men with pathologically confirmed mcrpc who had received previous
 SUPPLEMENTARY APPENDIX Methods Subjects COUAA30 enrolled men with pathologically confirmed mcrpc who had received previous treatment with docetaxel chemotherapy and had documented PSA progression according
SUPPLEMENTARY APPENDIX Methods Subjects COUAA30 enrolled men with pathologically confirmed mcrpc who had received previous treatment with docetaxel chemotherapy and had documented PSA progression according
Published on The YODA Project (
 Principal Investigator First Name: David Last Name: Lorente Degree: MD Primary Affiliation: Medical Oncology Service, Hospital Provincial de Castellón E-mail: lorente.davest@gmail.com Phone number: +34
Principal Investigator First Name: David Last Name: Lorente Degree: MD Primary Affiliation: Medical Oncology Service, Hospital Provincial de Castellón E-mail: lorente.davest@gmail.com Phone number: +34
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Charles B. Huggins. Despite regressions of great magnitude, it is obvious that there are many failures of endocrine therapy to control the disease.
 New Concepts in ADT Leonard G. Gomella, MD Chairman, Department of Urology President Society of Urologic Oncology Sidney Kimmel Cancer Center Thomas Jefferson University Hospital Charles B. Huggins Nobel
New Concepts in ADT Leonard G. Gomella, MD Chairman, Department of Urology President Society of Urologic Oncology Sidney Kimmel Cancer Center Thomas Jefferson University Hospital Charles B. Huggins Nobel
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE. Daan De Maeseneer, Medisch Oncoloog
 PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/