Urinary Bladder Cancer
|
|
|
- Emil Bradford
- 6 years ago
- Views:
Transcription

1 Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018
2 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b bladder cancer Systemic chemo-therapy PD1/PDL1-targeted therapy Non-urothelial bladder cancers
3 Bladder cancer 4 th most frequently diagnosed cancer in American males in times more prevalent in men than women Median age at diagnosis, around 77.3 y 4.7% of all new cancer cases in % of all cancer deaths in % of new cases are non-muscle invasive Even localized disease may not be curative. 5 y Survival rate for metastatic disease 5%
4 Survival by stage: SEER data SEER,
5 Challenges in bladder cancer Elderly patient population with comorbidity & poor tolerance to aggressive treatment Under-staging by TURBT & imaging (retrospective studies showed upstage up to 41%) High recurrence after loco-regional therapy Many patients are not cisplatin-eligible Lack of efficacy from salvage chemotherapy (RR of around 10-15%) Incide nce NMIBC 70-75% 70% MIBC 20% 15% MBC 5% 5% 5 Y survival


6 Morphologic Phenotypes 70% patients present with non-invasive & 30% with muscle invasive bladder cancer. Noninvasive papillary variants are single most common variants (60%).
7 AJCC staging, 2010 (7 th Ed) Level of invasion TNM Stage Ta Noninvasive papillary carcinoma T1N0M0 0a Tis Carcinoma in situ, flat TisN0M0 0is T1 Sub-epithelial connective tissue T1N0M0 I T2 Muscularis propria T2N0M0 II T3 Peri-vesical tissue (T3a: microscopic, T3b: macroscopic) T3N0M0 T4 T4a: prostate, uterus,vagina T4aN0M0 III T4b: pelvic or abdominal wall T4bN0M0 IV III N N1: single. N2: Multiple, N3: to Common iliac Tany Nany M0 IV M1 Distant metastasis Tany Nany M1 IV

8 Urinary Bladder Carcinogenesis Knowles & Hurst, Nat Rev Cancer, 2015
9 Non-muscle invasive bladder cancer

10 T stage 5 y recurrence rate Ta, Low Grade 50% Ta, High Grade 60% T1, Low-grade 50% T1, High grade 50%-70% Tis 50-90% NCCN V2.2015
11 Management of NMIBC TURBT is the mainstay of therapy Post-op intra-vesical therapy (BCG, mitomycin, doxorubicin) is needed for majority of NMIBCs Size, multifocal dz & prior recurrence are predictive of recurrence Close surveillance is critical with cystoscopy & urine cytology Recurrent NMIBCs & T1 high-grade cancers should be considered for cystectomy

12 Patient A A 75 yo M presented with 3 months of painless hematuria. PMHx included CAD with stents, HTN & DM. Cystoscopy shows a 2 cm papillary tumor. CT urogram showed no extra-vesical extension or hydronephrosis. Patient underwent TURBT. Pathology showed pt1 urothelial carcinoma with muscle in the specimen, but not involved What is the next step 1. Intravesical BCG 2. Cystectomy 3. Early repeat TURBT 4. Observation
13 Restaging TURBT: 27-78% patients can be under-staged in initial TURBT. Up to 30% can be upstaged to muscle invasive disease Early repeat TURBT (within 6 weeks) is indicated if Incomplete initial resection No muscle in specimen for high-grade dz Large (3 cm or more) or multifocal lesion Any T1 lesion All HG/G3 lesions, except primary CIS IBG 2011, EAU 2013
14 Patient A, continued Patient A underwent a repeat TURBT in 4 weeks. Pathology showed highgrade T1 tumor with adequate muscle in specimen. There is no evidence of muscle invasion What is the next step: 1. BCG 2. Early cystectomy 3. Intra-vesical chemotherapy 4. Observation
15 Indication for cystectomy in NMIBC Multiple, recurrent, HG tumors HG T1 tumors HG tumors with CIS Micro-papillary variant Muscle invasive on re-resection
16 SWOG-1605 Phase 2 trial of Atezolizumab in BCG-unresponsive non-muscle invasive bladder cancer (Ta/T1/ CIS) Open in VCU Massey Cancer Center 01/2018
17 MIBC & advanced bladder cancer T2-T4a T4b N+ : NA Chemotherapy -> radical cystectomy : Chemotherapy +- radiation : Chemotherapy +- radiation Metastatic : Systemic therapy NCCN V1.2018
18 Cystectomy in muscle-invasive bladder cancer Radical cystectomy is the primary treatment option for ct2, ct3, ct4a disease Should be preceded by neoadjuvant chemotherapy in cisplatin-eligible patients Bilateral pelvic lymphadenectomy is performed along with cystetcomy Partial cystetcomy is an option in carefully selected patient ct2 dz and a solitary lesion no CIS

19 5-year survival after cystectomy
20 Stein, JCO, 2001 While radical cystectomy had an acceptable outcome in bladder-confined disease in this series, there was a high recurrence rate & low-survival in patients with extra-vesical & node-positive disease. Adjuvant chemotherapy did not have an impact.


21 Patient with T2-T4a, MIBC Randomized to MVAC -> RC or RC Improved survival in MVAC->RC vs. RC alone Improved survival in patient with no residual disease after RC (38% vs. 15%, P<0.001) SWOG 8710, Grossman, NEJM, 2003

22 Selected neo-adjuvant randomized trials

23 11 trials, 3005 patients NA platinum-based combination, HR 0.86, P=0.003 Absolute benefit over 5 years, OS 5%, PFS 9% Eur Urology, 2005
24 Neoadjuvant Gem-Cis vs ddmvac/ MVAC: retrospective data Patients with ct2-ct4anomo, 28 centers Median age 63 years ddmvac/ MVAC, 3 cycles Patients Gem-Cis, 3 cycles pcr 29% 31% HR 0. 78, CI ,P=NS Galsky, Cancer, 2015


25 39 patients received 4 cycles of cis/gem prior to cystectomy At cystectomy, pt0 was 26%, <pt2 was 36%, comparable to MVAC (28% & 35%) All GC patients achieving <pt2 remained disease free at 30 months after cystectomy Dash, Cancer, 2008
26 Neoadjuvant Chemotherapy NAC is now standard for MIBC (T2-T4a), but is underutilized, used in about 20% of patients NAC should be offered to all cisplatin-eligible patients Cisplatin should not be substituted by carboplatin NAC has the benefit of down-staging disease, leading to better surgery & survival. Studies showed benefit from several cisplatin-based regimens, such as dd-mvac. MVAC & CMV. Cisplatin & gemcitabine (3 months) is used in USA because of toxicity of MVAC regimen. Phase II data showed feasibility of fractionated cisplatin with gemcitabine in patient with GFR ( Hussain,Cancer Letter, 2012) No data support use of adjuvant chemotherapy in patients with residual disease after NAC
27 Patient B, continued Mr B, A 68 yo patient with DM, HTN, CKD stage II & pt3 bladder cancer underwent radical cystectomy, b/l pelvic lymphadenectomy & ileal conduit. Pathology confirmed pt3, high-grade urothelial Ca with 1 of 3 pelvic LNs (external iliac) positive. Margins were negative. Patient s egfr improved to 60 ml/min at 4 weeks of surgery. Staging work-up was negative for distant metastasis What is the best next step? 1. Adjuvant chemotherapy with carboplatin 2. Adjuvant chemotherapy with cisplatin 3. Adjuvant radiation therapy 4. Observation
28 Who needs additional therapy after cystectomy?
29 Recurrence Survival Based on >9000 patients who received cystectomy and pelvic lymph node dissection in 12 centers J Clin Oncol 2005

30 nav=1&audience=1

31 PENN risk for local failure
32 Leow, Eur Eurology, patients in 9 RCTs pt2-t4a and or N+ HR for OS, 0.77 (CI: ) P=0.049 HR for DFS, 0.66, CI , P=0.014 DFS was more among patient with positive nodal status (P=0.010)

33 5653 patients, National cancer data base, pt3-t4 and or N+ All patient received multi-agent chemotherapy Improvement of OS (HR 0.70, CI ) Improved survival was consistent in all subgroups Galsky, JCO, 2016
 who did not receive NAC.")
34 Randomized adjuvant chemotherapy trials Prospective adjuvant studies in bladder cancer are inconclusive. Meta-analysis of RCTs, retrospective studies & recent data showed benefit of AC in patients (pt3-t4, N+) who did not receive NAC. Most of the benefit were from Cisplatin-based combination chemotherapy (MVEC, GC). Sonpavde, JCO, 2016

35 Role of adjuvant PD1/PDL1 therapy? To open in VCU soon
 with 48% disease free at 5 years, compared to 31.8% in deferred group No overall survival benefit in immediate vs.")
36 Option for deferred adjuvant treatment: EORTC trial Patient with T3,T4 or N+, following radical cystectomy Immediate adjuvant MVAC (max 4 cycles) or chemo at relapse (max 6 cycles). Median follow-up 7 years Immediate treatment prolonged DFS (HR 0.54, P<0.0001) with 48% disease free at 5 years, compared to 31.8% in deferred group No overall survival benefit in immediate vs. deferred group (5 y OS: 53.6% vs 47.7%) Sternberg, Lancet Oncol, 2015
37 Role of radiation in bladder cancer Settings Post-cystectomy adjuvant Bladder sparing chemo-radiation Definitive chemoradiation Palliative Candidate ct3, N+, positive margin ct2, ct3a T4b uncontrolled hematuria, large bladder mass with pain, oligometastatic lesion, solitary recurrence after cystectomy

38 Post-operative Radiotherapy Retrospective Study from Egypt 61% urothelial, 31% squamous DFS & locoregional control No survival benefit Bayoumi, Ca Manag Res, 2014 Data on adjuvant radiation is limited. Adjuvant radiation is reasonable in selective patients with pt3-t4 patients and patients with +ve surgical margin, because of risk of high local recurrence (32% & 68% respectively)
39 Bladder-preserving chemoradiation therapy Alternative to cystectomy in patients o Who are not a candidate for cystectomy o Who wants to preserve bladder
40 Bladder preserving chemo-radiation o Smaller, solitary tumor o T2 or T3a o Negative LNs o No CIS o No hydronephrosis Chemotherapy used with radiation: Cisplatin, paclitaxel, 5FU+mitomycin, Cisplatin+ Gemcitabine Reported outcome in MIBC: CR 60-80%, 5 y DFS 60-70%, Bladder-intact survival 40-45%, 5 y OS 57%, 10 Y OS 36%


41 Mak, J Clin Oncol, 2014
42 Phase III study Chemo-radiation therapy vs. Radiation alone 360 patients with MIBC Chemo-radiation arm includes: 5FU (500 mg/m2) with F1-5, F Mitomycin (12 mg/m2) D1 Radiation Radiation arm 55 Gy 20F, 64 Gy in 32 F 2 Y locoregional survival, 67% vs. 54%, HR 0.68, P= Y OS: 48% vs. 35%, HR 0.82 GIII-IV toxicity: 36% vs 27.5% BC2001, James, NEJM 2012

43 Meta-analysis of 8 studies including 9,554 patients 5 y or 10 y overall survival and PFS were not different between cystectomy & CMT: Not different Vahistha, Int J Rad Bio Phy, 2017

44 Vahistha, Int J Rad Bio Phy, 2017
45 Bladder Preserving Approach in VCU T2 MIBC Maximal TURBT Concurrent Chemo-radiation RTOG 8903* Pelvic RT daily to 39.6 Gy + cisplatin 100 mg/m2, Q 3 weeks X 2 Re-biopsy CR on Rebiopsy: Consolidation RT to 25.2 Gy + Cisplatin 100 mg/m2x 1 Residual disease on rebiopsy: Cystectomy Close cystoscopic monitoring, q 3 months *Shilpley, J Clin Oncol 1998
46 T4b Bladder cancer NCCN V1.2008
47 Metastatic Bladder Cancer
48

49 MBC: 1 st line Gemictabine/Cisplatin is the standard front line in US Split-dose cisplatin is better tolerated Carboplatin can substitute cisplatin in patients with GFR ml/min. RR 30-60%, Median PFS <1 year
50 Chemotherapy in mbc
51 ddmvac vs. MVAC: EORTC Metastatic bladder Ca, 263 patients ddmvac vs. MVAC CR 21% vs. 9%, ORR 62% vs. 50% *7 years updated survival analysis: PFS 9.5 m vs 8. 1 m, HR 0.76 Median OS 15.1 m vs months Progression-free survival Sternberg, J Clin Oncol, 2001 Sternberg. Eur J Cancer, 2006
52 Gem-Cis vs. MVAC: randomized phase III Stage IV, GC (n=203), MVAC (n=202) TTPD, TTF, OS were comparable GC was better tolerated than MVAC More GC patients completed 6 cycles Von Der Mosse, J Clin Oncol 2000
53 GC vs. MVAC: updated survival data Progression-free survival Overall survival Long-term FU confirmed comparable PFS & OS 5 Y OS rate: 13.0% vs. 15.3% (P=NS) Base-line PS & visceral metastasis had the highest impact on survival Von Der Mosse, J Clin Oncol 2005



54 Carboplatin-Gemcitabine in patient cisplatin-ineligible patients: EORTC Carboplatin D1 AUC 4.5 ; Gem D1, 8, Q21 D De Santis, J Clin Oncol, 2009

55 Salvage therapy in Bladder Cancer Sonpavde, Lancet Oncol, 2010

56 Ramucirumab & Docetaxel as 2 nd line: Phase II data Petrylak, J Clin Oncol, 2016

57 Retreatment with cisplatin-based regimen Recurrent Initial response & >6 months off treatment Resistant Refractory Initial response, but recurrence within 6 months of treatment No response, progression while on treatment Retreatment Yes No No Han BJC 2008, Edeline EJC 2012, Lee Cancer Res Treat 2014
58 PD-1/PD-L1 targeted therapy i

59 FDA approved PD1/PDL1 targeted immunotherapy in bladder cancer Drug Target Approval Pemborlizumomab PD1 May 2017 Avelomab PD-L1 May 2017 Dervalumab PD-L1 May 2017 Nivulomab PD-1 Feb 2017 Atezolizumab PD-L1 May 2016


60 PD-1/PD-L1 blockade in metastatic urothelial cancers: Major Trials

61 PD-1/PD-L1 blockade: response across the trials

62

63 1 st line: Cisplatin ineligible patients Chism, JNCCN 2017
64 Imvigor: Phase II of Atezolizumab in cisplatin-ineligible patients Balar et al, Lancet Oncol 2017 (Dec 2016)


65 Keynote 052: First-line pembrolizumab in cisplatin-ineligible patients, Phase 2 Balar et al, Lancet Oncol 2017 (Sept 2017)

66 2 nd line in Cisplatin-treated patients Chism, JNCCN 2017


67 Keynote 045: Phase 3 pembrolizumab vs. chemotherapy in platinum-treated patients PD-L1 expression: 10% or more Bellmunt et al, NEJM 2017 (Feb 2017)

68 Grade 3 or more AES: 15% vs 49% Belmunt et al, NEJM, 2017
 of choice (Vinflunine, paclitaxel or docetaxel) Patients with PDL1 5%, OS & PFS were not different ORR 23% vs. 22%, DOR 15.9 m vs. 8.")
69 Imvigor 211: Phase III Atezolizumab vs chemotherapy Platinum treated patients Atezolizumab (n=467) vs. Chemotherapy (n=464) of choice (Vinflunine, paclitaxel or docetaxel) Patients with PDL1 5%, OS & PFS were not different ORR 23% vs. 22%, DOR 15.9 m vs. 8.3 m, AES 20% vs. 43% Powles et al, Lancet Oncol 2017 (Dec 2017)

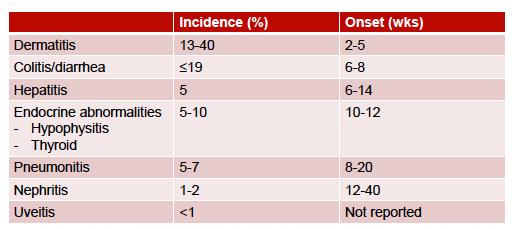
70 Selected Immune-mediated toxicities NCCN Webinar, 2018
71 Bladder cancer: Summary Multidisciplinary discussion is critical NMIBC has high-recurrence rate despite of localized therapy NAC should be considered for all cisplatin-eligible & T2-T4a, N0M0 BC. Cisplatin should not be substituted by carboplatin in NAC setting Radical Cystectomy for T2-T4a, N0M0 AC may be offered for high-risk patients (T3-T4, N+), who did not receive NAC Bladder preservation approach for selective patients (T2), although prospective data vs. cystectomy is lacking Cisplatin-based regimen for metastatic dz. Carboplatin based regimen or immunotherapy are the choices for cisplatin- ineligible patients RR of 2 nd line chemotherapy is low. Five PD1/PD-L1 targeted drugs have been approved for platinum-treated patients. Pembrolizumab showed survival over chemotherapy in 2 nd line setting and is the current standard of care.
 -> Cystetcomy or radiation Rx as small cell lung cancer ITP (Ifosfamide/ Paclitaxel/ Cisplatin) No role of NAC/AC, 5")
72 Non-urothelial bladder cancer Mixed with urothelial Any small cell component: Localized disease Any small cell component: Metastatic disease Pure Squamous Pure adenocarcinoma Treat as Urothelial CA NAC (Cis/etop) -> Cystetcomy or radiation Rx as small cell lung cancer ITP (Ifosfamide/ Paclitaxel/ Cisplatin) No role of NAC/AC, 5 FU, GemFLP
UROTHELIAL CELL CANCER
 UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Options for first-line cisplatin-eligible patients
 The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
The Past Options for first-line cisplatin-eligible patients Metastatic urothelial cancer Cisplatin-eligible Gemcitabine/ cisplatin MVAC or high-dose intensity MVAC Paclitaxel/ cisplatin/ gemcitabine Bellmunt
Treatment of muscle invasive bladder cancer. ie: pt2. N. Mottet
 Treatment of muscle invasive bladder cancer ie: pt2 N. Mottet Disclosures Astellas BMS Pierre Fabre Sanofi MIBC: really undertreated 28 691 MIBC in the US (national database). Gray Eur Urol 2013 Patients
Treatment of muscle invasive bladder cancer ie: pt2 N. Mottet Disclosures Astellas BMS Pierre Fabre Sanofi MIBC: really undertreated 28 691 MIBC in the US (national database). Gray Eur Urol 2013 Patients
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015
 Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Case 1. Receives induction BCG weekly x 6 without significant toxicity Next step should be:
 Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Neodjuvant chemotherapy
 Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Urothelial Cancers- New Strategies. Sandy Srinivas.MD Stanford University
 Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
Urothelial Cancers- New Strategies Sandy Srinivas.MD Stanford University Relevant financial relationships in the past twelve months by presenter or spouse/partner. Consultant: Genentech, Astra Zeneca The
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
AUA Guidelines for Invasive Bladder Cancer: What s New?
 AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
RECENT DEVELOPMENTS in Muscle Invasive Bladder Cancer
 RECENT DEVELOPMENTS in Muscle Invasive Bladder Cancer IX CIS and EURASIA ONCOLOGY and RADOLOGY CONGRESS, ONCOUROLOGY SESSION 16 June 2016 Richard E Greenberg, MD, FACS Chief Urologic Oncology, Fox Chase
RECENT DEVELOPMENTS in Muscle Invasive Bladder Cancer IX CIS and EURASIA ONCOLOGY and RADOLOGY CONGRESS, ONCOUROLOGY SESSION 16 June 2016 Richard E Greenberg, MD, FACS Chief Urologic Oncology, Fox Chase
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
PREVENTION & SCREENING
 A) PUBLIC HEALTH EPIDEMIOLOGY Incidence: 16 per 100,000 (males 26 per 100,000, females 7 per 100,000). Accounts for 6.1% of all new male cancer cases and 2.1% of all new female cancer cases in Canada.
A) PUBLIC HEALTH EPIDEMIOLOGY Incidence: 16 per 100,000 (males 26 per 100,000, females 7 per 100,000). Accounts for 6.1% of all new male cancer cases and 2.1% of all new female cancer cases in Canada.
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer
 Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Old and New Radiation for Bladder and Upper Tract Cancers. Bridget Koontz Radiation Oncology Duke Cancer Institute
 Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Non Muscle Invasive Bladder Cancer. Primary and Recurrent TCC 4/10/2010. Two major consequences: Strategies: High-Risk NMI TCC
 Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Bladder Cancer. Clinical Case Conference
 Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
Bladder Cancer Clinical Case Conference Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
I Tumori della Vescica Inquadramento clinico Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena
 I Tumori della Vescica Inquadramento clinico Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena XII Corso di aggiornamento AIRTUM per operatori dei Registri Tumori Reggio Emilia
I Tumori della Vescica Inquadramento clinico Roberto Sabbatini Azienda Ospedaliero Universitaria Policlinico di Modena XII Corso di aggiornamento AIRTUM per operatori dei Registri Tumori Reggio Emilia
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO
 AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO Montse Domènech Althaia, Xarxa Assistencial i Universitària Manresa Urothelial Cancer Therapeutics FDA approved drugs for bladder
AVANCES EN EL TRATAMIENTO DE PRIMERA LINEA EN EL CANCER DE VEJIGA AVANZADO Montse Domènech Althaia, Xarxa Assistencial i Universitària Manresa Urothelial Cancer Therapeutics FDA approved drugs for bladder
Oral Communications & Posters
 Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
Carcinoma uroteliale: Current and future directions of treatment of Muscle-Invasive Bladder cancer/ Multimodality approach of bladder cancer Oral Communications & Posters CRISTINA MASINI Oncologia Medica
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016
 BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
Open clinical uro-oncology trials in Canada
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
Invasive Bladder Transitional Cell Carcinoma OBJECTIVES
 Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Reviewing Immunotherapy for Bladder Carcinoma In Situ
 Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer
 Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Management options for high-risk, BCG-refractory NMIBC. Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center
 Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Cochrane metaanalysis 5 year OS Intent to treat
 RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline
 Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Prostate cancer Management of metastatic castration sensitive cancer
 18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
18 th Annual Advances in Oncology - 2017 Prostate cancer Management of metastatic castration sensitive cancer Urothelial carcinoma Non-muscle invasive urothelial carcinoma Updates in metastatic urothelial
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent
 Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent Jehonathan H Pinthus MD, Ph.D, FRCSC Associate Professor Department of Surgery/Urology McMaster University Life expectancy Current age
Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent Jehonathan H Pinthus MD, Ph.D, FRCSC Associate Professor Department of Surgery/Urology McMaster University Life expectancy Current age
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Controversies in the management of Non-muscle invasive bladder cancer
 Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Gynecologic Cancer InterGroup Cervix Cancer Research Network. Management of Cervical Cancer in Resource Limited Settings.
 Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Management of Cervical Cancer in Resource Limited Settings Linus Chuang MD Conflict of Interests None Cervical cancer is the fourth most common malignancy in women worldwide 530,000 new cases per year
Breast cancer Can I still keep my breast?
 Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BJUI. 35% had lymph node involvement at radical cystectomy or subsequent recurrence within the dissection template.
 2010 THE AUTHORS; 2010 Urological Oncology LYMPH NODE STATUS IN PT0 BLADDER CANCER KAAG ET AL. BJUI Regional lymph node status in patients with bladder cancer found to be pathological stage T0 at radical
2010 THE AUTHORS; 2010 Urological Oncology LYMPH NODE STATUS IN PT0 BLADDER CANCER KAAG ET AL. BJUI Regional lymph node status in patients with bladder cancer found to be pathological stage T0 at radical
Challenges in systemic treatment for metastatic bladder cancer. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Challenges in systemic treatment for metastatic bladder cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University OS PCG 15.8 vs GC 12.7 NS Cisplatin ineligible Second-line chemotherapy
Challenges in systemic treatment for metastatic bladder cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University OS PCG 15.8 vs GC 12.7 NS Cisplatin ineligible Second-line chemotherapy
Panel: A Case-based Approach to the Management of Bladder Cancer
 Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
Chemo-radiotherapy in muscle invasive bladder cancer. Dr Paula Wells St Bartholomew s Hospital London
 Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
Bladder Preservation Protocols in the Treatment of Muscle-Invasive Bladder Cancer
 Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Urothelial Carcinoma Highlights
 Urothelial Carcinoma Highlights Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano European Association of Urology Research Foundation Disclosures Consulting or Advisory Role: Company:
Urothelial Carcinoma Highlights Andrea Necchi Fondazione IRCCS Istituto Nazionale dei Tumori, Milano European Association of Urology Research Foundation Disclosures Consulting or Advisory Role: Company:
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
BCG Unresponsive NMIBC: What s Available?
 BCG Unresponsive NMIBC: What s Available? Michael S. Cookson, MD, MMHC, FACS Professor and Chair Department of Urology University of Oklahoma TwiLer @uromc Professional Practice Gap Gap 1: There is incomplete
BCG Unresponsive NMIBC: What s Available? Michael S. Cookson, MD, MMHC, FACS Professor and Chair Department of Urology University of Oklahoma TwiLer @uromc Professional Practice Gap Gap 1: There is incomplete
Neoadjuvant chemotherapy for bladder cancer: fighting between evidence 1 level and real life.
 THE INTERNATIONAL CONFERENCE PROGRESS IN URO-ONCOLOGY 5th Edition September, 25th 26th 2014 CLUJ-NAPOCA Neoadjuvant chemotherapy for bladder cancer: fighting between evidence 1 level and real life. Dr.
THE INTERNATIONAL CONFERENCE PROGRESS IN URO-ONCOLOGY 5th Edition September, 25th 26th 2014 CLUJ-NAPOCA Neoadjuvant chemotherapy for bladder cancer: fighting between evidence 1 level and real life. Dr.
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Organ-sparing treatment of invasive transitional cell bladder carcinoma
 Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D.
 Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Neoplasie uroteliali Posters & oral presentations
 UPDATES and NEWS from the Genitourinary Cancers Symposium 3 Marzo 2017, Milano Neoplasie uroteliali Posters & oral presentations Cristina Masini Oncologia Medica IRCCS-Arcispedale S.Maria Nuova - Reggio
UPDATES and NEWS from the Genitourinary Cancers Symposium 3 Marzo 2017, Milano Neoplasie uroteliali Posters & oral presentations Cristina Masini Oncologia Medica IRCCS-Arcispedale S.Maria Nuova - Reggio
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
THE SEARCH FOR BIOMARKERS IN BLADDER CANCER
 THE SEARCH FOR BIOMARKERS IN BLADDER CANCER CDDP and IO WORLD ALEJO RODRÍGUEZ-VIDA MD PhD Consultant Medical Oncologist Associate Professor Hospital del Mar, Barcelona November 23 rd 2018 DISCLOSURE OF
THE SEARCH FOR BIOMARKERS IN BLADDER CANCER CDDP and IO WORLD ALEJO RODRÍGUEZ-VIDA MD PhD Consultant Medical Oncologist Associate Professor Hospital del Mar, Barcelona November 23 rd 2018 DISCLOSURE OF
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Impact of adjuvant chemotherapy on patients with pathological Stage T3b and/or lymph node metastatic bladder cancer after radical cystectomy
 Japanese Journal of Clinical Oncology, 2015, 45(10) 963 967 doi: 10.1093/jjco/hyv098 Advance Access Publication Date: 29 July 2015 Original Article Original Article Impact of adjuvant chemotherapy on patients
Japanese Journal of Clinical Oncology, 2015, 45(10) 963 967 doi: 10.1093/jjco/hyv098 Advance Access Publication Date: 29 July 2015 Original Article Original Article Impact of adjuvant chemotherapy on patients
BCG Unresponsive Disease A Roadmap for Drug Development and Integra;on of Novel Therapies
 BCG Unresponsive Disease A Roadmap for Drug Development and Integra;on of Novel Therapies Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College of
BCG Unresponsive Disease A Roadmap for Drug Development and Integra;on of Novel Therapies Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College of
Pancreatic Adenocarcinoma
 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Treatment of Advanced Bladder Cancer, Where We've Been and How to Move Forward
 Treatment of Advanced Bladder Cancer, Where We've Been and How to Move Forward Maha Hussain, MD, FACP Professor of Medicine & Urology Co-Leader Prostate/GU Oncology Program Associate Director for Clinical
Treatment of Advanced Bladder Cancer, Where We've Been and How to Move Forward Maha Hussain, MD, FACP Professor of Medicine & Urology Co-Leader Prostate/GU Oncology Program Associate Director for Clinical