GENITOURINARY PATHOLOGY RESIDENT ROTATION DESCRIPTION (5/09)
|
|
|
- Ronald Perry
- 6 years ago
- Views:
Transcription
1 GENITOURINARY PATHOLOGY RESIDENT ROTATION DESCRIPTION (5/09) This rotation encompasses the evaluation of genitourinary pathology and deals with bladder, prostate, kidneys, penis and testis. It also includes, for historical reasons, adrenal tumors. The volume of pathologic specimens on this service has increased and continues to do so which should enhance the learning experience. This, however, requires the resident to be more than a passive observer and necessitates that the resident take responsibility for the efficient operation and complete accurate pathologic reports. Specimens must be grossed in and examined in an expeditious manner to ensure excellent clinical service to patients and our colleagues in the department of Urology. The rotation description, cancer checklists, educational materials and reference articles have been placed on the web. The web address is the current username is allan_robert@hotmail.com and the password is: GUPATH. PATHOLOGISTS: The Genitourinary Division has three pathologists with specialty interest and experience in Genitourinary pathology. Names and contact numbers for each are as below: Robert Allan, MD (pager , Shands cubicle ) Peter Drew, MD (pager , office ext , AGH ) Samer Al-Quran (pager , Shands cubicle ) WHAT TO DO ON DAY ONE: 1) Prior to the rotation Dr. Allan should have ed you the GU rotation description, read it and print this out. 2) On so-called switch day page Dr. Allan ( ), if he does not answer right away keep paging him. 3) Dr. Allan will meet with you and go over the resident rotation description form step by step and have you sign an acknowledgment that you have reviewed it (at the end) 4) If Dr. Allan is not at Shands that day, he will do this over the telephone. 5) If Dr. Allan is not in town, then have either Dr. Drew or Dr. Al-Quran go over the rotation description and sign the form. GUIDELINES FOR SIGN-OUT:
2 Pathology is best learned by doing and not by passively watching from the other side of the microscope. Even if this is your first day of doing GU or your first day of residency, you are expected to preview the slides prior to signing out the cases with the attending. Practicing pathologists often encounter situations where they have not seen or signed out a particular type of case and must learn how to do this; it is best learned while you are still in-training. PREVIEWING CASES: It is understood that previewing may take longer the first time on the rotation. However, if it is observed that you are not using this time wisely, the attending may cut this time short and ask to review the cases. It is expected that all resection cases be signed out within two days of grossing and biopsy cases be signed out as expeditiously as possible. One strategy to help achieve this is to quickly preview cases first thing in the morning (before conference if possible) and order immunohistochemical or special stains on those cases as soon as possible. As a specific example, scan the middle level slides of all the prostate needle cores of prostate biopsies to determine if there are slides which have a small focus that may be cancer that may need immunohistochemical stains. If there is doubt, grab the attending on service and ask if they would like immunohistochemical stains on that particular case. Cases marked RUSH are to be signed out in the morning with the attending. REPORTING: An important part of diagnostic pathology is the phrasing and structure of a coherent report. This should be complete in scope and devoid of typographical errors or blanks. This means that the gross description should be checked for accuracy and corrected. For the diagnosis, it is important for clarity and in many instances billing compliance to document the procedure that is performed as part of the diagnosis. Charge codes are different, for example, for a bladder biopsy (88305) and a TURBT (88307). The preferred format is shown in the following examples. Bladder, biopsy Bladder, TURBT Prostate, TURP Left apex, prostate, biopsy Left kidney, radical nephrectomy Right kidney, partial nephrectomy "Tumor mass in retroperitoneum", excision As noted in the last example, sometime the surgeon designates a specimen without a clear anatomic location-- in this instance put the location in parentheses. The generic procedure "excision" can be used if there is doubt as to the procedure.
3 Abbreviations are to be avoided with the exceptions shown above (TURBT, TURP). These are awfully long and it is well understood what they mean. Using BX, for example, as a shortened form of biopsy is unacceptable. An additional specimen that is very common is confirming diagnosis slides from outside facilities. These are to be written up in the following standardized manner in keeping with the department recommendations. If there are multiple biopsies under a given heading it is easier to group these with a header and list the different anatomic sites separately As examples, A) Prostate, biopsies, review of outside slides, XS , 1/12/08 Left apex: Adenocarcinoma of the prostate, Gleason 6 (3+3), involving 20% of one core, 3mm, perineural invasion is identified Left base: Negative for tumor etc. etc. A) Bladder, TURBT, review of outside slides XJ , 11/15/07 Invasive high grade urothelial carcinoma Carcinoma invades muscularis propria (detrusor muscle) etc. Please check to make sure that the slides reviewed match those in the gross description and are placed in the diagnostic line. This is because the gross is not transferred in the history tab display when looking at prior history. It is important to include the date of the procedure because many patients have received multiple treatments at multiple time points (bladder tumor patients) and this avoids confusion as to when the biopsy was done. This should be printed on the outside pathology reports. I have included some sample sign-outs at the end of this document for reference. Oncologic genitourinary pathology resection cases are REQUIRED to have a diagnostic cancer checklist in the footing of the report to ensure standardizing of cancer reporting. There are many reasons for this. First, the Urology department has asked that this be made part of our reports to assist in translational research activities. Second, the American College of Surgeons (ACS) requires that institutions that are certified as cancer centers through the ACS Commission of Cancer (ACS COC) include certain required elements in their reports and devised cancer checklists, in concert with the College of American Pathologists (CAP). Third, Medicare has begun including small monetary incentives to tumor cases (currently breast and colon) that include certain relevant tumor characteristics and tumor stage (ptnm). If these are not included, reimbursement is less. Finally, many private practice and other academic positions have adopted checklist reporting formats-- so it is likely that you will do it when you leave here and thus it can be considered part of your training.
4 The checklists have been placed on web and are accessible with username and password provided-- the web address is the current username is and the password is: GUPATH. I tried keeping them on the sign-out room computers but they have, at times, been deleted. In addition, the balkanization of the computer network between UF and Shands precludes any unified accessible network drive. This way you can get it from anywhere, including home. For biopsies containing cancer there are certain required elements that depend on the anatomic site. The two major sites are prostate and bladder. For prostate carcinomas on core biopsy report the following: Prostatic adenocarcinoma, Gleason score 7 (3+4), involving 30% of one of two cores, maximal linear extent 4mm, perineural invasion is present As shown this includes the Gleason score, percent involvement and number of cores, maximal linear measurement and, if present, perineural invasion. The absence of perineural invasion does not need to be reported. If there are discontinuous foci of carcinoma on a core it can be reported as "discontinuously involving 40% of core, 5mm in overall extent". For bladder tumors it is important to mention the type and grade of tumor and in addition report the presence of absence of the bladder muscularis propria (detrusor muscle) in the specimen. This is to determine the adequacy of the specimen for pt grading. A common way to report this is "Muscularis propria (detrusor muscle) is present and uninvolved by carcinoma". GROSSING FOR GU Grossing is to be performed on a daily basis; all tumor cases are to be handled by the residents. Should case load become unwieldy, it is acceptable to request assistance from the PAs. It is not acceptable to delay grossing in specimens. If there are questions about grossing these can be handled by the PAs or the GU pathology attending on service. Taking gross photographs of tumor cases is strongly encouraged. Diagrams of sections are highly encouraged. There are certain recurrent issues that warrant particular attention in grossing GU specimens. The GU portion of the grossing manual is available in electronic form. - The lymph node dissections of bladder, ureter and testicular/germ cell tumor the size of grossly positive lymph nodes should be measured. - Sample testicular tumors well- if feasible err on the side of submitting the entire tumor - Weigh adrenals
5 - For nephrectomy specimens, an important and usually undersampled area of tumor involvement is the relationship of the tumor to the renal sinus-- the fat in the hilum of the kidney. Make sure this is well sampled as some small (otherwise T1) tumors get upstaged to T3 if this is involved. Also, palpable the hilar fat for a lymph node-- if you feel something submit it, otherwise put in a section of hilar fat to look for a lymph node. RECOMMENDED READING: 1. Epstein, JI. et al. The World Health Organization International Society of Urological Pathology Consensus Classification of Urothelial (Transitional Cell) Neoplasms of the Urinary Bladder, American Journal of Surgical Pathology, 1998; 22; Epstein JI, et al. The 2005 International Society of Urologic Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma, American Journal of Surgical Pathology, 2005; 29; Zhou and Magi-Galluzzi. Genitourinary Pathology. 2007; Churchill Livingstone. 4. Epstein JI, Amin MB, Reuter VE. Bladder Biopsy Interpretation. 2002; Lippincott, Williams and Wilkins. 5. Murphy WM. Urologic Pathology, 2 nd Edition. 1997; WB Saunders. GU TUMOR BOARD The GU tumor board is held weekly at 7:00 AM in the Shands Medical Plaza, Radiation Oncology Conference Room, Rodney Million Room. The Urology department selects cases, many of which will have pathology slides for review. You may be asked to assist in collection material for tumor board conference and you are free to review the cases for conference if you so choose. It is understood that this conference conflicts with the scheduled morning lectures so attendance is difficult if not impossible. However, if there is no conference than attendance is strongly recommended. It is actually one of the better tumor boards. AGH During this rotation you may be signing out with a pathologist that is over at AGH. There is no agreed upon solution to this problem at present as resident are paired with another rotation during this month (i.e. GU/ENT) and this makes going back and forth difficult. One reasonable solution is to split the weeks on the rotation to a week of ENT then a week of GU or two preview both services, send the slides over to AGH after preview with the attending at AGH sending the cases back with follow-up comments. DR. MURPHY Dr. Murphy is coming to the department two days a week-- typically alternating Mon- Wed and Tues-Thursday and will be available for teaching and reviewing cases. Please try to avail yourself of this resource. ROTATION ASSESSMENT Resident evaluation will be done as a consensus opinion of attendings on service. The criteria for evaluation are similar to those of other services.
6 An end of rotation slide and knowledge evaluation is in development and may be initiated at the end of the rotation. As mentioned, this is in development and will consist of slides and a computer based images and knowledge evaluation. In addition, there are currently self-directed tutorials with examinations for Gleason grading of prostate carcinoma and bladder biopsies (normal, reactive, papillary lesions, dysplasia, carcinoma in-situ, invasive carcinoma). These are accessible on the website ( These have self-assessment modules at the end- Dr. Allan has the answers and will go over these when you are finished. Additional modules are currently in development for adult and pediatric renal tumors. ACKNOWLEDGEMENT OF RECEIPT: Print name: Signature: Date: GU Attending Print name: Signature: Date:
7 SAMPLE SIGNOUTS: Prostate biopsies: A) Prostate, left apex, biopsy: Benign prostatic tissue B) Prostate, left mid, biopsy: Prostatic adenocarcinoma, Gleason 6 (3+3), involving 20% of 1/1 cores, 3mm, perineural invasion is present Outside prostates: A) Prostate, biopsies, Review of outside slides, SP , 1/12/08 Left apex: Benign prostatic tissue Left mid: Prostatic adenocarcinoma, Gleason 6 (3+3) involving 10% of multiple fragmented cores, maximal extent 4mm Bladder: A) Bladder, TURBT Invasive high grade urothelial carcinoma Carcinoma invades lamina propria Muscularis propria (detrusor muscle) present and negative for carcinoma Negative for angiolymphatic invasion For the checklist-- delete the unused elements and keep the pathologic staging criteria Prostate, robot-assisted radical prostatectomy Prostatic adenocarcinoma, Gleason score 7 (3+4), tertiary pattern % Tumor predominantly involves left apex Maximal tumor nodule diameter measured on one slide: 1.3 cm (slide C3) Percent of prostate gland involved by tumor 15% (4 /25 tissue blocks contain tumor) Extraprostatic extension: Present- Focal, specify site: left mid posterior, 4 mm in extent Margins: Margins uninvolved by invasive carcinoma Angiolymphatic invasion: Absent Seminal vesicle invasion: Absent Pathologic Staging (ptnm) pt3a pn0 pmx Primary Tumor (pt)pt3a: Extraprostatic extension Regional Lymph Nodes (pn) pn0: No regional lymph node metastasis (0/4 lymph nodes 0/2 Left, 0/2 right) Distant Metastasis (pm)pmx: Distant metastasis cannot be assessed
8 GU PATHOLOGY CANCER CHECKLISTS WITH EXPLANATORY NOTES: -- For your reference-- these are on computers in the sign out rooms -- Adrenal Checklist cut and paste below line: Specimen Type: Subtotal adrenalectomy Total adrenalectomy Other (specify): Not specified Laterality Right Left Not specified Tumor Size Greatest dimension: cm Tumor Weight Specify: g Histologic type Adrenal cortical adenoma Adrenal cortical carcinoma Myelolipoma Pheochromocytoma Pathologic Staging Primary Tumor I: Confined to gland, 5 cm or less II: Confined to gland, greater than 5 cm III: Extraglandular extension without other organ involvement IV: Distant metastasis or extension into other organs Regional Lymph Nodes Cannot be assessed No regional lymph node metastasis (0/ ) Regional lymph node metastasis ( / ) Distant Metastasis Cannot be assessed Margins Margins uninvolved by tumor Margin(s) involved by tumor Specify margin(s): Cannot be determined Venous (Large Vessel) Invasion Absent Present Indeterminate
9 Additional notes do not cut and paste this: This checklist is for resections of the adrenal gland. Neuroblastomas have a separate checklist-- these usually go to the pediatric service. Select the above and cut and paste into power path editor. For each choice delete those that are not used-- This protocol is fairly straight forward and easy to fill out. Remember to weight the tumor as this is important in prognostication. There is no AJCC TNM for adrenal tumors. Prognostication: Adrenal cortical tumors are not usually graded on histologic grounds. Severe nuclear atypia, high mitotic count, vascular invasion, tumor necrosis, and other microscopic features may, in combination, support a diagnosis of adrenal cortical carcinoma over adenoma and should be recorded, but no precise clustering of histologic features is considered diagnostic of malignancy. However, when several malignant features are present together (eg, highly atypical nuclei, sheet-like growth, necrosis, and many mitoses), the risk of distant metastases is increased In some studies, specific combinations of features, such as mitotic rates of 6 or more per 50 high-power fields (HPF) along with atypical mitosis and venous invasion, have been found to correlate with metastasis or recurrence of adrenal cortical carcinomas. 2 Other studies have shown that mitotic rates greater than 20 per 50 HPF are associated with decreased survival, suggesting that a high mitotic index may be an important adverse prognostic factor. 3 Although this protocol does not cover medullary tumors, it should be noted that pheochromocytoma is usually diagnosed preoperatively by pharmacologic means. No pathologic criteria for differentiation of benign from malignant pheochromocytomas have been defined. Metastatic disease is considered the only irrefutable proof of malignancy. References 1. Hough AJ, Hollifield JW, Page DL, Hartmann WH. Prognostic factors in adrenocortical tumors: a mathematical analysis of clinical and morphologic data. Am J Clin Pathol. 1979;72: Weiss LM. Comparative histologic study of 43 metastasizing and non-metastasizing adrenocortical tumors. Am J Surg Pathol. 1984;8: Weiss LM, Medeiros LJ, Vickery AL. Pathologic features of prognostic significance in adrenal cortical carcinoma. Am J Surg Pathol. 1989;13: Medeiros LJ, Weiss LM. New developments in the pathologic diagnosis of adrenal cortical neoplasms: a review. Am J Clin Pathol. 1992;97:73-83.
10 Bladder (Urothelial) cancer TURBT items to mention For TURBT Mention tumor type, grade, presence or absence of invasion, presence or absence of invasion into muscularis propria, presence or absence of muscularis propria in biopsy, presence or absence of angiolymphatic invasion - Muscularis propria (detrusor muscle) is present and is uninvolved - Carcinoma invades into muscularis propria (detrusor muscle) - Negative for angiolymphatic invasion EXAMPLES: Trigone, TURBT - High grade papillary urothelial carcinoma - Negative for invasive carcinoma - Muscularis propria (detrusor muscle) is present and is uninvolved Lateral wall, TURBT - Invasive high grade papillary urothelial carcinoma - Carcinoma invades into lamina propria - Muscularis propria (detrusor muscle) is present and is uninvolved - Negative for angiolymphatic invasion
11 Bladder Cancer Checklist cut and paste below line: Specimen Type Partial cystectomy Total cystectomy Radical cystectomy Radical cystoprostatectomy Anterior exenteration Other (specify): Tumor Site Trigone Right lateral wall Left lateral wall Anterior wall Posterior wall Dome Other (specify): Tumor Size Greatest dimension: cm MICROSCOPIC Histologic Type Urothelial (transitional cell) carcinoma Urothelial (transitional cell) carcinoma with squamous differentiation Urothelial (transitional cell) carcinoma with glandular differentiation Urothelial (transitional cell) carcinoma with variant histology (specify): Squamous cell carcinoma, typical Squamous cell carcinoma, variant histology (specify): Adenocarcinoma, typical Adenocarcinoma, variant histology (specify): Small cell carcinoma Undifferentiated carcinoma (specify): Mixed cell type (specify): Other (specify): Carcinoma, type cannot be determined Associated Epithelial Lesions None identified Urothelial (transitional cell) papilloma (World Health Organization [WHO] / International Society of Urologic Pathology [ISUP], 1998) Urothelial (transitional cell) papilloma, inverted type Papillary urothelial (transitional cell) neoplasm, low malignant potential (WHO/ISUP 1998) Histologic Grade Not applicable Urothelial Carcinoma (WHO/ISUP, 1998) Low-grade High-grade
12 Other (specify): Adenocarcinoma and Squamous Carcinoma GX: Cannot be assessed G1: Well differentiated G2: Moderately differentiated G3: Poorly differentiated Other (specify): Tumor Configuration Papillary Solid/nodule Flat Ulcerated Pathologic Staging (ptnm) Primary Tumor (pt) ptx: Cannot be assessed pt0: No evidence of primary tumor pta: Noninvasive papillary carcinoma ptis: Flat carcinoma in situ pt1: Tumor invades subepithelial connective tissue (lamina propria) pt2: Tumor invades muscularis propria (detrusor muscle) pt2a: Tumor invades superficial muscle (inner half) pt2b: Tumor invades deep muscle pt3: Tumor invades perivesical tissue pt3a: Tumor microscopically invades perivesical tissue pt3b: Tumor macroscopically invades perivesical tissue (extravesicular mass) pt4: Tumor invades any of the following: prostate, uterus, vagina, pelvic wall, abdominal wall pt4a: Tumor invades prostate or uterus or vagina pt4b: Tumor invades pelvic wall or abdominal wall Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis (0/ ) pn1: Metastasis in a single regional lymph node, 2 cm or less in greatest dimension pn2: Metastasis in a single regional lymph node, more than 2 cm but not more than 5 cm in greatest dimension, or multiple lymph nodes, none more than 5 cm in greatest dimension (+ / ) pn3: Metastasis in a regional lymph node more than 5 cm in greatest dimension (+ / ) Distant Metastasis (pm) pmx: Cannot be assessed Margins Margins uninvolved by invasive carcinoma Distance of invasive carcinoma from closest margin: mm Specify margin: Margins involved by invasive carcinoma Specify margin: Margins uninvolved by carcinoma in situ Margins involved by carcinoma in situ
13 Specify margin: Venous/Lymphatic (Large/Small Vessel) Invasion (V/L) Absent Present Indeterminate Direct Extension of Invasive Tumor None identified Perivesical fat Rectum Prostatic stroma Seminal vesicle (specify laterality): Vagina Uterus and adnexae Pelvic sidewall (specify laterality): Ureter (specify laterality): Other (specify): Additional notes do not cut and paste this: This checklist is for bladder tumors, if it is a urothelial carcinoma in the renal pelvis or a resection only of the ureter there is a separate checklist!! Select the above and cut and paste into power path editor. Cut and paste the appropriate procedure, tumor site, size and type of tumor If appropriate select an associated epithelial lesion (for example papillary tumor), if there is none just select none identified. The grading of the tumor depends on the type-- most are urothelial but the rarer adenocarcinomas and squamous cells use a different grading scheme. For the staging select the most appropriate choice. Please leave in the full staging designation so it is apparent why it was staged as it was. So instead of saying pt3a only write "pt3a: Tumor microscopically invades perivesical tissue". This helps reinforce staging criteria, obviates the need to grab the staging book and helps clarify issues at tumor board conferences. For the pt3 and pt4 categories there are sub-choices under each major heading- select the most appropriate one. The designation of microscopic vs. macroscopic for pt3 lesions is based on gross examination. If on gross one could see the tumor growing into perivesicular tissue it is a pt3b, if it is only evident on microscopic slides it is pt3a. If there are grossly positive lymph nodes measure them, this is part of the staging criteria! If there is prior radiation or chemotherapy the tumor is staged according to what you have and this is indicated by placing a "y" prefix ahead of the pathologic stage. For example, ypt3 pn0 pmx. If there is no tumor left then the stage is ypt0.

14 For each choice delete those that are not used--
15 Kidney Cancer Checklist cut and paste below line: Specimen Type Right partial nephrectomy Left partial nephrectomy Right radical nephrectomy Left radical nephrectomy Tumor Site Upper pole Middle Lower pole Not specified Focality Unifocal Multifocal Tumor Size Greatest dimension: cm Macroscopic Extent of Tumor Tumor limited to kidney Tumor extension into perinephric tissues Tumor extension beyond Gerota s fascia Tumor extension into adrenal Tumor extension into major veins Histologic Type Clear cell (conventional) renal carcinoma Papillary renal cell carcinoma Chromophobe renal cell carcinoma Collecting duct carcinoma Sarcomatoid carcinoma arising in renal cell carcinoma Specify: subtype ; % of sarcomatoid element Renal cell carcinoma, unclassified Other (specify): Histologic Grade (Fuhrman Nuclear Grade) Not applicable G1: Nuclei round, uniform, approximately 10 µ; nucleoli inconspicuous or absent G2: Nuclei slightly irregular, approximately 15 µ; nucleoli evident G3: Nuclei very irregular, approximately 20 µ; nucleoli large and prominent G4: Nuclei bizarre and multilobated, 20 µ or greater, nucleoli prominent, chromatin clumped Pathologic Staging (ptnm) Primary Tumor (pt) pt0: No evidence of primary tumor pt1: Tumor 7 cm or less in greatest dimension, limited to the kidney pt1a: Tumor 4 cm or less in greatest dimension, limited to the kidney pt1b: Tumor more than 4 cm but not more than 7 cm in greatest dimension, limited to the kidney pt2: Tumor more than 7 cm in greatest dimension, limited to the kidney
16 pt3: Tumor extends into major veins or invades adrenal gland or perinephric tissues but not beyond Gerota s fascia pt3a: Tumor directly invades adrenal gland or perirenal and/or renal sinus fat but not beyond Gerota s fascia pt3b: Tumor grossly extends into the renal vein or its segmental (muscle-containing) branches, or vena cava below the diaphragm pt3c: Tumor grossly extends into vena cava above diaphragm or invades the wall of the vena cava pt4: Tumor invades beyond Gerota s fascia Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis (0/ ) pn1: Metastasis in a single regional lymph node (1/ ) pn2: Metastasis in more than 1 regional lymph node (+ / ) Distant Metastasis (pm) pmx: Cannot be assessed Margins Cannot be assessed Margins uninvolved by invasive carcinoma Margin involved by invasive carcinoma Renal capsular margin (partial nephrectomy only) Perinephric fat margin (partial nephrectomy only) Renal vein margin Gerota s fascial margin Ureteral margin Renal parenchymal margin (partial nephrectomy only) Other (specify): Partial nephrectomy: Distance of carcinoma to parenchymal margin: mm Adrenal Gland Not present Uninvolved by tumor Direct invasion (T3a) Metastasis (M1) Venous (Large Vessel) Invasion (V) (excluding renal vein and inferior vena cava) Absent Present Indeterminate Lymphatic (Small Vessel) Invasion (L) Absent Present Indeterminate
17 Additional notes do not cut and paste this: Select the above and cut and paste into power path editor. Cut and paste the appropriate specimen site, right or left, partial or radical For each choice delete those that are not used-- Select a tumor site-- if it is not clear from the gross- check radiology or else just put not specified If there are multiple tumors measure the largest tumor, make sure that you are not dealing with multilobulated single tumors-- for size discrepancies check the radiology reports For the extent of tumor include all that apply, there may be more than one. For staging it is important to not forget about the renal sinus fat. Take multiple sections showing the relationship of the tumor to the renal sinus. If microscopically tumor cells are seen touching adipose tissue without a fibrous capsule there is renal sinus invasion and it is a T3 lesion. For lymph nodes, there may be a single lymph node that is in the hilum of the kidney. Palpate for a lymph node and if found submit it. If not submit a section of hilar adipose tissue, there may or may not be a lymph node in there. The remainder should be self-explanatory, delete the choices that are not used.
18 Prostate cancer checklist, cut and paste below line: Prostate, radical prostatectomy Prostate, robot-assisted radical prostatectomy Prostatic adenocarcinoma Gleason score ( + ), tertiary pattern % Tumor predominantly involves Maximal tumor nodule diameter measured on one slide: cm Percent of prostate gland involved by tumor % ( / tissue blocks contain tumor) Extraprostatic extension Absent Present- Focal, specify site, mm Present- Established, specific site: Margins Benign glands at surgical margin Margins uninvolved by invasive carcinoma Margin focally involved by invasive carcinoma, location: Margin involved by invasive carcinoma: Apical Bladder neck Anterior Lateral Postero-lateral (neurovascular bundle) Posterior Other(s) (specify): Angiolymphatic invasion Absent Present Indeterminate Seminal vesicle invasion Absent Present Indeterminate Pathologic Staging (ptnm) Primary Tumor (pt) pt2a: Organ confined, Unilateral, involving one-half of 1 lobe or less pt2b: Organ confined, Unilateral, involving more than one-half of 1 lobe pt2c: Organ confined, Bilateral disease pt3: Extraprostatic extension pt3a: Extraprostatic extension pt3b: Seminal vesicle invasion pt4: Invasion of bladder and/or rectum Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis (0/ lymph nodes examined) pn1: Metastasis in regional lymph node or nodes (+ / lymph nodes)
19 Distant Metastasis (pm) pmx: Distant metastasis cannot be assessed Additional notes do not cut and paste this: Select the above and cut and paste into power path editor. Cut and paste the appropriate procedure-- radical or robot-assisted For each choice delete those that are not used-- It is assumed that it is conventional adenocarcinoma and not a variant such as ductal or small cell or adenoid cystic. If the tumor has interesting additional features (i.e. foamy gland etc. feel free to include it here). Fill in the appropriate Gleason score-- the common 3+3 is filled in already, if there is a higher grade tertiary pattern include and estimate the percentage of that pattern (i.e. tertiary pattern 5, 5%). If there is prior hormonal therapy these are not Gleason graded- include a note stating this. Measure the largest cross section of tumor diameter on a slide-- I realized this is imperfect but the urologists wanted a tumor nodule size Fill in a rough estimate of the volume of tumor-- 15% (5/ 25 blocks contain tumor). The percentage should be based on the overall estimate and not be derived from the block count on its own. For extraprostatic extension mention if it is focal (give a size estimate) or "established" and give a general description of where it is positive. For margins mention is benign glands are at ink. If carcinoma is at ink and list all the positive sites, preferably with slide designation (i.e. slide A11, A12) and use either the focal positive if there is a small focus or the generic positive margin if more than focal. If the margin is more than focally positive, it may be appropriate to stage the tumor pathologically with an x modifier to designated that it is unknown. For example, the tumor is "organ confined" but extends to a margin more than focally and thus in this location if cannot be determined if there is or is not extraprostatic extenstion. The stage using this example would be pt2x. This can additionally be designated with an R1 descriptor for microscopic residual disease following definitive surgery (for example: pt2x pn0 pmx R1). For the pathologic staging- I think it is helpful to include the words describing why the stage is what it is. This is educational for the residents and means that you do not have to look it up in the AJCC book- this also helps at tumor board where sometimes there is a "discussion" regarding what the appropriate stage is.
20 Testes (orchiectomy) Checklist cut and paste below line: Specimen Right orchiectomy Left orchiectomy Bilateral orchiectomy Focality of tumor Unifocal Multifocal Tumor Size Greatest dimension of main tumor mass: cm Greatest dimensions of additional tumor nodules: cm, cm, etc Histologic Type Intratubular germ cell neoplasm, only Seminoma, classic type Seminoma with syncytiotrophoblastic cells Mixed germ cell tumor (specify components and percentages): Embryonal carcinoma Yolk sac tumor Choriocarcinoma, biphasic Choriocarcinoma, monophasic Placental site trophoblastic tumor Mature teratoma Immature teratoma Teratoma with a secondary malignant component (specify type): Monodermal teratoma, carcinoid Monodermal teratoma, primitive neuroectodermal tumor Monodermal teratoma, other (specify): Polyembryoma Diffuse embryoma Spermatocytic seminoma Spermatocytic seminoma with a sarcomatous component Testicular scar Mixed germ cell-sex cord-stromal tumor, gonadoblastoma Mixed germ cell-sex cord-stromal tumor, others (specify): Pathologic Staging (ptnm) Primary Tumor (pt) ptx: Cannot be assessed pt0: No evidence of primary tumor ptis: Intratubular germ cell neoplasia only (carcinoma in situ) pt1: Tumor limited to the testis and epididymis without vascular/lymphatic invasion (tumor may invade tunica albuginea but not tunica vaginalis) pt2: Tumor limited to the testis and epididymis with vascular/lymphatic invasion or tumor extending through tunica albuginea with involvement of tunica vaginalis pt3: Tumor invades spermatic cord with or without vascular/lymphatic invasion pt4: Tumor invades scrotum with or without vascular/lymphatic invasion
21 Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis (0/ ) pn1: Metastasis with a lymph node mass less than 2 cm in greatest dimension and 5 or fewer positive nodes, none more than 2 cm in greatest dimension ( / ) pn2: Metastasis with a lymph node mass greater than 2 cm but not more than 5 cm in greatest dimension, or more than 5 nodes positive, none greater than 5 cm; or evidence of extranodal extension of tumor ( / ) pn3: Metastasis with a lymph node mass greater than 5 cm in greatest dimension ( / ) Distant Metastasis (pm) pmx: Cannot be assessed Margins Spermatic Cord Margin Cannot be assessed Uninvolved by tumor Involved by tumor Other Margin(s) Cannot be assessed Uninvolved by tumor (specify): Involved by tumor (specify): Direct Extension of Invasive Tumor Rete testis Epididymis Peri-hilar fat Spermatic cord Tunica vaginalis Scrotal wall None identified Venous/Lymphatic (Large/Small Vessel) Invasion (V/L) Absent Present Indeterminate Additional Pathologic Findings None identified Intratubular germ cell neoplasia Other: Serum Tumor Markers (S) SX: Serum marker studies not available or performed S0: Serum marker study levels within normal limits LDH: Reference range ( ) U/L HCG: Reference range (<2) miu/ml AFP: Reference range ( ) ng/ml Serum tumor marker stage:
22 Use this table below to calculate S stage, and then delete this table LDH HCG (miu/ml) AFP (ng/ml) S1: <1.5 x nl and <5,000 and <1,000 S2: x nl or 5,000-50,000 or 1,000-10,000 S3: >10 x nl or >50,000 or >10,000 Additional notes do not cut and paste this: This checklist is for orchiectomies which are relatively uncommon but important to understand. Select the above and cut and paste into power path editor. Measure the largest tumor mass, and if multiple measure satellite masses, sample different masses histologically and any areas that grossly look different within the tumor. Sample liberally. If there is a minor component of a more aggressive germ cell tumor it will be very important to identify. The 3-4 extra blocks may be very important. Cut and paste the appropriate procedure, tumor site, size and type of tumor Stage the tumor and leave the explanatory notes in the staging in the report. This is educational and helps to clarify why a tumor was staged the way it was and makes it easier to present at tumor board conferences. For the lymph nodes put the number involved/ positive after the staging criteria. We often do not get node dissections with the orchiectomy specimen. Notice that like other GU sites the size of involved lymph nodes is important so if there is a grossly positive node, measure it! For metastases stage them as pmx even if clinically they say he has lung mets or brain mets. etc. Only if we have a biopsy of these mets should if be staged as an M1. Including the serum marker studies may seem obsessive compulsive but important and it reinforces the important concept that these are helpful in diagnosis and monitoring of therapy. If the values warrant an S3 pathologic stage this clinically upstages patients so it is important. This is a laboratory value and should be included in the pathology report the same way we include ER and PR or cytogenetics findings in hematopathology reports. Look these up and include the values in the report-- the reference ranges are included next to them. Using this information, using the red table to calculate the S stage and include in the report and delete the table afterwards. A point worth emphasizing is that if there is a very high AFP and no evidence of a yolk sac component, or very high HCG and no evidence of a choriocarcinoma it is prudent to go back to the bucket and put more tissue in for sections. You may want to be proactive and check the serum levels prior to grossing in the orchiectomy-- if either of these is elevated put through more tissue of the tumor. In my experience, this will save trips back to the bucket. The author (RWA) almost always entirely submitted testicular tumors. If there is prior radiation or chemotherapy the tumor is staged according to what you have and this is indicated by placing a "y" prefix ahead of the pathologic stage. For example, ypt3 pn0 pmx. If there is no tumor left then the stage is ypt0. For each choice delete those that are not used--
23
24 Retroperitoneal lymphadenectomy Checklist cut and paste below line: Specimen Sites Specify: Size of Largest Metastasis Not applicable Greatest dimension: cm Viability of Tumor Viable tumor present Non viable tumor present No tumor present Histologic Type of Metastatic Tumor Seminoma, classic type Seminoma with syncytiotrophoblastic cells Mixed germ cell tumor (specify components and percentages): Embryonal carcinoma Yolk sac tumor Choriocarcinoma, biphasic Choriocarcinoma, monophasic Placental site trophoblastic tumor Mature teratoma Immature teratoma Teratoma with a secondary malignant component (specify type): Monodermal teratoma, carcinoid Monodermal teratoma, primitive neuroectodermal tumor Polyembryoma Diffuse embryoma Spermatocytic seminoma Spermatocytic seminoma with a sarcomatous component Other (specify): Malignant neoplasm, type cannot be determined Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis ( / ) pn1: Metastasis with a lymph node mass less than 2 cm in greatest dimension and 5 or fewer positive nodes, none greater than 2 cm in greatest dimension ( / ) pn2: Metastasis with a lymph node mass greater than 2 cm but no more than 5 cm in greatest dimension, or more than 5 nodes positive, none greater than 5 cm; or evidence of extranodal extension of tumor ( / ) pn3: Metastasis in a lymph node greater than 5 cm in greatest dimension ( / ) Nonregional Lymph Node Metastasis (M1a) Not applicable Absent Present
25 Prelymphadenectomy Treatment Chemo/radiation therapy No chemo/radiation therapy Unknown Serum Tumor Markers Unknown Serum marker studies within normal limits Alpha-fetoprotein (AFP) elevation: U/L (Reference ( ) U/L) Beta subunit of HCG (b-hcg) elevation: miu/ml (Reference (<2) miu/ml) Lactate dehydrogenase (LDH) elevation: U/L (Reference ( ) U/L) Additional notes do not cut and paste this: Select the above and cut and paste into power path editor. This checklist is for retroperitoneal lymph node dissections. These often occur after orchiectomies and after treatment so be sure to use the y staging prefix (see below). Not infrequently the orchiectomy is done outside and we do not know other than by report what the tumor is. For specimen site, just list whatever they call the specimen. For histologic type of tumor list what you have and if mixtures are present then list the various percentages of the different components. Often after treatment these contain mature teratomatous elements that presumably represent differentiated tumor- report these as listed above. Notice that positive nodes need measurements! Remember to do this when grossing. We do not usually get non-regional lymph node dissections with these. If there is prior chemo/radiation use the y prefix for staging. The y prefix indicates those cases in which classification is performed during or following initial multimodality therapy (ie, neoadjuvant chemotherapy, radiation therapy, or both chemotherapy and radiation therapy). The ptnm category is identified by a y prefix. The yptnm categorizes the extent of tumor actually present at the time of that examination. The y categorization is NOT an estimate of tumor prior to multimodality therapy (ie, before initiation of neoadjuvant therapy). If there is no tumor the pathologic stage is ypt0. For each choice delete those that are not used--
26 Renal pelvis Checklist cut and paste below line: Specimen Type Left nephroureterectomy, partial Left nephroureterectomy, complete Right nephroureterectomy, partial Right nephroureterectomy, complete Tumor Size Greatest dimension: cm Histologic Type Urothelial (transitional cell) carcinoma Urothelial (transitional cell) carcinoma with squamous differentiation Urothelial (transitional cell) carcinoma with glandular differentiation Urothelial (transitional cell) carcinoma with variant histology (specify): Squamous cell carcinoma, typical Squamous cell carcinoma, variant histology (specify): Adenocarcinoma, typical Adenocarcinoma, variant histology (specify): Small cell carcinoma Undifferentiated carcinoma (specify): Mixed cell type (specify): Other (specify): Carcinoma, type cannot be determined Associated Epithelial Lesions None identified Urothelial (transitional cell) papilloma (World Health Organization [WHO] / International Society of Urologic Pathology [ISUP], 1998) Urothelial (transitional cell) papilloma, inverted type Papillary urothelial (transitional cell) neoplasm, low malignant potential (WHO/ISUP 1998) Cannot be determined Histologic Grade Not applicable Urothelial Carcinoma (WHO/ISUP, 1998) Low-grade High-grade Other (specify): Adenocarcinoma and Squamous Carcinoma GX: Cannot be assessed G1: Well differentiated G2: Moderately differentiated G3: Poorly differentiated Other (specify): Pathologic Staging (ptnm)
27 Primary Tumor (pt) ptx: Cannot be assessed pt0: No evidence of primary tumor pta: Papillary noninvasive carcinoma ptis: Flat carcinoma in situ pt1: Tumor invades subepithelial connective tissue (lamina propria) pt2: Tumor invades muscularis pt3: Tumor invades beyond muscularis into peripelvic fat or the renal parenchyma pt4: Tumor invades adjacent organs, or through the kidney into the perinephric fat Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis (0/ ) pn1: Metastasis in a single regional lymph node, 2 cm or less in greatest dimension (+1/ ) pn2: Metastasis in a single regional lymph node, more than 2 cm but not more than 5 cm in greatest dimension, or multiple lymph nodes, none more than 5 cm in greatest dimension (+ / ) pn3: Metastasis in a regional lymph node more than 5 cm in greatest dimension Distant Metastasis (pm) pmx: Cannot be assessed Tumor Configuration Papillary Solid/nodule Flat Ulcerated Indeterminate Margins Margins uninvolved by invasive carcinoma Distance of invasive carcinoma from closest margin: mm Specify margin: Margin(s) involved by invasive carcinoma Specify margin(s): Margin(s) uninvolved by carcinoma in situ Margin(s) involved by carcinoma in situ Specify margin(s): Venous/Lymphatic (Large/Small Vessel) Invasion (V/L) Absent Present Indeterminate Additional notes do not cut and paste this: This checklist is for tumor that arise in the renal pelvis, typically urothelial carcinomas. Do not use the kidney checklist use this one. There is a separate checklist for bladder and pure ureter resections. Select the above and cut and paste into power path editor. Cut and paste the appropriate procedure, tumor site, size and type of tumor If appropriate select an associated epithelial lesion (for example papillary tumor), if there is none just select
28 none identified. The grading of the tumor depends on the type-- most are urothelial but the rarer adenocarcinomas and squamous cells use a different grading scheme. Measure grossly positive lymph nodes, this is used for staging. For the lymph node include the number examined and number positive after the stage information. For example, pn1: Metastasis in a single regional lymph node, 2 cm or less in greatest dimension (+1/5) Please leave the full staging description in the sign out. This way it is clear why it was staged the way it was, what the staging criteria are and it is useful for tumor boards. If there is prior radiation or chemotherapy the tumor is staged according to what you have and this is indicated by placing a "y" prefix ahead of the pathologic stage. For example, ypt3 pn0 pmx. If there is no tumor left then the stage is ypt0. For each choice delete those that are not used--
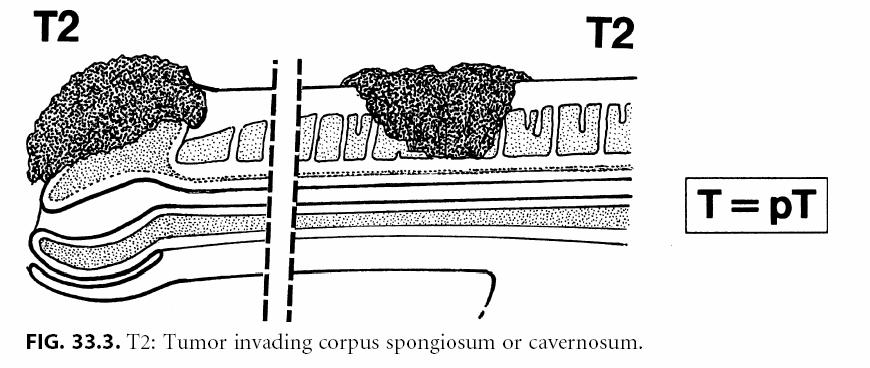
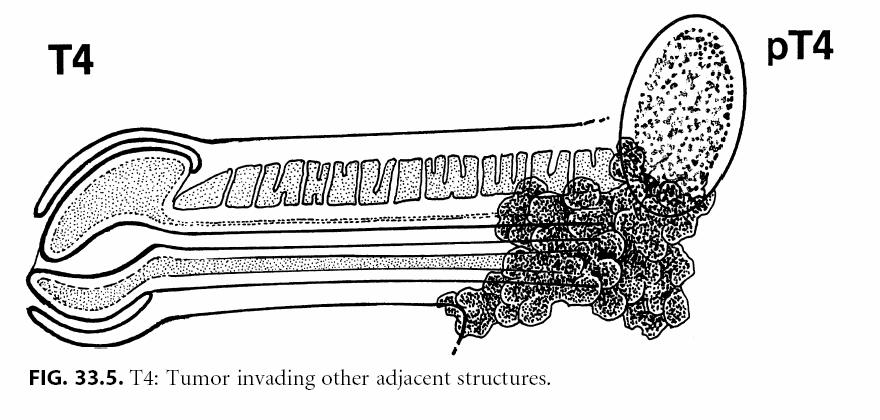
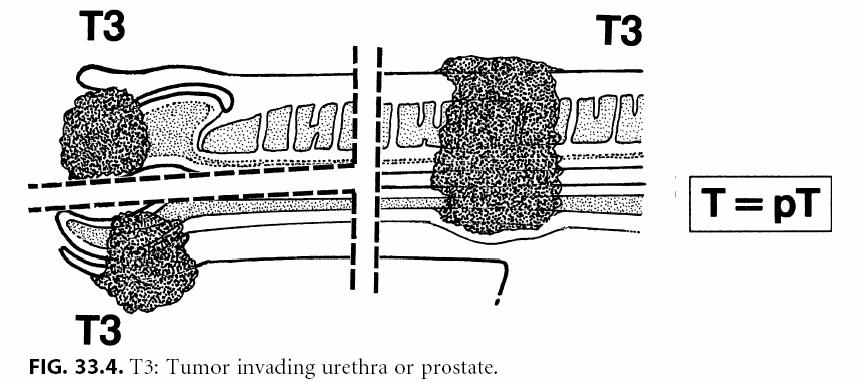
29 Penile Cancer Checklist cut and paste below line: Specimen Type Partial penectomy Other (specify): Tumor Site Glans Other: Tumor Size Greatest dimension: cm MICROSCOPIC Histologic Type Squamous cell carcinoma in-situ/ Bowen's disease Squamous cell carcinoma, NOS Squamous cell carcinoma, verrucous Adenocarcinoma, NOS Other: Histologic Grade G1 Well differentiated G2 Moderately differentiated G3-4 Poorly differentiated or undifferentiated Tumor Configuration Papillary Solid/nodule Ulcerated Pathologic Staging (ptnm) Primary Tumor (pt) ptx: Cannot be assessed pt0: No evidence of primary tumor ptis: Carcinoma in-situ pta: Non-invasive verrucous carcinoma pt1: Tumor invades subepithelial connective tissue pt2: Tumor invades corpus spongiosum or cavernosum pt3: Tumor invades urethra or prostate pt4: Tumor invades adjacent structures Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis (0/ ) pn1: Metastasis in a single superficial inguinal lymph node (+1/ ) pn2: Metastasis in a multiple or bilateral superficial inguinal lymph nodes (+ / ) pn3: Metastasis in a deep inguinal or pelvic lymph nodes unilateral or bilateral (+ / ) Distant Metastasis (pm) pmx: Cannot be assessed Margins Margins uninvolved by invasive carcinoma
30 Distance of invasive carcinoma from closest margin: mm Specify margin: Margins involved by invasive carcinoma Specify margin: Margins uninvolved by carcinoma in situ Margins involved by carcinoma in situ Specify margin: Venous/Lymphatic (Large/Small Vessel) Invasion (V/L) Absent Present Indeterminate Direct Extension of Invasive Tumor None identified Subepithelial connective tissue Corpus spongiosum Corpus cavernosum Urethra Other: Additional notes do not cut and paste this: This checklist is for penile tumors. Select the above and cut and paste into power path editor. Cut and paste the appropriate procedure, tumor site, size and type of tumor For each choice delete those that are not used-- If there is prior radiation or chemotherapy the tumor is staged according to what you have and this is indicated by placing a "y" prefix ahead of the pathologic stage. For example, ypt3 pn0 pmx. If there is no tumor left then the stage is ypt0. Diagrams of the different pathologic stages are shown below.
31
32 Ureter resection Checklist cut and paste below line: Specimen Type Left ureterectomy Left nephroureterectomy Right ureterectomy Right nephroureterectomy Tumor Size Greatest dimension: Histologic Type Urothelial (transitional cell) carcinoma Urothelial (transitional cell) carcinoma with squamous differentiation: Urothelial (transitional cell) carcinoma with glandular differentiation Urothelial (transitional cell) carcinoma with variant histology (specify): Squamous cell carcinoma, typical Squamous cell carcinoma, variant histology (specify): Adenocarcinoma, typical Adenocarcinoma, variant histology (specify): Small cell carcinoma Undifferentiated carcinoma (specify): Mixed cell type (specify): Other (specify): Carcinoma, type cannot be determined Associated Epithelial Lesions None identified Urothelial (transitional cell) papilloma (World Health Organization [WHO] / International Society of Urologic Pathology [ISUP], 1998) Urothelial (transitional cell) papilloma, inverted type Papillary urothelial (transitional cell) neoplasm, low malignant potential (WHO/ISUP 1998) Cannot be determined Histologic Grade Not applicable Cannot be determined Urothelial Carcinoma (WHO/ISUP, 1998) Low-grade High-grade Adenocarcinoma and Squamous Carcinoma GX: Cannot be assessed G1: Well differentiated G2: Moderately differentiated G3: Poorly differentiated Other (specify): Pathologic Staging (ptnm)
33 Primary Tumor (pt) ptx: Cannot be assessed pt0: No evidence of primary tumor pta: Papillary noninvasive carcinoma ptis: Carcinoma in situ pt1: Tumor invades subepithelial connective tissue (lamina propria) pt2: Tumor invades the muscularis pt3: Tumor invades beyond muscularis into periureteric fat pt4: Tumor invades adjacent organs Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis (0/ ) pn1: Metastasis in a single regional lymph node, 2 cm or less in greatest dimension (+1/ ) pn2: Metastasis in a single regional lymph node, more than 2 cm but not more than 5 cm in greatest dimension, or multiple lymph nodes, none more than 5 cm in greatest dimension (+ / ) pn3: Metastasis in a regional lymph node more than 5 cm in greatest dimension (+ / ) Distant Metastasis (pm) pmx: Cannot be assessed Tumor Configuration Papillary Solid/nodule Ulcerated Flat Indeterminate Other (specify): Margins Margins uninvolved by invasive carcinoma Distance of invasive carcinoma from closest margin: mm Specify margin(s): Margin(s) involved by invasive carcinoma Specify margin(s): Margins(s) involved by carcinoma in situ Margin(s) uninvolved by carcinoma in situ Other(s) (specify): Venous/Lymphatic (Large/Small Vessel) Invasion (V/L) Absent Present Indeterminate Additional notes do not cut and paste this: This checklist is for resections of the ureter only which are rather uncommon. In fact, if you are considering using this checklist you are more likely than not using the wrong checklist. Select the above and cut and paste into power path editor. Cut and paste the appropriate procedure, tumor site, size and type of tumor If appropriate select an associated epithelial lesion (for example papillary tumor), if there is none just select none identified.
34 The grading of the tumor depends on the type-- most are urothelial but the rarer adenocarcinomas and squamous cells use a different grading scheme. For the lymph node include the number examined and number positive after the stage information. Remember to measure the size of grossly positive lymph nodes. For example, pn1: Metastasis in a single regional lymph node, 2 cm or less in greatest dimension (+1/5) Please leave the full staging description in the sign out. This way it is clear why it was staged the way it was, what the staging criteria are and it is useful for tumor boards. If there is prior radiation or chemotherapy the tumor is staged according to what you have and this is indicated by placing a "y" prefix ahead of the pathologic stage. For example, ypt3 pn0 pmx. If there is no tumor left then the stage is ypt0. For each choice delete those that are not used--
35 Urethra urothelial cancer Checklist cut and paste below line: Specimen Type Specify: Tumor Site Specify: Tumor Size Greatest dimension: cm Histologic Type Urothelial (transitional cell) carcinoma Squamous cell carcinoma, NOS Other: Histologic Grade G1 Well differentiated G2 Moderately differentiated G3-4 Poorly differentiated or undifferentiated Pathologic Staging (ptnm) Primary Tumor (pt) (male or female) ptx: Cannot be assessed pt0: No evidence of primary tumor ptis: Carcinoma in-situ pta: Non-invasive papillary, polypoid or verrucous carcinoma pt1: Tumor invades subepithelial connective tissue pt2: Tumor invades any of the following: corpus spongiosum, prostate or periurethral muscle pt3: Tumor invades any of the following: corpus cavernosum, beyond prostatic capsule, anterior vagina, bladder neck pt4: Tumor invades other adjacent organs Urothelial (transitional cell carcinoma) of the prostate Primary tumor (pt) ptis (pu): Carcinoma in-situ, involvement of prostatic urethra ptis (pd): Carcinoma in-situ involvement of the prostatic ducts pt1: Tumor invades supepithelial connective tissue pt2: Tumor invades any of the following: prostatic stroma, corpus spongiosum, periurethral muscle pt3: Tumor invades any of the following: corpus cavernosum, beyond prostatic capsule, bladder neck (extraprostatic extenstion) pt4: Tumor invades adjacent organs (invasion of the bladder) Regional Lymph Nodes (pn) pnx: Cannot be assessed pn0: No regional lymph node metastasis (0/ ) pn1: Metastasis in a single lymph node 2cm or less in greatest dimension (+1/ ) pn2: Metastasis in a single lymph node more than 2cm or multiple nodes (+ / ) Distant Metastasis (pm) pmx: Cannot be assessed Margins Margins uninvolved by invasive carcinoma Distance of invasive carcinoma from closest margin: mm
 Invasion (V/L) Absent Present Indeterminate Direct Extension of Invasive Tumor None identified Subepithelial connective tissue Corpus")

36 Specify margin: Margins involved by invasive carcinoma Specify margin: Margins uninvolved by carcinoma in situ Margins involved by carcinoma in situ Specify margin: Venous/Lymphatic (Large/Small Vessel) Invasion (V/L) Absent Present Indeterminate Direct Extension of Invasive Tumor None identified Subepithelial connective tissue Corpus spongiosum Corpus cavernosum Prostatic stroma Periurethral muscle Bladder neck Additional notes do not cut and paste this: This checklist is for urethra tumors. These are very unusual. This includes women and men. Note if there is a urothelial carcinoma of the prostatic urethra this gets its own pt staging. Select the above and cut and paste into power path editor.
Testis. Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies.
 Testis Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies. Protocol revision date: January 2005 Based on AJCC/UICC
Testis Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies. Protocol revision date: January 2005 Based on AJCC/UICC
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Prognostic factors of genitourinary tumors: Do we have to care?
 Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Bladder Case 1 SURGICAL PATHOLOGY REPORT. Procedure: Cystoscopy, transurethral resection of bladder tumor (TURBT)
") Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
Procedures Needle Biopsy Transurethral Prostatic Resection Suprapubic or Retropubic Enucleation (Subtotal Prostatectomy) Radical Prostatectomy
 Radical Prostatectomy") Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Male genital tract tumors. SiCA. Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital.
 Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours
 60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
*OPERATIVE PROCEDURE. Serum tumour markers within normal limits S1.04 PRINCIPAL CLINICIAN
 Neoplasia of the Testis - Orchidectomy Histopathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Neoplasia of the Testis - Orchidectomy Histopathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Testicular Malignancies /8/15
 Collecting Cancer Data: Testis 2014-2015 NAACCR Webinar Series January 8, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Testis 2014-2015 NAACCR Webinar Series January 8, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Protocol applies to adrenal cortical carcinoma. Pheochromocytoma, neuroblastoma, and other adrenal medullary tumors of childhood are excluded.
 Adrenal Gland Protocol applies to adrenal cortical carcinoma. Pheochromocytoma, neuroblastoma, and other adrenal medullary tumors of childhood are excluded. Protocol revision date: January 2005 No AJCC/UICC
Adrenal Gland Protocol applies to adrenal cortical carcinoma. Pheochromocytoma, neuroblastoma, and other adrenal medullary tumors of childhood are excluded. Protocol revision date: January 2005 No AJCC/UICC
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Case Scenario 1 Discharge Summary Pathology Report Final Diagnosis: Oncology Consult
 Case Scenario 1 Discharge Summary A 31-year-old Brazilian male presented with a 6 month history of right-sided scrotal swelling. Backache was present for 2 months and a history of right epididymitis was
Case Scenario 1 Discharge Summary A 31-year-old Brazilian male presented with a 6 month history of right-sided scrotal swelling. Backache was present for 2 months and a history of right epididymitis was
Case Scenario 1 Discharge Summary Pathology Report Final Diagnosis: Oncology Consult
 Case Scenario 1 Discharge Summary A 31-year-old Brazilian male presented with a 6 month history of right-sided scrotal swelling. Backache was present for 2 months and a history of right epididymitis was
Case Scenario 1 Discharge Summary A 31-year-old Brazilian male presented with a 6 month history of right-sided scrotal swelling. Backache was present for 2 months and a history of right epididymitis was
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
TOPICS FOR DISCUSSION
 INTERNATIONAL SOCIETY OF UROLOGIC PATHOLOGY PATHOLOGIC STAGING OF SELECT UROLOGIC MALIGNANCIES Mahul B. Amin, MD Professor and Chairman Pathology and Laboratory Medicine Cedars-Sinai Medical Center Los
INTERNATIONAL SOCIETY OF UROLOGIC PATHOLOGY PATHOLOGIC STAGING OF SELECT UROLOGIC MALIGNANCIES Mahul B. Amin, MD Professor and Chairman Pathology and Laboratory Medicine Cedars-Sinai Medical Center Los
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Kidney. Protocol applies to all invasive carcinomas of renal tubular origin. It excludes Wilms tumors and tumors of urothelial origin.
 Kidney Protocol applies to all invasive carcinomas of renal tubular origin. It excludes Wilms tumors and tumors of urothelial origin. Procedures Incisional Biopsy (Needle or Wedge) Partial Nephrectomy
Kidney Protocol applies to all invasive carcinomas of renal tubular origin. It excludes Wilms tumors and tumors of urothelial origin. Procedures Incisional Biopsy (Needle or Wedge) Partial Nephrectomy
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Exercise. Discharge Summary
 Exercise Discharge Summary A 32-year-old Brazilian male presented with a 6 month history of right-sided scrotal swelling. Backache was present for 2 months and a history of right epididymitis was present
Exercise Discharge Summary A 32-year-old Brazilian male presented with a 6 month history of right-sided scrotal swelling. Backache was present for 2 months and a history of right epididymitis was present
GUIDELINES ON TESTICULAR CANCER
 38 (Text updated March 2005) P. Albers (chairman), W. Albrecht, F. Algaba, C. Bokemeyer, G. Cohn-Cedermark, A. Horwich, O. Klepp, M.P. Laguna, G. Pizzocaro Introduction Compared with other types of cancer
38 (Text updated March 2005) P. Albers (chairman), W. Albrecht, F. Algaba, C. Bokemeyer, G. Cohn-Cedermark, A. Horwich, O. Klepp, M.P. Laguna, G. Pizzocaro Introduction Compared with other types of cancer
S1.04 PRINCIPAL CLINICIAN G1.01 COMMENTS S2.01 SPECIMEN LABELLED AS G2.01 *SPECIMEN DIMENSIONS (PROSTATE) S2.03 *SEMINAL VESICLES
 S2.03 *SEMINAL VESICLES") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
A Practicum Approach to CS: GU Prostate, Testis, Bladder, Kidney, Renal Pelvis. Jennifer Ruhl, RHIT, CCS, CTR Janet Stengel, RHIA, CTR
 A Practicum Approach to CS: GU Prostate, Testis, Bladder, Kidney, Renal Pelvis Jennifer Ruhl, RHIT, CCS, CTR Janet Stengel, RHIA, CTR Survey Questions and Answers 250 Responses 2 Question #1 A gentleman
A Practicum Approach to CS: GU Prostate, Testis, Bladder, Kidney, Renal Pelvis Jennifer Ruhl, RHIT, CCS, CTR Janet Stengel, RHIA, CTR Survey Questions and Answers 250 Responses 2 Question #1 A gentleman
Quiz 1. Assign Race 1, Race 2 and Spanish Hispanic Origin to the following scenarios.
 Quiz 1 Assign Race 1, Race 2 and Spanish Hispanic Origin to the following scenarios. 1. 62 year old Brazilian female Race 1 Race 2 Spanish/Hispanic Origin 2. 43 year old Asian male born in Japan Race 1
Quiz 1 Assign Race 1, Race 2 and Spanish Hispanic Origin to the following scenarios. 1. 62 year old Brazilian female Race 1 Race 2 Spanish/Hispanic Origin 2. 43 year old Asian male born in Japan Race 1
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Protocol for the Examination of Specimens From Patients With Carcinoma of the Urethra and Periurethral Glands
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Urethra and Periurethral Glands Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition,
Protocol for the Examination of Specimens From Patients With Carcinoma of the Urethra and Periurethral Glands Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition,
Male Genital Cancers in the US in Frequency of Types
 Germ Cell Tumors of the Testis Pathology, Immunohistochemistry, and the Often Confusing Appearance of Their Metastases Charles Zaloudek, MD Department of Pathology UCSF Male Genital Cancers in the US in
Germ Cell Tumors of the Testis Pathology, Immunohistochemistry, and the Often Confusing Appearance of Their Metastases Charles Zaloudek, MD Department of Pathology UCSF Male Genital Cancers in the US in
Protocol for the Examination of Lymphadenectomy Specimens From Patients With Malignant Germ Cell and Sex Cord-Stromal Tumors of the Testis
 Protocol for the Examination of Specimens From Patients With Malignant Germ Cell and Sex Cord-Stromal Tumors of the Testis Version: Testis 4.0.1.1 Protocol Posting Date: February 2019 Accreditation Requirements
Protocol for the Examination of Specimens From Patients With Malignant Germ Cell and Sex Cord-Stromal Tumors of the Testis Version: Testis 4.0.1.1 Protocol Posting Date: February 2019 Accreditation Requirements
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
3/23/2017. Significant Changes in Prostate Cancer Classification, Grading, Staging and Reporting. Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood.
 or other renal tumors of childhood.") Wilms Tumor Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood. Procedures Cytology (No Accompanying Checklist) Incisional Biopsy (Needle or
Wilms Tumor Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood. Procedures Cytology (No Accompanying Checklist) Incisional Biopsy (Needle or
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas.
 Protocol applies to all carcinomas of the exocrine pancreas.") Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Neoplasms of the Prostate and Bladder
 Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Testis. Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies.
 Testis Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies. Protocol revision date: January 2004 Based on AJCC/UICC
Testis Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies. Protocol revision date: January 2004 Based on AJCC/UICC
Testis. Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies.
 Testis Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies. Protocol revision date: January 2005 Based on AJCC/UICC
Testis Protocol applies to all malignant germ cell and malignant sex cord-stromal tumors of the testis, exclusive of paratesticular malignancies. Protocol revision date: January 2005 Based on AJCC/UICC
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification
 Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
-The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
- In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Recommendations for the Reporting of Prostate Carcinoma
 Recommendations for the Reporting of Prostate Carcinoma Association of Directors of Anatomic and Surgical Pathology * ADASP Reporting Guidelines It has been evident for decades that pathology reports are
Recommendations for the Reporting of Prostate Carcinoma Association of Directors of Anatomic and Surgical Pathology * ADASP Reporting Guidelines It has been evident for decades that pathology reports are
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
2018 Grade PEGGY ADAMO, RHIT, CTR OCTOBER 11, 2018
 1 2018 Grade PEGGY ADAMO, RHIT, CTR ADAMOM@MAIL.NIH.GOV OCTOBER 11, 2018 2 Acknowledgements Donna Hansen, CCR Jennifer Ruhl, NCI SEER Introduction 3 Histologic Type vs. Grade Credit: Dr. Kay Washington
1 2018 Grade PEGGY ADAMO, RHIT, CTR ADAMOM@MAIL.NIH.GOV OCTOBER 11, 2018 2 Acknowledgements Donna Hansen, CCR Jennifer Ruhl, NCI SEER Introduction 3 Histologic Type vs. Grade Credit: Dr. Kay Washington
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do?
 Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Protocol for the Examination of Specimens From Patients With Carcinoma of the Ureter and Renal Pelvis
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Ureter and Renal Pelvis Protocol applies to invasive and in-situ carcinomas and/or associated epithelial lesions of the ureter
Protocol for the Examination of Specimens From Patients With Carcinoma of the Ureter and Renal Pelvis Protocol applies to invasive and in-situ carcinomas and/or associated epithelial lesions of the ureter
Protocol for the Examination of Specimens from Patients with Carcinoma of the Ureter and Renal Pelvis
 Protocol for the Examination of Specimens from Patients with Carcinoma of the Ureter and Renal Pelvis Protocol applies to invasive and in-situ carcinomas and/or associated epithelial lesions of the ureter
Protocol for the Examination of Specimens from Patients with Carcinoma of the Ureter and Renal Pelvis Protocol applies to invasive and in-situ carcinomas and/or associated epithelial lesions of the ureter
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
FINALIZED SEER SINQ QUESTIONS April July, 2017
 20170040 Source 1: 2016 SEER Manual pgs: 91 Source 2: 2007 MP/H Rules Notes: Lung MP/H Rules/Histology--Lung: What is the histology code for lung cancer case identified pathologically from a metastatic
20170040 Source 1: 2016 SEER Manual pgs: 91 Source 2: 2007 MP/H Rules Notes: Lung MP/H Rules/Histology--Lung: What is the histology code for lung cancer case identified pathologically from a metastatic
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
NAACCR Webinar Series 1
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES
 25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES SPEAKER DR DEEPAK ABROL CLINICAL ONCOLOGIST JAND K HEALTH SERVICES CONSULTANT ONCOLOGIST MAHARISHI DAYANAND HOSPITAL AND MEDICAL RESEARCH CENTER
25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES SPEAKER DR DEEPAK ABROL CLINICAL ONCOLOGIST JAND K HEALTH SERVICES CONSULTANT ONCOLOGIST MAHARISHI DAYANAND HOSPITAL AND MEDICAL RESEARCH CENTER
Protocol for the Examination of Cystectomy Specimens From Patients With Carcinoma of the Urinary Bladder
 Protocol for the Examination of Cystectomy Specimens From Patients With Carcinoma of the Urinary Bladder Version: UrinaryBladder 4.0.1.1 Protocol Posting Date: February 2019 CAP Laboratory Accreditation
Protocol for the Examination of Cystectomy Specimens From Patients With Carcinoma of the Urinary Bladder Version: UrinaryBladder 4.0.1.1 Protocol Posting Date: February 2019 CAP Laboratory Accreditation
Genitourinary. Presentation Outline. Genitourinary System 12/14/2011. FCDS 2011 Educational Webcast Series December 15, 2011
 Genitourinary FCDS 2011 Educational Webcast Series December 15, 2011 1 Susan Smith Pierce, CTR Gema Midence, MBA, CTR Steven Peace, BS, CTR Presentation Outline Overview including Anatomy and General Information
Genitourinary FCDS 2011 Educational Webcast Series December 15, 2011 1 Susan Smith Pierce, CTR Gema Midence, MBA, CTR Steven Peace, BS, CTR Presentation Outline Overview including Anatomy and General Information
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Protocol for the Examination of Specimens From Patients With Carcinoma of the Urinary Bladder
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Urinary Bladder Protocol applies primarily to invasive carcinomas and/or associated epithelial lesions, including carcinoma
Protocol for the Examination of Specimens From Patients With Carcinoma of the Urinary Bladder Protocol applies primarily to invasive carcinomas and/or associated epithelial lesions, including carcinoma
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
Kyle L. Ziegler, CTR. California Cancer Registry U.C. Davis Health System
 Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
UICC 8 th Edition Errata 25 th of May 2018
 UICC 8 th Edition Errata 25 th of May 2018 ions are in italics Head and Neck Tumours Page 19 Oral Cavity T2 T3 T4a Tumour 2 cm or less in greatest dimension and more than 5 mm but no more than 10 mm depth
UICC 8 th Edition Errata 25 th of May 2018 ions are in italics Head and Neck Tumours Page 19 Oral Cavity T2 T3 T4a Tumour 2 cm or less in greatest dimension and more than 5 mm but no more than 10 mm depth
Transitional Cell Papilloma 2-3% Inverted Papilloma Rare
 BLADDER TUMORS Benign Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
BLADDER TUMORS Benign Transitional Cell Papilloma 2-3% Inverted Papilloma Rare Malignant Transitional (Urothelial) Carcinoma90% Carcinoma In-Situ (By Itself) 5-10% Squamous Cell Carcinoma 3-7% Adenocarcinoma
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
FINALIZED SEER SINQ QUESTIONS
 0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
0076 Source 1: WHO Class CNS Tumors pgs: 33 MP/H Rules/Histology--Brain and CNS: What is the histology code for a tumor originating in the cerebellum and extending into the fourth ventricle described as
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Protocol for the Examination of Specimens from Patients with Carcinoma of the Urinary Bladder
 Protocol for the Examination of Specimens from Patients with Carcinoma of the Urinary Bladder Protocol applies primarily to invasive and noninvasive carcinomas, including carcinoma in situ. Version: Protocol
Protocol for the Examination of Specimens from Patients with Carcinoma of the Urinary Bladder Protocol applies primarily to invasive and noninvasive carcinomas, including carcinoma in situ. Version: Protocol
A301 VI- Various cancer tissues with corresponding normal tissues
 A301 VI- Various cancer tissues with (formalin fixed) For research use only Specifications: No. of cases: 28 Tissue type: Various cancer tissues with No. of spots: 2 spots from each cancer case (56 spots)
A301 VI- Various cancer tissues with (formalin fixed) For research use only Specifications: No. of cases: 28 Tissue type: Various cancer tissues with No. of spots: 2 spots from each cancer case (56 spots)
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate