MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs
|
|
|
- Edmund Hodge
- 6 years ago
- Views:
Transcription


1 MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany
2 Disclosure of speaker s interests Hans Michael Kvasnicka Research funding & Consulting: Novartis, Incyte

3 Principles and rationale of the WHO 2016 classification (updating the 4 th edition) the WHO classification emphasizes the identification of distinct clinicopathological entities, rather than just being a "cell of origin" classification stresses an integrated approach to disease definition by incorporation of key available information including morphology, molecular and cytogenetic findings, immunophenotype, and clinical features the work of a large number of hematopathologists, but developed with the active advice and consent of clinicians
4 Modification of the BCR/ABL-negative MPN classification according to WHO 2016/2017 Polycythemia vera (PV) lowering of hemoglobin or hematocrit thresholds role of BM morphology as a major criterion Essential thrombocythemia (ET) differentiation of "true ET" from prefibrotic/early primary myelofibrosis (prepmf) emphasizing the lack of reticulin fibrosis at onset Primary myelofibrosis (PMF) definition of minor clinical criteria in prepmf histomorphological features of prepmf inclusion of new molecular findings




5 Overlapping clinical and molecular features in MPN PMF Anemia LDH Leukoerythroblastosis Megakaryocytic and granulocytic proliferation & myelofibrosis Predominant megakaryocytic proliferation without atypia ET PLTs CALR or MPL Clonal marker JAK2 Splenomegaly Symptoms Hb HCT EPO PV Trilineage proliferation (panmyelosis)
6 Survival and impact of age at diagnosis in MPN Essential thrombocythemia Polycythemia vera Primary myelofibrosis Tefferi et al. Blood 2014;124: ; Srour SA, et al. Br J Haematol. 2016;174:382-96
7 WHO 2016/2017 criteria for MPN Major criteria Minor criteria Diagnosis PV ET prepmf PMF Hb > 16.5 g/dl in men, Hb > 16.0 g/dl in women OR, Hct > 49% in men, Hct >48% in women OR, increased red cell mass BM biopsy showing trilineage proliferation (panmyelosis) JAK2 mutation subnormal serum EPO level all three major criteria, or the first two major criteria and the minor criterion PLT 450 x 10 9 /L BM biopsy with predominent proliferation of megakaryocytes not meeting WHO criteria for other MPN subtype JAK2, CALR or MPL mutation presence of a clonal marker or absence of evidence for reactive THR all four major criteria or the first three major criteria and one of the minor criteria BM biopsy with megakaryocytic proliferation and atypia, without reticulin fibrosis >grade 1 not meeting WHO criteria for other MPN subtype or MDS, or other JAK2, CALR or MPL mutation or presence of other clonal markers* or absence of reactive myelofibrosis** at least one of the following: a. anemia b. leukocytosis >11K/uL c. splenomegaly d. LDH increase all three major criteria, and minor criteria BM biopsy with megakaryocytic proliferation and atypia, reticulin and/or collagen fibrosis grade 2/3 not meeting WHO criteria for other MPN subtype or MDS, or other JAK2, CALR or MPL mutation or presence of other clonal markers* or absence of reactive myelofibrosis** at least one of the following: a. anemia b. leukocytosis >11K/uL c. splenomegaly d. LDH increase e. leukoerythroblastosis all three major criteria, and minor criteria * in the absence of any of the 3 major clonal mutations, the search for the most frequent accompanying mutations (ASXL1, EZH2, TET2, IDH1/IDH2, SRSF2, SF3B1) are of help in determining the clonal nature of the disease. **bone marrow fibrosis secondary to infection, autoimmune disorder or other chronic inflammatory condition, hairy cell leukemia or other lymphoid neoplasm, metastatic malignancy, or toxic (chronic) myelopathies. Arber D, et al. Blood 2016 Apr 11 / PMID
 JAK2 (60%) JAK2 (>95%) CALR (20%-25%)")
 'wild-type' All MPN-associated JAK2 (V617F) mutations directly")
 result in abnormal activation of JAK/STAT TN and other")


8 The current genetic landscape concerning phenotypic driver mutations in MPN ET PMF PV JAK2 (60%) JAK2 (60%) JAK2 (>95%) CALR (20%-25%) CALR (20%-30%) MPL (3%-6%) MPL (5%-8%) 5%-15% 5%-10% ~ JAK2 Exon 12 (5%) 'wild-type' All MPN-associated JAK2 (V617F) mutations directly (JAK2), CALR Exon 9 indirectly (MPL) or through complex mechanisms MPL (CALR) result in abnormal activation of JAK/STAT TN and other signaling pathways JAK2 Exon 12 Vannucchi AM, et al. CA Cancer J Clin. 2009; 59:171-91; Akada H, et al. Blood. 2010;115: ; Harrison C & Vannucchi A, Blood 2016;127: ?? clonal / unknown 'triple-negative'?? clonal / unknown exclude reactive conditions exclude MDS/MPN or MDS
9 WHO criteria for Polycythemia vera (PV) Major criteria: 1. Hb > 16.5 g/dl in men, Hb > 16.0 g/dl in women OR, Hct > 49% in men, Hct >48% in women OR, Increased red cell mass 2. Bone marrow biopsy showing hypercellularity for age with trilineage growth (panmyelosis) including prominent erythroid, granulocytic and megakaryocytic proliferation with pleomorphic megakaryocytes (differences in size) 3. Presence of JAK2 mutation Minor criterion: Subnormal serum EPO level Diagnosis of PV requires meeting either all three major criteria, or the first two major criteria and the minor criterion Arber et al., Blood (2016) 127:

 including prominent erythroid,")

10 WHO criteria for Polycythemia vera (PV) Major criterion: Bone marrow biopsy showing hypercellularity for age with trilineage growth (panmyelosis) including prominent erythroid, granulocytic, and megakaryocytic proliferation with pleomorphic, mature megakaryocytes (differences in size)

 may be detected that indicates a more")
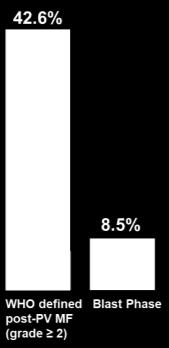
11 WHO 2016 criteria for PV In cases with sustained absolute erythrocytosis (Hb levels >18.5 g/dl, Hct >55.5 % in men or >16.5 g/dl, 49.5% in women, bone marrow biopsy may not be necessary for diagnosis if major criterion 3 and the minor criterion are present However, only by performing a bone marrow biopsy an initial myelofibrosis (up to 20%) may be detected that indicates a more rapid progression to overt myelofibrosis (post-pv MF) PV, MF-0 PV, MF-1 Barbui T et al. Blood 2012;119:
 Progression to overt MF (post-pv MF) Grade at")

12 Progression in PV stratified by the presence of initial BM fibrosis at diagnosis MF-0 post-pv MF n=262 MF 1 Myelofibrosis-free survival (months) Progression to overt MF (post-pv MF) Grade at diagnosis Incidence per 100 pts./yrs. cumulative incidence 5 yrs. 10 yrs. 15 yrs. MF MF Barbui et al. Blood, 2012, 119: Barraco et al., Blood Cancer J (2017) 7:e538
 dynamics of JAK2 allele")
 53:2210-2213 Passamonti et al.")
 35:177-182 Alvarez-Larran et al.")
13 JAK2 allele burden in PV correlates with risk of transformation to post-pv MF and blast phase (saml) dynamics of JAK2 allele burden Koren-Michowitz et al., Leuk Lymphoma (2012) 53: Passamonti et al., Leukemia (2010) 24: Silver et al., Leuk Res (2011) 35: Alvarez-Larran et al., Am J Hematol (2014) 89: Shirane S et al., Int J Hematol (2015) 101:

14 The rate of transformation from JAK2-mutated ET to PV is influenced by an accurate WHO-defined clinicomorphological diagnosis 5% 1% [n=268] ET JAK2+ [n=422] ET wt Kvasnicka HM & Thiele J, Am J Hematol, 2010, 85:62-99 Barbui et al., Leukemia, 2015, 29:
 risk at 10 years 0.15 (0.11-0.21) ET JAK2 pos early PV overt PV 3.01 (1.75-5.18) 0.11 (0.04-0.24) 0.28 (0.16-0.47) 1.99 (1.22-3.25) 0.")
 might be associated with less aggressive treatment less frequent use of phlebotomies and cytoreduction in early PV identification of early PV in")
15 Young patients (< 40 years) with early PV have a high incidence of thrombosis Incidence of Thrombosis IR % pts/yr 1.36 ( ) risk at 5 years 0.06 ( ) risk at 10 years 0.15 ( ) ET JAK2 pos early PV overt PV 3.01 ( ) 0.11 ( ) 0.28 ( ) 1.99 ( ) 0.08 ( ) 0.23 ( ) might be associated with less aggressive treatment less frequent use of phlebotomies and cytoreduction in early PV identification of early PV in young JAK2- mutated patients is important in order to reduce risk and optimize treatment Lussana F, et al. BJH 2014, 167:




16 Dynamics of the disease process in PV Early PV Manifestation Transformation ~10%-15% mimicking ET yrs. post-pv MF (MF-2/3) ~ 20 % JAK2 + EPO definite increase in red cell mass Evolution of high-risk disease features Resistance/intolerance to standard therapy (HU) < 10 % post-pv MF with blastic transformation increased need for phlebotomy leukocytosis, thrombocytosis splenomegaly symptoms thrombotic events increased need for phlebotomy leukocytosis, thrombocytosis progressive splenomegaly cytopenia burdensome symptoms
17 HU Resistance/Intolerance and Disease Progression in PV resistance and intolerance to HU occurs in 11%-13% resistance to HU is associated with a 5.6-fold increase in the risk of death (HR, 5.6; 95% CI, 2.7%-11.9%; p < 0.001) resistance to HU is associated with an 6.8 fold increased risk of transformation into acute leukemia or myelofibrosis (HR, 6.8; 95% CI, 3.0%-15.4%; p < 0.001) both resistance to HU and lack of WBC response are prognostically important Survival Progression/Transformation Alvarez-Larrán et al., Blood 2012;119:




18 BM morphology in progressive PV at time of treatment failure (HU resistance/intolerance) Post-PV myelofibrosis (MF) Heterogeneity of BM features MDS like features increased blast count toxic hypoplasia Kvasnicka et al., USCAP 2017
19 WHO criteria for essential thrombocythemia (ET) Major criteria: 1. Platelet count equal to or greater than 450 x 10 9 /ul 2. Bone marrow biopsy showing proliferation mainly of the megakaryocyte lineage with increased numbers of enlarged, mature megakaryocytes with hyperlobulated nuclei. No significant increase or left-shift of neutrophil granulopoiesis or erythropoiesis and very rarely minor increase in reticulin fibers. 3. Not meeting WHO criteria for BCR-ABL1+ CML, PV, PMF, myelodysplastic syndromes, or other myeloid neoplasms 4. Presence of JAK2, CALR or MPL mutation Minor criteria: Presence of a clonal marker or absence of evidence for reactive thrombocytosis Diagnosis of ET requires meeting all four major criteria or the first three major criteria and one of the minor criteria Arber et al., Blood (2016) 127:


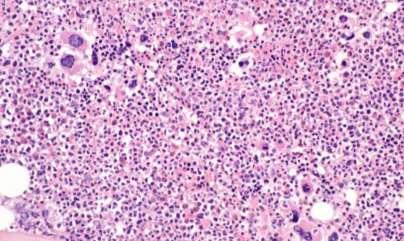
20 WHO criteria for ET Major criterion Bone marrow biopsy showing proliferation mainly of the megakaryocyte lineage with increased numbers of enlarged, mature megakaryocytes with hyperlobulated nuclei. No significant increase or left-shift in neutrophil granulopoiesis or erythropoiesis and very rarely minor increase in reticulin fibers.
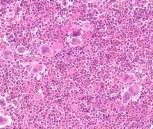
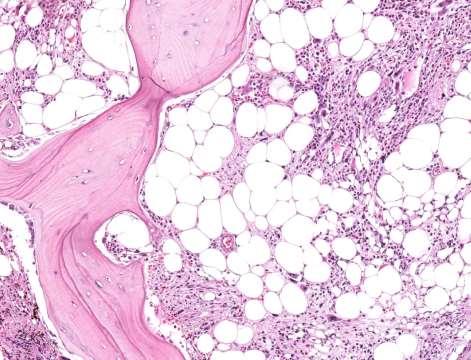
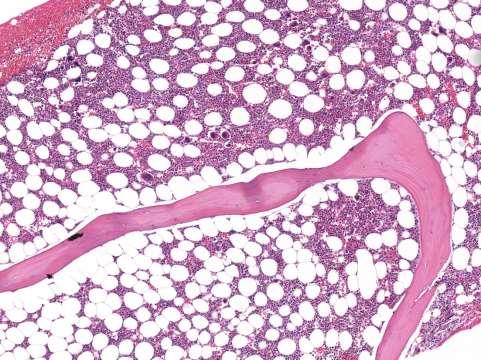
21 [ET] H&E
![[ET] PAS](/docs-images/75/71857000/images/22-0.jpg)
22 [ET] PAS
23 [ET] PAS


24 CALR mutated ET patients have lower rates of thrombosis CALR mutated and wild-type patients may be at a very low risk of thrombosis, and the effect of the CALR mutation may be particularly evident in younger patients P-value = P-value adjusted for age = 0.02 P-value adjusted for thrombosis history = 0.01 P-value adjusted for age, CV risk and thrombosis history = 0.02 HR 95% CI JAK MPL CALR Rotunno G, et al. Blood 2014, 6;123: Rumi E, et al. Blood 2014, 6;123: Gangat N, et al. Eur J Haematol 2015, 94:31-36 Elala et al., Am J Hematol (2016) 91:
25 Morphological criteria (major criteria) for the diagnosis of prepmf and ET according to WHO ET prepmf
26 WHO criteria for prepmf Major criteria: 1. Megakaryocytic proliferation and atypia, without reticulin fibrosis > grade 1 and accompanied by increased age-adjusted bone marrow cellularity, granulocytic proliferation and often decreased erythropoiesis 2. Not meeting WHO criteria for ET, PV, BCR-ABL1+ CML, myelodysplastic syndromes, or other myeloid neoplasms 3. Presence of JAK2, CALR or MPL mutation or in the absence of these mutations,presence of an other clonal marker* or absence of minor reactive myelofibrosis** * in the absence of any of the 3 major clonal mutations, the search for the most frequent accompanying mutations (ASXL1, EZH2, TET2, IDH1/IDH2, SRSF2, SF3B1) are of help in determining the clonal nature of the disease. **bone marrow fibrosis secondary to infection, autoimmune disorder or other chronic inflammatory condition, hairy cell leukemia or other lymphoid neoplasm, metastatic malignancy, or toxic (chronic) myelopathies. Arber et al., Blood (2016) 127:

 Histopathology of hematopoiesis Megakaryocyte changes are")

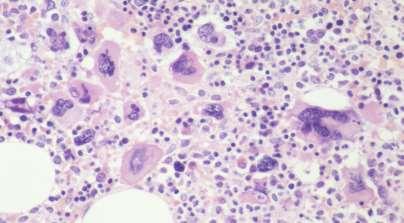
27 WHO criteria for prepmf Megakaryocytic proliferation and atypia (small to large megakaryocytes with an aberrant nuclear/ cytoplasmic ratio and hyperchromatic, bulbous, or irregularly folded nuclei and dense clustering) Histopathology of hematopoiesis Megakaryocyte changes are accompanied by an increased ageadjusted bone marrow cellularity, granulocytic proliferation and often decreased erythropoiesis (reticulin fibrosis grade 0 or 1)

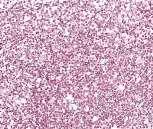
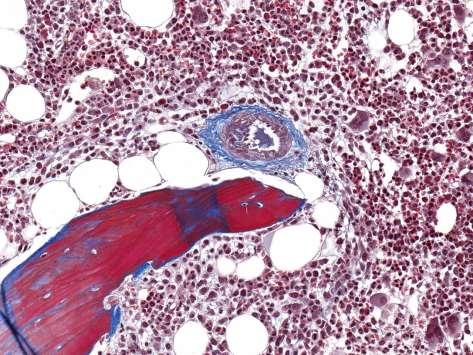
28 [prepmf / MF-0] CAS

29 [prepmf / MF-0] PAS

30 [prepmf / MF-0] PAS

31 Morphological features helpful in distinguishing ET from prepmf* ET prepmf ET Cellularity Normal Increased M/E ratio Normal Increased Megakaryocyte Rare Frequent dense clusters $$ Megakaryocyte size Large Variable prepmf Megakaryocyte nuclear lobulation Hyperlobated Bulbous/hypolobated Reticulin fibrosis grade 1** Rare More frequent * based on a representative BM biopsy (> 1.5 cm) age matched cellularity ** according to WHO grading $$ WHO definition of a megakaryocyte cluster: 3 or more megakaryocytes lying strictly adjacent - without other hematopoietic cells lying in between Florena et al., Haematologica, 2004;89: Thiele J & Kvasnicka HM, 2009, Curr Hematol Malig Rep, 4:33-40 Kvasnicka HM & Thiele J, 2010, Am J Hematol, 85:62-69 Thiele, J et al., 2011, Blood, 117: Gianelli U, et al., 2013, Mod Pathol, PMID:
32 Frequency of minor criteria in 954 patients with prepmf and ET Parameter Anemia cut-off M 13 g/dl F 12 g/dl prepmf [n=706] ET [n=248] 36.4 % 22.6 % Spleen 1 cm 43.6 % 26.6 % LDH 220 U/L 84.4 % 45.2 % Blasts 1 % (Myeloblasts + Erythroblasts) 6.2 % 1.2 % WBC 11 x 10 9 /L 51.3 % 33.1 % Kvasnicka et al., unpublished data
33 WHO criteria for prepmf Minor criteria: Presence of at least one of the following, confirmed in two consecutive determinations: a. Anemia not attributed to a comorbid condition b. Leukocytosis >11K/µL c. Palpable splenomegaly d. LDH increased to above upper normal limit of institutional reference range Diagnosis of prepmf requires meeting all three major criteria, and minor criteria. Arber et al., Blood (2016) 127:


34 ET vs. prepmf: Why does it matter? Differences in the biology of ET and prepmf prepmf has higher JAK2V617F and MPLW515L allele burden than ET alterations of megakaryocyte differentiation and function in vitro distinguishes prepmf from ET patients high mobilization of circulating endothelial colony forming cells (ECFCs) is characteristic of prepmf different gene signature in prepmf proplatelet architecture of in vitro derived MEGs Clinical differences between ET and prepmf clinical presentation risk of transformation outcome prediction Therapeutic considerations slow-down of disease progression in prepmf with a new molecularly targeted therapy Barosi, Best Practice & Research Clinical Haematology, 2014, 27,
35 Differences in mutation load in WHO defined ET and early PMF (prepmf) CALR JAK2 Palandri et al., Leukemia (2015) 29:
 Survival and Disease Progression in")

36 Survival in ET and prepmf Relative survival in ET and prepmf ET and pre-fibrotic MF vs Europe* Age- and sex-adjusted actuarial survival curves *EUROSTAT 2008 (crude death rates, all causes of death, EU 27 countries) Survival and Disease Progression in Essential Thrombocythemia Are Significantly Influenced by Accurate Morphologic Diagnosis: An International Study of 1,104 Patients. Barbui et al., J Clin Oncol 2011;29: Barbui et al., J Clin Oncol. 2011;29: Kvasnicka & Thiele, Semin Thromb Hemost. 2006;32:

37 Cumulative Incidence (%) Cumulative Incidence (%) Disease progression in ET and prepmf International Study on 1,104 Patients Transformation to overt MF ET prepmf Risk of leukemic transformation ET prepmf 8 4 p= p= years 10 yrears 15 years 0 5 years 10 yrears 15 years Barbui et al., J Clin Oncol. 2011;29:

38 Risk of thrombosis and bleeding in prepmf and ET major bleeding associated with thrombocytosis is more often seen in prepmf low-dose aspirin exacerbates these hemorrhagic events venous thrombosis (mainly atypical, i.e. splanchnic & mesenterial) are more common in prepmf higher leukocyte count in prepmf correlates with an increased risk for arterial thrombosis Risk of thrombosis prepmf Cumulative risk of thrombosis (at 15-years) p = ET Finazzi et al., Leukemia (2012) 26: Buxhofer-Ausch et al., Am J Hematol (2012) 87: Rupoli et al., Diagn Pathol (2015) 10:29
39 Features of prepmf and its distinction from ET higher JAK2 V617F allele burden higher numbers of circulating progenitor cells higher rate of progression to overt MF and greater incidence of blast phase and worse survival Combined event-free survival ET more bleeding at high platelet counts increased frequency of thrombotic events, particularly arterial factors associated with thrombosis in prepmf: Platelet count > 450 x 10 9 /L Presence of 1 cardiovascular risk factor Age > 60 y JAK2 mutation prior thrombosis prepmf: 3.43% ET: 1.29% patients/year, P=0.01 prepmf Barbui et al., Blood. 2010;115: Barbui et al., J Clin Oncol. 2011;29: Barbui et al., Blood. 2012;120: Cervantes et al., Leukemia. 2006;20:55-60 Elliott et al., Haematologica. 2010;95: Finazzi et al., Leukemia. 2012;26: Finazzi et al., Leukemia. 2015;29: Geissler et al., Am J Hematol. 2014;89: Palandri et al., Leukemia. 2015;29:
40 WHO criteria for overt PMF Major criteria: 1. Presence of megakaryocytic proliferation and atypia, usually accompanied by either reticulin and/or collagen fibrosis grades 2 or 3 2. Not meeting WHO criteria for ET, PV, BCR-ABL1+ CML, myelodysplastic syndromes, or other myeloid neoplasms 3. Presence of JAK2, CALR or MPL mutation or in the absence of these mutations,presence of an other clonal marker* or absence of reactive myelofibrosis** * in the absence of any of the 3 major clonal mutations, the search for the most frequent accompanying mutations (ASXL1, EZH2, TET2, IDH1/IDH2, SRSF2, SF3B1) are of help in determining the clonal nature of the disease. ** bone marrow fibrosis secondary to infection, autoimmune disorder or other chronic inflammatory condition, hairy cell leukemia or other lymphoid neoplasm, metastatic malignancy, or toxic (chronic) myelopathies. Arber et al., Blood (2016) 127:
41 WHO criteria for overt PMF Minor criteria : Presence of at least one of the following, confirmed in two consecutive determinations: a. Anemia not attributed to a comorbid condition b. Leukocytosis >11K/uL c. Palpable splenomegaly d. LDH increased to above upper normal limit of institutional reference range e. Leukoerythroblastosis Diagnosis of overt PMF requires meeting all three major criteria, and minor criteria. Arber et al., Blood (2016) 127:
")
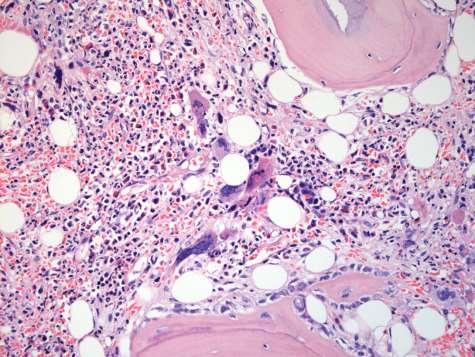
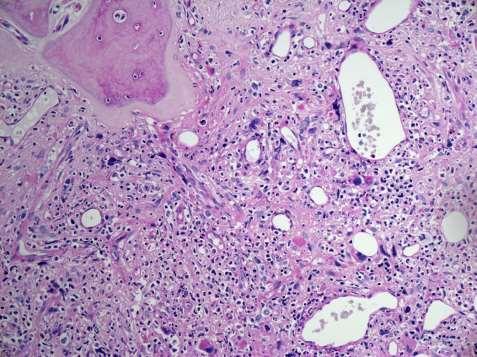
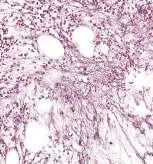
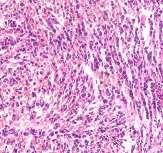
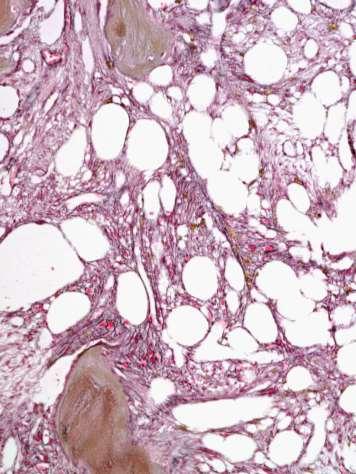
42 overt PMF (MF-3) heterogeneity of morphological presentation
")


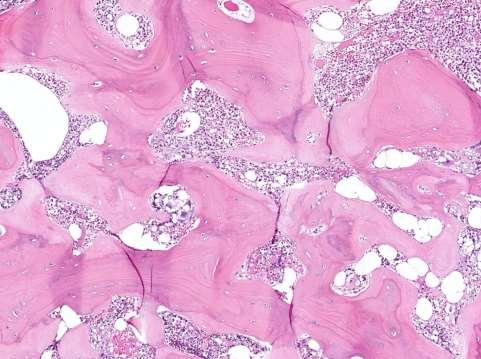
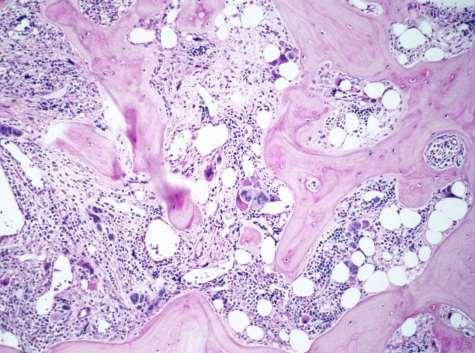
43 overt PMF (PMF-3) New WHO grading for collagen deposition osteosclerosis


")

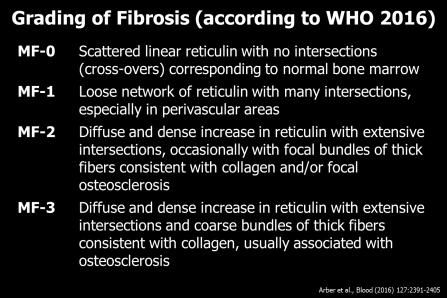
44 MF-0 MF-2 MF-1 MF-3 Arber et al., Blood (2016) 127:


45 Assessment of myelofibrosis after therapy fiber density should be assessed only in hematopoietic areas areas of prominent scleredema and/or scarring should be included in the overall grading of myelofibrosis if the pattern is heterogenous, the final score is determined by the highest grade present in at least 30% of the marrow area quality of the reticulin stain (Gomori or Gordon & Sweets) should be assessed by detection of normal staining in vessel walls as internal controls disregard lymphoid nodules and vessels and fibers framing adipocytes Thiele et al., Haematologica 2005 ELN consensus 2013


46 Problems of Reticulin Staining Kvasnicka et al., Histopathology, 2016, 68:



47 Grading of collagen Grade 0 Grade 1 Grade 2 Grade 3

48 Grading of osteosclerosis Grade 0 Grade 1 Grade 2 Grade 3
49 Comparison of survival among patients with PMF stratified by their mutational status Prognostic implication of triple-negative cases Prognostic implication of calreticulin type 1 or type 1-like variants Type-1/type-1 like CALR mutated CALR type 1: 52-bp deletion CALR type 2: 5-bp insertion (CALRdel52) (CALRins5) Tefferi et al., Blood, 2014, 124, Tefferi et al., Blood, 2014, 124, Tefferi et al., Abstract #2801, ASH 2015 Kourie et al., Br J Haematol. 2016; DOI: /bjh.14259
50 Number of somatically acquired mutations impacts prognosis in PMF Presence of adverse variants/mutations (ASXL1, SRSF2, CBL, KIT, RUNX1, SH2B3, CEBPA) Number of adverse variants/mutations Vannucchi et al., Leukemia, 2013, 27: Guglielmelli et al., Leukemia, 2014, 28: Tefferi et al., Blood Advances (2016) 1:



51 The type and the number of mutations determine the phenotype of PMF proliferation is driven mainly by signaling mutations (JAK2,CALR, and MPL) while most of the mutations in epigenetic regulators and spliceosome components lead to differentiation defects the heterogeneity of the disease and its prognosis are dependent on the respective levels of additional mutations 1 Mutation 2 Mutations 3 Mutations Vainchenker et al., F1000Res. 2016:5

52 Clinical impact of bone marrow fibrosis in PMF degree of fibrosis and its changes over time in patients with myelofibrosis is an area of ongoing research standard pharmacotherapy like HU has not been shown to result in bone marrow fibrosis improvement recent data suggest that degree of BM fibrosis is an independent prognostic factor in PMF in multivariate analysis Survival and BM Fibrosis Kvasnicka & Thiele, Semin Thromb Hemost, 2006, 32, Thiele J, Kvasnicka HM, et al. Histopathology. 2003;43: Guglielmelli, et al. Am J Hematol. 2016;91:




53 IPSS and Grading of MF in PMF The WHO grading of BM fibrosis significantly impacts clinical based prognostication of patients with PMF 80% 60% 40% 20% 0% Low Int-1 Int-2 High MF-0 MF-1 MF-2 MF-3 MF-0 MF-1 Hazard ratios for combined IPSS and MF Low Int-1 Int-2 High MF MF MF MF MF-2 MF-3 Gianelli U et al, Mod Pathol 2012; Vener et al, Blood 2008
54 Prognostic impact of bone marrow fibrosis in PMF impact of BM fibrosis is significant in low & int-1 IPSS risk categories Guglielmelli, et al. Am J Hematol. 2016;91:


55 Prognostic impact of bone marrow fibrosis in PMF no correlation between fibrosis grade and phenotypic driver mutations frequency of HMR pts increased progressively with grade of fibrosis significant association between grade of fibrosis and ASXL1 and EZH2 Guglielmelli, et al. ASH Abstract #351 Guglielmelli, et al. Am J Hematol. 2016;91:

56 Disease evolution in Myelofibrosis Morphological progression?? JAK2 allele burden?? Other Mutations ASXL1, SRSF2, EZH2, TET2, DNMT3A, CBL, IDH1/2 Bone marrow fibrosis / Osteosclerosis Accumulation of dysplastic features (MDS-like morphology) Complex karyotype Acquired new mutations Progression of MF




57 BM changes in PMF following HU Control of Myeloproliferation + Regression of BM fibrosis <13% Molecular response - Associated risk of MDS/AML +/?




58 Baseline BM fibrosis MF grade 3 osteosclerosis grade 3 variable cellularity 192 weeks post ruxolitinib major morphological remission normal cellularity BM fibrosis grade 0


59 BM changes in PMF following JAK Inhibitors Control of Myeloproliferation ++ Regression of BM fibrosis >30% Molecular response 11% Associated risk of MDS/AML -/-
 Time to treatment discontinuation (weeks) Patel et al.")
60 Molecular Risk & Time to Treatment Failure in Patients Treated with a JAK Inhibitor Spleen response ( 50%) was inversely correlated with the number of mutations Patients with 3 mutations also had a shorter time to treatment discontinuation and shorter overall survival than those with fewer mutations Time to treatment discontinuation (weeks) Time to treatment discontinuation (weeks) Patel et al., Blood (2015) 126:
61 Summary and Conclusion in PV morphology of the BM is up-graded to a major criterion and the diagnostic thresholds for Hb and Hct were lowered disease progression in PV is heterogeneous and significantly associated with HU resistance in ET differentiation from prepmf is underscored by standardization of BM features and by the lack of reticulin fibrosis (< 5%) at onset in prepmf minor clinical criteria are more clearly defined number of somatically acquired mutations impacts prognosis in PMF in addition to clinical data and mutation profile, BM findings will be maintained as major diagnostic criteria
New WHO Classification of Myeloproliferative Neoplasms
 New WHO Classification of Myeloproliferative Neoplasms Hans Michael Kvasnicka Senckenberg Institute of Pathology, University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Principles and rationale
New WHO Classification of Myeloproliferative Neoplasms Hans Michael Kvasnicka Senckenberg Institute of Pathology, University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Principles and rationale
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Bone marrow histopathology in Ph - CMPDs. - the new WHO classification - Juergen Thiele Cologne, Germany
 Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms
 Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Intro alla patologia. Giovanni Barosi. Fondazione IRCCS Policlinico San Matteo Pavia
 Settima Giornata Fiorentina dedicata ai pazienti con malattie mieloproliferative croniche Sabato 13 Maggio 2017 CRIMM Centro di Ricerca e Innovazione per le Malattie Mieloproliferative AOU Careggi Intro
Settima Giornata Fiorentina dedicata ai pazienti con malattie mieloproliferative croniche Sabato 13 Maggio 2017 CRIMM Centro di Ricerca e Innovazione per le Malattie Mieloproliferative AOU Careggi Intro
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Managing ET in Tiziano Barbui MD
 Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
Managing ET in 2019 Tiziano Barbui MD (tbarbui@asst-pg23.it) Hematology and Foundation for Clinical Research, Hospital Papa Giovanni XXIII Bergamo, Italy Managing ET in 2019 Establish diagnosis Risk Stratification
WHO 2016/17 update on Myeloproliferative Neoplasms. Anna Ruskova Auckland City Hospital New Zealand
 WHO 2016/17 update on Myeloproliferative Neoplasms Anna Ruskova Auckland City Hospital New Zealand BLOOD, 19 MAY 2016 x VOLUME 127, NUMBER 20 2 2016/17 Classification of Myeloproliferative Neoplasms Chronic
WHO 2016/17 update on Myeloproliferative Neoplasms Anna Ruskova Auckland City Hospital New Zealand BLOOD, 19 MAY 2016 x VOLUME 127, NUMBER 20 2 2016/17 Classification of Myeloproliferative Neoplasms Chronic
Prognostic models in PV and ET
 Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Emerging diagnostic and risk stratification criteria
 PV STATE OF MIND Polycythemia vera: Emerging diagnostic and risk stratification criteria Rami S. Komrokji, MD Moffitt Cancer Center, Tampa, Florida Disclosure These slides were developed by Incyte Corporation
PV STATE OF MIND Polycythemia vera: Emerging diagnostic and risk stratification criteria Rami S. Komrokji, MD Moffitt Cancer Center, Tampa, Florida Disclosure These slides were developed by Incyte Corporation
The prognostic relevance of serum lactate dehydrogenase and mild bone marrow reticulin fibrosis in essential thrombocythemia
 Received: 3 February 2017 Revised: 13 February 2017 Accepted: 14 February 2017 DOI: 10.1002/ajh.24689 RESEARCH ARTICLE The prognostic relevance of serum lactate dehydrogenase and mild bone marrow reticulin
Received: 3 February 2017 Revised: 13 February 2017 Accepted: 14 February 2017 DOI: 10.1002/ajh.24689 RESEARCH ARTICLE The prognostic relevance of serum lactate dehydrogenase and mild bone marrow reticulin
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms
 Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Molecular aberrations in MPN. and use in the clinic. Timothy Devos MD PhD
 Molecular aberrations in MPN and use in the clinic Timothy Devos MD PhD MB&C2017 24-3-2017 Introduction 1951: William Dameshek MPD MPN = clonal, hematopoietic stem cell disorders, proliferation in BM of
Molecular aberrations in MPN and use in the clinic Timothy Devos MD PhD MB&C2017 24-3-2017 Introduction 1951: William Dameshek MPD MPN = clonal, hematopoietic stem cell disorders, proliferation in BM of
Histological evaluation of myeloproliferative neoplasms
 Journal of clinical and experimental hematopathology Vol. 58 No.2, 45-50, 2018 JC lin EH xp ematopathol Review Article Histological evaluation of myeloproliferative neoplasms Hideyo Fujiwara In 2017, the
Journal of clinical and experimental hematopathology Vol. 58 No.2, 45-50, 2018 JC lin EH xp ematopathol Review Article Histological evaluation of myeloproliferative neoplasms Hideyo Fujiwara In 2017, the
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
MALATTIE MIELOPROLIFERATIVE CRONICHE
 MALATTIE MIELOPROLIFERATIVE CRONICHE Dott. Roberto Latagliata Policlinico Umberto I Università Sapienza, Roma Highlights from EHA 2017: some points to address today WHO 2016 MPN classification: hot topics
MALATTIE MIELOPROLIFERATIVE CRONICHE Dott. Roberto Latagliata Policlinico Umberto I Università Sapienza, Roma Highlights from EHA 2017: some points to address today WHO 2016 MPN classification: hot topics
Understanding Your Blood Work Results
 Understanding Your Blood Work Results Carlos Besses, MD, hd Hematology Department Hospital del Mar - IMIM, Barcelona Carlos Besses Disclosures Novartis Honorarium Speaker Shire Honorarium Speaker Galena
Understanding Your Blood Work Results Carlos Besses, MD, hd Hematology Department Hospital del Mar - IMIM, Barcelona Carlos Besses Disclosures Novartis Honorarium Speaker Shire Honorarium Speaker Galena
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Myeloproliferative Neoplasms and Treatment Overview
 Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Should Mutation Status in PMF Guide Therapy? No! Brady L. Stein, MD MHS Assistant Professor of Medicine Division of Hematology/Oncology
 Should Mutation Status in PMF Guide Therapy? No! Brady L. Stein, MD MHS Assistant Professor of Medicine Division of Hematology/Oncology Case presentation A 67 yo woman presents to transition care, as her
Should Mutation Status in PMF Guide Therapy? No! Brady L. Stein, MD MHS Assistant Professor of Medicine Division of Hematology/Oncology Case presentation A 67 yo woman presents to transition care, as her
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease
 The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
The Internists Approach to Polycythemia and Implications of Uncontrolled Disease Mary Jo K. Voelpel, DO, FACOI, MA, CS Associate Clinical Professor MSU-COM Disclosures NONE Overview 1. Objectives 2. Case
MYELOPROLIFERATIVE NEOPLASMS
 9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
MPNs: JAK2 inhibitors & beyond. Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt
 NCI, Cairo University, Egypt") MPNs: JAK2 inhibitors & beyond Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt Myeloproliferative Neoplasms (MPNs) AGENDA: 1. Molecular biology 2. New WHO diagnostic criteria. 3. Risk stratification
MPNs: JAK2 inhibitors & beyond Mohamed Abdelmooti (MD) NCI, Cairo University, Egypt Myeloproliferative Neoplasms (MPNs) AGENDA: 1. Molecular biology 2. New WHO diagnostic criteria. 3. Risk stratification
The myeloproliferative neoplasms, unclassifiable: clinical and pathological considerations
 2017 USCAP, Inc All rights reserved 0893-3952/17 $32.00 169 The myeloproliferative neoplasms, unclassifiable: clinical and pathological considerations Umberto Gianelli 1, Daniele Cattaneo 2, Anna Bossi
2017 USCAP, Inc All rights reserved 0893-3952/17 $32.00 169 The myeloproliferative neoplasms, unclassifiable: clinical and pathological considerations Umberto Gianelli 1, Daniele Cattaneo 2, Anna Bossi
Essential thrombocythemia treatment algorithm 2018
 Tefferi et al. (2018) 8:2 DOI 10.1038/s41408-017-0041-8 CURRENT TREATMENT ALGORITHM Essential thrombocythemia treatment algorithm 2018 Ayalew Tefferi 1, Alessandro M. Vannucchi 2 and Tiziano Barbui 3 Open
Tefferi et al. (2018) 8:2 DOI 10.1038/s41408-017-0041-8 CURRENT TREATMENT ALGORITHM Essential thrombocythemia treatment algorithm 2018 Ayalew Tefferi 1, Alessandro M. Vannucchi 2 and Tiziano Barbui 3 Open
Disclosures. I do not have anything to disclose. Shared Features of MPNs. Overview. Diagnosis and Molecular Monitoring in the
 Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Target Therapy Era C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not have
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Target Therapy Era C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not have
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes A critical reappraisal of anagrelide in the management of ET
 European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes 2012 Clinical i l Aspects of Polycythemia and Essential Thrombocythemia A critical reappraisal of anagrelide in the management
European Focus on Myeloproliferative Diseases and Myelodysplastic Syndromes 2012 Clinical i l Aspects of Polycythemia and Essential Thrombocythemia A critical reappraisal of anagrelide in the management
Post-ASH 2015 CML - MPN
 Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Post-ASH 2015 CML - MPN Fleur Samantha Benghiat, MD, PhD Hôpital Erasme, Brussels 09.01.2016 1. CML CML 1st line ttt Prognosis Imatinib Nilotinib Response Discontinuation Dasatinib Low RISK PROFILE High
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy
 Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
MDS/MPN MPN MDS. Discolosures. Advances in the Diagnosis of Myeloproliferative Neoplasms. Myeloproliferative neoplasms
 Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
How I Treat Myelofibrosis. Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom
 How I Treat Myelofibrosis Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom Primary Myelofibrosis Archiv Fur Pathol. 1879;78:475-96. 2 cases of leukemia with peculiar blood and marrow findings
How I Treat Myelofibrosis Adam Mead, MD, PhD University of Oxford Oxford, United Kingdom Primary Myelofibrosis Archiv Fur Pathol. 1879;78:475-96. 2 cases of leukemia with peculiar blood and marrow findings
ASBMT MDS/MPN Update Sunil Abhyankar, MD
 ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
London Cancer. Myelofibrosis guidelines. August Review August Version v1.0. Page 1 of 12
 London Cancer Myelofibrosis guidelines August 2013 Review August 2013 Version v1.0 Page 1 of 12 CONTENTS 1. DIAGNOSIS... 3 1a. BCSH (2012)... 3 1b. WHO (2009) diagnostic criteria for PMF:... 4 2. MOLECULAR
London Cancer Myelofibrosis guidelines August 2013 Review August 2013 Version v1.0 Page 1 of 12 CONTENTS 1. DIAGNOSIS... 3 1a. BCSH (2012)... 3 1b. WHO (2009) diagnostic criteria for PMF:... 4 2. MOLECULAR
Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated
 Updated") Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY
Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Polycythemia Vera: From New, Modified Diagnostic Criteria to New Therapeutic Approaches
 Polycythemia Vera: From New, Modified Diagnostic Criteria to New Therapeutic Approaches Margherita Maffioli, MD, Barbara Mora, MD, and Francesco Passamonti, MD Drs Maffioli and Mora are hematologists in
Polycythemia Vera: From New, Modified Diagnostic Criteria to New Therapeutic Approaches Margherita Maffioli, MD, Barbara Mora, MD, and Francesco Passamonti, MD Drs Maffioli and Mora are hematologists in
Disclosures for Angela Fleischman
 Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management
 AJH CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management Author: Ayalew Tefferi If you wish to receive credit for this activity,
AJH CME Information: Polycythemia vera and essential thrombocythemia: 2015 update on diagnosis, risk-stratification, and management Author: Ayalew Tefferi If you wish to receive credit for this activity,
Should Mutational Status in Primary Myelofibrosis (PMF) Guide Therapy..YES!!!
 Guide Therapy..YES!!!") Should Mutational Status in Primary Myelofibrosis (PMF) Guide Therapy..YES!!! Lindsay Anne Magura Rein, MD Division of Hematologic Malignancies and Cellular Therapy/BMT A Little Bit of History.. 1665 Advanced
Should Mutational Status in Primary Myelofibrosis (PMF) Guide Therapy..YES!!! Lindsay Anne Magura Rein, MD Division of Hematologic Malignancies and Cellular Therapy/BMT A Little Bit of History.. 1665 Advanced
[COMPREHENSIVE GENETIC ASSAY PANEL ON
 2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis. Francesco Passamonti Università degli Studi dell Insubria, Varese
 Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis Francesco Passamonti Università degli Studi dell Insubria, Varese DIPSS during f-up IPSS at diagnosis Diagnose MF and genotype
Classical Ph-1neg myeloproliferative neoplasms: Ruxolitinib in myelofibrosis Francesco Passamonti Università degli Studi dell Insubria, Varese DIPSS during f-up IPSS at diagnosis Diagnose MF and genotype
Clinical Perspective The Hematologist s View
 SPLANCHNIC VEIN THROMBOSIS. TYPICAL OR ATYPICAL MPN? Giovanni Barosi Unit of Clinical Epidemiology/Center ofr the Study of Myelofibrosis. IRCCS Policlinico S. Matteo Foundation, Pavia Lisbon, 4-5 May 2012
SPLANCHNIC VEIN THROMBOSIS. TYPICAL OR ATYPICAL MPN? Giovanni Barosi Unit of Clinical Epidemiology/Center ofr the Study of Myelofibrosis. IRCCS Policlinico S. Matteo Foundation, Pavia Lisbon, 4-5 May 2012
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Focus on aggressive polycythemia vera
 Focus on aggressive polycythemia vera Jerry L. Spivak, MD Professor of Medicine and Oncology Director, the Johns Hopkins Center for the Chronic Myeloproliferative Disorders Johns Hopkins University School
Focus on aggressive polycythemia vera Jerry L. Spivak, MD Professor of Medicine and Oncology Director, the Johns Hopkins Center for the Chronic Myeloproliferative Disorders Johns Hopkins University School
JAK2 Inhibitors for Myeloproliferative Diseases
 JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
JAK2 Inhibitors for Myeloproliferative Diseases Srdan (Serge) Verstovsek M.D., Ph.D. Associate Professor Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Myeloproliferative
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
How to monitor MPN patients
 How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
How to monitor MPN patients MPN carries significant burden and risk Transformation to MF or AML 1 Neurological complications 2 MPN-associated general symptoms (eg, pruritus, fatigue) 3 Microvascular symptoms
Polycythemia Vera and Essential Thombocythemia A Single Institution Experience
 INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 29 No 4, 2008 7 Original Article-I Polycythemia Vera and Essential Thombocythemia A Single Institution Experience CECIL ROSS, NAVYA, VANAMALA AND KARUNA
INDIAN JOURNAL OF MEDICAL & PAEDIATRIC ONCOLOGY Vol. 29 No 4, 2008 7 Original Article-I Polycythemia Vera and Essential Thombocythemia A Single Institution Experience CECIL ROSS, NAVYA, VANAMALA AND KARUNA
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
SUPPLEMENTARY INFORMATION
 Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology
 Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology Angela Fleischman MD PhD UC Irvine March 9, 2019 Disclosures: Angela Fleischman
Practical Considerations in the Treatment Myeloproliferative Neoplasms: Prognostication and Current Treatment Indy Hematology Angela Fleischman MD PhD UC Irvine March 9, 2019 Disclosures: Angela Fleischman
Survival and Disease Progression in Essential Thrombocythemia Are Significantly Influenced by Accurate Morphologic Diagnosis: An International Study
 Published Ahead of Print on July 11, 2011 as 10.1200/JCO.2010.34.5298 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.34.5298 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
Published Ahead of Print on July 11, 2011 as 10.1200/JCO.2010.34.5298 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2010.34.5298 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E
SESSION 1 Reactive cytopenia and dysplasia
 SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
Current Prognostication in Primary Myelofibrosis
 Current Prognostication in Primary Myelofibrosis Francisco Cervantes Hematology Department, Hospital Clínic, Barcelona, Spain Florence, April 2011 Survival in PMF No. patients: 1,054 Median Srv (95% CI):
Current Prognostication in Primary Myelofibrosis Francisco Cervantes Hematology Department, Hospital Clínic, Barcelona, Spain Florence, April 2011 Survival in PMF No. patients: 1,054 Median Srv (95% CI):
Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera
 Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera Alessandro M. Vannucchi, MD Laboratorio Congiunto MMPC Department of Experimental and Clinical Medicine University
Clinical trials with JAK inhibitors for essential thrombocythemia and polycythemia vera Alessandro M. Vannucchi, MD Laboratorio Congiunto MMPC Department of Experimental and Clinical Medicine University
Greater Manchester and Cheshire Cancer Network
 Greater Manchester and Cheshire Cancer Network Guidelines for the diagnosis and treatment of primary myelofibrosis, post-essential thrombocythaemia myelofibrosis and post-polycythaemia myelofibrosis Tim
Greater Manchester and Cheshire Cancer Network Guidelines for the diagnosis and treatment of primary myelofibrosis, post-essential thrombocythaemia myelofibrosis and post-polycythaemia myelofibrosis Tim
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update
 Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
Mayo Clinic Treatment Strategy in Essential Thrombocythemia, Polycythemia Vera and Myelofibrosis 2013 Update Ayalew Tefferi Mayo Clinic, Rochester, MN 0 20 40 60 80 100 Percent Survival in 337 Mayo Clinic
Stifel Nicolaus 2013 Healthcare Conference. John Scarlett, M.D. Chief Executive Officer September 11, 2013
 Stifel Nicolaus 2013 Healthcare Conference John Scarlett, M.D. Chief Executive Officer September 11, 2013 1 forward-looking statements Except for the historical information contained herein, this presentation
Stifel Nicolaus 2013 Healthcare Conference John Scarlett, M.D. Chief Executive Officer September 11, 2013 1 forward-looking statements Except for the historical information contained herein, this presentation
Reproducibility of Histologic Classification in Nonfibrotic Myeloproliferative Neoplasia
 Hematopathology / Morphologic Features in MPN Reproducibility of Histologic Classification in Nonfibrotic Myeloproliferative Neoplasia Suzanne M. Koopmans, MD, 1 Freek J. Bot, MD, PhD, 1,2 King H. Lam,
Hematopathology / Morphologic Features in MPN Reproducibility of Histologic Classification in Nonfibrotic Myeloproliferative Neoplasia Suzanne M. Koopmans, MD, 1 Freek J. Bot, MD, PhD, 1,2 King H. Lam,
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Mielofibrosi: inquadramento dei fattori prognostici
 Mielofibrosi: inquadramento dei fattori prognostici Francesco Passamon, Division of Hematology University Hospital, Fondazione Macchi Varese, Italy Reduced survival in PMF and causes of death Median OS
Mielofibrosi: inquadramento dei fattori prognostici Francesco Passamon, Division of Hematology University Hospital, Fondazione Macchi Varese, Italy Reduced survival in PMF and causes of death Median OS
Abstract. Hematopathology / Early Prepolycythemic Phase of PV
 Hematopathology / Early Prepolycythemic Phase of PV The Significance of Bone Marrow Biopsy and JAK2 V617F Mutation in the Differential Diagnosis Between the Early Prepolycythemic Phase of Polycythemia
Hematopathology / Early Prepolycythemic Phase of PV The Significance of Bone Marrow Biopsy and JAK2 V617F Mutation in the Differential Diagnosis Between the Early Prepolycythemic Phase of Polycythemia
Technical Bulletin No. 100
 CPAL Central Pennsylvania Alliance Laboratory Technical Bulletin No. 100 August 2, 2012 JAK2 AND MPL 515 MUTATIONAL ANALYSIS Contact: Dr. Jeffrey Wisotzkey, 717-851-1422 Technical Director, CPAL Jill A.
CPAL Central Pennsylvania Alliance Laboratory Technical Bulletin No. 100 August 2, 2012 JAK2 AND MPL 515 MUTATIONAL ANALYSIS Contact: Dr. Jeffrey Wisotzkey, 717-851-1422 Technical Director, CPAL Jill A.
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
CASE 106. Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation
 CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
CME Information: Primary myelofibrosis: 2017 update on diagnosis, risk-stratification and management
 CME ARTICLE AJH CME Information: Primary myelofibrosis: 2017 update on diagnosis, risk-stratification and management CME Editor: Ayalew Tefferi, M.D. Author: Ayalew Tefferi, M.D. If you wish to receive
CME ARTICLE AJH CME Information: Primary myelofibrosis: 2017 update on diagnosis, risk-stratification and management CME Editor: Ayalew Tefferi, M.D. Author: Ayalew Tefferi, M.D. If you wish to receive
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
JAK inhibitors in Phmyeloproliferative
 Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
9/25/2017. Disclosure. I have nothing to disclose. Young S. Kim MD Dept. of Pathology
 Disclosure MAST CELLNEOPLASM I have nothing to disclose. Young S. Kim MD Dept. of Pathology 1 Objectives What is mast cell lineage? Changes in updated WHO 2016 mastocytosis Issues of Mastocytosis CD30
Disclosure MAST CELLNEOPLASM I have nothing to disclose. Young S. Kim MD Dept. of Pathology 1 Objectives What is mast cell lineage? Changes in updated WHO 2016 mastocytosis Issues of Mastocytosis CD30
The Evolving Role of Transplantation for MPN
 The Evolving Role of Transplantation for MPN (PMF, PV, ET) H.Joachim Deeg MD Fred Hutchinson Cancer Research Center, University of Washington, Seattle WA, SCCA jdeeg@fhcrc.org 10 th J. Niblack Conference
The Evolving Role of Transplantation for MPN (PMF, PV, ET) H.Joachim Deeg MD Fred Hutchinson Cancer Research Center, University of Washington, Seattle WA, SCCA jdeeg@fhcrc.org 10 th J. Niblack Conference
Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]
![Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]](/thumbs/87/95709298.jpg "Highest rates of thrombosis = age > 70, history of thrombosis, active disease (> 6 phlebotomies/yr) [2]") Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
Polycythemia Vera Treatment Policy Prepared by Dr. Jeannie Callum Updated May 2003 Introduction PV is a chronic, clonal, myeloproliferative disorder, classically associated with an increase in red cell
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Disclosure: Objectives/Outline. Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations. Nothing to disclose.
 RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
Volume 28, Issue 4 Fall 2018 eissn:
 Volume 28, Issue 4 Fall 2018 eissn: 2368-8076 Myeloproliferative neoplasms (MPNs) Part 1: An overview of the diagnosis and treatment of the classical MPNs by Sabrina Fowlkes, Cindy Murray, Adrienne Fulford,
Volume 28, Issue 4 Fall 2018 eissn: 2368-8076 Myeloproliferative neoplasms (MPNs) Part 1: An overview of the diagnosis and treatment of the classical MPNs by Sabrina Fowlkes, Cindy Murray, Adrienne Fulford,
CASE REPORT. Abstract. Introduction
 CASE REPORT The Amelioration of Myelofibrosis with Thrombocytopenia by a JAK1/2 Inhibitor, Ruxolitinib, in a Post-polycythemia Vera Myelofibrosis Patient with a JAK2 Exon 12 Mutation Kazuhiko Ikeda 1,2,
CASE REPORT The Amelioration of Myelofibrosis with Thrombocytopenia by a JAK1/2 Inhibitor, Ruxolitinib, in a Post-polycythemia Vera Myelofibrosis Patient with a JAK2 Exon 12 Mutation Kazuhiko Ikeda 1,2,
Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases
 Article Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases Keming Lin 1,*, Gang Xu 1, Jie-Gen Jiang 1, Mayuko Imai 1, Zhao Wu 1, Paris Petersen 1, Kim Janatpour 1, and Bashar
Article Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases Keming Lin 1,*, Gang Xu 1, Jie-Gen Jiang 1, Mayuko Imai 1, Zhao Wu 1, Paris Petersen 1, Kim Janatpour 1, and Bashar
Treatment of polycythemia vera with recombinant interferon alpha (rifnα)
") Treatment of polycythemia vera with recombinant interferon alpha (rifnα) Richard T. Silver, MD Professor of Medicine Weill Cornell Medical College New York, New York Outline of Lecture What are interferons?
Treatment of polycythemia vera with recombinant interferon alpha (rifnα) Richard T. Silver, MD Professor of Medicine Weill Cornell Medical College New York, New York Outline of Lecture What are interferons?
New Perspectives on Polycythemia Vera: Overcoming Challenges in Diagnosis, Risk Assessment, and Disease Management
 New Perspectives on Polycythemia Vera: Overcoming Challenges in Diagnosis, Risk Assessment, and Disease Management Jorge E. Cortes, MD The University of Texas MD Anderson Cancer Center Houston, Texas Francesco
New Perspectives on Polycythemia Vera: Overcoming Challenges in Diagnosis, Risk Assessment, and Disease Management Jorge E. Cortes, MD The University of Texas MD Anderson Cancer Center Houston, Texas Francesco
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Approaching myeloid neoplasms: diagnostic algorithms
 Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Mutaciones y sus implicancias clínicas en neoplasias mieloproliferativas
 Mutaciones y sus implicancias clínicas en neoplasias mieloproliferativas Genetics and prognosis in myeloproliferative neoplasms Guglielmelli P, Rotunno G, Pacilli A, Vannucchi AM NEOPLASIAS MIELOPROLIFERATIVAS
Mutaciones y sus implicancias clínicas en neoplasias mieloproliferativas Genetics and prognosis in myeloproliferative neoplasms Guglielmelli P, Rotunno G, Pacilli A, Vannucchi AM NEOPLASIAS MIELOPROLIFERATIVAS
Winship Cancer Institute of Emory University New Determinants and Approaches for MPN
 Winship Cancer Institute of Emory University New Determinants and Approaches for MPN Elliott F. Winton August 8, 2014 Sea Island, Georgia Outline: MPN Determinants, Approaches Diagnosis Prognosis Treatment
Winship Cancer Institute of Emory University New Determinants and Approaches for MPN Elliott F. Winton August 8, 2014 Sea Island, Georgia Outline: MPN Determinants, Approaches Diagnosis Prognosis Treatment
CLINICAL POLICY DEPARTMENT: Medical Management DOCUMENT NAME: JakafiTM REFERENCE NUMBER: NH.PHAR.98
 PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
THE ITALIAN EXPERIENCE
 MYELOFIBROSIS THE ITALIAN EXPERIENCE Giovanni Barosi IRCCS Policlinico S. Matteo. Pavia. Italy Angers, 1-3 October 2004 Myelofibrosis in the eighties A poorly characterized biological syndrome Heterogeneity
MYELOFIBROSIS THE ITALIAN EXPERIENCE Giovanni Barosi IRCCS Policlinico S. Matteo. Pavia. Italy Angers, 1-3 October 2004 Myelofibrosis in the eighties A poorly characterized biological syndrome Heterogeneity
Polycythemia vera: Emerging diagnostic and risk stratification criteria
 This article, sponsed by Incyte Cpation, is based on a paid interview with Rami S. Komrokji, MD, of Moffitt Cancer Center, Tampa, Flida, conducted on May 4, 2015. Polycythemia vera: Emerging diagnostic
This article, sponsed by Incyte Cpation, is based on a paid interview with Rami S. Komrokji, MD, of Moffitt Cancer Center, Tampa, Flida, conducted on May 4, 2015. Polycythemia vera: Emerging diagnostic
Bone Marrow Biopsy in Myelodysplastic Syndromes & Myeloproliferative Neoplasms. A Review for Anatomic Pathologists.
 Bone Marrow Biopsy in Myelodysplastic Syndromes & Myeloproliferative Neoplasms A Review for Anatomic Pathologists Bakul I. Dalal MD FRCPC DABP FACP FASCP Clinical Professor, Department of Pathology, UBC
Bone Marrow Biopsy in Myelodysplastic Syndromes & Myeloproliferative Neoplasms A Review for Anatomic Pathologists Bakul I. Dalal MD FRCPC DABP FACP FASCP Clinical Professor, Department of Pathology, UBC
Biology Diagnosis and Classification of MPD
 Biology Diagnosis and Classification of MPD Jan Jacques Michiels 1,7, Hendrik De Raeve 2, Konnie Hebeda 3, King H. Lam 4, Freek Bot 5, Zwi Berneman 1, Wilfried Schroyens 1 Departments of Hematology 1 and
Biology Diagnosis and Classification of MPD Jan Jacques Michiels 1,7, Hendrik De Raeve 2, Konnie Hebeda 3, King H. Lam 4, Freek Bot 5, Zwi Berneman 1, Wilfried Schroyens 1 Departments of Hematology 1 and
Mutational Analysis of EXON 9 of the CALR Gene (Reference )
") Mutational Analysis of EXON 9 of the CALR Gene (Reference 2014.01.002) Notice of Assessment June 2014 DISCLAIMER: This document was originally drafted in French by the Institut national d'excellence en
Mutational Analysis of EXON 9 of the CALR Gene (Reference 2014.01.002) Notice of Assessment June 2014 DISCLAIMER: This document was originally drafted in French by the Institut national d'excellence en