Targeted Radioimmunotherapy for Lymphoma
|
|
|
- Andrew Hudson
- 6 years ago
- Views:
Transcription


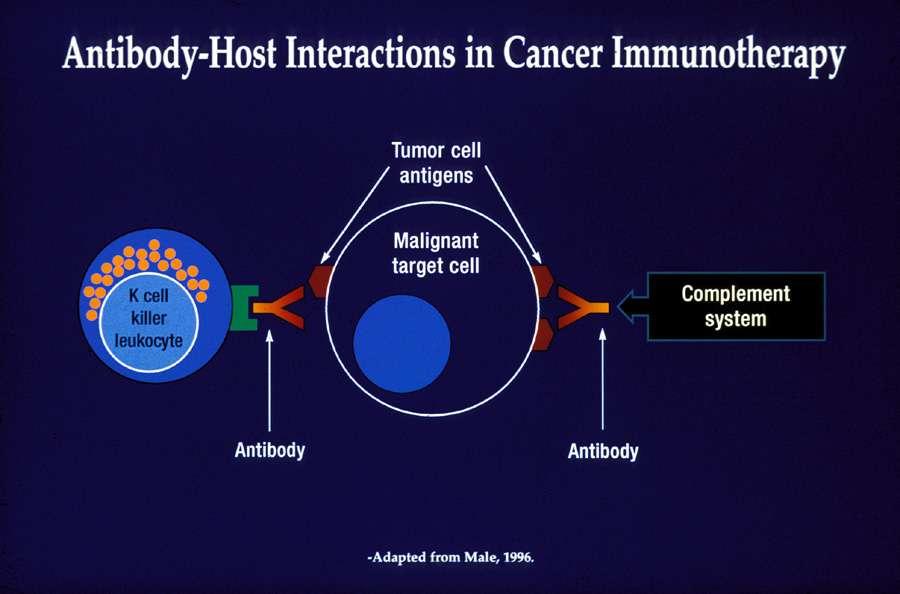
1 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by:
2 Financial Disclosures Disclosures Erik Mittra, MD, PhD(speaker) John Pagel, MD, PhD(speaker) Nothing to Disclose Nothing to Disclose Hossein Jadvar, MD (Co-Organizer): Andrei Iagaru, MD (Co-Organizer): Saima Hedrick, MPH (Moderator): FDA Disclosure Nothing to Disclose CytomX Consultant/Advisor Spectrum Pharmaceutical Consultant/Advisor Nothing to Disclose This presentation will not include discussion of any device or drug requiring FDA approval.
3 Non-Hodgkin Lymphoma Indolent No urgency to treat if asymptomatic Multiple chemotherapy regimens with responses/relapses Aggressive Curable with chemotherapy Relapses cured with high dose therapy and stem cell transplantation
4 Indolent NHL: Management Diagnosis Good or Intermediate Risk (IPI L or LI) Workup (Staging) High Risk (IPI HI or H) Treatment Indicated? Yes Initial Treatment No Observe Progression Indications for treatment include: -Threatened end-organ function -Massive bulk at presentation -Steady progression -Symptoms -Patient preference -Eligible for trial -Cytopenia(s) -Recurrent infections

5 Quality of Remission (CR Rate) Options for the Management of FL CONSOLIDATION MAINTENANCE Types of therapy: Radiolabeled immunotherapy Types of therapy: Immunotherapy INDUCTION Types of therapy: Combination chemo- or immunochemotherapy Goals of therapy over a patient s course of treatment Reduce tumor Maximize response by rapidly load and induce improving quality of response to initial response induction (increased CR rates, bcl-2 conversion) Prevent relapse by maintaining best response Remission Duration
6 Is CR Important in Indolent Disease? Bachy et al, JCO 2010 (pre-rituximab era, ) Treated patients who achieved a CR had a significantly longer OS than those only reaching a PR Bachy et al. JCO 2010;28:822-9.
7 Influence of CR Achievement during First Line Therapy Bachy et al. JCO 2010;28:822-9.
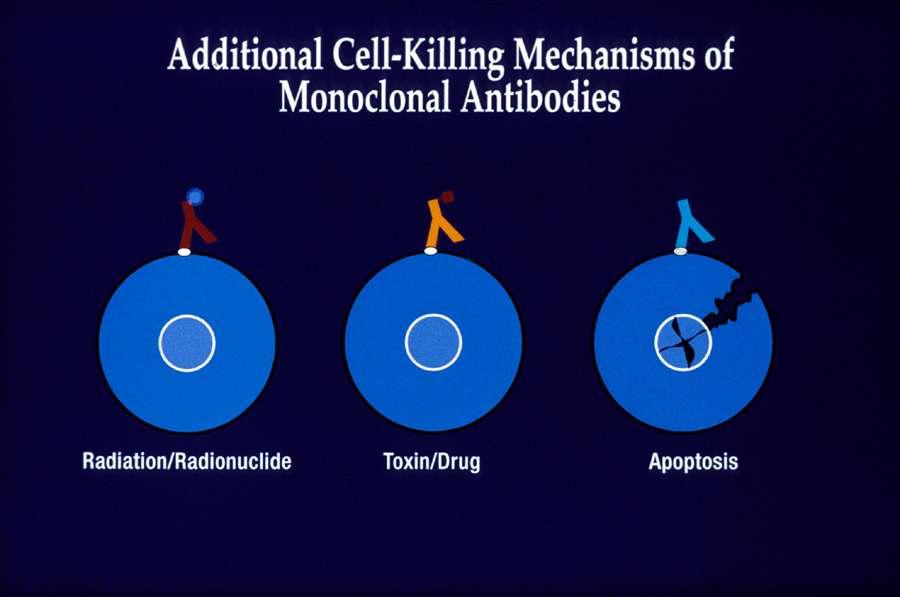
8 Strategies for Antibody Use Combination with chemotherapy e.g. CHOP plus Rituximab Prolonged therapy Combinations of multiple Abs Combinations with boosters to the immune system Combined with toxins and/or radioisotopes Detect minimal residual disease Transplantation
9
10 Limitations of Naked Antibodies All tumor cells need to be targeted by Ab Patient s immune mechanisms may not be functional Resistant tumor cells To direct anti-tumor mechanisms To immune mechanisms-mediated by the antibody Antigen-negative tumor cells may escape
11


12 Radioimmunotherapy

13 Principles of Radioimmunotherapy Targeted delivery of radiation to tumor cells Greater exposure of radiation to tumors vs surrounding normal organs Continuous exposure of tumor cells Retention of anti-tumor mechanisms of the antibody
14 Anti-CD20 Radioimmunoconjugates for NHL Zevalin Bexxar Parent antibody Ibritumomab Tositumomab Radionuclide Yttrium- Iodine-131 Properties Emission Pure b g and b Radiation penetration 5-10 mm 1 mm Half-life 2.7 days 8.1 days Dosimetry required No (optional) Yes
15 RIT: Where Does It Fit in a Treatment Plan? Chem 1 MAB 1 RIT MAB 2? Auto SCT Chem 2 Allo SCT Treatment plans differ with Patient s clinical status Patient s medical history Histologic type Presence of bulky disease
16 NCCN Treatment Guidelines
17 Randomized Phase III Study in Relapsed or Refractory Low Grade or Follicular NHL STUDY ELIGIBILITY N=130 Relapsed or refractory lowgrade or follicular B-cell NHL No prior rituximab therapy Histologically confirmed NHL requiring therapy WHO PS 2 Less than 25% bone marrow involvement by NHL No prior BMT Acceptable hematologic function R A N D O M I Z A T I O N ZEVALIN (n=64) Day 1: Rituximab 250mg/m 2 In-111 ZEVALIN 5mCi Day 8: Rituximab 250mg/m 2 Y- ZEVALIN 0.4 mci/kg Rituximab (n=66) Weeks 1-4: Rituximab 375 mg/m 2 ZEVALIN (ibritumomab tiuxetan) Package Insert, Witzig, TE et al. J Clin Oncol. May 2002;20:
18 Significantly Higher ORR and CR/CRu Rate in Zevalin Arm ZEVALIN (n=64) Rituximab (n=66) p-value* Overall RR 83% 55% <0.001 CR/CRu rate 38% 18% N/A Witzig, TE et al. J Clin Oncol. May 2002;20: ZEVALIN (ibritumomab tiuxetan) Package Insert, 2009.
19 Patients with Response (%) Earlier Treatment with Zevalin Produces Higher CR/CRu Rates # Prior Chemotherapy Regimens 1 (n = 63) 2 (n = 148) p = All patients 28 p = Patients with CR/CRu Emmanouilides et al. Leuk Lymph. April 2006;47(4):
20 Percent with Response Response Rate by Treatment Encounter BEXXAR and Chemotherapy Bexxar Chemotherapy nd 3rd 4th 5th 6th 7 or more Treatment Encounter Number
21 FIT Trial: Study Schema Enrollment in Study FIRST-LINE CHEMOTHERAPY CHOP/CHOP-like CVP/COP Rituximab combinations Chlorambucil Fludarabine/fludarabine combinations NR PD Not Included CR/CRu or PR R A N D O M I Z A T I O N ZEVALIN (n=208) Day 1, 7 rituximab 250 mg/m 2 IV Day 7 Y- ZEVALIN 0.4mCi/kg IV CONTROL (n=206) No Further Treatment Median 7 months interval from start of initial treatment until entry into the study PFS was calculated from time of randomization Morschhauser et al. J Clin Oncol. 2008;
22 Baseline Characteristics Characteristics Control (n = 202) Y-Ibritumomab (n = 207) Male, n (%) 101 (50) 99 (48) Age at randomization Median, y (range) 53 (27-74) 55 (29-78) Aged > 60 y, n (%) 48 (24) 58 (28) Ann Arbor classification, n (%) Stage III 62 (31) 73 (35) Stage IV 134 (66) 132 (64) Response to first-line treatment, n (%) CR/CRu 108 (53) 107 (52) PR 88 (44) 100 (48) Patient baseline characteristics and distribution of first-line induction treatments were well balanced between treatment arms
23 FIT: Baseline FLIPI Score FLIPI scores, n (%) Control) n = 146* (%) Y-Ib n = 150* (%) Low risk (0-1 factors) 62 (42.5) 56 (37.3) Intermediate risk (2 factors) 54 (37.0) 58 (38.7) High risk (3-5 factors) 30 (20.5) 36 (24.0) * FLIPI data could be collected retrospectively in 71% of intent-to-treat population. Morschhauser et al. J Clin Oncol. 2008;
24 Overall CR Rates After Randomization CR/CRu Control, % Y-Ibritumomab, % n = 202 n = 207 After induction therapy After randomization Morschhauser et al. J Clin Oncol. 2008;26:
25 Conversion to bcl-2 PCR- Negative Status in the Blood Number of patients converting from bcl-2 PCR-positive to PCR-negative status after randomization Control, n/n* (%) Y-ibritumomab, n/n* (%) Blood 21/59 (36) 61/68 () *Patients with PCR-positive status at randomization who had at least 1 post-randomization PCR assessment; all other patients were either PCR negative at randomization or lacked a second assessment. % of patients converted from bcl-2 PCR-positive to PCR-negative status after Y-ibritumomab consolidation
26 Y-Ibritumomab Tiuxetan Consolidation After (R)-Chemo in Follicular NHL Regimen FIT Y-ibritumomab arm: Chemo induction + Y-ibritumomab consolidation Patient Population Stage III-IV FL 64% stage IV 24% high FLIPI CR/CRu Rate After Y-ibritumomab Consolidation Reference 87% Morschhauser et al 1 R (4 weeks) + R-CHOP (3 cycles) + Y-ibritumomab consolidation Stage II-IV FL 66% stage IV 72% Hainsworth et al 2 R-CHOP (3 cycles) + Y-ibritumomab consolidation + R maintenance FL % stage III-IV 42% high FLIPI 89%* Jacobs et al 3 *Assessed by PET imaging 1. J Clin Oncol. 2008;26: Clin Lymphoma Myeloma. 2009;9: Clin Cancer Res. 2008;14:

27 Cumulative Percentage OVERALL PFS FOR TREATMENT GROUPS The 7-year overall PFS was 23% in the control arm compared with 47% in the Y-ibritumomab arm HR = 2.09 (95% CI: ); P < Y-ibritumomab: n = 207 Median PFS: 49.3 mo At risk: Y-ibritumomab Control 25 Y-ibritumomab Control N F PFS From Time of Randomization (months) Control: n = 202 Median PFS: 12.6 mo 25 14
28 Cumulative Percentage PFS for Patients in PR After Induction The 5-year PFS among patients with a PR after induction was 14% in the control arm compared with 38% in the Y-ibritumomab arm HR = 2.62 (95% CI: ); P < Y-ibritumomab: n = 100 Median PFS: 30 mo 25 0 At risk: Y-ibritumomab Control Y-ibritumomab Control N F PFS From Time of Randomization (months) Control: n = 94 Median PFS: 6 mo 34 11
; P < 0.")
29 Cumulative Percentage Time to Next Treatment (TTNT) Patients in the Y-ibritumomab arm had a greater than 5-year advantage in TTNT compared with patients in the control arm HR = 2.03 (95% CI: ); P < Y-ibritumomab: n = 207 Median TTNT: > 99 mo Control: n = 202 Median TTNT: 35 mo At risk: Y-ibritumomab Control Y-ibritumomab Control N F TTNT From Time of Randomization (months)
 Package Insert, 2009.")
30 Hematologic Toxicities: Timeline * Based on median time to nadir and recovery for ZEVALIN-treated patients ZEVALIN (ibritumomab tiuxetan) Package Insert, SAG Clinical Study Report.
31 Patients (%) Grade 3/4 Non-Hematologic Toxicity Control Y-Ib (N = 205) (N = 204) Any Grade G3 G3 Infections Hypertension G3 Pyrexia *Grade 3 or 4 AEs reported in 5 patients in either treatment arm Any Grade G4 Infections G4 Pyrexia Morschhauser et al. J Clin Oncol. 2008;
32 Secondary Malignancies That Have Emerged During Extended Follow-up Secondary Malignancy Control, n (%) Y-Ibritumomab, n (%) n = 202 n = 207 Basocellular carcinoma of the skin 1 (0.5) 2 (1) Basocellular epithelioma 1 (0.5) 1 (0.5) Breast cancer 1 (0.5) 2 (1) Endometrial carcinoma 1 (0.5) 0 Lung cancer 0 1 (0.5) MDS/AML 1 (0.5) 6 (2.9) Melanoma 1 (0.5) 0 Pancreatic cancer 0 2 (1) Papillary thyroid carcinoma 1 (0.5) 0 Pulmonary adenocarcinoma 1 (0.5) 0 Squamous cell carcinoma of the lung 1 (0.5) 0 Squamous cell carcinoma of the skin 0 1 (0.5) Vesical transitional cell carcinoma TgGA (0.5) Total 9 (4.5) 16 (7.7)
33 MDS/AML: Annualized Rates in Y-Ibritumomab Studies Compared With FL Patients Generally (SEER Data) FIT Study, 1 Y-ibritumomab group Witzig Studies 2 SEER data 3 (R)-Chemo) Annualized rate 0.55% 1.0% 1.03% 95% CI 0.25% % 0.4% - 1.7% 0.96% % The annualized rate of secondary MDS/AML in patients treated with Y-ibritumomab does not appear higher than the annualized rate of MDS/AML observed in patients treated for FL generally. 1. Morschhauser et al. J Clin Oncol. 2008;26: Czuczman et al. J Clin Oncol. 2007;25: Morton et al. J Clin Oncol. 2010;28:
34 Overall Survival All patients 40 deaths Control 22 deaths Y-ibritumomab 18 deaths At current follow-up, there is no significant difference in OS between treatment arms (P = 0.465) 5-year OS was 93% in the Y-ibritumomab arm compared with 89% in the control arm
35 Cumulative Percentage Overall Survival for Treatment Groups The 5-year OS was 89% in the control arm compared with 93% in the Y-ibritumomab arm HR = 1.26 (95% CI: ); P = Y-ibritumomab: n = 207 Median OS: > 98 mo Control: n = 202 Median OS: > 101 mo 25 0 At risk: Y-ibritumomab Control Y-ibritumomab Control N F OS From Time of Randomization (months)
36 Subsequent Management After PD Treatment After PD Control, n (%) Y-Ibritumomab, n (%) n = 141* n = 104* Rituximab 102 (72) 63 (61) Y-ibritumomab tiuxetan 12 (9) 1 (1) Autologous transplantation 31 (22) 13 (13) Allogeneic transplantation 3 (2) 1 (1) Fludarabine, FC (M), FM 15 (11) 9 (9) ICE 2 (1) 3 (3) DHA (P) / DHA (Oxa) / ESHA (P) 13 (9) 10 (10) Bendamustine 0 (0) 2 (2) Other 12 (9) 16 (15) No treatment given 19 (13) 22 (21) *Patients may have received 1 treatment.
37 Patients in Control and Y-Ibritumomab Arms Achieved Comparable Responses to Second-Line Therapy Response to Second-Line Therapy After Progressive Disease, % Control (n = 122*) Y-Ibritumomab (n = 82*) ORR 78% 79% CR/CRu 59% 57% PR 19% 22% SD 5% 1% *Number of patients who received treatment after progressive disease. ORR = overall response rate; CR = complete response; CRu = unconfirmed CR; PR = partial response; SD = stable disease.
38 Conclusions to FIT Study Y-Ibritumomab consolidation resulted in high conversion rates from PR to CR/CRu and high overall CR rate Y-Ibritumomab consolidation significantly prolonged median PFS compared with no further treatment in patients responsive to first-line induction treatment Y-Ibritumomab consolidation was well tolerated with manageable hematologic adverse events Annualized rate of 2 0 MDS/AML was 0.55 Y-Ibritumomab consolidation confers a durable PFS benefit Nearly 3-year PFS advantage for patients in the ITT population At least a 5-year PFS advantage with a CR/CRu after induction 2-year PFS advantage for patients with a PR after induction > 5-year advantage in time to next treatment At current follow-up, there is no significant difference in OS between treatment arms (P = 0.465)
39 Responses to CHOP Bexxar (N=84*) 100% 2% SD 2% 80% 60% 54% PR 24% * 40% 20% 44% CR 74% 0% * evaluable pt. After CHOP After Bexxar Press, et al., ASH 2005 (abstract)
40 Hematologic Toxicities (Grade 3-4) 60% 50% 40% 30% 46% CHOP (N=89) Bexxar (N=81) SWOG 9911 Treatment-Related Deaths: 0 20% 10% 0% 13% 1% 11% 13% 7% 6% 3% 2% 2% 2% 2% 3% ANC Platelets Anemia Infxn Febrile RBC Press, Blood 102:1606, 2003 neutropenia Transf. Platelet Transf.
41 Progression-Free and Overall Survival SWOG % 80% 60% 40% 20% Median FU = 5.1 yr Overall Survival Progression-Free Survival OS 5-Year Estimate 87% 67% PFS 0% Years from Registration Press, et al., ASH 2005 (abstract)
42 PCR Analysis: S informative patients: PCR + for t(14;18) at study entry and serial BM PCR available 32 (84%) PCR neg. after therapy PCR + after Rx 6 pt (16%) PCR neg. after CHOP 7 pt (18%) PCR neg. but timing unclear 1 pt (3%) PCR neg. after Bexxar 24 pt (63%)* *1 pt subsequently reconverted to PCR + Press, et al., ASH 2005 (abstract)
43 Progression-Free Survival SWOG-9911 vs. Historical CHOP Studies 100% 80% CHOP + Bexxar (S9911) 60% 40% 20% 0% CHOP + Bexxar Historical CHOP 5-Year Estimate 67% 44% Years from Registration CHOP (S7426,S7713) Press, et al., ASH 2005 (abstract)
44 Overall Survival SWOG-9911 vs. Historical CHOP Studies 100% CHOP + Bexxar (S9911) 80% 60% 40% 20% CHOP + I-131 Tx Historical CHOP 5-Year Estimate 87% 64% CHOP (S7426,S7713) 0% Years from Registration Press, et al., ASH 2005 (abstract)
45 CHOP vs R-CHOP vs Tositumomab I-Tositumomab in Untreated FL Untreated FL Grade 1-3 Stage III-IV R A N D O M I Z E R-CHOP 6 CHOP 6 + tositumomab I-tositumomab End points: response rates, toxicity, and molecular response rates of t(14;18)/bcl-2 rearrangements in BM
46 Bexxar: initial FL therapy 95% response rate! 75% complete response! 89% 5 yr overall survival!
47 Bexxar: initial FL therapy N=76 patients Kaminski et al, NEJM, 352:441, 2005

48 Single Agent Zevalin Overall survival

49 Results : Time to next treatment Median n.r.

50 NCCN Treatment Guidelines
51 Questions?
52 Join us for other webinars in the Targeted Radioisotope Therapy Series Visit SNMMI.org/webinars for more information You will receive a link for the post-webinar test in an . You must successfully complete the test to receive the credit.
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
SEQUENCING FOLLICULAR LYMPHOMA
 SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
SEQUENCING FOLLICULAR LYMPHOMA Thomas E. Witzig, MD October 24, 2015 Disclosures All presenters were independently selected by the organizing committee. Those presenters who disclosed affiliations or financial
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Patterns of Care in Medical Oncology. Follicular Lymphoma
 Patterns of Care in Medical Oncology Follicular Lymphoma CASE 1: A 72-year-old man with multiple comorbidities including COPD/asthma presents with slowly progressive cervical adenopathy. Bone marrow biopsy
Patterns of Care in Medical Oncology Follicular Lymphoma CASE 1: A 72-year-old man with multiple comorbidities including COPD/asthma presents with slowly progressive cervical adenopathy. Bone marrow biopsy
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma
 12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
The case against maintenance rituximab in Follicular lymphoma. Jonathan W. Friedberg M.D., M.M.Sc.
 The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
Open questions in the treatment of Follicular Lymphoma. Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland
 Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES
 How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Managing patients with relapsed follicular lymphoma. Case
 Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes
 Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Is there a role of HDT ASCT as consolidation therapy for first relapse follicular lymphoma in the post Rituximab era? Yes Bertrand Coiffier Service d Hématologie Hospices Civils de Lyon Equipe «Pathologie
Digital Washington University School of Medicine. Russell Schilder Fox Chase Comprehensive Cancer Center. Arturo Molina Biogen Idec
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2004 Follow-up results of a phase II study of ibritumomab tiuetan radioimmunotherapy in patients with relapsed or
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2004 Follow-up results of a phase II study of ibritumomab tiuetan radioimmunotherapy in patients with relapsed or
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
Ibritumomab Tiuxetan in Lymphoma: A Clinical Practice Guideline
 Evidence-based Series #6-17: Section 1 Ibritumomab Tiuxetan in Lymphoma: A Clinical Practice Guideline M. Cheung, A.E. Haynes, A. Stevens, R.M. Meyer, K. Imrie, and the members of the Hematology Disease
Evidence-based Series #6-17: Section 1 Ibritumomab Tiuxetan in Lymphoma: A Clinical Practice Guideline M. Cheung, A.E. Haynes, A. Stevens, R.M. Meyer, K. Imrie, and the members of the Hematology Disease
This tutorial gives an overview of Radioimmunotherapy in Non-Hodgkin s Lymphoma. After completing this tutorial, attendees will be able to:
 This tutorial gives an overview of Radioimmunotherapy in Non-Hodgkin s Lymphoma. After completing this tutorial, attendees will be able to: Name the radiopharmaceutical approved by the FDA for performance
This tutorial gives an overview of Radioimmunotherapy in Non-Hodgkin s Lymphoma. After completing this tutorial, attendees will be able to: Name the radiopharmaceutical approved by the FDA for performance
FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting?
 Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
ZEVALIN (ibritumomab tiuxetan) Information for Authorized Users and Administration Facilities
 Information for Authorized Users and Administration Facilities") 0133-049104 ZEVALIN (ibritumomab tiuxetan) Information for Authorized Users and Administration Facilities Please see slides 3-7 for BOXED WARNINGS and Important Safety Information. Please see full Prescribing
0133-049104 ZEVALIN (ibritumomab tiuxetan) Information for Authorized Users and Administration Facilities Please see slides 3-7 for BOXED WARNINGS and Important Safety Information. Please see full Prescribing
The case for maintenance rituximab in FL
 New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
Jonathan W Friedberg, MD, MMSc
 I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
Scottish Medicines Consortium
 Scottish Medicines Consortium ibritumomab tiuxetan (Zevalin ) No. (171/05) Schering Health Care Ltd 8 April 2005 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Scottish Medicines Consortium ibritumomab tiuxetan (Zevalin ) No. (171/05) Schering Health Care Ltd 8 April 2005 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
Il trattamento del Linfoma Follicolare in prima linea
 Il trattamento del Linfoma Follicolare in prima linea Dr.ssa Carola Boccomini SC Ematologia Dr. U. Vitolo AO Città della Salute e della Scienza Torino, Italy Median follow-up 3 years Median follow-up 6
Il trattamento del Linfoma Follicolare in prima linea Dr.ssa Carola Boccomini SC Ematologia Dr. U. Vitolo AO Città della Salute e della Scienza Torino, Italy Median follow-up 3 years Median follow-up 6
THE USE OF IBRITUMOMAB AS CONSOLIDATION THERAPY AFTER REMISSION INDUCTION IN PREVIOUSLY UNTREATED FOLLICULAR LYMPHOMA
 THE USE OF IBRITUMOMAB AS CONSOLIDATION THERAPY AFTER REMISSION INDUCTION IN PREVIOUSLY UNTREATED FOLLICULAR LYMPHOMA Wolfson Unit Claremont Place Newcastle upon Tyne NE2 4HH May 2009 n THE USE OF IBRITUMOMAB
THE USE OF IBRITUMOMAB AS CONSOLIDATION THERAPY AFTER REMISSION INDUCTION IN PREVIOUSLY UNTREATED FOLLICULAR LYMPHOMA Wolfson Unit Claremont Place Newcastle upon Tyne NE2 4HH May 2009 n THE USE OF IBRITUMOMAB
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Address correspondence to: Brad S. Kahl, MD 1111 Highland Avenue, 4059 WIMR Madison, WI
 Yttrium 90-Ibritumomab Tiuxetan Plus Rituximab Maintenance as Initial Therapy for Patients With High-Tumor-Burden Follicular Lymphoma: A Wisconsin Oncology Network Study Saurabh Rajguru, MD, Thorhildur
Yttrium 90-Ibritumomab Tiuxetan Plus Rituximab Maintenance as Initial Therapy for Patients With High-Tumor-Burden Follicular Lymphoma: A Wisconsin Oncology Network Study Saurabh Rajguru, MD, Thorhildur
Bendamustine for relapsed follicular lymphoma refractory to rituximab
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine for relapsed follicular lymphoma refractory to rituximab Bendamustine for relapsed follicular lymphoma refractory to rituximab Contents Summary 1
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Bendamustine for relapsed follicular lymphoma refractory to rituximab Bendamustine for relapsed follicular lymphoma refractory to rituximab Contents Summary 1
try George Sgouros, Ph.D. Russell H. Morgan Dept of Radiology & Radiological Science Baltimore MD
 Bexxar Dosimet try George Sgouros, Ph.D. Russell H. Morgan Dept of Radiology & Radiological Science Johns Hopkins University, School of Medicine Baltimore MD Clinical i l Experi ience with anti- CD-20
Bexxar Dosimet try George Sgouros, Ph.D. Russell H. Morgan Dept of Radiology & Radiological Science Johns Hopkins University, School of Medicine Baltimore MD Clinical i l Experi ience with anti- CD-20
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Antibody-Based Immunotherapeutic Agents for Treatment of Non-Hodgkin Lymphoma
 Antibody-Based Immunotherapeutic Agents for Treatment of Non-Hodgkin Lymphoma Steven I. Park, MD, 1* and Kristy L. Richards, PhD, MD 1 ABSTRACT Antibody-based immunotherapeutic agents have emerged as important
Antibody-Based Immunotherapeutic Agents for Treatment of Non-Hodgkin Lymphoma Steven I. Park, MD, 1* and Kristy L. Richards, PhD, MD 1 ABSTRACT Antibody-based immunotherapeutic agents have emerged as important
Challenges in the Treatment of Follicular Lymphoma
 Challenges in the Treatment of Follicular Lymphoma Prof. Michele Ghielmini Clinical Director Oncology Institute of Southern Switzerland Bellinzona ESMO guidelines 2014 (simplified) Low tumor burden High
Challenges in the Treatment of Follicular Lymphoma Prof. Michele Ghielmini Clinical Director Oncology Institute of Southern Switzerland Bellinzona ESMO guidelines 2014 (simplified) Low tumor burden High
Follicular Lymphoma 2016:
 Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
MMAE disrupts cell division and triggers apoptosis. Pola binds to cell surface antigen CD79b. Pola is internalized; linker cleaves, releasing MMAE
 Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Tiuxetan ( 90 Y-IT) as a consolidation
 as a consolidation") Aim of the study: To evaluate the efficacy and safety of Yttrium-90 Ibritumomab Tiuxetan ( 90 Y-IT) as a consolidation therapy in the management of DLBCL. Material and methods: Patients with primary refractory
Aim of the study: To evaluate the efficacy and safety of Yttrium-90 Ibritumomab Tiuxetan ( 90 Y-IT) as a consolidation therapy in the management of DLBCL. Material and methods: Patients with primary refractory
Disclosures for Dr. Peter Borchmann 48 th ASH Annual meeting, Orlando, Florida
 Phase II Study of Pixantrone in Combination with Cyclophosphamide, Vincristine, and Prednisone (CPOP) in Patients with Relapsed Aggressive Non-Hodgkin s Lymphoma P Borchmann Universitaet de Koeln, Koeln,
Phase II Study of Pixantrone in Combination with Cyclophosphamide, Vincristine, and Prednisone (CPOP) in Patients with Relapsed Aggressive Non-Hodgkin s Lymphoma P Borchmann Universitaet de Koeln, Koeln,
eastern cooperative oncology group Michael Williams, Fangxin Hong, Brad Kahl, Randy Gascoyne, Lynne Wagner, John Krauss, Sandra Horning
 Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 18 July 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2012 MABTHERA 100 mg, concentrate for solution for infusion B/2 (CIP code: 560 600-3) MABTHERA 500 mg, concentrate
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 18 July 2012 MABTHERA 100 mg, concentrate for solution for infusion B/2 (CIP code: 560 600-3) MABTHERA 500 mg, concentrate
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma
 How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
How to incorporate new therapies into the treatment algorithm of patients with mantle cell lymphoma Dr. Guillermo Rodríguez García Hospital Universitario Virgen Macarena Hospital Universitario Virgen del
Mantle Cell Lymphoma: Update in Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency
 Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Mantle Cell Lymphoma: Update in 2015 Diego Villa, MD MPH FRCPC Medical Oncologist BC Cancer Agency Disclosures Research funding: Roche provides research funding to support the Centre for Lymphoid Cancer
Radiotherapy in aggressive lymphomas. Umberto Ricardi
 Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009
 Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
R/R DLBCL Treatment Landscape
 An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège. 14 th post-ash meeting, January 6 th 2011, Brussels
 Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Chapter 5. M.J. Wondergem 1, J.M. Zijlstra 1, M. de Rooij 1, O.J. Visser 1, P.C. Huijgens 1, S. Zweegman 1
 Chapter 5 Improving survival in patients with transformed B-cell non Hodgkin lymphoma: consolidation with 90 Yttrium ibritumomab tiuxetan-beam and autologous stem cell transplantation M.J. Wondergem 1,
Chapter 5 Improving survival in patients with transformed B-cell non Hodgkin lymphoma: consolidation with 90 Yttrium ibritumomab tiuxetan-beam and autologous stem cell transplantation M.J. Wondergem 1,
Obinutuzumab in combination with bendamustine for treating rituximab-refractory follicular lymphoma
 Obinutuzumab in combination with bendamustine for treating rituximab-refractory follicular lymphoma 1 st Appraisal Committee meeting Background and Clinical Effectiveness Committee A Lead team John Watkins
Obinutuzumab in combination with bendamustine for treating rituximab-refractory follicular lymphoma 1 st Appraisal Committee meeting Background and Clinical Effectiveness Committee A Lead team John Watkins
Updates in the Treatment of Non-Hodgkin Lymphoma: ASH Topics
 Updates in the Treatment of Non-Hodgkin Lymphoma: ASH 2008 Joseph Tuscano, M.D. UC Davis Cancer Center 1 Topics Mantle Cell Lymphoma What is the standard of care for younger patients? (abstracts 581, 769,
Updates in the Treatment of Non-Hodgkin Lymphoma: ASH 2008 Joseph Tuscano, M.D. UC Davis Cancer Center 1 Topics Mantle Cell Lymphoma What is the standard of care for younger patients? (abstracts 581, 769,
Angioimmunoblastic T-cell lymphoma: nobody knows what to do...
 Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham
 Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
Curing Myeloma So Close and Yet So Far! Luciano J. Costa, MD, PhD Associate Professor of Medicine University of Alabama at Birmingham What is cure after all? Getting rid of it? Stopping treatment without
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center
 Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Today, how many PTCL patients are cured? Some but not as many
Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Today, how many PTCL patients are cured? Some but not as many
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Mathias J Rummel, MD, PhD
 I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
I N T E R V I E W Mathias J Rummel, MD, PhD Prof Rummel is Head of the Department of Hematology at the Hospital of the Justus-Liebig University in Gießen, Germany. Tracks 1-17 Track 1 Track 2 Track 3 Track
Radioimmunotherapy for lymphoma analysis of clinical trials and treatment algorithms
 Review Nuclear Medicine Review 2007 Vol. 10, No. 2, pp. 110 115 Copyright 2007 Via Medica ISSN 1506 9680 Radioimmunotherapy for lymphoma analysis of clinical trials and treatment algorithms Wojciech Jurczak
Review Nuclear Medicine Review 2007 Vol. 10, No. 2, pp. 110 115 Copyright 2007 Via Medica ISSN 1506 9680 Radioimmunotherapy for lymphoma analysis of clinical trials and treatment algorithms Wojciech Jurczak
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
CME Information. Y-ibritumomab tiuxetan to that of rituximab maintenance for patients with newly diagnosed follicular lymphoma (FL).
.") CME Information LEARNING OBJECTIVES Compare the efficacy of consolidation therapy with a single dose of 90 Y-ibritumomab tiuxetan to that of rituximab maintenance for patients with newly diagnosed follicular
CME Information LEARNING OBJECTIVES Compare the efficacy of consolidation therapy with a single dose of 90 Y-ibritumomab tiuxetan to that of rituximab maintenance for patients with newly diagnosed follicular
Non Transplant-Related Treatment Options in Follicular Lymphoma
 Biology of Blood and Marrow Transplantation 12:53-58 (2006) 2006 American Society for Blood and Marrow Transplantation 1083-8791/06/1201-0111$32.00/0 doi:10.1016/j.bbmt.2005.10.003 Non Transplant-Related
Biology of Blood and Marrow Transplantation 12:53-58 (2006) 2006 American Society for Blood and Marrow Transplantation 1083-8791/06/1201-0111$32.00/0 doi:10.1016/j.bbmt.2005.10.003 Non Transplant-Related
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Radioimmunotherapy of Non. Hodgkin Lymphoma with
 Amar U. Kishan, MS Amar IV U. Kishan, MSIV Gillian Lieberman, Gillian MD Lieberman, MD June 2011 Click to edit Master title style Click to edit Master text styles Radioimmunotherapy of Non Second level
Amar U. Kishan, MS Amar IV U. Kishan, MSIV Gillian Lieberman, Gillian MD Lieberman, MD June 2011 Click to edit Master title style Click to edit Master text styles Radioimmunotherapy of Non Second level
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Immunotherapy in haematological malignancies. Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona
 Immunotherapy in haematological malignancies Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona Conflicts of interest Roche Celgene Mundipharma Janssen Gilead Bayer Millenium What
Immunotherapy in haematological malignancies Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona Conflicts of interest Roche Celgene Mundipharma Janssen Gilead Bayer Millenium What
CLINICAL RESEARCH RESULTS FROM THE ANNUAL MEETINGS OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY AND THE SOCIETY OF NUCLEAR MEDICINE
 FOR IMMEDIATE RELEASE CLINICAL RESEARCH RESULTS FROM THE ANNUAL MEETINGS OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY AND THE SOCIETY OF NUCLEAR MEDICINE Results of Studies of BEXXAR TM Therapy Show Promise
FOR IMMEDIATE RELEASE CLINICAL RESEARCH RESULTS FROM THE ANNUAL MEETINGS OF THE AMERICAN SOCIETY OF CLINICAL ONCOLOGY AND THE SOCIETY OF NUCLEAR MEDICINE Results of Studies of BEXXAR TM Therapy Show Promise
The radiolabeled monoclonal antibodies 90 Y-ibritumomab
 Journal of Nuclear Medicine, published on October 17, 2007 as doi:10.2967/jnumed.107.043489 Comparison of Y-Ibritumomab Tiuxetan and I-Tositumomab in Clinical Practice Heather A. Jacene*, Ross Filice*,
Journal of Nuclear Medicine, published on October 17, 2007 as doi:10.2967/jnumed.107.043489 Comparison of Y-Ibritumomab Tiuxetan and I-Tositumomab in Clinical Practice Heather A. Jacene*, Ross Filice*,
A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Iodine-131 Tositumomab in Lymphoma
, Cancer Care Ontario (CCO) Iodine-131 Tositumomab in Lymphoma") Evidence-based Series 6-19 EDUCATION AND INFORMATION 2013 A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Iodine-131 Tositumomab in Lymphoma The Hematology
Evidence-based Series 6-19 EDUCATION AND INFORMATION 2013 A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Iodine-131 Tositumomab in Lymphoma The Hematology
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
The treatment of DLBCL. Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona
 The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents
 Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
POST ICML Indolent lymphomas relapse treatment
 POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
Blood Cancers. Blood Cells. Blood Cancers: Progress and Promise. Bone Marrow and Blood. Lymph Nodes and Spleen
 Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
Blood Cancers: Progress and Promise Mike Barnett & Khaled Ramadan Division of Hematology Department of Medicine Providence Health Care & UBC Blood Cancers Significant health problem Arise from normal cells
To Maintain or Not to Maintain? Lymphoma and Myeloma 2015 Waldorf Astoria Hotel, New York
 To Maintain or Not to Maintain? Lymphoma and Myeloma 2015 Waldorf Astoria Hotel, New York Sundar Jagannath Director, Multiple Myeloma Program Tisch Cancer Institute Mount Sinai Medical Center Maintenance
To Maintain or Not to Maintain? Lymphoma and Myeloma 2015 Waldorf Astoria Hotel, New York Sundar Jagannath Director, Multiple Myeloma Program Tisch Cancer Institute Mount Sinai Medical Center Maintenance
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES!
 Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Non-Hodgkin lymphomas (NHLs) constitute a heterogeneous. Original Articles
 constitute a heterogeneous. Original Articles") CANCER BIOTHERAPY AND RADIOPHARMACEUTICALS Volume 28, Number 5, 2013 ª Mary Ann Liebert, Inc. DOI: 10.1089/cbr.2012.1387 Original Articles Phase I Study of a Modified Regimen of 90 Yttrium Ibritumomab
CANCER BIOTHERAPY AND RADIOPHARMACEUTICALS Volume 28, Number 5, 2013 ª Mary Ann Liebert, Inc. DOI: 10.1089/cbr.2012.1387 Original Articles Phase I Study of a Modified Regimen of 90 Yttrium Ibritumomab
Linfoma de Hodgkin. Novos medicamentos. Otavio Baiocchi CRM-SP
 Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Anti-CD20-based therapy of B cell lymphoma: state of the art
 (2002) 16, 2004 2015 2002 Nature Publishing Group All rights reserved 0887-6924/02 $25.00 www.nature.com/leu REVIEW Anti-CD20-based therapy of B cell lymphoma: state of the art C Kosmas 1, K Stamatopoulos
(2002) 16, 2004 2015 2002 Nature Publishing Group All rights reserved 0887-6924/02 $25.00 www.nature.com/leu REVIEW Anti-CD20-based therapy of B cell lymphoma: state of the art C Kosmas 1, K Stamatopoulos
Management of high-risk diffuse large B cell lymphoma: case presentation
 Management of high-risk diffuse large B cell lymphoma: case presentation Daniel J. Landsburg, MD Assistant Professor of Clinical Medicine Perelman School of Medicine University of Pennsylvania January
Management of high-risk diffuse large B cell lymphoma: case presentation Daniel J. Landsburg, MD Assistant Professor of Clinical Medicine Perelman School of Medicine University of Pennsylvania January
TRANSPARENCY COMMITTEE OPINION. 8 November 2006
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 8 November 2006 MABTHERA 100 mg, concentrate for solution for infusion (CIP 560 600-3) Pack of 2 MABTHERA 500 mg,
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 8 November 2006 MABTHERA 100 mg, concentrate for solution for infusion (CIP 560 600-3) Pack of 2 MABTHERA 500 mg,
Study No.: Title: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Follicular Lymphoma. Michele Ghielmini. Oncology Institute of Southern Switzerland Bellinzona
 Follicular Lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona Conflicts of interest Astra Zeneca Roche Cellgene Mundipharma Janssen Gilead Bayer Abbvie FL remains an incurable
Follicular Lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona Conflicts of interest Astra Zeneca Roche Cellgene Mundipharma Janssen Gilead Bayer Abbvie FL remains an incurable
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients
 Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
Mantle cell lymphoma Allo stem cell transplantation in relapsed and refractory patients Olivier Hermine MD, PhD Department of Hematology INSERM and CNRS, Imagine Institute Necker Hospital Paris, France
Tositumomab and iodine I 131 tositumomab (Bexxar ) Corixa Corporation; marketed by GlaxoSmithKline 1
 Corixa Corporation; marketed by GlaxoSmithKline 1") Generic (Trade Name): Manufacturer: Tositumomab and iodine I 131 tositumomab (Bexxar ) Corixa Corporation; marketed by GlaxoSmithKline 1 NO. 64 OCTOBER 2005 Indication: Current Regulatory Status: In the
Generic (Trade Name): Manufacturer: Tositumomab and iodine I 131 tositumomab (Bexxar ) Corixa Corporation; marketed by GlaxoSmithKline 1 NO. 64 OCTOBER 2005 Indication: Current Regulatory Status: In the
What is the best approach to the initial therapy of PTCL? standards of treatment? Should all
 What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL):
:") Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Radioimmunotherapy for B-Cell Non-Hodgkin Lymphomas
 Radioimmunotherapy is an effective but underutilized treatment option for patients with B-cell non-hodgkin lymphoma in both the front-line and the relapsed/refractory setting. George Van Hook. Flyfishing.
Radioimmunotherapy is an effective but underutilized treatment option for patients with B-cell non-hodgkin lymphoma in both the front-line and the relapsed/refractory setting. George Van Hook. Flyfishing.
Notification to Implement Issued by pcodr: December 14, 2012
 PROVINCIAL FUNDING SUMMARY Bendamustine hydrochloride (Treanda) for indolent Non-Hodgkin Lymphoma and Mantle Cell Lymphoma (first-line and relapsed/refractory) perc Recommendation: Recommends For further
PROVINCIAL FUNDING SUMMARY Bendamustine hydrochloride (Treanda) for indolent Non-Hodgkin Lymphoma and Mantle Cell Lymphoma (first-line and relapsed/refractory) perc Recommendation: Recommends For further
trial update clinical
 trial update clinical by John W. Mucenski, BS, PharmD, Director of Pharmacy Operations, UPMC Cancer Centers Recent advances in radiation therapy, such as intensity modulated radiation therapy (IMRT), have
trial update clinical by John W. Mucenski, BS, PharmD, Director of Pharmacy Operations, UPMC Cancer Centers Recent advances in radiation therapy, such as intensity modulated radiation therapy (IMRT), have
Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL
 Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
UBS European Conference 2013
 UBS European Conference 2013 Tuesday, 12 November 2013 Karl Mahler, Head of Investor Relations Stefan Frings, Oncology/Immunology Therapeutic Area Head,Roche Partnering Group: Continued strong sales growth
UBS European Conference 2013 Tuesday, 12 November 2013 Karl Mahler, Head of Investor Relations Stefan Frings, Oncology/Immunology Therapeutic Area Head,Roche Partnering Group: Continued strong sales growth
Firenze, settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo
 Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
How I treat High-risk follicular lymphoma
 How I treat High-risk follicular lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona 1) median OS raised from 10 to 18 y 2) advanced FL remains uncurable Stanford, n = 1334
How I treat High-risk follicular lymphoma Michele Ghielmini Oncology Institute of Southern Switzerland Bellinzona 1) median OS raised from 10 to 18 y 2) advanced FL remains uncurable Stanford, n = 1334
Brad S Kahl, MD. Tracks 1-21
 I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
I N T E R V I E W Brad S Kahl, MD Dr Kahl is Associate Professor and Director of the Lymphoma Service at the University of Wisconsin School of Medicine and Public Health and Associate Director for Clinical
CLL: disease specific biology and current treatment. Dr. Nathalie Johnson
 CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck
CLL: disease specific biology and current treatment Dr. Nathalie Johnson Disclosures Consultant and Advisory boards Roche, Abbvie, Gilead, Jansson, Lundbeck,Merck Research funding Roche, Abbvie, Lundbeck