Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern
|
|
|
- Roderick McCarthy
- 6 years ago
- Views:
Transcription

1 Polypoid Melanoma, A Virulent Variant of the Nodular Growth Pattern ELIZABETH A. MANCI, M.D., CHARLES M. BALCH, M.D..TARIQ M. MURAD, M.D., PH.D., AND SENG/JAW SOONG, PH.D. Manci, Elizabeth A., Balch, Charles M., Murad, Tariq M., and Soong, Seng-Jaw: Polypoid melanoma, a virulent variant of the nodular growth pattern. Am J Clin Pathol 75: , Thirty-two patients who had polypoid melanoma were identified in a registry of 552 melanoma patients. The tumor is regarded as a variant of nodular melanoma and is associated with an increased thickness, more frequent ulceration than the nodular variant of melanoma, younger patient age, and higher probability of occult metastasis. Polypoid melanomas were most frequently present on the trunk, and were also encountered in unusual sites, such as the mucosa of the nose, hard palate, and anorectal junction. In terms of survival, the patients with the polypoid nodular variant fared significantly worse than those with nonpolypoid nodular (P =.5) and those with superficial spreading (P =.3) melanomas. The five-year survival rate for the polypoid variant was 42%, in contrast to 57% for the nonpolypoid nodular and 77% for the superficial spreading melanomas. The poor prognosis of patients who have polypoid melanoma is most likely due to its being the type of melanoma with the deepest penetration at the time of surgical excision. (Key words: Polypoid melanoma; Nodular melanoma; Ulceration; Melanoma growth pattern; Melanoma registry; Survival.) FOUR MAJOR GROWTH PATTERNS of melanoma have been described in the literature: superficial spreading, lentigo maligna, nodular, and acrallentigenous types. 91,1314 These growth patterns have been useful as therapeutic and prognostic parameters for patients who have melanoma. The nodular growth pattern has been associated with the most malignant expression of the disease. It has been further subdivided into three distinct variants: a smooth uniform nodule beneath the epidermal surface, an elevated blue-black plaque with an irregular outline, and a pedunculated or polypoid tumor. 9 Of these three variants of nodular melanoma, patients with polypoid tumors have the poorest prognosis. In the present paper, we will present our data for 32 patients who had the polypoid variant of nodular melanoma. Materials and Methods The University of Alabama (UAB) Melanoma Registry contains computerized data for 552 melanoma Received August 4, 198; received revised manuscript and accepted for publication October 17, 198. Address reprint requests to Dr. Murad: Department of Pathology, University of Alabama Medical Center, University Station, Birmingham, Alabama University of Alabama Medical Center, Departments of Pathology, Surgery, and Biostatistics, and the Comprehensive Cancer Center, Birmingham, Alabama patients treated at this institution between 1958 and Pertinent clinical and histologic information has been extracted and analyzed statistically. 1-2,4 The growth pattern of each melanoma has been classified as superficial spreading, lentigo maligna, or nodular, as defined by Clark and associates. 9 The polypoid variant of nodular melanoma was defined as a tumor in which the bulk of the lesion is located above the epidermis, the lateral margins are everted, giving the mass a cauliflower-shape, and lateral extension of the lesion into the adjacent epidermis is limited to less than three rete ridges. Pathologic parameters measured for each lesion included the thickness (Breslow's microstaging); level of invasion (Clark's microstaging); presence or absence of metastases, microscopic ulceration, pigmentation, and lymphocytic infiltration according to criteria defined previously. 2,4,7,9 The clinical data available for each patient included race, sex, age, location and size of the primary lesion, past medical history, family history of malignancy, clinical stage, gross evidence of ulceration, date of diagnosis, and periodic follow-up. Actuarial survival rates were calculated by the method of Kaplan and Meier, and a generalized Wilcoxson test was used to determine whether significant differences in patient survival existed between the polypoid variant and other growth patterns. 8 Chisquare tests were also employed in statistical assessments where appropriate. A discriminant analysis was also employed to discern those features that significantly distinguished patients with polypoid tumor from patients with other types of nodular melanoma. 15 Results Thirty-two (18%) of the 176 nodular melanomas in our series had a polypoid configuration. Nineteen (59%) were in men and 13 (41%) in women. The overall median age at the time of diagnosis was 37 years; ages ranged from 2 to 73 years. Most patients (56%), however, were in the third and fourth decades. The average /81/6/81 $.8 American Society of Clinical Pathologists 81 Downloaded from on 6 March 218
, and the upper")
, but it was involved in 22% of female patients in our registry whose lesions had the other growth patterns of melanoma.")
2 Vol. 75 No. 6 POLYPOID MELANOMA age for men was 41 years (range, 21 to 73 years), and that for women was 48 years (range, 26 to 73 years). The trunk was the most frequently involved body site; however, when the data were analyzed by sex, the lower extremity was found to be the most frequent primary site in women (75%), and the upper trunk (71%) in men. The upper extremity was rarely involved in female patients who had polypoid melanomas (7.7%), but it was involved in 22% of female patients in our registry whose lesions had the other growth patterns of melanoma. A few mucosal lesions, including the nasal mucosa, hard palate, and anorectal junction, were encountered. Clinically, polypoid melanoma was a pedunculated, cauliflower-like lesion whose major growth was above the surface. The median diameter of the lesion was 2 cm (range,.5 to 15 cm). Gross ulceration and pigmentation were present in most of our cases. At the time of diagnosis, 69% of the cases were classified as clinical stage I (without clinically detectable metastasis) and 31% as clinical stage II (with clinical evidence of metastasis). Satellite nodules were identified in 11% of 811 Table I. Clinical Comparison of Polypoid and Nonpolypoid Nodular Melanomas Polypoid Total no. of patients Age (yrs) < >6 Sex Male Female Site of primary lesion Lower extremity Upper extremity Head and neck Trunk Other Clinical staging Nonpolypoid (56%) 5 (16%) 9 (28%) 4 (3%) 4 (28%) 6 (42%) 39 (26%) 1 19 (59%) 13 (41%) 75 (52%) 69 (48%) 8 (25%) 7 (22%) 4(13%) 13 (41%) 36 (25%) 28 (19%) 29 (2%) 47 (33%) 4 (3%) 22 (69%) 1(31%) 114(79%) 28 (2%) 2(1%) P Value* * The P value refers to the comparison between the polypoid and nonpolypoid nodular melanomas with respect to the distribution of the factors specified. t Statistically significant P value. FIG. 1. The bulk of the polypoid melanoma lesion is located above the epidermis, and the lateral margins are everted, giving the mass a cauliflower shape. Direct photography. x6. Downloaded from on 6 March 218

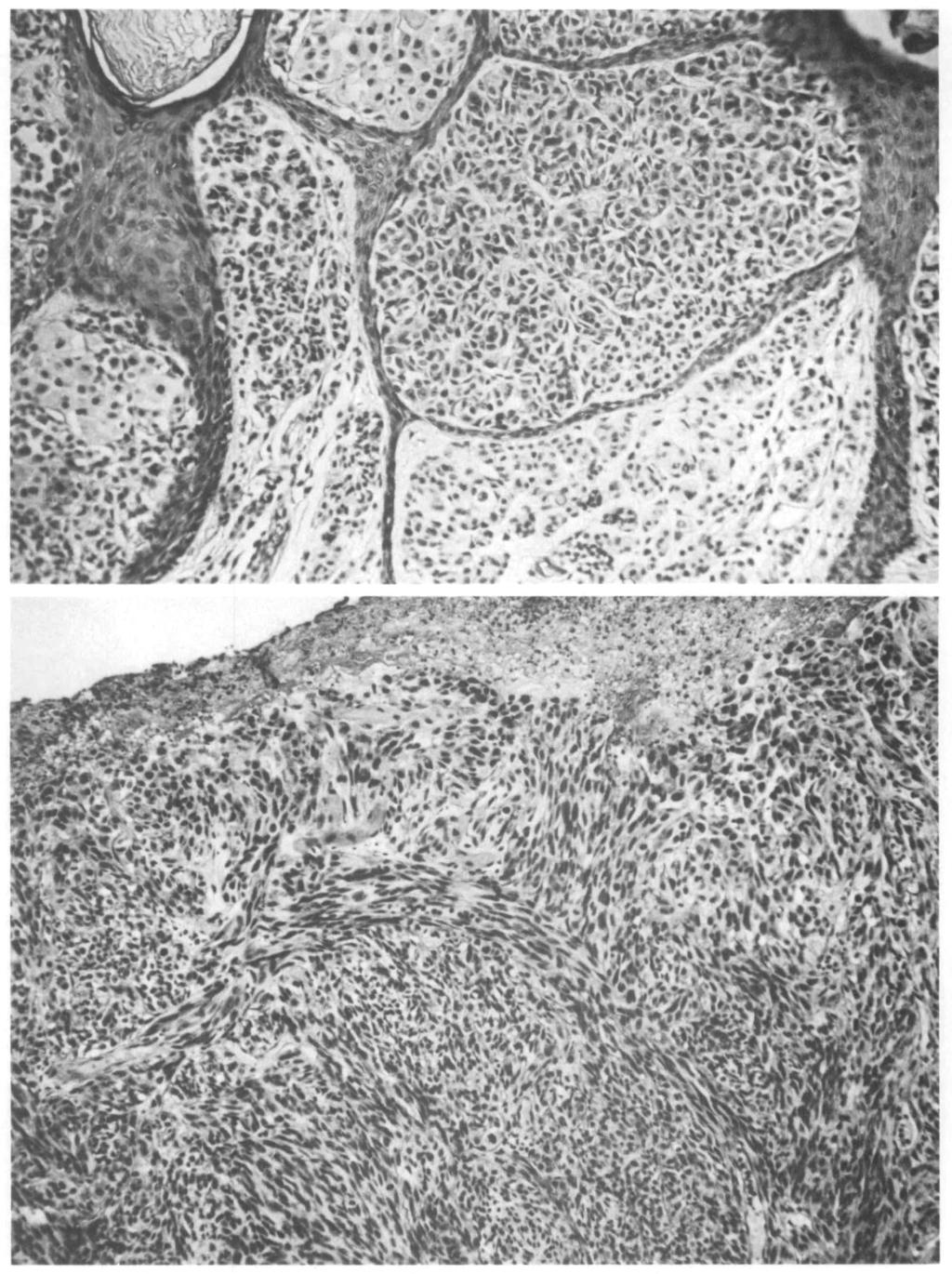
3 812 A.J.C.P. June1981 MANCI ET AL. eosin. x 11. Downloaded from on 6 March 218


4 Vol. 75 No. 6 POLYPOID MELANOMA 813 FIG. 4. Moderate lymphocytic infiltration is present at the base of the polypoid melanoma. The leading edge of the lesions frequently appeared sharply demarcated from the adjacent dermis. Vascular channels were most numerous at the base of the lesion, and lymphatic permeation was a frequent finding. Hematoxylin and eosin. x 15. the patients who had polypoid melanoma and were seen only in patients who had lesions of the dorsal trunk. A summary of the clinical data is presented in Table 1. Histologically, the polypoid growth pattern mushroomed over the adjacent skin (Fig. 1). In most cases, the melanoma cells were polyhedral (Fig. 2); in a few patients the tumor was formed primarily of spindletype cells (Fig. 3). The lesions were large and deep, ranging from 1.5 to 12.6 mm in depth and having an overall median vertical thickness of 4.85 mm. Pigmentation and surface ulceration were identified in approximately 75% of the cases (Fig. 3). In most cases, the tumor had invaded the reticular dermis (Clark's level IV) at the time of histologic examination. Most polypoid melanomas had a diminished host response evidenced by only mild to moderate lymphocytic infiltration of the adjacent stroma (Fig. 4). Although the leading edges of the lesions frequently appeared to be pushing into the adjacent dermis and were sharply demarcated, lymphatic permeation was frequently seen at the bases of the lesions (Fig. 4). The incidence of lymph node metastases appeared to be directly related to tumor thickness. In this regard, the median thickness of the polypoid melanomas with no histologically demonstrable metastasis (pathologic stage 1) was 3.2 mm, whereas the median thickness for lesions with nodal metastases (pathologic stage Downloaded from on 6 March 218 2) was 7.2 mm. The histologic data are summarized in Table 2. The five-year survival rate for patients with polypoid melanoma was 42%, whereas the rate for patients with nonpolypoid nodular melanoma was 57%. The fiveyear survival rate was better for patients who had superficial spreading melanoma (77%) (Table 3). T h e P value for comparing the differences in survival between the polypoid and nodular melanomas was.5 and that for comparing the polypoid and superficial spreading melanomas was.3. For patients with pathologic stage I lesions, tumor thickness was inversely correlated with survival. Patients with the longest survival time (1-11 years) had tumors ranging in thickness from 2 to 3.1 mm (median, 2.6 mm); patients with the shortest survival (1-2 years) had tumors ranging in thickness from 2.6 to 8 mm (median, 4.4 mm). However, for patients with pathologic stage II lesions, this inverse correlation of thickness with survival was not found. Instead, survival was more directly correlated with the number of positive lymph nodes at the time of diagnosis. In this regard, the average survival for patients with four or more positive lymph nodes was ten months, and for patients with two or less lymph nodes it was 2 months. The number of positive nodes in patients with pathologic stage II lesions varied from one to five nodes (a
 1.5-2.99 7 (22%) 45(31%) 3-3.99 6(19%) 19(13%) >4.")
5 814 MANCI 7/AL. A.J.C.P. June 1981 Table 2. Histologic Comparison of Polypoid and Nonpolypoid Nodular Melanomas Polypoid Nonpolypoid Total no. of patients Thickness (mm) (1%) (24%) (22%) 45(31%) (19%) 19(13%) >4. 19 (59%) 31 (22%) 1 Clark's level II III IV V Microscopic ulceration Present Absent Pigmentation Present Absent Lymphocytic infiltration Mild Moderate Heavy Pathologic stage (I) No evidence of metastasis (II) With lymph node metastases (III) With distant metastases * Statistically significant P value. 1 (3%) 9 (28%) 18 (56%) 4 (13%) 22 (72%) 8 (25%) 1 (3%) 24 (75%) 7 (22%) 1 (3%) 11 (35%) 19 (59%) 2 (6%) 21 (66%) 11 (34%) 13 (9%) 49 (35%) 54 (38%) 26(18%) 2 69 (48%) 72 (5%) 3 (2%) 11 (77%) 25 (17%) 9 (6%) 48 (33%) 56 (39%) 23 (16%) 17 (12%) 119 (83%) 22(15%) 3 (2%) P Value.5*.25.37* * median of two positive nodes per patient). The average survival of patients with metastases was 1.9 years. To compare polypoid tumors with other nodular melanomas, all clinical and pathologic variables were subjected to discriminant analysis. After simultaneously accounting for all other variables, three factors were found to be statistically significant in distinguishing the polypoid tumors from other nodular melanomas: thickness, ulceration, and age. lesions require a marked vessel proliferation that facilitates early metastasis. 11 Our data support these observations, since lymphatic permeation was present in many of our lesions in spite of their well-demarcated or pushing borders (Fig. 4). In our series, polypoid melanomas were typically 2 cm in diameter, invading to Clark's level IV, 4.85 mm thick, ulcerated, and heavily pigmented. Patients with these tumors had a younger median age at the time of diagnosis, a high rate of metastases, and a poor prognosis. The UAB data are generally similar to those of the Queensland Melanoma Project except for a higher ratio of nodular melanomas and chest lesions at UAB. 5,1 Among the variables that were analyzed, tumor thickness strongly correlated with prognosis for patients with pathologic stage I polypoid melanoma. The thinnest polypoid melanoma in the UAB series (1.5 mm) was in the range associated with a 57% risk of harboring regional metastases at the time of diagnosis. 2 Most patients had tumors greater than 4 mm in thickness, which are associated with an extremely high risk (8%) of harboring occult regional and distant metastases. 2 In the presence of regional metastases, however, tumor thickness appears to be a less important prognostic indicator than the number of lymph nodes containing the tumor. In a previous study, thickness also had a less significant correlation with prognosis for those patients who had been treated by wide local excision and regional node dissection. 3 The lack of association between thickness and lymph node metastasis may indicate a tendency for some of these tumors to regress after regional metastases are established. Smith and Stehlin have reported the case of a patient who had a well-documented "toadstool" melanoma that appeared and spontaneously regressed during a two-year interval; however, within the following year it disseminated widely and was fatal. 18 Clinical recognition of the characteristic gross morphologic features of polypoid melanoma should alert physicians to the high risk of underlying metastatic disease at the time of diagnosis. The differential diagnosis of such lesions should include benign neurofibroma, seborrheic keratosis, pyogenic granuloma, squamous cell carcinoma, basal cell carcinoma, hemangioma, and hematoma Since tumor Discussion The polypoid growth pattern of melanoma was first mentioned in the literature by Vogler and associates in 1958 as a "pedunculated" melanoma lesion. 19 In 1968, Bodenham noted that "mushroom shaped" melanomas were associated with a poor prognosis. 6 In 1972, Little postulated that the rapid growth and expansion of these Table 3. Comparison of Actuarial Survival Rates for Three Growth Patterns of Melanoma No. of Growth Pattern Patients 1 Year 3 Years 5 Years Polypoid 32 88% 48% 42% Nodular 144 9% 74% 57% Superficial spreading 67 98% 85% 77% Downloaded from on 6 March 218

6 Vol. 75 No. 6 POLYPOID MELANOMA 815 thickness is an important factor in predicting metastatic disease in patients who have melanoma, a suspected lesion should never be excised by a shave or a curette biopsy technic that would disrupt the deep margin of the tumor. An excisional biopsy extending down to the subcutaneous tissue is required for accurate microstaging. In our small series, when metastases were present with a polypoid melanoma, accurate assessment of the number of nodes containing the tumor was the most important prognostic indicator for this most virulent form of melanoma. References 1. Balch CM, Murad TM, Soong S, et al: A multifactorial analysis of melanoma: prognostic histopathological features comparing Clark's and Breslow's staging methods. Ann Surg 188: , Balch CM, Murad TM, Soong S, et al: Tumor thickness as a guide to surgical management of clinical stage 1 melanoma patients. Cancer 43: , Balch CM, Soong SJ, Murad TM, et al: A multifactorial analysis of melanoma II: prognostic factors in patients with stage 1 (localized) melanoma. Surgery 86: , Balch CM, Wilkerson JA, Murad RM, et al: The prognostic significance of ulceration of cutaneous melanoma. Cancer 45: , Beardmore GL: Primary cutaneous polypoidal nonstageable melanomas in Queensland. Aust J Dermatol 18:73-76, Bodenham DC: A study of 65 observed malignant melanomas in the southwest region. Ann R Coll Surg Engl 43: , Breslow A: Thickness, cross-sectional areas and depth of invasion in the prognosis of cutaneous melanoma. Ann Surg 172:92-98, Burnette WJ, Gehan EA: Planning and analysis of clinical studies. Springfield, Charles C Thomas, 197, pp Clark WH, From L, Bernardino EA, et al: The histogenesis and biologic behavior of primary human malignant melanomas of the skin. Cancer Res 29:75-727, Davis N: Malignant melanoma in Queensland: a review. Aust J Dermatol 19:13-18, Little JH: Histology and prognosis in cutaneous malignant melanoma, Melanoma and skin cancer, proceedings of the Informational Cancer Conference, Sydney. Edited by V. C. N. Blight. New South Wales, Government Printer, 1972, pp Little JH, Davis NC: Frozen section diagnosis of suspected malignant melanoma of the skin. Cancer 34: , McGovern VJ: The classification of melanoma and its relationship with prognosis. Pathology 2:85-98, Mihm MC, Clark WH, Reed RJ: The clinical diagnosis of malignant melanoma. Semin Oncol 2:15-118, Morrison DF: Multivariate statistical analysis. Second edition. New York, McGraw-Hill, 1976, pp Niven J, Lubin J: Pedunculated malignant melanoma. Arch Dermatol 111: , Shapiro L, Bodian EL: Malignant melanoma in the form of pedunculated papules. Arch Dermatol 99:49-5, Smith JL, Stehlin JS: Spontaneous regression of primary malignant melanomas with regional metastases. Cancer 18: , Vogler WR, Perdue GD, Wilkins SA: A clinical evaluation of malignant melanoma. Surg Gynecol Obstet 16: ,1958 Downloaded from on 6 March 218
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases
 Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Amelanotic melanoma of the skin detailed review of the problem
 of the skin detailed review of the problem Strahil Strashilov 1, Veselin Kirov 2, Angel Yordanov 3, Yoana Simeonova 4 and Miroslava Mihailova 5 1. Department of Plastic Restorative, Reconstructive and
of the skin detailed review of the problem Strahil Strashilov 1, Veselin Kirov 2, Angel Yordanov 3, Yoana Simeonova 4 and Miroslava Mihailova 5 1. Department of Plastic Restorative, Reconstructive and
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Breslow Thickness and Clark Level Evaluation in Albanian Cutaneous Melanoma
 Research DOI: 10.6003/jtad.16104a2 Breslow Thickness and Clark Level Evaluation in Albanian Cutaneous Melanoma Daniela Xhemalaj, MD, Mehdi Alimehmeti, MD, Susan Oupadia, MD, Majlinda Ikonomi, MD, Leart
Research DOI: 10.6003/jtad.16104a2 Breslow Thickness and Clark Level Evaluation in Albanian Cutaneous Melanoma Daniela Xhemalaj, MD, Mehdi Alimehmeti, MD, Susan Oupadia, MD, Majlinda Ikonomi, MD, Leart
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Thin Melanoma. N Context. The incidence of malignant melanoma is
 Thin Melanoma David E. Elder, MB ChB, FRCPA N Context. The incidence of malignant melanoma is increasing and a preponderance of the melanomas diagnosed today are thin in terms of Breslow criteria. Although
Thin Melanoma David E. Elder, MB ChB, FRCPA N Context. The incidence of malignant melanoma is increasing and a preponderance of the melanomas diagnosed today are thin in terms of Breslow criteria. Although
Acral Melanoma in Japan
 Acral Melanoma in Japan MAKOTO SEUI, M.D., HIDEAKI TAKEMATSU, M.D., MICHIKO HOSOKAWA, M.D., MASAAKI OBATA, M.D., YASUSHI TOMITA, M.D., TAIZO KATO, M.D., MASAAKI TAKAHASHI, M.D., AND MARTIN C. MIHM, JR.,
Acral Melanoma in Japan MAKOTO SEUI, M.D., HIDEAKI TAKEMATSU, M.D., MICHIKO HOSOKAWA, M.D., MASAAKI OBATA, M.D., YASUSHI TOMITA, M.D., TAIZO KATO, M.D., MASAAKI TAKAHASHI, M.D., AND MARTIN C. MIHM, JR.,
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Clinical and Pathological Features of Cutaneous Malignant Melanoma: A Retrospective Analysis of 124 Japanese Patients
 Clinical and Pathological Features of Cutaneous Malignant Melanoma: A Retrospective Analysis of 24 Japanese Patients Yoshie Kuno, Kazuyuki Ishihara, Naoya Yamazaki and Kiyoshi Mukai 2 'Dermatology Division
Clinical and Pathological Features of Cutaneous Malignant Melanoma: A Retrospective Analysis of 24 Japanese Patients Yoshie Kuno, Kazuyuki Ishihara, Naoya Yamazaki and Kiyoshi Mukai 2 'Dermatology Division
Lichenoid Tissue Reaction in Malignant Melanoma A Potential Diagnostic Pitfall
 natomic Pathology / LICHENOID TISSUE RECTION IN MLIGNNT MELNOM Lichenoid Tissue Reaction in Malignant Melanoma Potential Diagnostic Pitfall CPT Scott R. Dalton, MC, US, 1,3 Capt Matt. aptista, USF, MC,
natomic Pathology / LICHENOID TISSUE RECTION IN MLIGNNT MELNOM Lichenoid Tissue Reaction in Malignant Melanoma Potential Diagnostic Pitfall CPT Scott R. Dalton, MC, US, 1,3 Capt Matt. aptista, USF, MC,
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Melanoma of the Skin INTRODUCTION SUMMARY OF CHANGES
 24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44.6 Skin of upper limb
24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44.6 Skin of upper limb
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
MALIGNANT MELANOMA OF THE HEEL
 MALIGNANT MELANOMA OF THE HEEL Pages with reference to book, From 50 To 53 Fazli M. Qazi ( Departments of Pathology, Khyber Medical College, Peshawar. ) Rahjm Gul ( Departments of Surgery, Khyber Medical
MALIGNANT MELANOMA OF THE HEEL Pages with reference to book, From 50 To 53 Fazli M. Qazi ( Departments of Pathology, Khyber Medical College, Peshawar. ) Rahjm Gul ( Departments of Surgery, Khyber Medical
Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]](/thumbs/71/65936251.jpg "Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ]") MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
MelanomaSkin CS Tumor Size Collaborative Stage for TNM 7 - Revised 07/14/2009 [ Schema ] Code 000 No mass/tumor found Description 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters
Directly Coded Summary Stage Melanoma
 Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
ORIGINAL ARTICLE. Clinical Node-Negative Thick Melanoma
 ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Melanoma of the Skin
 24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44. Skin of upper limb
24 Melanoma of the Skin C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of other and unspecified parts of face C44.4 Skin of scalp and neck C44.5 Skin of trunk C44. Skin of upper limb
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Prognostic value of tumour thickness in cutaneous malignant melanoma
 J Clin Pathol 1983;36:51-56 Prognostic value of tumour thickness in cutaneous malignant melanoma IONA JEFFREY, PATRICK ROYSTON, CHRISTOPHER SOWTER, GERARD SLAVIN, ASHLEY PRICE, ARIELA POMERANCE,* SALEEM
J Clin Pathol 1983;36:51-56 Prognostic value of tumour thickness in cutaneous malignant melanoma IONA JEFFREY, PATRICK ROYSTON, CHRISTOPHER SOWTER, GERARD SLAVIN, ASHLEY PRICE, ARIELA POMERANCE,* SALEEM
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Interesting Case Series. Desmoplastic Melanoma
 Interesting Case Series Desmoplastic Melanoma Anthony Maurice Kordahi, MD, Joshua B. Elston, MD, Ellen M. Robertson, MD, and C. Wayne Cruse, MD Division of Plastic Surgery, Department of Surgery, University
Interesting Case Series Desmoplastic Melanoma Anthony Maurice Kordahi, MD, Joshua B. Elston, MD, Ellen M. Robertson, MD, and C. Wayne Cruse, MD Division of Plastic Surgery, Department of Surgery, University
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Collaborative Staging Manual and Coding Instructions Part II: Primary Site Schema
 C44.0-C44.9, C51.0-C51.2, C51.8-C51.9, C60.0-C60.2, C60.8-C60.9, C63.2 (M-8720-8790) C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of ear and unspecified parts of face C44.4 Skin of
C44.0-C44.9, C51.0-C51.2, C51.8-C51.9, C60.0-C60.2, C60.8-C60.9, C63.2 (M-8720-8790) C44.0 Skin of lip, NOS C44.1 Eyelid C44.2 External ear C44.3 Skin of ear and unspecified parts of face C44.4 Skin of
1
 www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Assisting diagnosis of melanoma through the noninvasive biopsy of skin lesions
 Assisting diagnosis of melanoma through the noninvasive biopsy of skin lesions Symon D Oyly Cotton Ela Claridge School of Computer Science, The University of Birmingham Birmingham B15 2TT, UK Per Hall
Assisting diagnosis of melanoma through the noninvasive biopsy of skin lesions Symon D Oyly Cotton Ela Claridge School of Computer Science, The University of Birmingham Birmingham B15 2TT, UK Per Hall
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin. Suraj Venna
 AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
MALIGNANT MELANOMA IN QUEENSLAND x
 MALIGNANT MELANOMA IN QUEENSLAND 35 MALIGNANT MELANOMA IN QUEENSLAND x NEVILLE C. DAVIS, F.R.C.S., FJLA.C.S. Co-ordinator, Queensland Melanoma Project, Princess Alexandra Hospital, Brisbane. Between July
MALIGNANT MELANOMA IN QUEENSLAND 35 MALIGNANT MELANOMA IN QUEENSLAND x NEVILLE C. DAVIS, F.R.C.S., FJLA.C.S. Co-ordinator, Queensland Melanoma Project, Princess Alexandra Hospital, Brisbane. Between July
أملس عضلي غرن = Leiomyosarcoma. Leiomyosarcoma 1 / 5
 Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Leiomyosarcoma 1 / 5 EPIDEMIOLOGY Exact incidence is unknown, but older studies suggest that leiomyosarcomas comprise approximately 3 percent of soft-tissue sarcomas. Superficial leiomyosarcoma occurs
Multiple Primary Melanoma in a Thai Male: A Case Report
 Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
ORAL MELANOMA Definition Epidemiology Clinical Presentation
 ORAL MELANOMA Definition Melanoma is a highly malignant neoplasia, arising from melanocytes, the cells that produce the brownish pigment melanin. Melanin is the determinant in skin colour and protects
ORAL MELANOMA Definition Melanoma is a highly malignant neoplasia, arising from melanocytes, the cells that produce the brownish pigment melanin. Melanin is the determinant in skin colour and protects
World Articles of Ear, Nose and Throat Page 1
 World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre
 Malaysian J Pathol 202; (2) : 97 0 ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre Jayalakshmi PAILOOR, Kein-Seong
Malaysian J Pathol 202; (2) : 97 0 ORIGINAL ARTICLE Cutaneous malignant melanoma: clinical and histopathological review of cases in a Malaysian tertiary referral centre Jayalakshmi PAILOOR, Kein-Seong
Growth rate of melanoma in vivo and correlation with dermatoscopic and dermatopathologic findings
 Dermatology Practical & Conceptual www.derm101.com Growth rate of melanoma in vivo and correlation with dermatoscopic and dermatopathologic findings Jürgen Beer, M.D. 1, Lina Xu, M.D. 1, Philipp Tschandl,
Dermatology Practical & Conceptual www.derm101.com Growth rate of melanoma in vivo and correlation with dermatoscopic and dermatopathologic findings Jürgen Beer, M.D. 1, Lina Xu, M.D. 1, Philipp Tschandl,
Subject Index. Dry desquamation, see Skin reactions, radiotherapy
 Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
Malignant melanoma of the eyelid skin:
 British Journal of Ophthalmology, 1985, 69, 180-186 Malignant melanoma of the eyelid skin: histopathology and behaviour A GARNER,' L KOORNNEEF,2 A LEVENE,3 AND J R 0 COLLIN4 From the 'Department of Pathology,
British Journal of Ophthalmology, 1985, 69, 180-186 Malignant melanoma of the eyelid skin: histopathology and behaviour A GARNER,' L KOORNNEEF,2 A LEVENE,3 AND J R 0 COLLIN4 From the 'Department of Pathology,
Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]](/thumbs/82/86783199.jpg "Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ]") CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
CS Tumor Size Collaborative Stage for TNM 7 - Revised 12/02/2009 [ Schema ] Note: the specific tumor size as documented in the medical record. If the ONLY information regarding tumor size is the physician's
Contrast with Australian Guidelines A/Pr Pascale Guitera,
 Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Contrast with Australian Guidelines A/Pr Pascale Guitera, Dermatologist, Sydney University NO CONFLICT OF INTEREST Sydney Melanoma Diagnostic Centre, RPAH 2011 2008 225 pages 16 pages http://www.cancer.org.au/file/healthprofessionals/clinica
Pathology. Skin Tumor. Bayan N. Mohammad 15/10/2015. Mohammad al-orjani. Page 0 of 23
 #7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
#7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
Surgical Margins in Cutaneous Melanoma (2 cm Versus 5 cm for Lesions Measuring Less Than 2.1-mm Thick)
") 1941 Surgical Margins in Cutaneous Melanoma (2 cm Versus 5 cm for Lesions Measuring Less Than 2.1-mm Thick) Long-Term Results of a Large European Multicentric Phase III Study David Khayat, M.D., Ph.D.
1941 Surgical Margins in Cutaneous Melanoma (2 cm Versus 5 cm for Lesions Measuring Less Than 2.1-mm Thick) Long-Term Results of a Large European Multicentric Phase III Study David Khayat, M.D., Ph.D.
Da Costa was the first to coin the term. Marjolin s Ulcer: A Case Report and Literature Review. Case Report. Introduction
 E-Da Medical Journal 2016;3(2):24-28 Case Report Marjolin s Ulcer: A Case Report and Literature Review Yue-Chiu Su 1, Li-Ren Chang 2 Marjolin s ulcer is an aggressive cutaneous malignancy, which is common
E-Da Medical Journal 2016;3(2):24-28 Case Report Marjolin s Ulcer: A Case Report and Literature Review Yue-Chiu Su 1, Li-Ren Chang 2 Marjolin s ulcer is an aggressive cutaneous malignancy, which is common
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Malignant Melanoma of the Head and Neck: A Brief Review of Pathophysiology, Current Staging, and Management
 The Ochsner Journal 8:181 185, 2008 f Academic Division of Ochsner Clinic Foundation Malignant Melanoma of the Head and Neck: A Brief Review of Pathophysiology, Current Staging, and Management Christian
The Ochsner Journal 8:181 185, 2008 f Academic Division of Ochsner Clinic Foundation Malignant Melanoma of the Head and Neck: A Brief Review of Pathophysiology, Current Staging, and Management Christian
Dr. Brent Doolan, BSc MBBS MPH
 Impact of partial biopsies on the need for complete excisional surgery in the management of cutaneous melanomas: A multi-centre review Dr. Brent Doolan, BSc MBBS MPH Peter MacCallum Cancer Centre, Melbourne
Impact of partial biopsies on the need for complete excisional surgery in the management of cutaneous melanomas: A multi-centre review Dr. Brent Doolan, BSc MBBS MPH Peter MacCallum Cancer Centre, Melbourne
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
University of Groningen
 University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors: