Prognostic Diagnosis for HR+/HER2 Early Breast Cancer Patients Based on the Algorithm through the Gene Expression Signature
|
|
|
- Beverly Hutchinson
- 6 years ago
- Views:
Transcription



, The")
1 Prognostic Diagnosis for HR+/HER2 Early Breast Cancer Patients Based on the Algorithm through the Gene Expression Signature Young Kee Shin, M.D., Ph.D. Seoul National University College of Pharmacy N BIO (Institutes of Entrepreneurial BioConvergence), The center for Anti cancer Companion Diagnostics LOGONE Bio Convergence Research Foundation
2 Introduction To make an optimal treatment decision for early state breast cancer, it is important to identify risk of recurrence. Current clinicopathological parameters alone have limited predictive or prognostic value for recurrence risk in patients with early breast cancer. Gene expression based approaches provide significant prognostic or predictive information with respect to breast cancer.several commercial assays based on expression of multiple genes in frozen or FFPE samples have been developed Oncotype DX, PAM50, MammaPrint, and EndoPredict. However, none of the available assays provide a clear answer about prognostic information in HR+/HER2 early breast cancer because these assays do not differentiate patients with HR+/HER2 early breast cancer. There is an urgent clinical need to identify novel prognostic markers to provide a clear answer about prognostic value in HR+/HER2 early breast cancer. Here, we developed and validated a new prognostic model for predicting the risk of distant metastasis in patients with pn0 N1 HR+/HER2 breast cancer treated with hormone therapy alone
3 GenesWell BCT Overview
4 GenesWell BCT : Overview GenesWell BCT is a qrt PCR based in vitro diagnostic assay using RNA extracted from FFPE (Formalin Fixed Paraffin Embedded) samples of breast tumor tissues. The test uses gene expression data of 6 prognostic genes, 3 reference genes, and 3 breast cancer related genes weighted together with 2 clinical variables to generate BCT score through Algorithm, to assess a patient s risk of distant recurrence within 10 years by using. GenesWell BCT Report Form BCT Score Result High Risk 7 Probability of Distant Metastasis Within 10 years 100% 80% 60% 40% 20% 0% Low Risk High Risk BCT Score

 GENCURIX Automated Prognosis")






![[Breast Cancer] Prognosis Diagnostics Kit [Lung & Colorectal Cancer]](/docs-images/75/72675826/images/5-8.jpg "Companion Diagnostics Kit Providing the result of diagnostic analysis")
5 GenesWell BCT : Competitive Advantage AQS Key technology of GenesWell BCT is customized and fully automated AQS (Automatic Quantification System) using FFPE Sample. Tissue Preparation System (TPS, SEIMENS) GENCURIX Automated Prognosis Diagnostic System (AQS: Automated Quantification System) 1 AQS Unit: 1TPS, 1ADS, 1RT PCR : 1 AQS Unit Capacity 24,000 Tests/year(96 tests/day) by 3 researchers ( 8,000 tests/researcher) : Superior efficiency than competitors Genomic Health: Manual method 115,000 tests/year by 144 researchers (800 tests/researcher) Great consistency by Automated System & expandability Price competitiveness due to mass processing with little manpower A fully automated solution for extraction of nucleic acids from FFPE as the first step MFD IVD approved Automatic Dispense System (ADS, Custom made by HAMILTON) GenesWell TM Diagnostic Kits Gene Amplifying & Analysis (LightCycler480 II, Roche) Custom made Automated Dispense System (ADS) MFDS IVD approved Probe/Primer Pre coated GenesWell Brand Kits: [Breast Cancer] Prognosis Diagnostics Kit [Lung & Colorectal Cancer] Companion Diagnostics Kit Providing the result of diagnostic analysis to clinical field using GENCURIX s own algorithm : Applying to diagnostic service MFDS IVD approved

6 GenesWell BCT : Request & Result forms
7 GenesWell BCT Developmental History
8 Developmental history of GenesWell TM BCT Identification of Novel reference genes 1) Biomarker discovery for prognostic diagnosis of breast cancer 2 3) Singapore Joint Grant Clinical Validation (AMC) 4) MFDS class III approval* Discovery data set (SMC+AMC) Algorithm design Development of GeneWell TM BCT Clinical validation Analytical validation 1) Kwon, Mi Jeong, et al. "Identification of novel reference genes using multiplatform expression data and their validation for quantitative gene expression analysis." PloS one 4.7 (2009): e ) Oh, Ensel, et al. "A prognostic model for lymph node negative breast cancer patients based on the integration of proliferation and immunity." Breast cancer research and treatment (2012): ) Han, Jinil et al. MMP11 and CD2 as Novel Prognostic Factors in Hormone Receptor Negative, HER2 Positive Breast Cancer. Breast cancer research and treatment (2017) (Accepted) 4) Gong, Gyungyub, et al. "A new molecular prognos c score for predic ng the risk of distant metastasis in pa ents with HR+/HER2 early breast cancer." Scientific Reports 7 (2017): *Class III: Critical impact for diagnostic and treatment decision

9 Identification of Novel Reference Genes Normalization of mrna levels using endogenous reference genes is critical for an accurate comparison of gene expression between different samples. Despite the popularity of traditional endogenous reference genes such as GAPDH and ACTB, their expression variability in different tissues or disease status has been reported. Therefore, novel reference genes were needed for accurate measurement in quantitative methods. Biomarker I Reference Gene (House keeping gene) β Actin, GAPDH etc Gene expression ratio in Cancer cell Biomarker II Gene expression ratio in Normal cell
 were selected to normalize expression levels of prognostic genes High expression stability in FFPE tissues, frozen tissues and cell lines Lower expression levels")
10 Identification of Novel Reference Genes 13 novel endogenous reference genes (nergs) were selected using human gene expression data from different platforms including EST, SAGE, and microarray Among them, 3 ERGs (CTBP1, CUL1, UBQLN1) were selected to normalize expression levels of prognostic genes High expression stability in FFPE tissues, frozen tissues and cell lines Lower expression levels than those of traditional endogenous reference genes <The mrna levels of tergs and 13 nergs in Cp values> Low expression High expression Red: traditional ERGs GAPDH, ACTB, B2M, PPIA, HPRT1, HMBS, TBP Blue: novel ERGs ZNF207, OAZ1, LUC7L2, CTBP1, TRIM27, GPBP1, UBQLN1, ARL8B, PAPOLA, CUL1, DIMT1L, FBXW2, SPG21 PLoS One Jul 7;4(7):e6162. Identification of novel reference genes using multiplatform expression data and their validation for quantitativegene expression analysis.
11 Novel Prognostic Genes in GenesWell BCT Prognostic genes of GenesWell TM BCT were selected to show clear difference of distant metastasis free survival between high risk group and low risk group through large scale analysis of early breast cancer patients. 6 prognostic genes Gene Group Gene Symbol Full name GO terms (biological process) UBE2C ubiquitin conjugating enzyme E2C cell division; mitotic cell cycle; mitotic spindle assembly checkp oint TOP2A topoisomerase (DNA) II alpha DNA topological change; mitotic cell cycle Proliferation RRM2 ribonucleotide reductase M2 G1/S transition of mitotic cell cycle; mitotic cell cycle FOXM1 forkhead box M1 G2/M transition of mitotic cell cycle; mitotic cell cycle MKI67 marker of proliferation Ki 67 DNA metabolic process; cell proliferation Immune Response BTN3A2 butyrophilin, subfamily 3, member A2 T cell mediated immunity; interferon gamma secretion
12 dataset summary GEO number Publi catio n Total cases # of N- Survival type Median follow-up time(yr) Sample sources Date of diagnosis Treatment Discovery data set GSE2034 [4] Distant meta 7.17 Erasmus medical center, the Netherlands 1980 ~ 1995 No systemic adjuvant therapy GSE6532 (1) [8,37] Distant meta 5.99 John Radcliffe Hospital, UK Guys Hospital, UK Uppsala Univ. Hospital, Sweden 1987~ 1989 tamoxifen only GSE7390 [13] Distant meta Institut Gustaye Roussy, France Karolinska Institute, Sweden Guys Hospital, UK John Radcliffe Hospital, UK Centre Rene Huguenin, France 1980~1998 No systematic adjuvant therapy GSE11121 [32] Distant meta 7.54 Johannes Guteberg Univ., Germany 1988 ~ 1998 No systematic adjuvant therapy GSE Distant meta 7.08 Ljubljana, Slovenia National Cancer Institute, Italy Technische Universitaet Muenchen, Germany Cleveland Clinic Foundation, US 1981 ~ 2000 tamoxifen only Validation data set 1 GSE1456 [9] GSE3494 [10] few Overall 7.05 Karolinska Hospital, Sweden 1994~ 1996 Tamoxifen + chemotherapy (104) Overall Uppsala Univ. Hospital, Sweden 1987~ 1989 For all node positive patients, chemotherapy or tamoxifen Validation data set 2 van t Veer et al Distant meta 6.61 Netherlands Cancer Institute, the Netherlands 1984~ 1995 node positive patients -Chemotherapy only (90) - tamoxifen only (20) - both (20) Validation data set3 GSE6532 (2) Distant meta 8.98 Guys Hospital, UK 1980~ all tamoxifen only
13 A Figure 1 Data preparation 7 independent data sets (1557 cases) Remove duplicated cases 1371 unique cases Preprocessing : RMA (.CEL) Normalized 1371 cases B Select differentially expressed genes (SAM) Define good outcome and poor outcome Good : > 10yrs distant-meta free Poor : < 5yrs develop distant-meta ER- Good : 71 samples Poor : 71 samples Good.up : 226 genes Poor.up : 23 genes (FDR < 0.1) 1104 samples Lymph node negative No chemotherapy Good : 281 samples Poor : 217 samples Pool of candidate genes (1019 unique genes) ER+ Good : 210 samples Poor : 146 samples Select differentially expressed genes (SAM) Good.up : 625 genes Poor.up : 247 genes (FDR = 0.000) Mining of a prognostic gene signature for early breast cancer patients Determine ER status with ESR1 expression levels (ER+ or ER-) Identify expression patterns K-means clustering (by genes) Visualization by TreeView ER+ : 1084 cases ER- : 287 cases Identify 2 distinct expression patterns Discovery 1104 cases (5 data sets) Validation set cases (2 data sets) Validation set cases Validation set cases Proliferation (61 genes) GO analysis (by pattern) Fold change IQR Average expression Immune response (93 genes) prognostic genes Proliferation : 8 genes Immune resp. : 8 genes
14 Method(2) survival data Type Status Total Survival time (yr) min 1Q 2Q 3Q max Dist. meta Yes (total 851) no relapse Yes (total 369) No overall Dead (total 267) alive Distant meta Relapse 74.0% 6.5% Poor Good Good Overall
 Immune response (i-genes) low high G1 G2 G3 T1 T2 T3 N- N+ ER- ER+ No data Distant meta within 5")
15 p3 ER- Expression pattern of proliferation and immune response ER+ p2 High (p3) Intermediate (p2) Low (p1) proliferation Proliferation (p-genes) Immune response (i-genes) low high G1 G2 G3 T1 T2 T3 N- N+ ER- ER+ No data Distant meta within 5 yrs
16 symbol name location p-genes (proliferationrelated genes) UBE2C ubiquitin-conjugating enzyme E2C 20q13.12 ZWINT ZW10 interactor 10q21-q22 CKS2 CDC28 protein kinase regulatory subunit 2 9q22 RACGAP1 Rac GTPase activating protein 1 12q13 PRC1 protein regulator of cytokinesis 1 15q26.1 CCNB2 cyclin B2 15q21.3 PTTG1 pituitary tumor-transforming 1 5q35.1 CDC20 cell division cycle 20 homolog (S. cerevisiae) 1p34.1 i-genes (immune responserelated genes) CXCL13 chemokine (C-X-C motif) ligand 13 4q21 IGHM immunoglobulin heavy constant mu 14q32.32-q32.33 TRBC1 T cell receptor beta constant 1 7q34 GZMB granzyme B (granzyme 2, cytotoxic T-lymphocyteassociated 14q11.2 serine esterase 1) UBD ubiquitin D 6p21.3 LCP1 lymphocyte cytosolic protein 1 (L-plastin) 13q14.3 BTN3A3 butyrophilin, subfamily 3, member A3 6p22.1 STAT1 signal transducer and activator of transcription 1, 91kDa 2q32.2-q32.3
17 A KM survival curves of p-genes ER+ Proliferation (p-genes) ER- Proliferation (p-genes) Figure 4-1 Survival Probability Low (p1) Intermediate (p2) High (p3) HR (intermed/low) : 2.44 ( ) *** HR (high/low) : 5.82 ( ) *** 10 Low (p1) Intermediate (p2) High (p3) HR (intermed/low) : 5.03 ( ) HR (high/low) : 4.54 ( ) Time (yr) B KM survival curves of i-genes ER+ Immune response (i-genes) ER- Immune response (i-genes) Low (i1) Intermediate (i2) High (i3) HR (intermed/high) : 3.31 ( ) *** HR (low/high) : 4.54 ( ) *** HR (intermed/high) : 1.74 ( ) HR (low/high) : 2.82 ( ) **
18 Validation 1 (Agilent Hu25K) distant meta ER+ 70 genes p+i Hazard Ratio : 4.92 Hazard Ratio : 3.62 ER- 70 genes p+i Hazard Ratio : 0.93 Hazard Ratio : 2.16
19 Validation 2 (Affy U133A) overall survival ER+ ER Hazard Ratio : 4.5 Hazard Ratio : 1.48 Validation 3 (Affy U133Plus2) distant meta ER Hazard Ratio : 3.99
 684 breast cancer cases were collected from 3 independent microarray data sets i) All the cases were LN, and none of them received tamoxifen and adjuvant chemotherapy after surgery.")
 C) A total of 384 genes showing a significant differential expression between two clinical outcome (good/poor) groups were selected as candidate prognostic genes i) Good Up: 159 genes ii) Poor")
20 Discovery of Novel Prognostic Genes 384 candidate genes 30 candidate genes 16 candidate genes 6 prognostic genes Microarray dataset qrt PCR of 30 genes qrt PCR of 16 genes GenesWell BCT A) B) C) D) A) 684 breast cancer cases were collected from 3 independent microarray data sets i) All the cases were LN, and none of them received tamoxifen and adjuvant chemotherapy after surgery. B) According to the distribution of the DMFS, 212 cases were assigned to the good outcome group (no DM for more than 10 years), and 159 cases were assigned to the poor outcome group (DM within 5 years) C) A total of 384 genes showing a significant differential expression between two clinical outcome (good/poor) groups were selected as candidate prognostic genes i) Good Up: 159 genes ii) Poor Up: 225 genes D) The candidate genes were classified into two functional categories proliferation and immune response Breast cancer research and treatment, 132(2), A prognostic model for lymph node negative breast cancer patients based on the integration of proliferation and immunity.
21 Discovery of Novel Prognostic Genes 384 candidate genes identified based on public gene expression microarray datasets 30 candidate genes 16 candidate genes 6 prognostic genes High correlation with either proliferation or immune response High expression variability between samples (large interquartile range) High mean expression values qrt PCR of 30 genes in paired FFPE and frozen tissues from the same patients High expression correlation between FFPE and frozen tissues based on qrt PCR qrt PCR of 16 genes in breast cancer FFPE tissues Univariate analysis of 16 genes for DMFS according to subtypes of breast cancer Significant or marginally significant associated with distant metastasis in LN, HR+/HER2 breast cancer
22 Discovery of Novel Prognostic Genes 384 candidate genes 30 candidate genes 16 candidate genes 6 prognostic genes Microarray dataset qrt PCR of 30 genes qrt PCR of 16 genes GenesWell BCT qrt PCR of 30 genes in paired FFPE and frozen tissues from the same patients 16 candidate genes: High expression correlation between FFPE and frozen tissues based on qrt PCR
23 Discovery of Novel Prognostic Genes 384 candidate genes 30 candidate genes 16 prognostic genes 6 prognostic genes Microarray dataset qrt PCR of 30 genes qrt PCR of 16 genes qrt PCR of 16 genes in breast cancer FFPE tissues (n=819) Univariate analysis of 16 genes for DMFS according to subtypes of breast cancer GenesWell BCT All HR+/HER2 HR+/HER2+ HR /HER2+ TNBC HR 95% CI P value HR 95% CI P value HR 95% CI P value HR 95% CI P value HR 95% CI P value No. of patients (No. of events) 421 (64) 202 (29) 45 (7) 58 (12) 116 (16) p genes AURKA CCNB FOXM MKI MMP PTTG RACGAP RRM TOP2A UBE2C i genes BTN3A CCL CD CD HLADPA TRBC Breast cancer related genes ESR PGR ERBB Prognostic genes: Significant or marginally significant associated with distant metastasis in LN, HR+/HER2 breast cancer Breast cancer research and treatment (accepted). MMP11 and CD2 as Novel Prognostic Factors in Hormone Receptor Negative, HER2 Positive Breast Cancer
24 Development of Prognostic Model 384 candidate genes 30 candidate genes 16 prognostic genes 6 prognostic genes Microarray dataset qrt PCR of 30 genes qrt PCR of 16 genes GenesWell BCT Scientific Reports (accepted). A new molecular prognos c score for predic ng the risk of distant metastasis in pa ents with HR+/HER2 early breast cancer
25 Development of Prognostic Model Two clinical variables (pn status and tumor size) were identified as independent negative prognostic factors for distant metastasis in HR+/HER2 breast cancer patients. Univariate analysis Multivariate analysis HR 95% CI p value HR 95% CI p value Age pn Pathologic Stage I II Histologic Grade Tumor Size < NPI Abbreviations: HR, hazard ratio; CI, confidence interval; pn, pathological nodal status; NPI, Nottingham prognostic index; HRs with P values of less than 0.05 are marked in bold.
26 Development of Prognostic Model A new molecular predictor of distant metastasis (BCT Score) was developed based on the combination of six prognostic genes and two clinical variables. BCT Score = (0.63 Ct_UBE2C) + (0.32 Ct_TOP2A) + (0.13 Ct_RRM2) + (0.02 Ct_FOXM1) + (0.04 Ct_MKI67) (0.42 Ct_BTN3A2) + (0.89 Tumor_size) + (1.22 pn) 5 proliferation related genes 1 immune response related gene 2 clinical variables Higher values of the BCT score indicate a higher risk of distant recurrence. A cutoff BCT score value to distinguish patients with low and high risk for distant metastasis was set to 4, which maximized sum of sensitivity and specificity. Category BCT Score (BS, 0 10) Low risk BS<4 High risk BS 4
27 GenesWell BCT Clinical Performance
28 Characteristics of the patients Discovery cohort Validation cohort Hormone therapy alone (A) Hormone therapy alone (B) Hormone therapy plus che motherapy (C) No. of patient s (n=174) (n=222) (n=510) % No. of patient s % No. of patient s % P value betw een A and B P value betw een B and C DMFS rate at 10 years 92.0% (87.9%-96.3%) 92.2% (88.0%-96.6%) 84.7% (81.4%-88.2%) Median age (range), years ( ) ( ) ( ) c c Age, years a <0.001 a < % % % % % % Menopausal status a a Pre % % % Post % % % NA % % % pn a <0.001 a % % % % % % Tumor size, cm b <0.001 b % % % % % % > % % % Pathologic stage a <0.001 a IA % % % IIA % % % IIB % % % Histologic grade a a % % % % % % % % % NPI a <0.001 a % % % % % % % % %
29 Probabilities of DMFS The Kaplan Meier survival curve showed a statistically significant difference in DMFS between the low risk and high risk groups distinguished by the BCT score (p values<0.001). <Discovery set (n=174)> Samsung Medical Center & Asan Medical Center <Validation set (n=222)> Asan Medical Center Low risk: 97.1% Low risk: 96.2% P value < P value < High risk: 73.7% High risk Low risk High risk: 60.3% High risk Low risk Product Reference High Inter Low Low High Oncotype Dx Paik (2004) 69.5% 85.7% 93.2% 23.7% Prosigna 510(k) 84.3% 90.4% 96.6% 12.3% EndoPredict Filipits (2011) 72.0% 96.0% 24.0% 78.0% 96.0% 18.0% Discovery 60.3% 97.1% 36.8% GenesWell TM BCT Validation 73.7% 96.2% 22.5% Total 68.0% 96.9% 28.9%
30 Probabilities of DMFS (Early/Late stage) Discovery set Early stage ( 5 years) Late stage (>5 years) Low risk: 97.9% Low risk: 99.2% High risk: 85.7% High risk: 70.3% High risk Low risk P <0.001 High risk Low risk P <0.001 Validation set Low risk: 98.9% Low risk: 97.3% High risk: 85.1% High risk: 86.5% High risk High risk Low risk P <0.001 Low risk P <0.026
31 Probabilities of DFS The Kaplan Meier survival curve showed a statistically significant difference in DFS between the low risk and high risk groups distinguished by the BCT score (p values<0.001). <Discovery set (n=174)> Samsung Medical Center & Asan Medical Center <Validation set (n=222)> Asan Medical Center Low risk: 97.2% Low risk: 94.0% P value < High risk Low risk High risk: 53.9% P value < High risk Low risk High risk: 63.9%
32 Probabilities of OS The Kaplan Meier survival curve showed a statistically significant difference in OS between the low risk and high risk groups distinguished by the BCT score (p values<0.001). <Discovery set (n=174)> Samsung Medical Center & Asan Medical Center <Validation set (n=222)> Asan Medical Center Low risk: 96.1% Low risk: 98.9% High risk: 77.0% P value < High risk Low risk High risk: 63.4% P value < High risk Low risk


33 Multivariate analysis of the BCT score and clinicopathological parameters Multivariate analysis revealed that the BCT score was independently associated with distant metastasis

34 Comparison of prognostic performance BCT score showed the best performance in predicting the risk of distant metastasis with the highest C index. <Discovery Set> <Validation Set> The BCT score provides more significant prognostic information about risk ofdistantmetastasis than clinical variables and established prognostic models based on clinicopathological parameters.
35 Performance of the BCT score in chemotherapy treated patients A significant difference in 10 year distant metastasis rates between the high and low risk groups <Validation set (n=510)> Asan Medical Center & Samsung Medical Center Low risk: 90.7% High risk: 78.2% High-risk Low-risk P <0.001 BCT score can discriminate patients at high risk and low risk of distant metastasis after chemotherapy treatment.

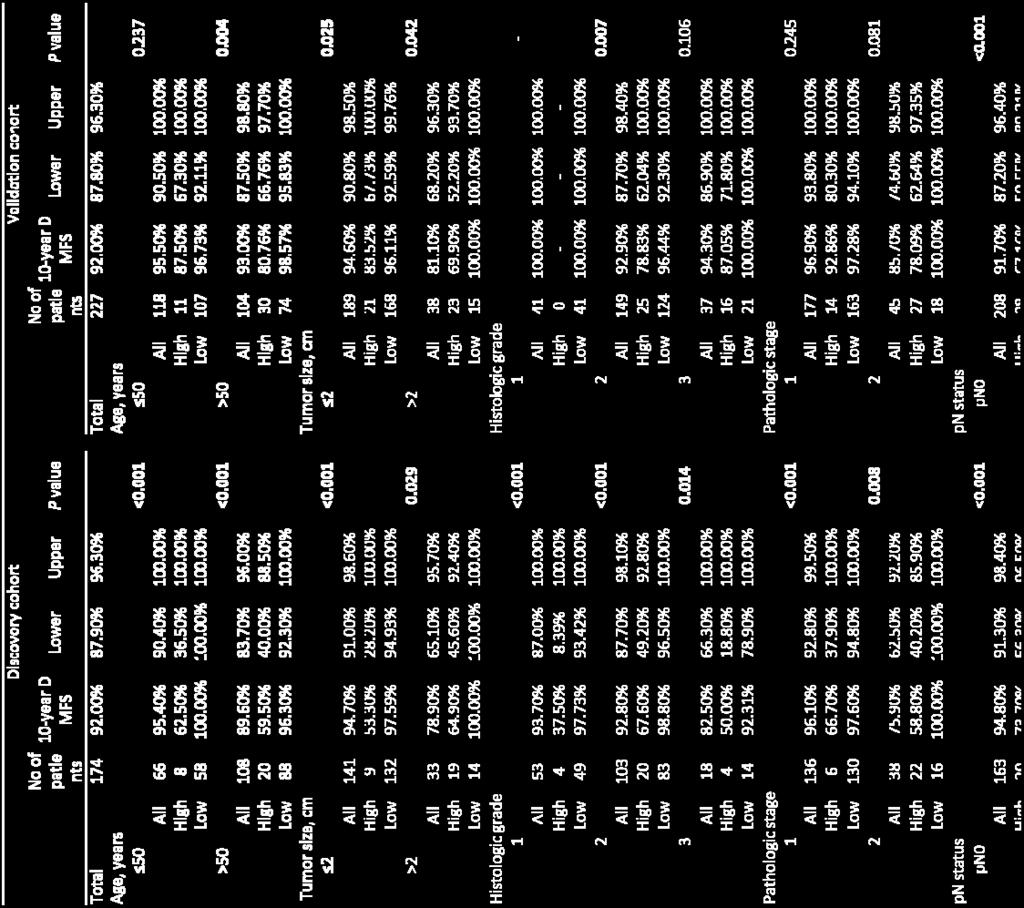


36 Risk of Distant Metastasis in subgroups
37 Commercially available multigene expression signatures in breast cancer

 HER2( ) Ready to launch 2004 2004 2013 2011 Centralization Yes Yes Yes Yes No FDA Approval 510k pre sub MFDS")
 ncounter (Liquid hybridization)")
38 Available multi gene expression signatures Product GenesWell BCT Oncotype DX MammaPrint Prosigna Endopredict Image Manufacturer Number of Genes Sample Type FFPE FFPE Fresh / FFPE FFPE FFPE Target patient Time to Launch Node(+/ ) ER/PR(+) HER2( ) Node( /+) ER(+) HER2( ) Node( ) ER(+/ ) HER2(+/ ) Node( /+) ER/PR(+) Node( /+) ER(+) HER2( ) Ready to launch Centralization Yes Yes Yes Yes No FDA Approval 510k pre sub MFDS approval CLIA 510K 510K N/A Service price $3,000 $4,510 $4,200 $3,500 $3,500 Turnaround Time Ground Technology 1 week 2weeks 2weeks 2~3weeks 1week qrt PCR qrt PCR Microarray (Solid hybridization) ncounter (Liquid hybridization) qrt PCR

 if 0 RS U 100 RS=100 if RS U >100 NSABP B 14 LN, ER+ breast cancer retrospective result NSABP B")
39 Oncotype DX RS U = x HER2 Group Score 0.34 x ER Group Score x Proliferation Group Score x Invasion Group Score x CD x GSTM X BAG1 RS=0 if RS U <0 RS=20 x (RS U 6.7) if 0 RS U 100 RS=100 if RS U >100 NSABP B 14 LN, ER+ breast cancer retrospective result NSABP B 20 LN, ER+ breast cancer retrospective result Low risk High risk Paik et al., 2006 Paik et al., 2004
 To confirm that patients with a low RS (<11) had excellent outcomes with hormonal therapy")

40 Oncotype DX Major clinical trials TAILORx trial HR+/HER2, LN breast cancer RxPONDER trial HR+/HER2, LN+ (1 3) breast cancer To determine in a randomized trial whether chemotherapy impacted clinical outcomes in patients with a mid range RS (11~25) To confirm that patients with a low RS (<11) had excellent outcomes with hormonal therapy alone To determine the effect of the addition of chemotherapy to hormonal therapy in patients with Node+ breast cancer who have RS 25 Patients with RS<11: very low rates of recurrence at 5 years with endocrine therapy alone Sparano et al., 2015 Reference cancer.oncotypedx.com/en US/Professional Invasive/Resources/ClinicalTrials
 k062694 RASTER trial ct1 3, N0M0, chemo+nonchemo van t Veer et al., 2010 Drukker et al.")
41 MammaPrint <Algorithm Development> TRNASBIG trial LN, no adjuvant therapy, size 5cm Buyse et al., (K) k RASTER trial ct1 3, N0M0, chemo+nonchemo van t Veer et al., 2010 Drukker et al., 2013

 was achieved")


42 MammaPrint Prospective trial clow/glow clow/ghigh chigh/glow chigh/ghigh Chemo? Yes No Chemo? Yes No Lower boundary of the 95% C.I.>92% => Primayr object(dmfs rate>92%) was achieved The results from the primary test showed MammaPrint Low Risk patients had a 94.7% 5 year Distant Metastasis Free Survival (DMFS) without chemotherapy, even in presence of high risk clinical factors. Cardoso et al., 2016

 Buyse TRANSBIG (2013) Drukker RASTER (2016) Cardoso MINDACT (2010) Ishitobi (2011) Na 5 European")
43 MammaPrint Different results in Asian patients 100.0% 90.0% 80.0% 70.0% 60.0% 50.0% 40.0% 30.0% 63.2% 36.8% High risk Low risk 44.1% 55.9% 35.8% 64.2% 80.4% 86.1% Ethnic difference? age standardised rate per 100, % 10.0% 19.6% 13.9% 0.0% (2006) Buyse TRANSBIG (2013) Drukker RASTER (2016) Cardoso MINDACT (2010) Ishitobi (2011) Na 5 European centers Netherlands 9 European countries Japan Korea <Trends in incident from female breast cancer >
44 MammaPrint Different results in Asian patients Clinical outcomes of breast cancer patients according to intrinsic subtypes in Korea % 95.00% 35 years years >50 years % 95.00% 35 years years >50 years 90.00% 90.00% 85.00% 85.00% 80.00% 80.00% 75.00% 75.00% 70.00% 70.00% 65.00% 65.00% 60.00% 60.00% HR+/HER2 HR+/HER2+ HR /HER2+ TNBC HR+/HER2 HR+/HER2+ HR /HER2+ TNBC 5 year Recurrence Free Survival Rate (%) 5 year Overall Survival Rate (%) Park et al., 2015

 A ROR score was")
45 Prosigna ROR (risk of relapse): a risk score based on correlation to subtypes The Prosigna Score is a numerical value on a 0 to 100 scale that correlates with the probability of distant recurrence within 10 years The gene expression profile of a patient s tumor is compared with each of the 4 PAM50 prototypical molecular profiles to determine the degree of similarity. The results in combination with a proliferation score and tumor size produce an individualized Prosigna Score Heatmap of the centroid models of subtype (PAM50) A ROR score was assigned to each test case using correlation to subtype alone (1) (ROR-S) or using subtype correlation along with tumor size (2) (ROR-C) Parker et al., 2009


46 Prosigna TransATAC trial Postmenopausal women with ER+ BC ABCSG 8 Postmenopausal women with HR+ BC Dowsett et al, 2013 Gnant et al, 2014
47 EndoPredict EP Score (s) Epclin Score (S clin ) Unscaled EP Score (s u ) s u =0.41 C t (BIRC5) 0.35 C t (RBBP8) C t (UBE2C) 0.31 C t (IL6ST) 0.26 C t (AZGP1) C t (DHCR7) 0.18 C t (MGP) 0.15 C t (STC2) 2.63 Rescaled EP Score (s) s=0, if 1.5 s u <0 s=15, 1.5 s u >15 s=1.5 s u , otherwise Clinical Validation ABCSG 6 Women with ER+/HER2 BC EPclin (S clin ) S clin =0.35 t n s, t (tumor size) 1 ( 1cm), 2(>1 to 2cm), 3 (>2 to 5cm), and 4: >5cm n (nodal status) 1 (negative), 2 (1 3 positive nodes), 3 (4 10 positive nodes), and 4 (>10 positive nodes) s (EP Score) 0 s 15 ABCSG 8 Women with ER+/HER2 BC EP Score EPclin Score EP Score EPclin Score Filipits et al., 2011
48 Clinical Performance of GenesWell BCT FDA Clearance Product Reference Clinical Trial Comparison between Risk groups Hazard ratio for Distant metastasis GenesWell TM BCT Gong et al., 2017 Discovery (AMC+SMC) High risk vs. Low risk ( ) Validation (AMC) High risk vs. Low risk 8.57 ( ) Cleared Prosigna 510(k) K ABCSG 8 Trial (pn0) High risk vs. Low risk 3.96 ( ) Inter. risk vs. Low risk 2.60 ( ) ABCSG 8 Trial (pn1) High risk vs. Low risk 4.22 ( ) Cleared MammaPrint 510(k) k TRANSBIG Trial High risk vs. Low risk 2.32 ( ) Cleared MammaPrint FFPE 510(k) k RASTER Trial High risk vs. Low risk 5.44 ( ) LDT Oncotype DX Dowsett et al., 2010 TransATAC Trial (Node ) TransATAC Trial (Node+) High risk vs. Low risk 5.20 ( ) Inter. risk vs. Low risk 2.60 ( ) High risk vs. Low risk 2.70 ( ) Inter. risk vs. Low risk 1.80 ( ) EndoPredict Filipits et al., 2010 ABCSG 6 Trial High risk vs. Low risk 7.97 ( ) ABCSG 8 Trial High risk vs. Low risk 4.27 ( ) H: High risk, IM: Intermediate risk, L: Low risk
49 GenesWell BCT Comparative Study
 High risk ( 4) Low")
 High risk ( 31)")
50 Histogram of risk scores Low risk (<4) High risk ( 4) Low risk (0~17) Inter. risk (18~30) High risk ( 31) GenesWell BCT Oncotype DX
51 NCC+SMC+AMC BCT Oncotype Inter. Low High ( 18, <3 (RS<18) (RS 31) 1) Sum Low (BS<4) High (BS 4) Sum Oncotype 기본분류 Low: 0~17 Inter.: 18~30 High: 31 or more BCT Oncotype Low (RS<18) High (RS 31) Sum Low (BS<4) High (BS 4) Sum OPA: 78.96% NPA: 80.43% PPA: 68.00% BCT Oncotype Low (RS<18) High (RS 18) Sum Low (BS<4) High (BS 4) Sum OPA: 60.49% NPA: 80.43% PPA: 34.29% BCT Oncotype Low (RS<31) High (RS 31) Sum Low (BS<4) High (BS 4) Sum OPA: 76.85% NPA: 77.59% PPA: 68.00% *OPA: 전체일치율, NPA: 음성일치율 (low risk 일치율 ), PPA: 양성일치율 (high risk 일치율 )
52 NCC+SMC+AMC BCT Low (RS<11) Oncotype Inter. ( 11, 25) High (RS>25) Sum Low (BS<4) High (BS 4) Sum TAILORx study 기준분류 Low: 0~10 Inter.: 11~25 High: more than 25 BCT Oncotype Low (RS<11) High (RS>25) Sum Low (BS<4) High (BS 4) Sum OPA: 76.84% NPA: 87.50% PPA: 61.54% BCT Oncotype Low (RS<11) High (RS 11) Sum Low (BS<4) High (BS 4) Sum OPA: 38.89% NPA: 87.50% PPA: 28.73% BCT Oncotype Low (RS 25) High (RS>25) Sum Low (BS<4) High (BS 4) Sum OPA: 76.85% NPA: 78.95% PPA: 61.54% *OPA: 전체일치율, NPA: 음성일치율 (low risk 일치율 ), PPA: 양성일치율 (high risk 일치율 )
53 OncotypeDX 기존분류기준적용결과비교 Samples Grouping OPA NPA PPA Reference n=34 (EP Score) Oncotype vs EndoPred ict n=34 (EPclin) n=739 (ROR*) Oncotype vs Prosigna n=739 (ROR) Oncotype vs Prosigna n=52 (All) Oncotype vs MammaP n=57 (All) rint Oncotype vs MammaP n=135 (All) rint Oncotype vs MammaP n=86 (All) rint Oncotype vs BCT Oncotype vs BCT Oncotype vs BCT Oncotype vs BCT n=91 (SMC) n=185 (AMC) n= (NCC) n=276 (SMC&AMC &NCC) Low vs Inter-Hi gh Low vs Inter-Hi gh Low vs Inter vs High Low vs Inter vs High Low vs Inter vs High Low-Inter vs Hi gh Low vs Inter-Hi gh Low-Inter vs Hi gh Low vs Inter-Hi gh Low-Inter vs Hi gh Low vs Inter-Hi gh Low-Inter vs Hi gh Low vs Inter-Hi gh Low-Inter vs Hi gh Low vs Inter-Hi gh Low-Inter vs Hi gh Low vs Inter-Hi gh Low-Inter vs Hi gh Low vs Inter-Hi gh 76.47% 60.00% 89.47% Varga, Zsuzsanna, et al. "Comparison of EndoPredict and Oncotype DX test results in 64.70% 73.33% 57.89% hormone receptor positive invasive breast cancer." PloS one 8.3 (2013): e % 72.20% 35.29% Dowsett, Mitch, et al. "Comparison of PAM50 risk of recurrence score with oncotype DX and IHC4 for predicting risk of distant recurrence after endocrine therapy." Journ 66.44% 87.19% 34.15% al of Clinical Oncology (2013): JCO % 59.46% 33.33% Alvarado, Michael D., et al. "A prospective comparison of the 21-gene recurrence sco re and the pam50-based prosigna in estrogen receptor-positive early-stage breast c ancer." Advances in therapy (2015): % 61.82% 50.00% Poulet, Bruno, et al. "Risk classification of early stage breast cancer as assessed by M ammaprint and Oncotype DX genomic assays." San Antonio Breast Cancer Symposiu 61.40% 69.70% 50.00% m (SABCS) % 63.55% 85.71% Shivers, S. C., et al. "Abstract P : Direct comparison of risk classification betwe en MammaPrint, Oncotype DX and MammoStrat assays in patients with early s 68.89% 70.83% 66.67% tage breast cancer." (2013): P % 61.04% 77.78% Maroun, Ralph, et al. "A head-to-head comparison of Mammaprint and Oncotype Dx 60.47% 64.71% 54.29% : A McGill University Health Center Experience." (2015): % 79.55% 33.33% 64.84% 81.25% 25.93% 74.05% 74.40% 70.59% 60.00% 78.57% 39.08% 85.42% 86.05% 80.00% 54.17% 86.36% 26.91% 76.85% 77.59% 68.00% 60.49% 80.43% 34.29%
54 Correlation between risk score and Ki 67 SMC 결과 Low risk High risk <10 10 & <20 20 Ki 67 <10 10 & <20 20 Ki 67 Low risk Inter. risk High risk
55 Prediction of chemotherapy response in HR+/HER2 breast cancer patients




56 Response to medical therapy Endocrine ER % HER % TN 15% Chemotherapy Breast cancer Molecular subtypes Response to therapy
57 Biomarkers for adjuvant systemic therapy in early breast cancer Use of Biomarkers to Guide Decisions on Adjuvant Systemic Therapy for Women With Early Stage Invasive Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline Product Target Guide Type Oncotype DX EndoPredict MammaPrint PAM50 Breast Cancer Index Mammostrat IHC4 Evidence quality Strength of recommendation HR+,HER2- (node negative) use to guide decisions on adjuvant systemic chemotherapy Evidence-based High Strong HR+,HER2- (node positive) should not use the Oncotype DX to guide decisions on adjuvant systemic chemotherapy Evidence-based intermediate Moderate HER2+ or TNBC should not use the Oncotype DX to guide decisions on adjuvant systemic therapy informal consensus insufficient Strong HR+,HER2- (node negative) use EndoPredict to guide decisions on adjuvant systemic chemotherapy Evidence-based intermediate Moderate HR+,HER2- (node positive) should not use the EndoPredict to guide decisions on adjuvant systemic chemotherapy Evidence-based insufficient moderate HER2+ or TNBC should not use the EndoPredict to guide decisions on adjuvant systemic therapy informal consensus insufficient Strong HR+,HER2- (LN+ or LN-) should not use the MammaPrint to guide decisions on adjuvant systemic chemotherapy Evidence-based intermediate moderate HER2+ not use to guide decisions on adjuvant systemic therapy informal consensus low moderate TNBC not use to guide decisions on adjuvant systemic therapy informal consensus insufficient Strong HR+,HER2- (node negative) use the PAM50 to guide decisions on adjuvant systemic therapy Evidence-based High Strong HR+,HER2- (node positive) not use PAM50 to guide decisions on adjuvant systemic therapy Evidence-based intermediate Moderate HER2+ not use PAM50 to guide decisions on adjuvant systemic therapy informal consensus insufficient Strong TNBC not use PAM50 to guide decisions on adjuvant systemic therapy informal consensus insufficient Strong HR+,HER2- (node negative) use the Breast cancer Index to guide decisions on adjuvant systemic therapy Evidence-based intermediate Moderate HR+,HER2- (node positive) not use the Breast cancer Index to guide dicisions on adjuvant systemic therapy informal consensus insufficient Strong HER2+ not use the Breast cancer Index to guide dicisions on adjuvant systemic therapy informal consensus insufficient Strong HR+,HER2- (LN+ or LN-) not use the Mammostrat to guide decisions on adjuvant systemic therapy Evidence-based intermediate Moderate HER2+ not use the Mammostrat to guide decisions on adjuvant systemic therapy informal consensus insufficient Strong HR+,HER2- (LN+ or LN-) not use IHC4 to guide decisions on adjuvant systemic chemotherapy Evidence-based intermediate Moderate HER2+ or TNBC not use IHC4 to guide decisions on adjuvant systemic therapy informal consensus insufficient Strong Reference: +Therapy+in+Early+Breast+Cancer
58 Systemic adjuvant treatment HR+/HER2 disease ff Other rprognostic multigene assays may be considered to help assess risk of recurrence but have not been validated to predict response to chemotherapy.
59 Predictive information for HR+/HER2 breast cancer patients Assays such as Oncotype DX or Prosigna target ER+ breast cancer but do not discriminate between ER+/HER2 and ER+/HER2+ subtypes in all published validation results. Although both are subtypes of ER+ breast cancer, they have different prognoses after hormone therapy and show different responses to adjuvant chemotherapy. Oncotype DX NSABP B 20 Study Patients with LN & ER+ SWOG 8814 Study Patients with LN+ & ER+ Paik et al., Albain et al., 2010.
60 Predictive information for HR+/HER2 breast cancer patients Assays such as Oncotype DX or Prosigna target ER+ breast cancer but do not discriminate between ER+/HER2 and ER+/HER2+ subtypes in all published validation results. Although both are subtypes of ER+ breast cancer, they have different prognoses after hormone therapy and show different responses to adjuvant chemotherapy. MammaPrint Knauer et al., 2010.
61 GenesWell BCT: Chemotherapy benefit according to risk groups A GenesWell BCT prognostic signature for LN, HR+/HER2 breast cancer patients in a single center study GenesWell BCT risk All patients; only a 3% absolute CTx benefit Low risk patients; Little to no CTx benefit High risk patients; Large CTx benefit 94.5% 91.9% 96.4% 96.0% 91.9% 26.5% 65.4% P = n DM HTx + CTx HTx P = n DM HTx + CTx 86 3 HTx P = n DM HTx + CTx 57 4 HTx 23 7
 Modified Adjuvant!")

62 GenesWell BCT: Chemotherapy benefit according to risk groups Clinical risk assessment according to modified Adjuvant! Online (LN, HR+/HER2 breast cancer) Modified Adjuvant! Online All patients; only a 3% absolute CTx benefit Clinical low risk; Little to no CTx benefit Clinical high risk; Little CTx benefit 94.5% 91.9% 94.8% 91.2% 96.4% 13.4% 83.0% P = n DM HTx + CTx HTx P = n DM HTx + CTx 50 4 HTx P = n DM HTx + CTx 93 3 HTx 44 6
63 GenesWell BCT Further Study
 Concordance between risk")

64 Further Study 1. Comparative study with Oncotype DX 1) Concordance between risk groups 2) Evaluation of prognostic values 2. Prospective validation study 3. Pro and Retro spective study for young breast cancer 4. Clinical trials for FDA 510(k) clearance




65 Further Studies Prospective validation study Pro and retro spective studies for young breast cancer Prof. Seok Jin Nam Prof. Jeong Eon Lee DCIS study Comparison study between FFPE and core biopsy Prof. Doo Ho Choi Prof. Gyung Yup Gong
66 GenesWell BCT Conclusion
67 Conclusion GenesWell TM BCT was developed to predict the risk of distant metastasis in patients with pn0 1, HR+/HER2 breast cancer and validated in independent cohorts of AMC. The BCT score of GenesWell TM BCT has a prognostic value for late distant metastasis. The BCT score provided better prognostic information about distant metastasis than other prognostic models based on traditional clinicopathological factors. The GenesWell TM BCT may help inform decisions about the need for additional adjuvant therapies in patients with pn0 N1, HR+/HER2 breast cancer.
OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER
 OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER Aleix Prat, MD PhD Medical Oncology Department Hospital Clínic of Barcelona University of Barcelona esmo.org Disclosures Advisory role for
OVERVIEW OF GENE EXPRESSION-BASED TESTS IN EARLY BREAST CANCER Aleix Prat, MD PhD Medical Oncology Department Hospital Clínic of Barcelona University of Barcelona esmo.org Disclosures Advisory role for
Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI
 Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI UOC Oncologia Medica, A.O. Papardo, Messina Dir. Prof. V. Adamo BREAST CANCER Brain Adjuvant Medical Therapies
Profili Genici e Personalizzazione del trattamento adiuvante nel carcinoma mammario G. RICCIARDI UOC Oncologia Medica, A.O. Papardo, Messina Dir. Prof. V. Adamo BREAST CANCER Brain Adjuvant Medical Therapies
Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer
 Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Comparison of prognostic signatures for ER positive breast cancer in TransATAC:
 Comparison of prognostic signatures for ER positive breast cancer in TransATAC: EndoPredict, a high performance test in node negative and node positive disease Ivana Sestak, PhD Centre for Cancer Prevention
Comparison of prognostic signatures for ER positive breast cancer in TransATAC: EndoPredict, a high performance test in node negative and node positive disease Ivana Sestak, PhD Centre for Cancer Prevention
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY
 Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY Methodology The test is based on the reported 50-gene classifier algorithm originally named PAM50 and is performed on the ncounter Dx Analysis System
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY Methodology The test is based on the reported 50-gene classifier algorithm originally named PAM50 and is performed on the ncounter Dx Analysis System
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY
 Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY GENE EXPRESSION PROFILING WITH PROSIGNA What is Prosigna? Prosigna Breast Cancer Prognostic Gene Signature Assay is an FDA-approved assay which provides
Prosigna BREAST CANCER PROGNOSTIC GENE SIGNATURE ASSAY GENE EXPRESSION PROFILING WITH PROSIGNA What is Prosigna? Prosigna Breast Cancer Prognostic Gene Signature Assay is an FDA-approved assay which provides
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
30 years of progress in cancer research
 Breast Cancer Molecular Knowledge Integrated in Clinical Practice Personalized Medicine Laura J. Esserman UCSF Comprehensive Cancer Center Retreat Breast Cancer Management Advances 80-90s 1) Screening
Breast Cancer Molecular Knowledge Integrated in Clinical Practice Personalized Medicine Laura J. Esserman UCSF Comprehensive Cancer Center Retreat Breast Cancer Management Advances 80-90s 1) Screening
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer
 Node Positive Breast Cancer") Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Profili di espressione genica
 Profili di espressione genica Giampaolo Bianchini MD Ospedale San Raffaele, Milan - Italy Gene expression profiles Transcriptomics Gene DNA mrna mirnas Protein metilation Metabolite Genomics Transcriptomics
Profili di espressione genica Giampaolo Bianchini MD Ospedale San Raffaele, Milan - Italy Gene expression profiles Transcriptomics Gene DNA mrna mirnas Protein metilation Metabolite Genomics Transcriptomics
Adjuvant endocrine therapy (essentials in ER positive early breast cancer)
") Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Adjuvant endocrine therapy (essentials in ER positive early breast cancer) Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Experimental Therapeutics Outline Picking optimal adjuvant endocrine
Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension?
 Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension? Ivana Sestak, PhD Centre for Cancer Prevention Wolfson Institute of Preventive Medicine Queen Mary University London
Hormone therapyduration: Can weselectthosepatientswho benefitfromtreatmentextension? Ivana Sestak, PhD Centre for Cancer Prevention Wolfson Institute of Preventive Medicine Queen Mary University London
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Contemporary Classification of Breast Cancer
 Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
Contemporary Classification of Breast Cancer Laura C. Collins, M.D. Vice Chair of Anatomic Pathology Professor of Pathology Beth Israel Deaconess Medical Center and Harvard Medical School Boston, MA Outline
DIAGNOSTICS ASSESSMENT PROGRAMME
 DIAGNOSTICS ASSESSMENT PROGRAMME Evidence overview Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10) This overview summarises the key issues
DIAGNOSTICS ASSESSMENT PROGRAMME Evidence overview Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10) This overview summarises the key issues
RNA preparation from extracted paraffin cores:
 Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Breast cancer classification: beyond the intrinsic molecular subtypes
 Breast cancer classification: beyond the intrinsic molecular subtypes Britta Weigelt, PhD Signal Transduction Laboratory CRUK London Research Institute Summary Breast cancer heterogeneity Molecular classification
Breast cancer classification: beyond the intrinsic molecular subtypes Britta Weigelt, PhD Signal Transduction Laboratory CRUK London Research Institute Summary Breast cancer heterogeneity Molecular classification
The Oncotype DX Assay A Genomic Approach to Breast Cancer
 The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
The Oncotype DX Assay A Genomic Approach to Breast Cancer Pathology: 20 th and 21 st Century Size Age Phenotype Nodal status Protein/Gene Genomic Profiling Prognostic & Predictive Markers Used in Breast
CARCINOMA DELLA MAMMELLA La scelta del trattamento adiuvante: utilità clinica dei tests genomici
 CARCINOMA DELLA MAMMELLA La scelta del trattamento adiuvante: utilità clinica dei tests genomici Dott.ssa Gaia Griguolo DiSCOG-Università di Padova IOV Istituto Oncologico Veneto I.R.C.C.S. Tutor: Prof.
CARCINOMA DELLA MAMMELLA La scelta del trattamento adiuvante: utilità clinica dei tests genomici Dott.ssa Gaia Griguolo DiSCOG-Università di Padova IOV Istituto Oncologico Veneto I.R.C.C.S. Tutor: Prof.
Clinical utility of multigene profiling assays in early-stage breast cancer
 PRACTICE GUIDELINE CLINICAL UTILITY OF MULTIGENE PROFILING ASSAYS, Chang et al. Clinical utility of multigene profiling assays in early-stage breast cancer M.C. Chang md phd,* L.H. Souter phd, S. Kamel-Reid
PRACTICE GUIDELINE CLINICAL UTILITY OF MULTIGENE PROFILING ASSAYS, Chang et al. Clinical utility of multigene profiling assays in early-stage breast cancer M.C. Chang md phd,* L.H. Souter phd, S. Kamel-Reid
A new way of looking at breast cancer tumour biology
 A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
A new way of looking at breast cancer tumour biology Contents Intrinsic subtypes of breast cancer 3 Gene expression assays 3 Basis of the Prosigna test 4 Information provided by Prosigna 5 The accuracy
Rationale For & Design of TAILORx. Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York
 Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Rationale For & Design of TAILORx Joseph A. Sparano, MD Albert Einstein College of Medicine Montefiore-Einstein Cancer Center Bronx, New York Declining Breast Cancer Mortality & Event Rates in Adjuvant
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Breast Cancer Assays of Genetic Expression in Tumor Tissue
 Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/02/2008 Line(s) of Business: Current Effective Date Section: 05/25/2018 Other Miscellaneous
Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/02/2008 Line(s) of Business: Current Effective Date Section: 05/25/2018 Other Miscellaneous
Session thématisée Les Innovations diagnostiques en cancérologie
 10 èmes Journées Scientifiques du Cancéropôle Nord-Ouest 10-12 mai 2017, Deauville Session thématisée Les Innovations diagnostiques en cancérologie Les signatures multigéniques pronostiques dans le cancer
10 èmes Journées Scientifiques du Cancéropôle Nord-Ouest 10-12 mai 2017, Deauville Session thématisée Les Innovations diagnostiques en cancérologie Les signatures multigéniques pronostiques dans le cancer
TABLE OF CONTENTS. Executive Summary The EndoPredict Test Intended Use Population Breast Cancer Clinical Dilemma. Analytical Validity
 Clinical Dossier TABLE OF CONTENTS Executive Summary The EndoPredict Test Intended Use Population Breast Cancer Clinical Dilemma 1 2 3 Analytical Validity 4 Clinical Validity 4 Clinical Utility 7 Medicare
Clinical Dossier TABLE OF CONTENTS Executive Summary The EndoPredict Test Intended Use Population Breast Cancer Clinical Dilemma 1 2 3 Analytical Validity 4 Clinical Validity 4 Clinical Utility 7 Medicare
She counts on your breast cancer expertise at the most vulnerable time of her life.
 HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
HOME She counts on your breast cancer expertise at the most vulnerable time of her life. Empowering the right treatment choice for better patient outcomes. The comprehensive genomic assay experts trust.
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
The Current Status and the Future Prospects of Multigene testing in Europe
 The Current Status and the Future Prospects of Multigene testing in Europe Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam St. Gallen Recommendations 2009 =
The Current Status and the Future Prospects of Multigene testing in Europe Emiel J. Rutgers The Netherlands Cancer Institute Antoni Van Leeuwenhoek Hospital Amsterdam St. Gallen Recommendations 2009 =
Genomic platforms in breast cancer
 Genomic platforms in breast cancer Prof. Miguel Martín Instituto de Investigación Sanitaria Hospital Gregorio Marañón Universidad Complutense Madrid mmartin@geicam.org Disclosure Dr. Martin has received
Genomic platforms in breast cancer Prof. Miguel Martín Instituto de Investigación Sanitaria Hospital Gregorio Marañón Universidad Complutense Madrid mmartin@geicam.org Disclosure Dr. Martin has received
Genomic Profiling of Tumors and Loco-Regional Recurrence
 1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer
 The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
Type: Evidence Based Evidence Quality: High Strength of Recommendation: Strong
 Clinical Question 1: For women with early-stage invasive breast cancer and with known estrogen and progesterone receptor (ER/PgR) and human epidermal growth factor receptor 2 (HER2 status), which other
Clinical Question 1: For women with early-stage invasive breast cancer and with known estrogen and progesterone receptor (ER/PgR) and human epidermal growth factor receptor 2 (HER2 status), which other
MammaPrint, the story of the 70-gene profile
 MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
MammaPrint, the story of the 70-gene profile René Bernards Professor of Molecular Carcinogenesis The Netherlands Cancer Institute Amsterdam Chief Scientific Officer Agendia Amsterdam The breast cancer
MP Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients With Breast Cancer. Related Policies None
 Medical Policy Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients With Breast BCBSA Ref. Policy: 2.04.36 Last Review: 11/15/2018 Effective Date: 02/15/2019 Section:
Medical Policy Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients With Breast BCBSA Ref. Policy: 2.04.36 Last Review: 11/15/2018 Effective Date: 02/15/2019 Section:
Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013
 Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013 Changing Phases claudin low Lum A Lum B Basal Her2 NIH Consensus Development Panel,
Is Gene Expression Profiling the Best Method for Selecting Systemic Therapy in EBC? Norman Wolmark Miami March 8, 2013 Changing Phases claudin low Lum A Lum B Basal Her2 NIH Consensus Development Panel,
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 67 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 67 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN
 GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN Adam Brufsky, MD, PhD Professor of Medicine Associate Chief, Hematology-Oncology Associate Director, Clinical Investigation University
GENOMIC TESTS FOR BREAST CANCER: FACT, MYTH, AND EVERYTHING IN BETWEEN Adam Brufsky, MD, PhD Professor of Medicine Associate Chief, Hematology-Oncology Associate Director, Clinical Investigation University
National Medical Policy
 National Medical Policy Subject: Policy Number: MammaPrint, Prosigna and Other Gene Expression Tests for Breast Cancer NMP520 Effective Date*: May 2013 Updated: June 2017 This National Medical Policy is
National Medical Policy Subject: Policy Number: MammaPrint, Prosigna and Other Gene Expression Tests for Breast Cancer NMP520 Effective Date*: May 2013 Updated: June 2017 This National Medical Policy is
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 55 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 55 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
Molecular in vitro diagnostic test for the quantitative detection of the mrna expression of ERBB2, ESR1, PGR and MKI67 in breast cancer tissue.
 Innovation for your breast cancer diagnostics PGR G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C ERBB2
Innovation for your breast cancer diagnostics PGR G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C G AT C G A A A G A A G T TA G ATA G C G A C ERBB2
Oncotype DX MM /01/2008. HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
 of Service: Office") Oncotype DX Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
Oncotype DX Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 03/01/2014 Section: Other/Miscellaneous Place(s) of Service: Office
Breast Cancer Assays of Genetic Expression in Tumor Tissue
 Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/16/2016
Breast Cancer Assays of Genetic Expression in Tumor Tissue Policy Number: Original Effective Date: MM.12.009 12/01/2008 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/16/2016
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 47 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 47 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10).
.") Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10). Erratum to the EAG Diagnostic Assessment Report Produced by: Sheffield University School of
Tumour profiling tests to guide adjuvant chemotherapy decisions in people with breast cancer (update of DG10). Erratum to the EAG Diagnostic Assessment Report Produced by: Sheffield University School of
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Medical Policy Manual Genetic Testing, Policy No. 42 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Next Review: December 2018 Last Review:
Medical Policy Manual Genetic Testing, Policy No. 42 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Next Review: December 2018 Last Review:
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 54 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Assays of Genetic Expression in Tumor Tissue as a Technique Page 1 of 54 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Assays of Genetic Expression in Tumor Tissue
Reliable Evaluation of Prognostic & Predictive Genomic Tests
 Reliable Evaluation of Prognostic & Predictive Genomic Tests Richard Simon, D.Sc. Chief, Biometric Research Branch National Cancer Institute http://brb.nci.nih.gov Different Kinds of Biomarkers Prognostic
Reliable Evaluation of Prognostic & Predictive Genomic Tests Richard Simon, D.Sc. Chief, Biometric Research Branch National Cancer Institute http://brb.nci.nih.gov Different Kinds of Biomarkers Prognostic
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 1/2019 Origination: 1/2006 Next Review: 9/2019 Policy
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 1/2019 Origination: 1/2006 Next Review: 9/2019 Policy
The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer. California Technology Assessment Forum
 As a Guide for the Management of Early Stage Breast Cancer. California Technology Assessment Forum") TITLE: The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department
TITLE: The 70-Gene Signature (MammaPrint) As a Guide for the Management of Early Stage Breast Cancer AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department
Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón
 Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón Universidad Complutense Madrid The new technologies
Relevancia práctica de la clasificación de subtipos intrínsecos en cáncer de mama Miguel Martín Instituto de Investigación Sanitaria Gregorio Marañón Universidad Complutense Madrid The new technologies
Molecular Characterization of Breast Cancer: The Clinical Significance
 Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
Molecular Characterization of : The Clinical Significance Shahla Masood, M.D. Professor and Chair Department of Pathology and Laboratory Medicine University of Florida College of Medicine-Jacksonville
Section: Genetic Testing Last Reviewed Date: March Policy No: 42 Effective Date: June 1, 2014
 Medical Policy Manual Topic: Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis In Patients With Breast Cancer Date of Origin: October 5, 2004 Section: Genetic Testing Last
Medical Policy Manual Topic: Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis In Patients With Breast Cancer Date of Origin: October 5, 2004 Section: Genetic Testing Last
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 9/2018 Origination: 1/2006 Next Review: 9/2019 Policy
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Policy Number: 2.04.36 Last Review: 9/2018 Origination: 1/2006 Next Review: 9/2019 Policy
Morphological and Molecular Typing of breast Cancer
 Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
Morphological and Molecular Typing of breast Cancer Ian Ellis Molecular Medical Sciences, University of Nottingham Department of Histopathology, Nottingham University Hospitals NHS Trust Histological
TAILORx: Established and Potential Implications for Clinical Practice
 TAILORx: Established and Potential Implications for Clinical Practice Joseph A. Sparano, MD Study Chair, TAILORx Vice-Chair, ECOG-ACRIN Cancer Research Group Hello Healthcare Summit Berlin, Germany March
TAILORx: Established and Potential Implications for Clinical Practice Joseph A. Sparano, MD Study Chair, TAILORx Vice-Chair, ECOG-ACRIN Cancer Research Group Hello Healthcare Summit Berlin, Germany March
Medical Policy. Description. Related Policies. Policy. Effective Date January 1, 2015 Original Policy Date December 1, 2005
 2.04.36 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Section 2.0 Medicine Subsection 2.04 Pathology/Laboratory Effective Date January
2.04.36 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Section 2.0 Medicine Subsection 2.04 Pathology/Laboratory Effective Date January
CME Information LEARNING OBJECTIVES
 CME Information LEARNING OBJECTIVES Evaluate the EndoPredict signature together with a predefined combination of clinicopathologic factors and molecular data as a predictor of late metastases for patients
CME Information LEARNING OBJECTIVES Evaluate the EndoPredict signature together with a predefined combination of clinicopathologic factors and molecular data as a predictor of late metastases for patients
Accepted Manuscript. Molecular Signatures in Breast Cancer. Samir Lal, Amy E McCart Reed, Xavier M de Luca, Peter T Simpson
 Accepted Manuscript Molecular Signatures in Breast Cancer Samir Lal, Amy E McCart Reed, Xavier M de Luca, Peter T Simpson PII: S1046-2023(17)30058-0 DOI: http://dx.doi.org/10.1016/j.ymeth.2017.06.032 Reference:
Accepted Manuscript Molecular Signatures in Breast Cancer Samir Lal, Amy E McCart Reed, Xavier M de Luca, Peter T Simpson PII: S1046-2023(17)30058-0 DOI: http://dx.doi.org/10.1016/j.ymeth.2017.06.032 Reference:
A Prospective Comparison of the 21-Gene Recurrence Score and the PAM50-Based Prosigna in Estrogen Receptor-Positive Early-Stage Breast Cancer
 Adv Ther (2015) 32:1237 1247 DOI 10.1007/s12325-015-0269-2 ORIGINAL RESEARCH A Prospective Comparison of the 21-Gene Recurrence Score and the PAM50-Based Prosigna in Estrogen Receptor-Positive Early-Stage
Adv Ther (2015) 32:1237 1247 DOI 10.1007/s12325-015-0269-2 ORIGINAL RESEARCH A Prospective Comparison of the 21-Gene Recurrence Score and the PAM50-Based Prosigna in Estrogen Receptor-Positive Early-Stage
1 INTRODUCTION REVIEW ARTICLE
 Received: 12 December 2016 Revised: 15 December 2016 Accepted: 15 December 2016 DOI 10.1002/jso.24561 REVIEW ARTICLE Selecting postoperative adjuvant systemic therapy for early stage breast cancer: A critical
Received: 12 December 2016 Revised: 15 December 2016 Accepted: 15 December 2016 DOI 10.1002/jso.24561 REVIEW ARTICLE Selecting postoperative adjuvant systemic therapy for early stage breast cancer: A critical
THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE. Dr Husam Marashi 03/02/2017
 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE Dr Husam Marashi 03/02/2017 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER TODAY S TALK: CENTRE EXPERIENCE
THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER CENTRE EXPERIENCE Dr Husam Marashi 03/02/2017 THE 21-GENE RECURRENCE SCORE: BEATSON WEST OF SCOTLAND CANCER TODAY S TALK: CENTRE EXPERIENCE
Learning Objectives. Financial Disclosure. Breast Cancer Quality Improvement Project with Oncotype DX. Nothing to disclose
 Breast Cancer Quality Improvement Project with Oncotype DX Denise Johnson Miller, MD, FACS Medical Director Breast Surgery Hackensack Meridian Health Legacy Meridian (Jersey Shore University Medical Center,
Breast Cancer Quality Improvement Project with Oncotype DX Denise Johnson Miller, MD, FACS Medical Director Breast Surgery Hackensack Meridian Health Legacy Meridian (Jersey Shore University Medical Center,
Molecular in vitro diagnostic test for the quantitative detection of the mrna expression of ERBB2, ESR1, PGR and MKI67 in breast cancer tissue.
 Innovation for your breast cancer diagnostics Now valid ated on: -Roche cob as z 480 A nalyzer -Roche L ightcycle r 480 II - ABI 750 0 Fast -Versant kpcr Cyc ler PGR ESR1 MKI67 Molecular in vitro diagnostic
Innovation for your breast cancer diagnostics Now valid ated on: -Roche cob as z 480 A nalyzer -Roche L ightcycle r 480 II - ABI 750 0 Fast -Versant kpcr Cyc ler PGR ESR1 MKI67 Molecular in vitro diagnostic
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
Adjuvan Chemotherapy in Breast Cancer
 Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
Biologic Subtypes and Prognos5c Factors. Claudine Isaacs, MD Georgetown University
 Biologic Subtypes and Prognos5c Factors Claudine Isaacs, MD Georgetown University Prognos5c Factor Defini5on Predicts outcome in absence of systemic therapy Thus tell us when (not how) to treat a pa5ent
Biologic Subtypes and Prognos5c Factors Claudine Isaacs, MD Georgetown University Prognos5c Factor Defini5on Predicts outcome in absence of systemic therapy Thus tell us when (not how) to treat a pa5ent
Harmesh Naik, MD. Hope Cancer Clinic
 Harmesh Naik, MD. Hope Cancer Clinic A brief review of adjuvant therapy of breast cancer Summarize selected new developments in adjuvant therapy of breast cancer Discussion is limited to early stage breast
Harmesh Naik, MD. Hope Cancer Clinic A brief review of adjuvant therapy of breast cancer Summarize selected new developments in adjuvant therapy of breast cancer Discussion is limited to early stage breast
Oncotype DX tools User Guide
 Oncotype DX tools User Guide This guide provides an overview of the data and quick access to the Oncotype DX tools Oncotype DX tools offers two quantitative calculator tools that may be used together with
Oncotype DX tools User Guide This guide provides an overview of the data and quick access to the Oncotype DX tools Oncotype DX tools offers two quantitative calculator tools that may be used together with
A breast cancer gene signature for indolent disease
 Breast Cancer Res Treat (2017) 164:461 466 DOI 10.1007/s10549-017-4262-0 EPIDEMIOLOGY A breast cancer gene signature for indolent disease Leonie J. M. J. Delahaye 1 Caroline A. Drukker 2,3 Christa Dreezen
Breast Cancer Res Treat (2017) 164:461 466 DOI 10.1007/s10549-017-4262-0 EPIDEMIOLOGY A breast cancer gene signature for indolent disease Leonie J. M. J. Delahaye 1 Caroline A. Drukker 2,3 Christa Dreezen
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
Development and verification of the PAM50-based Prosigna breast cancer gene signature assay
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2015 Development and verification of the PAM50-based Prosigna breast cancer gene signature assay Jacqueline Snider
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2015 Development and verification of the PAM50-based Prosigna breast cancer gene signature assay Jacqueline Snider
Bradley M Turner MD, MPH, MHA. Assistant Professor University of Rochester Department of Pathology and Laboratory Medicine
 Bradley M Turner MD, MPH, MHA Assistant Professor University of Rochester Department of Pathology and Laboratory Medicine My real job!!! I have nothing to disclose although Oncotype Dx year end revenues
Bradley M Turner MD, MPH, MHA Assistant Professor University of Rochester Department of Pathology and Laboratory Medicine My real job!!! I have nothing to disclose although Oncotype Dx year end revenues
Postoperative Adjuvant Chemotherapies. Stefan Aebi Luzerner Kantonsspital
 Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer
 Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer Hee Jung Kwon, Nuri Jang, Min Hui Park, Young Kyung Bae Department of Pathology, Yeungnam
Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer Hee Jung Kwon, Nuri Jang, Min Hui Park, Young Kyung Bae Department of Pathology, Yeungnam
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: April 15, 2017 Related Policies: None Assays of Genetic Expression in Tumor Tissue as a Technique to Description Laboratory tests have been developed that detect
FEP Medical Policy Manual Effective Date: April 15, 2017 Related Policies: None Assays of Genetic Expression in Tumor Tissue as a Technique to Description Laboratory tests have been developed that detect
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives
 Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
CanAssist-Breast: New test for prediction of risk of recurrence in ER+/Her2- early stage breast cancer patients Manjiri Bakre, Ph.D.
 CanAssist-Breast: New test for prediction of risk of recurrence in ER+/Her2- early stage breast cancer patients Manjiri Bakre, Ph.D. Founder and CEO OncoStem Diagnostics Pvt. Ltd. Treatment Decision: HR+/HER2-
CanAssist-Breast: New test for prediction of risk of recurrence in ER+/Her2- early stage breast cancer patients Manjiri Bakre, Ph.D. Founder and CEO OncoStem Diagnostics Pvt. Ltd. Treatment Decision: HR+/HER2-
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer
 Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana
Assays of Genetic Expression in Tumor Tissue as a Technique to Determine Prognosis in Patients with Breast Cancer Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana
Early Stage Disease. Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center
 SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
ISPOR 4 th Asia Pacific Conference IP2 Gilberto de Lima Lopes
 Health Economic Considerations for Personalized Medicine in Asia: Using Genomic Profiling to Guide Treatment Decisions in Early Breast Cancer Gilberto de Lima Lopes, Jr., M.D., M.B.A Assistant Director
Health Economic Considerations for Personalized Medicine in Asia: Using Genomic Profiling to Guide Treatment Decisions in Early Breast Cancer Gilberto de Lima Lopes, Jr., M.D., M.B.A Assistant Director
Kathy Albain, MD. Chemotherapy in Luminal Breast Cancer: Who Benefits? Loyola University Chicago Stritch School of Medicine
 Chemotherapy in Luminal Breast Cancer: Who Benefits? Kathy Albain, MD Loyola University Chicago Stritch School of Medicine, Director, Breast Clinical Research Program, Cardinal Bernardin Cancer Center,
Chemotherapy in Luminal Breast Cancer: Who Benefits? Kathy Albain, MD Loyola University Chicago Stritch School of Medicine, Director, Breast Clinical Research Program, Cardinal Bernardin Cancer Center,
High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX
 High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX Test: An Independent Quality Assurance Study DAVID J DABBS, MD Professor and Chief of Pathology
High False-Negative Rate of HER2 Quantitative Reverse Transcription Polymerase Chain Reaction of the Oncotype DX Test: An Independent Quality Assurance Study DAVID J DABBS, MD Professor and Chief of Pathology
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
MammaPrint Improving treatment decisions in breast cancer Support and Involvement of EU
 MammaPrint Improving treatment decisions in breast cancer Support and Involvement of EU 1 Bas van der Baan VP Clinical Affairs Irvine, California Amsterdam, The Netherlands 2 Two Crucial Questions in Cancer
MammaPrint Improving treatment decisions in breast cancer Support and Involvement of EU 1 Bas van der Baan VP Clinical Affairs Irvine, California Amsterdam, The Netherlands 2 Two Crucial Questions in Cancer
Breast cancer pathology
 Breast cancer pathology Giancarlo Pruneri, M.D. National Cancer Institute (INT) Milan University of Milan, School of Medicine Giancarlo.Pruneri@unimi.it Currently accepted prognostic/predictive parameters
Breast cancer pathology Giancarlo Pruneri, M.D. National Cancer Institute (INT) Milan University of Milan, School of Medicine Giancarlo.Pruneri@unimi.it Currently accepted prognostic/predictive parameters
I test molecolari nei protocolli di diagnosi e di trattamento
 I test molecolari nei protocolli di diagnosi e di trattamento Anna Sapino IRCCs Candiolo Dip Scienze Mediche, Università degli Studi di Torino 2016: Pathological report of breast cancer MINIMAL REQUIREMENTS
I test molecolari nei protocolli di diagnosi e di trattamento Anna Sapino IRCCs Candiolo Dip Scienze Mediche, Università degli Studi di Torino 2016: Pathological report of breast cancer MINIMAL REQUIREMENTS
PMRT for N1 breast cancer :CONS. Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center
 PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
MEDICAL POLICY. SUBJECT: GENETIC ASSAY OF TUMOR TISSUE TO DETERMINE PROGNOSIS OF BREAST CANCER (OncotypeDX TM, MammaPrint )
") MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 8 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
The Role of Novel Assays in the Prediction of Benefit from Extended Adjuvant Endocrine Therapy for Breast Cancer
 The Role of Novel Assays in the Prediction of Benefit from Extended Adjuvant Endocrine Therapy for Breast Cancer Erin Roesch, MD, and Claudine Isaacs, MD Abstract Endocrine therapy in the adjuvant setting
The Role of Novel Assays in the Prediction of Benefit from Extended Adjuvant Endocrine Therapy for Breast Cancer Erin Roesch, MD, and Claudine Isaacs, MD Abstract Endocrine therapy in the adjuvant setting
Oncotype DX reveals the underlying biology that changes treatment decisions 37% of the time
 Oncotype DX reveals the underlying biology that changes treatment decisions 37% of the time Even when treatment decisions based on traditional measures seem conclusive, Oncotype DX can lead to a different
Oncotype DX reveals the underlying biology that changes treatment decisions 37% of the time Even when treatment decisions based on traditional measures seem conclusive, Oncotype DX can lead to a different