Checkpoint-Inhibitoren beim Lungenkarzinom. Dr. Helge Bischoff Thoraxklinik Heidelberg
|
|
|
- Antony Stephens
- 6 years ago
- Views:
Transcription

1 Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg
2
3 Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year surival benefit 1% Median survival benefit: 1.5 months (6 vs 8 months) Significant symptom reduction Best Supportive Care Meta-analysis of 52 randomized trials Supportive care Supportive care plus chemotherapy Time From Randomization (months) No. at Risk Non-Small Cell Lung Cancer Collaborative Group. BMJ. 1995;311:
4 Metastatic Lung Cancer developments and challenges Reck et al. Lancet 382 (213): 79
5
6
7
8

9 RECIST 1.1 guidelines versus irrc guidelines


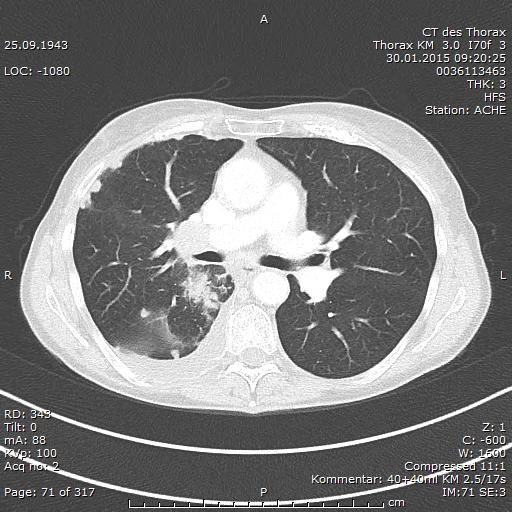
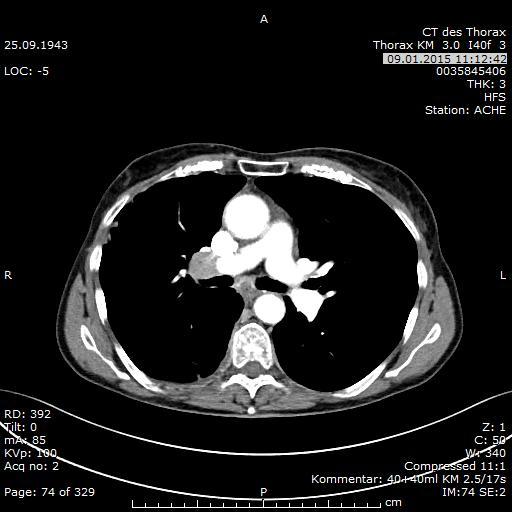
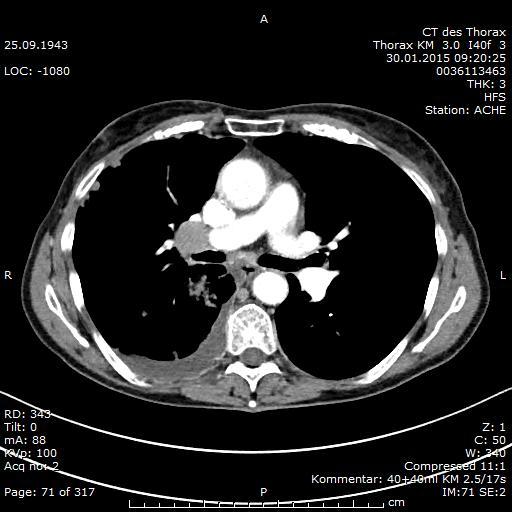
10 Verlauf nach 1. Applikation Nivolumab
11
12 Lungenkarzinom IV - Behandlungsempfehlungen Nichtkleinzelliges CA - Erstlinientherapie - Zweitlinientherapie - Mehrlinientherapie Kleinzelliges CA - Erstlinientherapie - Zweitlinientherapie - Mehrlinientherapie
13 CA184-41: Design of a Phase II trial to evaluate Ipilimumab in combination with chemotherapy* in NSCLC and SCLC 1st line First-line Stage IIIb/IV NSCLC (n=24) ED-SCLC (n=13) Induktion Erhaltung R A N D O M I Z E 1:1:1 Concurrent IPI + Pac/Carbo Phased* IPI + Pac/Carbo Control p + Pac/Carbo C C C C C C IPI IPI IPI IPI p p C C C C C C p p IPI IPI IPI IPI C C C C C C IPI IPI p IPI IPI p Follow-up Follow-up Follow-up * Paclitaxel/Carboplatin p p p p p p q3w q12w Lynch et al, J Clin Oncol 3: 246, Reck et al, Ann Oncol. 213; 24: 75 13
14 CA184-41: Phase II trial to evaluate Ipilimumab in combination with chemotherapy (carboplatin/paclitaxel) in lung cancer (NSCLC and SCLC): Immunrelated progression free survival Endpoints (months) Control Pbo + chemo. Concurrent IPI + chemo. Phased IPI + chemo. NSCLC 1 n=66 n=7 n=68 Median irpfs 4,6 Median mwho-pfs 4,2 5,5 (HR=,81, P=,13) 4,1 (HR=,88, P=,25) 5,7 (HR=,72, P=,5 a ) 5,1 (HR=,69, P=,2 a ) ED-SCLC 2 n=45 n=43 n=42 Median irpfs 5,3 Median mwho-pfs 5,2 5,7 (HR=,75, P=,11) 3,9 (HR=,93, P=,38) 6,4 (HR=,64, P=,3 a ) 5,2 (HR=,93, P=,37) Data support further evaluation of combination on a phased schedule 1,2 The safety profile was consistent with previous studies of Ipilimumab in other tumour types 1,2 Data from trial CA a Statistically significant per protocol-stipulated one-sided =.1; P values not adjusted for multiple comparisons HR = hazard ratio; Ipi = ipilimumab; irpfs = PFS by immune-related response criteria (irrc); mwho-pfs = PFS 14 y modified WHO criteria (mwho); Pbo = placebo; PFS = progression-free survival 1. Lynch et al, J Clin Oncol 212; 3: 246; 2. Reck et al, Ann Oncol 213; 24: 75
15 CA29-3: Design of a Phase I trial to evaluate Nivolumab monotherapy in different tumor types 8-week treatment cycle Rapid PD or clinical deterioration Off study Day 1 a 15 a 29 a 43 a 57 SCANS a Eligibility: Advanced NSCLC, melanoma, RCC, or CRC with PD after 1 5 systemic therapies Unacceptable toxicity CR/PR/SD or PD but clinically stable Follow-up every 8 weeks x 6 (48 weeks) Treat until confirmed CR, worsening PD, unacceptable toxicity, or 12 cycles (96 weeks) In this study, patients (n=36) with advanced NSCLC (n=129), melanoma (n=17), RCC (n=34), colorectal cancer (CRC; n=19), or castrate-resistant prostate cancer (CRPC; n=17) who were enrolled between October 28 and January 212 received Nivolumab,1 1 mg/kg every 2 weeks for a maximum of twelve 8-week treatment cycles Primary Objective: To evaluate the survival and long-term safety profile of patients being treated with Nivolumab Secondary Objective: Assess the efficacy of Nivolumab as monotherapy (Protocol was amended January 212 to evaluate overall survival (OS)) a Dose administered IV every 2 weeks; Hodi et al, Poster presentation at ECC 213:abstract 88 CR = 15 complete response; PD = progressive disease; PR = partial response; SD = stable disease
16 OS CA29-3: ASCO Update 214 Median OS according to dose (NSCLC) 1,,9,8,7,6,5,4,3,2,1, Zensiert OS Rate % ( 95 % KI) [Patienten unter Progressionsrisiko] Group Died/Treated Median OS (95% KI) 1-Jahr 2-Jahre 1 mg/kg 26/33 9,2 ( 5,3, 11,1) 32 (16,49) [8] 12 (3, 27) [2] 3 mg/kg 2/37 14,9 (7,3, ) 56 (38, 71) [17] 45 (27, 61) [9] 1 mg/kg 48/59 9,2 (5,2, 12,4) 4 (27, 52) [23] 19 (1, 31) [9] 1-year OS Rate 56% (17 patients at risk) 2-year OS Rate 45% (9 patients at risk) Monate seit Behandlung Initiation Patienten unter Progressionsrisiko Nivolumab 1 mg/kg Nivolumab 3 mg/kg Nivolumab 1 mg/kg Brahmer et al, oral presentation at ASCO
17 Nivolumab (Melanom, NSCLC, RCC) CA29-3: Clinical activity of Nivolumab Tumor Type ORR a n/n (%) [95% KI] Median Duration of Response, b wk (range) Stable Disease, n/n (%) [95% KI] 24 wk Median PFS, mo [95% KI] NSCLC c 22/129 (17,1) [11,, 24,7] 74, (6,1+, 133,9+) 13/129 (1,1) [5,5, 16,6] 2,3 [1,9, 3,7] Squamous 9/54 (16,7) [17,9, 29,3] NR d (16,1, 133,9+) 8/54 (14.8) [6,6, 27,1] 3,7 [1,8, 7,2] Non-squamous 13/74 (17,6) [9,7, 28,2] 63,9 (6,1+, 74,+) 5/74 (6,8) [2,2, 15,1] 2, [1,8, 3,6] MEL e 33/17 (3,8) [22,3, 4,5] 14, (18,4, 117,+) 7/17 (6,5) [2,7, 13,] 3,7 [1,9, 9,1] RCC e 1/34 (29,4) [15,1, 47,5] 56,1 (36,6, 126,7+) 9/34 (126,5) [12,9, 44,4] 7,3 [3,7, 12,9] CI = confidence interval; NR = not reached; ORR = objective response rate; PFS = progression-free survival a ORRS ({[CR + PR] / n} x 1) have been calculated based on confirmed responses. Individual patient responses were adjudicated per RECIST v1. with modification 11 ; b Kaplan-Meier estimate; time form first response to time of documented progression, death, or for censored data (denoted by + ); time to last tumor assessment; c Of 129 patients with NSCLC, 1 had an unknown histology and did not show an OR; d NR indicates that the time point at which the probability that responders progress drops below 5% has not been reached due to insufficient number of events and/or follow-up; e 1 CR was noted in melanoma and 1 CR was noted in RCC Hodi et al, Poster presentation at ECC 213:abstract 88 17
18 Nivolumab (Melanom, NSCLC, RCC) CA29-3: Treatment-related select AEs that occurred in >1% of all treated patients (n=36) Select AEs Any Grade, n (%) Grade 3 4, n (%) Select AEs Any Grade, n (%) Grade 3 4, n (%) Any select AEs 14 (45,8) 19 (6,2) Skin 75 (24,5) 1 (,3) Rash 45 (14,7) Pruritus 32 (1,5) 1 (,3) Rash pruritic 7 (2,3) Urticaria 6 (2,) Photosensitivity reaction 5 (1,6) Rash macular 4 (1,3) 1 (,3) Gastrointenstinal 44 (14,1) 3 (1,) Pulmonary 17 (5,6) 6 (2,) Pneumonitis c 12 (3,9) 4 (1,3) Infusion reaction 15 (4,9) 2 (,7) Infusion-related reaction 12 (3,9) Hypersensitivity 4 (1,3) 2 (,7) Renal 6 (2,) 1 (,3) Blood creatinine increased 4 (1,3) 1 (,3) Diarrhea 41 (13,4) 3 (1,) Colitis 6 (2,) 2 (,7) Endocrinopathies 29 (9,5) 3 (1,) Blood thyroid-stimulating hormone increased 11 (3,6) 1 (,3) Hypothyroidism 11 (3,6) 1 (,3) Hyperthyroidism 4 (1,3) 1 (,3) Hepatic 18 (5,9) 4 (1,3) Alanine aminotransferase increased 11 (3,6) 1 (,3) Aspartate aminotransferase increased 9 (2,9) a Select AEs with potential immune-related causality were defined as AEs requiring vigilant monitoring and/or unique intervention and were based on a prespecified list of MedDRA Terms, as determined by the sponsor; b Select AEs occuring in 1% of patients included lung infiltration (n=3; 1,%), acute respiratory distress syndrome (n=1;,3%), acute respiratory failure (n=1;,3%), diabetes mellitus (n=1;,3%), hypophysitis (n=1;,3%), renal failure (n=3; 1,%), and tubulointerstitial nephritis (n=2;,7%); c There were 3 (1%) deaths in patients with pneumonitis (2 NSCLC, 1 CRC) Hodi et al, Poster presentation at ECC 213: abstract 88 18
19 LBA43: Antitumor activity of pembrolizumab (Pembro; MK-3475) and correlation with programmed death ligand 1 (PD-L1) expression in a pooled analysis of patients (pts) with advanced non-small cell lung carcinoma (NSCLC) Garon E et al Study objective To evaluate the efficacy and safety of pembrolizumab among a number of cohorts of patients with EGFR+ or ALK+ advanced NSCLC Nonrandomised (n=33) PD-L1 + tumours a 2 previous therapies Nonrandomised (n=4) PD-L1 tumours a 2 previous therapies b Randomised (n=144) PD-L1 + tumours a 1 previous therapy b R (3:2) Randomised (n=45) PD-L1 + tumours a Treatment naïve R c (1:1) Nonrandomised (n=45) PD-L1 + tumours a 1 previous therapy b Pembro 1 mg/kg Q3W Pembro 1 mg/kg Q2W Pembro 1 mg/kg Q3W Pembro 1 mg/kg Q2W Pembro 2 mg/kg Q3W Pembro 1 mg/kg Q3W Pembro 1 mg/kg Q2W Pembro 2 mg/kg Q3W Primary endpoint ORR a Tumour PD-L1 expression was determined by a prototype assay to inform enrolment. Samples were independently reanalysed using a clinical trial IHC assay b Including 1 therapy platinum-containing doublet. c First 11 patients randomised to 2 mg/kg q3w and 1 mg/kg q3w. The remaining 34 patients were randomised to 1 mg/kg q2w and 1 mg/kg q3w. Analysis cut-off date is September 11, 214 for the nonrandomised cohort of 45 patients treated at 2 mg/kg q3w Secondary endpoints Immune-related response criteria Garon et al. Ann Oncol 214; 25 (suppl 4): abstr LBA43
20 Progression-free survival, % Overall survival, % LBA43: Antitumor activity of pembrolizumab (Pembro; MK-3475) and correlation with programmed death ligand 1 (PD-L1) expression in a pooled analysis of patients (pts) with advanced non-small cell lung carcinoma (NSCLC) Garon E et al Key results Robust antitumour activity was observed in both treatment-naïve and previously treated advanced NSCLC observed for all doses and schedules assessed 1 PFS (RECIST v1.1, Central Review) 1 OS Treatment naïve Previously treated n at risk Treatment naïve Previously treated Analysis cutoff date: March 3, Time, weeks Treatment naïve Median PFS: 27 weeks (95% CI 14, 45) 24-week PFS: 51% Previously treated Median PFS: 1 weeks (95% CI 9.1, 15.3) 24-week PFS: 26% Time, months Treatment naive Median OS: NR (95% CI NE, NE) 6-month OS: 86% Previously treated Median OS: 8.2 months (95% CI 7.3, NR) 6-month OS: 59% Garon et al. Ann Oncol 214; 25 (suppl 4): abstr LBA
21 LBA43: Antitumor activity of pembrolizumab (Pembro; MK-3475) and correlation with programmed death ligand 1 (PD-L1) expression in a pooled analysis of patients (pts) with advanced non-small cell lung carcinoma (NSCLC) Garon E et al Progression-free survival, % Overall survival, % Key results (cont.) - Strong PD-L1 tumour expression correlated with improved response, PFS and OS PFS (RECIST v1.1, Central Review) OS Strong Weak Negative n at risk Strong Weak Negative Time, weeks Conclusions - Pembrolizumab was effective in patients with treatment-naïve or previously treated advanced NSCLC - In particular, patients with strong PD-L1 tumour expression may benefit from this treatment Strong PD-L1 positivity defined as staining in 5% of tumour cells, and weak PD-L1 positivity as staining in 1 49% of tumour cells. Negative staining is no PD-L1 staining in tumour cells. Data cutoff: March 3, Time, months Garon et al. Ann Oncol 214; 25 (suppl 4): abstr LBA

22 MPDL328A: PCD4989g phase Ia study Expansion phase ongoing q3w dosing DLT window cycle 1 days 1 21 Standard phase I DLT criteria used Standard at doses.3mg/kg.1mg/kg.3mg/kg.1mg/kg n=1 n=1 n=1.3mg/kg n=3 1mg/kg n=3 3mg/kg n=3 1mg/kg n=6 2mg/kg n=12 Phase Ia expansion ongoing NSCLC n=85 Melanoma RCC Mandatory serial tumour biopsies Other tumour types Patients enrolled at 1, 15 and 2mg/kg UBC TNBC 1 patients with cutaneous or subcutaneous tumours that are amenable to serial excisional or punch biopsy will be enrolled; serial tumour biopsies will be performed for those 1 patients but will be optional for all other patients Hodi, et al. 213; Soria, et al. 213
23 MPDL328A: PCD4989g phase Ia study NSCLC cohort* Patient demographics and disease characteristics Characteristic All doses (n=85) Median age (range), y 6 (24 84) Male/female, n (%) Most patients were heavily 48 (56)/37 (44) pretreated, with more than ECOG PS, /1, n (%) half the cohort having 27 (32)/58 (68) Histology, n (%) Squamous received more than two lines of prior systemic therapy 2 (24) Nonsquamous 65 (76) Prior systemic regimens, n (%) 1 13 (15) 2 23 (27) 3 47 (55) CNS metastasis, n (%) 4 (5) Current/previous smoker 68 (8) EGFR status, n (%) Wild type 51 (6) Mutant 11 (13) Unknown 23 (27) *Safety evaluable patients (n=85) with NSCLC. Data cutoff 3 Apr 213 Systemic regimens administered in the metastatic, adjuvant or neoadjuvant setting; 3% of patients had no prior systemic regimens Soria, et al. 213
24 MPDL328A: PCD4989g phase Ia study NSCLC cohort Safety summary Adverse event * No MTD or DLTs No grade 3 5 pneumonitis One treatment-related death ; one immune-related grade 3/4 AE Treatment-related, n (%) (n=85) Any grade * Grade 3/4 Any AE 56 (66) 9 (11) Fatigue 17 (2) 2 (2) Nausea Most AEs were grade 1 or 2 12 (14) 1 (1) and did not require intervention Decreased appetite 1 (12) () Dyspnoea 8 (9) 1 (1) Diarrhoea 7 (8) () Asthenia 6 (7) () Headache 6 (7) () Rash 6 (7) () Pyrexia 5 (6) () Vomiting 5 (6) 1 (1) Upper respiratory tract infection 4 (5) () *Investigator assessed. Data cutoff 3 Apr 213 Patient had sinus thrombosis and cardiac/great vessel invasion by tumour at baseline Diabetes mellitus in patient with large cell neuroendocrine NSCLC Soria, et al. 213
25 % of patients MPDL328A: PCD4989g phase Ia study NSCLC cohort Efficacy summary (investigator assessed) NSCLC (n=53) Non-squamous (n=42) Squamous (n=11) * 27 Efficacy observed in both squamous and non-squamous histologies ORR SD for 24 weeks 24-week PFS rate Patients first dosed at 1 2 mg/kg by 1 Oct 212; data cutoff 3 Apr 213 * ORR includes investigator-assessed unconfirmed and confirmed PR where response was confirmed by repeat assessment 4 weeks after initial documentation. Assessment was by RECIST and irrc. Six patients with no post-baseline scan were included as non-responders Soria, et al. 213
26 MPDL328A: PCD4989g phase Ia study NSCLC cohort Best response by PD-L1 IHC status Diagnostic population (IC)* (n=53) ORR, % (n/n) PD, % (n/n) IHC 3 83 (5/6) 17 (1/6) IHC 2 and 3 46 (6/13) 23 (3/13) The subgroup with the highest proportion of PD-L1+ tumour- IHC 1 3 infiltrating cells also has the 31 (8/26) 38 (1/26) highest ORR All patients 23 (12/53) 4 (21/53) Patients first dosed at 1 2mg/kg by 1 Oct 212; data cutoff 3 Apr 213 * IHC 3: 1% tumour-infiltrating immune cells positive for PD-L1 (IC+); IHC 2 and 3: 5% tumour-infiltrating immune cells positive for PD-L1 (IC+); IHC 1/2/3: 1% tumour-infiltrating immune cells positive for PD-L1 (IC+); IHC /1/2/3: all patients with evaluable PD-L1 tumour IC status; ORR includes investigator-assessed unconfirmed and confirmed PR where response was confirmed by repeat assessment 4 weeks after initial documentation. Assessment by RECIST and irrc All patients includes patients with IHC /1/2/3 and 7 patients have an unknown diagnostic status Soria, et al. 213
27 Nivolumab + Ipilimumab (NSCLC) CA29-12: Interim Analysis of a Phase I study with Nivolumab and Ipilimumab in First-Line NSCLC Chemotherapy-naïve patients with stage IIIB or IV NSCLC Squamous Non-squamous Squamous Non-squamous Nivolumab 1 mg/kg IV Q3W + Ipilimumab 3 mg/kg IV Q3W (four 21-day cycles) Nivolumab 3 mg/kg IV Q3W + Ipilimumab 1 mg/kg IV Q3W (four 21-day cycles) Nivolumab 3 mg/kg IV Q2W until disease progression or unacceptable toxicity a Primary objective: safety and tolerability Secondary objectives: ORR and PFS rate at 24 weeks a Patients were permitted to continue study treatment beyond RECIST 1.1 defined progression if they were considered to be deriving clinical benefit and tolerating study treatment Antonia et al, Poster at ASCO
28 CA29-12: Tumor response in First-Line NSCLC patients Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg Squamous (n=9) Non-squamous (n=15) Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg Squamous (n=9) Non-squamous (n=16) ORR, n (%) [95% CI] 1 (11) [,3, 48] 2 (13) [2, 41] 3 (33) [8, 7] 2 (13) [2, 38] Ongoing responders, n (%) 1 (1%) 2 (1%) 1 (33%) 2 (1%) Best overall response, n (%) Complete response a Partial response a SD Progressive disease Unable to determine 1 (11) 2 (22) 4 (44) 2 (22) 2 (13) 5 (33) 4 (27) 3 (2) 3 (33) 5 (56) 1 (11) Estimated median DOR, b weeks (95% CI) NR NR 21 (12, 21) NR 2 (13) 4 (25) 6 (38) 2 (13) Response duration by patient, weeks , , 14+, , 49+ Patients with ongoing SD, n (%) 1 (2) 1 (2) 1 (25) SD duration, weeks 16, 45 16, 33, 34, 35+, 47 14, 14, 15, 24+, 27 13, 16, 22, 36+ a All complete and partial responses were confirmed by a subsequent tumor assessment per RECIST 1.1. Patients with an unconfirmed response are not shown b Time from first response to documented progression, death within 1 days of last nivolumab dose, or last tumor assessment (for censored + data). Estimated median DORs were determined from Kaplan-Meier curves + = response ongoing; CI = confidence interval; NR = not reached Antonia et al, Poster at ASCO
 Non-squamous (n=15) Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg Squamous (n=9) Non-squamous (n=16) 25 (4, 56) 51 (21, 74) 44 (14, 72) 2 (5, 43) 41 (2, 61) 29 (13, 48) 8,9 (,1+, 44,7) 32,9 (,1+,")
29 CA29-12: Survival outcomes in First-Line NSCLC patients PFS PFS rate at 24 weeks, % (95% CI) Median PFS, weeks (range) OS Median OS, weeks (range) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg Squamous (n=9) Non-squamous (n=15) Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg Squamous (n=9) Non-squamous (n=16) 25 (4, 56) 51 (21, 74) 44 (14, 72) 2 (5, 43) 41 (2, 61) 29 (13, 48) 8,9 (,1+, 44,7) 32,9 (,1+, 54,1+) 2,6 (9,7, 33,3+) 9,9 (4,1+, 58,1+) 16,1 (,1+, 54,1+) 14,4 (4,1+, 58,1+) 44,3 (1,4, 53,1+) NR (4,9+, 54,1+) NR (9,7, 5,1+) NR (8,1, 58,1+) NR (1,4, 54,1+) NR (8,1, 58,1+) Antonia et al, Poster at ASCO
30 CA29-12: Treatment-related AEs (based on grade 3/4 AEs reported in 2% of all patients) in First-Line NSCLC patients Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg Squamous (n=9) Non-squamous (n=15) Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg Squamous (n=9) Non-squamous (n=16) Total (n=49) Treatment-related AE, n (%) All Grades Grade 3/4 All Grades Grade 3/4 All Grades Grade 3/4 All Grades Grade 3/4 All Grades Grade 3/4 Patients with any AE 7 (78) 4 (44) 15 (1) 1 (67) 7 (78) 2 (22) 14 (88) 8 (5) 43 (88) 24 (49) Diarrhea 3 (33) 1 (11) 7 (47) 2 (13) 2 (22) 1 (11) 3 (19) 1 (6) 15 (31) 5 (1) Increased ALT 4 (27) 3 (2) 1 (11) 1 (11) 5 (1) 4 (8) Increased AST 4 (27) 3 (2) 1 (11) 1 (11) 5 (1) 4 (8) Colitis 1 (7) 1 (7) 4 (25) 3 (19) 5 (1) 4 (8) Increased lipase 3 (2) 2 (13) 2 (22) 1 (11) 2 (13) 1 (6) 7 (14) 4 (8) Fatigue 3 (33) 1 (67) 2 (13) 2 (22) 7 (44) 1 (6) 22 (45) 3 (6) Pneumonitis 2 (22) 1 (11) 2 (13) 1 (7) 1 (11) 1 (6) 1 (6) 6 (12) 3 (6) Adrenal insufficiency 1 (11) 1 (11) 1 (7) 1 (6) 1 (6) 3 (6) 2 (4) Increased amylase 3 (2) 1 (7) 1 (11) 2 (13) 1 (6) 6 (12) 2 (4) Rash 1 (11) 4 (27) 1 (7) 2 (22) 5 (31) 1 (6) 12 (24) 2 (4) ALT = alanine aminotransferase; AST = aspartate aminotransferase Antonia et al, Poster at ASCO 214 3
31
32
33
34 Aktive Studien Immuntherapie Thoraxklinik: 1st Line

35 Aktive Studien Immuntherapie Thoraxklinik: 2nd Line

36 Aktive Studien Immuntherapie Thoraxklinik: 3rd Line
37 Herausforderungen Immuntherapie LC Patientenauswahl Biomarker / Testung NW Mangement Responsebeurteilung Kosten

38
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Inmunoterapia en cáncer de pulmón. Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro
 Inmunoterapia en cáncer de pulmón Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Current Therapeutic Landscape for NSCLC Current treatment strategies in NSCLC Various
Inmunoterapia en cáncer de pulmón Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Current Therapeutic Landscape for NSCLC Current treatment strategies in NSCLC Various
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Checkpointinhibitoren in der Uro-Onkologie. Carsten Grüllich
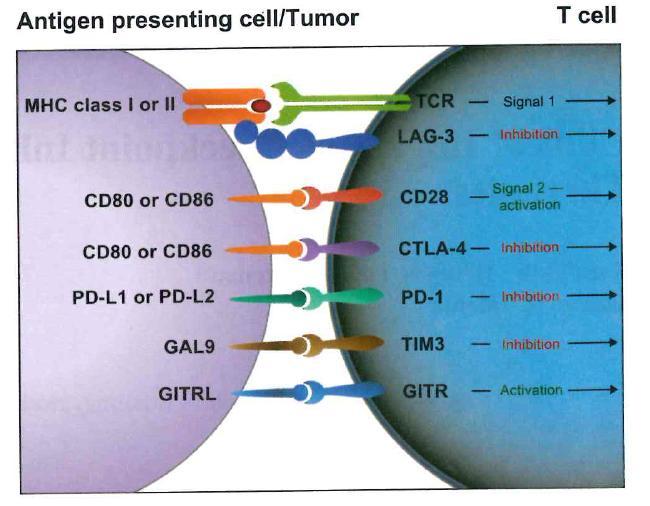
 Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 Study
 Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Weitere Kombinationspartner der Immunotherapie
 1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
1 Weitere Kombinationspartner der Immunotherapie Rolf Stahel University Hospital of Zürich Zürich, 9.12.216 2 Immunotherapy in a multimodality approach NSCLC Advanced disease Checkpoint inhibitors for
Immunotherapy in Patients with Non-Small Cell Lung Cancer
 LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
Supplementary Online Content
 Supplementary Online Content Powles T, O Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 openlabel
Supplementary Online Content Powles T, O Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 openlabel
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
KEYTRUDA is also indicated in combination with pemetrexed and platinum chemotherapy for the
 FDA-Approved Indication for KEYTRUDA (pembrolizumab) in Combination With Carboplatin and Either Paclitaxel or Nab-paclitaxel for the Firstline Treatment of Patients With Metastatic Squamous Non Small Cell
FDA-Approved Indication for KEYTRUDA (pembrolizumab) in Combination With Carboplatin and Either Paclitaxel or Nab-paclitaxel for the Firstline Treatment of Patients With Metastatic Squamous Non Small Cell
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies
 Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142
 Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
INMUNOTERAPIA I. Dra. Virginia Calvo
 INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
Cancer Immunotherapy Patient Forum. for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015
 Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Atezolizumab Is a Humanized Anti-PDL1 Antibody That Inhibits the Binding of PD-L1 to PD-1 and B7.1
 Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Phase II, Single-Arm Trial (BIRCH) of Atezolizumab as First-Line or Subsequent Therapy for Locally Advanced or Metastatic PD-L1-Selected Non-Small Cell Lung Cancer (NSCLC) Abstract 16LBA Besse B, Johnson
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Update on the development of immune checkpoint inhibitors
 Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies. Eric H. Rubin, MD Merck Research Laboratories
 Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial
: Results of a phase I trial") Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Presenter Disclosure Information
 Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
Presenter Disclosure Information Tara C. Gangadhar, M.D. The following relationships exist related to this presentation: Research funding (Institution): Incyte Corporation and Merck & Co., Inc Preliminary
NEW ZEALAND DATA SHEET
 NEW ZEALAND DATA SHEET 1. PRODUCT NAME Tecentriq 1200 mg concentrate for solution for infusion. atezolizumab (rch) CAS: 1380723-44-3 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Tecentriq is supplied as
NEW ZEALAND DATA SHEET 1. PRODUCT NAME Tecentriq 1200 mg concentrate for solution for infusion. atezolizumab (rch) CAS: 1380723-44-3 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Tecentriq is supplied as
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
PD-(L)1 Inhibitors and CTLA-4 Inhibitors: Rationale for Combinations and Recent Data in Non-Small Cell Lung Cancer
1 Inhibitors and CTLA-4 Inhibitors: Rationale for Combinations and Recent Data in Non-Small Cell Lung Cancer") PD-(L)1 Inhibitors and CTLA-4 Inhibitors: Rationale for Combinations and Recent Data in Non-Small Cell Lung Cancer Rebecca S. Heist, MD, MPH Abstract The recent success of PD-1 and PD-L1 inhibitors in
PD-(L)1 Inhibitors and CTLA-4 Inhibitors: Rationale for Combinations and Recent Data in Non-Small Cell Lung Cancer Rebecca S. Heist, MD, MPH Abstract The recent success of PD-1 and PD-L1 inhibitors in
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management
 Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
NEW ZEALAND DATA SHEET
 NEW ZEALAND DATA SHEET 1 PRODUCT NAME KEYTRUDA 50 mg powder for solution for infusion. 2 QUALITATIVE AND QUANTITATIVE COMPOSITION CAS No.: 1374853-91-4 One vial contains 50 mg of pembrolizumab. After reconstitution,
NEW ZEALAND DATA SHEET 1 PRODUCT NAME KEYTRUDA 50 mg powder for solution for infusion. 2 QUALITATIVE AND QUANTITATIVE COMPOSITION CAS No.: 1374853-91-4 One vial contains 50 mg of pembrolizumab. After reconstitution,
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Inmunoterapia en el carcinoma de Células de Merkel. Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona
 Inmunoterapia en el carcinoma de Células de Merkel Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Epidemiology Merkel cell carcinoma is an uncommon neuroendocrine carcinoma that mostly arises
Inmunoterapia en el carcinoma de Células de Merkel Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Epidemiology Merkel cell carcinoma is an uncommon neuroendocrine carcinoma that mostly arises
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
NSCLC with squamous histology: Current treatment and new options on horizon
 NSCLC with squamous histology: Current treatment and new options on horizon Prof. Yasser A.Kader Professor of Oncology Faculty of Medicine, Cairo University 2015 Lung Cancer: Incidence and Mortality New
NSCLC with squamous histology: Current treatment and new options on horizon Prof. Yasser A.Kader Professor of Oncology Faculty of Medicine, Cairo University 2015 Lung Cancer: Incidence and Mortality New
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
AUSTRALIAN PRODUCT INFORMATION Tecentriq (atezolizumab)
") AUSTRALIAN PRODUCT INFORMATION Tecentriq (atezolizumab) 1 NAME OF THE MEDICINE Atezolizumab 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each vial contains a total of 1200 mg atezolizumab. For the full list
AUSTRALIAN PRODUCT INFORMATION Tecentriq (atezolizumab) 1 NAME OF THE MEDICINE Atezolizumab 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each vial contains a total of 1200 mg atezolizumab. For the full list
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS
 CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
CONSIDERATIONS IN DEVELOPMENT OF PEMBROLIZUMAB IN MSI-H CANCERS December 2017 Christine K. Gause, Ph.D Executive Director, Biostatistics. 2 Microsatellite Instability-High Cancer - USPI KEYTRUDA is indicated
Post-ASCO 2017 Cancer du sein Triple Négatif
 Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf
 MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer
 Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer Benjamin Besse, MD, PhD Chair, EORTC Lung Group Chair, Gustave Roussy Thoracic Unit Villejuif, France What
Updates From the European Lung Cancer Conference: Immunotherapy and Non-Small Cell Lung Cancer Benjamin Besse, MD, PhD Chair, EORTC Lung Group Chair, Gustave Roussy Thoracic Unit Villejuif, France What
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Clinical Activity and Safety of Anti-PD-1 (BMS , MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer
 in Patients with Advanced Non-Small-Cell Lung Cancer") Clinical Activity and Safety of Anti-PD-1 (BMS-936558, MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer J.R. Brahmer, 1 L. Horn, 2 S.J. Antonia, 3 D. Spigel, 4 L. Gandhi, 5 L.V. Sequist,
Clinical Activity and Safety of Anti-PD-1 (BMS-936558, MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer J.R. Brahmer, 1 L. Horn, 2 S.J. Antonia, 3 D. Spigel, 4 L. Gandhi, 5 L.V. Sequist,
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
NECN CHEMOTHERAPY HANDBOOK PROTOCOL
 Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
ALK positive Lung Cancer. Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan
 ALK positive Lung Cancer Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan Objectives What is ALK translocation? What drugs are used in what sequence? How many times
ALK positive Lung Cancer Shirish M. Gadgeel, MD. Director of the Thoracic Oncology program University of Michigan Objectives What is ALK translocation? What drugs are used in what sequence? How many times
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
2019 ASCO-SITC. Nektar Therapeutics Investor & Analyst Call. March 1, 2019
 Nektar Therapeutics Investor & Analyst Call March 1, 2019 This presentation includes forward-looking statements regarding Nektar s proprietary drug candidates, the timing of the start and conclusion of
Nektar Therapeutics Investor & Analyst Call March 1, 2019 This presentation includes forward-looking statements regarding Nektar s proprietary drug candidates, the timing of the start and conclusion of
Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations
 Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Media Release. Basel, 21 July 2017
 Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Media Release Basel, 21 July 2017 CHMP recommends EU approval for Roche s TECENTRIQ (atezolizumab) in a specific type of metastatic lung and two types of metastatic bladder cancer TECENTRIQ as a potential
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
NSCLC: Terapia medica nella fase avanzata. Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza
 NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
Emerging Strategies in Triple-Negative Breast Cancer
 Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Presentation Number: LBA18_PR. Lecture Time: 09:15-09:27. Speakers: Heinz-Josef J. Lenz (Los Angeles, US) Background
 Background") LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
LBA18_PR - Durable Clinical Benefit With Nivolumab (NIVO) Plus Low-Dose Ipilimumab (IPI) as First-Line Therapy in Microsatellite Instability-High/Mismatch Repair Deficient (MSI-H/dMMR) Metastatic Colorectal
New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer
 New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN BY PRODUCT
 PAGE 175 PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN BY PRODUCT Summary of risk management plan for pembrolizumab This is a summary of the risk management plan (RMP) for pembrolizumab. The RMP details
PAGE 175 PART VI: SUMMARY OF THE RISK MANAGEMENT PLAN BY PRODUCT Summary of risk management plan for pembrolizumab This is a summary of the risk management plan (RMP) for pembrolizumab. The RMP details