SURGICAL MANAGEMENT OF GASTRIC CANCER
|
|
|
- Erika Bishop
- 6 years ago
- Views:
Transcription
1 SURGICAL MANAGEMENT OF GASTRIC CANCER Irina Kovatch, PGY 4 Kings County Medical Center Morbidity and Mortality January 13, 2011
2 Case Presentation 60 yo M admitted to medicine on 10/24/2010 with c/o persistent N/V x 3 weeks, weight loss 40lb/1 year HPI: diagnosed with gastric cancer at Brookdale in 12/2009, refused surgery PMH: GERD, PUD, CKD, PVD PSH: LIHR Meds: nexium SH: denies x3 FH: gastric cancer - parent, ovarian cancer - sister
3 Physical Exam VS: 98.7, 111/77, 96, 16, 100% On exam cachectic bitemporal wasting palpable abdominal mass umbilical nodule guaiac +
4 Labs CBC /14.2/40.7/423 BMP - 142/3.1/78/47/44/3.97/112 LFTs - 7.0/4.0/31/17/59/0.4 Coags /28.2/1.0 VBG /68.9/38.3/49.5/28 Lipase 120
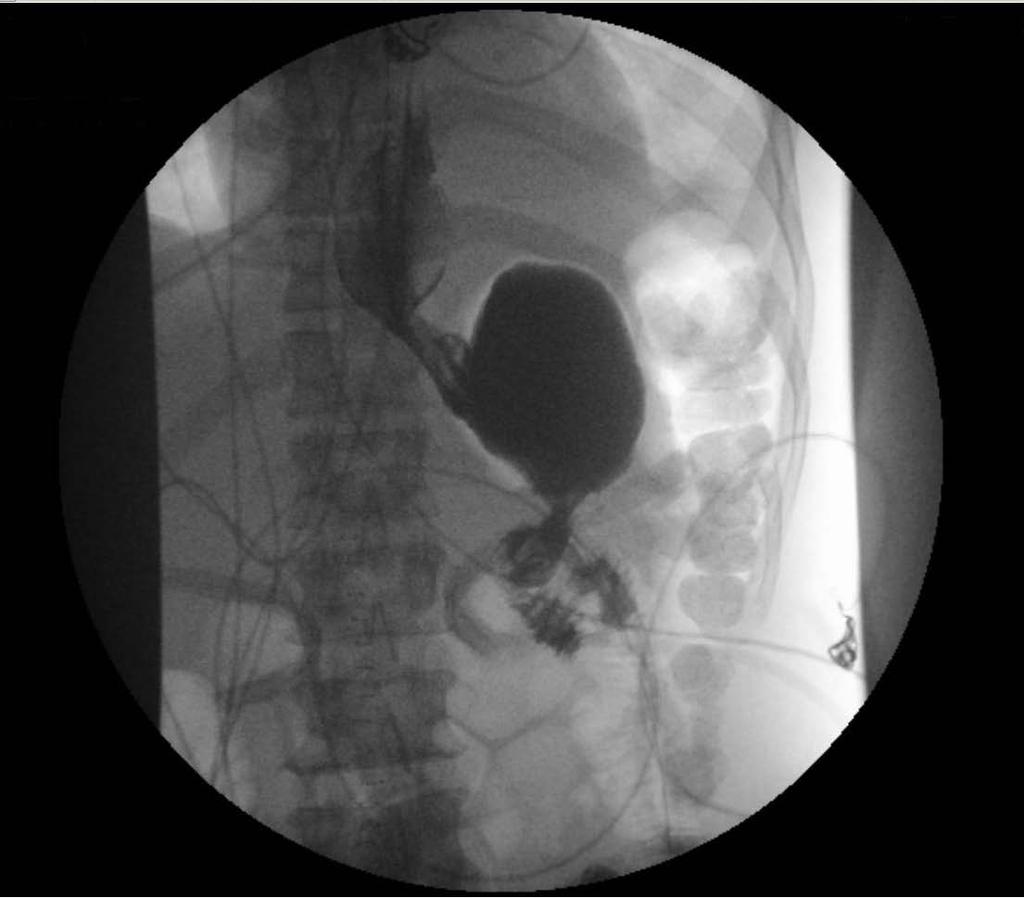
5 Imaging CXR (10/24) - neg CT Abd (10/25) - thickening in the gastric antrum, limited evaluation for hematogenous metastasis w/o IV contrast, no bulky intraabdominal LAD CT Chest (10/27) - no evidence of metastatic disease, limited w/o IV contrast, nonspecific lucent lesion within L2 vertibral body RUQ US (10/28) - heterogeneous liver

6 CT Abdomen
7 Hospital Course Management: NPO, IVF, nexium drip, GI/Surgery EGD (10/28) - copious dark liquid in the stomach, attempt at aspiration -> vomiting -> patient refused NGT -> procedure aborted Transferred to surgery, scheduled for OR NGT placed - 600cc of clear fluid Brookdale records 11/09 gastric biopsy: adenoca w/signet ring cells 10/18/10 bone scan: neg
8 Operation Ex-lap, no gross mets Palpable mass in pylorus/antrum Enter lesser sac after dividing omentum from transverse colon Stomach mass extending along lesser curvature to GE junction Mobilized pylorus and 1 st portion of duodenum Large firm LNs posterior to mid stomach Large left gastric artery suture ligated
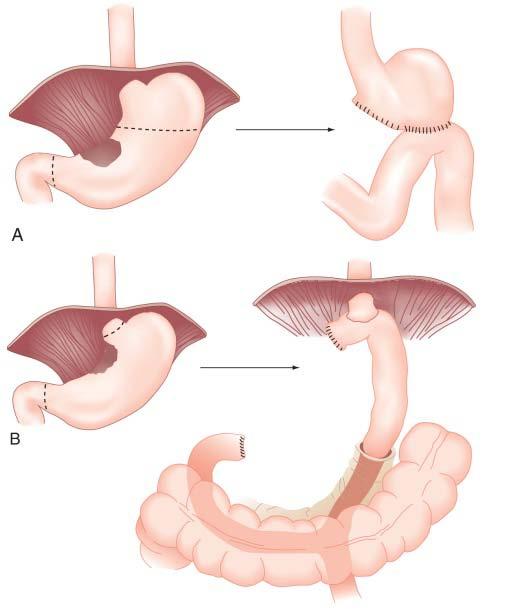
9 Operation Mobilized greater curvature to splenic hilum, short gastrics preserved Transected 1 st portion of duodenum and proximal stomach for subtotal gastrectomy Billroth II reconstruction (retrocolic) Left 2 JPs (duodenal stump, anastomosis site) Excision of umbilicus and closure EBL 1L, transfusion 2 Units PRBC, 7L crystalloids
10 Pathology Gastric adenocarcinoma Poorly differentiated Some signet ring cells Diffuse type Tumor invades through serosa (T4) 12/17 lymph nodes positive (N2) Metastasis in umbilical tissue (M1) Stage IV
11 Post-op Course POD 0 - SICU intubated POD 1 - extubated POD 2 - transfer to floor, NGT not draining Esophagram: intact anastomosis, no leak or obstruction POD 3 - advanced to clears POD diet slowly advanced to solids POD 6 - JPs removed POD 7 - discharged home
12
13 Outpatient Follow-up Surgery POD 19: asymptomatic, good appetite, gained weight, wound healing well, staples removed Oncology POD 20: reluctant to receive any chemo, wants to wait until symptoms for palliative chemotherapy

14 Questions
15 Gastric Cancer Adenocarcinoma (95%) Squamous cell carcinoma Adenoacanthoma Carcinoid tumors GI stromal tumors Lymphoma

16 Risk Factors
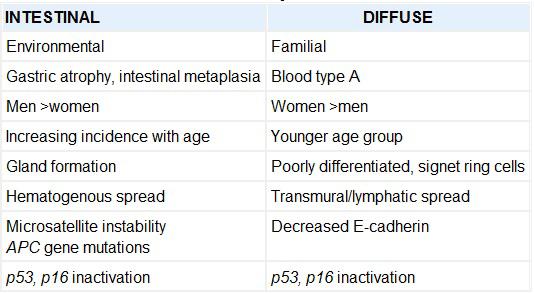
17 Lauren Classification System
18 TNM Classification
19 Staging
20 Clinical Presentation Early symptoms vague epigastric discomfort, indigestion Advanced disease weight loss, anorexia, fatigue, vomiting Physical Exam palpable abdominal mass Virchow's lymph node Sister Mary Joseph's node Blummer's shelf Krukenberg's tumor
21 Preoperative Evaluation EGD with multiple biopsies EUS for staging (some centers) Labs CBC, BMP, LFTs, Coags Imaging CXR, CT Abd, CT Chest (proximal tumors) Laparoscopy (for T3-T4 tumors) - can identify unsuspected metastatic disease in 13-57%
22 Surgical Treatment In the absence of distant mets: goal - R0 resection Proximal tumor total gastrectomy Norwegian Stomach Cancer Trial morbidity and mortality rates for Proximal gastric resection - 52% and 16% Total gastrectomy - 38% and 8% Distal tumor subtotal or total gastrectomy 5-6 cm luminal margin recommended Reconstruction: Billroth II or Roux-en-Y
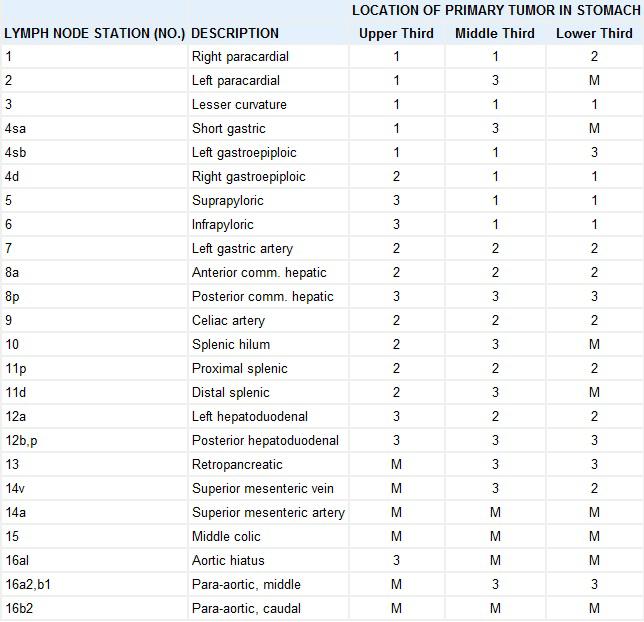
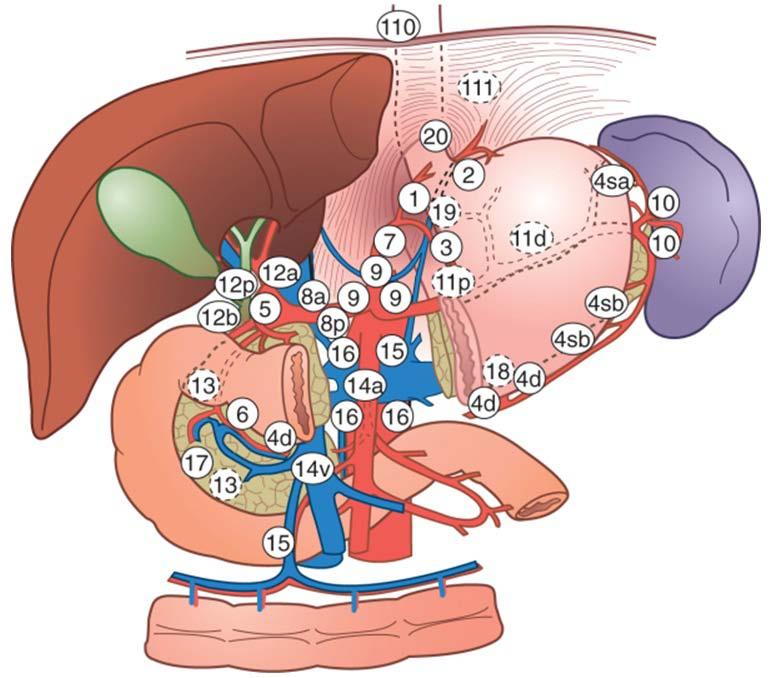
23 Lymph Nodes Japanese Classification for Gastric Carcinoma 16 lymph node stations or echelons stations classified into groups that correspond to the location of the primary tumor presence of metastasis to a lymph node group determines the N classification metastases to group 1 lymph nodes (and absence of disease in more distant lymph node groups) is classified as N1
24
25
26 Lymphadenectomy D1 resection - removal of group 1 lymph nodes D2 resection - removal of group 1 & 2 lymph nodes D3 resection - D2 resection plus removal of paraaortic lymph nodes Japanese surgeons perform splenectomy and partial pancreatectomy during D2 resections Western surgeons do not typically resect the spleen or pancreas because of the increased morbidity NCCN guidelines - minimum of a D1 resection with excision of at least 15 lymph nodes
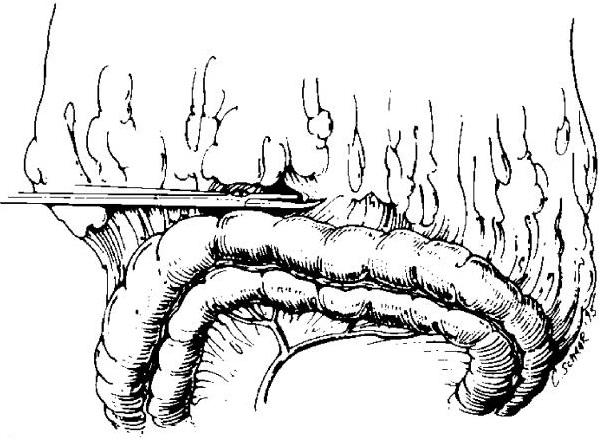
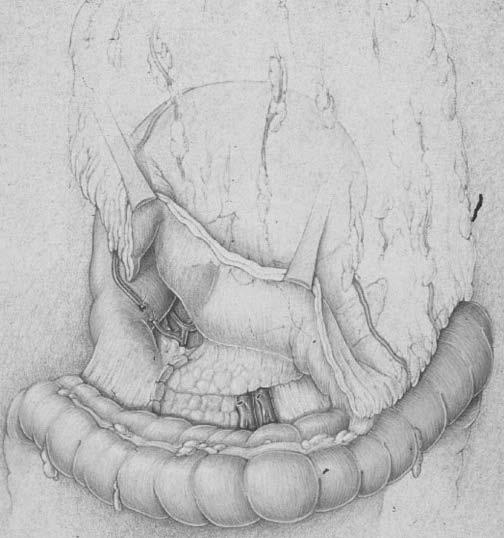
27 Operative Technique Avascular plane between the greater omentum and transverse colon is incised Dissection continues along the avascular plane between the anterior and posterior sheaths of the transverse mesocolon to the level of the pancreas Lateral attachments of the stomach and short gastric vessels are divided
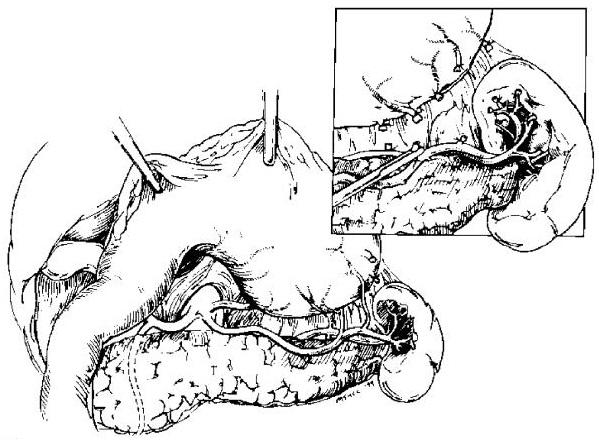
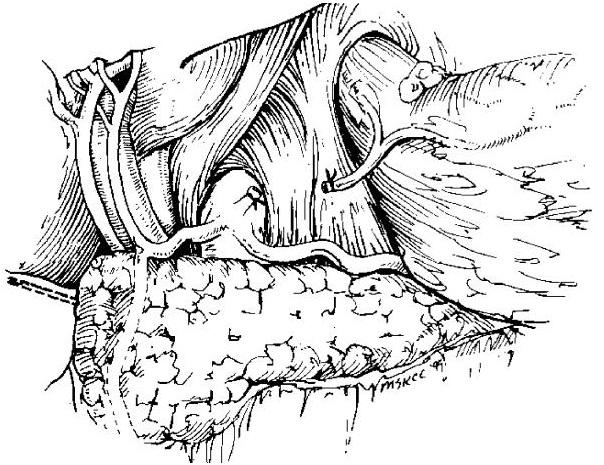
28 Operative Technique Splenic artery and nodal tissue is dissected down to the level of splenic hilum Duodenum is identified and divided Nodal dissection proceeds from the porta hepatis toward the celiac axis, left gastric artery is divided at its origin Nodal dissection continues along the right diaphragmatic crus and esophageal hiatus
29
30
31
32
33
34
35
36 Palliative Treatment 20-30% of patients present with stage IV disease Goal - relief of symptoms with minimal morbidity Surgical palliation - resection or bypass Other techniques percutaneous, endoscopic, radiotherapy Palliation of bleeding or proximal gastric obstruction laser recanalization endoscopic dilation stent placement
37 Outcomes Overall 5-year survival 10-21% 5-year survival for patients who undergo a potentially curative resection 24-57% Recurrence rates after gastrectomy 40-80% (most within 3 years) locoregional failure rate 38-45% (gastric remnant at the anastomosis, gastric bed, regional nodes) peritoneal dissemination in 54% isolated distant metastases are uncommon Hematogenous spread occurs to the liver, lung, and bone
38 Total vs. Subtotal Gastrectomy RCTs Ann Surg Aug;230(2): Subtotal versus total gastrectomy for gastric cancer: five-year survival rates in a multicenter randomized Italian trial. Italian Gastrointestinal Tumor Study Group. Bozzetti F, Marubini E, Bonafanti G, et al 618 patients with distal gastric cancer underwent TG or STG with at least 6cm margin Ann Surg Feb;209(2): Total versus subtotal gastrectomy for adenocarcinoma of the gastric antrum. A French prospective controlled study. Gouzi JL, Huguier M, Fagniez PL, et al 169 patients with antral gastric cancer underwent TG or STG Both studies showed no 5-year survival difference
39 Journal of Clinical Oncology, Vol 22, No 11, 2004: pp Extended Lymph Node Dissection for Gastric Cancer: Who May Benefit? Final Results of the Randomized Dutch Gastric Cancer Group Trial H.H. Hartgrink, C.J.H. van de Velde, H. Putter, et al Prospective RCT of 711 patients with gastric adenocarcinoma who underwent D1 or D2 lymph node dissection and were followed > 10 years Morbidity (25% v 43%; P < 0.001) and mortality (4% v 10%; P = 0.004) were significantly higher in the D2 dissection group After 11 years there is no overall difference in survival (30% v 35%; P =.53)
40 The Lancet Oncology - Volume 7, Issue 4 (April 2006) Nodal dissection for patients with gastric cancer: a randomized controlled trial Chew-Wun Wu, Chao A Hsiung, Su-Shun Lo, et al Single institution trial of 335 patients who underwent D1 and D3 surgery with median follow-up of 94.5 months Overall 5-year survival was in D3 group compared to D1 group was 59.5% vs 53.6% (difference between groups 5.9%, log-rank p=0.041) Patients who had R0 resection had recurrence at 5 years of 50.6% for D1 surgery and 40.3% for D3 surgery, results not statistically significant
41 National Comprehensive Cancer Network Practice Guidelines in Oncology v Principles of Gastric Cancer Surgery Tis-T1a tumors: candidates for endoscopic resection T1b-T3: distal, subtotal or total gastrectomy to achieve R0 resection (typically >= 4cm from gross tumor) T4 tumors: en bloc resection of involved structures Gastric resection should include the regional lymphatics perigastric (D1) and those along the named vessels of the celiac axis (D2), with a goal of examining >= 15 nodes Routine or prophylactic splenectomy is not required
42 National Comprehensive Cancer Network Practice Guidelines in Oncology v Principles of Gastric Cancer Surgery Criteria for unresectability for cure: Locoregionally advanced Distant metastases or peritoneal seeding Unresectable tumors: Palliative resection should not be performed unless patient is symptomatic Lymph node dissection is not required Gastric bypass with gastrojejunostomy may be useful in palliating obstructive symptoms
GASTRIC CANCER. Joyce Au SUNY Downstate Grand Rounds July 11, 2013
 GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ.
 Professor of Surgery, Taibah Univ.") By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Gastric Cancer: Surgery and Regional Therapy. Epidemiology. Risk factors
 Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Laparoscopy-assisted D2 radical distal subtotal gastrectomy
 Masters of Gastrointestinal Surgery Laparoscopy-assisted D2 radical distal subtotal gastrectomy Xiaogeng Chen, Weihua Li, Jinsi Wang, Changshun Yang Department of Tumor Surgery, Fujian Provincial Hospital,
Masters of Gastrointestinal Surgery Laparoscopy-assisted D2 radical distal subtotal gastrectomy Xiaogeng Chen, Weihua Li, Jinsi Wang, Changshun Yang Department of Tumor Surgery, Fujian Provincial Hospital,
Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition
 22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Surgical Treatment of Localized Gastric Cancer
 13 Surgical Treatment of Localized Gastric Cancer JOHN I. LEW, MD MITCHELL C. POSNER, MD Theodor Billroth performed the first successful gastric resection (a distal subtotal gastrectomy for stomach cancer)
13 Surgical Treatment of Localized Gastric Cancer JOHN I. LEW, MD MITCHELL C. POSNER, MD Theodor Billroth performed the first successful gastric resection (a distal subtotal gastrectomy for stomach cancer)
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Surgical Treatment of Gastric Cancer
 SMGr up Surgical Treatment of Gastric Cancer Igor Correia de Farias 1 *, Maria Luiza Leite de Medeiros 2, Wilson Luiz da Costa Júnior 1, Heber Salvador de Castro Ribeiro 1, Alessandro Landskron Diniz 1,
SMGr up Surgical Treatment of Gastric Cancer Igor Correia de Farias 1 *, Maria Luiza Leite de Medeiros 2, Wilson Luiz da Costa Júnior 1, Heber Salvador de Castro Ribeiro 1, Alessandro Landskron Diniz 1,
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
GASTRIC CANCER DR AMIR ASHRAFI
 GASTRIC CANCER DR AMIR ASHRAFI Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common
GASTRIC CANCER DR AMIR ASHRAFI Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Approaches to Surgical Treatment of Gastric Cancer. Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service
 Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Subtotal versus total gastrectomy for T3 adenocarcinoma of the antrum
 Gastric Cancer (2003) 6: 237 242 DOI 10.1007/s10120-003-0261-4 Original article 2003 by International and Japanese Gastric Cancer Associations Subtotal versus total gastrectomy for T3 adenocarcinoma of
Gastric Cancer (2003) 6: 237 242 DOI 10.1007/s10120-003-0261-4 Original article 2003 by International and Japanese Gastric Cancer Associations Subtotal versus total gastrectomy for T3 adenocarcinoma of
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Guidelines for Extended Lymphadenectomy in Gastric Cancer: A Prospective Comparative Study
 Ann Surg Oncol DOI 10.1245/s10434-012-2544-7 ORIGINAL ARTICLE GASTROINTESTINAL ONCOLOGY Guidelines for Extended Lymphadenectomy in Gastric Cancer: A Prospective Comparative Study Oktar Asoglu, MD 1, Tugba
Ann Surg Oncol DOI 10.1245/s10434-012-2544-7 ORIGINAL ARTICLE GASTROINTESTINAL ONCOLOGY Guidelines for Extended Lymphadenectomy in Gastric Cancer: A Prospective Comparative Study Oktar Asoglu, MD 1, Tugba
Case Presentation. PMH: HTN, BPH, strabismus PSH: appendectomy Medications: norvasc, tamsulosin NKDA SH/FH: negative
 Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
Case Presentation 68yM referred for incidental finding of pancreatic head mass on CT scan for elevated PSA. No symptoms. Denied pruritus, jaundice, change in color of urine/stool, anorexia, or weight loss.
General Data. Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission :
 General Data Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission : 92-07-09 1 Chief complaint Upper abdominal fullness 30 minutes after having foods with sometimes epigastralgia
General Data Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission : 92-07-09 1 Chief complaint Upper abdominal fullness 30 minutes after having foods with sometimes epigastralgia
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN
 Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Therapeutic effect of laparoscopy-assisted D2 radical gastrectomy in 106 patients with advanced gastric cancer
 JBUON 2013; 18(3): 689-694 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Therapeutic effect of laparoscopy-assisted D2 radical gastrectomy in
JBUON 2013; 18(3): 689-694 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Therapeutic effect of laparoscopy-assisted D2 radical gastrectomy in
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Minimally Invasive Esophagectomy
 American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Surgical Management of Gastroesophageal Cancer in China
 Surgical Management of Gastroesophageal Cancer in China Yihong SUN, M.D., Ph.D., FRCS, Fudan University General Surgery Research Institute of Fudan University 01/14/2017; Detriot Disclosure I have no relevant
Surgical Management of Gastroesophageal Cancer in China Yihong SUN, M.D., Ph.D., FRCS, Fudan University General Surgery Research Institute of Fudan University 01/14/2017; Detriot Disclosure I have no relevant
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
CT Findings in the Abdomen and Pelvis After Gastric Carcinoma Resection
 CT Findings in the Abdomen and Pelvis After Gastric Carcinoma Resection Kyeong Ah Kim 1, Cheol Min Park 1, Sang Woo Park 1, Sang Hoon Cha 1, Hae Young Seol 1, In Ho Cha 1, Ki Yeol Lee 2 G astric carcinoma
CT Findings in the Abdomen and Pelvis After Gastric Carcinoma Resection Kyeong Ah Kim 1, Cheol Min Park 1, Sang Woo Park 1, Sang Hoon Cha 1, Hae Young Seol 1, In Ho Cha 1, Ki Yeol Lee 2 G astric carcinoma
TUMORS OF THE STOMACH AND SMALL BOWEL
 gastrointestinal tract and abdomen TUMORS OF THE STOMACH AND SMALL BOWEL L. Mark Knab, MD, David J. Bentrem, MD, FACS, and Jeffrey D. Wayne, MD, FACS * Gastric Adenocarcinoma The incidence of gastric carcinoma
gastrointestinal tract and abdomen TUMORS OF THE STOMACH AND SMALL BOWEL L. Mark Knab, MD, David J. Bentrem, MD, FACS, and Jeffrey D. Wayne, MD, FACS * Gastric Adenocarcinoma The incidence of gastric carcinoma
Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer
 Masters of Gastrointestinal Surgery Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer Xin Ye, Jian-Chun Yu, Wei-Ming
Masters of Gastrointestinal Surgery Totally laparoscopic distal gastrectomy reconstructed by Rouxen-Y with D2 lymphadenectomy and needle catheter jejunostomy for gastric cancer Xin Ye, Jian-Chun Yu, Wei-Ming
Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy
 Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
Original Article Satisfactory surgical outcome of T2 gastric cancer after modified D2 lymphadenectomy Shupeng Zhang 1, Liangliang Wu 2, Xiaona Wang 2, Xuewei Ding 2, Han Liang 2 1 Department of General
AATS Focus on Thoracic Surgery: Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017?
 AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
Subtotal gastrectomy for gastric cancer
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v20.i38.13667 World J Gastroenterol 2014 October 14; 20(38): 13667-13680 ISSN 1007-9327
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v20.i38.13667 World J Gastroenterol 2014 October 14; 20(38): 13667-13680 ISSN 1007-9327
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
GASTRIC CANCER RANDOMIZED CONTROLLED TRIAL ON D2 LINPHADENECTOMY VS STANDARD D1 LINPHADENECTOMY
 GASTRIC CANCER RANDOMIZED CONTROLLED TRIAL ON D2 LINPHADENECTOMY VS STANDARD D1 LINPHADENECTOMY Maurizio Degiuli, MD Coordinator of the IGCSG (Italian Gastric Cancer Study Group) Antonio Ponti, MD MPH
GASTRIC CANCER RANDOMIZED CONTROLLED TRIAL ON D2 LINPHADENECTOMY VS STANDARD D1 LINPHADENECTOMY Maurizio Degiuli, MD Coordinator of the IGCSG (Italian Gastric Cancer Study Group) Antonio Ponti, MD MPH
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Laparoscopic Subtotal Gastrectomy for Gastric Cancer
 SCIENTIFIC PAPER Laparoscopic Subtotal Gastrectomy for Gastric Cancer Danny Rosin, MD, Yuri Goldes, MD, Barak Bar Zakai, MD, Moshe Shabtai, MD, Amram Ayalon, MD, Oded Zmora, MD ABSTRACT Background: The
SCIENTIFIC PAPER Laparoscopic Subtotal Gastrectomy for Gastric Cancer Danny Rosin, MD, Yuri Goldes, MD, Barak Bar Zakai, MD, Moshe Shabtai, MD, Amram Ayalon, MD, Oded Zmora, MD ABSTRACT Background: The
Cancer of the Stomach
 Cancer of the Stomach Review of Consecutive Ten Year Intervals KENNETH ADASHEK, M.D.,* JAMES SANGER, M.D.,t WILLIAM P. LONGMIRE, JR., M.D.* Records were reviewed for all patients who underwent primary
Cancer of the Stomach Review of Consecutive Ten Year Intervals KENNETH ADASHEK, M.D.,* JAMES SANGER, M.D.,t WILLIAM P. LONGMIRE, JR., M.D.* Records were reviewed for all patients who underwent primary
Laparoscopy-assisted radical total gastrectomy plus D2 lymph node dissection
 Masters of Gastrointestinal Surgery Laparoscopy-assisted radical total gastrectomy plus D2 lymph node dissection Chaohui Zheng, Changming Huang, Ping Li, Jianwei Xie, Jiabin Wang, Jianxian Lin, Jun Lu
Masters of Gastrointestinal Surgery Laparoscopy-assisted radical total gastrectomy plus D2 lymph node dissection Chaohui Zheng, Changming Huang, Ping Li, Jianwei Xie, Jiabin Wang, Jianxian Lin, Jun Lu
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Printed by Hadi Ranjkeshzadeh on 11/12/2010 4:40:23 PM. For personal use only. Not approved for distribution. Copyright 2010 National Comprehensive
 Discussion Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform consensus. Category 2A: The recommendation
Discussion Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform consensus. Category 2A: The recommendation
 Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Gastric (Stomach) Cancer
 Cancer") Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
Gastric (Stomach) Cancer Gastric cancer is a disease in which malignant (cancer) cells form in the lining of the stomach. The stomach is a J-shaped organ in the upper abdomen. It is part of the digestive
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Stomach. R.B. Kolachalam, MD
 Stomach R.B. Kolachalam, MD Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum Gastric Anatomy body of the stomach: site of mechanical
Stomach R.B. Kolachalam, MD Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum Gastric Anatomy body of the stomach: site of mechanical
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Treatment Strategy for Non-curative Resection of Early Gastric Cancer. Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea
 Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Patient. Male 76 year old C.C: abdominal pain
 Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Case Report Late Onset Remnant Gastric Cancer with Afferent Loop Syndrome 47 Years after Billroth II Surgery
 Case Reports in Surgery Volume 2015, Article ID 730897, 4 pages http://dx.doi.org/10.1155/2015/730897 Case Report Late Onset Remnant Gastric Cancer with Afferent Loop Syndrome 47 Years after Billroth II
Case Reports in Surgery Volume 2015, Article ID 730897, 4 pages http://dx.doi.org/10.1155/2015/730897 Case Report Late Onset Remnant Gastric Cancer with Afferent Loop Syndrome 47 Years after Billroth II
ARROCase: Borderline Resectable Pancreatic Cancer
 ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
CT EVALUATION OF GASTRIC LESIONS:
 CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
Thymic Tumors. Feiran Lou MD. MS. Kings County Hospital Department of Surgery
 Thymic Tumors Feiran Lou MD. MS. Kings County Hospital Department of Surgery Case HPI 53 yo man referred from OSH for anterior mediastinal mass. Initially presented with leg weakness and back pain for
Thymic Tumors Feiran Lou MD. MS. Kings County Hospital Department of Surgery Case HPI 53 yo man referred from OSH for anterior mediastinal mass. Initially presented with leg weakness and back pain for
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
Positive impact of adding No.14v lymph node to D2 dissection on survival for distal gastric cancer patients after surgery with curative intent
 Original Article Positive impact of adding No.14v lymph node to D2 dissection on survival for distal gastric cancer patients after surgery with curative intent Yuexiang Liang 1,2 *, Liangliang Wu 1 *,
Original Article Positive impact of adding No.14v lymph node to D2 dissection on survival for distal gastric cancer patients after surgery with curative intent Yuexiang Liang 1,2 *, Liangliang Wu 1 *,
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
UCLA General Surgery Residency Program Rotation Educational Policy Goals and Objectives
 UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
I patients with nonendocrine pancreas carcinoma
 LYMPH NODE INVOLVEMENT IN CARCINOMA OF THE HEAD OF THE PANCREAS AREA ANTONIO L. CUBILLA, MD,* JOSEPH FORTNER, MD,+~ AND PATRICK J. FITZGERALD, MD*~ A prospective study to determine the lymph node involvement
LYMPH NODE INVOLVEMENT IN CARCINOMA OF THE HEAD OF THE PANCREAS AREA ANTONIO L. CUBILLA, MD,* JOSEPH FORTNER, MD,+~ AND PATRICK J. FITZGERALD, MD*~ A prospective study to determine the lymph node involvement
I. Technical Issues. Surgical Resection of Gastric Cancer. Surgical Resection of Gastric Cancer Evidence & Issues. French and Italian RCT Antral Ca
 Surgical Resection of Gastric Cancer Evidence & Issues Carol J. Swallow Department of Surgical Oncology Princess Margaret and Mount Sinai Hospitals University of Toronto Surgical Problems in Proximal GI
Surgical Resection of Gastric Cancer Evidence & Issues Carol J. Swallow Department of Surgical Oncology Princess Margaret and Mount Sinai Hospitals University of Toronto Surgical Problems in Proximal GI
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Imaging techniques in the diagnosis, staging and follow up of GI cancers. Moderators: Banke Agarwal, MD and Paul Schultz, MD
 Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Clinical Significance of Total Gastrectomy for Proximal Gastric Cancer
 Clinical Significance of Total Gastrectomy for Proximal Gastric Cancer AKIRA OOKI, KEISHI YAMASHITA, SHIRO KIKUCHI, SHINICHI SAKURAMOTO, NATSUYA KATADA, NOBUE HUTAWATARI and MASAHIKO WATANABE Department
Clinical Significance of Total Gastrectomy for Proximal Gastric Cancer AKIRA OOKI, KEISHI YAMASHITA, SHIRO KIKUCHI, SHINICHI SAKURAMOTO, NATSUYA KATADA, NOBUE HUTAWATARI and MASAHIKO WATANABE Department
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer
 Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph
Appendix 1: Regional Lymph Node Stations for Staging Esophageal Cancer Locoregional (N stage) disease was redefined in the seventh edition of the AJCC Cancer Staging Manual as any periesophageal lymph