Trends in Prostate Cancer Bob Weir AVP Underwriting Research Canada Life Reinsurance
|
|
|
- Rodney Fleming
- 6 years ago
- Views:
Transcription

1 Trends in Prostate Cancer Bob Weir AVP Underwriting Research Canada Life Reinsurance Metropolitan Underwriting Discussion Group Annual Meeting January 30, 2017




2 Prostate Cancer is Common Rudy Giuliani Dx d age 55 FH+ Tx d with hormones, radiation and seeds Frank Zappa Dx d age 50 and died 2 years later. Bob Dole Dx d in 1991 Tx d with surgery Early spokesman for Viagra Joe Torre Dx d at age 58 In Tx d with surgery
3 The Prostate Gland Is an exocrine gland. Secretes fluid that makes up 20 to 30% of semen. Seminal vesicles make most of the fluid. Is situated just under the urinary bladder and surrounds the origin of the urethra. It is about the size of a walnut and weighs about 20 to 30 grams. An enlarged prostate can weigh up to 100 grams. Can be affected by prostatitis, benign prostate hyperplasia and cancer. The prostate needs male hormones (androgens) to function. Mainly testosterone in the form of DHT. It s the Rodney Dangerfield of organs

4 Prostate Anatomy
5 Prostate Cancer (PCa) Stats Incidence PCa is the most common cancer in men 181,000 new cases in 2016 (10.7% of all new cancer cases) Lifetime risk of developing prostate cancer = 16% Mortality PCa is the second leading cause of cancer death for men, next to lung cancer 26,100 deaths in 2015 Risk of dying of prostate cancer = 2.9% More than 2.5 million men in the US are living with prostate cancer CA CANCER J CLIN 2016;66:7
6 Leading Cancer Types 2015 CA: A Cancer Journal for Clinicians Volume 65 Number 1, pages 5-29, 5 JAN 2015 DOI: /caac.21254
7 Trends in PCa Incidence and Mortality Rates Data from SEER Program, NCI
8 PCa Risk Factors Age rare under age 45. Most cases over age 65 Race/ethnicity More common in African-American men. Less common in Asian and Hispanic men. Family History Having a father or brother with prostate cancer more than doubles your risk. However most PCa occurs in men without a family history of it. Genetics some gene changes increase PCa risk BRCA1 and BRCA2 increase PCa risk in men Lynch Syndrome (aka HNPCC) increases risk for a number of cancers including Pca Hx of PIN malignant cells are contained within individual ducts and glands (prostatic intraepithelial neoplasia) Questionable RF s diet, obesity, smoking, chemical exposures, hx of prostatitis, hx of std s, hx of vasectomy
9 Percent of New Cases by Age Group Percent of New Cases by Age Group 32.9% 37.6% % 9.5% 3.8% 0 0.6% < >84 Median Age at Diagnosis = 66
10 Percent of Deaths by Age Group 40% 35% 30% 35.1% 33.5% 25% 20% 20.8% 15% 10% 5% 0% 9.0% 0% 0.1% 1.6% < >84 Median Age at Death = 80
11 Prostate Cancer Prevalence Autopsy studies show that prostate cancer is detected in: 30% of men age 55 60% of men age 80 Suggests that in many men prostate cancer grows so slowly that they die of other causes Int J Cancer 2015: 137:1749
12 Prostate Cancer Prevalence Estimated 2,850,139 Americans have had a prostate cancer diagnosis and are still alive Compares with: 3,069,231 with breast cancer 1,177,586 with colorectal cancer 1,034,460 with melanoma 415,707 with lung cancer These are the people we are underwriting From SEER database

13 5 year relative survival
14 Percent of Cases by Stage 4% 4% Percent by Stage 12% Localized - primary site Regional - to regional lymph nodes Distant - Metastasized Unknown 80%
15 PSA Testing PSA is a glycoprotein produced by prostate epithelial cells PSA may be elevated in men with prostate cancer (and also men with BPH or prostatitis, as well as other benign conditions) PSA was widely adopted for cancer screening in the early 1990 s and led to a dramatic increase in the incidence of prostate cancer. Survival rates also increased from 70-75% prior to PSA availability to 98.2% by Detecting more early stage cancer PSA raised incidence rates and also lowered mortality rates.
16 PSA Testing Traditional normal PSA cutoff is 4.0 ng/ml At this level: estimated sensitivity only 21%, specificity 91% For men with BPH, PSA has poor discriminating ability Positive Predictive Value (% of men with cancer) PSA s between 4 and 10 = 25% PSA s between 10 and 20 = 42 to 64% Negative Predictive Value (% of men without cancer) PSA <4.0 ng/ml = 85% No clear cut point between normal and abnormal. Setting the upper limit of normal involves a trade-off between sensitivity and specificity
17 Improving the PSA screening test Age adjusted PSA norms % free PSA Free = not protein bound Free psa/total psa = % free psa PSA density >25 % usually benign <15% not good Psa/estimated volume of the prostate (measured by TRUS) Over 0.15 = high risk PSA velocity (change over time) Rise of more than 0.75 ng/ml per year Need three readings obtained over a 12 to 24 month period
18 PSA, BPH and Rx BPH is common and often treated by medication including 5- alpha reductase inhibitors (5ARI s) Finasteride (Proscar) Dutasteride (Avodart) These reduce the volume of the prostate It has been reported that they decease PSA level by 50% after one year of treatment This must be taken into account in evaluating the psa of anyone on these drugs Tamsulosin (Flomax) and Terazosin (Hytrin) are another class of drugs and don t have this effect J Urol 2006;175:
19 PSA Testing the down side PSA cannot distinguish between aggressive and benign prostate cancers. It has been estimated that between 17-50% of men diagnosed with prostate cancer through PSA testing have tumors that would not have resulted in symptoms throughout their lifetime. Clearly there is over-treatment Therefore many men had biopsies, surgery, radiation, and other therapies that they didn t actually need. These all have side effects including erectile dysfunction, urinary incontinence, bowel problems
20 PSA screening studies These two studies have dominated the discussion The European Randomised Study of Screening Prostate Cancer (ERSPC) studied 162,000 men aged 50-74, after 13 years of follow-up routine PSA testing reduced the number of PC deaths by 21% and lowered the risk of advanced PC. It was calculated that 37 additional men need to be dx d with PCa through screening to save 1 PCa death On the other hand the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial found that between 1993 and 2001 PSA screening appeared to have no mortality benefits compared with a DRE. ERSPC study Lancet. 2014;384: PLCO study J Natl Cancer Inst. 2012;104:
21 PSA Screening Recommendations In 2012 the US Preventive Services Task Force (USPSTF) issued a recommendation against PSA screening for men of all ages who do not have symptoms This was met by criticism this could take us back to an era when prostate cancer was often discovered at advanced and incurable stages The CDC supported the USPSTF s recommendations The American Cancer Society did not provide a recommendation, instead emphasizing that men must make an informed decision with their doctor (starting age 50) The PLCO trial was reinvestigated in 2016 and found to be flawed. The recommendation is being revisited.
, treated robotic laparoscopic prostatectomy.")
22 PSA test saved my life Ben Stiller Baseline PSA suggested at age 46. Rising PSA, MRI, Bx showed Gleason 7 (3+4), treated robotic laparoscopic prostatectomy. Became vocal advocate for PSA testing.
23 What are the downstream effects of the 2012 recommendation? The use of PSA screening has decreased as has the incidence of early stage prostate cancer Rates of prostate bx s and radical prostatectomies has also decreased by 28.7% and 16.2% respectively Bx s due to abnormal PSA s decreased but Bx s due to surveillance actually increased. Also PC incidence overall has been decreasing. The indolent nature of most PC means that it will likely take many years to observe negative impacts JAMA Surg. Published online November 2, 2016
24 Newer tests Prostate Health Index (PHI) p2psa assay, an isoform of free psa Combined with psa and free psa by an algorithm Said to improve specificity and thereby reduce negative bx s For men age 50+, psa 2 10, and negative DRE 4K score Human kallikein-related peptidase 2, combined with total, free and intact psa in an algorithm PCA3 prostate cancer antigen 3 gene Expressed in PC but not normal or hypertrophied tissue Insufficient data for screening yet
25 Insurance Company PSA Testing Insurance companies believe in psa testing 2015 Life Underwriting Requirement Survey showed: Most companies are testing PSA at some level Age 55, $300,000 75% are testing Age 55, at some amount, 90% are testing 57% reflex to free-psa when psa is elevated Informal questioning shows no companies reducing psa testing This has been confirmed by one of the major labs
26 Insurance PSA testing results PSA Value U.S. Canada % 96.6% % 3.1% % 0.3% % 0.1% Source: Private correspondence from Exam One
27 Relative Risk (Median=1) PSA in the insurance setting Mortality Implications of PSA in Males Age Multivariate Univariate PSA This shows total mortality associated with PSA levels Source: Private correspondence from Exam One
28 Towards a Better Prostate Biopsy Unique in that we stick needles blindly into tissue...often False negative rate is 10% to 20% 12+ cores have increased the detection rate New multi-parametric mri s will improve diagnostic accuracy allow 27% of patients to avoid a primary bx as well as finding a higher percentage of clinically significant cancers
29 Gleason Grading Scale of patterns ranked 1 to 5 1 closest to normal; 5 most poorly differentiated Poorly differentiated suggests that the cancer is growing Score = primary pattern plus secondary pattern Total score = primary plus secondary score Eg. (3 + 4) = Gleason 7 Gleason score has prognostic significance *Pathologists have decided to only use Gleason patterns 3, 4 and 5. Therefore the lowest score you should see is Gleason 6 (3+3) Bear in mind that analysing biopsy slides is somewhat subjective.
30 Gleason Grading Percent cancers diagnosed on biopsy Gleason 6 = 60% to 70% Gleason 7 = 20% to 30% Gleason 8 to 10 = about 5% Which Gleason 7 is better? (3+4) or (4+3)? Gleason Grade Groups (newly adopted) Gleason Grade Gleason Grade Gleason Grade Gleason Grade 4 4+4, 3+5, 5+3 Gleason Grade 5 4+5, 5+4, 5+5
31 Clinical Staging vs Pathological Staging Radiation and active surveillance treatment = clinical staging Radical prostatectomy = pathological staging Gleason upgrading at RP is common 34% of patients were reassigned to a higher Gleason grade group (44% 3+3 and 19% of 3+4) 6% were upgraded by 2 or more Gleason grade Factors influencing upgrading Higher age (>60) Clinical stage (T2 vs. T1c) Increasing PSA % positive cores Urology 2016; 96:148
32 Prostate Cancer - TNM Stage T1 s - clinically inapparent tumor neither palpable nor visible by imaging T2 s - tumor confined within prostate T2a one-half of one lobe or less T2b more that one-half of one lobe but not both lobes T2c invades both lobes T3 s Tumor extends through the prostate capsule T3a extracapsular extension T3b extends to seminal vesicles T4 Tumor is fixed or invades adjacent structures other than seminal vesicles pt = pathologic staging
33 Risk Stratification Methods The D Amico classification Low Risk: PSA less than or equal to 10 Gleason score less than or equal to 6 And clinical stage T1-2a Intermediate Risk: PSA between 10 and 20 Gleason score 7 Clinical stage T2b High Risk: PSA more than 20 Gleason score 8 or more Clinical stage T2c 3a Commonly used but does not account for multiple risk factors
34 Risk Stratification Nomograms (online calculators) Use multiple variables to produce models that predict likelihood of disease progression or recurrence Memorial Sloan Kettering Cancer Center provides several at their website 4 prostate cancer calculators: Pre-radical prostatectomy Post-radical prostatectomy Salvage radiation therapy Risk of dying of prostate cancer in men with a rising psa after radical prostatectomy Based on MSK data which may be more favorable experience than average
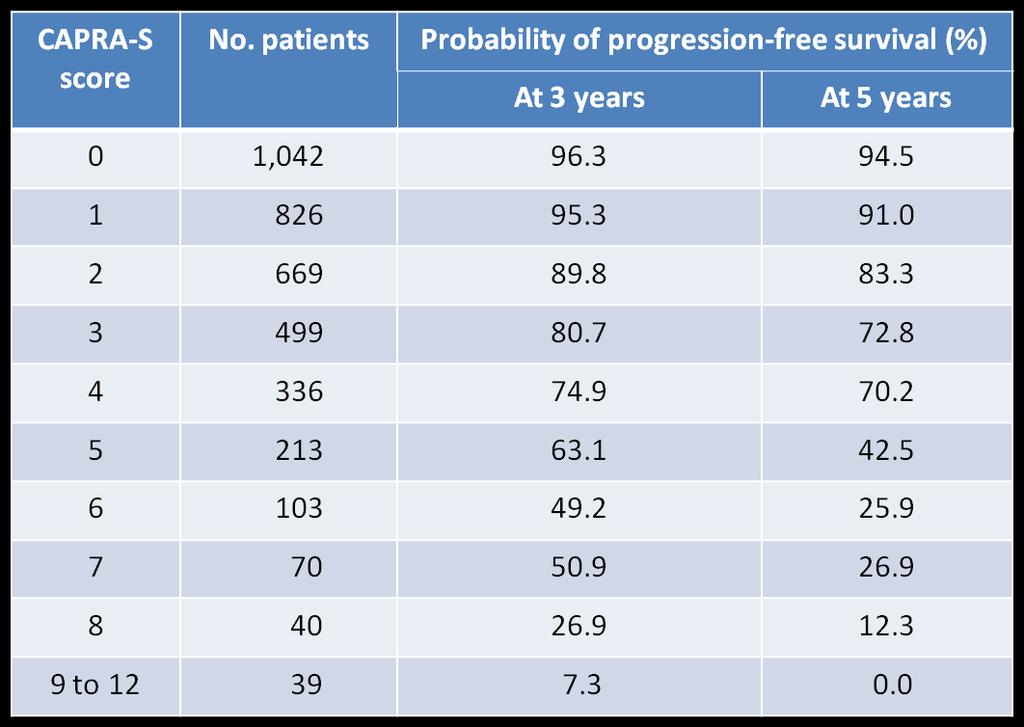
35 Risk Stratification - UCSF-CAPRA score Based on 5 variables (age, PSA, Gleason score, T stage, % of bx cores) Gives you a score from 0 to 10 (0-2 = low risk, 3-5 intermediate risk, 6-10 high risk) Data from CAPSURE, from 40 mostly community based sites, therefore may be more real life experience CAPRA (S) is for predicting recurrence after surgery, gives a score from 0 to 12
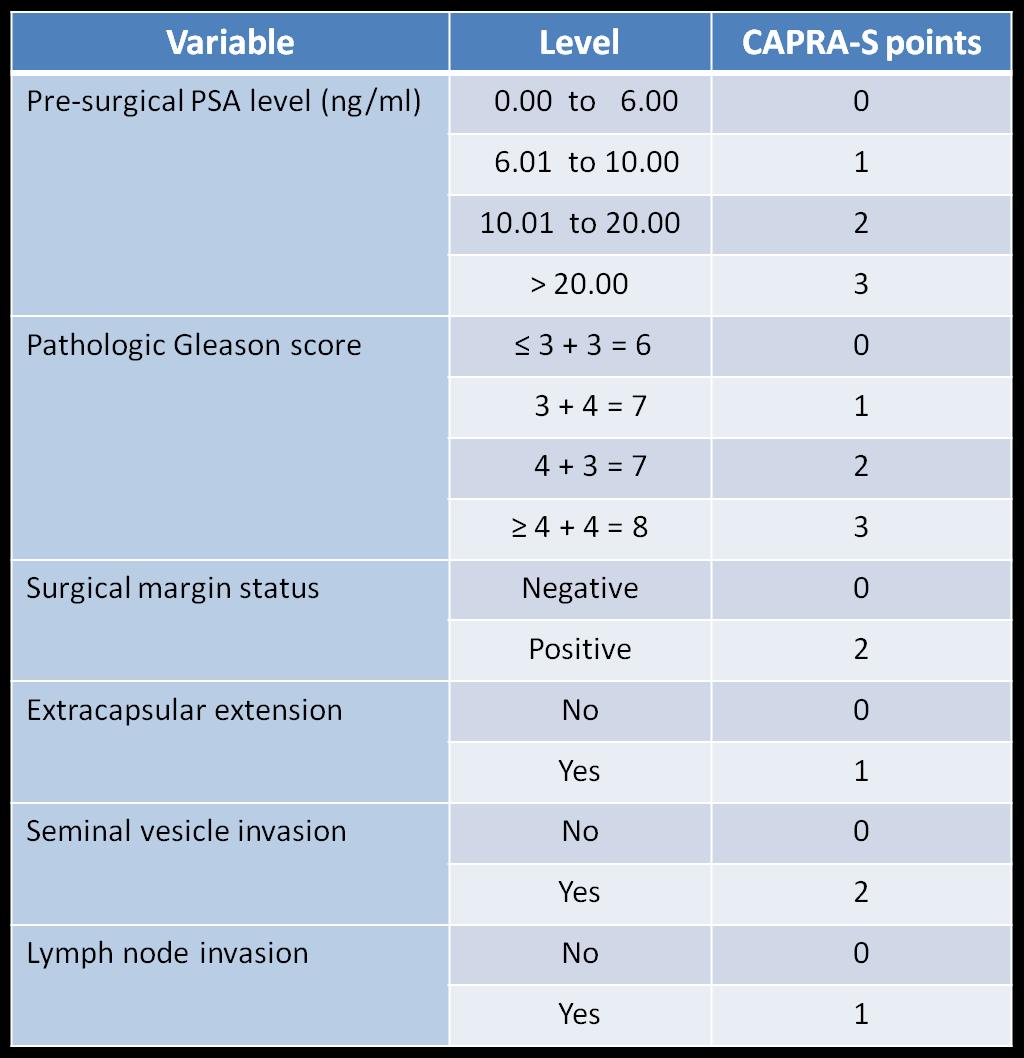
36 CAPRA (S) Calculation
37
38 Anatomic Stage/Prognostic Groups for Risk Stratification Stage T N M PSA* Gleason T1a-c N0 M0 PSA < 10 Gleason 6 I T2a N0 M0 PSA < 10 Gleason 6 T1-T2a N0 M0 PSA X Gleason X T1a-c N0 M0 PSA < 20 Gleason 7 T1a-c N0 M0 PSA 10 but < 20 Gleason 6 IIA T2a N0 M0 PSA < 20 Gleason 7 T2b N0 M0 PSA < 20 Gleason 7 T2b N0 M0 PSA X Gleason X T2c N0 M0 Any PSA Any Gleason IIB T1-2 N0 M0 PSA 20 Any Gleason T1-2 N0 M0 Any PSA Gleason 8 III T3a-b N0 M0 Any PSA Any Gleason T4 N0 M0 Any PSA Any Gleason IV Any T N1 M0 Any PSA Any Gleason Any T Any N M1 Any PSA Any Gleason
39 Treatment of Localized PCa Most dx d PCa s are clinically localized (organ confined) Choice of Tx depends on risk stratification (stage, Gleason grade, baseline PSA, extent in # of bx cores involved) combined with age and health, personal preference Radical Prostatectomy Open or robotic Radiation Therapy External beam Brachytherapy Active Surveillance Other Treatments: Androgen Deprivation therapy (ADT) not recommended as primary therapy, but is used as adjuvant therapy Ablation Therapy cryotherapy and HIFU outcomes not well established
40 Radical Prostatectomy Suitable for tumors confined to the prostate Patient must be in good health Can be done by perineal or retropubic approach; or by laparoscopy/robotic nerve sparing surgery available, however potency rates considerably under 100% There will be a path report Margin positive disease and seminal vesicle invasion are poor prognostic signs which may lead to recurrence PSA should be undetectable within 6 weeks Biochemical recurrence = PSA 0.2 ng/ml confirmed by a second test result. Complications = incontinence and ED
41 Radiation Therapy RT Goal of RT therapeutic dose while minimizing radiation to normal tissues Both external beam and brachytherapy are widely used as a single modality Now using intensity modulated (IMRT) radio therapy; will see more of the Cyberknife Staging not based on surgical path report, clinical only Some prostatic tissue will remain so PSA levels will not fall to undetectable levels Criteria for biochemical recurrence: An increase of 2.0 ng/ml greater than the nadir after radiotherapy Complications = radiation proctitis, urinary problems, ED
42 Active Surveillance #1 Not the same as watchful waiting Watchful waiting: Alternative for elderly men with limited life expectancy and/or substantial co-morbidity. No intent to have definitive Tx. Active Surveillance: For men with localized, well-differentiated prostate cancer, thought to be at low risk for progression Postpone immediate definitive therapy The patient is monitored regularly by psa, dre and biopsy Definitive treatment to be used if there is evidence of progression Twin Goals of reducing overtreatment and identifying lethal tumors while still treatable
43 Active Surveillance #2 Assumption for many men Tx may never be needed or can be postponed for many years without significantly reducing the chances for a cure Growth rate of prostate cancer is slow and relatively constant over time (unlike most other cancers) Selection of appropriate patients is the critical issue. PSA < 10 ng/ml Normal DRE Gleason score of 6 or less May also look at: Number of positive cores, percentage of positive cores, extent of tumor involvement within a biopsy core PSA density and PSA kinetics J Urol 2005; 174:1785.
44 Active Surveillance #3 Johns Hopkins AS experience 1,300 men, ave. age 66 2/3 very low risk, 1/3 low risk 0.4% developed metastatic disease or died of prostate cancer at 15 years Risk of death from a cause other than prostate cancer 24 to 1 Over 15 years, 5% of men developed an aggressive cancer (Gleason 4 +3 or greater) J Clin Oncol 33:
45 Comparison of Treatments RP, RT and brachytherapy all provide biochemical relapse-free survival of 80% or more in studies of 5 to 10 years More than 95% of patients remain free of local recurrence and distant mets For low risk disease there is not much difference between these therapies. For higher risk disease there is no consensus as to which treatment is best The most reliable studies suggest that the difference in 10 year cancer specific survival between RP and RT are small, possibly <1%. Int J Radiation Oncology, Biology, Physics. Aug 2015
46 Comparison of Treatments ProtecT Trial 10 year study, 1999 to 2009, designed to directly compare surgery, radiotherapy and active monitoring, for low and intermediate risk PCa looking at freedom from mets, prostate cancer specific survival and overall survival 1,643 men enrolled, ages 50 69, comparable numbers in each group. No difference in overall survival Prostate cancer survival was not significantly different among the three groups (PC mortality was about 1% in each group 17 actual prostate cancer deaths), The active monitoring group had a higher rate of disease progression and metastases Men over 65 were a little more likely to die of PC if in the active monitoring group N Engl J Med 2016; 375:1415
47 Recurrence Each year nearly 60,000 men undergo radical prostatectomy Approx 15 to 40% will experience cancer recurrence within 5 years, usually manifested only by PSA level (biochemical recurrence) Must rule out distant metastases as the cause If disease is confined to prostatic bed then salvage RT may prolong disease-free survival If left untreated most of those with biochemical or local recurrence will develop metastases and die of PC (8 years to clinical metastases and 5 more years to die) Better outcome with T2 vs T3, neg vs pos surgical margins, Gleason 6 vs 7 or 8, lower pre RT PSA
48 Recurrence A study of 635 US men undergoing radical prostatectomy from , followed through 12/07 and experienced biochemical and/or recurrence 397 received no salvage radiation 160 received salvage radiotherapy alone 78 received salvage radiotherapy and hormone treatment There were 119 deaths Salvage radiotherapy group had a 3-fold increase in PC specific survival and also increased overall survival. Best result if initiated shortly after biochemical recurrence JAMA, June 18, 2008, Vol. 299, No 23
49 Case #1 Male age 61 applying for $1,000,000 No Sx, no FH of PC, DRE neg. Moderate enlargement 2004 seen for rising PSA of 3.6 (12% free) Bx focal HG PIN 2009 PSA 5.4 (14% free) Bx focal HG PIN and ASAP 2/10 PSA 7.0 3/11 start Rx Avodart 4/11 PSA 3.8 4/11 Bx Benign BPH 3/13 stopped Avodart due to side effects 5/15 PSA 9.2 (10% free) 6/15 PSA 6.1 (15% free)
50 Case #2 Male age 77 applying for $5,000, PC on bx, one core Gleason 6, followed by Active Surveillance 2008 Bx similar 2009 Bx two cores of Gleason Bx neg for malignancy 7/12 Bx 3 cores of Gleason 7, PSA 4.3 3/13 MRI multi-focal tumor in the prostate, no capsular invasion; susp left iliac bone lesion, to have bone scan 4/13 robot assisted radical prostatectomy, Gleason 8 (3+5), confined to prostate, peri-neural invasion, T2N0Mx 5/13 PSA less than /15 PSA still undetectable
51 Case #3 Male age 71 applying for $350, radical prostatectomy, Gleason 7, capsular invasion 2007 salvage radiation 2014 PSA < PSA < post-op urinary retention, bladder neck contracture, dilated 10/16 insurance PSA <0.04
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Prostate Cancer Incidence
 Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Prostate Cancer. David Wilkinson MD Gulfshore Urology
 Prostate Cancer David Wilkinson MD Gulfshore Urology What is the Prostate? Male Sexual Gland Adds nutrients and fluids for sperm This fluid is added to sperm during ejaculation Urethra (urine channel)
Prostate Cancer David Wilkinson MD Gulfshore Urology What is the Prostate? Male Sexual Gland Adds nutrients and fluids for sperm This fluid is added to sperm during ejaculation Urethra (urine channel)
Prostate-Specific Antigen (PSA) Test
 Test") Prostate-Specific Antigen (PSA) Test What is the PSA test? Prostate-specific antigen, or PSA, is a protein produced by normal, as well as malignant, cells of the prostate gland. The PSA test measures the
Prostate-Specific Antigen (PSA) Test What is the PSA test? Prostate-specific antigen, or PSA, is a protein produced by normal, as well as malignant, cells of the prostate gland. The PSA test measures the
Introduction. Growths in the prostate can be benign (not cancer) or malignant (cancer).
 or malignant (cancer).") This information was taken from urologyhealth.org. Feel free to explore their website to learn more. Another trusted website with good information is the national comprehensive cancer network (nccn.org).
This information was taken from urologyhealth.org. Feel free to explore their website to learn more. Another trusted website with good information is the national comprehensive cancer network (nccn.org).
When to worry, when to test?
 Focus on CME at the University of Calgary Prostate Cancer: When to worry, when to test? Bryan J. Donnelly, MSc, MCh, FRCSI, FRCSC Presented at a Canadian College of Family Practitioner s conference (October
Focus on CME at the University of Calgary Prostate Cancer: When to worry, when to test? Bryan J. Donnelly, MSc, MCh, FRCSI, FRCSC Presented at a Canadian College of Family Practitioner s conference (October
Elevated PSA. Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017
 Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Fellow GU Lecture Series, Prostate Cancer. Asit Paul, MD, PhD 02/20/2018
 Fellow GU Lecture Series, 2018 Prostate Cancer Asit Paul, MD, PhD 02/20/2018 Disease Burden Screening Risk assessment Treatment Global Burden of Prostate Cancer Prostate cancer ranked 13 th among cancer
Fellow GU Lecture Series, 2018 Prostate Cancer Asit Paul, MD, PhD 02/20/2018 Disease Burden Screening Risk assessment Treatment Global Burden of Prostate Cancer Prostate cancer ranked 13 th among cancer
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
The Selenium and Vitamin E Prevention Trial
 The largest-ever-prostate cancer prevention trial is now underway. The study will include a total of 32,400 men and is sponsored by the National Cancer Institute and a network of researchers known as the
The largest-ever-prostate cancer prevention trial is now underway. The study will include a total of 32,400 men and is sponsored by the National Cancer Institute and a network of researchers known as the
Prostate Biopsy. Prostate Biopsy. We canʼt go backwards: Screening has helped!
 We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
Newer Aspects of Prostate Cancer Underwriting
 Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10/2/2018 OBJECTIVES PROSTATE HEALTH BACKGROUND THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION
 THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION Lenette Walters, MS, MT(ASCP) Medical Affairs Manager Beckman Coulter, Inc. *phi is a calculation using the values from PSA, fpsa and p2psa
THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION Lenette Walters, MS, MT(ASCP) Medical Affairs Manager Beckman Coulter, Inc. *phi is a calculation using the values from PSA, fpsa and p2psa
Overview. What is Cancer? Prostate Cancer 3/2/2014. Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014
 Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen).
.") What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen). It is a very common cancer in men; some cancers grow very slowly,
What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen). It is a very common cancer in men; some cancers grow very slowly,
Detection & Risk Stratification for Early Stage Prostate Cancer
 Detection & Risk Stratification for Early Stage Prostate Cancer Andrew J. Stephenson, MD, FRCSC, FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Risk Stratification:
Detection & Risk Stratification for Early Stage Prostate Cancer Andrew J. Stephenson, MD, FRCSC, FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Risk Stratification:
Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement
 Clinical Review & Education JAMA US Preventive Services Task Force RECOMMENDATION STATEMENT Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement US Preventive Services
Clinical Review & Education JAMA US Preventive Services Task Force RECOMMENDATION STATEMENT Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement US Preventive Services
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT
 MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
PSA Screening and Prostate Cancer. Rishi Modh, MD
 PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
PROSTATE CANCER CONTENT CREATED BY. Learn more at
 PROSTATE CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Ask your doctor about screening and treatment options. WHAT IS PROSTATE CANCER? 4 WATCHFUL
PROSTATE CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK WITH YOUR DOCTOR Table of Contents Ask your doctor about screening and treatment options. WHAT IS PROSTATE CANCER? 4 WATCHFUL
Controversies in Prostate Cancer Screening
 Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Financial Disclosures. Prostate Cancer Screening and Surgical Management
 Prostate Cancer Screening and Surgical Management Dr. Ken Jacobsohn Director, Minimally Invasive Urologic Surgery Assistant Professor, Department of Urology Medical College of Wisconsin Financial Disclosures
Prostate Cancer Screening and Surgical Management Dr. Ken Jacobsohn Director, Minimally Invasive Urologic Surgery Assistant Professor, Department of Urology Medical College of Wisconsin Financial Disclosures
Response to United States Preventative Services Task Force draft PSA Screening recommendation: Donald B. Fuller, M.D. Genesis Healthcare Partners
 Response to United States Preventative Services Task Force draft PSA Screening recommendation: Donald B. Fuller, M.D. Genesis Healthcare Partners October 2011 Cancer Incidence Statistics, 2011 CA: A Cancer
Response to United States Preventative Services Task Force draft PSA Screening recommendation: Donald B. Fuller, M.D. Genesis Healthcare Partners October 2011 Cancer Incidence Statistics, 2011 CA: A Cancer
Chapter 2. Understanding My Diagnosis
 Chapter 2. Understanding My Diagnosis With contributions from Nancy L. Brown, Ph.D.,Palo Alto Medical Foundation Research Institute; and Patrick Swift, M.D., Alta Bates Comprehensive Cancer Program o Facts
Chapter 2. Understanding My Diagnosis With contributions from Nancy L. Brown, Ph.D.,Palo Alto Medical Foundation Research Institute; and Patrick Swift, M.D., Alta Bates Comprehensive Cancer Program o Facts
Disclosures. Prostate and Bladder Cancer: Jonathan E. Rosenberg, M.D. U.S. Cancer Statistics: Prostate Cancer Known Risk Factors
 Prostate and Bladder Cancer: 2012 Jonathan E. Rosenberg, M.D. Associate Attending Section Head, Non-Prostate Genitourinary Oncology Service Memorial Sloan-Kettering Cancer Center Disclosures Consulting
Prostate and Bladder Cancer: 2012 Jonathan E. Rosenberg, M.D. Associate Attending Section Head, Non-Prostate Genitourinary Oncology Service Memorial Sloan-Kettering Cancer Center Disclosures Consulting
Prostate Cancer: Screening, Treatment, and Survivorship
 Prostate Cancer: Screening, Treatment, and Survivorship Timothy C. Brand, MD, FACS LTC(P), MC, USA Urology Residency Director Associate Professor of Surgery, USUHS Madigan Army Medical Center No Disclosures
Prostate Cancer: Screening, Treatment, and Survivorship Timothy C. Brand, MD, FACS LTC(P), MC, USA Urology Residency Director Associate Professor of Surgery, USUHS Madigan Army Medical Center No Disclosures
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
PROSTATE CANCER: A Primer of Diagnosis and Treatment. Jay C. Lee, MD, FRCSC Clinical Associate Professor University of Calgary
 PROSTATE CANCER: A Primer of Diagnosis and Treatment Jay C. Lee, MD, FRCSC Clinical Associate Professor University of Calgary Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
PROSTATE CANCER: A Primer of Diagnosis and Treatment Jay C. Lee, MD, FRCSC Clinical Associate Professor University of Calgary Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality
 Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
3/6/2018 PROSTATE CANCER IN 2018 OBJECTIVE WHAT IS THE PROSTATE? WHAT DOES IT DO? Rahul Mehan, MD
 PROSTATE CANCER IN 2018 Rahul Mehan, MD East Valley Urology Center 6116 E Arbor Ave, Bldg 2, Suite 108 Mesa, AZ 85206 rmehan@evucenter.com www.evucenter.com Snapchat: Dr.NoodleKing OBJECTIVE Offer interactive
PROSTATE CANCER IN 2018 Rahul Mehan, MD East Valley Urology Center 6116 E Arbor Ave, Bldg 2, Suite 108 Mesa, AZ 85206 rmehan@evucenter.com www.evucenter.com Snapchat: Dr.NoodleKing OBJECTIVE Offer interactive
Objectives. Prostate Cancer Screening and Surgical Management
 Prostate Cancer Screening and Surgical Management Dr. Ken Jacobsohn Director, Minimally Invasive Urologic Surgery Assistant Professor, Department of Urology Medical College of Wisconsin Objectives Update
Prostate Cancer Screening and Surgical Management Dr. Ken Jacobsohn Director, Minimally Invasive Urologic Surgery Assistant Professor, Department of Urology Medical College of Wisconsin Objectives Update
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
2015 myresearch Science Internship Program: Applied Medicine. Civic Education Office of Government and Community Relations
 2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
GUIDELINEs ON PROSTATE CANCER
 GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
Screening and Diagnosis Prostate Cancer
 Screening and Diagnosis Prostate Cancer Daniel Heng MD MPH FRCPC Chair, Genitourinary Tumor Group Tom Baker Cancer Center University of Calgary, Canada @DrDanielHeng Outline Screening Evidence Recommendations
Screening and Diagnosis Prostate Cancer Daniel Heng MD MPH FRCPC Chair, Genitourinary Tumor Group Tom Baker Cancer Center University of Calgary, Canada @DrDanielHeng Outline Screening Evidence Recommendations
BLADDER PROSTATE PENIS TESTICLES BE YO ND YO UR CA NC ER
 BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
Questions and Answers about Prostate Cancer Screening with the Prostate-Specific Antigen Test
 Questions and Answers about Prostate Cancer Screening with the Prostate-Specific Antigen Test About Cancer Care Ontario s recommendations for prostate-specific antigen (PSA) screening 1. What does Cancer
Questions and Answers about Prostate Cancer Screening with the Prostate-Specific Antigen Test About Cancer Care Ontario s recommendations for prostate-specific antigen (PSA) screening 1. What does Cancer
Prostate Cancer: Is There Standard Treatment? Who has prostate cancer? In this article:
 Focus on CME at l Université de Montréal Prostate Cancer: Is There Standard Treatment? Pierre I. Karakiewicz, MD, FRCSC; Paul Perrotte, MD, FRCSC; Fred Saad, MD, FRCSC In this article: 1. Risk factors
Focus on CME at l Université de Montréal Prostate Cancer: Is There Standard Treatment? Pierre I. Karakiewicz, MD, FRCSC; Paul Perrotte, MD, FRCSC; Fred Saad, MD, FRCSC In this article: 1. Risk factors
The Changing Landscape of Prostate Cancer
 The Changing Landscape of Prostate Cancer helping make the complicated, understandable Marc B. Garnick, MD FACP Clinical Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School
The Changing Landscape of Prostate Cancer helping make the complicated, understandable Marc B. Garnick, MD FACP Clinical Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC
 PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
Prostate Overview Quiz
 Prostate Overview Quiz 1. The path report reads: Gleason 3 + 4 = 7. The Gleason s score is a. 3 b. 4 c. 7 d. None of the above 2. The path report reads: Moderately differentiated adenocarcinoma of the
Prostate Overview Quiz 1. The path report reads: Gleason 3 + 4 = 7. The Gleason s score is a. 3 b. 4 c. 7 d. None of the above 2. The path report reads: Moderately differentiated adenocarcinoma of the
Chapter 18: Glossary
 Chapter 18: Glossary Sutter Health Cancer Service Line: Prostate Committee Advanced cancer: When the cancer has spread to other parts of the body (including lymph nodes, bones, or other organs) and is
Chapter 18: Glossary Sutter Health Cancer Service Line: Prostate Committee Advanced cancer: When the cancer has spread to other parts of the body (including lymph nodes, bones, or other organs) and is
HIGH MORTALITY AND POOR SURVIVAL OF MEN WITH PROSTATE CANCER IN RURAL AND REMOTE AUSTRALIA
 HIGH MORTALITY AND POOR SURVIVAL OF MEN WITH PROSTATE CANCER IN RURAL AND REMOTE AUSTRALIA The prostate is a small gland the size of a walnut which produces fluid to protect and lubricate the sperm It
HIGH MORTALITY AND POOR SURVIVAL OF MEN WITH PROSTATE CANCER IN RURAL AND REMOTE AUSTRALIA The prostate is a small gland the size of a walnut which produces fluid to protect and lubricate the sperm It
Where are we with PSA screening?
 Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
2008_Prostate_Awareness 12/22/08 1:47 PM Page 1
 2008_Prostate_Awareness 12/22/08 1:47 PM Page 1 2008_Prostate_Awareness 12/22/08 1:47 PM Page 2 A Message from Dr. Frank Critz Prostate cancer is the most common cancer in men, other than skin cancers.
2008_Prostate_Awareness 12/22/08 1:47 PM Page 1 2008_Prostate_Awareness 12/22/08 1:47 PM Page 2 A Message from Dr. Frank Critz Prostate cancer is the most common cancer in men, other than skin cancers.
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet
 S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet Why HIFU? Efficacy demonstrated Real time control of the target Early control of the necrosis area is possible with MRI or TRUS using contrast
S Crouzet, O Rouvière, JY Chapelon, F Mege, X martin, A Gelet Why HIFU? Efficacy demonstrated Real time control of the target Early control of the necrosis area is possible with MRI or TRUS using contrast
Prostate Cancer. Biomedical Engineering for Global Health. Lecture Fourteen. Early Detection. Prostate Cancer: Statistics
 Biomedical Engineering for Global Health Lecture Fourteen Prostate Cancer Early Detection Prostate Cancer: Statistics Prostate gland contributes enzymes, nutrients and other secretions to semen. United
Biomedical Engineering for Global Health Lecture Fourteen Prostate Cancer Early Detection Prostate Cancer: Statistics Prostate gland contributes enzymes, nutrients and other secretions to semen. United
PROSTATE CANCER 101 WHAT IS PROSTATE CANCER?
 PROSTATE CANCER 101 WHAT IS PROSTATE CANCER? Prostate cancer is cancer that begins in the prostate. The prostate is a walnut-shaped gland in the male reproductive system located below the bladder and in
PROSTATE CANCER 101 WHAT IS PROSTATE CANCER? Prostate cancer is cancer that begins in the prostate. The prostate is a walnut-shaped gland in the male reproductive system located below the bladder and in
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
1. Benign Prostate Hyperplexia (BPH) 2. Prostate Cancer (PCa)
 2. Prostate Cancer (PCa)") Objectives: Our first segment focused in the anatomy and functions of the prostate gland, to get a clear understanding of the male Genito-Urinary System. Now, we will explore two of the main problems associated
Objectives: Our first segment focused in the anatomy and functions of the prostate gland, to get a clear understanding of the male Genito-Urinary System. Now, we will explore two of the main problems associated
Questions and Answers About the Prostate-Specific Antigen (PSA) Test
 Test") CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Questions and Answers
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Questions and Answers
The Royal Marsden. Prostate case study. Presented by Mr Alan Thompson Consultant Urological Surgeon
 Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer
 Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer Gleason score Gleason score 2-4: well differentiated (seldom reported now): Low risk
Causes of Raised PSA A very large prostate Gland Infection of urine or Prostate Gland Possibility of prostate Cancer Gleason score Gleason score 2-4: well differentiated (seldom reported now): Low risk
Providing Treatment Information for Prostate Cancer Patients
 Providing Treatment Information for Prostate Cancer Patients For all patients with localized disease on biopsy For all patients with adverse pathology after prostatectomy See what better looks like Contact
Providing Treatment Information for Prostate Cancer Patients For all patients with localized disease on biopsy For all patients with adverse pathology after prostatectomy See what better looks like Contact
MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of
 POLICY: PG0367 ORIGINAL EFFECTIVE: 08/26/16 LAST REVIEW: 09/27/18 MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of Prostate Cancer GUIDELINES This policy does not certify
POLICY: PG0367 ORIGINAL EFFECTIVE: 08/26/16 LAST REVIEW: 09/27/18 MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of Prostate Cancer GUIDELINES This policy does not certify
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Navigating the Stream: Prostate Cancer and Early Detection. Ifeanyi Ani, M.D. TPMG Urology Newport News
 Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Compliments of. In Partnership with. NewsTalk WSB s Scott Slade, Neal Boortz and Captain Herb Emory
 Compliments of In Partnership with NewsTalk WSB s Scott Slade, Neal Boortz and Captain Herb Emory A Message from the Radiotherapy Clinics of Georgia Prostate cancer is the most common cancer in men, other
Compliments of In Partnership with NewsTalk WSB s Scott Slade, Neal Boortz and Captain Herb Emory A Message from the Radiotherapy Clinics of Georgia Prostate cancer is the most common cancer in men, other
Localized Prostate Cancer and Its Treatment- A Patient Guide
 Your Health Matters Localized Prostate Cancer and Its Treatment- A Patient Guide Department of Urology UCSF Helen Diller Family Comprehensive Cancer Center University of California. San Francisco 550 16th
Your Health Matters Localized Prostate Cancer and Its Treatment- A Patient Guide Department of Urology UCSF Helen Diller Family Comprehensive Cancer Center University of California. San Francisco 550 16th
Prostate Cancer Update 2017
 Prostate Cancer Update 2017 Arthur L. Burnett, MD, MBA, FACS Patrick C. Walsh Distinguished Professor of Urology The James Buchanan Brady Urological Institute The Johns Hopkins Medical Institutions Baltimore,
Prostate Cancer Update 2017 Arthur L. Burnett, MD, MBA, FACS Patrick C. Walsh Distinguished Professor of Urology The James Buchanan Brady Urological Institute The Johns Hopkins Medical Institutions Baltimore,
Prostate Cancer. What is the prostate?
 Prostate Cancer Prostate cancer is the third-leading cause of cancer deaths among men in the United States. Yet, when detected in its early stages, prostate cancer can be effectively treated and cured.
Prostate Cancer Prostate cancer is the third-leading cause of cancer deaths among men in the United States. Yet, when detected in its early stages, prostate cancer can be effectively treated and cured.
Prostate Cancer Innovations in Surgical Strategies Update 2007!
 Prostate Cancer Innovations in Surgical Strategies Update 2007! Curtis A. Pettaway, M.D. Professor Department of Urology The University of Texas M. D. Anderson Cancer Center Radical Prostatectomy Pathologic
Prostate Cancer Innovations in Surgical Strategies Update 2007! Curtis A. Pettaway, M.D. Professor Department of Urology The University of Texas M. D. Anderson Cancer Center Radical Prostatectomy Pathologic
AFTER DIAGNOSIS: PROSTATE CANCER Understanding Your Treatment Options
 AFTER DIAGNOSIS: PROSTATE CANCER Understanding Your Treatment Options INTRODUCTION This booklet describes how prostate cancer develops, how it affects the body and the current treatment methods. Although
AFTER DIAGNOSIS: PROSTATE CANCER Understanding Your Treatment Options INTRODUCTION This booklet describes how prostate cancer develops, how it affects the body and the current treatment methods. Although
Contemporary Approaches to Screening for Prostate Cancer
 Contemporary Approaches to Screening for Prostate Cancer Gerald L. Andriole, MD Robert K. Royce Distinguished Professor Chief of Urologic Surgery Siteman Cancer Center Washington University School of Medicine
Contemporary Approaches to Screening for Prostate Cancer Gerald L. Andriole, MD Robert K. Royce Distinguished Professor Chief of Urologic Surgery Siteman Cancer Center Washington University School of Medicine
Prostate Cancer Screening. Eric Shreve, MD Bend Urology Associates
 Prostate Cancer Screening Eric Shreve, MD Bend Urology Associates University of Cincinnati Medical Center University of Iowa Hospitals and Clinics PSA Human kallikrein 3 Semenogelin is substrate Concentration
Prostate Cancer Screening Eric Shreve, MD Bend Urology Associates University of Cincinnati Medical Center University of Iowa Hospitals and Clinics PSA Human kallikrein 3 Semenogelin is substrate Concentration
The U.S. Preventive Services Task Force (USPSTF) makes
 makes") Annals of Internal Medicine Clinical Guideline Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement Virginia A. Moyer, MD, MPH, on behalf of the U.S. Preventive Services
Annals of Internal Medicine Clinical Guideline Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement Virginia A. Moyer, MD, MPH, on behalf of the U.S. Preventive Services
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
Prostate Cancer. Axiom. Overdetection Is A Small Issue. Reducing Morbidity and Mortality
 Overdetection Is A Small Issue (in the context of decreasing prostate cancer mortality rates and with appropriate, effective, and high-quality treatment) Prostate Cancer Arises silently Dwells in a curable
Overdetection Is A Small Issue (in the context of decreasing prostate cancer mortality rates and with appropriate, effective, and high-quality treatment) Prostate Cancer Arises silently Dwells in a curable
General information about prostate cancer
 Prostate Cancer General information about prostate cancer Key points Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the prostate. Signs of prostate cancer include
Prostate Cancer General information about prostate cancer Key points Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the prostate. Signs of prostate cancer include
PCA MORTALITY VS TREATMENTS
 PCA MORTALITY VS TREATMENTS Terrence P McGarty White Paper No 145 July, 2017 In a recent NEJM paper the authors argue that there is no material difference between a prostatectomy and just "observation"
PCA MORTALITY VS TREATMENTS Terrence P McGarty White Paper No 145 July, 2017 In a recent NEJM paper the authors argue that there is no material difference between a prostatectomy and just "observation"
PROSTATE CANCER 101 WHAT IS PROSTATE CANCER?
 PROSTATE CANCER 101 WHAT IS PROSTATE CANCER? Prostate cancer is cancer that begins in the prostate. The prostate is a walnut-shaped gland in the male reproductive system located below the bladder and in
PROSTATE CANCER 101 WHAT IS PROSTATE CANCER? Prostate cancer is cancer that begins in the prostate. The prostate is a walnut-shaped gland in the male reproductive system located below the bladder and in
THE HISTORY AND EVOLUTION OF PROSTATE CANCER DIAGNOSIS AND TREATMENT BY: DR. ANDREW GROLLMAN ALBUQUERQUE UROLOGY ASSOCIATES
 THE HISTORY AND EVOLUTION OF PROSTATE CANCER DIAGNOSIS AND TREATMENT BY: DR. ANDREW GROLLMAN ALBUQUERQUE UROLOGY ASSOCIATES OVERVIEW Diagnosis Laboratory Tests PSA Free and Total PSA PCA-3 4K Score The
THE HISTORY AND EVOLUTION OF PROSTATE CANCER DIAGNOSIS AND TREATMENT BY: DR. ANDREW GROLLMAN ALBUQUERQUE UROLOGY ASSOCIATES OVERVIEW Diagnosis Laboratory Tests PSA Free and Total PSA PCA-3 4K Score The
Collaborative Staging
 Slide 1 Collaborative Staging Site-Specific Instructions Prostate 1 In this presentation, we are going to take a closer look at the collaborative staging data items for the prostate primary site. Because
Slide 1 Collaborative Staging Site-Specific Instructions Prostate 1 In this presentation, we are going to take a closer look at the collaborative staging data items for the prostate primary site. Because
Tumor Markers Yesterday, Today & Tomorrow. Steven E. Zimmerman M.D. Vice President & Chief Medical Director
 Tumor Markers Yesterday, Today & Tomorrow Steven E. Zimmerman M.D. Vice President & Chief Medical Director Tumor Marker - Definition Substances produced by cancer cells or other cells in response to cancer
Tumor Markers Yesterday, Today & Tomorrow Steven E. Zimmerman M.D. Vice President & Chief Medical Director Tumor Marker - Definition Substances produced by cancer cells or other cells in response to cancer
Prostate Cancer Case Study 1. Medical Student Case-Based Learning
 Prostate Cancer Case Study 1 Medical Student Case-Based Learning The Case of Mr. Powers Prostatic Nodule The effervescent Mr. Powers is found by his primary care provider to have a prostatic nodule. You
Prostate Cancer Case Study 1 Medical Student Case-Based Learning The Case of Mr. Powers Prostatic Nodule The effervescent Mr. Powers is found by his primary care provider to have a prostatic nodule. You
If you have aggressive cancer, you would want treatment in time for a cure.
 Prostate cancer: PSA screening, biopsy, new technologies The treatment/cure should never be worse than the disease. If you have aggressive cancer, you would want treatment in time for a cure. What is PSA?
Prostate cancer: PSA screening, biopsy, new technologies The treatment/cure should never be worse than the disease. If you have aggressive cancer, you would want treatment in time for a cure. What is PSA?
Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
PROSTATE CANCER. Mr. Jawad Islam. Consultant Urologist. MBBS, MSc, FRCS(Ed), FEBU, FRCS(Urology) People Centred Positive Compassion Excellence
, FEBU, FRCS(Urology) People Centred Positive Compassion Excellence") PROSTATE CANCER Mr. Jawad Islam MBBS, MSc, FRCS(Ed), FEBU, FRCS(Urology) Consultant Urologist Where is prostate located and what is its function? What is prostate cancer? How common is prostate cancer?
PROSTATE CANCER Mr. Jawad Islam MBBS, MSc, FRCS(Ed), FEBU, FRCS(Urology) Consultant Urologist Where is prostate located and what is its function? What is prostate cancer? How common is prostate cancer?
Outcomes of Radical Prostatectomy in Thai Men with Prostate Cancer
 Original Article Outcomes of Radical Prostatectomy in Thai Men with Prostate Cancer Sunai Leewansangtong, Suchai Soontrapa, Chaiyong Nualyong, Sittiporn Srinualnad, Tawatchai Taweemonkongsap and Teerapon
Original Article Outcomes of Radical Prostatectomy in Thai Men with Prostate Cancer Sunai Leewansangtong, Suchai Soontrapa, Chaiyong Nualyong, Sittiporn Srinualnad, Tawatchai Taweemonkongsap and Teerapon
Prostate Cancer- Screening and Selected Treatment Dilemmas COPYRIGHT. Marc B. Garnick MD. Update in Internal Medicine.
 Prostate Cancer- Screening and Selected Treatment Dilemmas Marc B. Garnick MD Update in Internal Medicine 4 December 2016 Financial Disclosures Marc B. Garnick MD, FACP Gorman Brothers Clinical Professor
Prostate Cancer- Screening and Selected Treatment Dilemmas Marc B. Garnick MD Update in Internal Medicine 4 December 2016 Financial Disclosures Marc B. Garnick MD, FACP Gorman Brothers Clinical Professor
11/10/2015. Prostate cancer in the U.S. Multi-parametric MRI of Prostate Diagnosis and Treatment Planning. NIH estimates for 2015.
 Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer
 Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer after prostatectomy, radiation therapy and HiFU R. Schwartzberg, E. Günther, N. Klein, S. Zapf, R. El-Idrissi, J. Cooper, B.
Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer after prostatectomy, radiation therapy and HiFU R. Schwartzberg, E. Günther, N. Klein, S. Zapf, R. El-Idrissi, J. Cooper, B.
PCa Commentary. Seattle Prostate Institute CONTENTS. Volume 71 September-October 2011
 Volume 71 September-October 2011 PCa Commentary CONTENTS PERMANENT SEED BRACHYTHERAPY FOR HIGH- RISK PROSTATE CANCER: 1 CABOZANTINIB: Startling Responses Reported at June ASCO Meeting in Metastatic Castrate
Volume 71 September-October 2011 PCa Commentary CONTENTS PERMANENT SEED BRACHYTHERAPY FOR HIGH- RISK PROSTATE CANCER: 1 CABOZANTINIB: Startling Responses Reported at June ASCO Meeting in Metastatic Castrate
Early detection the key to prostate cancer
 Early detection the key to prostate cancer Kirby R. Early detection the key to prostate cancer. The Practitioner 2009;253 (1715):17 22 Professor Roger Kirby MA MD FRCS Director, The Prostate Centre, London
Early detection the key to prostate cancer Kirby R. Early detection the key to prostate cancer. The Practitioner 2009;253 (1715):17 22 Professor Roger Kirby MA MD FRCS Director, The Prostate Centre, London
16:30-18:30 WS #67: Urology Forum - Prostate Cancer, Stones, Renal Tumours, Voiding Dysfunction (120 minutes, not repeated) -
 -") Dr Anna Lawrence Urologist Auckland Dr Andrew Williams Urologist Auckland Madhu Koya Urologist Auckland Andrew Lienert Urologist Auckland Dr Louise Tomlinson Consultant Gynaecologist Auckland 16:30-18:30
Dr Anna Lawrence Urologist Auckland Dr Andrew Williams Urologist Auckland Madhu Koya Urologist Auckland Andrew Lienert Urologist Auckland Dr Louise Tomlinson Consultant Gynaecologist Auckland 16:30-18:30
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative