Management of Cancer Associated Thrombosis (CAT) where data is lacking. Tim Nokes Haematologist, Derriford Hospital, Plymouth
|
|
|
- Amber Andrews
- 6 years ago
- Views:
Transcription
")

1 Management of Cancer Associated Thrombosis (CAT) where data is lacking Tim Nokes Haematologist, Derriford Hospital, Plymouth
2 Contents Overview of the statistics and aetiology for Cancer Associated Thrombosis (CAT) When should we use CT scans to detect cancer in those with unprovoked VTE? Thrombocytopenia in CAT patients Recurrent VTE in CAT patients Bleeding in CAT patients
3 Cancer-associated VTE (Thein et al 2016) Cancer-associated thrombosis (CAT) accounts for about 20% of all thrombosis worldwide. Risk for VTE in cancer patients is 4-7 times higher than baseline. Risk for recurrent VTE, 3 times higher in cancer patients compared to those without Cancer. Survival of cancer patients with VTE, lower than that of patients without VTE -?effects of VTE or increased tumour aggression
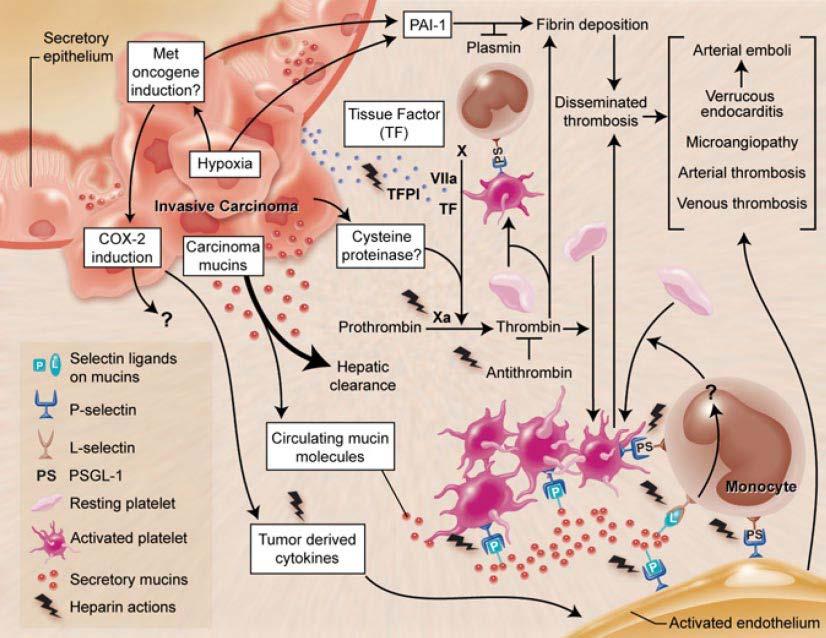
4 Why does Cancer increase the risk for VTE? (Watson H, BCSH 2015) Expression of tissue factor and cytokines on tumour cells & microparticles Interaction between tumour cells and endothelium, causing endothelial damage & platelet activation Prothrombotic properties of Mucins Mass effect impairing venous return Surgery, IV catheters, chemoradiotherapy & intercurrent medical problems eg infection
5
6 In dwelling catheter Chemotherapy Hospitalisation Surgery CANCER Radiotherapy Sepsis Imaging
7 VTE & Cancer VTE is second most common cause for death after the malignancy itself in cancer patients (Korhana 2010) Highest risk sites are: Lung, brain, pancreas, stomach, ovary, kidney, Lymphoma & Myeloma VTE + Cancer also leads to increased risk for hospitalisation, bleeding, recurrent VTE on anticoagulants (Trujilo-Santos 2008)
8 Investigating patients with unprovoked VTE for Cancer - background Historically, unprovoked VTE associated with occult cancer in 10% of patients within a year (Carrier, 2008) NICE: CG 144 (2012) states that in patients >40 years, with first unprovoked VTE, CT scan of abdomen & pelvis (& mammograms in women) is recommended. More recent data has placed the incidence of occult cancer lower at 4%
9 CT scans for unprovoked VTE CT scans convey a high exposure to radiation equivalent to 234 CXRs or 39 mammograms Psychological and biological morbidity may be associated with further investigations Significant cost associated with false positive findings ( incidentalomas ) requiring further investigations Incorrect to assume that earlier detection results in improved clinical outcomes
10 Suggested routine screening for unprovoked VTE History: Older age, smoking Worrying symptoms: Weight loss GI bleeding Constitutional symptoms Physical examination CXR Basic blood tests: FBC, Ca, LFTs, PSA, Igs, Urinalysis
11 Cancer screening in VTE (SOMIT study) 2 years follow-up Screened group 13/99 detected occult cancer by 1/12 1 cancer became apparent later Cancer related mortality 2.0% Non-screened group 10/102 developed cancer later mean of 11.6 months Cancer related mortality 3.9% Piccioli et al JTH 2004
12 VTE cancer screening: 630 idiopathic VTE Extensive Screen Standard Care All cancers 8.8% 7.3% Curable Ca 3.8% 3.8% HR 95% CI All cause mortality 7.6% 8.3% 1.22 ( ) Cancer death 5% 2.8% 1.8 ( ) Associated cost analysis: Routine screening = E165 v Extensive screening = E530 mainly investigating from false positive findings (86 patients) Van Doormaal et al JTH 2011
13 Guidance for the prevention and treatment of cancer-associated venous thromboembolism. (Korhana A. 2016) Patients with unprovoked VTE should undergo a through medical history and physical examination, basic laboratory investigations (complete blood counts, metabolic profile and liver function tests) and chest X-ray. We suggest that if not up-to-date, patients undergo age and gender-specific cancer screening (i.e. cervical, breast, prostate and colon)
14 Limited v Extensive Cancer screening in unprovoked VTE (Khan F, BMJ 2017) Study Study & (Size) Frequency of occult Cancers diagnosed Cancer deaths Quality of evidence Robertson 2015 Cochrane review of 2 studies (396) OR 1.32 (P=0.5) OR 0.49 (P=0.26) Moderate Carrier 2015 RCT (845) 19 v 14 (P=0.28) 1.4% v 0.9% (P=0.75) High Robin 2016 Prandoni 2016 RCT (394) 4 v 11 (P=0.065) 2.5% v 1.0% High RCT (195) 8 v 10 (P=0.81) 4% v 2% Moderate Salih 2016 Meta-analysis unpublished (1250) OR 1.36 (P= 0.25) OR 0.57 (P=0.22) Unknown
15 What should we tell patients currently? NICE states: Consider screening for cancer with CT Most recent data suggests 1 in 25 people with unprovoked VTE may have underlying cancer Limited evidence to support the benefit of extensive screening, particularly involving harm from ionising radiation. All such patients should receive routine cancer screening plus additional investigations depending on signs and symptoms If patients opt out of CT scanning, maintain low threshold for suspicion of cancer

16 Bleeding Thrombosis
17 Thrombocytopenia (BCSH, 2015) When present, the risk-benefit balance of anticoagulation needs reassessment In first 3 months after VTE, risk for recurrence is higher - every effort should be made to maintain safe administration of therapeutic anticoagulation. Full anticoagulation is probably safe when platelets are >50x10 9 /l (Carrier 2013)
18 Thrombocytopenia in CAT: Considerations Causes (consider potential to reverse): Chemotherapy effect ITP DIC TTP HITT Increased risks for bleeding Advanced age, Renal failure Abnormal clotting eg Vit K deficiency
19 Thrombocytopenia, Cancer & VTE BCSH, 2015 Support platelet count (to >50 x10 9 /l) to allow full dose anticoagulation to continue through highest risk period for recurrence (3/12). (2D) Temporary IVC filter should be considered if thrombocytopenia is persistent and difficult to overcome or other bleeding risk is present. If platelet count cannot be increased, then consider giving 50% dose LMWH with platelets x10 9 /l with frequent assessment (2D) Below 25 x 10 9 /l, withhold anticoagulation (1D) Some evidence that prophylactic LMWH dose may be beneficial (Drakos, 1992)

20 Thrombocytopenia in patients with CAT (Lee A, Blood : )
21 Risk of Bleeding associated with Anticoagulation in patients with CAT Increased risk for bleeding in patients with CAT receiving VKA 12%. 1/3 in initial stage of anticoagulation (Prandoni, 2002) No correlation between risk for bleeding and INR level in patients with cancer (Paleretti 2000) Similar bleeding rates: LMWH & VKA (Hull 2006) Bleeding risk in cancer patients dependent on many patient factors: Type and location of Ca, need for biopsies, thrombocytopenia, DIC, renal & liver impairment and sepsis.
22 Management of Bleeding associated with anticoagulation in patients with CAT (BCSH) Individual assessment of bleeding versus recurrent thrombotic risk before starting anticoagulation. Minor bleeding: continue full dose anticoagulation with close follow-up In patients with moderate to serious bleeding or absolute contraindications to anticoagulation: withold and consider IVC filter. Platelet transfusions may allow anticoagulation according to previous flow-chart
23 Recurrent VTE in cancer patients Cancer confers higher risk for recurrent VTE than those without cancer (4-fold increase) - Both during & after anticoagulation Assess for compliance with anticoagulation Assess for mechanical compression of large vein from tumour masses Consider HITT Registries show very heterogeneous approach to recurrent VTE in patients with cancer
24 Anticoagulation for Recurrent VTE in CAT The optimal duration of primary anticoagulation in CAT is unknown (NICE suggests 6 months & review) Patients with recurrent VTE can either be: Bridged with LMWH if on VKA Transitioned to treatment dose LMWH if already using prophylaxis Treated with full dose escalation (eg Enoxaparin 1mg/kg twice daily) If primary anticoagulation discontinued because of bleeding risk, consider IVC filter. This may not reduce recurrence risk (Decousus 1998)
25 Cancer Patients with Symptomatic Recurrent VTE (Korhana A. J Thromb Thrombolysis. 2016) Therapeutic anticoagulation with an agent other than LMWH: Transition to therapeutic LMWH. Optimal anticoagulation with LMWH: Continue LMWH at a higher dose, starting at an increase of ~25 % of the current dose Non-therapeutic dose at the time of recurrence: Switch to therapeutic dose of LMWH Do not use IVC filters except in presence of absolute contraindications to anticoagulation (e.g. active bleeding). Retrievable filters should be used.

26 Recurrent VTE in CAT (Lee A, Blood 2013)
27 Summary Cancer increases VTE risk 4 fold Those with cancer & VTE have worse prognosis CT scanning for patients with unprovoked VTE identifies cancer in about 4% of people. Current advice is that routine screening and clinical history generally sufficient to rule out cancer. Bleeding is generally higher in anticoagulated Cancer patients Thrombocytopenia is relatively common and needs monitoring in those anticoagulated with CAT, with platelet support if necessary Bleeding needs careful assessment of patient and IVC filter if anticoagulation essential Recurrent VTE requires increased anticoagulation where possible
28 Preventing Catheter-related thrombosis Prospective study (Bern 1990): 82 patients showed benefit of low dose warfarin in reducing risk of catheter-related thrombosis WARP study (Young 2009): RCT of 812 patients randomized to warfarin or no therapy found no difference in risk for catheter-related thrombosis. Cochrane review (Akl 2011): demonstrated that neither warfarin or prophylactic LMWH reduced risk for catheter-related thrombosis Routine anticoagulation is not recommended (1A)
29 Thromboprophylaxis in cancer patients admitted to hospital Patients with active cancer should be considered for thromboprophylaxis when admitted to hospital, as long as benefit outweighs risk for bleeding. (Kahn, 2012) Active Cancer should be considered in those diagnosed or treated within the previous 6 months or recurrent / metastatic cancer.
30 Thromboprophylaxis in ambulatory Cancer patients Cochrane review of 9 RCTs (3538 patients) in cancer patients, comparing controls against LMWH (8) or warfarin (1), found reduction in VTE risk with LMWH, without a significant increase in bleeds (DeNisio, 2012) 60 patients treated to prevent 1 VTE, indicates that TP should not be routine but considered in those with particularly high VTE risk (BCSH, 2015) Identification of these high risk patients may be done using scoring systems (Khorana 2008, Farge 2013)
31 Predictive model for Chemotherapyrelated VTE (Khorana et al 2008) Patient characteristic Risk score Very high risk for VTE: stomach & pancreas 2 High risk for VTE: Lung, NHL, Gynae, bladder, testicular Pre-chemotherapy platelet count 1 Haemoglobon level <100g/l or use of ESA s 1 Pre-chemotherapy leucocyte count >11 x 10 9 /l 1 Body Mass Index >35 kg/m 2 1 Score Actual Score Thrombosis rate per 2-5 months (%) Low Intermediate High >
32 Incidental VTE Cancer patients with incidental PE or DVT should be therapeutically anticoagulated as for symptomatic disease (1C) In Plymouth about 50 incidental VTE events per year for last 6 years. >75% of these are cancer-related events. >75% dead one year later.
Venous Thrombo-Embolism. John de Vos Consultant Haematologist RSCH
 Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
Venous Thrombo-Embolism John de Vos Consultant Haematologist RSCH overview The statistics Pathogenesis Prophylaxis Treatment Agent Duration Incidental VTE Recurrence of VTE IVC filters CVC related thrombosis
CANCER ASSOCIATED THROMBOSIS. Pankaj Handa Department of General Medicine Tan Tock Seng Hospital
 CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
CANCER ASSOCIATED THROMBOSIS Pankaj Handa Department of General Medicine Tan Tock Seng Hospital My Talk Today 1.Introduction 2. Are All Cancer Patients at Risk of VTE? 3. Should All VTE Patients Be Screened
Venous Thromboembolism (VTE) in Myeloma. Christine Chen May 2017
 in Myeloma. Christine Chen May 2017") Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Venous Thromboembolism (VTE) in Myeloma Christine Chen May 2017 Objectives 1. Review the magnitude of the problem and why myeloma patients are at risk of VTE 2. Discuss thromboprophylaxis approaches in
Cancer and Thrombosis
 Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
Cancer and Thrombosis The close relationship between venous thromboembolism and cancer has been known since at least the 19th century by Armand Trousseau. Thrombosis is a major cause of morbidity and mortality
PROGNOSIS AND SURVIVAL
 CANCER ASSOCIATED THROMBOSIS PROGNOSIS AND SURVIVAL Since French internist Armand Trousseau reported the occurrence of mysterious thrombotic disorders in cancer patients in the mid-19th century, the link
CANCER ASSOCIATED THROMBOSIS PROGNOSIS AND SURVIVAL Since French internist Armand Trousseau reported the occurrence of mysterious thrombotic disorders in cancer patients in the mid-19th century, the link
Epidemiology of Thrombosis in Patients with Malignancy. Cancer and Venous Thromboembolism. Chew HK, Arch Int Med, Feb Blom et al, JAMA, Feb 2005
 Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
Cancer and Venous Thromboembolism Objectives 1. Epidemiology of thrombosis in patients with malignancy 2. Anticancer agents and thrombosis 3. Current treatment protocols at UHN 4. Prevention of DVT 5.
In the Clinic: Annals Sweta Kakaraparthi 1/23/15
 In the Clinic: Annals Sweta Kakaraparthi 1/23/15 Case Scenerio 56 year old female with breast cancer presents to the clinic for her 3 month followup! She is concerned about blood clots and asks you about
In the Clinic: Annals Sweta Kakaraparthi 1/23/15 Case Scenerio 56 year old female with breast cancer presents to the clinic for her 3 month followup! She is concerned about blood clots and asks you about
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES
 PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES Mario Mandalà, MD Unit of Clinical Research Department of Oncology and Haematology Papa Giovanni XXIII Hospital Cancer Center
PRIMARY THROMBOPROPHYLAXIS IN AMBULATORY CANCER PATIENTS: CURRENT GUIDELINES Mario Mandalà, MD Unit of Clinical Research Department of Oncology and Haematology Papa Giovanni XXIII Hospital Cancer Center
Cancer Associated Thrombosis
 Cancer Associated Thrombosis Pantep Angchaisuksiri, MD Professor of Medicine Mahidol University, Thailand Adjunct Associate Professor University of North Carolina, Chapel Hill, USA Piccioli A. J Thromb
Cancer Associated Thrombosis Pantep Angchaisuksiri, MD Professor of Medicine Mahidol University, Thailand Adjunct Associate Professor University of North Carolina, Chapel Hill, USA Piccioli A. J Thromb
Frequently Asked Questions about Cancer Associated Thrombosis
 + Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
+ Frequently Asked Questions about Cancer Associated Thrombosis Atlantic Canada Oncology Group Annual Meeting June 13 th, 2015 Sudeep Shivakumar, Dalhousie University + Conflict of Interest Disclosures
Tissue Factor-positive Microparticles in Cancerassociated
 Tissue Factor-positive Microparticles in Cancerassociated Thrombosis Nigel Mackman, Ph.D., FAHA John C. Parker Distinguished Professor of Medicine Director of the UNC McAllister Heart Institute Co-Director
Tissue Factor-positive Microparticles in Cancerassociated Thrombosis Nigel Mackman, Ph.D., FAHA John C. Parker Distinguished Professor of Medicine Director of the UNC McAllister Heart Institute Co-Director
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT
 VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Thromboembolism and cancer: New practices. Marc Carrier
 Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
Thromboembolism and cancer: New practices Marc Carrier Marc Carrier Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific Advisory Board Leo Pharma, BMS No relevant
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Dr. Pierpaolo Di Micco Internal Medicine and Emergency Room Fatebenefratelli Hospital of Naples, Italy
 ? Para què sirve el recuento de leucocitos en lospacientescon cancer? Dr. Pierpaolo Di Micco Internal Medicine and Emergency Room Fatebenefratelli Hospital of Naples, Italy ? Para què sirve el recuento
? Para què sirve el recuento de leucocitos en lospacientescon cancer? Dr. Pierpaolo Di Micco Internal Medicine and Emergency Room Fatebenefratelli Hospital of Naples, Italy ? Para què sirve el recuento
DOACs in CAT. Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD
 DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
DOACs in CAT Fellow: Shweta Jain, MD Faculty Discussant: David Garcia, MD Case 65 year old post menopausal female Left breast lesion Oct 2015 Biopsy Invasive ductal carcinoma Lumpectomy with SNB- pt1cno
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Duration of Anticoagulant Therapy. Linda R. Kelly PharmD, PhC, CACP September 17, 2016
 Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Cancer Associated Thrombosis
 Cancer Associated Thrombosis Can we use DOACs? D R. C Y N T H I A W U MD F R C P ( C ) D I V I S I O N O F H E M A T O L O G Y F A M I L Y P H Y S I C I A N S A N D C A N C E R C O N T R O L A P R I L
Cancer Associated Thrombosis Can we use DOACs? D R. C Y N T H I A W U MD F R C P ( C ) D I V I S I O N O F H E M A T O L O G Y F A M I L Y P H Y S I C I A N S A N D C A N C E R C O N T R O L A P R I L
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
New Hope for VTE Burden in Ambulatory Cancer Patients
 New Hope for VTE Burden in Ambulatory Cancer Patients Essam Abo-El-Nazar MS, FRCS Consultant Liver Surgeon King Fahd Hospital Jeddah-KSA Prof. of Surgery Imperial College London-UK My talk today What is
New Hope for VTE Burden in Ambulatory Cancer Patients Essam Abo-El-Nazar MS, FRCS Consultant Liver Surgeon King Fahd Hospital Jeddah-KSA Prof. of Surgery Imperial College London-UK My talk today What is
La terapia del TEV nel paziente oncologico nell'era dei DOAC
 XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
XXVI CONGRESSO NAZIONALE FCSA Bologna, 5-7 Novembre 2015 Tromboembolismo venoso La terapia del TEV nel paziente oncologico nell'era dei DOAC ANNA FALANGA Immunoematologia e Medicina Trasfusionale e Centro
Is There a Role for Prophylaxis in Cancer Patients During Therapy?
 Victor F. Tapson, MD, FCCP, FRCP Professor of Medicine Director, Center for Pulmonary Vascular Disease Division of Pulmonary and Critical Care Duke University Medical Center Durham, N.C. USA Is There a
Victor F. Tapson, MD, FCCP, FRCP Professor of Medicine Director, Center for Pulmonary Vascular Disease Division of Pulmonary and Critical Care Duke University Medical Center Durham, N.C. USA Is There a
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
RISK FACTORS. Cancer type. Cancer stage
 CANCER ASSOCIATED THROMBOSIS RISK FACTORS The link between cancer and thrombosis is well established, with malignancy recognised as the most important individual risk factor for venous thromboembolism
CANCER ASSOCIATED THROMBOSIS RISK FACTORS The link between cancer and thrombosis is well established, with malignancy recognised as the most important individual risk factor for venous thromboembolism
Management of Cancer Associated VTE
 Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
Management of Cancer Associated VTE Jean M. Connors, MD 2017 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Assistant Professor of Medicine HMS
THROMBOPROPHYLAXIS IN CANCER PATIENTS
 CANCER ASSOCIATED THROMBOSIS THROMBOPROPHYLAXIS IN CANCER PATIENTS Cancer is an important risk factor for venous thromboembolism (VTE). Research has shown that 4-20% of 1 patients with cancer experience
CANCER ASSOCIATED THROMBOSIS THROMBOPROPHYLAXIS IN CANCER PATIENTS Cancer is an important risk factor for venous thromboembolism (VTE). Research has shown that 4-20% of 1 patients with cancer experience
Understanding thrombosis in venous thromboembolism. João Morais Head of Cardiology Division and Research Centre Leiria Hospital Centre Portugal
 Understanding thrombosis in venous thromboembolism João Morais Head of Cardiology Division and Research Centre Leiria Hospital Centre Portugal Disclosures João Morais On the last year JM received honoraria
Understanding thrombosis in venous thromboembolism João Morais Head of Cardiology Division and Research Centre Leiria Hospital Centre Portugal Disclosures João Morais On the last year JM received honoraria
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Update on the Management of Cancer Associated VTE
 Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
Update on the Management of Cancer Associated VTE Jean M. Connors, MD 2018 Master Class Course Anticoagulation Management Services BWH/DFCI Hemostatic Antithrombotic Stewardship BWH Associate Professor
incidence of cancer-associated thrombosis (CAT) is further increased by additional risk factors such as chemotherapeutic 2
 is further increased by additional risk factors such as chemotherapeutic 2") CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the ability of tumour cells to activate the
Anticoagulation in Special populations. Ng Heng Joo Department of Haematology Singapore General Hospital
 Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
Anticoagulation in Special populations Ng Heng Joo Department of Haematology Singapore General Hospital roymatheson.com Objectives Safer anticoagulation for The elderly Chronic kidney disease Obese patients
The Evidence Base for Treating Acute DVT
 The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
The Evidence Base for Treating Acute DVT Mr Chung Sim Lim Consultant Vascular Surgeon and Honorary Lecturer Royal Free London NHS Foundation Trust and University College London NIHR UCLH Biomedical Research
IRB protocol Yair Lev, MD 11/25/08
 IRB protocol Yair Lev, MD 11/25/08 Abdominal and Pelvic CT as a screening modality for occult malignant disease in unprovoked Venous Thromboembolism: A randomized, controlled prospective study. A. Study
IRB protocol Yair Lev, MD 11/25/08 Abdominal and Pelvic CT as a screening modality for occult malignant disease in unprovoked Venous Thromboembolism: A randomized, controlled prospective study. A. Study
Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1
 CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
CANCER ASSOCIATED THROMBOSIS TREATMENT Patients with cancer are at a greater risk of developing venous thromboembolism than non-cancer patients, partly due to the 1 ability of tumour cells to activate
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Cancer Associated Thrombosis An update.
 Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
Cancer Associated Thrombosis An update. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway LIQUID
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range
 Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range") Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
Suspected Deep Vein Thrombosis (DVT) Pathway for Non Pregnant patients Updated November 2016, with new D-dimer reference range Suspect a DVT? Complete a Two-level DVT Wells score on ICE system (see page
VTE Risk Assessment. Challenges of Hemostasis in Cancer Patients. Cihan Ay, MD Associate Professor
 Challenges of Hemostasis in Cancer Patients VTE Risk Assessment Cihan Ay, MD Associate Professor Clinical Division of Haematology and Haemostaseology Department of Medicine I, Comprehensive Cancer Center
Challenges of Hemostasis in Cancer Patients VTE Risk Assessment Cihan Ay, MD Associate Professor Clinical Division of Haematology and Haemostaseology Department of Medicine I, Comprehensive Cancer Center
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
VTE General Background
 VTE General Background VTE incidence is about 1:1000 persons annually >250,000 admissions for VTE annually >100,000 people die of PE annually >90% of PE s arise from lower limb DVT 50% of DVT at diagnosis
VTE General Background VTE incidence is about 1:1000 persons annually >250,000 admissions for VTE annually >100,000 people die of PE annually >90% of PE s arise from lower limb DVT 50% of DVT at diagnosis
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS
 ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
ROLE OF LOW MOLECULAR WEIGHT HEPARIN IN THE AGE OF DIRECT ORAL ANTICOAGULANTS Chee Yen Lin Consultant Haematologist NCIS Haematology National University Hospital Singapore Nomenclature direct oral anticoagulant
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM
 PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
PREVENTION AND TREATMENT OF VENOUS THROMBOEMBOLISM International Consensus Statement 2013 Guidelines According to Scientific Evidence Developed under the auspices of the: Cardiovascular Disease Educational
Are guidelines for anticoagulation useful in cancer patients?
 Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Session 3 Striking a Balance Between Bleeding and the Risk of Thrombosis in Cancer Patients Are guidelines for anticoagulation useful in cancer patients? Sebastian Szmit Department of Pulmonary Circulation
Is Oral Rivaroxaban Safe and Effective in the Treatment of Patients with Symptomatic DVT?
 Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Philadelphia College of Osteopathic Medicine DigitalCommons@PCOM PCOM Physician Assistant Studies Student Scholarship Student Dissertations, Theses and Papers 1-1-2013 Is Oral Rivaroxaban Safe and Effective
Cancer Associated Thrombosis: six months and beyond. Farzana Haque Hull York Medical School
 Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Cancer Associated Thrombosis: six months and beyond Farzana Haque Hull York Medical School Disclosure I have no disclosure The Challenge of Anticoagulation in Patients with Venous Thromboembolism and Cancer
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Clinical Policy Title: Genetic testing for G1691A polymorphism factor V Leiden
 Clinical Policy Title: Genetic testing for G1691A polymorphism factor V Leiden Clinical Policy Number: 05.01.03 Effective Date: January 1, 2016 Initial Review Date: July 15, 2015 Most Recent Review Date:
Clinical Policy Title: Genetic testing for G1691A polymorphism factor V Leiden Clinical Policy Number: 05.01.03 Effective Date: January 1, 2016 Initial Review Date: July 15, 2015 Most Recent Review Date:
VENOUS THROMBOEMBOLISM, CANCER AND CKD ANOTHER TRIAD TO MANAGE
 VENOUS THROMBOEMBOLISM, CANCER AND CKD ANOTHER TRIAD TO MANAGE I. ELALAMY Service d Hématologie Biologique HOPITAL TENON PARIS INSERM UMR U938 DISCLOSURES Conferences Clinical Studies Board Sanofi X X
VENOUS THROMBOEMBOLISM, CANCER AND CKD ANOTHER TRIAD TO MANAGE I. ELALAMY Service d Hématologie Biologique HOPITAL TENON PARIS INSERM UMR U938 DISCLOSURES Conferences Clinical Studies Board Sanofi X X
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients. David Liff MD Oklahoma Heart Institute Vascular Center
 DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
DVT Pathophysiology and Prophylaxis in Medically Hospitalized Patients David Liff MD Oklahoma Heart Institute Vascular Center Overview Pathophysiology of DVT Epidemiology and risk factors for DVT in the
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
PE Pathway. The charts are listed as follows:
 PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
PE Pathway This document comprises 6 simple flow charts to assist clinicians in the investigation and treatment of suspected or confirmed Acute Pulmonary Emboli. The pathway has been put together using
Heparin-Induced Thrombocytopenia. Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital
 Heparin-Induced Thrombocytopenia Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital Heparin-induced thrombocytopenia (HIT) A serious concern associated with thrombosis development following
Heparin-Induced Thrombocytopenia Steven Baroletti, PharmD., M.B.A., BCPS Brigham and Women s Hospital Heparin-induced thrombocytopenia (HIT) A serious concern associated with thrombosis development following
Cancer Associated Thrombosis Review and Update. Family Practice Oncology CME Day November 21 st 2015 Erica Peterson
 Cancer Associated Thrombosis Review and Update Family Practice Oncology CME Day November 21 st 2015 Erica Peterson Disclosures No conflicts of interest to declare Objectives To review evidence in cancer-associated
Cancer Associated Thrombosis Review and Update Family Practice Oncology CME Day November 21 st 2015 Erica Peterson Disclosures No conflicts of interest to declare Objectives To review evidence in cancer-associated
Cancer associated thrombosis palliative care and the end of life. Tracy Anderson May 2017
 Cancer associated thrombosis palliative care and the end of life Tracy Anderson May 2017 Treatment at the end of life Can be challenging to know what treatments are appropriate Benefit vs burden Patients
Cancer associated thrombosis palliative care and the end of life Tracy Anderson May 2017 Treatment at the end of life Can be challenging to know what treatments are appropriate Benefit vs burden Patients
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach
 Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Treatment of cancer-associated venous thromboembolism by new oral anticoagulants: a meta-analysis
 Original Article Page of 9 Treatment of cancer-associated venous thromboembolism by new oral anticoagulants: a meta-analysis Satyanarayana R. Vaidya, Sonu Gupta, Santhosh R. Devarapally, Department of
Original Article Page of 9 Treatment of cancer-associated venous thromboembolism by new oral anticoagulants: a meta-analysis Satyanarayana R. Vaidya, Sonu Gupta, Santhosh R. Devarapally, Department of
Venous thrombosis in the patient with cancer
 Venous thrombosis in the patient with cancer Wessels PF, MBChB MMed, CertClin Hematology(CMSA) Private Practice, LCM Hospital, Pretoria, and Consultant, Ampath Laboratories Part-Time Consultant, Department
Venous thrombosis in the patient with cancer Wessels PF, MBChB MMed, CertClin Hematology(CMSA) Private Practice, LCM Hospital, Pretoria, and Consultant, Ampath Laboratories Part-Time Consultant, Department
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
New Guidance in AT10 Clive Kearon, MD, PhD,
 New Guidance in AT10 Clive Kearon, MD, PhD, Professor, Department of Medicine, McMaster University; Program Director, McMaster Clinical Investigator Program, McMaster University Head, Clinical Thromboembolism
New Guidance in AT10 Clive Kearon, MD, PhD, Professor, Department of Medicine, McMaster University; Program Director, McMaster Clinical Investigator Program, McMaster University Head, Clinical Thromboembolism
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON
 Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON How to Prevent and Manage the Post-Thrombotic Syndrome? Jean-Philippe Galanaud Clinical Thromboembolism & Division of GIM Sunnybrook,
Canadian Society of Internal Medicine Annual Meeting 2017 Toronto, ON How to Prevent and Manage the Post-Thrombotic Syndrome? Jean-Philippe Galanaud Clinical Thromboembolism & Division of GIM Sunnybrook,
PULMONARY EMBOLISM MANAGEMENT GUIDELINES
 PULMONARY EMBOLISM MANAGEMENT GUIDELINES This document is adapted from the NICE guidelines titled Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia
PULMONARY EMBOLISM MANAGEMENT GUIDELINES This document is adapted from the NICE guidelines titled Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia
Joost van Veen Consultant Haematologist
 Joost van Veen Consultant Haematologist Bridging anticoagulation - conclusion Aim Questions What is the evidence? Does oral anticoagulation need to be stopped and if so when? When and at what dose is alternative
Joost van Veen Consultant Haematologist Bridging anticoagulation - conclusion Aim Questions What is the evidence? Does oral anticoagulation need to be stopped and if so when? When and at what dose is alternative
Clinical Policy Title: Genetic testing for G1691A polymorphism factor V Leiden
 Clinical Policy Title: Genetic testing for G1691A polymorphism factor V Leiden Clinical Policy Number: 05.01.03 Effective Date: January 1, 2016 Initial Review Date: July 15, 2015 Most Recent Review Date:
Clinical Policy Title: Genetic testing for G1691A polymorphism factor V Leiden Clinical Policy Number: 05.01.03 Effective Date: January 1, 2016 Initial Review Date: July 15, 2015 Most Recent Review Date:
Top 5 (or so) Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE
 Hematology Consults. Tom DeLoughery, MD FACP FAWM. Oregon Health and Sciences University DISCLOSURE") Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Top 5 (or so) Hematology Consults Tom FACP FAWM Oregon Health and Sciences University DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau - None Consultant/Research none 1 What I am Talking About
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
Perioperative Management of the Anticoagulated Patient
 Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Perioperative Management of the Anticoagulated Patient Citywide Resident Perioperative Medical Consultation Conference 5/5/17 Matthew Eisen, MD Director, Anticoagulation Services MetroHealth Medical Center
Duration anticoagulation VTE. Clinical case WGA april 2017 Dr Borgoens
 Duration anticoagulation VTE Clinical case WGA april 2017 Dr Borgoens Clinical case 70 y old, sedentary computer engineer 1 st episode intermediate high risk pulmonaryembolism(rv dysfunction, positives
Duration anticoagulation VTE Clinical case WGA april 2017 Dr Borgoens Clinical case 70 y old, sedentary computer engineer 1 st episode intermediate high risk pulmonaryembolism(rv dysfunction, positives
New oral anticoagulants and Palliative Care.
 New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
New oral anticoagulants and Palliative Care. Simon Noble Marie Curie Professor of Supportive and Palliative Medicine Marie Curie Palliative Care Research Centre Cardiff University The coagulation pathway
Anticoagulation Forum: Management of Tiny Clots
 Anticoagulation Forum: Management of Tiny Clots Casey O Connell, MD FACP Associate Professor Jane Anne Nohl Division of Hematology Keck School of Medicine USC DISCLOSURES None 4/11/2017 Objectives Define
Anticoagulation Forum: Management of Tiny Clots Casey O Connell, MD FACP Associate Professor Jane Anne Nohl Division of Hematology Keck School of Medicine USC DISCLOSURES None 4/11/2017 Objectives Define
Pulmonary Embolism Pathway
 Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
Pulmonary Embolism Pathway Ambulatory Care Pathway Dr. A. Zafar, Dr. A. Rehman, Dr. T. Malik September, 2011. Patient Identification Label Pulmonary Embolism Pathway Clinical History Comments Hospital
Obesity, renal failure, HIT: which anticoagulant to use?
 Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
Obesity, renal failure, HIT: which anticoagulant to use? Mark Crowther with thanks to Dr David Garcia and others. This Photo by Unknown Author is licensed under CC BY-SA 1 2 Drug choices The DOACs have
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
Anticoagulation therapy following endovascular treatment of iliofemoral deep vein thrombosis
 Anticoagulation therapy following endovascular treatment of iliofemoral deep vein thrombosis Tim Sebastian, M.D. University Hospital Zurich Clinic for Angiology Disclosure Speaker name: Tim Sebastian I
Anticoagulation therapy following endovascular treatment of iliofemoral deep vein thrombosis Tim Sebastian, M.D. University Hospital Zurich Clinic for Angiology Disclosure Speaker name: Tim Sebastian I
DOACs in SPECIAL POPULATIONS
 DOACs in SPECIAL POPULATIONS Ann K Wittkowsky PharmD, CACP, FASHP, FCCP Clinical Professor University of Washington School of Pharmacy Director, Anticoagulation Services UWMedicine Department of Pharmacy
DOACs in SPECIAL POPULATIONS Ann K Wittkowsky PharmD, CACP, FASHP, FCCP Clinical Professor University of Washington School of Pharmacy Director, Anticoagulation Services UWMedicine Department of Pharmacy
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
Diagnosis and Management of Venous Thromboembolism
 Diagnosis and Management of Venous Thromboembolism Muhammad Sajid Pervaiz Consultant Haematologist Chairman VTE committee Pennine Acute Hospitals NHS trust TOPICS 1-Introduction (Seriousness of problem)
Diagnosis and Management of Venous Thromboembolism Muhammad Sajid Pervaiz Consultant Haematologist Chairman VTE committee Pennine Acute Hospitals NHS trust TOPICS 1-Introduction (Seriousness of problem)
Epidermiology Early pulmonary embolism
 Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Prevention and management of venous thromboembolism M. AAPRO
 Prevention and management of venous thromboembolism M. AAPRO Thromboprophylaxisof DVT and PE in AmbulatoryCancerPatients Zurich, February 2017 M. AAPRO Based on a lesson in April 2016 by M. DICATO M.D.,
Prevention and management of venous thromboembolism M. AAPRO Thromboprophylaxisof DVT and PE in AmbulatoryCancerPatients Zurich, February 2017 M. AAPRO Based on a lesson in April 2016 by M. DICATO M.D.,
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales
 John Fletcher Wound Care Association of New South Wales") Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
Prevention and management of deep venous thrombosis (DVT) John Fletcher Wound Care Association of New South Wales Merimbula, 6 th November 2010 University of Sydney Department of Surgery Westmead Hospital
NICE Guidance: Venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital 1
 in patients admitted to hospital 1") The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
Cancer and the Heparins
 Cancer and the Heparins Wim P Ceelen, MD, PhD, FACS Department of GI Surgery - UZ Gent Senior Clinical Researcher - FWO Overview Mechanisms of cancer induced thrombosis Guidelines for prevention and treatment
Cancer and the Heparins Wim P Ceelen, MD, PhD, FACS Department of GI Surgery - UZ Gent Senior Clinical Researcher - FWO Overview Mechanisms of cancer induced thrombosis Guidelines for prevention and treatment
Prostate Biopsy Alerts
 Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum
 Online Data Supplement Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum Stacey M. Kassutto, C. Jessica Dine, Maryl Kreider, Rupal
Online Data Supplement Changing the Ambulatory Training Paradigm: The Design and Implementation of an Outpatient Pulmonology Fellowship Curriculum Stacey M. Kassutto, C. Jessica Dine, Maryl Kreider, Rupal
UvA-DARE (Digital Academic Repository) Cancer, thrombosis and low-molecular-weight heparins Piccioli, A. Link to publication
 Cancer, thrombosis and low-molecular-weight heparins Piccioli, A. Link to publication") UvA-DARE (Digital Academic Repository) Cancer, thrombosis and low-molecular-weight heparins Piccioli, A. Link to publication Citation for published version (APA): Piccioli, A. (2015). Cancer, thrombosis
UvA-DARE (Digital Academic Repository) Cancer, thrombosis and low-molecular-weight heparins Piccioli, A. Link to publication Citation for published version (APA): Piccioli, A. (2015). Cancer, thrombosis
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,