Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
|
|
|
- Scott Sherman
- 6 years ago
- Views:
Transcription
1 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
2
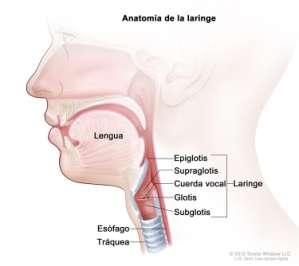
3 Larynx Hypopharynx

4
5 The goal of treatment is to achieve larynx preservation with good function without compromising survival Witch is the optimal primary endpoint? - Larynx preservation rate - Larynguectomy- FS? - Survival Rate at 2, 5, 10 years? - QoL.
6 Summary of the Relevant Literature
7 Induction chemotherapy 3 randomized studies: - VA - EORTC GETTEC larynx hypopharynx T3 larynx VALCSG. N Engl J Med 1991 Lefebvre JL et al. J Natl Cancer Inst 1996 Richard JM et al. Oral Oncol 1998 Surgery + RT Surveillance PF x 3 no response surgery + RT surveillance response RT +/- salvage surgery
8 Veterans Affairs Laryngeal Cancer Study Group 332 pts, laryngeal SCC stage III/IV Surgery Adjuvant RT RT: 5000cGy/25fx RT: cGy T1/T2 9% T3 65% T4 26% Glottis 37% IC x 2 Cisplatin 100mg/m2, D1 5FU 1000mg/m2/d x 5d q3w IC x 1 Poor respond Definitive RT Surgery +/- RT Residual disease Supraglottis 63% 2yr DFS OS Recur at primary Recur at regional Distant mets Surgery 75% 68% 2% 5% 17% Laryngectomyfree survival IC RT 65% 68% 12% 8% 11% 39% p value NS New England Journal of Medicine 1991; 324: LPR: 64% (2y)
9 EORTC pts, hypopharynx SCC stage II/III/IV Surgery Adjuvant RT RT: 5000cGy/25fx RT: 7000cGy IC x 2 IC x 1 Definitive RT T2 20% T3 75% Cisplatin 100mg/m2, D1 5FU 1000mg/m2/d x 5d q3w Poor respond Surgery +/- RT Residual disease T4 5% Pyriform sinus 78% 5yr DFS OS Recur at local Recur at regional Distant mets Laryngectomyfree survival Aryepiglottic fold 22% Surgery 32% 35% 17% 23% 36% IC RT 25% 30% 12% 19% 25% 42% (2y) 35% (5y) p value NS NS NS NS Journal of National Cancer Institute 1996; 8:
10 Induction chemotherapy Trial/ site of tumour N Therapy aproach Larynx Preservation LFS Survival Difference VALCSG (larynx) EORTC (hypopharynx) 332 S RT vs PF 1 x3 RT 202 S RT vs PFx3 RT 64%(2y) 39%(2y) No difference 40,5% (5y) 42% (2y) 35% (5y) No difference 1 CDDP 100mg/m²/ev d1 5-FU 1000mg/m²/ev d 1-5 (ic) every 3w x 3courses Induction PF + RT can be effective in preserving the larynx in a high percentage of patients, without compromising overall survival
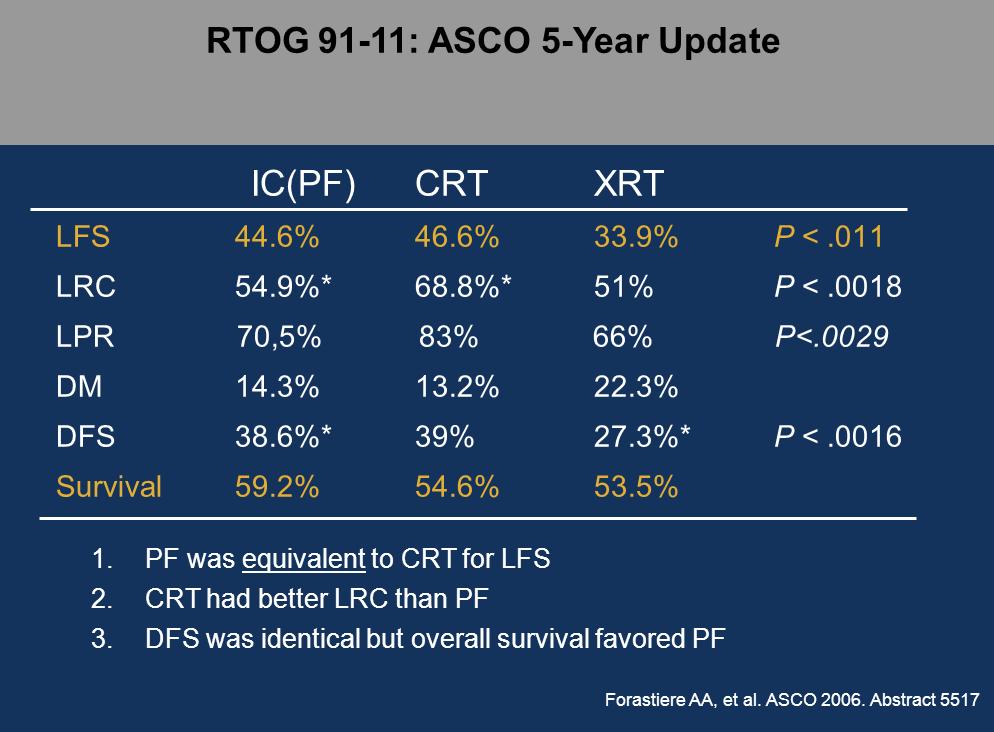
11 Chemoradiotherapy RTOG (USA) larynx RT RT-CT concomitantly (cisplatin days 1, 22 and 43) N=547pt PF induction 1 CDDP 100mg/m²/ev d1 5-FU 1000mg/m²/ev d 1-5 (ic) every 3w x 3courses no response surgery + RT surveillance response RT +/- salvage surgery T2 12% T3 78% T4 10% Supraglottis 69% Glottis 31% Forastiere A et al. N Engl J Med 2003
 15% Difficulties in p Speech/swallow : similar (2y) 15% 0.02(C v A) 0.006(B v A) NS 0.005(B v C) 0.001(B v A) 0.004(B v C) 0.001(B v A) 0.49(BvC) 0.01 (AvB) 0.")
12 Chemoradiotherapy RTOG (USA) larynx 2yr DFS OS Intact larynx LR control LFS Distant mets A: RT 27% 56 % 70% 56% 53% 38% (5y) 22% B: CCRT 36% 54 % 88% 78% 66% 45% (5y) 12% C: IC RT 38% 55 % 75% 61% 59% 43% (5y) 15% Difficulties in p Speech/swallow : similar (2y) 15% 0.02(C v A) 0.006(B v A) NS 0.005(B v C) 0.001(B v A) 0.004(B v C) 0.001(B v A) 0.49(BvC) 0.01 (AvB) 0.03(B v A) Forastiere A et al. N Engl J Med 2003
13
14

15 Toxicity: - The rate of high grade toxic effects was greater in Ch-based regimens 81% (Chi->RT), 82% (Ch-RT) & 61% (XRT) - The mucosal toxicity of concurrent RT-CDDP was nearly twice as frequent as the mucosal toxicity of the other two treatments during RT - No differences in late toxicity or speech or swallowing function were demonstrated between treatment groups
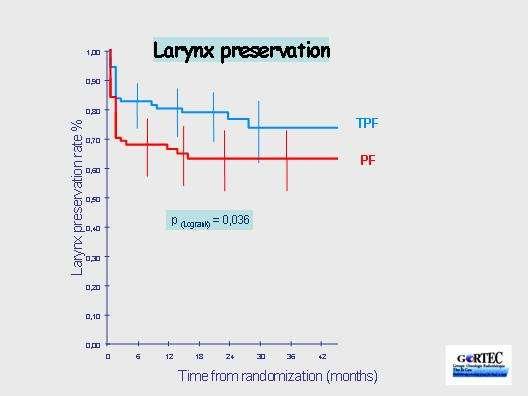
16 GORTEC Induction chemotherapy Induction CT Larynx Preservation Larynx or hypopharynx tumors Resectable tumors or nodes requiring total (pharyngo[p] laryngectomy) No previous treatment TPF arm Docetaxel (75 mg/m² d1) Cisplatin (75 mg/m² d1) 5-FU (750 mg/m²/dx5) Q 3 weeks x 3 cycles PF arm Cisplatin (100 mg/m²) 5-FU (1000 mg/m²/dx5) Q 3 weeks x 3 cycles No Response to induction treatment Yes Non-responders: Total (P)laryngectomy + post-op RT Responders: RT T2 18% T3 67% T4 15% Primary Objective: larynx preservation rate Pointreau et al. ASCO 2006 Calais G, et al. ASCO 2006, abstract 5506.

17 GORTEC Induction chemotherapy
18 GORTEC Induction chemotherapy Grade 3/4 Acute Toxicities % of patients NCI/CTC Grade 3/4* TPF PF p Mucositis Neutropenia Febrile neutropenia Thrombocytopenia Deaths *Among patients treated with RT alone, no differences were observed between the 2 arms in: xerostomia, fibrosis, larynx edema, dysphagia, % of patients with permanent feeding tube. Pointreau Y, et al. Cancer/Radiotherapie. 2006:10:493, Abstract C03; Calais G, et al. ASCO 2006, Abstract 5506.


19 TAX 324 Induction chemotherapy Sequential therapy for locally advanced larynx and hypopharynx cancer: Subgroup analysis from TAX 324 study


20 TAX 324 Induction chemotherapy -Significant improvement in PFS (Hazard Ratio 0.61 ( ) p= Strong trend for OS (Hazard Ratio 0.67 ( ) p =0.12 ASCO 2008
21 Five phase III trials (VALSG, EORTC 24891, RTOG 91-11, GORTEC , TAX 324) STUDY LFS LPR VETERANS (L) EORTC (H) RTOG PF (L) RTOG QT+RT (L) GORTEC PF (L&H) GORTEC TPF (L&H) TAX 324 PF (L&H) TAX324 TPF (L&H) 39% (2y) 42% (2y) 35% (5y) 59% (2y) 43% (5y) 66% (2y) 45% (5y) 37% (3y) 53%(3y) 32% (3y) 52%(3y) 64% (2y) 75%(2y) 88%(2y) 57% (3y) 70%(3y)
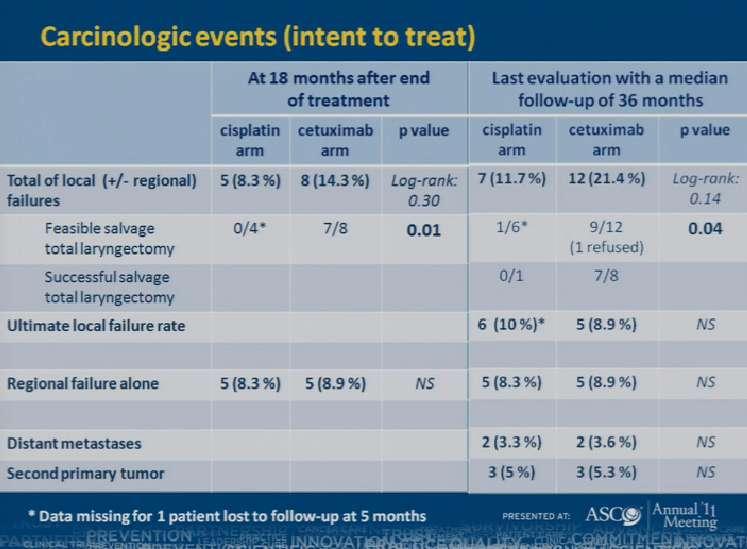
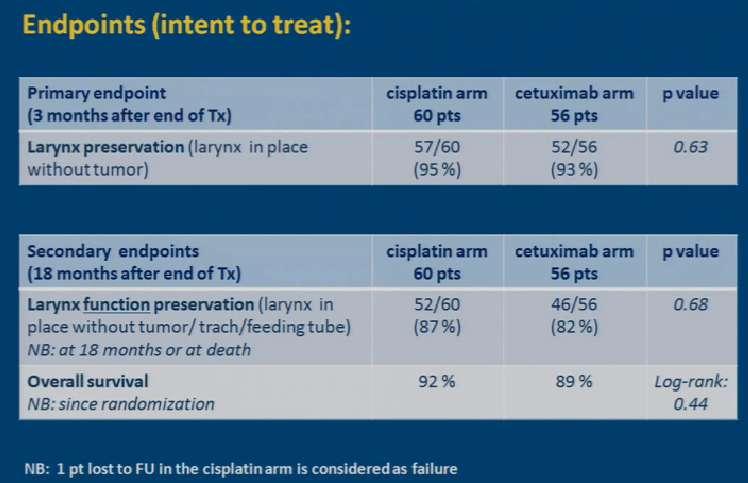
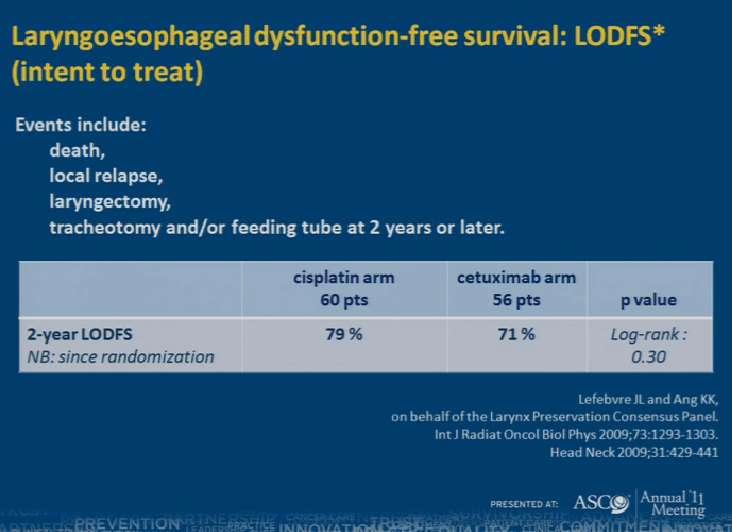
22 TREMPLIN: French randomized phase II study of laryngeal preservation Resp. RT + cetuximab TPF x 3 RT + cisplatin N=153 Larynx/hypopharynx suitable for TL No resp. S + PORT Randomized phase II, GORTEC-GETTEC) ASCO 2009 i ASCO 2011 JCO 2013
23
24
25
26
27 From these studies we have learnt that: - Ch combined with RT has allowed to preserve a significant number of larynx without compromising survival - PF followed by RT and Ch-RT show similar efficacy in LFS - LCR and LPR were significantly improved with Ch-RT - Ch decreased the incidence of DM without impact in OS - TPF is better than PF in LFS & PFS - Chemoradiotherapy & Induction Chemotherapy are alternatives -TPF-based ICT followed CRT or BRT was feasible but had substantial overall toxicity None of the ch-based protocols has provided better results than surgery except in terms of larynx preservation
28 There is currently no good evidence base from larynx preservation trials with which to assess the functional outcomes achieved with different larynx preservation strategies

29 The Oncologist 2010;15 (suppl3): 25-29
30
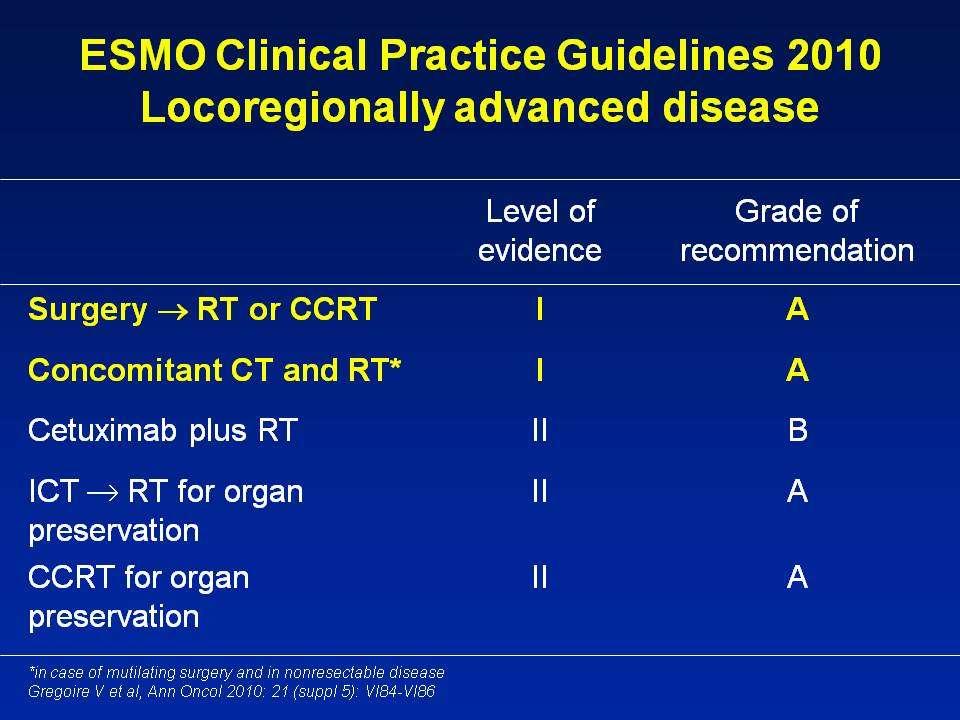
31 Suggested approaches to management
32
33 T1, T2 TT Intent to preserve the larynx RT or larynx preservation surgery tt selection depends on: pt factors, local expertise & rehabilitation services Concurrent Ch-RT only in: Stage III, T2 N+ pts whom total LT is the only surgical option OR larynx-preservation surgery is expected to yield an unsatisfactory functional outcome OR organpreservation surgical expertise is unavailable Narrow margin excision followed by postoperative radiation therapy IS NOT an acceptable treatment approach
34 T3, T4 Organ preservation surgery, Ch-RT, Chi RT and Rt alone offer potential for larynx preservation without compromising survival Tt selection depends on: pt factors, local expertise and rehabilitation services Pt with tumor penentration through cartilage into soft tissues are considered poor candidates for larynxpreservation approach. LT is recommended in these cases
35 Factors associated with decreased larynxpreservation outcomes: Male gender Anemia (at start of treatment) Smoking Advanced T stage Clinically detectable impaired vocal cord mobility Subglottic extension Involvement of anterior commissure Large tumor volume Invasion of specific anatomic sites (determined by CT or MRI)
,")
36 Recommended management approach for treatment of resectable T3-4 N0-3 laryngeal cancer JCO, Vol 31, No7 (march1), 2013:pp
37 CONCLUSIONS Larynx-preservation therapy is intended to offer improved function and quality of life without compromising survival. All patients with T1-T2 should be treated initially with intent to preserve the larynx. Pt with T3- selected T4 should be offered a larynxpreservation treatment option. Chemoradiotherapy & Induction Chemotherapy are alternatives
38 CONCLUSIONS Preservation of the laryngeal structure is not considered a functional success if persistent dysphagia, aspiration, or chronic tracheostomy. Selection of treatment for laryngeal cancer should always depend on patient factors, local expertise, and appropiated support and rehabilitative services. A multidisciplinary team with specialized expertise is necessary to ensure optimal outcomes.

39
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. American Society of Clinical Oncology Clinical Practice Guideline
 Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer. Dr P Vijay Anand Reddy Director Apollo Cancer Hospital
 Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Laryngeal and hypopharyngeal cancers
 Laryngeal and hypopharyngeal cancers Induction Chemotherapy in combined modality approaches Atenas 16.09.2017 Ana Ferreira Castro, MD Medical Oncology Centro Hospitalar do Porto Instituto de Ciências Biomédicas
Laryngeal and hypopharyngeal cancers Induction Chemotherapy in combined modality approaches Atenas 16.09.2017 Ana Ferreira Castro, MD Medical Oncology Centro Hospitalar do Porto Instituto de Ciências Biomédicas
Larynx Hypopharynx. Therapy algorithms. Why larynx preservation at all? State of the art Jean Louis Lefebvre,Lille Jan Klozar,Prague
 Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and NeckCancer: multi-modal therapeuticintegration
 Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer
 to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer") The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology 2018 www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck. Mei Tang, MD
 Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX
 Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Sanguineti s (2)Comment: When it was initially published in 2003 with a median follow-up of 3.8 years (4), the RTOG study led to a change in
Comment: When it was initially published in 2003 with a median follow-up of 3.8 years (4), the RTOG study led to a change in") Commento di due Soci AIRO pubblicati su due prestigiose riviste internazionali al Trial della forastiere et al. Long term results of RTOG:91-11 (a cura di Dr. Russi e Dr. Testolin )! Forastiere)et)al.)Long/Term)Results)of)RTOG)91/11:)A)Comparison)of)
Commento di due Soci AIRO pubblicati su due prestigiose riviste internazionali al Trial della forastiere et al. Long term results of RTOG:91-11 (a cura di Dr. Russi e Dr. Testolin )! Forastiere)et)al.)Long/Term)Results)of)RTOG)91/11:)A)Comparison)of)
Guillaume Janoray, Yoann Pointreau, Pascal Garaud, Sophie Chapet, Marc Alfonsi, Christian Sire, Eric Jadaud, Gilles Calais
 JNCI J Natl Cancer Inst (016) 108(4): djv368 doi:10.1093/jnci/djv368 First published online December 16, 015 Article Long-Term Results of a Multicenter Randomized Phase III Trial of Induction Chemotherapy
JNCI J Natl Cancer Inst (016) 108(4): djv368 doi:10.1093/jnci/djv368 First published online December 16, 015 Article Long-Term Results of a Multicenter Randomized Phase III Trial of Induction Chemotherapy
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC)
") Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC) Amanda Psyrri, MD,FACP Attikon University Hospital Athens, Greece Learning objectives After reading and reviewing this material,
Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC) Amanda Psyrri, MD,FACP Attikon University Hospital Athens, Greece Learning objectives After reading and reviewing this material,
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
Survey of Laryngeal Cancer at SBUH comparing 108 cases seen here from to the NCDB of 9,256 cases diagnosed nationwide in 2000
 Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Survey of Laryngeal Cancer at comparing 108 cases seen here from 1998 2002 to the of 9,256 cases diagnosed nationwide in 2000 Stony Brook University Hospital Cancer Program Annual Report 2002-2003 Gender
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head & Neck Cancer: When to Irradiate
 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck. Raul Giglio
 State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
5/20/ ) Haffty GB: Concurrent chemoradiation in the treatment of head and neck cancer. Hematol. Oncol. Clin: North Am.
 Haffty GB: Concurrent chemoradiation in the treatment of head and neck cancer. Hematol. Oncol. Clin: North Am.") Prague, 24-25 25 April 29 ALTERNATING CHEMORADIATION: FOR WHOM? M. Merlano MD Holy Cross Gen. Hospital Cuneo - Italy ALTERNATING CHEMORADIATION: FOR WHOM? Definition of alternating chemoradiation Targets
Prague, 24-25 25 April 29 ALTERNATING CHEMORADIATION: FOR WHOM? M. Merlano MD Holy Cross Gen. Hospital Cuneo - Italy ALTERNATING CHEMORADIATION: FOR WHOM? Definition of alternating chemoradiation Targets
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
State of the art for radiotherapy of SCCHN
 State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
The Role of Docetaxel in the Treatment of Head and Neck Cancer
 GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Practice teaching course on head and neck cancer management
 28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Nicolas Magné France
28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Nicolas Magné France
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations
 Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Adjuvant Chemotherapy
 State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
The management of advanced supraglottic and
 ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
ORIGINAL ARTICLE ORGAN PRESERVATION FOR ADVANCED LARYNGEAL CARCINOMA Robert L. Foote, MD, 1 R. Tyler Foote, 1 Paul D. Brown, MD, 1 Yolanda I. Garces, MD, 1 Scott H. Okuno, MD, 2 Scott E. Strome, MD 3 1
Head and Neck Cancer:
 Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Title. CitationInternational Journal of Clinical Oncology, 20(6): 1. Issue Date Doc URL. Rights. Type. File Information
: 1. Issue Date Doc URL. Rights. Type. File Information") Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
Title Clinical outcomes of weekly cisplatin chemoradiother Sakashita, Tomohiro; Homma, Akihiro; Hatakeyama, Hir Author(s) Takatsugu; Iizuka, Satoshi; Onimaru, Rikiya; Tsuchiy CitationInternational Journal
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER
 ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
ORIGINAL ARTICLE CHEMOTHERAPY ALONE FOR ORGAN PRESERVATION IN ADVANCED LARYNGEAL CANCER Vasu Divi, MD, 1 * Francis P. Worden, MD, 1,2 * Mark E. Prince, MD, 1 Avraham Eisbruch, MD, 3 Julia S. Lee, MD, 4
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
RT +/- Surgery. Concurrent ChemoRT +/- Surgery
 Molecular targeted approaches to head and neck cancer Lillian L. Siu Department of Medical Oncology & Hematology Princess Margaret Hospital, University of Toronto Locally Advanced HNSCC Locally Advanced
Molecular targeted approaches to head and neck cancer Lillian L. Siu Department of Medical Oncology & Hematology Princess Margaret Hospital, University of Toronto Locally Advanced HNSCC Locally Advanced
Diagnosis and what happens after referral
 Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
T1/T2 LARYNX CANCER. Click to edit Master Presentation Date. Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery
 ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
ADVANCES IN TREATMENT OF T1/T2 LARYNX CANCER Click to edit Master Presentation Date Thomas J Gernon, MD Otolaryngology-Head and Neck Surgery I have nothing to disclose CHANGING TRENDS IN HNSCC GLOTTIC
RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus
 RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus Department of Radiation Oncology Mallinckrodt Institute of Radiology/
RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus Department of Radiation Oncology Mallinckrodt Institute of Radiology/
Head and Neck Cancer: 2016 It s Not What You Think!
 Head and Neck Cancer: 2016 It s Not What You Think! New Treatments, Improved Outcomes, and A Sexually Transmitted Disease? John R. Clark, MD Clinical Director, Center for Head and Neck Oncology Massachusetts
Head and Neck Cancer: 2016 It s Not What You Think! New Treatments, Improved Outcomes, and A Sexually Transmitted Disease? John R. Clark, MD Clinical Director, Center for Head and Neck Oncology Massachusetts
journal of medicine The new england Concurrent Chemotherapy and Radiotherapy for Organ Preservation in Advanced Laryngeal Cancer abstract
 The new england journal of medicine established in 1812 november 27, 2003 vol. 349 no. 22 Concurrent Chemotherapy and Radiotherapy for Organ Preservation in Advanced Laryngeal Cancer Arlene A. Forastiere,
The new england journal of medicine established in 1812 november 27, 2003 vol. 349 no. 22 Concurrent Chemotherapy and Radiotherapy for Organ Preservation in Advanced Laryngeal Cancer Arlene A. Forastiere,
Prognostic significance of thyroid or cricoid cartilage invasion in laryngeal or hypopharyngeal cancer treated with organ preserving strategies
 Wagner et al. Radiation Oncology 2012, 7:219 RESEARCH Open Access Prognostic significance of thyroid or cricoid cartilage invasion in laryngeal or hypopharyngeal cancer treated with organ preserving strategies
Wagner et al. Radiation Oncology 2012, 7:219 RESEARCH Open Access Prognostic significance of thyroid or cricoid cartilage invasion in laryngeal or hypopharyngeal cancer treated with organ preserving strategies
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
Adjuvant radiotherapy for completely resected early stage NSCLC
 Adjuvant radiotherapy for completely resected early stage NSCLC ESMO Preceptorship on lung Cancer Manchester March 2018 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique
Adjuvant radiotherapy for completely resected early stage NSCLC ESMO Preceptorship on lung Cancer Manchester March 2018 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique
Recent Advances & Ongoing Challenges in Head & Neck Cancers
 Recent Advances & Ongoing Challenges in Head & Neck Cancers Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School Boston, MA Disclosures
Recent Advances & Ongoing Challenges in Head & Neck Cancers Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School Boston, MA Disclosures
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing.
 The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
The aim of the horizontal supra-glottic laryngectomy is: To remove the tumour with good safety margin, To leave a functioning i larynx i.e. respiration, phonation & swallowing. Disadvantages of classical
Accepted 2 December 2008 Published online in Wiley InterScience (www.interscience.wiley.com). DOI: /hed.21081
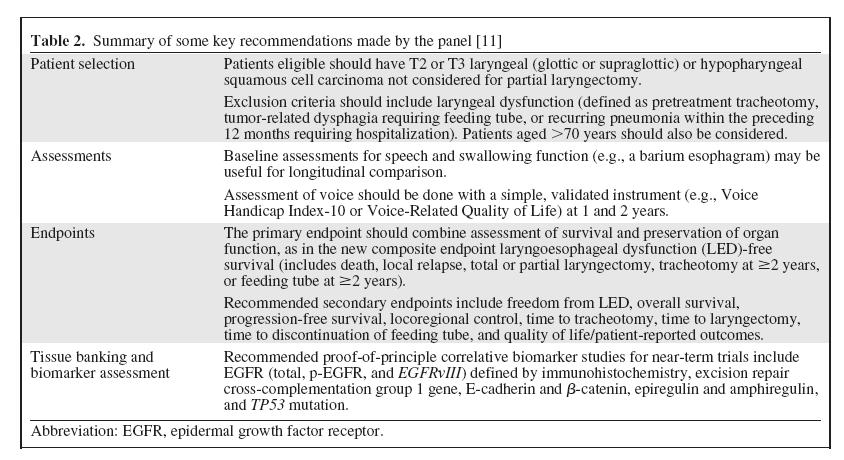
. DOI: /hed.21081") CONSENSUS DOCUMENT LARYNX PRESERVATION CLINICAL TRIAL DESIGN: KEY ISSUES AND RECOMMENDATIONS A CONSENSUS PANEL SUMMARY Jean-Louis Lefebvre, MD, 1 K. Kian Ang, MD, 2 on behalf of the Larynx Preservation
CONSENSUS DOCUMENT LARYNX PRESERVATION CLINICAL TRIAL DESIGN: KEY ISSUES AND RECOMMENDATIONS A CONSENSUS PANEL SUMMARY Jean-Louis Lefebvre, MD, 1 K. Kian Ang, MD, 2 on behalf of the Larynx Preservation
RAMY R. GHALI, M.D.*; EMAN EL-SHARAWY, M.D.*; AZZA M. ADEL, M.D.* and SAMER A. IBRAHIM, M.D.**
 Med. J. Cairo Univ., Vol. 79, No. 2, June: 13-18, 2011 www.medicaljournalofcairouniversity.com Induction Docetaxel, Cisplatin and 5 Fluorouracil (TPF) Followed by Concomitant Chemoradiotherapy Versus Concomitant
Med. J. Cairo Univ., Vol. 79, No. 2, June: 13-18, 2011 www.medicaljournalofcairouniversity.com Induction Docetaxel, Cisplatin and 5 Fluorouracil (TPF) Followed by Concomitant Chemoradiotherapy Versus Concomitant
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience. Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore
 Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
Surf, Sea and Supracricoid Laryngectomy: A Queensland Experience Jeeve Kanagalingam Associate Consultant Tan Tock Seng Hospital Singapore Queensland 2500 times the size of Singapore Same population as
FRCS Otolarynoglogy VIVA Course Dundee Guidelines. Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool
 FRCS Otolarynoglogy VIVA Course Dundee www.frcsentvivacourse.co.uk Guidelines Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool Marking Descriptors Available from JCIE website if search for
FRCS Otolarynoglogy VIVA Course Dundee www.frcsentvivacourse.co.uk Guidelines Andrew Kinshuck ST-8 ENT Aintree University Hospital, Liverpool Marking Descriptors Available from JCIE website if search for
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Nasopharyngeal Cancer:Role of Chemotherapy
 Nasopharyngeal Cancer:Role of Chemotherapy PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 16/9/2017 2 nd Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Nasopharyngeal Cancer:Role of Chemotherapy PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 16/9/2017 2 nd Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Quality of life in patients treated for advanced hypopharyngeal or laryngeal cancer
 European Annals of Otorhinolaryngology, Head and Neck diseases (2011) 128, 218 223 ORIGINAL ARTICLE Quality of life in patients treated for advanced hypopharyngeal or laryngeal cancer M. Guibert a, B.
European Annals of Otorhinolaryngology, Head and Neck diseases (2011) 128, 218 223 ORIGINAL ARTICLE Quality of life in patients treated for advanced hypopharyngeal or laryngeal cancer M. Guibert a, B.
NEWER DRUGS IN HEAD AND NECK CANCER. Prof. Anup Majumdar. HOD, Radiotherapy, IPGMER Kolkata
 NEWER DRUGS IN HEAD AND NECK CANCER Prof. Anup Majumdar HOD, Radiotherapy, IPGMER Kolkata 1 Included Oral cavity Nasal cavity Pharynx Larynx Lymph node in upper part of neck Excluded Brain Eye Cancer arising
NEWER DRUGS IN HEAD AND NECK CANCER Prof. Anup Majumdar HOD, Radiotherapy, IPGMER Kolkata 1 Included Oral cavity Nasal cavity Pharynx Larynx Lymph node in upper part of neck Excluded Brain Eye Cancer arising
Chemoselection as a Strategy for Organ Preservation in Patients with T4 Laryngeal Squamous Cell Carcinoma with Cartilage Invasion
 The Laryngoscope VC 2009 The American Laryngological, Rhinological and Otological Society, Inc. Chemoselection as a Strategy for Organ Preservation in Patients with T4 Laryngeal Squamous Cell Carcinoma
The Laryngoscope VC 2009 The American Laryngological, Rhinological and Otological Society, Inc. Chemoselection as a Strategy for Organ Preservation in Patients with T4 Laryngeal Squamous Cell Carcinoma
Radio(chemo)therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology
therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology") Radio(chemo)therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology March 2018 > Half million new cases HNC/year in world 50-60% cured not cured
Radio(chemo)therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology March 2018 > Half million new cases HNC/year in world 50-60% cured not cured
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
ASCO Highlights Head and Neck Cancer
 ASCO Highlights Head and Neck Cancer Anne S. Tsao, M.D. Director, Mesothelioma Program Assistant Professor July 11, 2009 The University of Texas MD ANDERSON CANCER CENTER Department of Thoracic/Head &
ASCO Highlights Head and Neck Cancer Anne S. Tsao, M.D. Director, Mesothelioma Program Assistant Professor July 11, 2009 The University of Texas MD ANDERSON CANCER CENTER Department of Thoracic/Head &
North of Scotland Cancer Network Clinical Management Guideline for Oropharyngeal Cancer
 Nth of Scotland Cancer Netwk Clinical Management Guideline f Oropharyngeal Cancer UNCONTROLLED WHEN PRINTED Based on NHST CMG with further extensive consultation within NOSCAN DOCUMENT CONTROL Original
Nth of Scotland Cancer Netwk Clinical Management Guideline f Oropharyngeal Cancer UNCONTROLLED WHEN PRINTED Based on NHST CMG with further extensive consultation within NOSCAN DOCUMENT CONTROL Original
Nasopharyngeal Cancer/Multimodality Treatment
 Nasopharyngeal Cancer/Multimodality Treatment PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 22/10/2016 1 st Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Nasopharyngeal Cancer/Multimodality Treatment PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 22/10/2016 1 st Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
The effect of induction chemotherapy followed by chemoradiotherapy in advanced head and neck cancer: a prospective study
 International Journal of Research in Medical Sciences Nikam BM et al. Int J Res Med Sci. 2014 May;2(2):476-480 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: 10.5455/2320-6012.ijrms20140519
International Journal of Research in Medical Sciences Nikam BM et al. Int J Res Med Sci. 2014 May;2(2):476-480 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: 10.5455/2320-6012.ijrms20140519
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
ROLE OF ALTERED FRACTIONATION & CHEMORADIATION IN HEAD AND NECK CANCER
 ROLE OF ALTERED FRACTIONATION & CHEMORADIATION IN HEAD AND NECK CANCER What is conventional fractionation? Radiation is given at doses of 1.8 to 2.0 Gy delivered once daily, 5 days weekly for 6 to 7 weeks.
ROLE OF ALTERED FRACTIONATION & CHEMORADIATION IN HEAD AND NECK CANCER What is conventional fractionation? Radiation is given at doses of 1.8 to 2.0 Gy delivered once daily, 5 days weekly for 6 to 7 weeks.
Present and Future of Head and Neck Cancer Therapy (Focus at systemic therapy)
") Present and Future of Head and Neck Cancer Therapy (Focus at systemic therapy) Jan B; Vermorken, MD, PhD Department of Medical Oncology Antwerp University Hospital Edegem, Belgium 1st Hellenic Conference
Present and Future of Head and Neck Cancer Therapy (Focus at systemic therapy) Jan B; Vermorken, MD, PhD Department of Medical Oncology Antwerp University Hospital Edegem, Belgium 1st Hellenic Conference
Therapy of Locally Advanced Head and Neck Cancer: State of the Art
 Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Persistent tracheostomy after primary chemoradiation for advanced laryngeal or hypopharyngeal cancer
 ORIGINAL ARTICLE Persistent tracheostomy after primary chemoradiation for advanced laryngeal or hypopharyngeal cancer Paul A. Tennant, MD, * Elizabeth Cash, PhD, Jeffrey M. Bumpous, MD, Kevin L. Potts,
ORIGINAL ARTICLE Persistent tracheostomy after primary chemoradiation for advanced laryngeal or hypopharyngeal cancer Paul A. Tennant, MD, * Elizabeth Cash, PhD, Jeffrey M. Bumpous, MD, Kevin L. Potts,
PROSTATA MULTIDISCIPLINARITA IN URO-ONCOLOGIA INTEGRAZIONE TERAPIA SISTEMICA-TRATTAMENTO LOCALE. Dr.ssa Ori Ishiwa Dr Sergio Bracarda
 15 anno di fondazione del GUONE MULTIDISCIPLINARITA IN URO-ONCOLOGIA Aviano, 10 settembre 2010 INTEGRAZIONE TERAPIA SISTEMICA-TRATTAMENTO LOCALE PROSTATA Dr.ssa Ori Ishiwa Dr Sergio Bracarda UOC Oncologia
15 anno di fondazione del GUONE MULTIDISCIPLINARITA IN URO-ONCOLOGIA Aviano, 10 settembre 2010 INTEGRAZIONE TERAPIA SISTEMICA-TRATTAMENTO LOCALE PROSTATA Dr.ssa Ori Ishiwa Dr Sergio Bracarda UOC Oncologia
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue
 Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
Wojciech K. Mydlarz, M.D. Pharyngocutaneous Fistulas after Salvage Laryngectomy: Need for Vascularized Tissue Disclosures No Relevant Financial Relationships or Commercial Interests Educational Objectives
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI
 XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
Hypopharynx. 1. Introduction. 1.1 General Information and Aetiology
 Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the
Hypopharynx 1. Introduction 1.1 General Information and Aetiology The human pharynx is the part of the throat situated between the nasal cavity and the esophagus and can be divided into three parts: the