Curative approach for prostate cancer with 1-2 Bone Metastases
|
|
|
- Theodora Wood
- 6 years ago
- Views:
Transcription
1 Curative approach for prostate cancer with 1-2 Bone Metastases Mack Roach III, MD Professor of Radiation Oncology & Urology UCSF Helen-Diller Family Comprehensive Cancer Center Department of Radiation Oncology, Mt Zion Hospital, San Francisco, CA
2 Disclosure Potential conflicts of interest: Employment: University of California San Francisco, The National Cancer Institute (Funding & Board Member of the National Cancer Advisory Board (NCAB)) Consulting: Ferring, Johnson & Johnson (Janssen) Pharmaceuticals and the International Atomic Energy Agency (IAEA) (consultant) Speaker Support: An honorarium is provided by Accuray for this presentation Leadership: American Cancer Society (ACS), NCAB, NRG (NSABP/RTOG/GOG)
3 Disclaimer The views expressed in this presentation are those of the presenters and do not necessarily reflect the views or policies of Accuray Incorporated or its subsidiaries. No official endorsement by Accuray Incorporated or any of its subsidiaries of any vendor, products or services contained in this presentation is intended or should be inferred.
4 Analysis of risk factors for progression in patients with pathologically confined prostate cancers after radical retropubic prostatectomy. Lerner et al. J Urol 156: , 1996 All 904 men treated with curative intent: If you don t treat for cure, you wont cure those you treated Ted Phillips Kaplan-Meir progression-free (PSA> 0.2 ng/ml) survival estimates for 904 patients with pathologically organ confined prostate cancer (pt2 or less)
5 Roach et al. IJROBP 2015 Figures1b: Graphical summary of the median difference in the estimated 10 year CSS (b) by the dichotomized reliability score (RS) (< to 12 vs. >12). Above 0 indicates benefit for RP, at 0 no differences between treatments and below 0 a benefit to RT +/- androgen deprivation therapy (ADT). Broken lines (---) indicate the pointwise 95% CI based on bootstrap estimation of 100,000 replicates, and the black dotted line indicates the overall differences.
6 Acta Oncologica, 2015; 54: ORIGINAL ARTICLE Radical prostatectomy versus high-dose irradiation in localized/locally advanced prostate cancer: A Swedish multicenter randomized trial with patient-reported outcomes. Lennermas et al. RP vs HDR+EBRT + 6 mo. ADT in PC pts in Sweden M & M: T1b-T3a, N0, M0 and PSA</=50 ng/ml RESULTS: survival rate ~ 76%. Only eight pts (9%) died of PC. CONCLUSION: RP and HDR + EBRT appeared to be comparable...

7 Selected Papers on Non-classic Radiation and ADT 2/1/ Modified from Corso Ali and Diaz Am J Cancer Res 2011; 1(3):
8 Non-classic Radiation Effects Zhang et al. JEM 204:49-55, 2007 * *C3H Rag2-/- mice have stroma incapable of cross-presenting tumor antigens
9 Selected Papers on Non-classic Radiation and ADT Antigens No. of models Type of Model P-Selectin / E-Selectin 11 In Vivo & Vitro ICAM-1 (CD54)/ NCAM (CD56) / V-CAM 16 In Vivo & Vitro PECAM-1 (CD31) 5 In Vivo & Vitro α2β3 Integrin / B1 Integrin 3 In Vitro E-Cadherin (CD324) 2 In Vivo & Vitro MHC Class 1 10 In Vitro CD80(B7.1) / CD20 7 In Vitro NKG2D Ligand (MICA, MICB, ULBP1,2,3) / Fas (CD95/Apo-1) 6 In Vivo & Vitro FasL / Trail-R1 &Trail-R2 (DR4 & DR5) / GRP78 (BiP) 7 In Vivo & Vitro Calreticulin / 2 In Vitro ERp57 (grp58 / PDIA3) 1 In Vitro CEA 5 In Vitro TIP-1 1 In Vivo & Vitro Modified from Corso Ali and Diaz Am J Cancer Res 2011; 1(3):
10
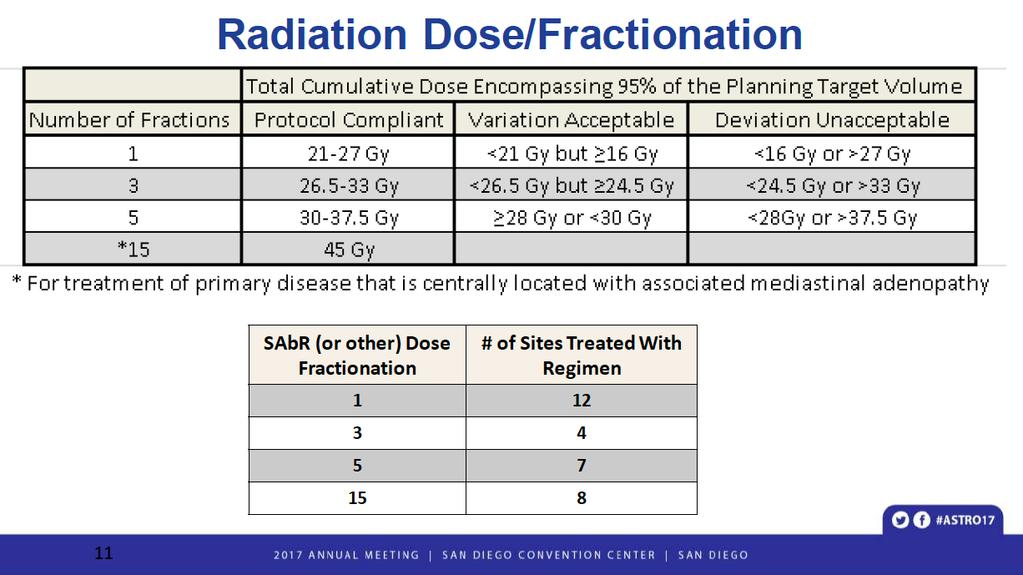
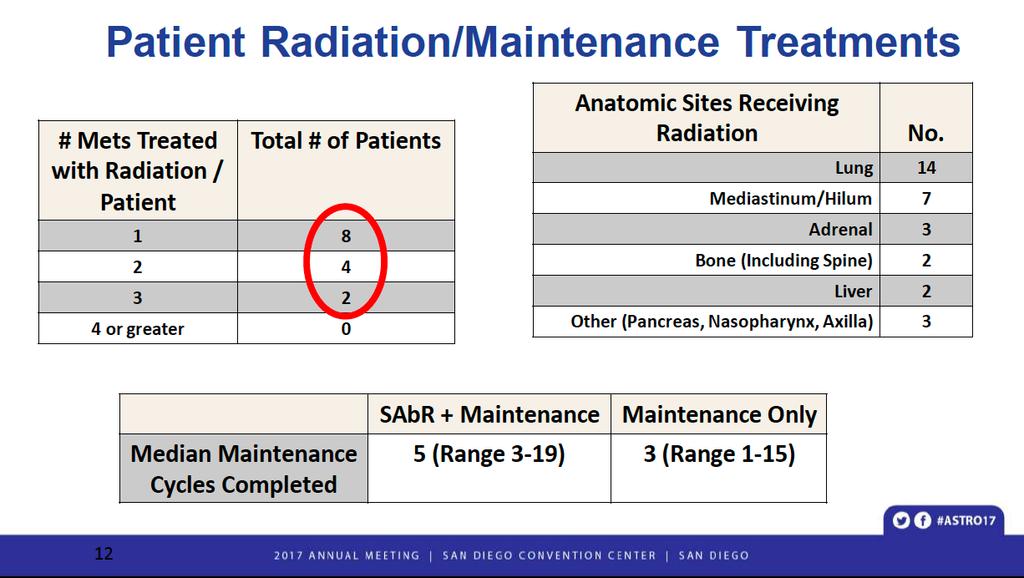
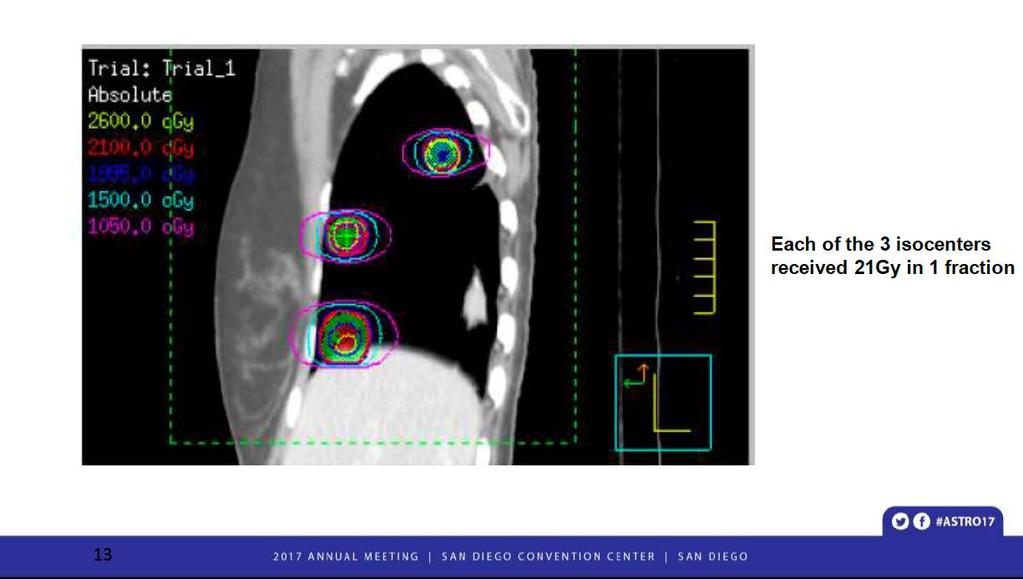
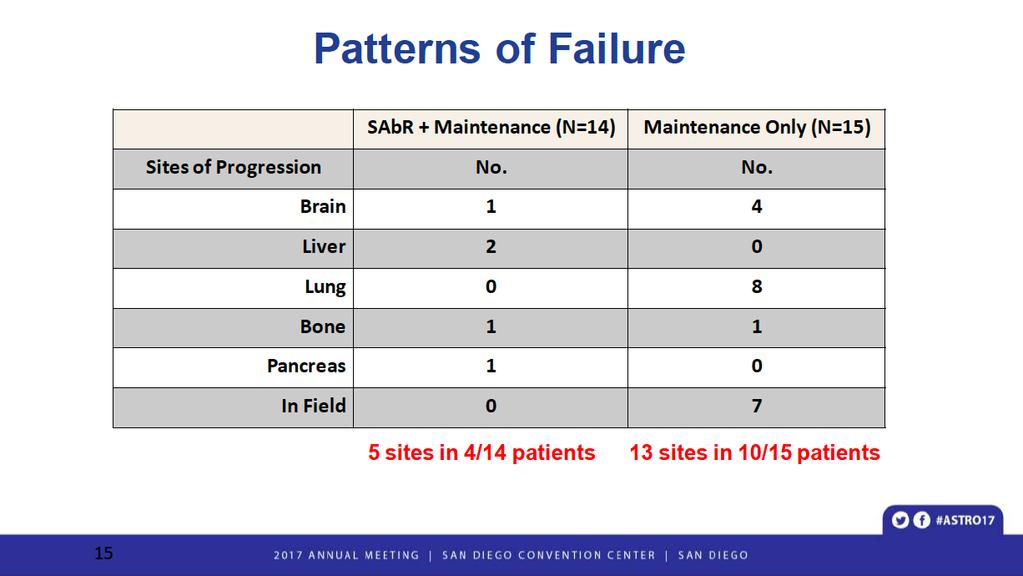
11 Consolidative Radiotherapy for Limited Metastatic Non-Small Cell Lung Cancer (NSCLC): A Randomized Phase II Trial P. Iyengar, V. Tumati, D. Gerber, Z. Wardak, C. Ahn, R. Hughes, J. Dowell, N. Cheedella, L. A. Nedzi, K. D. Westover, S. Pulipparacharuvil, H. Choy and R. D. Timmerman University of Texas Southwestern Medical Center, Dallas, TX
12
13
14
15
16
17
18 Harris et al. Prostate 68: , 2008
19 Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, Lambert B, Delrue L, Bultijnck R, Claeys T, Goetghebeur E, Villeirs G, De Man K, Ameye F, Billiet I, Joniau S, Vanhaverbeke F, De Meerleer G. J Clin Oncol Dec 14:JCO Multicenter, randomized, phase II study, patients with asymptomatic PCa were eligible if they had had a biochemical recurrence after primary PCa treatment with curative intent, three or fewer extracranial metastatic lesions on choline PET/CT, and serum testosterone levels > 50 ng/ml. Patients were randomly assigned (1:1) to either surveillance or MDT of all detected lesions (surgery or SBRT). Surveillance was performed with PSA follow-up Q 3 months, with repeated imaging at PSA progression or clinical suspicion for progression. Random assignment was balanced dynamically on the basis of two factors: PSA doubling time (</= 3 v > 3 months) and nodal versus non-nodal mets. The primary end point was ADT-free survival. ADT was started at symptomatic progression, progression to more than 3 mets, or local progression of known mets.

20 Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, Lambert B, Delrue L, Bultijnck R, Claeys T, Goetghebeur E, Villeirs G, De Man K, Ameye F, Billiet I, Joniau S, Vanhaverbeke F, De Meerleer G.
21 Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, Lambert B, Delrue L, Bultijnck R, Claeys T, Goetghebeur E, Villeirs G, De Man K, Ameye F, Billiet I, Joniau S, Vanhaverbeke F, De Meerleer G. Results Between August 2012 and August 2015, 62 patients were enrolled. At a median follow-up time of 3 years, the median ADT-free survival was 13 months (80% CI, 12 to 17 months) for the surveillance group and 21 months (80% CI, 14 to 29 months) for the MDT group (hazard ratio, 0.60 [80% CI, 0.40 to 0.90]; log-rank P =.11). QOL was similar between arms at baseline and remained comparable at 3-month and 1-year fu. Six pts developed grade 1 toxicity in the MDT arm. No grade 2 to 5 toxicity was observed. Conclusion ADT-free survival was longer with MDT than with surveillance alone for oligorecurrent PCa, suggesting that MDT should be explored further in phase III trials.
22 Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, Lambert B, Delrue L, Bultijnck R, Claeys T, Goetghebeur E, Villeirs G, De Man K, Ameye F, Billiet I, Joniau S, Vanhaverbeke F, De Meerleer G.
23 Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, Lambert B, Delrue L, Bultijnck R, Claeys T, Goetghebeur E, Villeirs G, De Man K, Ameye F, Billiet I, Joniau S, Vanhaverbeke F, De Meerleer G. Forest plots of the association between MDT and ADT free survival (A) intent-to-treat and (B) per protocol (C) Kaplan-meier plot comparing biochemical recurrence-free survival intension-to-treat analysis
24 Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, Lambert B, Delrue L, Bultijnck R, Claeys T, Goetghebeur E, Villeirs G, De Man K, Ameye F, Billiet I, Joniau S, Vanhaverbeke F, De Meerleer G. The Devil is in the details 1. Feasibility of Phase III Trial 2. Up to 3 extra-cranial sites by Choline PET/CT 3. Castrate sensitive 4. Controlled primary: a) (-) multi-parametric MRI or Bx (i.e. local control) with (-) PET
25 Contemporary Phase III Prostate Cancer Trials (ADT +/- RT) Widmark et al. (2009) Warde et al. (2011) Conclusion: Better survival with ADT (mostly antiandrogens) + RT. Median-Follow Up: 7.6; NNT: 10.2; Curves separate beyond 5 years Conclusion: Better survival with RT+ADT (LHRH drug used) Median-Follow Up: 6; NNT: 9.9; Curves separate beyond 5 years

26 The Concept of Bone Mets Spawn More Bone Mets 1 Recently Demonstrated The bone matrix is fertile soil that stimulates growth of tumor cells 2 The same tumor cells travel from site to site and establish additional metastatic lesions 1 Supports seed and soil theory where subclones develop the potential to metastasize on their own and spread, rather than being a property of the primary tumor 1 Gundem G et al. Nature. 2015;520(7547): Yin JJ et al. Cell Res. 2005;15(1):57-62.
27 Major Take Home Message: Curative approach for Prostate Cancer with 1-2 Bone Metastases 1. We have NO level I evidence that patients are curable when treated for 1-2 bone metastases. They live longer, but: a. There are suggestive data and a plausible biologic rationale b. Radiotherapy may be uniquely suited to combine with immunotherapy and may enhance control systemic disease! c. Bone to bone mets a real problem? d. Much work remains to be done!!!!!!!!
28 Palliation of urinary obstruction from advanced prostate cancer with SBRT. Lauren Boreta, David Ronan Raleigh, Mack Roach III; University of California San Francisco, San Francisco, CA ASCO PALLIATIVE & SUPPORTIVE CARE ONCOLOGY SYMPOSIUM 2017 Background: In patients with advanced prostate cancer (PCa), urinary obstruction (UO) can lead to urinary retention requiring indwelling or suprapubic catheterization, which negatively impacts quality of life. Palliative options for UO from advanced PCa include surgical and medical treatment. Surgical intervention, including prostatectomy, pelvic exenteration and TURP, may confer undue risk to patients... Medical palliation may require months to take effect. Stereotactic Body Radiotherapy (SBRT) is a non-invasive technique that delivers high-dose and highly conformal radiation in 5 fractions... Methods: A retrospective review of patients undergoing SBRT for UO was completed at a single institution between 2011 and Stage, PSA at diagnosis and time of treatment were recorded. Assessment of urinary function by IPSS/SHIM and documentation of catheterization were reviewed at consultation and subsequent follow-up. Results: A total of 3 patients were treated with SBRT to the prostate for the palliation of urinary obstruction. Patient ages were 67, 57 and 52 years, and all had high risk, stage IV disease, Gleason 4+4 or 4+5, T3 or T4, with regional nodal, bony or visceral metastases. All patients required indwelling catheterization for an average 4 months prior to SBRT. Two patients were treated with whole pelvis irradiation after SBRT. In those who received subsequent pelvic irradiation, the SBRT doses to the prostate were 19 Gy in 2 fractions. The patient treated with SBRT monotherapy received 38 Gy in 4 fractions. Catheters were successfully removed in all 3 patients, one at the completion of radiation, and the others within 4 weeks of completion. With fu (1.2 to 6 yrs), no patients required re-catheterization, and there were no reports of grade 3 acute or long-term toxicity. Conclusions: SBRT is an effective treatment to palliate UO from locally advanced PCa, leading to removal of urinary catheters and presumed improved in quality of life. Further investigation is required to establish the optimal dose and fractionation of palliative SBRT for UO from PCa
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
SIMPOSIO. Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico
 SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Oligometastasis. Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie?
 Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Non-systemic treatment of low-volume metastatic disease.
 Non-systemic treatment of low-volume metastatic disease. Gert De Meerleer, M.D., Ph.D. Gent University Hospital om behalf of POMP study group Background Patients with metastatic prostate cancer are considered
Non-systemic treatment of low-volume metastatic disease. Gert De Meerleer, M.D., Ph.D. Gent University Hospital om behalf of POMP study group Background Patients with metastatic prostate cancer are considered
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps?
 Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Does Imaging of Advanced PC change a suggested treatment?
 Does Imaging of Advanced PC change a suggested treatment? Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials and conflict
Does Imaging of Advanced PC change a suggested treatment? Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials and conflict
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer
 Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer after prostatectomy, radiation therapy and HiFU R. Schwartzberg, E. Günther, N. Klein, S. Zapf, R. El-Idrissi, J. Cooper, B.
Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer after prostatectomy, radiation therapy and HiFU R. Schwartzberg, E. Günther, N. Klein, S. Zapf, R. El-Idrissi, J. Cooper, B.
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology
 Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy combined HDR + EBRT 574 HDR monotherapy Total Patients
 Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Salvage Stereotactic Body Radiotherapy for Patients With Limited Prostate Cancer Metastases: Deferring Androgen Deprivation Therapy
 Salvage Stereotactic Body Radiotherapy for Patients With Limited Prostate Cancer Metastases: Deferring Androgen Deprivation Therapy Patrick Berkovic, 1 Gert De Meerleer, 1 Louke Delrue, 2 Bieke Lambert,
Salvage Stereotactic Body Radiotherapy for Patients With Limited Prostate Cancer Metastases: Deferring Androgen Deprivation Therapy Patrick Berkovic, 1 Gert De Meerleer, 1 Louke Delrue, 2 Bieke Lambert,
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience.
 Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience. Elisabetta Ponti MD, Gianluca Ingrosso MD, Alessandra Carosi PhD, Luana
Stereotactic body radiation therapy in oligometastatic patient with lymph node recurrent prostate cancer: a single centre experience. Elisabetta Ponti MD, Gianluca Ingrosso MD, Alessandra Carosi PhD, Luana
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE. ELENA CASTRO Spanish National Cancer Research Centre
 VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
SRO Tutorial: Prostate Cancer Clinics
 SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Novel Imaging in Advanced Prostate Cancer
 Novel Imaging in Advanced Prostate Cancer Robert J. Hamilton, MD MPH FRCSC Princess Margaret Cancer Centre ICUC Saturday January 21, 2017 Company/Organizati Details Faculty/Presenter on Disclosures I am
Novel Imaging in Advanced Prostate Cancer Robert J. Hamilton, MD MPH FRCSC Princess Margaret Cancer Centre ICUC Saturday January 21, 2017 Company/Organizati Details Faculty/Presenter on Disclosures I am
Stereotactic Ablative Radiotherapy for Prostate Cancer
 Stereotactic Ablative Radiotherapy for Prostate Cancer Laurie Cuttino, MD Associate Professor of Radiation Oncology VCU Massey Cancer Center Director of Radiation Oncology Sarah Cannon Cancer Center at
Stereotactic Ablative Radiotherapy for Prostate Cancer Laurie Cuttino, MD Associate Professor of Radiation Oncology VCU Massey Cancer Center Director of Radiation Oncology Sarah Cannon Cancer Center at
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
PSMA PET in patients with prostate cancer
 PSMA PET in patients with prostate cancer Thomas Hope, MD Assistant Professor of Radiology, UCSF Abdominal Imaging and Nuclear Medicine Co-director, PET/MRI Chief of MRI, San Francisco VA Medical Center
PSMA PET in patients with prostate cancer Thomas Hope, MD Assistant Professor of Radiology, UCSF Abdominal Imaging and Nuclear Medicine Co-director, PET/MRI Chief of MRI, San Francisco VA Medical Center
GUIDELINEs ON PROSTATE CANCER
 GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update
 Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update DONALD B. FULLER, M.D. RADIATION ONCOLOGIST GENESIS HEALTHCARE Disclosure & Disclaimer The
Prostate SBRT Heterogeneous Dose Distribution: Rationale, Methods, Outcomes and Future Direction: 2017 Update DONALD B. FULLER, M.D. RADIATION ONCOLOGIST GENESIS HEALTHCARE Disclosure & Disclaimer The
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
Treating Multiple. Brain Metastases (BM)
") ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
ESTRO 36 5-9 May 2017, Vienna Austria, Accuray Symposium Treating Multiple Brain Metastases (BM) with CyberKnife System Frederic Dhermain MD PhD, Radiation Oncologist Gustave Roussy University Hospital,
PACE Study. Hypofractionation 17/12/2014. Traditional Model of Fractionation 200 Response. What s the fraction sensitivity of prostate cancer?
 0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
0 0 17/12/2014 2 Outline of today s talk PACE Study Background rationale for PACE? Dr Nicholas van As A bit about technology. What is PACE? How can I get involved? London: 1 December 2014 250 Hypofractionation
Thoracic Recurrences. Soft tissue recurrence
 Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey
 Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Accepted Manuscript. Keeping Surgery Relevant in Oligometastatic Non-Small Cell Lung Cancer. Jessica S. Donington, MD, MSCR
 Accepted Manuscript Keeping Surgery Relevant in Oligometastatic Non-Small Cell Lung Cancer Jessica S. Donington, MD, MSCR PII: S0022-5223(18)32903-9 DOI: https://doi.org/10.1016/j.jtcvs.2018.10.124 Reference:
Accepted Manuscript Keeping Surgery Relevant in Oligometastatic Non-Small Cell Lung Cancer Jessica S. Donington, MD, MSCR PII: S0022-5223(18)32903-9 DOI: https://doi.org/10.1016/j.jtcvs.2018.10.124 Reference:
Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer
 ORIGINAL ARTICLE Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer Giorgio Lamanna, MD,* Claire Tabouret-Viaud,
ORIGINAL ARTICLE Long-term Results of a Comparative PET/CT and PET/MRI Study of 11 C-Acetate and 18 F-Fluorocholine for Restaging of Early Recurrent Prostate Cancer Giorgio Lamanna, MD,* Claire Tabouret-Viaud,
Oli-P and beyond Endpoints for PSMA based local ablative Radiotherapy. Dr. med. Fabian Lohaus Klinik und Poliklinik für Radioonkologie der TU Dresden
 Oli-P and beyond Endpoints for PSMA based local ablative Radiotherapy Dr. med. Fabian Lohaus Klinik und Poliklinik für Radioonkologie der TU Dresden Conflicts of interest none 1. The natural course of
Oli-P and beyond Endpoints for PSMA based local ablative Radiotherapy Dr. med. Fabian Lohaus Klinik und Poliklinik für Radioonkologie der TU Dresden Conflicts of interest none 1. The natural course of
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer in comparison to Radiotherapy alone:
 Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
University of California, Los Angeles, Los Angeles, CA, 2 FROS Radiation Oncology and CyberKnife Center, Flushing, NY, 3
 Long-Term Outcomes of Stereotactic Body Radiation Therapy for Low- and Intermediate-Risk Prostate Adenocarcinoma: A Multi-Institutional Consortium Study A. U. Kishan 1, A. Katz 2, C. A. Mantz 3, F. I.
Long-Term Outcomes of Stereotactic Body Radiation Therapy for Low- and Intermediate-Risk Prostate Adenocarcinoma: A Multi-Institutional Consortium Study A. U. Kishan 1, A. Katz 2, C. A. Mantz 3, F. I.
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
How to deal with patients who fail intracavitary treatment
 How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
J Clin Oncol 28: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 28 NUMBER 1 JANUARY 1 2010 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Clinical Results of Long-Term Follow-Up of a Large, Active Surveillance Cohort With Localized Prostate Cancer
VOLUME 28 NUMBER 1 JANUARY 1 2010 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Clinical Results of Long-Term Follow-Up of a Large, Active Surveillance Cohort With Localized Prostate Cancer
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Immunotherapy & radiotherapy
 Immunotherapy & radiotherapy Eric Deutsch MD PhD Gustave Roussy Cancer Campus Image courtesy of Gustave Roussy Institute Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation
Immunotherapy & radiotherapy Eric Deutsch MD PhD Gustave Roussy Cancer Campus Image courtesy of Gustave Roussy Institute Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice
 european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
Vertebral Body Compression Fracture Following Spine SBRT
 RADIATION ONCOLOGY & MOLECULAR RADIATION SCIENCES Vertebral Body Compression Fracture Following Spine SBRT Kristin J. Redmond, MD, MPH Disclosure & Disclaimer An honorarium is provided by Accuray for this
RADIATION ONCOLOGY & MOLECULAR RADIATION SCIENCES Vertebral Body Compression Fracture Following Spine SBRT Kristin J. Redmond, MD, MPH Disclosure & Disclaimer An honorarium is provided by Accuray for this
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
ADT vs chemo + ADT as initial treatment for advanced prostate cancer
 ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
Clinical Study Oncologic Outcomes of Surgery in T3 Prostate Cancer: Experience of a Single Tertiary Center
 Advances in Urology Volume 22, Article ID 64263, 8 pages doi:.55/22/64263 Clinical Study Oncologic Outcomes of Surgery in T3 Prostate Cancer: Experience of a Single Tertiary Center D. Milonas, G. Smailyte,
Advances in Urology Volume 22, Article ID 64263, 8 pages doi:.55/22/64263 Clinical Study Oncologic Outcomes of Surgery in T3 Prostate Cancer: Experience of a Single Tertiary Center D. Milonas, G. Smailyte,
State-of-the-art: vision on the future. Urology
 State-of-the-art: vision on the future Urology Francesco Montorsi MD FRCS Professor and Chairman Department of Urology San Raffaele Hospital Vita-Salute San Raffaele University Milan, Italy Disclosures
State-of-the-art: vision on the future Urology Francesco Montorsi MD FRCS Professor and Chairman Department of Urology San Raffaele Hospital Vita-Salute San Raffaele University Milan, Italy Disclosures
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Comparison of external radiation therapy vs radical prostatectomy in lymph node positive prostate cancer patients
 Comparison of external radiation therapy vs radical prostatectomy in lymph node positive prostate cancer patients R Kuefer 1, BG Volkmer 1, M Loeffler 1, RL Shen 2, L Kempf 3, AS Merseburger 4, JE Gschwend
Comparison of external radiation therapy vs radical prostatectomy in lymph node positive prostate cancer patients R Kuefer 1, BG Volkmer 1, M Loeffler 1, RL Shen 2, L Kempf 3, AS Merseburger 4, JE Gschwend
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC
 PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Prostatectomy as salvage therapy. Cases. Paul Cathcart - Guy s & St Thomas NHS Trust, London
 Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
When radical prostatectomy is not enough: The evolving role of postoperative
 When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
Navigating the Stream: Prostate Cancer and Early Detection. Ifeanyi Ani, M.D. TPMG Urology Newport News
 Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #104 (NQF 0390): Prostate Cancer: Combination Androgen Deprivation Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS
Quality ID #104 (NQF 0390): Prostate Cancer: Combination Androgen Deprivation Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #104 (NQF 0390): Prostate Cancer: Adjuvant Hormonal Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL
Measure #104 (NQF 0390): Prostate Cancer: Adjuvant Hormonal Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL
High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November D. Maruzzi - L. Ruggera
 High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November 2014 D. Maruzzi - L. Ruggera HIFU development Second prototype 1995-2000 Integrated Imaging 2006-2010 1993
High Intensity Focused Ultrasounds for the treatment of Prostate Cancers Clinical update November 2014 D. Maruzzi - L. Ruggera HIFU development Second prototype 1995-2000 Integrated Imaging 2006-2010 1993
PET imaging of cancer metabolism is commonly performed with F18
 PCRI Insights, August 2012, Vol. 15: No. 3 Carbon-11-Acetate PET/CT Imaging in Prostate Cancer Fabio Almeida, M.D. Medical Director, Arizona Molecular Imaging Center - Phoenix PET imaging of cancer metabolism
PCRI Insights, August 2012, Vol. 15: No. 3 Carbon-11-Acetate PET/CT Imaging in Prostate Cancer Fabio Almeida, M.D. Medical Director, Arizona Molecular Imaging Center - Phoenix PET imaging of cancer metabolism
Introduction. Original Article
 bs_bs_banner International Journal of Urology (2015) 22, 363 367 doi: 10.1111/iju.12704 Original Article Prostate-specific antigen level, stage or Gleason score: Which is best for predicting outcomes after
bs_bs_banner International Journal of Urology (2015) 22, 363 367 doi: 10.1111/iju.12704 Original Article Prostate-specific antigen level, stage or Gleason score: Which is best for predicting outcomes after
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
Section: Therapy Effective Date: October 15, 2016 Subsection: Therapy Original Policy Date: December 7, 2011 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
Last Review Status/Date: September 2016 Page: 1 of 10 Description High-dose rate (HDR) temporary prostate brachytherapy is a technique of delivering a high-intensity radiation source directly to the prostate
PSA Screening and Prostate Cancer. Rishi Modh, MD
 PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
One stop shop. Natalie D. Klass, MD
 One stop shop Natalie D. Klass, MD AERO Academy Conference Innovation & Safety Lisbon 26th and 27th January 2018 Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The views
One stop shop Natalie D. Klass, MD AERO Academy Conference Innovation & Safety Lisbon 26th and 27th January 2018 Disclosure & Disclaimer An honorarium is provided by Accuray for this presentation The views
Oligometastatic Disease
 Oligometastatic Disease Fact or Fantasy? Jennifer R Bellon MD, FASTRO Dana-Farber Cancer Institute Harvard Medical School Alexander V Louie MD PhD, FRCPC London Health Sciences Center Western University
Oligometastatic Disease Fact or Fantasy? Jennifer R Bellon MD, FASTRO Dana-Farber Cancer Institute Harvard Medical School Alexander V Louie MD PhD, FRCPC London Health Sciences Center Western University
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE
 CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
Perspectives on oligometastasis: challenges and opportunities
 Editorial Perspectives on oligometastasis: challenges and opportunities Jana Heitmann, Matthias Guckenberger Department of Radiation Oncology, University Hospital Zürich, Zürich, Switzerland Correspondence
Editorial Perspectives on oligometastasis: challenges and opportunities Jana Heitmann, Matthias Guckenberger Department of Radiation Oncology, University Hospital Zürich, Zürich, Switzerland Correspondence
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update
 BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Table of Contents Data Supplement 1: Additional Evidence Table(s) Table
BRACHYTHERAPY FOR PATIENTS WITH PROSTATE CANCER: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update Table of Contents Data Supplement 1: Additional Evidence Table(s) Table
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male