9/17/2013. Presentation Outline. Overview
|
|
|
- Robyn Wade
- 6 years ago
- Views:
Transcription




1 FCDS 2013 Educational Webcast Series September 19, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff Presentation Outline Overview of Lung Cancer Signs, Symptoms and Risk Factors Anatomy of the Lungs Histologic Types of Lung Cancer New Lung Cancer Screening Recommendations Multiple Primary and Histology Coding Rules Refresher Collaborative Stage Data Collection System (CSv02.04) C.S. Site Specific Factors NCCN/ASCO Treatment Guidelines by Stage Text Documentation 2 Overview 3 1


2 Definition of Lung Cancer *Lung cancer or bronchogenic cancer is defined as a malignant tumor of the lung arising within the wall or epithelium of the bronchus 4 Incidence and Mortality Lung Cancer 5 Incidence and Mortality Lung Cancer Estimated Number* of New Cancer Cases and Deaths by Sex US & FL ,190 new lung cancers 159,480 lung cancers deaths 118,080 new Male lung cancer 87,260 Male lung cancer deaths 110,110 new Female lung cancer 72,220 Female lung cancer deaths 17,960 FL new cases lung cancer 12,070 FL lung cancers deaths *ACS Cancer Facts & Figures



3 * * Lung Cancer Kills More People Than 3

4 * Lung Cancer Survival by Stage 11 Lung Cancer Survival by Stage *The 5-year survival for small cell lung cancer (6%) is lower than that for non-small cell (18%). *5-year survival rate for all stages combined is only 16%. *Only 15% of lung cancers are diagnosed at a localized stage, for which the 5-year survival rate is 52%. *1-year relative survival for lung cancer increased from 37% in to 44% in , largely due to improvements in surgical techniques and combined therapies. Cancer Facts & Figures



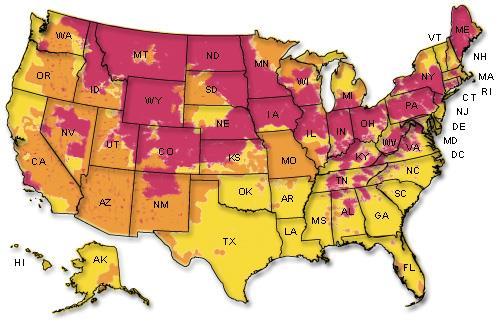
5 Geographic Patterns in Lung Cancer Death Rates* by State, US, : Males Cancer Facts & Figures 2013, *Age adjusted to the 2000 US standard population. Source: US Mortality Data, National Center for Health Statistics, Centers for Disease Control and Prevention. American Cancer Society, Surveillance Research, Geographic Patterns in Lung Cancer Death Rates* by State, US, : Females Cancer Facts & Figures 2013, *Age adjusted to the 2000 US standard population. Source: US Mortality Data, National Center for Health Statistics, Centers for Disease Control and Prevention. American Cancer Society, Surveillance Research, Appalachia and Major U.S. Rivers Poverty Rates in Appalachia, Mississippi River, Ohio River, Missouri River


 *Sputum with")

6 U.S. Adult Smoking Rates Adult Smoking Rates 16 Signs and Symptoms Symptoms may include persistent cough, sputum streaked with blood, shortness of breath, wheezing, chest pain, voice change, and recurrent pneumonia or bronchitis, hoarseness, pain when swallowing, high pitched sound when breathing. 17 Signs and Symptoms *Persistent cough *Unexplained dyspnea (SOB) *Sputum with blood (Hemoptysis) *Excessive sputum production *Weight loss & fatigue & anorexia *Hoarseness or change in voice *Shoulder or other joint pain *Chest, back or arm pain *Recurring episodes of pleural effusion, pneumonia or bronchitis 18 6





7 Signs and Symptoms 19 Risk Factors *Cigarette smoking *Other tobacco smoking *Passive smoking - 2 nd hand smoke *Occupational carcinogens * Asbestos exposure *Residential carcinogens * Radon exposure *Having had certain other cancers *Family member with lung cancer *Having had other lung disease *TB, bronchitis & emphysema *Nutritional deficiencies *Air pollution *Viruses 20 *Smoking main contributor *Cigarette smoke contains over 69 known carcinogens *Radioisotopes *Nitrosamine *Benzene *Acetone *Cadmium Tobacco Use



8 Tobacco Use 22 Radon Gas 23 Radon Gas







9 Asbestos Asbestos and lung cancer Asbestos and mesothelioma 25 High levels of air pollution Drinking water containing high levels of arsenic Air and Water Pollution 26 Viruses Implicated viruses include Human Papilloma Virus (HPV), Simian Virus (SV40), cytomegalovirus (CMV). These viruses may effect the cell cycle allowing uncontrolled cell division

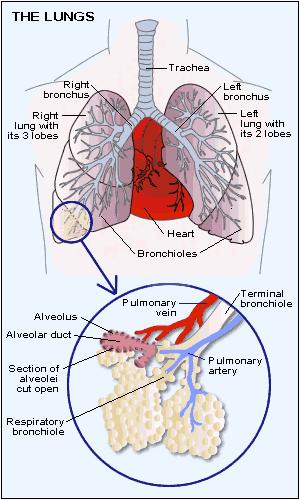
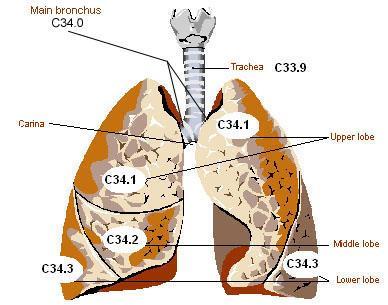

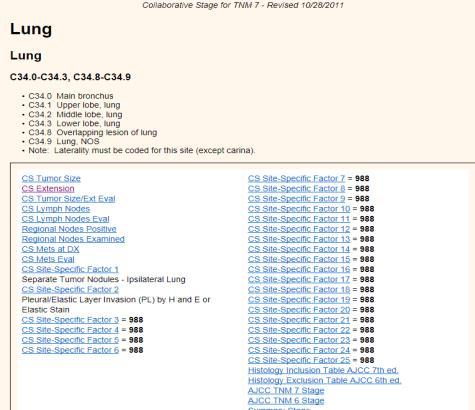
10 28 Lung Anatomy Lung Anatomy * C34.0 Main bronchus * C34.1 Upper lobe, lung * C34.2 Middle lobe, lung (right lung only) * C34.3 Lower lobe, lung * C34.8 Overlapping lesion * C34.9 Lung, NOS * Source: SEER Training: ICD-O-3 Site Codes 30 10



11 Lung Anatomy The hilum is the space in each lung where the bronchus and blood vessels enter the lung. The apex is the rounded area at the top of each lung. 31 Lung Anatomy The lingula, found only in the left lung, is a projection of the upper lobe of the left lung thought to be a remnant of an ancient middle lobe of the left lung. 32 Lung Anatomy Great Vessels Source: Springer Images. Figure adapted from Atlas of Human Anatomy, 2 nd ed. Contents of the superior and middle mediastinum

12 Lung Anatomy Laterality Code laterality for all lung sub-sites except carina Code the laterality for the lung in which the tumor originated Count cancer in both lungs as separate primaries unless metastasis from one side to the other is documented Always check that multiple pulmonary nodules are not metastasis from another primary site If both lungs have nodules or tumors and the lung of origin is not known, assign code 4. Diffuse bilateral lung nodules is the only time when laterality = 4 Always check that multiple pulmonary nodules are not metastasis from another primary site 34 Lung Anatomy Regional Lymph Nodes * NX Regional lymph nodes cannot be assessed * N0 No regional lymph node metastases * N1 Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes, including involvement by direct extension * N2 Metastasis in ipsilateral mediastinal and/or subcarinal lymph node(s) * N3 Metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s) 35 Lung Anatomy Regional Lymph Nodes N1 is defined as metastasis in ipsilateral peribronchial (left side of diagram) and/or ipsilateral hilar lymph nodes (right side of diagram) and intrapulmonary nodes, including involvement by direct extension of the primary tumor
 (right side of diagram).")
, whereas M1b is defined as distant metastasis (in")
 in a contralateral lobe; tumor with pleural")
13 Lung Anatomy Regional Lymph Nodes N2 is defined as metastasis in ipsilateral mediastinal (left side of diagram) and/or subcarinal lymph node(s) (right side of diagram). 37 Lung Anatomy Regional Lymph Nodes N3 is defined as metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s), whereas M1b is defined as distant metastasis (in extrathoracic organs), and this would include distant lymph nodes. 38 Lung Anatomy Pleural Effusion M1a is defined as separate tumor nodule(s) in a contralateral lobe; tumor with pleural nodules or malignant pleural (or pericardial) effusion. This is an image of tumor with malignant pleural effusion.lymph nodes



14 Lung Anatomy Layers of the Pleura Parietal pleura Visceral pleura Elastic Layer of pleura Visceral pleura Visceral pleura A tumor that falls short of completely traversing the elastic layer of the visceral pleura is defined as PL0. A tumor that extends through the elastic layer is defined as PL1 and one that extends to the surface of the visceral pleural as PL2. Extension of the tumor to the parietal pleura is defined as PL3. 40 Lung Anatomy Metastatic Sites Types of Lung Cancer
 Non-Small Cell Lung Cancer (NSCLC) Large Cell Carcinoma Large Cell Neuroendocrine Carcinoma Squamous Cell Carcinoma Adenocarcinoma")
15 Lung Cancer Type *World Health Organization (WHO) divides lung cancer into two major classes based on histology, therapy and prognosis. *The main classes of lung cancer are: Small Cell Lung Cancer (SCLC) Non-Small Cell Lung Cancer (NSCLC) Large Cell Carcinoma Large Cell Neuroendocrine Carcinoma Squamous Cell Carcinoma Adenocarcinoma Bronchoalveolar Carcinoma 43 Lung Cancer Type 44 Lung Cancer Type Wahbah M, et al. Ann Diagn Pathol. 2007; 110:
 *A type of lung cancer made up of small, round cells.")
 when viewed under a")
 Non-small cell lung cancer is divided into 3 subcategories Large cell carcinomas make up")

16 Lung Cancer Type Kenfield SA, Wei EK, Stampfer MJ, Rosner BA, Colditz GA (2008), Tobacco Control 17 (3): Small Cell Lung Carcinoma (SCLC) *A type of lung cancer made up of small, round cells. *Small cell lung cancer is less common than nonsmall cell lung cancer *Often grows more quickly *The name is often shortened to SCLC. Another name for SCLC is oat cell cancer because the cancer cells may look like oats (Flat shape) when viewed under a microscope, grows rapidly and quickly spreads to other organs 47 Source: webmd.com Non-Small Cell Lung Carcinoma (NSCLC) Non-small cell lung cancer is divided into 3 subcategories Large cell carcinomas make up a group of cancers that look large and abnormal under a microscope. * Non-Small Cell Lung Cancer is the most common type of Lung Cancer * Is usually grows and spreads more slowly than small cell lung cancer Squamous cell carcinoma originates in the thin, flat cells that line the passages of the respiratory tract. Adenocarcinoma begins in the cells that form the lining of the lungs
--usually slow-growing, but can metastasize widely; usually a peripheral lesion.")
--also called giant cell or clear cell. * Other subtypes of adenocarcinoma are acinar, papillary, and mucinous.")
. * Melanomas, sarcomas and lymphomas may also arise in the lung.")
17 Non-Small Cell Lung Carcinoma * Squamous or epidermoid (807_3)-- least likely to recur after resection; frequently a central or bronchial lesion. * Adenocarcinoma (814_3)--usually slow-growing, but can metastasize widely; usually a peripheral lesion. * Bronchioloalveolar (82503)--a very specific subtype adenocarcinoma with a distinct characteristic presentation and behavior. These tumors arise in the alveolar sacs in the lungs. * Large cell carcinoma (80123)--also called giant cell or clear cell. * Other subtypes of adenocarcinoma are acinar, papillary, and mucinous. * Adenosquamous carcinoma (85603)-- a specific histologic variant containing both epithelial (squamous and glandular (adeno-) cells (NSCLC) * Carcinoids (824_3)--arise from neuroectoderm (which generates supporting structures of lung). * Melanomas, sarcomas and lymphomas may also arise in the lung. * Mesothelioma (905_3)--linked to asbestos exposure; usually involves the pleura, not the lung. * Non-small cell carcinoma (80463)--a general term used sloppily to separate small cell from the "nonsmall cell" types (such as adenocarcinoma, Squamous cell carcinoma, large cell, etc.). * Only use 8046/3 when there is no other type of non-small cell carcinoma contained in the source documents. Source: FCDS Monthly Memo Nov Large Cell Carcinoma Often grows to large tumor Growth rate: rapid growth Incidence: 15% More often peripheral mass; either single or multiple masses; may be central Named for the large, round cells seen in this cancer Grow quickly and spread so usually are diagnosed in later stage Source: 50 Squamous Cell Carcinoma Arises from bronchial epithelium (i.e. major bronchi), confined to bronchial wall with no lymph node metastases As growth occurs, cavitation may develop in lung distal to tumor. Tumor may occur in apex & upper respiratory zone Growth rate: slow growth Five year survival is 90% or more if no 2 nd SCC present Sources: Adam and Medline Plus 51 17


18 Adenocarcinoma 52 Adenocarcinoma Majority Arises from terminal bronchioles Tend to be located in the periphery of the lung Cancer that begins in the cells that line the alveoli and make substances such as mucous. 80% contain mucin A slow growing cancer that can take years to develop into invasive cancer Most common subtype in nonsmokers In US, 50% of lung carcinomas in women are adenocarcinoma Incidence: >40% Clinical features May be associated with scarring Grows slower than SCC 5 year survival: Stage I - 69% Stage II - 40% Stage IIIA - 17% Stage IIIB - 5% Stage IV - 8% 53 Gross description Poorly circumscribed grayyellow lesions, single or multiple, may be mucoid 77% involve visceral pleura producing puckering/pleural retraction, 65% are peripheral Usually not cavitary Often associated with a peripheral scar or honeycombing (scar appears to be response to tumor) Rarely spreads into pleural space to coat visceral and parietal pleura and resemble diffuse mesothelioma Adenocarcinoma This is a peripheral adenocarcinoma of the lung
 <3cm nodule with <5mm invasion These neoplasms have a better prognosis than other lung")



19 Bronchoalveolar Adenocarcinoma Travis Classification Adenocarcinoma in situ (AIS) (formerly Bronchioalveolar Carcinoma - BAC) which is a pre-invasive lesion Minimally invasive adenocarcinoma (MIA) <3cm nodule with <5mm invasion These neoplasms have a better prognosis than other lung cancers. Composed of columnar cells that proliferate along the framework of alveolar septae, a so-called "lepidic" growth pattern. The cells are well-differentiated 55 This is another type of adenocarcinoma of lung known as adenocarcinoma-insitu (formerly called bronchoalveolar adenocarcinoma) Bronchoalveolar Adenocarcinoma Under the microscope, an image such as that on the left shows thickened walls of the gas-exchanging sacs in the lungs called alveoli. The classic description of this pattern is lepidic, meaning scale-like. X-rays and other imaging shows a picture that looks remarkably like pneumonia, as shown on the right. Patients with BAC are routinely diagnosed as having pneumonia for weeks or months before a diagnosis of cancer is actually established. 56 Lung Cancer Histology Groups
 Results *Screening with low-dose spiral CT compared to CXR reduced lung cancer deaths among older heavy smokers by 20%.")
20 Lung Cancer Screening Low Dose Helical CT (LDCT or also known as spiral CT) 58 *August National Lung Screening Trial (NLST) Results *Screening with low-dose spiral CT compared to CXR reduced lung cancer deaths among older heavy smokers by 20%. *Improved detection of lung cancer at early stage is key to increased survival and improved mortality. *Weigh Benefits/Risk of lung cancer screening using CT scan *Recommend Screening in High Risk Population: *Current/Former Smoker *Age Years Lung Cancer Screening *Smoking History of at least pack-years (varies by organization) *No personal history of lung cancer *Frequency of Screening - Annual 59 Lung Cancer Screening *Endorsement/Adoption of Guideline *American Cancer Society (ACS) *American Lung Association (ALA) *American College of Chest Physicians (ACCP) *American Association for Thoracic Surgery (AATS) *ASCO/NCCN Clinical Practice Guidelines (ASCO/NCCN) *United States Preventative Services Task Force 60 20
 * That not all lung cancers will be detected through use of low dose CT scanning *ALA issued a Call to")

21 Lung Cancer Screening *ALA Developing an Educational Portfolio for Patients to Explain: * The difference between a screening process and a diagnostic test * Cancer Screening is testing for cancer before there are any symptoms * The benefits, risks and costs (emotional, physical and economic) * That not all lung cancers will be detected through use of low dose CT scanning *ALA issued a Call to Action for Hospitals and Screening Centers to: * Establish ethical policies for advertising /promoting lung cancer screening svcs * Develop educational materials to assist patients in having thoughtful discussions between patients and physicians regarding lung cancer screening * Provide lung cancer screening services with access to multidisciplinary teams that can deliver the needed follow-up for evaluation of nodules. 61 Lung Workup





22 Lung Workup 64 Lung Cancer Workup Chest X-ray vs. CT 65 Lung Cancer Workup * Bronchosopy Mediastinoscopy If a mediastinal mass or mediastinal adenopathy is reported on x-ray or mediastinoscopy, assume that mediastinal lymph nodes are involved




23 Lung Cancer Workup Endoscopic ultrasound (EUS) CT-Guided Needle Aspiration Biopsy Illustration Lung Cancer Workup Thoracentesis Thoracotomy 68 Lung Cancer Workup Biomarkers *Data show that targeted therapy is potentially very effective in patients with specific gene mutations or rearrangements. *Several biomarkers have emerged as prognostic (patient survival) and predictive (therapeutic efficacy) for NSCLC
24 Lung Cancer Workup Biomarkers *EGFR * Epidermal Growth Factor Receptor *ERCC1 * Endonuclease of the nucleotide excision repair complex *K-ras oncogene *RRM1 * Regulatory subunit of ribonucleotide reductase *EML4-ALK Fusion Oncogene 70 TTF-1 is very important in distinguishing primary from metastatic adenocarcinoma. Most primary lung adenocarcinomas are TTF-1 positive. Squamous cell lung carcinomas are often TTF-1 negative Other squamous cell IHC tests - p63 positive and cytokeratin positive Other adenocarcinoma IHC tests - CEA, B72.3, BER-EP4, and MOC3. These stains are negative for mesothelioma. Thyroglobulin is present in tumors from patients with thyroid cancer, but it is negative in lung cancer tumors. Pulmonary adenocarcinoma is usually CK7+ and CK20-, whereas metastatic adenocarcinoma of the colorectum is usually CK7- and CK20+. NCCN Guidelines Lung Cancer Workup Immunohistochemical Stains (IHC) 71 Lung Cancer Workup Small Cell Lung CA Biomarkers *Nearly all SCLCs are immunoreactive for keratin, epithelial membrane antigen, and thyroid transcription factor-1 (TTF-1). *Most SCLCs also stain positive for markers of neuroendocrine differentiation, including chromogranin A, neuron-specific enolase, neural cell adhesion molecule (NCAM; CD56) and synaptophysin. *However, these markers alone cannot distinguish SCLC from NSCLC because approximately 10% of NSCLC will be immunoreactive for at least one of these neuroendocrine markers

25 Lung MPH Rules Terms and Definitions
26 76 Lung MPH Rules Multiple Primary Rules
27
28 Lung MPH Rules Histology Coding Rules


29 Lung Cancer Histology Groups

30 Nair A et al. Radiographics 2011;31:

.")
.")
31 91 CS and TNM T1a T1b 2CM T1a >2-3CM T1 is defined as a tumor 3 cm or less in greatest dimension, surrounded by lung or visceral pleura, without bronchoscopic evidence of invasion more proximal than the lobar bronchus (i.e., not in the main bronchus). T1a is defined as a tumor 2 cm or less in greatest dimension (upper left). T1a is also defined as a superficial spreading tumor of any size with its invasive component limited to the bronchial wall, which may extend proximally to the main bronchus (lower left). T1b is defined as a tumor more than 2 cm but 3 cm or less in greatest dimension (right). 92 CS and TNM 93 31


32 CS Ext Code 100 vs 300 *Can you please clarify the difference between the two codes. For example, you are staging a case based on x-ray findings and the MD states there is a mass in RUL. He gives no further information on extension. I would think code 100 would apply. If so, when would be the proper time to use code 300? *Code 100 is generally used when there is a tumor size and the lesion/mass is clearly confined to the lung. Code 300 would be used when you have limited information, such as this case. Do you have a size from the x-ray or any other type of report? *If you can find a size, then you could use 100 with that size. Based on the information you have given, you would not get a T value on this case unless you can find a tumor size. *Code 300 would also be used if the only information you had was "tumor confined to lung." 94 CS and TNM 95 CS and TNM T2a T2a >3-5CM >3-5CM T2a T2a T2a T2a 5CM 5CM 2CM >2CM 2CM T2b >5-7CM Atelectasis or obstructive pneumonia 5CM 5CM T2a T2a T2b T2b >5-7CM 96 32

33 Atelectasis Due to Pleural Effusion *15mm mass in left lung apex highly suspicious for malignancy. *There is massive left sided pleural effusion with atelectasis and collapse of the left lung. *Would I use code 550 for CS Ext if atelectasis is caused by pleural effusion and the pleural effusion is malignant? *Extension code 550 is the appropriate code, based on the atelectasis and the collapse of the left lung *The pleural effusion, now coded in CS Mets at DX, would be code 15 since malignant pleural effusion is on the same side as the primary malignancy. 97 CS and TNM Atelectasis *The collapse or closure of the lung resulting in reduced or absent gas exchange (not same as pneumothorax) *May affect part or all of one lung *May be acute or chronic *Respiratory distress Bronchopneumonia *Acute inflammation of the walls of the bronchioles *Characterized by multiple foci of isolated, acute consolidation in one or more pulmonary lobules *Consolidation is the swelling (edema or inflammatory exudate) or hardening of the lung tissue 98 CS and TNM 99 33


34 Layers of the Pleura Parietal pleura Visceral pleura Elastic Layer of pleura Visceral pleura Visceral pleura A tumor that falls short of completely traversing the elastic layer of the visceral pleura is defined as PL0. A tumor that extends through the elastic layer is defined as PL1 and one that extends to the surface of the visceral pleural as PL2. Extension of the tumor to the parietal pleura is defined as PL Pleural and Pericardial Effusion 101 CS and TNM T3 includes separate tumor nodule(s) in the same lobe. T4 includes separate tumor nodule(s) in a different ipsilateral lobe

, vertebral body (lower left), carina (middle left and")

35 CS and TNM 103 CS and TNM T4 is defined as tumor of any size that invades any of the following: mediastinum, heart, great vessels (upper right), trachea (upper left), recurrent laryngeal nerve, esophagus (lower right), vertebral body (lower left), carina (middle left and right), separate tumor nodule(s) in a different ipsilateral lobe 104 CS and TNM T4 includes tumor invasion of the superior vena cava and heart



36 CS and TNM T4 includes tumor invasion of the aorta, esophagus, and vertebral body. 106 CS TS/Ext Eval 107 CS Lymph Nodes
 * N3 Metastasis in contralateral mediastinal,")
 * Intrapulmonary Lymph node(s) * Peribronchial Lymph node(s) * N2 Same side * Mediastinal Lymph node(s) *")
37 CS Lymph Nodes REGIONAL LYMPH NODES * NX Regional lymph nodes cannot be assessed * N0 No regional lymph node metastases * N1 Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes, including involvement by direct extension * N2 Metastasis in ipsilateral mediastinal and/or subcarinal lymph node(s) * N3 Metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph node(s) 109 N3 N1 N2 N2 CS Lymph Nodes REGIONAL LYMPH NODES N3 N3 * NX Regional lymph nodes cannot be assessed * N0 No regional lymph node metastases * N1 Same side * Direct Extension * HilarLymph node(s) * Intrapulmonary Lymph node(s) * Peribronchial Lymph node(s) * N2 Same side * Mediastinal Lymph node(s) * Subcarinal Lymph node(s) * N3 Contralateral * Hilar Lymph node(s) * Mediastinal Lymph node(s) * Any scalene Lymph node(s) * Any supraclavicular lymph node(s)



38 112 Layers of the Pleura Parietal pleura Visceral pleura Elastic Layer of pleura Visceral pleura Visceral pleura A tumor that falls short of completely traversing the elastic layer of the visceral pleura is defined as PL0. A tumor that extends through the elastic layer is defined as PL1 and one that extends to the surface of the visceral pleural as PL2. Extension of the tumor to the parietal pleura is defined as PL Treatment Options

39 115 Small Cell Lung Cancer LIMITED STAGE EXTENSIVE STAGE Any T Any N M0 Confined to Chest Exception: T3-4 due to multiple lung nodules that do not fit in a tolerable radiation field 116 Any T Any N M1a M1b Includes: T3-4 due to multiple lung nodules or tumor/nodal volume too large to be encompassed in a tolerable radiation plan Small Cell Lung Cancer LIMITED STAGE * Combination chemotherapy and radiation therapy to the chest. * Combination chemotherapy for patients with lung problems or who are very ill. * Surgery followed by chemotherapy or chemotherapy plus radiation therapy to the chest. * Clinical trials of new chemotherapy, surgery, and radiation treatments EXTENSIVE STAGE * Combination chemotherapy. * Radiation therapy to the brain, spine, bone, or other parts of the body where the cancer has spread, as palliative therapy to relieve symptoms and improve quality of life. * Clinical trials of new chemotherapy treatments
. A clinical trial of chemotherapy or radiation therapy following surgery.")
40 118 Lung Treatment Options by Stage Stage I Non-Small Cell Lung Cancer Surgery (wedge resection, segmental resection, sleeve resection, or lobectomy). External radiation therapy (for patients who cannot have surgery or choose not to have surgery). A clinical trial of chemotherapy or radiation therapy following surgery. A clinical trial of surgery followed by chemoprevention. A clinical trial of treatment given through an endoscope, such as photodynamic therapy (PDT). 119 Lung Treatment Options by Stage Stage II Non-Small Cell Lung Cancer Surgery (wedge resection, segmental resection, sleeve resection, lobectomy, or pneumonectomy). Chemotherapy followed by surgery. Surgery followed by chemotherapy. External radiation therapy (for patients who cannot have surgery or choose not to have surgery). A clinical trial of radiation therapy following surgery
41 Non-Small Cell Lung Cancer Source: National Cancer Institute Cancer Topics NSCLC Stage (TNM Staging Criteria) Standard Treatment Options Occult NSCLC Stage 0 NSCLC Surgery Surgery Endobronchial therapies Stage I NSCLC Surgery Radiation therapy Stage II NSCLC Surgery Neoadjuvant chemotherapy Adjuvant chemotherapy Radiation therapy 121 Lung Treatment Options by Stage: Stage IIIA Non-Small Cell Lung Cancer Surgery followed by chemotherapy. Chemotherapy followed by surgery. Surgery followed by chemotherapy combined with radiation therapy. Surgery followed by radiation therapy. A clinical trial of new combinations of treatments 122 Lung Treatment Options by Stage Cancer Cannot be Removed w/ Surgery Chemotherapy and radiation therapy given as separate treatments over the same period of time. External radiation therapy alone (for patients who cannot be treated with combined therapy, as palliative treatment to relieve symptoms / improve quality of life). Internal radiation therapy or laser surgery, as palliative treatment to relieve symptoms and improve the quality of life. A clinical trial of new combinations of treatments

42 Non-Small Cell Lung Cancer Source: National Cancer Institute Cancer Topics NSCLC Stage (TNM Staging Criteria) Standard Treatment Options Stage IIIA NSCLC Resected or resectable disease Unresectable disease Superior sulcus tumors Chest wall tumors Surgery Neoadjuvant therapy Adjuvant therapy Radiation therapy Chemoradiation therapy Radiation therapy alone Radiation therapy and surgery Concurrent chemotherapy with radiation therapy and surgery Surgery alone (for selected patients) Surgery Surgery and radiation therapy Chemotherapy combined with radiation therapy and/or surgery 124 Stage IIIB NSCLC Stage IV NSCLC Non-Small Cell Lung Cancer Source: National Cancer Institute Cancer Topics NSCLC Stage (TNM Staging Criteria) Standard Treatment Options Sequential or concurrent chemotherapy and radiation therapy Chemotherapy followed by surgery (for selected patients) 125 Radiation therapy alone Combination chemotherapy Combination chemotherapy with bevacizumab or cetuximab Epidermal growth factor receptor tyrosine kinase inhibitors (for patients with EGFR mutations) Maintenance therapy following first-line chemotherapy External-beam radiation therapy (for palliation) Endobronchial laser therapy and/or brachytherapy (for obstructing lesions) Coding Lung Cancer Surgery


43 Surgical Removal Surgical Removal Wedge or Segmental Resection Removal of one or more lung segment Lobectomy Removal of entire lobe of the lung Pneumonectomy Removal of entire lung Note: If a lobectomy was performed, assume that the tumor was more than 2 cm distal to the carina. 128 Surgery Codes DAM Appendix F
 include date(s)")
] Location include facility/physician/other location where the event occurred (test/study/treatment/other) Abbreviated text Be brief but complete use abbreviations correctly.")
44 Surgery Codes DAM Appendix F 130 Text Documentation OMG Avoid non-standard text Keep it simple No repetition Justify coded items FCDS DAM Appendix L DEFENSIVE ABSTRACTING CYA-Cover your abstract Support ALL codes and dates with text - primary site, histology, staging workup, tumor size, nodal status, stage of disease, first course of RX 131 Text Documentation Date(s) include date(s) references this allows the reviewer to determine event chronology Date(s) note when date(s) are estimated [i.e. Date of DX 3/15/2011 (est.)] Location include facility/physician/other location where the event occurred (test/study/treatment/other) Abbreviated text Be brief but complete use abbreviations correctly. Text fields If information is missing from the record, state that it is missing type not available (NA) Edit your text documentation DO NOT REPEAT INFORMATION from section to section Operative text - DO not enter the pathology info in the Op TEXT Ex 8/26/12 ABC Facility Liver biopsy this should be part of pathology Pathology text - Example 8/26/12 ABC facility Liver biopsy metastatic adenocarcinoma
 133 Questions http://media.mlive.")
45 References * National Cancer Institute * FCDS Data Acquisition Manual * American Society of Clinical Oncology * American Society for Radiation Oncology * 2013 Cancer Facts and Figures, American Cancer Society *Collaborative Stage Data Collection System *2007 MPH Rules for Solid Tumors *National Lung Screening Trial (NLST) 133 Questions
FCDS 2013 Educational Webcast Series September 19, Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff
 FCDS 2013 Educational Webcast Series September 19, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff Presentation Outline Overview of Lung Cancer Signs, Symptoms and Risk Factors Anatomy
FCDS 2013 Educational Webcast Series September 19, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff Presentation Outline Overview of Lung Cancer Signs, Symptoms and Risk Factors Anatomy
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
Lung 8/7/14. Collecting Cancer Data: Lung NAACCR Webinar Series. August 7, 2014
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Lung /1/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
Lung Cancer: Diagnosis, Staging and Treatment
 PATIENT EDUCATION patienteducation.osumc.edu Lung Cancer: Diagnosis, Staging and Treatment Cancer starts in your cells. Cells are the building blocks of your tissues. Tissues make up the organs of your
PATIENT EDUCATION patienteducation.osumc.edu Lung Cancer: Diagnosis, Staging and Treatment Cancer starts in your cells. Cells are the building blocks of your tissues. Tissues make up the organs of your
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
The 8th Edition Lung Cancer Stage Classification
 The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Lung tumors & pleural lesions
 Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
NAACCR Webinar Series 1
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL
 LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק
 Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Non Small Cell Lung Cancer Histopathology ד"ר יהודית זנדבנק 26.06.09 Lecture outlines WHO histological classification Macro/Micro assessment Early diagnosis Minimal pathology Main subtypes SCC, AdCa, LCLC
Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Cancer in the United States, 2004
 Cancer in the United States, 2004 Five-year Cancer Survival Rates (%) US 1974-1998 100 90 80 70 60 50 40 30 20 10 0 1974-1976 1983-1985 1992-1998 Prostate Lung Colon Breast Source: CA Cancer J Clin 2000;50:7-33
Cancer in the United States, 2004 Five-year Cancer Survival Rates (%) US 1974-1998 100 90 80 70 60 50 40 30 20 10 0 1974-1976 1983-1985 1992-1998 Prostate Lung Colon Breast Source: CA Cancer J Clin 2000;50:7-33
Lung /4/18. Please submit all questions concerning the webinar content through the Q&A panel.
 Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Definition. Epidemiology. Lung Cancer is a disease which cancer (malignant tumors) cells grow in the lungs. LUNG CANCER Debra Mercer BSN, RN, RRT
 cells grow in the lungs. LUNG CANCER Debra Mercer BSN, RN, RRT") LUNG CANCER Debra Mercer BSN, RN, RRT Definition Lung Cancer is a disease which cancer (malignant tumors) cells grow in the lungs. Epidemiology Leading cancer killer in both men and women in the US - 169,
LUNG CANCER Debra Mercer BSN, RN, RRT Definition Lung Cancer is a disease which cancer (malignant tumors) cells grow in the lungs. Epidemiology Leading cancer killer in both men and women in the US - 169,
The Spectrum of Management of Pulmonary Ground Glass Nodules
 The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
The Spectrum of Management of Pulmonary Ground Glass Nodules Stanley S Siegelman CT Society 10/26/2011 No financial disclosures. Noguchi M et al. Cancer 75: 2844-2852, 1995. 236 surgically resected peripheral
8/22/2016. Major risk factors for the development of lung cancer are: Outline
 Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
Carcinomas of the Lung: Changes in Staging, Adenocarcinoma Classification and Genetics Grace Y. Lin, M.D., Ph.D. Outline Background Staging of Lung Cancer: Review of the 2010 7 th Edition of the AJCC Cancer
Lung cancer is a disease in which malignant (cancer) cells form in the tissues of the lung.
 cells form in the tissues of the lung.") Lung Cancer Lung cancer is a disease in which malignant (cancer) cells form in the tissues of the lung. The lungs are a pair of cone-shaped breathing organs in the chest. The lungs bring oxygen into the
Lung Cancer Lung cancer is a disease in which malignant (cancer) cells form in the tissues of the lung. The lungs are a pair of cone-shaped breathing organs in the chest. The lungs bring oxygen into the
Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors.
 Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors. o Classify bronchogenic carcinoma. o Discuss etiopathogenesis of bronchogenic ca. o Discuss morphological features of squamous
Pathology of Tumors of Lung Pathology of Tumors of Lung o Classify lung tumors. o Classify bronchogenic carcinoma. o Discuss etiopathogenesis of bronchogenic ca. o Discuss morphological features of squamous
LUNG CANCER. Agnieszka Słowik, MD. Department of Oncology, University Hospital in Cracow Jagiellonian University
 LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
YOUR LUNG CANCER PATHOLOGY REPORT
 UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
UNDERSTANDING SERIES YOUR LUNG CANCER PATHOLOGY REPORT 1-800-298-2436 LungCancerAlliance.org A GUIDE FOR THE PATIENT 1 CONTENTS What is a Pathology Report?...2 The Basics...3 Sections of a Pathology Report...6
Lung Cancer Risks. Cancer in the United States, Cancer Death Rates, US The Scheme: From Nicotine Addiction to Lung Cancer
 Cancer in the United States, 2004 Lung Cancer Risks Cigarette Smoking Environmental Tobacco Smoke Other Carcinogens Asbestos, Arsenic, Radon, Bis(chloromethyl) ether, Chromium, Foundry fumes, nickel, mustard
Cancer in the United States, 2004 Lung Cancer Risks Cigarette Smoking Environmental Tobacco Smoke Other Carcinogens Asbestos, Arsenic, Radon, Bis(chloromethyl) ether, Chromium, Foundry fumes, nickel, mustard
WHITE PAPER - SRS for Non Small Cell Lung Cancer
 WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Lung Cancer. This reference summary will help you better understand lung cancer and the treatment options that are available.
 Lung Cancer Introduction Lung cancer is the number one cancer killer of men and women. Over 165,000 people die of lung cancer every year in the United States. Most cases of lung cancer are related to cigarette
Lung Cancer Introduction Lung cancer is the number one cancer killer of men and women. Over 165,000 people die of lung cancer every year in the United States. Most cases of lung cancer are related to cigarette
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
The Respiratory System. Dr. Ali Ebneshahidi
 The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
The Respiratory System Dr. Ali Ebneshahidi Functions of The Respiratory System To allow gases from the environment to enter the bronchial tree through inspiration by expanding the thoracic volume. To allow
Surgical management of lung cancer
 Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
3/30/2009 Lung Cancer Deaths 2008 Lung Cancer Deaths Lung Cancer Deaths--Males Males 5
 LUNG CANCER 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Very common Very lethal Lung Cancer Median age of diagnosis approximately 70 years, but affects all ages(even pediatric!) Advances in
LUNG CANCER 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Very common Very lethal Lung Cancer Median age of diagnosis approximately 70 years, but affects all ages(even pediatric!) Advances in
Lung Cancer Incidence 2008 Lung Cancer Deaths-Males 2008 Incidence Total U.S.(all types): 1,437,180 Lung Cancer Deaths-Females Lung cancer 215,000(15%
: 1,437,180 Lung Cancer Deaths-Females Lung cancer 215,000(15%") Multidisciplinary approach 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Neurology Neurosurgery Orthopedic surgery General surgery Vascular surgery Gastroenterology Cardiology Lung Cancer Very
Multidisciplinary approach 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Neurology Neurosurgery Orthopedic surgery General surgery Vascular surgery Gastroenterology Cardiology Lung Cancer Very
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
WELLNESS INITIATIVE NOW
 WELLNESS INITIATIVE NOW To promote personal well-being, fitness and nutrition for all TDCJ employees. November 2008 Lung cancer is cancer that forms in tissues of the lung, usually in the cells lining
WELLNESS INITIATIVE NOW To promote personal well-being, fitness and nutrition for all TDCJ employees. November 2008 Lung cancer is cancer that forms in tissues of the lung, usually in the cells lining
Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer. Quick Reference Chart and Diagrams
 CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
Master Class: Fundamentals of Lung Cancer
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
6 th Reprint Handbook Pages AJCC 7 th Edition
 6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
Lung Cancer-a primer. Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo
 Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Small Cell Lung Cancer Early Detection, Diagnosis, and Staging
 Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
Guide to Understanding Lung Cancer
 Guide to Understanding Lung Cancer Lung cancer is the second most common cancer overall for men and women in the U.S., with an estimated 222,500 new cases in 2017. However, lung cancer is the most common
Guide to Understanding Lung Cancer Lung cancer is the second most common cancer overall for men and women in the U.S., with an estimated 222,500 new cases in 2017. However, lung cancer is the most common
Reparatory system 18 lectures Heyam Awad
 Reparatory system 18 lectures 8-10 Heyam Awad These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Reparatory system 18 lectures 8-10 Heyam Awad These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
What is lung cancer? Contents
 13 11 20 Information and support What is lung cancer? Contents About the lungs What is lung cancer? How common is it? Different types of lung cancer Causes Symptoms Information reviewed by About the lungs
13 11 20 Information and support What is lung cancer? Contents About the lungs What is lung cancer? How common is it? Different types of lung cancer Causes Symptoms Information reviewed by About the lungs
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Reparatory system lectures Heyam Awad
 Reparatory system lectures 8-10 Heyam Awad note These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Reparatory system lectures 8-10 Heyam Awad note These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Non small cell Lung Cancer
 Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
LungStage. Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies
 LungStage Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies Medical Team: Bram Stieltjes, MD PhD; Alex Sauter, MD; Gregor Sommer, MD;
LungStage Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies Medical Team: Bram Stieltjes, MD PhD; Alex Sauter, MD; Gregor Sommer, MD;
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer. Doug Rahn 6/1/12
 Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Mediastinal Mysteries: What can be solved with EBUS?
 Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the highest incidence
 LUNG CANCER 2010 Mark B. Stoopler, M.D. Division of Medical Oncology Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the
LUNG CANCER 2010 Mark B. Stoopler, M.D. Division of Medical Oncology Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the
Lung cancer forms in tissues of the lung, usually in the cells lining air passages.
 Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Lung Neoplasia II Resection specimens Pathobasic. Lukas Bubendorf Pathology
 Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Neoplasia II Resection specimens Pathobasic Lukas Bubendorf Pathology Agenda Preneoplastic lesions Histological subtypes of lung cancer Histological patterns of AC Cells of origin and characteristic
Lung Cancer and CT Screening
 Lung Cancer and CT Screening Samer Kanaan, MD February 17 th, 2012 Goals Understand the Societal impact of Lung Cancer Identify Risk Factors for Lung Cancer List Diagnostic Tests Available for Lung Cancer
Lung Cancer and CT Screening Samer Kanaan, MD February 17 th, 2012 Goals Understand the Societal impact of Lung Cancer Identify Risk Factors for Lung Cancer List Diagnostic Tests Available for Lung Cancer
Table 1 Major Classifications of Lung Cancer. Non Small Cell Lung Cancer Adenocarcinoma
 VIII LUNG CANCER Jeffrey Crawford, m.d. Definition and Classifications Bronchogenic carcinoma of the lung lung cancer comprises a group of malignant neoplasms that arise from bronchial epithelium. The
VIII LUNG CANCER Jeffrey Crawford, m.d. Definition and Classifications Bronchogenic carcinoma of the lung lung cancer comprises a group of malignant neoplasms that arise from bronchial epithelium. The
Lung cancer LUNG CANCER. Box 1 Clinical signs
 22 LUNG CANCER Lung cancer Bronchial carcinoma refers to two distinct clinical entities small cell and non-small cell carcinoma. Although these conditions have much in common, with broadly similar presenting
22 LUNG CANCER Lung cancer Bronchial carcinoma refers to two distinct clinical entities small cell and non-small cell carcinoma. Although these conditions have much in common, with broadly similar presenting
Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging
 Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Lung Cancer Staging: The Revised TNM Classification
 Norwegian Society of Thoracic Imaging Oslo, October 2011 Lung Cancer Staging: The Revised TNM Classification Sujal R Desai King s College Hospital, London Lung Cancer The Scale of the Problem Leading cause
Norwegian Society of Thoracic Imaging Oslo, October 2011 Lung Cancer Staging: The Revised TNM Classification Sujal R Desai King s College Hospital, London Lung Cancer The Scale of the Problem Leading cause
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Lung Cancer. Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD
 Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Lung Cancer Update. HARMESH R NAIK, MD. February 28, 2001
 Lung Cancer Update HARMESH R NAIK, MD. February 28, 2001 Progress update Prevention Screening Staging Treatment Epidemiology Estimated 169,500 new cases Estimated 157,400 deaths Second commonest cancer
Lung Cancer Update HARMESH R NAIK, MD. February 28, 2001 Progress update Prevention Screening Staging Treatment Epidemiology Estimated 169,500 new cases Estimated 157,400 deaths Second commonest cancer
I appreciate the courtesy of Kusumoto at NCC for this presentation. What is Early Lung Cancers. Early Lung Cancers. Early Lung Cancers 18/10/55
 I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
I appreciate the courtesy of Kusumoto at NCC for this presentation. Dr. What is Early Lung Cancers DEATH Early period in its lifetime Curative period in its lifetime Early Lung Cancers Early Lung Cancers
LUNG CANCER. pathology & molecular biology. Izidor Kern University Clinic Golnik, Slovenia
 LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
LUNG CANCER pathology & molecular biology Izidor Kern University Clinic Golnik, Slovenia 1 Pathology and epidemiology Small biopsy & cytology SCLC 14% NSCC NOS 4% 70% 60% 50% 63% 62% 61% 62% 59% 54% 51%
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Lung Cancer Resection
 Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Recurrent lung cancer icd 10
 Search... Recurrent lung cancer icd 10 1-10-2017 2018 ICD - 10 -CM Diagnosis unsp part of unsp bronchus or lung ; The 2018 edition of ICD - 10 -CM C34.90 became due to small cell lung cancer ; Free, official
Search... Recurrent lung cancer icd 10 1-10-2017 2018 ICD - 10 -CM Diagnosis unsp part of unsp bronchus or lung ; The 2018 edition of ICD - 10 -CM C34.90 became due to small cell lung cancer ; Free, official
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD. November 18, 2017
 Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Diagnosis and Staging of Non-Small Cell Lung Cancer Carlos Eduardo Oliveira Baleeiro, MD November 18, 2017 Disclosures I do not have a financial interest/arrangement or affiliation with one or more organizations
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Steering Committee. Waiting on photo. Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD.
 Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Steering Committee Paul A. Bunn, Jr., MD Kavita Garg, MD Kim Geisinger, MD Fred R. Hirsch, Gregory Riely, MD, PhD MD, PhD Waiting on photo Paul Van Schil, MD, PhD William D. Travis, MD Ming-Sound Tsao,
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Lung Carcinoid Tumor Early Detection, Diagnosis, and Staging
 Lung Carcinoid Tumor Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Lung Carcinoid Tumor Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Lung Cancer. Definition of lung cancer Malignancy arising from lung tissue
 Lung Cancer Definition of lung cancer Malignancy arising from lung tissue Epidemiology of lung cancer Commonest malignancy in western world Commonest cause of death in men and women in the UK Approximately
Lung Cancer Definition of lung cancer Malignancy arising from lung tissue Epidemiology of lung cancer Commonest malignancy in western world Commonest cause of death in men and women in the UK Approximately
Pulmonary Neoplasms & Chest Disorders Ahmed Mahmoud
 Pulmonary Neoplasms & Chest Disorders Ahmed Mahmoud Lung Ca ;Pathological types Adenocarcinoma More common in females Peripheral location Spread mainly by blood(brain..) Incidence is increasing (the most
Pulmonary Neoplasms & Chest Disorders Ahmed Mahmoud Lung Ca ;Pathological types Adenocarcinoma More common in females Peripheral location Spread mainly by blood(brain..) Incidence is increasing (the most