Clinical Prostate Cancer Imaging
|
|
|
- Morgan Fisher
- 6 years ago
- Views:
Transcription




1 Clinical Prostate Cancer Imaging Steven C. Eberhardt, MD Professor and Vice Chair of Clinical Operations Chief of Abdominal and Oncology Radiology UNM Health Sciences Center UNM Comprehensive Cancer Center
 Seminal vesicles joined at the")
2 The Prostate Gland Part of male sexual organs Size of a walnut Between bladder and penis Anterior to the rectum Surrounds the urethra Provides fluid for ejaculate (30%) Seminal vesicles joined at the base
3 Common Prostate Diseases Benign Prostatitis Infectious (antibiotics) Noninfectious (more common) Benign prostatic hypertrophy (BPH) 50% men > age 50 95% men > age 90 Significant morbidity Malignant Primary: adenocarcinoma (common acinar, 95%) Secondary: direct (bladder, urethra)
4 Uncommon Prostatic Malignancies ~5% Epithelial Adenocarcinoma variants Comedocarcinoma Mucinous carcinoma Adenoid cystic carcinoma Signet ring cell carcinoma Adenosquamous carcinoma Squamous cell Transitional cell Neuroendocrine (carcinoid, small cell) Nonepithelial Rhabdosarcoma Leiomyosarcoma Fibrosarcoma MFH Osteosarcoma Angiosarcoma Chondrosarcoma Carcinosarcoma Malignant phyllodes Lymphoma Leukemia PSS and PSPUMP (Prostatic stromal sarcoma and prostatic stromal proliferation of uncertain malignant potential)

 Source: American Cancer Society, http://www.")
5 Prostate Cancer in 2017 Most common malignancy in American men About 160,000 new cases per year Second leading cause of cancer death (26,700/ year) Source: American Cancer Society,
6 Cancer Death Rates*, for Men, US, Lung Stomach Colon and rectum Leukemia Liver


7 Prostate Cancer
8 Established Screening Methods PSA blood test (serum PSA) 0 to 4 ng/ml normal range 4 to 10 ng/ml slightly elevated 10 to 20 ng/ml moderately elevated Greater than 20 highly elevated Increases with age, BPH, prostatitis Digital rectal exam (DRE) Imaging NOT used for screening
9 PSA Controversy Goal of PSA Screening = reduce disease specific mortality PSA: low specificity, cannot discriminate between lethal and nonlethal cancers. Has led to over-diagnosis and over-treatment. Conflicting results from trials on mortality have not given a clear picture of PSAs utility as a screening test.
10 PSA Controversy March 2009 European (ERSPC): Showed PSA screening led to lower death rate from prostate cancer (but is also associated with a high risk of over-diagnosis). Incidence 8.2% in the PSA screening group: 20% less likely to die from prostate cancer. Incidence 4.8% in the control group. The absolute risk difference between the two groups was 0.71 deaths per 1,000 men. To prevent one death from prostate cancer, 1,410 men would need to be screened with PSA testing and 48 additional cases of prostate cancer would need to be treated.
11 PSA Controversy March 2009 European (ERSPC): Showed PSA screening led to lower death rate from prostate cancer (but is also associated with a high risk of over-diagnosis). Incidence 8.2% in the PSA screening group: 20% less likely to die from prostate cancer. Incidence 4.8% in the control group. The absolute risk difference between the two groups was 0.71 deaths per 1,000 men. To prevent one death from prostate cancer, 1,410 men would need to be screened with PSA testing and 48 additional cases of prostate cancer would need to be treated. USA (PLCO): Showed no evidence of reduced death rate from prostate cancer with annual PSA screening compared with usual medical care. 13 yrs of f/u: mortality rates from prostate cancer for intervention and control groups: 3.7 and 3.4 deaths per 10,000 person-years, no significant difference. Based on results: U.S. Preventive Service Task Force (USPSTF) advised against PSA screening in Nevertheless, experts continue to believe that not using PSA screening would result in the deaths of many men with curable prostate cancer. Many large, national urological associations (American Urological Association [AUA], Canadian Urological Association [CUA] and European Urological Association [EAU]) endorse benefit of PSA screening for men after age 45 to 50, recommend physician-patient discussions about screening on an individual basis.

12 USPSTF 2012
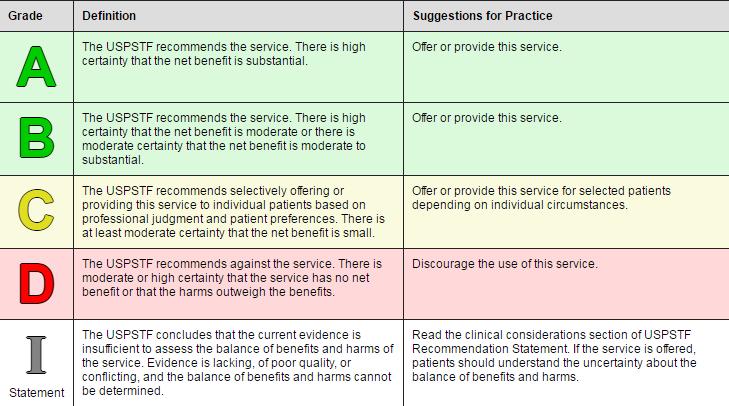
13 USPSTF



14
15 AUA Guidelines: Men < 40 yo: no screening 2. Men yo: no routine screening at average risk 3. Men yo: shared decision-making 4. An interval of two years or more may be preferred over annual screening. 5. Men 70 yo: no routine screening 6. Men with < y life expectancy: no routine screening

16 Comment period ended May 8, 2017 USPSTF 2017
)")
17 Needle biopsy Standard approach - image guidance using transrectal ultrasound usual for 1 st attempt at diagnosis Result: Normal or Cancer or Other (Inflammation or Prostatic intraepithelial neoplasia (PIN)) Diagnosis
18 Ultrasound For imaging Dx: as accurate as the DRE Biopsy tool Systematic biopsies US guided Directed to suspicious sites Local size/extent in some cases (not very accurate staging) Color Doppler helpful in studies, not widely practiced. Elastography good for peripheral zone cancers in studies, but not widely practiced. Therapy guidance Brachy, cryo-, high intensity focused US

19 US not very good at visualizing tumor sites. Systematic Biopsy needle core samples Diagnosis
20 Other imaging prior to diagnosis? Limited studies of MRI use in biopsy naïve patients. Effective but more expensive. Studies have shown approach to be cost effective, but not widely adopted.
21 Prostate Cancer Data available at diagnosis PSA DRE / TRUS (T-stage) Biopsy Histologic grade (Gleason score, 2-10) Sum of Major (listed first) and Minor (listed second) histology. Cancer = pattern 3,4,5; Sum (i.e.): 3+3 = 6 (best), 3+4=7,4+3=7, 4+4=8, 4+5=9, 5+4=9, 5+5=10 (worst). Map: # cores, locations (volume estimate) Imaging results MRI results (if used to guide bx and/or stage) CT and bone scan results (appropriate in higher risk pts.)
22 Clinical Staging (AJCC 2017) T Stage TX Primary tumor cannot be assessed T0 No evidence of primary tumor T1 Clinically not palpable T1a Incidental histologic finding in 5% or less of tissue resected (TURP) T1b Incidental histologic finding >5% of tissue resected T1c Tumor in needle biopsy but not palpable T2 Tumor is palpable and confined within prostate T2a Tumor involves one-half of one side or less T2b Tumor involves more than one-half of one side but not both sides T2c Tumor involves both sides T3 Extraprostatic tumor that is not fixed or does not invade adjacent structures T3a Extraprostatic extension (unilateral or bilateral) T3b Tumor invades seminal vesicle(s) T4 Tumor is fixed or invades adjacent structures other than seminal vesicles, such as external sphincter, rectum, bladder, levator muscles, and/or pelvic wall Lymph nodes NX: Regional nodes cannot be assessed N0: No regional lymph node metastasis N1: Regional lymph node metastasis Distant Metastases MX: distant metastasis cannot be evaluated M0: No distant metastases M1: Distant metastasis M1a: nonregional lymph node M1b: bone M1c: Other sites
23 Use of Nomograms Individual parameters limited PSA Gleason score Clinical T-stage Combined are good predictors of actual disease Tumor extent (stage) Likely outcomes

24 Nomograms: example Partin Table for PSA ng/ml Partin AW, et al., Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional update.jama, 277(18):
25 Prostate Cancer Treatment goals - individualized Risk adjusted Patient specific Maximize cancer control Minimize risks of complications Not over-treat Treatment selection Surveillance watchful waiting Prostatectomy Radiation therapy (RT) +/- hormones Hormones/castration
26 Prostate Cancer Imaging Imaging Goals Disease (tumor) detection, monitoring (active surveillance) Accurate state of disease (Stage) MRI is more accurate than nomograms Determine specific patient risk (risk stratification) Evolution over last decade: When and how to use imaging. Newer methods for disease assessments in suspected recurrence

27 Prostate Cancer: Computed Tomography Not effective local staging Routine screening for comorbid disease not cost effective* Nodes: routine imaging not justified** Selected criteria for use: PSA > 20 ng/ml Gleason score > 7 T3 lesion by DRE Nodes, Bone, Gross local dx * Forman, AJR 1994 **Partin, J Urol 1993 Blaustein J Urol 1994 Wolf, J Urol 1995
 Poor sensitivity 35% (25-75) Misses lots of small metastases CT and MRI equivalent Image")
28 Prostate Cancer CT Lymph Nodes Size criteria (usually 1.0 cm) Poor sensitivity 35% (25-75) Misses lots of small metastases CT and MRI equivalent Image abdomen if regional adenopathy present

29 PROSTATE CANCER Radionuclide Bone Scan Pre-Treatment Evaluation: Staging Radionuclide bone scan is NOT needed if PSA value is < 10ng/ml & there are no skeletal symptoms* * JAMA 1993


30 MRI Prostate T2-weighted Images Prostate zonal anatomy displayed Multi-planar assessment for anatomic cross-referencing Lesion detection/characterization: based on signal characteristics and morphology Periprostatic tissues well assessed Axial T2WI Coronal T2WI

31 Zonal anatomy Coronal at urethra CZ TZ AX T2WI PZ COR T2WI

32 Zonal anatomy Coronal anterior to urethra CZ TZ TZ AX T2WI PZ COR T2WI


")
33 Prostate - MRI Benign Prostatic Hyperplasia (BPH) Small vol. Moderate vol. Large vol. Transition zone = 95% Rare BPH nodules in PZ, CZ, exophytic besides median lobe Trend but not direct causative relationship between volume of BPH and symptoms Secondary importance to cancer for almost all MRI exams Gland volumes: g (or ml) young males to > 200 g (ml) older males from BPH
34 Prostate MRI, 1.5 T fairly standardized Best image quality with use of an endorectal coil 3.0 T (More powerful MRI) - with or without ER coil MRI Technique
35 Prostate MRI, 1.5 T fairly standardized Best image quality with use of an endorectal coil 3.0 T (More powerful MRI) - with or without ER coil MRI Technique

36 Prostate MRI, 1.5 T fairly standardized Best image quality with use of an endorectal coil 3.0 T (More powerful MRI) - with or without ER coil MRI Technique

37 Prostate homogeneous low intensity like CT Bone lesions More sensitive than bone scan for small intramedulary mets* Enlarged nodes Post-biopsy hemorrhage MRI Prostate T1-weighted Pelvis *Taoka T, et al., AJR Dec Axial T1WI

38 MRI Prostate T1-weighted Pelvis Prostate homogeneous low intensity like CT Bone lesions Enlarged nodes Post-biopsy hemorrhage Axial T1WI
 after bx")
39 MRI Prostate T1-weighted Pelvis Prostate homogeneous low intensity like CT Bone lesions Enlarged nodes Post-biopsy hemorrhage image 3-4 weeks (minimum) after bx Axial T1WI

 appx.")
40 Reporting gland volume Method of volume estimation 3 dimensions Use sagittal and transaxial imitates sono technique Be sure to extend AP back to anterior rectal margin Calculate ellipsoid volume (4/3 PI * width axis radius * length axis radius * height axis radius. ) appx. = W*H*L/2 or W*L*H*0.52
 Measures free diffusion of water Restricted diffusion high SI on high b value image")

41 MRI: Diffusion weighted imaging = DWI A method of prostate cancer detection in the peripheral zone (PZ) Measures free diffusion of water Restricted diffusion high SI on high b value image set = cancer suspicious lesion Dark lesions in PZ on ADC map = cancer suspect lesions b = 1000 Gleason 4+3 = 7, 2 cores from right, 30%, Gleason 6, 2 cores from left 20%. PSA 8.4. ADC map

42 T2 Tumor localization: PZ Dominant mass Confluent low signal centered in PZ Tumor bulge Loss of internal architecture left PZ

43 Tumor localization: PZ Dominant mass Confluent low signal Tumor bulge Loss of internal architecture Apical PZ

44 Transition Zone Tumors Confluent low signal Lack of low signal capsule Loss of internal architecture smudged charcoal sign Crossing/invading nodules Through TZ/PZ pseudocapsule Anterior fibromuscular stromal invasion AX T2WI

45 Extraglandular Extension Signs Asymmetric NVB Squared Pointed Spicules Retraction Extension to rectoprostatic angle Extension through capsular margin Bulging with irregularity AX T2WI
 Type I+II, 28% Ohori et al, Am J Surg Pathol.")
46 Seminal Vesicle Invasion Types Superiorly up the ducts (Type I, 26%) From ECE to SVI (Type II, 33%) Metastatic (Type III, 13%) Type I+II, 28% Ohori et al, Am J Surg Pathol Dec;17(12): /312 RRP with SVI (21%) COR T2WI
, transition Filled in vesicles Recognition based upon firm sense of normal AX")
47 Seminal Vesicle Invasion Signs Thickened walls Asymmetric, side of tumor (Type II) Up the ducts (Type I), transition Filled in vesicles Recognition based upon firm sense of normal AX T2WI

48 T4 Disease Rectum Gross invasion Not with broad contact and bulge Bladder neck Early difficult Invasion of muscular wall AX T2WI

49 T4 Disease Rectum Gross invasion Not with broad contact and bulge Bladder neck Early difficult Invasion of muscular wall AX T2WI


50 Multifocal DWI and T2WI: Suspected TZ and PZ tumors Possible FMS extension, questionable ECE Positive lesions on DWI (ADC map) Path showed no ECE, Gleason 3+4 = 7, tumor at both sites
51 Dynamic Contrast Enhanced (DCE) Normal Suspect Ca Rising Plateau Early peak Washout



52 Small L PZ prostate cancer T2WI ADC DCE early
53 Prostate Cancer Interpretation and Reporting System: PI-RADS v2 (2105) Based on T2WI, DWI and DCE PI-RADS v2 Assessment Categories PIRADS 1 Very low (clinically significant cancer is highly unlikely to be present) PIRADS 2 Low (clinically significant cancer is unlikely to be present) PIRADS 3 Intermediate (the presence of clinically significant cancer is equivocal) PIRADS 4 High (clinically significant cancer is likely to be present) PIRADS 5 Very high (clinically significant cancer is highly likely to be present)
 that would merit definitive treatment. Filson CP, Marks LS, Litwin MS.CA Cancer J Clin. 2015 Jul-Aug;65(4):265-82.")
54 Active Surveillance aim to maintain the opportunity of curing more aggressive disease via structured monitoring (e.g., with PSA testing and repeat prostate biopsies), which attempts to identify any change in disease risk (e.g., an increase in Gleason score) that would merit definitive treatment. Filson CP, Marks LS, Litwin MS.CA Cancer J Clin Jul-Aug;65(4):
55 MRI in Active surveillance MRI used to verify clinically insignificant disease Small tumor or none Safe to delay treatment Continue PSA monitoring Repeat biopsy, sometimes with another MRI to find target Sometimes finds target for biopsy or repeat biopsy
56 MR guided biopsy US-MRI fusion Cognitive In-bore



57 MR guided biopsy US-MRI fusion Cognitive In-bore
58 Imaging after treatment Indications (when appropriate) Suspected local recurrence after prostatectomy or radiation therapy (PSA recurrence ) Suspected metastatic disease based on clinical features and absence of disease at the treated prostate site. Re-imaging detected metastatic disease to judge treatment effect May allow for localized recurrence or metastatic treatments. Options CT, MRI, Bone scan FDG PET (Only some utility for very aggressive advanced disease) Newer nuclear medicine tests

59 18 F Sodium Fluoride PET/CT More sensitive than traditional bone scan Risk of false positive sites detected Example: 2 hot spots the larger one is a metastasis, the smaller one is degenerative bone changes Available at VAMC, many insurances not covering Oldan JD, Hawkins AS, Chin BB. 18F Sodium Fluoride PET/CT in Patients with Prostate Cancer: Quantification of Normal Tissues, Benign Degenerative Lesions, and Malignant Lesions. World journal of nuclear medicine May;15(2):102.
 Detection of recurrence after radiation therapy more challenging but possible Oppenheimer DC, Weinberg EP, Hollenberg GM, Meyers SP.")
60 MRI for local recurrence Effective for detection of local disease recurrence after prostatectomy when PSA recurs More likely positive for higher PSA (1.5 or higher) Detection of recurrence after radiation therapy more challenging but possible Oppenheimer DC, Weinberg EP, Hollenberg GM, Meyers SP. Multiparametric magnetic resonance imaging of recurrent prostate cancer. Journal of clinical imaging science. 2016;6.
 Has shown efficacy in detection of metastatic disease in normal sized nodes, bone mets without CT")
61 Axumin (18F-fluciclovine or FACBC) FDA approved since May 2016 for detection of recurrence suspected from elevated PSA after treatment Axumin (fluciclovine) Has shown efficacy in detection of metastatic disease in normal sized nodes, bone mets without CT abnormality
Mx cancer. Francesco Ceci et al.")
62 C-11 Choline PET Post RRP, PSA up, mets detected Progressed on anti-androgen Localized treatments partial response 62-y-old patient with Gleason score of and pt3b N1(8/24)Mx cancer. Francesco Ceci et al. J Nucl Med 2016;57:49S-54S (c) Copyright 2014 SNMMI; all rights reserved

63 68Ga-PSMA PET/CT 68Ga-PSMA PET/CT Multiple studies showing ability to detect bone and lymph node metastases where other modalities fail
64 Thank You Q and A
11/10/2015. Prostate cancer in the U.S. Multi-parametric MRI of Prostate Diagnosis and Treatment Planning. NIH estimates for 2015.
 Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
Multi-parametric MRI of Prostate Diagnosis and Treatment Planning Temel Tirkes, M.D. Associate Professor of Radiology Director, Genitourinary Radiology Indiana University School of Medicine Department
I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a product in my presentation.
 Prostate t Cancer MR Report Disclosure Information Vikas Kundra, M.D, Ph.D. I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a g product
Prostate t Cancer MR Report Disclosure Information Vikas Kundra, M.D, Ph.D. I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a g product
Prostate MRI. Overview. Introduction 2/20/2015. Prostate cancer is most frequently diagnosed noncutaneous cancer in males (25%)
") Prostate MRI John Bell, MD Introduction Prostate Cancer Screening Staging Anatomy Prostate MRI overview Functional MRI Multiparametric Approach Indications Example Cases Overview Introduction Prostate
Prostate MRI John Bell, MD Introduction Prostate Cancer Screening Staging Anatomy Prostate MRI overview Functional MRI Multiparametric Approach Indications Example Cases Overview Introduction Prostate
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
Prostate MRI: Who needs it?
 Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
Prostate MRI: Who needs it? Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Abdominal Imaging Magnetic Resonance Science Center
PROSTATE MRI. Dr. Margaret Gallegos Radiologist Santa Fe Imaging
 PROSTATE MRI Dr. Margaret Gallegos Radiologist Santa Fe Imaging Topics of today s talk How does prostate MRI work? Definition of multiparametric (mp) MRI Anatomy of prostate gland and MRI imaging Role
PROSTATE MRI Dr. Margaret Gallegos Radiologist Santa Fe Imaging Topics of today s talk How does prostate MRI work? Definition of multiparametric (mp) MRI Anatomy of prostate gland and MRI imaging Role
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Chapter 2. Understanding My Diagnosis
 Chapter 2. Understanding My Diagnosis With contributions from Nancy L. Brown, Ph.D.,Palo Alto Medical Foundation Research Institute; and Patrick Swift, M.D., Alta Bates Comprehensive Cancer Program o Facts
Chapter 2. Understanding My Diagnosis With contributions from Nancy L. Brown, Ph.D.,Palo Alto Medical Foundation Research Institute; and Patrick Swift, M.D., Alta Bates Comprehensive Cancer Program o Facts
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Low risk. Objectives. Case-based question 1. Evidence-based utilization of imaging in prostate cancer
 Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Evidence-based utilization of imaging in prostate cancer Fergus Coakley MD, Professor of Radiology and Urology, Vice Chair for Clinical Services, Chief of Abdominal Imaging, UCSF Objectives State the modalities,
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017
 Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate cancer ~ diagnosis and impact of pathology on prognosis ESMO 2017 Dr Puay Hoon Tan Division of Pathology Singapore General Hospital Prostate cancer (acinar adenocarcinoma) Invasive carcinoma composed
Prostate MRI for local staging and surgical planning in prostate cancer
 Prostate MRI for local staging and surgical planning in prostate cancer 15th Annual Floyd A. Fried Advances in Urology Symposium June 23, 2017 Ray Tan, MD, MSHPM Assistant Professor Disclosures None Objectives
Prostate MRI for local staging and surgical planning in prostate cancer 15th Annual Floyd A. Fried Advances in Urology Symposium June 23, 2017 Ray Tan, MD, MSHPM Assistant Professor Disclosures None Objectives
Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Collaborative Staging
 Slide 1 Collaborative Staging Site-Specific Instructions Prostate 1 In this presentation, we are going to take a closer look at the collaborative staging data items for the prostate primary site. Because
Slide 1 Collaborative Staging Site-Specific Instructions Prostate 1 In this presentation, we are going to take a closer look at the collaborative staging data items for the prostate primary site. Because
GUIDELINEs ON PROSTATE CANCER
 GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
GUIDELINEs ON PROSTATE CANCER (Text update March 2005: an update is foreseen for publication in 2010. Readers are kindly advised to consult the 2009 full text print of the PCa guidelines for the most recent
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Essentials of Clinical MR, 2 nd edition. 73. Urinary Bladder and Male Pelvis
 73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
PSA. HMCK, p63, Racemase. HMCK, p63, Racemase
 Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Case 1 67 year old male presented with gross hematuria H/o acute prostatitis & BPH Urethroscopy: small, polypoid growth with a broad base emanating from the left side of the verumontanum Serum PSA :7 ng/ml
Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144
 Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144 Objectives: Detection of prostate cancer the need for better imaging What
Prostate MRI Hamidreza Abdi, MD,FEBU Post Doctoral Fellow Vancouver Prostate Centre UBC Department of Urologic Sciences May-20144 Objectives: Detection of prostate cancer the need for better imaging What
S1.04 PRINCIPAL CLINICIAN G1.01 COMMENTS S2.01 SPECIMEN LABELLED AS G2.01 *SPECIMEN DIMENSIONS (PROSTATE) S2.03 *SEMINAL VESICLES
 S2.03 *SEMINAL VESICLES") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Problems: TRUS Bx. Clinical questions in PCa. Objectives. Jelle Barentsz. Prostate MR Center of Excellence.
 Multi-parametric MR imaging in Problems: TRUS Bx Low Risk Prostate Cancer Important cancers are missed Jelle Barentsz Clinically insignificant cancers are identified by Prostate MR Center of Excellence
Multi-parametric MR imaging in Problems: TRUS Bx Low Risk Prostate Cancer Important cancers are missed Jelle Barentsz Clinically insignificant cancers are identified by Prostate MR Center of Excellence
Essential Initial Activities and Clinical Outcomes
 Essential Initial Activities and Clinical Outcomes Crystal Farrell 1,2 & Sabrina L. Noyes 2, Joe Joslin 2, Manish Varma 2,3, Andrew Moriarity 2,3, Christopher Buchach 2,3, Leena Mammen 2,3, Brian R. Lane
Essential Initial Activities and Clinical Outcomes Crystal Farrell 1,2 & Sabrina L. Noyes 2, Joe Joslin 2, Manish Varma 2,3, Andrew Moriarity 2,3, Christopher Buchach 2,3, Leena Mammen 2,3, Brian R. Lane
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
Prostate MRI: Not So Difficult. Neil M. Rofsky, MD, FACR, FSCBTMR, FISMRM Dallas, TX
 Prostate MRI: Not So Difficult Neil M. Rofsky, MD, FACR, FSCBTMR, FISMRM Dallas, TX What is the biggest barrier to your practice incorporating prostate MRI? 1) I don t know how to read the cases 2) I don
Prostate MRI: Not So Difficult Neil M. Rofsky, MD, FACR, FSCBTMR, FISMRM Dallas, TX What is the biggest barrier to your practice incorporating prostate MRI? 1) I don t know how to read the cases 2) I don
Current Clinical Practice. MR Imaging Evaluations. MRI Anatomic Review. Imaging to Address Clinical Challenges. Prostate MR
 BETH ISRAEL DEACONESS MEDICAL CENTER Prostate MR Neil M. Rofsky, MD Harvard Medical School Current Clinical Practice DIGITAL RECTAL EXAMINATION PSA ( ~ 20% False negative) BIOPSY (18-25% False negative)
BETH ISRAEL DEACONESS MEDICAL CENTER Prostate MR Neil M. Rofsky, MD Harvard Medical School Current Clinical Practice DIGITAL RECTAL EXAMINATION PSA ( ~ 20% False negative) BIOPSY (18-25% False negative)
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know
 MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know Michael S. Cookson, MD, FACS Professor and Chair Department of Urology Director of Prostate and Urologic Oncology University
MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know Michael S. Cookson, MD, FACS Professor and Chair Department of Urology Director of Prostate and Urologic Oncology University
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Prostate Overview Quiz
 Prostate Overview Quiz 1. The path report reads: Gleason 3 + 4 = 7. The Gleason s score is a. 3 b. 4 c. 7 d. None of the above 2. The path report reads: Moderately differentiated adenocarcinoma of the
Prostate Overview Quiz 1. The path report reads: Gleason 3 + 4 = 7. The Gleason s score is a. 3 b. 4 c. 7 d. None of the above 2. The path report reads: Moderately differentiated adenocarcinoma of the
Collecting Cancer Data: Prostate Q&A. Overview. NAACCR Webinar Series June 11, 2009
 Collecting Cancer Data: Prostate NAACCR 2008-2009 Webinar Series June 11, 2009 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview 2008-2009 NAACCR Webinar Series
Collecting Cancer Data: Prostate NAACCR 2008-2009 Webinar Series June 11, 2009 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview 2008-2009 NAACCR Webinar Series
AJCC Cancer Staging 8 th Edition. Prostate Chapter 58. Executive Committee, AJCC. Professor and Director, Duke Prostate Center
 AJCC Cancer Staging 8 th Edition Prostate Chapter 58 Judd W Moul, MD, FACS Executive Committee, AJCC Professor and Director, Duke Prostate Center Duke University Durham, North Carolina Validating science.
AJCC Cancer Staging 8 th Edition Prostate Chapter 58 Judd W Moul, MD, FACS Executive Committee, AJCC Professor and Director, Duke Prostate Center Duke University Durham, North Carolina Validating science.
PI-RADS V2 IN PRACTICE A PICTORIAL REVIEW
 PI-RADS V2 IN PRACTICE A PICTORIAL REVIEW KP Murphy, A Walsh, C Donagh, R Aljurayyan, AC Harris, SD Chang Department of Abdominal and GU Radiology, Vancouver General Hospital & University of British Columbia,
PI-RADS V2 IN PRACTICE A PICTORIAL REVIEW KP Murphy, A Walsh, C Donagh, R Aljurayyan, AC Harris, SD Chang Department of Abdominal and GU Radiology, Vancouver General Hospital & University of British Columbia,
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Stephen McManus, MD David Levi, MD
 Stephen McManus, MD David Levi, MD Prostate MRI Indications INITIAL DETECTION, STAGING, RECURRENT TUMOR LOCALIZATION, RADIATION THERAPY PLANNING INITIAL DETECTION Clinically suspected prostate cancer before
Stephen McManus, MD David Levi, MD Prostate MRI Indications INITIAL DETECTION, STAGING, RECURRENT TUMOR LOCALIZATION, RADIATION THERAPY PLANNING INITIAL DETECTION Clinically suspected prostate cancer before
Utility of Prostate MRI. John R. Leyendecker, MD
 Utility of Prostate MRI John R. Leyendecker, MD Professor of Radiology and Urology Executive Vice Chair of Clinical Operations Section Head, Abdominal Imaging Wake Forest University School of Medicine;
Utility of Prostate MRI John R. Leyendecker, MD Professor of Radiology and Urology Executive Vice Chair of Clinical Operations Section Head, Abdominal Imaging Wake Forest University School of Medicine;
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Outline (1) Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer
 Outline (2) Concepts in Prostate Pathology. Peculiarities of Prostate Cancer. Peculiarities of Prostate Cancer") Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
Concepts in Prostate Pathology Murali Varma Cardiff, UK wptmv@cf.ac.uk Sarajevo Nov 2013 Outline (1) Peculiarities of prostate cancer Peculiarities of prostate needle biopsy Needle bx vs. TURP Prostate
1. Benign Prostate Hyperplexia (BPH) 2. Prostate Cancer (PCa)
 2. Prostate Cancer (PCa)") Objectives: Our first segment focused in the anatomy and functions of the prostate gland, to get a clear understanding of the male Genito-Urinary System. Now, we will explore two of the main problems associated
Objectives: Our first segment focused in the anatomy and functions of the prostate gland, to get a clear understanding of the male Genito-Urinary System. Now, we will explore two of the main problems associated
Anatomic Imaging of Prostate Cancer
 Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute of Cancer Research Senior Scientist, Sunnybrook Research Institute Chief, Dept of Medical
Masoom Haider, MD, FRCP(C) Professor of Radiology, University of Toronto Clinician Scientist, Ontario Institute of Cancer Research Senior Scientist, Sunnybrook Research Institute Chief, Dept of Medical
What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen).
.") What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen). It is a very common cancer in men; some cancers grow very slowly,
What Is Prostate Cancer? Prostate cancer is the development of cancer cells in the prostate gland (a gland that produces fluid for semen). It is a very common cancer in men; some cancers grow very slowly,
How to detect and investigate Prostate Cancer before TRT
 How to detect and investigate Prostate Cancer before TRT Frans M.J. Debruyne Professor of Urology Andros Men s Health Institutes, The Netherlands Bruges, 25-26 September 2014 PRISM Recommendations for
How to detect and investigate Prostate Cancer before TRT Frans M.J. Debruyne Professor of Urology Andros Men s Health Institutes, The Netherlands Bruges, 25-26 September 2014 PRISM Recommendations for
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Introduction. Growths in the prostate can be benign (not cancer) or malignant (cancer).
 or malignant (cancer).") This information was taken from urologyhealth.org. Feel free to explore their website to learn more. Another trusted website with good information is the national comprehensive cancer network (nccn.org).
This information was taken from urologyhealth.org. Feel free to explore their website to learn more. Another trusted website with good information is the national comprehensive cancer network (nccn.org).
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
General information about prostate cancer
 Prostate Cancer General information about prostate cancer Key points Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the prostate. Signs of prostate cancer include
Prostate Cancer General information about prostate cancer Key points Prostate cancer is a disease in which malignant (cancer) cells form in the tissues of the prostate. Signs of prostate cancer include
Prostate Cancer DFP Case of the Week
 Prostate Cancer DFP Case of the Week Antonio C. Westphalen, MD PhD Clinical Prostate MR Imaging Program, Director Associate Professor of Radiology and Urology University of California, San Francisco Case
Prostate Cancer DFP Case of the Week Antonio C. Westphalen, MD PhD Clinical Prostate MR Imaging Program, Director Associate Professor of Radiology and Urology University of California, San Francisco Case
Diagnosis of prostate cancer
 Diagnosis of prostate cancer Epidemiology Prostate cancer (PC) is the most common cancer in men and the 2 nd cause of cancer death in the developed world. Incidence with age, reaching 80% at age 80 (at
Diagnosis of prostate cancer Epidemiology Prostate cancer (PC) is the most common cancer in men and the 2 nd cause of cancer death in the developed world. Incidence with age, reaching 80% at age 80 (at
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Brief History. Identification : Past History : HTN without regular treatment.
 Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
ADENOCARCINOMA OF THE PROSTATE
 Ref : ADENOCARCINOMA OF THE PROSTATE Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera Utara Clinical Manual of Urology, (Philip M. Hanno et al eds), McGraw-Hill Int ed, 3 rd ed, 2001
Ref : ADENOCARCINOMA OF THE PROSTATE Div. of Urology, Dept. Surgery Medical Faculty, University of Sumatera Utara Clinical Manual of Urology, (Philip M. Hanno et al eds), McGraw-Hill Int ed, 3 rd ed, 2001
Neoplasms of the Prostate and Bladder
 Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
MR-US Fusion Guided Biopsy: Is it fulfilling expectations?
 MR-US Fusion Guided Biopsy: Is it fulfilling expectations? Kenneth L. Gage MD, PhD Assistant Member Department of Diagnostic Imaging and Interventional Radiology 4 th Annual New Frontiers in Urologic Oncology
MR-US Fusion Guided Biopsy: Is it fulfilling expectations? Kenneth L. Gage MD, PhD Assistant Member Department of Diagnostic Imaging and Interventional Radiology 4 th Annual New Frontiers in Urologic Oncology
Using PET/CT in Prostate Cancer
 Using PET/CT in Prostate Cancer Legal Disclaimer These materials were prepared in good faith by MITA as a service to the profession and are believed to be reliable based on current scientific literature.
Using PET/CT in Prostate Cancer Legal Disclaimer These materials were prepared in good faith by MITA as a service to the profession and are believed to be reliable based on current scientific literature.
Diagnosis, pathology and prognosis including variant pathology
 PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
PROSTATE CANCER Diagnosis, pathology and prognosis including variant pathology No Conflict of Interest Universitat Autónoma de Barcelona F.Algaba Section of Pathology PROSTATE CANCER Diagnosis, pathology
Controversies in Prostate Cancer Screening
 Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Procedures Needle Biopsy Transurethral Prostatic Resection Suprapubic or Retropubic Enucleation (Subtotal Prostatectomy) Radical Prostatectomy
 Radical Prostatectomy") Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA
 Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA ESMO Cape Town 14 Feb 2018 Disclosures Advisory boards/lecturer/consultant-
Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA ESMO Cape Town 14 Feb 2018 Disclosures Advisory boards/lecturer/consultant-
1 Uniform hyperintense signal intensity (normal). 2 Linear (arrow), wedge-shaped, or diffuse mild hypointensity, usually indistinct margin.
. 2 Linear (arrow), wedge-shaped, or diffuse mild hypointensity, usually indistinct margin.") Figure 3 PI-RADS assessment for peripheral zone on T2-weighted imaging. 1 Uniform hyperintense signal intensity (normal). 2 Linear (arrow), wedge-shaped, or diffuse mild hypointensity, usually indistinct
Figure 3 PI-RADS assessment for peripheral zone on T2-weighted imaging. 1 Uniform hyperintense signal intensity (normal). 2 Linear (arrow), wedge-shaped, or diffuse mild hypointensity, usually indistinct
Prostate Cancer MRI. Accurate Diagnosis and Treatment. PSA to Prostate MRI. for patients and curious doctors
 6 Prostate Cancer MRI Accurate Diagnosis and Treatment PSA to Prostate MRI for patients and curious doctors Samuel Aronson, M.D. Vincent Pelsser, M.D. Franck Bladou, M.D. Armen Aprikian, M.D. & Marc Emberton,
6 Prostate Cancer MRI Accurate Diagnosis and Treatment PSA to Prostate MRI for patients and curious doctors Samuel Aronson, M.D. Vincent Pelsser, M.D. Franck Bladou, M.D. Armen Aprikian, M.D. & Marc Emberton,
Prostate Cancer: Screening, Treatment, and Survivorship
 Prostate Cancer: Screening, Treatment, and Survivorship Timothy C. Brand, MD, FACS LTC(P), MC, USA Urology Residency Director Associate Professor of Surgery, USUHS Madigan Army Medical Center No Disclosures
Prostate Cancer: Screening, Treatment, and Survivorship Timothy C. Brand, MD, FACS LTC(P), MC, USA Urology Residency Director Associate Professor of Surgery, USUHS Madigan Army Medical Center No Disclosures
Supplemental Information
 Supplemental Information Prediction of Prostate Cancer Recurrence using Quantitative Phase Imaging Shamira Sridharan 1, Virgilia Macias 2, Krishnarao Tangella 3, André Kajdacsy-Balla 2 and Gabriel Popescu
Supplemental Information Prediction of Prostate Cancer Recurrence using Quantitative Phase Imaging Shamira Sridharan 1, Virgilia Macias 2, Krishnarao Tangella 3, André Kajdacsy-Balla 2 and Gabriel Popescu
Multiparametric MRI diagnostic value in a case of prostate cancer
 CASE REPORT J. Transl. Med. Res 2015;20(3):162-167 Multiparametric MRI diagnostic value in a case of prostate cancer Gelu Adrian Popa 1,4, Ioana Gabriela Lupescu 1,4, Emi M. Preda 1,4, Cristina Nicolae
CASE REPORT J. Transl. Med. Res 2015;20(3):162-167 Multiparametric MRI diagnostic value in a case of prostate cancer Gelu Adrian Popa 1,4, Ioana Gabriela Lupescu 1,4, Emi M. Preda 1,4, Cristina Nicolae
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Diagnosis and management of prostate cancer in the
 Diagnosis and management of prostate cancer in the Jeremy Teoh ( 張源津 ) Assistant Professor, Department of Surgery, The Chinese University of Hong Kong. Email: jeremyteoh@surgery.cuhk.edu.hk Estimated age-standardised
Diagnosis and management of prostate cancer in the Jeremy Teoh ( 張源津 ) Assistant Professor, Department of Surgery, The Chinese University of Hong Kong. Email: jeremyteoh@surgery.cuhk.edu.hk Estimated age-standardised
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT
 MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
Prostate Cancer Incidence
 Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Cancer. Description. Section: Surgery Effective Date: October 15, 2016 Subsection: Original Policy Date: September 9, 2011 Subject:
 Subject: Saturation Biopsy for Diagnosis, Last Review Status/Date: September 2016 Page: 1 of 9 Saturation Biopsy for Diagnosis, Description Saturation biopsy of the prostate, in which more cores are obtained
Subject: Saturation Biopsy for Diagnosis, Last Review Status/Date: September 2016 Page: 1 of 9 Saturation Biopsy for Diagnosis, Description Saturation biopsy of the prostate, in which more cores are obtained
Detection, Screening and. Jelle Barentsz, Radboudumc, Nijmegen, NL
 Detection, Screening and Staging with mpmri Jelle Barentsz, Radboudumc, Nijmegen, NL NO CONFLICT OF INTEREST Paradigm shift Past staging TRUS-GBx ERC, MRSI invasive Current detection agressive PCa mpmri-directed
Detection, Screening and Staging with mpmri Jelle Barentsz, Radboudumc, Nijmegen, NL NO CONFLICT OF INTEREST Paradigm shift Past staging TRUS-GBx ERC, MRSI invasive Current detection agressive PCa mpmri-directed
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Prostate Cancer Imaging :What the Urologist Needs to Know
 Prostate Cancer Imaging :What the Urologist Needs to Know Poster No.: C-2513 Congress: ECR 2015 Type: Educational Exhibit Authors: C. Aimeur, M. tabouche, A. habouchi, A. Habba, B. Mansouri; Algiers/DZ
Prostate Cancer Imaging :What the Urologist Needs to Know Poster No.: C-2513 Congress: ECR 2015 Type: Educational Exhibit Authors: C. Aimeur, M. tabouche, A. habouchi, A. Habba, B. Mansouri; Algiers/DZ
Prostate Biopsy. Prostate Biopsy. We canʼt go backwards: Screening has helped!
 We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
We canʼt go backwards: Screening has helped! Robert E. Donohue M.D. Denver V.A. Medical Center University of Colorado Prostate Biopsy Is cure necessary; when it is possible? Is cure possible; when it is
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Elevated PSA. Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017
 Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
When to worry, when to test?
 Focus on CME at the University of Calgary Prostate Cancer: When to worry, when to test? Bryan J. Donnelly, MSc, MCh, FRCSI, FRCSC Presented at a Canadian College of Family Practitioner s conference (October
Focus on CME at the University of Calgary Prostate Cancer: When to worry, when to test? Bryan J. Donnelly, MSc, MCh, FRCSI, FRCSC Presented at a Canadian College of Family Practitioner s conference (October
BLADDER PROSTATE PENIS TESTICLES BE YO ND YO UR CA NC ER
 BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
Some prostatic diseases
 Some prostatic diseases Benign Prostatic Hyperplasia (Nodular Hyperplasia) Extremely common Present in a significant number of men by the age of 40 & its frequency rises progressively with age, reaching
Some prostatic diseases Benign Prostatic Hyperplasia (Nodular Hyperplasia) Extremely common Present in a significant number of men by the age of 40 & its frequency rises progressively with age, reaching
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Prostate Cancer Case Study 1. Medical Student Case-Based Learning
 Prostate Cancer Case Study 1 Medical Student Case-Based Learning The Case of Mr. Powers Prostatic Nodule The effervescent Mr. Powers is found by his primary care provider to have a prostatic nodule. You
Prostate Cancer Case Study 1 Medical Student Case-Based Learning The Case of Mr. Powers Prostatic Nodule The effervescent Mr. Powers is found by his primary care provider to have a prostatic nodule. You
Localized at a focus, central point or locus. Localized finding distinct from neighboring tissues, not a threedimensional
 LEXICON ABNORMALITY Focal abnormality Focus Index Lesion Lesion Localized at a focus, central point or locus Localized finding distinct from neighboring tissues, not a threedimensional space occupying
LEXICON ABNORMALITY Focal abnormality Focus Index Lesion Lesion Localized at a focus, central point or locus Localized finding distinct from neighboring tissues, not a threedimensional space occupying
Prostate Cancer. David Wilkinson MD Gulfshore Urology
 Prostate Cancer David Wilkinson MD Gulfshore Urology What is the Prostate? Male Sexual Gland Adds nutrients and fluids for sperm This fluid is added to sperm during ejaculation Urethra (urine channel)
Prostate Cancer David Wilkinson MD Gulfshore Urology What is the Prostate? Male Sexual Gland Adds nutrients and fluids for sperm This fluid is added to sperm during ejaculation Urethra (urine channel)
Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Carcinoma of the Prostate Gland Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Multiparametric Prostate MRI: PI-RADS V.2
 Multiparametric Prostate MRI: PI-RADS V.2 Katarzyna J. Macura, MD, PhD, FACR, FSCBTMR The Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University, Baltimore, MD SCBT
Multiparametric Prostate MRI: PI-RADS V.2 Katarzyna J. Macura, MD, PhD, FACR, FSCBTMR The Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University, Baltimore, MD SCBT
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
The Selenium and Vitamin E Prevention Trial
 The largest-ever-prostate cancer prevention trial is now underway. The study will include a total of 32,400 men and is sponsored by the National Cancer Institute and a network of researchers known as the
The largest-ever-prostate cancer prevention trial is now underway. The study will include a total of 32,400 men and is sponsored by the National Cancer Institute and a network of researchers known as the
MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of
 POLICY: PG0367 ORIGINAL EFFECTIVE: 08/26/16 LAST REVIEW: 09/27/18 MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of Prostate Cancer GUIDELINES This policy does not certify
POLICY: PG0367 ORIGINAL EFFECTIVE: 08/26/16 LAST REVIEW: 09/27/18 MEDICAL POLICY Genetic and Protein Biomarkers for Diagnosis and Risk Assessment of Prostate Cancer GUIDELINES This policy does not certify
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Trends in Prostate Cancer Bob Weir AVP Underwriting Research Canada Life Reinsurance
 Trends in Prostate Cancer Bob Weir AVP Underwriting Research Canada Life Reinsurance Metropolitan Underwriting Discussion Group Annual Meeting January 30, 2017 Prostate Cancer is Common Rudy Giuliani Dx
Trends in Prostate Cancer Bob Weir AVP Underwriting Research Canada Life Reinsurance Metropolitan Underwriting Discussion Group Annual Meeting January 30, 2017 Prostate Cancer is Common Rudy Giuliani Dx
Case Scenario 1: Breast
 Case Scenario 1: Breast A 63 year old white female presents with a large mass in her left breast. 4/15/13 Mammogram/US: 1. Left breast mammographic and sonographic at 3:00 measuring 7.1 cm highly suggestive
Case Scenario 1: Breast A 63 year old white female presents with a large mass in her left breast. 4/15/13 Mammogram/US: 1. Left breast mammographic and sonographic at 3:00 measuring 7.1 cm highly suggestive
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Newer Aspects of Prostate Cancer Underwriting
 Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Newer Aspects of Prostate Cancer Underwriting Presented By: Jack Swanson, M.D. Keith Hoffman, NFP Moments Made Possible Objectives To review and discuss Conflicting messages about PSA testing Cautions
Prostate Cancer: Imaging in Diagnosis and Treatment
 March 2002 Prostate Cancer: Imaging in Diagnosis and Treatment David Sher, Harvard Medical School III Introduction The prostate gland is a walnut-sized exocrine gland that surrounds the urethra between
March 2002 Prostate Cancer: Imaging in Diagnosis and Treatment David Sher, Harvard Medical School III Introduction The prostate gland is a walnut-sized exocrine gland that surrounds the urethra between
They Do Look Alike : Mimics of Prostate Cancer in Biopsy Samples
 They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
They Do Look Alike : in Biopsy Samples Gladell P. Paner, MD Departments of Pathology and Surgery (Urology) University of Chicago, IL USA Gladell.paner@uchospitals.edu Benign in Needle Biopsy 1. Benign
Overview. What is Cancer? Prostate Cancer 3/2/2014. Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014
 Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C.
 Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,