SBI Breast Imaging Symposium 2016 Austin Texas, April 7, 2016
|
|
|
- Ellen Francis
- 6 years ago
- Views:
Transcription


1 Guidelines for Breast Cancer Screening: An Update SBI Breast Imaging Symposium 2016 Austin Texas, April 7, 2016 Robert A. Smith, PhD Cancer Control Department American Cancer Society Atlanta, GA
2 I have no conflicts of interest to report
3 Some Historic Observations about Breast Cancer Screening Guidelines For the past 30+, organizations have differed in their recommendations Over time, a growing number of organizations have issued guidelines, and these guidelines have clustered among like-minded organizations Endorsement and use of guidelines also have clustered among like-minded policy makers While end-users lament different recommendations, there is little chance that this situation will change soon
4 Breast Cancer Screening Guidelines At what age should average risk women start, and how often should screening take place? Organization Starting Age Screening Interval ACS, ASBS, ASCO ACR, ACOG, NCCN, NCBC USPSTF, AAFP, ACP 45; with the option to start at 40 Annual 40-54: Biennial 55+, with option to continue annual screening 40 Annual 50; the decision to begin screening between ages should be individualized based on risk and values Biennial, 40+ ACS=American Cancer Society; ASBS=American Society of Breast Surgeons; ASCO=American Society of Surgical Oncology; USPSTF=U.S. Preventive Services Task Force; ACOG=American College of Obstetricians and Gynecologists; NCCN=National Comprehensive Cancer Network; NCBC= National Consortium of Breast Centers; AAFP=American Academy of Family Physicians; ACP=American College of Physicians;
5 Breast Cancer Screening Guidelines At what age should average risk women stop screening? Organization ACS, ASBS, ASCO Stopping Age Continue screening as long as health is good and life expectancy is at least 10 ACOG Shared decisions 75+ ACR NCCN USPSTF, AAFP, ACP Continue screening as long as health is good and life expectancy is at least 5-7, and there is willingness to undergo additional testing Consider comorbidity and therapeutic decisions 74; Insufficient evidence to recommend for or against screening ACS=American Cancer Society; ASBS=American Society of Breast Surgeons; ASCO=American Society of Surgical Oncology; USPSTF=U.S. Preventive Services Task Force; ACOG=American College of Obstetricians and Gynecologists; NCCN=National Comprehensive Center Network; NCBC=National Consortium of Breast Centers; AAFP=American Academy of Family Physicians; ACP=American College of Physicians;
6 What accounts for the differences between the ACS and USPSTF Guidelines? Decisions Age to begin screening: 40 vs. 45 vs. 50? The inter-screening interval: 1 vs. 2? Age to stop screening: Age vs. health status Basic building blocks What data were considered, and not considered? Are judgments/opinions apparent? If so, what factors appear to influence judgments/opinions
7 Current Breast Cancer Screening Guideline for Average Risk Women: ACS (2015) & USPSTF (2016) Areas of Agreement Areas of Disagreement Recommendation ACS USPSTF Breast Self Exam (BSE) Clinical Breast Exam (CBE) Mammography USPSTF GRADES (A & B, C, D, I) ACS S = Strong Q = Qualified, if not labeled Not recommended Not recommended 40-44: Opportunity for informed decision, Annual (S): Annual 55+ Biennial, with option to continue annual screening 75+ Continue screening as long as health is good and life expectancy 10+ yrs. Against clinicians teaching BSE (D) Insufficient evidence (I) : Individual decision (C) Biennial Ages 50-74: Biennial (B) Ages 75+ : Insufficient evidence (I)
8 Guideline Development Methodology, ACS & USPSTF Areas of Similarity Areas of Dissimilarity Measuring disease burden ACS Absolute risk in 1, 5, 10 year age groups Incidence, Mortality, Incidencebased mortality, Premature mortality USPSTF Absolute risk in 10 year age groups Mortality Evidence of benefit Emphasis on benefit Emphasis on harms Randomized controlled trials (less) Observational studies (more) Modeling (less) Individual Absolute benefit (higher) False positives (less) Biopsy (less) Anxiety (less) Overdiagnosis (less) Randomized controlled trials (more) Modeling (more) Population Absolute benefit (lower) False positives (more) Biopsy (more) Anxiety (more) Overdiagnosis (more)
9 Age to Begin Screening Key Issues & Evidence Data on the burden of disease Incidence Incidence-based mortality Premature mortality Data on the relative and absolute benefit of screening Mortality reduction is the common denominator between guidelines How endpoints are measured is a key difference between guidelines Data on harms associated with screening To what degree is the magnitude of harms considered? How good are the data on different harms
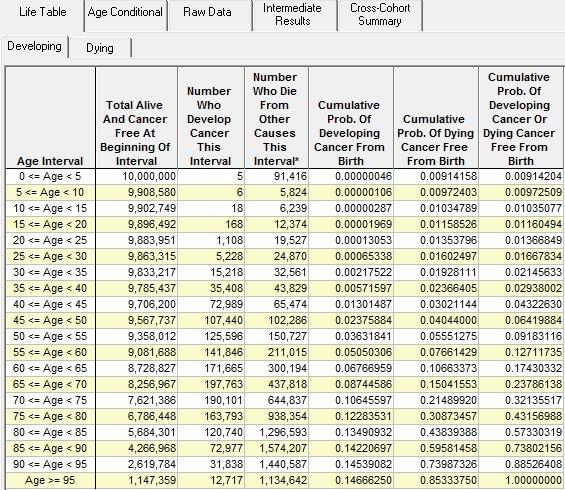
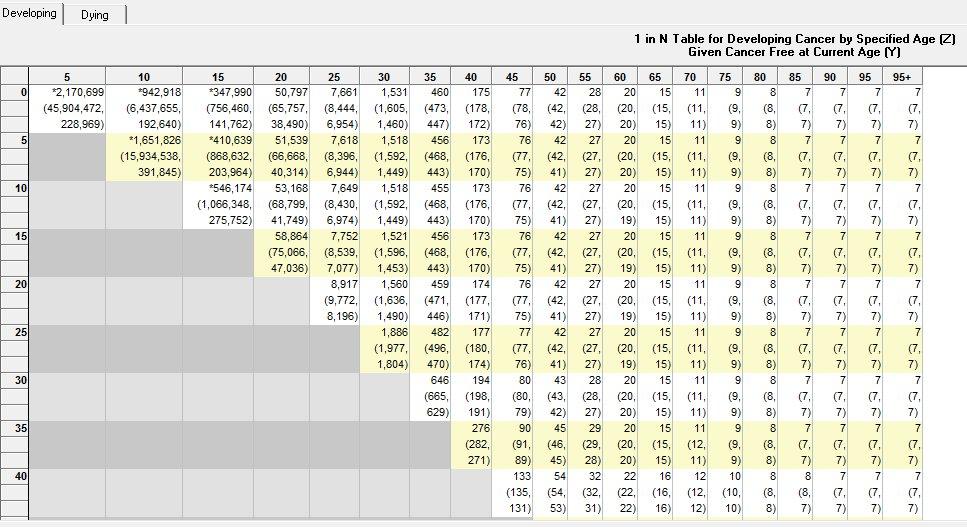
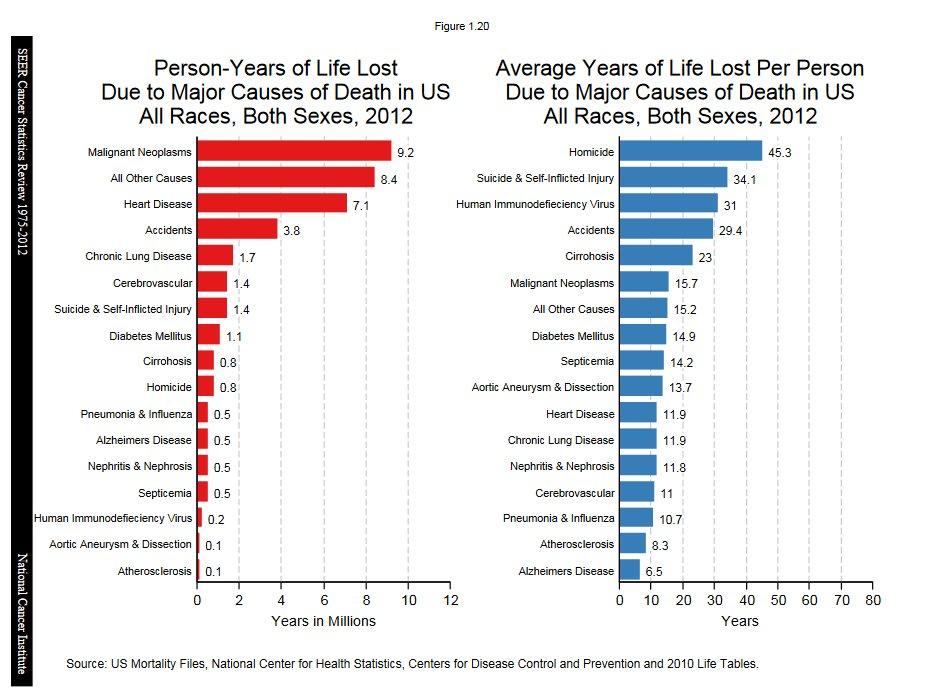
10 Age-Specific Disease Burden

11
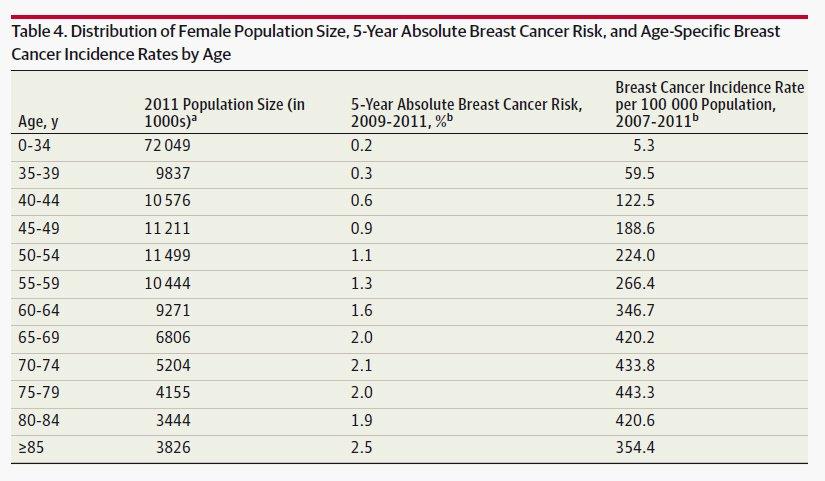
12 Breast Cancer in Younger Women Breast cancer in younger women Incidence rate per Probability of being diagnosed in the 1 year interval b % of BC deaths by age at 100,000 a % 1 in N diagnosis c % 2,212 1% % 1,943 1% % 1,713 1% % 1,440 1% % 1,232 1% % 1,076 1% % 954 1% % 857 1% % 774 1% % 706 2% % 648 2% Risk between ages is 9 in 10,000. The recall rate is 1,600 2,000 per 10,000 (about 1 in 5) a. Delay-adjusted incidence rates, SEER 18, b. SEER 18, c. Distribution of BC deaths ( ) from a BC diagnosis up to 15 prior, S

13 Age Distribution of Invasive Female Breast Cancer Cases, % 12% 13% 12% 12% 12% 10% 10% 9% 8% 8% 6% 6% 6% 6% 4% 3% 2% 0% <1% <1% % Source: SEER 18 registries.
14 Distribution of Breast Cancer Deaths by Age at Diagnosis, ,000 1,800 11% 11% 11% No. of breast cancer deaths 1,600 1,400 1,200 1, % 5% 7% 10% 9% 9% 9% 8% 8% <1% % Age at diagnosis Source: SEER 9 registries, patients followed for 15 after diagnosis.
15 Distribution of Years of Life Lost due to Death from Breast Cancer by Age at Diagnosis Distribution of YLL from breast cancer by age at diagnosis 16% 15% 15% 14% 12% 13% 12% % of total YLL due to BC 10% 8% 6% 4% 5% 9% 10% 7% 5% 4% 2% 2% 2% 2% 0% 0% 0% Age at diagnosis 15
16 Perspective on risk between ages At ages 40-44, risk of being diagnosed with breast cancer is low, but is increasing every year. During the 10 year period between ages and 50-54, risk also is increasing, but for these 22 million women, risk is more similar than different Three conclusions: 1. The period between age is characterized by a period of lower risk in the early 40s, and higher risk in the later 40s 2. The logic for beginning screening at age 50 also extends to age Considering risk in 10 year age groups obscures important differences between large age-specific subgroups




17 The Evolving Evidence for Mammography Screening the Randomized Trials
18 RCTs of screening mammography: Overall results in terms of breast cancer mortality Study ID Canadian NBSS-1 Canadian NBSS-2 Edinburgh HIP Two-County Trial Malmo-1 Malmo-2 Stockholm Gothenburg UK Age Trial Overall RR (95% CI) 1.06 (0.80, 1.40) 1.02 (0.78, 1.33) 0.71 (0.53, 0.95) 0.77 (0.62, 0.97) 0.69 (0.56, 0.84) 0.82 (0.67, 1.00) 0.64 (0.39, 1.06) 0.91 (0.65, 1.27) 0.76 (0.56, 1.04) 0.83 (0.66, 1.04) 0.79 (0.73, 0.86) Overall RR = 0.79 (95% CI: 0.73, 0.86) Tabar, et al. Breast J, 2014 Heterogeneity p = 0.3
19 Tabar, et al. Breast J, 2014
20 Summary of RCT Relative Incidence of Node Positive Tumors and Relative Mortality Women Aged Study Relative Incidence Node + Tumor (N+) Relative Mortality Two County (W-E).84 (16% < N+).87 (13% < deaths) Malmo.56 (44% < N+).64 (36% < deaths) Gothenburg.64 (36% < N+).56 (44% < deaths) Stockholm.98 (2% < N+) 1.01 (1% > deaths) HIP.82 (18% < N+).77 (27% < deaths) Edinburgh.73 (27% < N+).81 (19% < deaths) NBSS (40% > N+).97 (3% < deaths) * * * Mortality reductions are statistically significant
21 USPSTF Meta-Analysis of the RCTs, Women Ages Overall RR = 0.92, or an 8% breast cancer mortality reduction associated with an invitation to screening. Adjusting RCT RR s to the long accrual method diminishes the estimate of benefit Nelson, et al. Annals of Internal Medicine, 2016
22 Figure 2: Effects of Invitation to screening on the relative risk of being diagnosed with a stage III+ tumor, or tumor 4 or 5 cm in size Women aged yrs Women aged 50+ yrs
23 USPSTF Meta-Analysis of the RCTs, Women Ages 39-49, and Estimate of Absolute Benefit over 10 of screening Age Mortality rate per 100,000 person What s wrong with this estimate? Screening period and follow-up period are contemporaneous, and follow-up is too short Expected deaths are too low Relative benefit of mammography is too low Overall net benefit is underestimated Nelson, et al. Annals of Internal Medicine, 2016 Breast cancer mortality reduction RR Deaths prevented with screening 10, 000 women over







24 The Evolving Evidence for Mammography Screening Beyond the RCTs: Trend Studies, Incidence-Based Mortality Studies, Case Control Studies
, and the")
25 Incidence-Based Mortality Evaluations of the Impact of Modern Service Screening in Europe EUROSCREEN Group IBM studies: N = 20 In an IBM study all breast cancer deaths occurring in a population over a period of time are enrolled in the study only if the breast cancer diagnosis occurred in a certain time/age window (taking into account eligibility and opportunity to be screened), and the population is classified by screening or by invitation to screening. J Med Screen 2012;19 Suppl1:14 25
26 EUROSCREEN Incidence-based mortality estimates for breast cancer mortality reduction in women ages 50-69, exposed versus not-exposed to screening J Med Screen 2012;19 Suppl1:14 25

27 Effectiveness of Population-Based Service Screening With Mammography for Women Ages 40 to 49 Years Contemporaneous comparison of breast cancer mortality in Swedish counties offering mammography vs. those not offering mammography Average follow-up = 16 Cancer 2010; published online: 29 SEP 2010

28 Map of Study and Control Group Areas, and Crude Cumulative Breast Cancer Mortality per 100,000 Person Years Control Group Study Group Cancer 2010; published online: 29 SEP 2010 RR = 0.74; 95% CI )
 and nonexposed women, 1990-2009 7 of 12 Canadian breast cancer programs, representing 85% of the population SMRs were calculated comparing observed")
29 Pan-Canadian Study of Mammography Screening Comparison of breast cancer screening among exposed (2.8 million) and nonexposed women, of 12 Canadian breast cancer programs, representing 85% of the population SMRs were calculated comparing observed mortality in participants to that expected based upon nonparticipant rates.
30 Standardized mortality ratios (SMRs) by Canadian province for ages at entry: Summary estimates are based upon random effects models. All statistical tests were two-sided % fewer deaths JNCI 2014;106(11) 40% fewer deaths
31 Perspective on the Benefit of Screening in Average Risk Women: ACS (2015) & USPSTF (2016) Areas of Agreement Areas of Disagreement Evidence ACS USPSTF Randomized Trials (RCT) Meta-analysis of the RCTs Observational Studies Modeling Studies Low RCT relative risks measure efficacy, Not effectiveness Discount value of meta-analysis Consider features of individual RCTs More influential for measuring effectiveness than RCTs Emphasis on exposure to screening Accepts relative benefits are similar in all age groups Considered, but less influential than empirical data Low RCT relative risks measure efficacy and effectiveness Benefits increasing with age Prioritize meta-analysis Does not consider outcomes of individual RCTs Reviewed, but did not influence estimate of benefit Very influential, and preferred over observational data

32 The Screening Interval There have been no trials that have compared annual screening with biennial screening The screening interval has been influenced by estimates of tumor growth rates & interval cancer rates Screening intervals also have been recommended based on tradeoffs between estimated mortality rates and false positive rates

33 Interval Cancer Rate as a Percent of the Expected Incidence in the Unscreened Population by Year Since Negative Screen, Swedish Two County Study Faster tumor growth in premenopausal women results in a higher interval cancer rate. Thus, screening intervals should be tailored to the age of the woman.
34 Supplemental analysis on the screening interval from NCI funded Breast Cancer Surveillance Consortium Miglioretti D, et al. Risk of less-favorable breast tumor characteristics with biennial versus annual mammography by age and menopausal status Design, setting, and participants: --15,440 women aged with breast cancer diagnosed within 1 year of an annual or within 2 of a biennial screening mammogram performed from Updated previous analyses by using narrower screening intervals, specifically months for annual and months for biennial screening intervals. Main finding--among premenopausal women, biennial screeners had higher proportions of tumors with advanced stage (relative risk [RR]=1.28), larger size (RR=1.21), and any less-favorable prognostic characteristic (RR=1.11) compared with annual screeners [all RR were statistically significant]. 34

35 RR (95% CI) of Less-favorable Invasive Cancer Characteristics for Biennial versus Annual Screeners, by Age, Menopausal Status, and Current Hormone Therapy Use, Adjusted for Race/Ethnicity, First-Degree Family History of Breast Cancer 35
36 Perspective on the Screening Interval: ACS (2015) & USPSTF (2016) Areas of Agreement Areas of Disagreement Evidence ACS USPSTF Randomized Trials (RCT) Observational Studies Modeling studies Benefit vs. harms Compared interval cancer rates in the RCTs by age Relied on supplemental analysis of Breast Cancer Surveillance Consortium data Judged modeling studies not suitable due to lack of hybrid models that tailored age and screening interval Harms not a factor in determining the screening interval Focused on lack of head to head RCTs comparing 1 vs. 2 year screening Discounted results of observational studies Relied entirely on modeling. Harms an important factor in determining the screening interval, both false positives & overdiagnosis
37 Distribution of breast cancer deaths by age at diagnosis, ,000 1,800 11% 11% 11% 34% Number of Breast Cancer Deaths 1,600 1,400 1,200 1, % 5% 7% 10% 9% 9% 9% 8% 8% <1% 1% Age at diagnosis Source: SEER 9 registries, patients followed for 15 after diagnosis.
38 38
39 Perspective on Age to Stop Screening: ACS (2015) & USPSTF (2016) Areas of Agreement Areas of Disagreement Evidence ACS USPSTF Randomized Trials (RCT) RCT data are limited RCT data are limited Observational and Modeling Studies Yes No Primary Emphasis Longevity and remaining of life in good health Ease of detection & treatment Lack of RCT data Comorbidity Overdiagnosis Benefit vs. harms Favorable within defined boundaries (good health and longevity) Uncertain


40 Adverse Outcomes Associated with Screening (aka harms ) In recent there has been growing concerns about harms associated with screening Guideline developers are obliged to scrutinize harms as well as benefits This is a challenge because there are not equivalent metrics for measuring benefits and harms 40

41 10 Year Probability of a False Positive Exam Based on Age at First Mammogram Annual Biennial 0 Overall False-positive recall probability: 16.3% at first mammogram 9.6% at subsequent exams Probability of false-positive biopsy recommendation: 2.5% at first mammogram 1.0% at subsequent exams

42 New data of the rate of False Positive Mammography results from digital mammography. First mammogram not included. Women in their 40s have the highest rate. (Source, BCSC data, Pacific NW EPC, 2015) 42
43 Overdiagnosis Overdiagnosis is the detection of a cancer by screening that would not have progressed to become symptomatic in a woman s lifetime. Estimates of overdiagnosis range from 0% to > 50%, and vary greatly in terms of methodologic rigor The ACS systematic evidence review Duke group judged the quality of evidence for the existence of some overdiagnosis to be HIGH, but judged the quality of evidence on the magnitude of overdiagnosis to be LOW. 43
![The Marmot Report concluded that approximately 19% of cancers were overdiagnosed [This estimate was judged by many to be too high] Of the 307,000 women aged 50 52 who are invited to screening each](/docs-images/77/75847757/images/44-0.jpg "year, [approximately] 1% would have an overdiagnosed cancer during the next 20. Given the uncertainties around the estimates, the figures quoted give a spurious impression of accuracy.")
44 The Marmot Report concluded that approximately 19% of cancers were overdiagnosed [This estimate was judged by many to be too high] Of the 307,000 women aged who are invited to screening each year, [approximately] 1% would have an overdiagnosed cancer during the next 20. Given the uncertainties around the estimates, the figures quoted give a spurious impression of accuracy. Source: Marmot MG, et al. BMJ (2013) 108,
45 Perspective on Overdiagnosis: ACS (2015) & USPSTF (2016) Areas of Agreement Areas of Disagreement Evidence ACS USPSTF Randomized Trials (RCT) Observational Studies Modeling Studies Critical Evaluation of Estimates Estimate Ideal method for measuring overdiagnosis, but existing RCTs too limited Wide range of estimates (0-> 50%) Methodology highly variable Considered, but less influential than empirical data Yes Judged quality of estimates to be low Lifetime risk approach (1%) Accept estimates from some RCTs (Malmo and CNBSS) and ignore others (Two County & UK Age Trial) Noted, but USPSTF relied on RCT estimates Very influential, and preferred over observational data No Lives saved (1) vs. number overdiagnosed (2-3).this approach exaggerates the estimate of harm
46 Conclusions-1 There are important differences in current guidelines, but also important similarities All organizations emphasize that benefits outweigh harms at all ages All organizations endorse informed decision making All organizations endorse the importance of women being informed about benefits and limitations of screening
47 Conclusions-2 Ironically, the 2016 systematic review produced for the USPSTF recommendation update cites less benefit and more harms associated with mammography compared with the 2009 review However, the narrative of the USPSTF recommendation is more favorable about the benefits of screening, including screening in women under age 50
48 USPSTF perspective on risk between ages For women in their 40s, the benefit still outweighs the harms, but to a smaller degree; this balance may therefore be more subject to individual values and preferences than it is in older women. Women who value the possible benefit of screening mammography more than they value avoiding its harms can make an informed decision to begin screening.
49 USPSTF perspective on risk between ages It is, however, a false dichotomy to assume that the only options are to begin screening at age 40 or to wait until age 50. As women advance through their 40s, the incidence of breast cancer rises. The balance of benefit and harms may also shift accordingly over this decade, such that women in the latter half of the decade likely have a more favorable balance than women in the first half. Indeed, the CISNET models suggest that most of the benefit of screening women aged 40 to 49 would be realized by starting screening at age 45.

50 Conclusions-3 High adherence to even the least aggressive guideline would save more lives than the current weak adherence to regular screening The new ACS guideline allows clinicians and women to choose among options about when to begin screening, and how often to be screened The new guideline provides stronger evidence to support a choice among options.
51 Still.There are Legitimate Concerns About Guideline Differences The guidelines are too complicated Weak adherence to creating opportunities for informed decision making Referring clinicians are not prepared to discuss benefits, limitations, and harms associated with screening Lack of reminder systems will result in weaker adherence to recommended screening intervals 51
52 ACOG Consensus Workshop Core groups presented guidelines and rationale Other organizations summarized their guidelines, but also their opinions about guideline differences There is a clear sense that we must move beyond the status quo 52
53 Thank you
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Breast Cancer Screening September 21, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Breast Cancer Screening September 21, 2017 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer Screening American
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Breast Cancer Screening September 21, 2017 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer Screening American
CANCER SCREENING GUIDELINE CHALLENGES AND CONTROVERSIES
 CANCER SCREENING GUIDELINE CHALLENGES AND CONTROVERSIES RICHARD C. WENDER, MD CHIEF CANCER CONTROL OFFICER AMERICAN CANCER SOCIETY @RichWender In 1996, the American Cancer Society issued a challenge goal
CANCER SCREENING GUIDELINE CHALLENGES AND CONTROVERSIES RICHARD C. WENDER, MD CHIEF CANCER CONTROL OFFICER AMERICAN CANCER SOCIETY @RichWender In 1996, the American Cancer Society issued a challenge goal
5/24/16. Current Issues in Breast Cancer Screening. Breast cancer screening guidelines. Outline
 Disclosure information: An Evidence based Approach to Breast Cancer Karla Kerlikowske, MDDis Current Issues in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla
Disclosure information: An Evidence based Approach to Breast Cancer Karla Kerlikowske, MDDis Current Issues in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla
Current Strategies in the Detection of Breast Cancer. Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF
 Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
SCREENING FOR BREAST CANCER BREAST IMAGING
 SCREENING FOR BREAST CANCER BREAST IMAGING Liane Philpotts, MD, FSBI, FACR Professor, Radiology and Biomedical Imaging Division Chief, Breast Imaging Dec. 5, 2017 Warner, E. NEJM 2011 Screening for
SCREENING FOR BREAST CANCER BREAST IMAGING Liane Philpotts, MD, FSBI, FACR Professor, Radiology and Biomedical Imaging Division Chief, Breast Imaging Dec. 5, 2017 Warner, E. NEJM 2011 Screening for
Breast Cancer Screening
 Breast Cancer Screening Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Breast Cancer Screening Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
BREAST CANCER SCREENING:
 BREAST CANCER SCREENING: controversies D David Dershaw Memorial Sloan Kettering Cancer Center New York, NY Areas of general agreement about mammographic screening Screening mammography has been demonstrated
BREAST CANCER SCREENING: controversies D David Dershaw Memorial Sloan Kettering Cancer Center New York, NY Areas of general agreement about mammographic screening Screening mammography has been demonstrated
Controversies in Breast Cancer Screening
 Controversies in Breast Cancer Screening Arash Naeim, MD PhD Associate Professor of Medicine Divisions of Hematology-Oncology and Geriatric Medicine David Geffen School of Medicine University of California,
Controversies in Breast Cancer Screening Arash Naeim, MD PhD Associate Professor of Medicine Divisions of Hematology-Oncology and Geriatric Medicine David Geffen School of Medicine University of California,
Breast Screening: risks if you do and risks if you don t. Stephen W. Duffy Wolfson Institute of Preventive Medicine
 Breast Screening: risks if you do and risks if you don t Stephen W. Duffy Wolfson Institute of Preventive Medicine General principle There is often discussion of benefits and harms of breast screening
Breast Screening: risks if you do and risks if you don t Stephen W. Duffy Wolfson Institute of Preventive Medicine General principle There is often discussion of benefits and harms of breast screening
Breast Cancer Screening
 Breast Cancer Screening Claire Frost, MD R3 Talks 1 Objective 1. Understand risks and benefits of screening by reviewing current literature 2. Evaluate major society recommendations on breast cancer screening
Breast Cancer Screening Claire Frost, MD R3 Talks 1 Objective 1. Understand risks and benefits of screening by reviewing current literature 2. Evaluate major society recommendations on breast cancer screening
Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow
 Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow Debra A. Walz, RN, MS, AOCNP, WHNP-BC, RNFA Advanced Oncology & Women s Health Nurse Practitioner Oneida
Untangling the Confusion: Multiple Breast Cancer Screening Guidelines and the Ones We Should Follow Debra A. Walz, RN, MS, AOCNP, WHNP-BC, RNFA Advanced Oncology & Women s Health Nurse Practitioner Oneida
3/21/11 Tabar et al Lancet 2003;361:
 1 2 3 Tabar et al Lancet 2003;361:1405-1410 4 Tabar et al Lancet 2003;361:1405-1410 Tabar Rad Clin NA 2000;38:625-652, via R. Edward Hendrick, PhD, U. Colorado 5 6 7 8 Screening 40-49 50-59 60-69 Interval
1 2 3 Tabar et al Lancet 2003;361:1405-1410 4 Tabar et al Lancet 2003;361:1405-1410 Tabar Rad Clin NA 2000;38:625-652, via R. Edward Hendrick, PhD, U. Colorado 5 6 7 8 Screening 40-49 50-59 60-69 Interval
Update in Breast Cancer Screening
 Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla Kerlikowske, MD
Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla Kerlikowske, MD
Update in Breast Cancer Screening
 Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute and Grail - and - Karla Kerlikowske,
Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute and Grail - and - Karla Kerlikowske,
Breast Cancer Screening for Women at Average Risk
 1/51 Special Communication October 20, 2015 Breast Cancer Screening for Women at Average Risk 2015 Guideline Update From the American Cancer Society 1 2 3 Kevin C. Oeffinger, MD ; Elizabeth T. H. Fontham,
1/51 Special Communication October 20, 2015 Breast Cancer Screening for Women at Average Risk 2015 Guideline Update From the American Cancer Society 1 2 3 Kevin C. Oeffinger, MD ; Elizabeth T. H. Fontham,
The U.S. Preventive Services Task Force (USPSTF) CLINICAL GUIDELINE
 CLINICAL GUIDELINE") Annals of Internal Medicine CLINICAL GUIDELINE Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement Albert L. Siu, MD, MSPH, on behalf of the U.S. Preventive Services
Annals of Internal Medicine CLINICAL GUIDELINE Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement Albert L. Siu, MD, MSPH, on behalf of the U.S. Preventive Services
Screening Mammography for Women Aged 40 to 49 Years at Average Risk for Breast Cancer
 Ontario Health Technology Assessment Series 2007; Vol. 7, No. 1 Screening Mammography for Women Aged 40 to 49 Years at Average Risk for Breast Cancer An Evidence-Based Analysis January 2007 Medical Advisory
Ontario Health Technology Assessment Series 2007; Vol. 7, No. 1 Screening Mammography for Women Aged 40 to 49 Years at Average Risk for Breast Cancer An Evidence-Based Analysis January 2007 Medical Advisory
Population Prospective. Big Picture
 Mai Elezaby, MD? Population Prospective Big Picture Breast Cancer Most common cancer in women 2 nd leading cause of death U.S. 2016 estimates 246,660 new cases 40,450 deaths from breast cancer https://seer.cancer.gov/statfacts/html/breast.html
Mai Elezaby, MD? Population Prospective Big Picture Breast Cancer Most common cancer in women 2 nd leading cause of death U.S. 2016 estimates 246,660 new cases 40,450 deaths from breast cancer https://seer.cancer.gov/statfacts/html/breast.html
Screening Mammography Policy and Politics. Kevin L. Piggott, MD, MPH August 29, 2015
 Screening Mammography Policy and Politics Kevin L. Piggott, MD, MPH August 29, 2015 Objectives 1. To review the current recommendations for screening mammography by various national groups 2. To provide
Screening Mammography Policy and Politics Kevin L. Piggott, MD, MPH August 29, 2015 Objectives 1. To review the current recommendations for screening mammography by various national groups 2. To provide
Guidelines in Breast Screening Mammography: Pros and Cons JOSLYN ALBRIGHT, MD SURGICAL ONCOLOGIST, ADVOCATE CHRIST MEDICAL CENTER OCTOBER 1, 2016
 Guidelines in Breast Screening Mammography: Pros and Cons JOSLYN ALBRIGHT, MD SURGICAL ONCOLOGIST, ADVOCATE CHRIST MEDICAL CENTER OCTOBER 1, 2016 FACT Breast Cancer Screening Saves Lives Since 1990, screening
Guidelines in Breast Screening Mammography: Pros and Cons JOSLYN ALBRIGHT, MD SURGICAL ONCOLOGIST, ADVOCATE CHRIST MEDICAL CENTER OCTOBER 1, 2016 FACT Breast Cancer Screening Saves Lives Since 1990, screening
Updates In Cancer Screening: Navigating a Changing Landscape
 Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Overdiagnosis of Breast Cancer: Myths and Facts
 Overdiagnosis of Breast Cancer: Myths and Facts Mark A. Helvie, MD Department of Radiology Comprehensive Cancer Center University of Michigan Health System April 7, 2016 Objectives Define overdiagnosis
Overdiagnosis of Breast Cancer: Myths and Facts Mark A. Helvie, MD Department of Radiology Comprehensive Cancer Center University of Michigan Health System April 7, 2016 Objectives Define overdiagnosis
Breast Cancer Screening and Diagnosis
 Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Breast Cancer Screening and Diagnosis Priya Thomas, MD Assistant Professor Clinical Cancer Prevention and Breast Medical Oncology University of Texas MD Anderson Cancer Center Disclosures Dr. Thomas has
Otis W. Brawley, MD, MACP, FASCO, FACE
 Otis W. Brawley, MD, MACP, FASCO, FACE Chief Medical and Scientific Officer American Cancer Society Professor of Hematology, Medical Oncology, Medicine and Epidemiology Emory University Atlanta, Georgia
Otis W. Brawley, MD, MACP, FASCO, FACE Chief Medical and Scientific Officer American Cancer Society Professor of Hematology, Medical Oncology, Medicine and Epidemiology Emory University Atlanta, Georgia
Breast Cancer Risk Factors 8/3/2014
 Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Session Objectives Explain the rationale for initiation and frequency of clinical breast exams to clients
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Session Objectives Explain the rationale for initiation and frequency of clinical breast exams to clients
NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER
 GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER") NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER Guidelines 1. American Cancer Society (ACS). (1) ACS guidelines for breast cancer screening: update 2003. (2) American
NATIONAL GUIDELINE CLEARINGHOUSE (NGC) GUIDELINE SYNTHESIS SCREENING FOR BREAST CANCER Guidelines 1. American Cancer Society (ACS). (1) ACS guidelines for breast cancer screening: update 2003. (2) American
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens
 Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Disclosures Merck Nexplanon trainer Session Objectives Explain the rationale for initiation and frequency
Breast Cancer Screening: Changing Philosophies in Educating Women and Teens Courtney Benedict CNM MSN Disclosures Merck Nexplanon trainer Session Objectives Explain the rationale for initiation and frequency
News You Can Use: Recent Studies that Changed My Practice
 News You Can Use: Recent Studies that Changed My Practice Melissa McNeil, MD, MPH Chief, Section of Women s Health Division of General Internal Medicine University of Pittsburgh Sarah Tilstra, MD, MSc
News You Can Use: Recent Studies that Changed My Practice Melissa McNeil, MD, MPH Chief, Section of Women s Health Division of General Internal Medicine University of Pittsburgh Sarah Tilstra, MD, MSc
Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement
 Clinical Review & Education JAMA US Preventive Services Task Force RECOMMENDATION STATEMENT Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement US Preventive Services
Clinical Review & Education JAMA US Preventive Services Task Force RECOMMENDATION STATEMENT Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement US Preventive Services
Screening Overdiagnosis. Archie Bleyer, MD Department of Radiation Medicine Knight Cancer Institute at the Oregon Health & Science University
 Screening Overdiagnosis Archie Bleyer, MD Department of Radiation Medicine Knight Cancer Institute at the Oregon Health & Science University NNS Bottom Line I To prevent 1 death from breast cancer, 2,250
Screening Overdiagnosis Archie Bleyer, MD Department of Radiation Medicine Knight Cancer Institute at the Oregon Health & Science University NNS Bottom Line I To prevent 1 death from breast cancer, 2,250
General principles of screening: A radiological perspective
 General principles of screening: A radiological perspective Fergus Coakley MD, Professor and Chair, Diagnostic Radiology, Oregon Health and Science University General principles of screening: A radiological
General principles of screening: A radiological perspective Fergus Coakley MD, Professor and Chair, Diagnostic Radiology, Oregon Health and Science University General principles of screening: A radiological
Supplementary Online Content
 Supplementary Online Content Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. doi:10.1001/jama.2015.12783.
Supplementary Online Content Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. doi:10.1001/jama.2015.12783.
Examine breast cancer trends, statistics, and death rates, and impact of screenings. Discuss benefits and risks of screening
 Define Breast Cancer Screening Examine breast cancer trends, statistics, and death rates, and impact of screenings Discuss benefits and risks of screening Compare and contrast Screening Guidelines Optimal
Define Breast Cancer Screening Examine breast cancer trends, statistics, and death rates, and impact of screenings Discuss benefits and risks of screening Compare and contrast Screening Guidelines Optimal
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Quality ID #112 (NQF 2372): Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care
: Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care") Quality ID #112 (NQF 2372): Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #112 (NQF 2372): Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
ESTIMATING OVERDIAGNOSIS FROM TRIALS AND POPULATIONS OVERCOMING CHALLENGES, AVOIDING MISTAKES
 ESTIMATING OVERDIAGNOSIS FROM TRIALS AND POPULATIONS OVERCOMING CHALLENGES, AVOIDING MISTAKES NAVIGATING THE METHODS MINEFIELD Goal: establish conditions for valid estimation of overdiagnosis Excess incidence
ESTIMATING OVERDIAGNOSIS FROM TRIALS AND POPULATIONS OVERCOMING CHALLENGES, AVOIDING MISTAKES NAVIGATING THE METHODS MINEFIELD Goal: establish conditions for valid estimation of overdiagnosis Excess incidence
Screening for Breast Cancer: A Systematic Review to Update the 2009 U.S. Preventive Services Task Force Recommendation
 Evidence Synthesis Number 124 Screening for Breast Cancer: A Systematic Review to Update the 2009 U.S. Preventive Services Task Force Recommendation Prepared for: Agency for Healthcare Research and Quality
Evidence Synthesis Number 124 Screening for Breast Cancer: A Systematic Review to Update the 2009 U.S. Preventive Services Task Force Recommendation Prepared for: Agency for Healthcare Research and Quality
Screening for Breast Cancer
 Understanding Task Force Recommendations Screening for Breast Cancer U.S. Preventive Services Task Force (Task Force) has issued a final recommendation statement on Screening for Breast Cancer. se final
Understanding Task Force Recommendations Screening for Breast Cancer U.S. Preventive Services Task Force (Task Force) has issued a final recommendation statement on Screening for Breast Cancer. se final
Are We Ready to Predict Who is at Risk For What Kind of Breast Cancer? NOT YET NO DISCLOSURES 3/7/2015. Laura Esserman MD MBA
 Are We Ready to Predict Who is at Risk For What Kind of Breast Cancer? NOT YET But soon.... Laura Esserman MD MBA 2 Breast Cancer Gene Expression Profiling Prognostic Tests 1. OncotypeDX Recurrence Score
Are We Ready to Predict Who is at Risk For What Kind of Breast Cancer? NOT YET But soon.... Laura Esserman MD MBA 2 Breast Cancer Gene Expression Profiling Prognostic Tests 1. OncotypeDX Recurrence Score
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY
 EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY
 EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
EARLY DETECTION: MAMMOGRAPHY AND SONOGRAPHY Elizabeth A. Rafferty, M.D. Avon Comprehensive Breast Center Massachusetts General Hospital Harvard Medical School Breast Cancer Screening Early detection of
Melissa Hartman, DO Women s Health Orlando VA Medical Center
 Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Melissa Hartman, DO Women s Health Orlando VA Medical Center Most common non-skin cancer and Second deadliest cancer in women Majority are diagnosed by abnormal screening study An approach to breast cancer
Page 1. Cancer Screening for Women I have no conflicts of interest. Overview. Breast, Colon, and Lung Cancer. Jeffrey A.
 Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Cancer Screening for Women 2017 Breast, Colon, and Lung Cancer Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine University of California, San Francisco I have no conflicts
Shared Decision Making in Breast and Prostate Cancer Screening. An Update and a Patient-Centered Approach. Sharon K. Hull, MD, MPH July, 2017
 Shared Decision Making in Breast and Prostate Cancer Screening An Update and a Patient-Centered Approach Sharon K. Hull, MD, MPH July, 2017 Overview Epidemiology of Breast and Prostate Cancer Controversies
Shared Decision Making in Breast and Prostate Cancer Screening An Update and a Patient-Centered Approach Sharon K. Hull, MD, MPH July, 2017 Overview Epidemiology of Breast and Prostate Cancer Controversies
Introduction to Cost-Effectiveness Analysis
 Introduction to Cost-Effectiveness Analysis Janie M. Lee, MD, MSc RSNA Clinical Trials Methodology Workshop January 13, 2016 Why is Clinical Research Important to Radiology? Radiology currently occupies
Introduction to Cost-Effectiveness Analysis Janie M. Lee, MD, MSc RSNA Clinical Trials Methodology Workshop January 13, 2016 Why is Clinical Research Important to Radiology? Radiology currently occupies
Ge elastography cpt codes
 Ge elastography cpt codes Aetna considers digital mammography a medically necessary acceptable alternative to film mammography. Currently, there are no guideline recommendations from leading medical professional
Ge elastography cpt codes Aetna considers digital mammography a medically necessary acceptable alternative to film mammography. Currently, there are no guideline recommendations from leading medical professional
Measure #112 (NQF 2372): Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care
: Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care") Measure #112 (NQF 2372): Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Measure #112 (NQF 2372): Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Cancer Screening: Evidence, Opinion and Fact Dialogue on Cancer April Ruth Etzioni Fred Hutchinson Cancer Research Center
 Cancer Screening: Evidence, Opinion and Fact Dialogue on Cancer April 2018? Ruth Etzioni Fred Hutchinson Cancer Research Center Three thoughts to begin 1. Cancer screening is a good idea in principle Detect
Cancer Screening: Evidence, Opinion and Fact Dialogue on Cancer April 2018? Ruth Etzioni Fred Hutchinson Cancer Research Center Three thoughts to begin 1. Cancer screening is a good idea in principle Detect
TMIST A Bridge to Personalized Screening. Canadian Society of Breast Imaging April 26, 2018
 TMIST A Bridge to Personalized Screening Canadian Society of Breast Imaging April 26, 2018 Topics 1. Overview of TMIST Aims and Methods 2. Status of the Study (4/13/18) 3. How your site (in Canada) can
TMIST A Bridge to Personalized Screening Canadian Society of Breast Imaging April 26, 2018 Topics 1. Overview of TMIST Aims and Methods 2. Status of the Study (4/13/18) 3. How your site (in Canada) can
DESCRIPTION: Percentage of women years of age who had a mammogram to screen for breast cancer
 Quality ID #112 (NQF 2372): Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Quality ID #112 (NQF 2372): Breast Cancer Screening National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS ONLY MEASURE TYPE: Process DESCRIPTION: Percentage
Controversies in Breast Cancer Screening Strategies. Breast Cancer Screening Guidelines
 Controversies in Breast Cancer Screening Strategies Facilitator: Mary Lou Smith, JD, MBA Research Advocacy Network Panel: Therese Bevers, MD, The University of Texas MD Anderson Cancer Center Representing:
Controversies in Breast Cancer Screening Strategies Facilitator: Mary Lou Smith, JD, MBA Research Advocacy Network Panel: Therese Bevers, MD, The University of Texas MD Anderson Cancer Center Representing:
Evidence-based Cancer Screening & Surveillance
 Oncology for Scientists Spring 2014 Evidence-based Cancer Screening & Surveillance Martin C. Mahoney, MD, PhD, FAAFP Departments of Medicine & Health Behavior /Oncology_Feb 2014.ppt 1 Objectives: Principles
Oncology for Scientists Spring 2014 Evidence-based Cancer Screening & Surveillance Martin C. Mahoney, MD, PhD, FAAFP Departments of Medicine & Health Behavior /Oncology_Feb 2014.ppt 1 Objectives: Principles
Rudy Owens April 28, 2011 Case 16, Day 1. LO: Explore whether increasing early screening is the best way to lower death rates.
 Rudy Owens April 28, 2011 Case 16, Day 1 LO: Explore whether increasing early screening is the best way to lower death rates. Despite Mammography Screening Guideline Disagreements, the Early Detection
Rudy Owens April 28, 2011 Case 16, Day 1 LO: Explore whether increasing early screening is the best way to lower death rates. Despite Mammography Screening Guideline Disagreements, the Early Detection
10.2 Summary of the Votes and Considerations for Policy
 CEPAC Voting and Policy Implications Summary Supplemental Screening for Women with Dense Breast Tissue December 13, 2013 The last CEPAC meeting addressed the comparative clinical effectiveness and value
CEPAC Voting and Policy Implications Summary Supplemental Screening for Women with Dense Breast Tissue December 13, 2013 The last CEPAC meeting addressed the comparative clinical effectiveness and value
Breast Cancer Update Michael B. Peyser MS MD FACS Fellow Society of Surgical Oncology Windsong Breast Care
 Breast Cancer Update 2017 Michael B. Peyser MS MD FACS Fellow Society of Surgical Oncology Windsong Breast Care Used with permission by Anna Chen MD, Windsong Radiology Group Statistics as of 2013 230,815
Breast Cancer Update 2017 Michael B. Peyser MS MD FACS Fellow Society of Surgical Oncology Windsong Breast Care Used with permission by Anna Chen MD, Windsong Radiology Group Statistics as of 2013 230,815
Page 1. Selected Controversies. Cancer Screening! Selected Controversies. Breast Cancer Screening. ! Using Best Evidence to Guide Practice!
 Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening I have no conflicts of interest. Principles of screening. Cancer in the World Page 1. Letting Evidence Be Our Guide
 Cancer Screening 2012 Letting Evidence Be Our Guide Jeffrey A. Tice, MD Division of General Internal Medicine University of California, San Francisco I have no conflicts of interest Principles of screening
Cancer Screening 2012 Letting Evidence Be Our Guide Jeffrey A. Tice, MD Division of General Internal Medicine University of California, San Francisco I have no conflicts of interest Principles of screening
Cancer Screening: Controversial Topics 10/27/17. Vijay Kudithipudi, MD Kettering Cancer Care Radiation Oncology
 Cancer Screening: Controversial Topics 10/27/17 Vijay Kudithipudi, MD Kettering Cancer Care Radiation Oncology Meet the Radiation Oncologists E Ronald Hale, MD, MPH Matthew Knecht, MD Anthony Paravati,
Cancer Screening: Controversial Topics 10/27/17 Vijay Kudithipudi, MD Kettering Cancer Care Radiation Oncology Meet the Radiation Oncologists E Ronald Hale, MD, MPH Matthew Knecht, MD Anthony Paravati,
U.S. Preventive Services Task Force: Draft Prostate Cancer Screening Recommendation (April 2017)
") 1 U.S. Preventive Services Task Force: Draft Prostate Cancer Screening Recommendation (April 2017) Alex Krist MD MPH Professor and Director of Research Department of Family Medicine and Population Health
1 U.S. Preventive Services Task Force: Draft Prostate Cancer Screening Recommendation (April 2017) Alex Krist MD MPH Professor and Director of Research Department of Family Medicine and Population Health
2018 CMS Web Interface
 CMS Web Interface PREV-5 (NQF 2372): Breast Cancer Screening Measure Steward: NCQA CMS Web Interface V2.1 Page 1 of 18 06/25/ Contents INTRODUCTION... 3 CMS WEB INTERFACE SAMPLING INFORMATION... 4 BENEFICIARY
CMS Web Interface PREV-5 (NQF 2372): Breast Cancer Screening Measure Steward: NCQA CMS Web Interface V2.1 Page 1 of 18 06/25/ Contents INTRODUCTION... 3 CMS WEB INTERFACE SAMPLING INFORMATION... 4 BENEFICIARY
Dense Breasts, Over-diagnosis, Screening Guideline Controversies & Genetic Risk Stratification The Road to Customized Care
 Dense Breasts, Over-diagnosis, Screening Guideline Controversies & Genetic Risk Stratification The Road to Customized Care Jason Cord, M.D. SCPMG Regional Chief of Breast Imaging PIC for Breast Imaging,
Dense Breasts, Over-diagnosis, Screening Guideline Controversies & Genetic Risk Stratification The Road to Customized Care Jason Cord, M.D. SCPMG Regional Chief of Breast Imaging PIC for Breast Imaging,
Breast Cancer Screening
 Breast Cancer Screening October 7, 2011 Donna Fitzpatrick-Lewis, Nicole Hodgson, Donna Ciliska, Leslea Peirson, Mary Gauld, Yan Yun Liu McMaster University Hamilton, Ontario, Canada CTFPHC Leads: Marcello
Breast Cancer Screening October 7, 2011 Donna Fitzpatrick-Lewis, Nicole Hodgson, Donna Ciliska, Leslea Peirson, Mary Gauld, Yan Yun Liu McMaster University Hamilton, Ontario, Canada CTFPHC Leads: Marcello
Mammography Screening: A New Estimate of Number Needed to Screen to Prevent One Breast Cancer Death
 Women s Imaging Original Research Hendrick and Helvie Mammography Screening Women s Imaging Original Research R. Edward Hendrick 1 Mark A. Helvie 2 Hendrick RE, Helvie MA Keywords: mammography screening,
Women s Imaging Original Research Hendrick and Helvie Mammography Screening Women s Imaging Original Research R. Edward Hendrick 1 Mark A. Helvie 2 Hendrick RE, Helvie MA Keywords: mammography screening,
GENERAL COMMENTS. The Task Force Process Should be Fully Open, Balanced and Transparent
 December 9, 2013 Submitted Electronically United States Preventive Services Task Force c/o Dr. Robert Cosby Agency for Healthcare Research and Quality 540 Gaither Road Rockville, MD 20850 RE: USPSTF Draft
December 9, 2013 Submitted Electronically United States Preventive Services Task Force c/o Dr. Robert Cosby Agency for Healthcare Research and Quality 540 Gaither Road Rockville, MD 20850 RE: USPSTF Draft
IL Balance Sheet dei programmi di screening mammografici dell Unione Europea
 Seminario di studio LA SORVEGLIANZA EPIDEMIOLOGICA DELLO SCREENING DEI TUMORI DELLA MAMMELLA NELLA REGIONE EMILIA-ROMAGNA Bologna, 18 marzo 2013 IL Balance Sheet dei programmi di screening mammografici
Seminario di studio LA SORVEGLIANZA EPIDEMIOLOGICA DELLO SCREENING DEI TUMORI DELLA MAMMELLA NELLA REGIONE EMILIA-ROMAGNA Bologna, 18 marzo 2013 IL Balance Sheet dei programmi di screening mammografici
Steven Jubelirer, MD Clinical Professor Medicine WVU Charleston Division Senior Research Scientist CAMC Research Institute
 Steven Jubelirer, MD Clinical Professor Medicine WVU Charleston Division Senior Research Scientist CAMC Research Institute Objectives Develop a systematic way to think about benefits and harms of cancer
Steven Jubelirer, MD Clinical Professor Medicine WVU Charleston Division Senior Research Scientist CAMC Research Institute Objectives Develop a systematic way to think about benefits and harms of cancer
REPORT 6 OF THE COUNCIL ON SCIENCE AND PUBLIC HEALTH (A-12) Screening Mammography (Resolution 509-A-10, Resolve 1) (Reference Committee E)
 Screening Mammography (Resolution 509-A-10, Resolve 1) (Reference Committee E)") REPORT 6 OF THE COUNCIL ON SCIENCE AND PUBLIC HEALTH (A-) Screening Mammography (Resolution 509-A-0, Resolve ) (Reference Committee E) EXECUTIVE SUMMARY Objectives. In November 009, the United States Preventive
REPORT 6 OF THE COUNCIL ON SCIENCE AND PUBLIC HEALTH (A-) Screening Mammography (Resolution 509-A-0, Resolve ) (Reference Committee E) EXECUTIVE SUMMARY Objectives. In November 009, the United States Preventive
BREAST CANCER SCREENING IS A CHOICE
 BREAST CANCER SCREENING IS A CHOICE by ELAINE SCHATTNER, MD no financial disclosures (ES) American Association for Cancer Research Typical headlines focus on controversy 2 Data: Breast Cancer Incidence
BREAST CANCER SCREENING IS A CHOICE by ELAINE SCHATTNER, MD no financial disclosures (ES) American Association for Cancer Research Typical headlines focus on controversy 2 Data: Breast Cancer Incidence
Cancer Screening 2014
 Thomas Jefferson University Jefferson Digital Commons Department of Family & Community Medicine Presentations and Grand Rounds Department of Family & Community Medicine 4-11-2014 Cancer Screening 2014
Thomas Jefferson University Jefferson Digital Commons Department of Family & Community Medicine Presentations and Grand Rounds Department of Family & Community Medicine 4-11-2014 Cancer Screening 2014
Why study changes in breast cancer rates over time? How did we study these changes in breast cancer rates?
 Breast Cancer Trends in Hong Kong: What are the Implications for Screening, Diagnosis and Management in All Chinese Women? GM Leung, TH Lam, TQ Thach, AJ Hedley Department of Community Medicine, HKU W
Breast Cancer Trends in Hong Kong: What are the Implications for Screening, Diagnosis and Management in All Chinese Women? GM Leung, TH Lam, TQ Thach, AJ Hedley Department of Community Medicine, HKU W
Selected Controversies. Cancer Screening. Breast Cancer Screening. Selected Controversies. Page 1. Using Best Evidence to Guide Practice
 Cancer Screening Using Best Evidence to Guide Practice Judith M.E. Walsh, MD, MH Division of General Internal Medicine Women s Health Center of Excellence University of California, San Francisco Selected
Cancer Screening Using Best Evidence to Guide Practice Judith M.E. Walsh, MD, MH Division of General Internal Medicine Women s Health Center of Excellence University of California, San Francisco Selected
Cancer Screening 2009: New Tests, New Choices
 Objectives Cancer Screening 2009: New Tests, New Choices UCSF Annual Review in Family Medicine April 21, 2009 Michael B. Potter, MD Professor, Clinical Family and Community Medicine UCSF School of Medicine
Objectives Cancer Screening 2009: New Tests, New Choices UCSF Annual Review in Family Medicine April 21, 2009 Michael B. Potter, MD Professor, Clinical Family and Community Medicine UCSF School of Medicine
2019 CMS Web Interface
 CMS Web Interface PREV-5 (NQF 2372): Breast Cancer Screening Measure Steward: NCQA CMS Web Interface V3.0 Page 1 of 18 xx/xx/2018 Contents INTRODUCTION... 3 CMS WEB INTERFACE SAMPLING INFORMATION... 4
CMS Web Interface PREV-5 (NQF 2372): Breast Cancer Screening Measure Steward: NCQA CMS Web Interface V3.0 Page 1 of 18 xx/xx/2018 Contents INTRODUCTION... 3 CMS WEB INTERFACE SAMPLING INFORMATION... 4
Screening Mammography as an example of Access to Healthcare A starting point for safe affordable medical treatment. Prof C A Benn
 Screening Mammography as an example of Access to Healthcare A starting point for safe affordable medical treatment Prof C A Benn to screen or not to screen may be To be or not the to be question? re national
Screening Mammography as an example of Access to Healthcare A starting point for safe affordable medical treatment Prof C A Benn to screen or not to screen may be To be or not the to be question? re national
DESCRIPTION: Percentage of final reports for screening mammograms that are classified as probably benign
 Quality ID #146 (NQF 0508): Radiology: Inappropriate Use of Probably Benign Assessment Category in Screening Mammograms National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS F INDIVIDUAL
Quality ID #146 (NQF 0508): Radiology: Inappropriate Use of Probably Benign Assessment Category in Screening Mammograms National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS F INDIVIDUAL
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Epidemiologic Methods for Evaluating Screening Programs. Rosa M. Crum, MD, MHS Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Running head: BREAST CANCER SCREENING 1
 Running head: BREAST CANCER SCREENING 1 Breast Cancer Screening Carol A. Lamoureux-Lewallen Briar Cliff University BREAST CANCER SCREENING 2 Breast Cancer Screening Policy Problem The federally appointed
Running head: BREAST CANCER SCREENING 1 Breast Cancer Screening Carol A. Lamoureux-Lewallen Briar Cliff University BREAST CANCER SCREENING 2 Breast Cancer Screening Policy Problem The federally appointed
6. SUMMARY. 6.1 Breast cancer
 6. SUMMARY 6.1 Breast cancer Breast cancer is the most commonly diagnosed cancer in women and the most common cause of cancer death in women worldwide. Globally, it is estimated that in 2012 there were
6. SUMMARY 6.1 Breast cancer Breast cancer is the most commonly diagnosed cancer in women and the most common cause of cancer death in women worldwide. Globally, it is estimated that in 2012 there were
Systematic Review of Cancer Screening Literature for Updating American Cancer Society Breast Cancer Screening Guidelines
 Systematic Review of Cancer Screening Literature for Updating American Cancer Society Breast Cancer Screening Guidelines Prepared for: American Cancer Society, Inc. 250 Williams Street Atlanta, GA 30303
Systematic Review of Cancer Screening Literature for Updating American Cancer Society Breast Cancer Screening Guidelines Prepared for: American Cancer Society, Inc. 250 Williams Street Atlanta, GA 30303
Breast Imaging! Ravi Adhikary, MD!
 Breast Imaging! Ravi Adhikary, MD! ACS Estimated Cancers Statistics 2014! Breast! New Cases in Women! 232,670 (+67,570 in situ)! Deaths in Women! 40,000! Colon! 48,380! 24,040! Cervical! 12,360! 4,020!
Breast Imaging! Ravi Adhikary, MD! ACS Estimated Cancers Statistics 2014! Breast! New Cases in Women! 232,670 (+67,570 in situ)! Deaths in Women! 40,000! Colon! 48,380! 24,040! Cervical! 12,360! 4,020!
SHARED DECISION MAKING FOR PROSTATE CANCER SCREENING
 SHARED DECISION MAKING FOR PROSTATE CANCER SCREENING 16 TH A N N U A L M A S S A C H U S E T T S P R O S T A T E C A N C E R S Y M P O S I U M Mary McNaughton-Collins, MD, MPH Foundation Medical Director
SHARED DECISION MAKING FOR PROSTATE CANCER SCREENING 16 TH A N N U A L M A S S A C H U S E T T S P R O S T A T E C A N C E R S Y M P O S I U M Mary McNaughton-Collins, MD, MPH Foundation Medical Director
North American Menopause Society (NAMS)
") North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
North American Menopause Society (NAMS) 2012 Hormone Therapy Position Statement Cynthia B. Evans, MD Assistant Professor-Clinical Department of Obstetrics and Gynecology The Ohio State University College
Objectives. I have no financial interests in any product I will discuss today. Cervical Cancer Screening Guidelines: Updates and Controversies
 Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
A senior s guide for preventative healthcare services Ynolde F. Smith D.O.
 A senior s guide for preventative healthcare services Ynolde F. Smith D.O. What can we do to prevent disease? Exercise Eating Well Keep a healthy weight Injury prevention Mental Health Social issues (care
A senior s guide for preventative healthcare services Ynolde F. Smith D.O. What can we do to prevent disease? Exercise Eating Well Keep a healthy weight Injury prevention Mental Health Social issues (care
DESCRIPTION: Percentage of final reports for screening mammograms that are classified as probably benign
 Measure #146 (NQF 0508): Radiology: Inappropriate Use of Probably Benign Assessment Category in Screening Mammograms National Quality Strategy Domain: Efficiency and Cost Reduction 2016 PQRS OPTIONS F
Measure #146 (NQF 0508): Radiology: Inappropriate Use of Probably Benign Assessment Category in Screening Mammograms National Quality Strategy Domain: Efficiency and Cost Reduction 2016 PQRS OPTIONS F
Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program
 Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program A B C D USPSTF recommends the service. There is high certainty that Offer or provide
Camelia Davtyan, MD, FACP Clinical Professor of Medicine Director of Women s Health UCLA Comprehensive Health Program A B C D USPSTF recommends the service. There is high certainty that Offer or provide
The Northern Ireland breast screening programme
 The Northern Ireland breast screening programme Guide for health professionals The HSC offers breast screening to reduce the number of women who die from breast cancer. Breast cancer is the second most
The Northern Ireland breast screening programme Guide for health professionals The HSC offers breast screening to reduce the number of women who die from breast cancer. Breast cancer is the second most
Cancer Treatment Centers of America: Supercharge Your Knowledge: A Focus on Breast, Cervical and Prostate Screening Guidelines and Controversies
 8 ACOFP 55th Annual Convention & Scientific Seminars Cancer Treatment Centers of America: Supercharge Your Knowledge: A Focus on Breast, Cervical and Prostate Screening Guidelines and Controversies Anthony
8 ACOFP 55th Annual Convention & Scientific Seminars Cancer Treatment Centers of America: Supercharge Your Knowledge: A Focus on Breast, Cervical and Prostate Screening Guidelines and Controversies Anthony
I have no financial interests in any product I will discuss today.
 Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
The status of Lung Cancer Screening Guidelines. Peter B. Bach, MD, MAPP Memorial Sloan Kettering Cancer Center
 The status of Lung Cancer Screening Guidelines Peter B. Bach, MD, MAPP Memorial Sloan Kettering Cancer Center bachp@mskcc.org @peterbachmd Homogeneity of guidelines But what about these? Outside the box
The status of Lung Cancer Screening Guidelines Peter B. Bach, MD, MAPP Memorial Sloan Kettering Cancer Center bachp@mskcc.org @peterbachmd Homogeneity of guidelines But what about these? Outside the box
Guidelines for Breast, Cervical and Colorectal Cancer Screening
 Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
TMIST: Frequently Asked Questions
 TMIST: Frequently Asked Questions Key Topics for Site Investigators and Staff This document answers frequently asked questions about the Tomosynthesis Mammographic Imaging Screening Trial (TMIST/EA1151);
TMIST: Frequently Asked Questions Key Topics for Site Investigators and Staff This document answers frequently asked questions about the Tomosynthesis Mammographic Imaging Screening Trial (TMIST/EA1151);
MethodologicOverview of Screening Studies
 MethodologicOverview of Screening Studies Diana L. Miglioretti, PhD University of California Davis Thanks to William Black, MD for many of these slides! 1/11/17 RSNA CTMW 2017 1 Learning Objectives Understand
MethodologicOverview of Screening Studies Diana L. Miglioretti, PhD University of California Davis Thanks to William Black, MD for many of these slides! 1/11/17 RSNA CTMW 2017 1 Learning Objectives Understand
Breast Cancer Screening
 Breast Cancer Screening Ravinder S. Legha 1, Jessica Wai Ting Leung After skin cancer, breast cancer is the cancer most diagnosed in U.S. women and has the second highest death rate. Breast cancer will
Breast Cancer Screening Ravinder S. Legha 1, Jessica Wai Ting Leung After skin cancer, breast cancer is the cancer most diagnosed in U.S. women and has the second highest death rate. Breast cancer will
Rethinking Breast Cancer Screening
 Rethinking Breast Cancer Screening NAMS Meeting, October, 2014 Russell Harris, MD, MPH University of North Carolina, Chapel Hill Conflicts of Interest Financial: none Intellectual: I have been researching
Rethinking Breast Cancer Screening NAMS Meeting, October, 2014 Russell Harris, MD, MPH University of North Carolina, Chapel Hill Conflicts of Interest Financial: none Intellectual: I have been researching
United States Preventive Services Task Force Screening Mammography Recommendations: Science Ignored
 Women s Imaging Perspective Hendrick and Helvie Mammography Screening Recommendations Women s Imaging Perspective FOCUS ON: R. Edward Hendrick 1 Mark A. Helvie 2 Hendrick RE, Helvie MA Keywords: breast,
Women s Imaging Perspective Hendrick and Helvie Mammography Screening Recommendations Women s Imaging Perspective FOCUS ON: R. Edward Hendrick 1 Mark A. Helvie 2 Hendrick RE, Helvie MA Keywords: breast,
RALOXIFENE Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA Is the request for the prevention (risk reduction) of breast cancer?
 of breast cancer?") Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA 16917 GUIDELINES FOR USE 1. Is the request for the prevention (risk reduction) of breast cancer? If yes, continue to #2. If no, approve by HICL
Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA 16917 GUIDELINES FOR USE 1. Is the request for the prevention (risk reduction) of breast cancer? If yes, continue to #2. If no, approve by HICL
CLINICAL GUIDELINES. Screening Mammography Guidelines
 CLINICAL GUIDELINES Screening Mammography Guidelines Paula George, M.D. and C. Todd Cunningham, M.D., Karen F. Goodhope, M.D., Valerie C. Reichert, M.D. Hayley Sheldon, M.D., Michelle Walters, D.O. 2/17/2016
CLINICAL GUIDELINES Screening Mammography Guidelines Paula George, M.D. and C. Todd Cunningham, M.D., Karen F. Goodhope, M.D., Valerie C. Reichert, M.D. Hayley Sheldon, M.D., Michelle Walters, D.O. 2/17/2016
Disclosures. Overview. Selection the most accurate statement: Updates in Lung Cancer Screening 5/26/17. No Financial Disclosures
 Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional
Updates in Lung Cancer Screening Disclosures No Financial Disclosures Neil Trivedi, MD Associate Professor of Clinical Medicine SF VAMC Pulmonary and Critical Care Director, Bronchoscopy & Interventional