Management of castration resistant prostate cancer after first line hormonal therapy fails
|
|
|
- Justin Tate
- 6 years ago
- Views:
Transcription

1 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton
2 WHAT ARE THE AIMS OF TREATMENT?
3 Cure?
4 Nothing I will discuss today will cure anyone. We need to remember to mention this to our patients.
5 Other aims that matter to our patients Prolonged survival Improved quality of life Reduction in pain Reduction in skeletal related events Time to do things Improved progression free survival Reduction in PSA
6 GENERAL OPTIONS FOR TREATMENT
7 Metastatic prostate cancer 2010 Pre-docetaxel Docetaxel Post-docetaxel Other hormonal e.g. steroids, stilboestrol, ketoconazole Testosterone suppression e.g. LHRHa 2 nd line hormonal e.g. bicalutamide Docetaxel Docetaxel retreat Mitoxantrone Other chemo Zoledronate Clodronate
8 Metastatic prostate cancer 2012 Pre-docetaxel Docetaxel Post-docetaxel Other hormonal e.g. steroids, stilboestrol, ketoconazole Abiraterone Testosterone suppression e.g. LHRHa 2 nd line hormonal e.g. bicalutamide Docetaxel Cabazitaxel MDV3100? Sipuleucel T Alpharadin Zoledronate Clodronate Denosumab
9 Metastatic prostate cancer 2013 Pre-docetaxel Docetaxel Post-docetaxel Testosterone suppression e.g. LHRHa Other hormonal e.g. steroids, stilboestrol, ketoconazole? 2 nd line hormonal e.g. bicalutamide? Docetaxel Abiraterone Cabazitaxel MDV3100? Sipuleucel T Alpharadin Abiraterone Zoledronate Clodronate Denosumab
10 A BIT OF BIOLOGY
11 Androgen Receptor Central mediator of male reproductive function and development (also impacts on bone, skin, muscle, brain ) Nuclear hormone receptor 5α-dihydrotestosterone >>> testosterone Involved in all stages of prostate cancer
12
13
14
15
16 Potential post ADT mechanisms AR becomes promiscuous AR gets over-expressed Cancer cells make their own androgens AR mutates to become active without hormone Other signalling pathways activate abnormally Other


17 Persistent Androgen Signaling in CRPC With Bone Metastases AR CYP17 Efstathiou JCO 2012

18 Rubin JCO 2011
19 Biology conclusions Prostate cancer is driven by abnormal hormone signalling by androgens This is the case in virtually all stages of the disease pathway Hormonal therapy is central to this disease as a result Other signalling pathways are coming into focus with potential therapeutic implications
20 PATIENT SELECTION
21 Treatment selection Performance status PSA PSA velocity Clinical velocity Metastatic sites Prior therapy Response to prior therapy Small cell/neuroendocrine differentiation Co-morbidities Drug access? Age???
22 Treatment selection Performance status PSA PSA velocity Clinical velocity Metastatic sites Prior therapy Response to prior therapy Small cell/neuroendocrine differentiation Co-morbidities Drug access? Age??? Patient choice
23 Treatment selection Performance status PSA PSA velocity Clinical velocity Metastatic sites Prior therapy Response to prior therapy Small choice? cell/neuroendocrine differentiation Co-morbidities Drug access? Age??? Patient s wife s
24 Clever breast cancer treatment HER2 +ve ER/PR +ve Host Factors ER/PR/HER2 -ve Clinical Staging Treatment pathway HER2 Treatment pathway ER/PR Treatment pathway triple negative
25 Less clever prostate cancer treatment Host Factors AR +ve Clinical Staging Treatment pathway AR
26 Best supportive care (alone) is always a treatment option.
27 Should we treat M0 disease that is biochemically progressive through ADT? There is no evidence that doing this is of value. But we do it a lot. We should test this in clinical trials.
28 Patient selection conclusions Treatment selection is primarily driven by clinical factors We cant generally select by biology (yet) Selection strategies are perhaps our key research need When to treat in M0 disease is unclear
29 SECOND LINE HORMONAL THERAPY (OLD DRUGS)
30 Second line hormone therapies ADT effective for ~1-3 years on average No survival or QOL advantage proven for any conventional (i.e. older) second line agents Addition of an anti-androgen is standard e.g. bicalutamide, flutamide, nilutamide Other old options stilboestrol, ketoconazole, low dose steroids
31 Bicalutamide post ADT (+/- F) PSA response rate (>50%) = 22.5% No QOL data Joyce et al, J Urol, 1998
 No")
32 Kassouf et al, J Urol, 2003 Nilutamide post ADT (+/- F or B) No QOL data
33 Flutamide v prednisone post ADT QOL data favoured prednisone Fossa et al, JCO, 2001
34 Anti-androgen withdrawal response 210 patients 64% flutamide 32% bicalutamide 3% nilutamide 21% had confirmed PSA decrease > 50% No radiographic responses Median PFS 3 months (19% >12) Longer anti-androgen use predicted PSA response No QOL data Sartor et al, Cancer, 2008

35 Ketoconazole PSA-PFS Survival No QOL data Small et al, JCO, 2004
36 Stilboestrol No QOL difference Shamash et al, BJC, 2011
37 Second line hormones conclusions No survival or QOL benefit (other than prednisone> flutamide) 2 nd line anti-androgen ( MAB ) is standard (but not-evidence based) None of this would not be approved today Some patients probably do benefit!
38 CHEMOTHERAPY

39 Mitoxantrone No OS benefit Kantoff et al, JCO, 1999


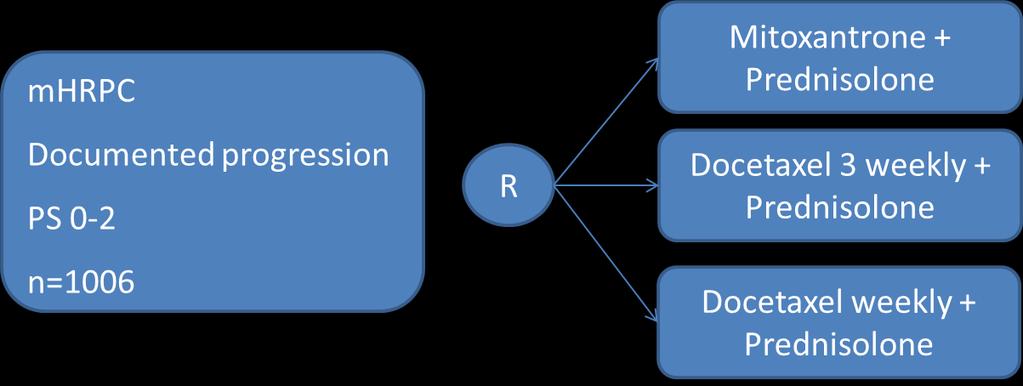
40 Docetaxel Tannock et al, NEJM, 2004
41 Docetaxel Median survival D months D months M 16.3 months Improvements also seen in: QOL Pain PSA response Berthold et al, JCO, 2008 Tannock et al, NEJM, 2004

42 Docetaxel Tannock et al, NEJM, 2004



43 Cabazitaxel Semi-synthetic taxane Anti-tumour activity in models resistant to paclitaxel and docetaxel De Bono et al, Lancet, 2010
44 Cabazitaxel Median OS 15 1 (95% CI ) v 12 7 months ( ) Median PFS 2 8 (95% CI ) v 1 4 months ( ) De Bono et al, Lancet, 2010

45 No QOL data in this trial De Bono et al, Lancet, 2010

46 De Bono et al, Lancet, 2010

47 Causes of death De Bono et al, Lancet, 2010
48 Chemotherapy conclusions Docetaxel remains the first line standard of care Only viable in about 50% of patients Modest improvement in survival Cabazitaxel now 2 nd line standard for chemotherapy Predictors of toxicity and benefit required Unclear how to sequence with new drugs
49 NEW HORMONAL THERAPIES

50 Steroid Hormone Synthesis Attard, G. et al. J Clin Oncol; 26:

51 Abiraterone Mechanism Attard, G. et al. J Clin Oncol; 26:

52 Phase II abiraterone PSA responses Not everyone benefits BUT this is CRPC after chemo! Attard, G. et al. J Clin Oncol; 26:
53 COU-AA-301 design mcrpc Disease progression 2 Abiraterone + prednisone 1-2 prior chemo regimes Castrate PS 0-2 n=1195 R 1 Placebo + prednisone de Bono et al, NEJM 2011

54 COU-AA-301 survival outcome de Bono et al, NEJM 2011

55 de Bono et al, NEJM 2011
56 COU-AA-302 Ryan et al, NEJM, 2012

57 COU-AA-302 Ryan et al, NEJM, 2012
58 AFFIRM design mcrpc Disease progression 2 Enzalutamide 1 or more prior chemo regimes Castrate PS 0-2 n=1199 R 1 Placebo Scher et al, NEJM 2012
59 Enzalutamide (MDV3100) 18.4 v 13.6 months QOL benefit also seen Scher et al, NEJM 2012

60 Enzalutamide (MDV3100) Scher et al, NEJM 2012
61 New hormonal therapy conclusions Abiraterone and enzalutamide prove AR signalling remains critical throughout Relatively easy treatments We don t know when best to use them Predictors of benefit required
62 IMMUNOTHERAPY
63 Sipuleucel T P = HR0.775 Median survival 25.8 v 21.7 months
64 Sipuleucel conclusions Proves immunotherapy can work Probably in minimally symptomatic patients without visceral disease Minimal toxicity An irrelevance in the UK? - $93000
65 RADIO-PHARMACEUTICALS
66 Radionuclides Strontium 89 Samarium 153 Rhenium 186 Alpharadin

67 Periodic table
68 Alpharadin HR = % CI, 0.581, P = % Placebo, n = 307 Median OS: 11.3 months Radium-223, n = 614 Median OS: 14.9 months 0 Month Radium Placebo Vogelzang, J Clin Oncol 31, 2013 (suppl 6; abstr 11)
69 Alphardin Improvements also seen in QOL Time to first SRE Generally good toxicity profile
70 BONE DIRECTED THERAPIES
71 Bisphosphonates Inhibitors of osteoclasts and therefore bone re-absorption Used in osteoporosis with proven benefit Used to treat malignant hypercalcaemia Used for malignant bone pain Investigated in a variety of solid malignancies including prostate
72 Clodronate PR with mets on ADT Clodronate vs placebo 3yrs PR non-mets RT/ADT/both Clodronate vs placebo 5yrs Dearnaley et al, Lancet Oncology 2009
73 Zoledronate Skeletal-related events: pathologic bone fractures spinal cord compression surgery to bone radiation therapy to bone antineoplastic therapy to treat bone pain No QOL difference Saad et al, JNCI 2002
74 Denosumab v Zoledroante in bony mcrpc time to first on-study skeletal related event: pathological fracture radiation therapy surgery to bone spinal cord compression No QOL difference Fizazi et al, Lancet, 2011
75 Trapeze
76 Case history 64 year old retired engineer LUTS No PMH, no other medications PSA 12, abnormal DRE TRUS biopsies: Gleason 9 (4+5), vascular invasion No small cell or neuro-endocrine elements MRI pelvis/bone scan: T2c N0 M0 Radical prostatectomy Tumour fixed to rectum Final pathology showed seminal vesicle involvement and extra-prostatic spread
77 Case history Swift biochemical progression (months) PSA rose from 7 to 13 Pelvic MRI lymphadenopathy and bone metastases Commenced CAB (goserelin and bicalutamide) 4 months later PSA 16 PS=0 Referred for further palliative systemic therapy Clinically well Restaged: minor increase in pelvic lymphadenopathy and bony metastases PSA 19 Left hip pain, moderate severity but patient remained active PS=1 Stopped bicalutamide
78 Treatment options Observation Dexamethasone Stilboestrol Abiraterone Docetaxel chemotherapy Ketoconazole Sipuleucel T Other

79 Outcome PS=0 Pain free (never had RT to hip) Reduction in lymphadenopathy Sclerotic change in bony disease Transient BP rise
80 EXPERIMENTAL APPROACHES
 67% pain improvement Smith, JCO,")
81 Cabozantinib (XL184) Oral cmet and VEGFR2 inhibitor Phase II At 12 weeks, DCR=80% 72% soft tissue response rate 68% bone scan response rate (12%CR) 67% pain improvement Smith, JCO, 2013
82 Ipilimumab Lenalidamide VEGF-Trap PI3K/AKT inhibitors Src inhibitors Dasatinib Saracatinib Sunitinib Others in testing
83 DRUG ACCESS
84 Drug Access early 2013 Pre-docetaxel Docetaxel Post-docetaxel Routinely available Other hormonal e.g. steroids, stilboestrol, ketoconazole NICE approved NICE approved Abiraterone Testosterone suppression e.g. LHRHa 2 nd line hormonal e.g. bicalutamide Docetaxel Cabazitaxel MDV3100? Sipuleucel T Alpharadin Abiraterone Zoledronate Clodronate Denosumab
85 Drug Access early 2013 Pre-docetaxel Docetaxel Post-docetaxel Other hormonal e.g. steroids, stilboestrol, ketoconazole CDF (for some) (NICE rejected) Abiraterone Testosterone suppression e.g. LHRHa 2 nd line hormonal e.g. bicalutamide Docetaxel Cabazitaxel MDV3100? Sipuleucel T Alpharadin CDF (for some) (NICE in progress) Abiraterone Access for some (NICE rejected) Zoledronate Clodronate Denosumab
86 Drug Access early 2013 Pre-docetaxel Docetaxel Post-docetaxel Other hormonal e.g. steroids, stilboestrol, ketoconazole Licence 2013 (EAP) Abiraterone Testosterone suppression e.g. LHRHa 2 nd line hormonal e.g. bicalutamide Docetaxel Cabazitaxel MDV3100 Sipuleucel T Alpharadin Abiraterone Licence 2013 (EAP) Zoledronate Clodronate Denosumab
87 Metastatic prostate cancer 2013 Pre-docetaxel Docetaxel Post-docetaxel Other hormonal e.g. steroids, stilboestrol, ketoconazole Abiraterone Testosterone suppression e.g. LHRHa 2 nd line hormonal e.g. bicalutamide Docetaxel Cabazitaxel MDV3100 Sipuleucel T Alpharadin Abiraterone No chance! Zoledronate Clodronate Denosumab
88 General conclusions Major changes in treatment options have and are occurring Sequencing remains unclear Treatment selection strategies urgently needed Access remains an issue for many Further research needed
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC
 Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
Hormonal Manipulations in CRPC. NW Clarke Professor of Urological Oncology Manchester UK
 Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Elderly men with prostate cancer + ADT
 Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Until 2004, CRPC was consistently a rapidly lethal disease.
 Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Prostate Cancer: Vision of the Future By: H.R.Jalalian
 1 H. R. Jalalian Hematologist&Oncologist Baqiyatallah University of Medical Sciences 2 State of the art: vision on the future Diagnosis Surgery Radiotherapy Medical Oncology 3 Early Detection PSA sensitivity
1 H. R. Jalalian Hematologist&Oncologist Baqiyatallah University of Medical Sciences 2 State of the art: vision on the future Diagnosis Surgery Radiotherapy Medical Oncology 3 Early Detection PSA sensitivity
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
Bone-targeted therapies for prostate cancer in Institut Gustave Roussy Villejuif, France
 Bone-targeted therapies for prostate cancer in 2012 Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards or speaker for: Amgen, Astellas-Medivation,
Bone-targeted therapies for prostate cancer in 2012 Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards or speaker for: Amgen, Astellas-Medivation,
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey
 Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Management of castrate resistant disease; after first line hormone therapy fails
 Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Castrate-resistant prostate cancer: Bone-targeted agents. Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Castrate-resistant prostate cancer: Bone-targeted agents Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for: Amgen, Astellas,
Castrate-resistant prostate cancer: Bone-targeted agents Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for: Amgen, Astellas,
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Management Options in Advanced Prostate Cancer: What is the Role for Sipuleucel-T?
 Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Treatment of Prostate cancer and why I refuse to know my PSA. Outline of Presentation
 Treatment of Prostate cancer and why I refuse to know my PSA Ian F Tannock MD, PhD, DSc Princess Margaret Hospital and University of Toronto Outline of Presentation 1. Requirements for screening to be
Treatment of Prostate cancer and why I refuse to know my PSA Ian F Tannock MD, PhD, DSc Princess Margaret Hospital and University of Toronto Outline of Presentation 1. Requirements for screening to be
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy).
.") Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT
![Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT](/thumbs/71/65630457.jpg "Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT") Evolution of Treatment Options for Patients with and Bone Metastases Trials of Treatments for Castration-Resistant Prostrate Cancer Mentioned in This Review Bisphosphonates (Zometa) 4 mg IV 8 mg IV ( to
Evolution of Treatment Options for Patients with and Bone Metastases Trials of Treatments for Castration-Resistant Prostrate Cancer Mentioned in This Review Bisphosphonates (Zometa) 4 mg IV 8 mg IV ( to
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc
 SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
Board Review 2017: Prostate Cancer. Dana Rathkopf, MD Associate Attending
 Board Review 2017: Prostate Cancer Dana Rathkopf, MD Associate Attending www.mskcc.org The Paradox of Prostate Cancer High prevalence in the general population: over diagnosis of clinically insignificant
Board Review 2017: Prostate Cancer Dana Rathkopf, MD Associate Attending www.mskcc.org The Paradox of Prostate Cancer High prevalence in the general population: over diagnosis of clinically insignificant
American Urological Association (AUA) Guideline
 Guideline") 1 Approved by the AUA Board of Directors April 2014 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2014 by the American Urological
1 Approved by the AUA Board of Directors April 2014 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2014 by the American Urological
8/31/ ) Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases
 Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases") Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223
 SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC
 Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Management of mcrpc: Hormonal therapy and treatment sequence for CRPC Professor Bertrand Tombal, MD, PhD Cliniques universitaires Saint-Luc Université catholique de Louvain Brussels, Belgium Credentials
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Evolution or revolution in the treatment of prostate cancer
 Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Group Sequential Design: Uses and Abuses
 Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD
 Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD The University of Athens Medical School Dept of Clinical Therapeutics Prostate Cancer Evolution Chemotherapy
Mapping the Complexity of Androgen Signaling In Prostate Cancer Progression Eleni Efstathiou MD PhD The University of Athens Medical School Dept of Clinical Therapeutics Prostate Cancer Evolution Chemotherapy
Castrate resistant prostate cancer: the future of anti-androgens.
 Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Prostate Cancer Update 2017
 Prostate Cancer Update 2017 Arthur L. Burnett, MD, MBA, FACS Patrick C. Walsh Distinguished Professor of Urology The James Buchanan Brady Urological Institute The Johns Hopkins Medical Institutions Baltimore,
Prostate Cancer Update 2017 Arthur L. Burnett, MD, MBA, FACS Patrick C. Walsh Distinguished Professor of Urology The James Buchanan Brady Urological Institute The Johns Hopkins Medical Institutions Baltimore,
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
The management and treatment options for secondary bone disease. Omi Parikh July 2013
 The management and treatment options for secondary bone disease Omi Parikh July 2013 Learning Objectives: The assessment and diagnostic process of patients with suspected bone metastases e.g bone scan,
The management and treatment options for secondary bone disease Omi Parikh July 2013 Learning Objectives: The assessment and diagnostic process of patients with suspected bone metastases e.g bone scan,
NAVIGATING THE mcrpc LANDSCAPE: EXPLORING KEY CLINICAL DECISION POINTS
 NAVIGATING THE mcrpc LANDSCAPE: EXPLORING KEY CLINICAL DECISION POINTS Summary of presentations from the Bayer-supported satellite symposium, held at the European Association of Urology (EAU) Congress,
NAVIGATING THE mcrpc LANDSCAPE: EXPLORING KEY CLINICAL DECISION POINTS Summary of presentations from the Bayer-supported satellite symposium, held at the European Association of Urology (EAU) Congress,
ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS.
 ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS. ÁLVARO PINTO Servicio de Oncología Médica Hospital Universitario La Paz IdiPAZ, Madrid INTRODUCTION High
ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS. ÁLVARO PINTO Servicio de Oncología Médica Hospital Universitario La Paz IdiPAZ, Madrid INTRODUCTION High
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer?
 Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Have we optimized the use of Androgen Receptor pathway targeted drugs in Castrate-Resistant Prostate Cancer? Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to
Navigating Prostate Cancer Therapy. Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA
 Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
New Treatment Options for Prostate Cancer
 New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
Medical Treatments for Prostate Cancer
 Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
American Urological Association (AUA) Guideline
 Guideline") 1 Approved by the AUA Board of Directors May 2018 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2018 by the American Urological
1 Approved by the AUA Board of Directors May 2018 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2018 by the American Urological
- La Terapia Farmacologica -
 XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
XXV Congresso Nazionale AIRO Simposio AIRO-AIMN: Trattamento delle Metastasi Ossee nel Paziente con Tumore della Prostata "Ormonorefrattario": - La Terapia Farmacologica - Sergio Bracarda, Medical Oncology
Bone targeting: bisphosphonates, RANK-ligands and radioisotopes. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Bone targeting: bisphosphonates, RANK-ligands and radioisotopes Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee
Bone targeting: bisphosphonates, RANK-ligands and radioisotopes Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
PCa Commentary. Volume 74 March April 2012
 1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2490 www.seattleprostate.com PCa Commentary Volume 74 March April 2012 CONTENTS 1 AN ALTERNATIVE TO LUPRON 2 MDV3100 Phase III AFFIRM Trial Demonstrates
1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2490 www.seattleprostate.com PCa Commentary Volume 74 March April 2012 CONTENTS 1 AN ALTERNATIVE TO LUPRON 2 MDV3100 Phase III AFFIRM Trial Demonstrates
To treat or not to treat: When to treat! A case presentation
 To treat or not to treat: When to treat! A case presentation Filip Ameye, MD,Phd Universitary Hospitals Leuven, Belgium Departement of Urology Prostate Center A case presentation Pt. 76 y. Mild LUTS (07/1999)
To treat or not to treat: When to treat! A case presentation Filip Ameye, MD,Phd Universitary Hospitals Leuven, Belgium Departement of Urology Prostate Center A case presentation Pt. 76 y. Mild LUTS (07/1999)
Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering
 > Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
> Hormone sensitive prostate cancer To add abiraterone or docetaxel? Dr Lisa Pickering Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Honoraria Scientific
SIMPOSIO. Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico
 SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
SIMPOSIO Radioterapia stereotassica e nuovi farmaci nel tumore e della prostata metastatico Definition of Oligometastatic PCa 1-3 synchronous metastases (bone and/or lymph nodes) 2-5 synchronous metastases
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Sequencing treatment for metastatic prostate cancer
 11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
The Role of the Medical Oncologist in the Treatment of Prostate Cancer. Alireza saadat hematologist and oncologist
 The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist When should you see an oncologist? High risk localized disease Rising PSA after local therapy
The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist When should you see an oncologist? High risk localized disease Rising PSA after local therapy
Con$nuing Care for Your Pa$ents with Metasta$c CRPC
 27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
27 th Annual InternaAonal Prostate Cancer Symposium Update January 26, 2017 Con$nuing Care for Your Pa$ents with Metasta$c CRPC Michael S. Cookson, MD, MMHC Professor and Chair Department of Urology University
Advanced Prostate Cancer. Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options
 Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Advanced Prostate Cancer Searching for Optimal Therapy Sequence and Assessing Emerging Treatment Options Disclaimer This slide deck in its original and unaltered format is for educational purposes and
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Denosumab (AMG 162) for bone metastases from solid tumours and multiple myeloma
 for bone metastases from solid tumours and multiple myeloma") Denosumab (AMG 162) for bone metastases from solid tumours and multiple myeloma September 2008 This technology summary is based on information available at the time of research and a limited literature
Denosumab (AMG 162) for bone metastases from solid tumours and multiple myeloma September 2008 This technology summary is based on information available at the time of research and a limited literature
Patients Living Longer: The Promise of Newer Therapies
 Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Anti-Androgen Therapies for Prostate Cancer: A Focused Review
 Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
ESMO SUMMIT MIDDLE EAST 2018
 ESMO SUMMIT MIDDLE EAST 2018 14 Years of progress in Prostate Cancer Standards of Care and new targets Name Ronald de Wit 6-7 April 2018, Dubai, UAE CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche
ESMO SUMMIT MIDDLE EAST 2018 14 Years of progress in Prostate Cancer Standards of Care and new targets Name Ronald de Wit 6-7 April 2018, Dubai, UAE CONFLICT OF INTEREST DISCLOSURE Sub-title Sanofi Roche
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE. Daan De Maeseneer, Medisch Oncoloog
 PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/