Review Article Redefining Hormone Sensitive Disease in Advanced Prostate Cancer
|
|
|
- Morgan Greene
- 6 years ago
- Views:
Transcription
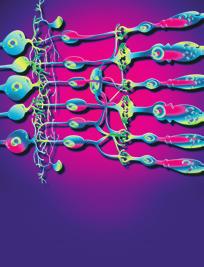
1 Advances in Urology Volume 2012, Article ID , 6 pages doi: /2012/ Review Article Redefining Hormone Sensitive Disease in Advanced Prostate Cancer Xiaoyu Hou and Thomas W. Flaig Division of Medical Oncology, University of Colorado Denver School of Medicine, E. 17th Avenue, Room L , Aurora, CO 80045, USA Correspondence should be addressed to Thomas W. Flaig, thomas.flaig@ucdenver.edu Received 4 August 2011; Accepted 20 December 2011 Academic Editor: Hirotsugu Uemura Copyright 2012 X. Hou and T. W. Flaig. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Prostate cancer is the most common cancer among men in the United States. For decades, the cornerstone of medical treatment for advanced prostate cancer has been hormonal therapy, intended to lower testosterone levels, known as Androgen Deprivation Therapy (ADT). The development of hormone-resistant prostate cancer (now termed castration-resistant prostate cancer:crpc) remains the key roadblock in successful long-term management of prostate cancer. New advancements in medical therapy for prostate cancer have added to the hormonal therapy armamentarium. These new therapeutic agents not only provide a survival benefit but also show potential for reversing hormonal resistance in metastatic CRPC, and thus redefining hormonally sensitive disease. 1. Background Prostate cancer is the 2nd most frequently diagnosed cancer and the 6th leading cause of death among males worldwide [1]. In 2011, it is estimated that there will be 240,890 new cases of prostate cancer and an estimated 33,720 deaths due to prostate cancer in the USA [2]. A variety of primary treatment modalities exist to treat localized cancer of the prostate including surgery, external beam radiation therapy, brachytherapy, cryosurgery, and High Intensity Focused Ultrasound (HIFU). However, for metastatic prostate cancer, the initial treatment has traditionally been hormonal therapy. ADT is effective for 2-3 years on average, and when hormonal therapy fails, chemotherapy provides a survival and palliative benefit, at the cost of considerable side effects. ADT has been given standalone and as an adjunct with other treatment modalities such as chemotherapy, radiation, and surgery [3]. 2. History of Androgen Deprivation Therapy in Prostate Cancer Hormonal therapy has long been an integral part of prostate cancer treatment. In 1811, Scottish surgeon John Hunter ( ) observed the relationship between prostate growth and testicular function for the first time in his textbook Practical Observations on the Treatment of Diseases of the Prostate Gland [4]. Louis Auguste Mercier ( ) of France first performed orchiectomy for the treatment of an enlarged prostate in 1857 [4]. In 1941, Huggins first used estrogen to treat metastatic prostate cancer, which led to a Nobel prize in 1966, representing one of the first successful systemic therapies for cancer [5]. Similar to breast cancer, prostate cancer is a hormonally driven solid malignancy. Androgens are the key driver of growth for both the normal prostate and prostate cancer cells. Vital in the definition of castrate-resistant disease is the recognition of the potential sources of androgen and approaches aimed at the reduction of their levels. While we have historically focused on the testicular production of androgens, other sites of production include the adrenal glands and the more recently appreciated source of intratumoral androgen production. Normally 90 95% of circulating testosterone is produced by the Leydig cells of the testes. Another 5 10% of systemic testosterone is synthesized by the adrenal glands [6]. While production by the testis is the main source of androgen in prostate cancer prior to castration, it has now been appreciated that traditionally
2 2 Advances in Urology defined CRPC is frequently driven by intratumoral androgen production and synthesis of testosterone from weak adrenal androgen precursors [7, 8]. Given the multiple sources and associated biosynthesis pathways of androgen productions, hormonal therapy in prostate cancer is achieved through multiple mechanisms with several different classes of agents (Table 1). Though in limited use today, estrogen was initially used to systematically treat prostate cancer decades ago. Beyond an agent simply to induce a reduction in testosterone levels, Serrate et al. reported in 2009 that diethylstilbestrol (DES) is a reasonable option for salvage therapy for CRPC in patients previously treated with docetaxel chemotherapy, suggesting a direct anticancer effect and larger hormone sensitive treatmentwindow [9]. Surgical orchiectomy remains a viable option to achieve androgen deprivation to this day [10]. Medical castration can be achieved by using gonadotropinreleasing hormone (GnRH) agonists such as goserelin, leuprolide, and histrelin acetate, which induce androgen deprivation through persistent overstimulation and subsequent downregulation at the level of the GnRH receptor [11, 12]. GnRH antagonists such as degarelix can also disrupt androgen production and are a more recent addition to our medical treatment options [13]. Antiandrogens such as bicalutamide, nilutamide, and flutamide block the effect of androgen directly at the androgen receptor, although the blockade of the androgen receptor is incomplete and partial agonist properties are observed with these agents [14]. In contrast, MDV3100 is a new generation antiandrogen with great affinity for the androgen receptor and no known agonist effect [15]. Ketoconazole is a nonspecific inhibitor of cytochrome P450 enzyme-mediated androgen biosynthesis [16]. Glucocorticoids such as prednisone have been used as a palliative agent and likely act by suppressing ACTH secretion and thus reducing adrenal androgen production [17](Figure 1). Common side effects of hormonal therapy in prostate cancer treatment include hot flashes, weight gain, gynecomastia, and osteoporosis [18]. Estrogen additionally has cardiovascular side effects including blood clots [19] and there is also evidence of increased cardiovascular risk with GnRH agonist in this setting [20]. Side effects of ketoconazole include elevated liver transaminases and gastrointestinal complaints [21]. Hormonal therapy can produce dramatic clinical responses when initially used to treat advanced prostate cancer. Unfortunately, prostate cancer patients become resistant to androgen deprivation after about 2-3 years on average with progressive disease, despite castrate levels of testosterone [22, 23]. It is hypothesized that despite reduced androgen levels, one mechanism of resistance is the production of androgen for growth via intratumoral and extragonadal pathways. Other mechanisms of hormonal resistance include upregulation of androgen receptors with increased sensitivity to androgen at the androgen receptors, and mutations of androgen receptors itself [24, 25]. 3. Current Advancement in Hormonal Therapy Historically, a serum testosterone level of <50 ng/dl (<1.74 nmol/l) has been used as the benchmark to assess the efficiency of hormonal therapy, as comparable to the level of suppression achieved with surgical castration [26]. Subsequently, disease progression after achieving castration levels of serum testosterone has been used as the definition of CRPC. For many years, clinicians lacked rigorously proven therapeutic hormonal options for the treatment of prostate cancer after the development of castration-resistant disease, with only docetaxel chemotherapy providing a clear survival benefit in this setting [27, 28]. However, the introduction of several new hormonal agents has challenged the traditional definition of CRPC. The CYP17 enzyme is a member of the cytochrome P450 family of enzymes that mediates the biosynthesis of dehydroepiandrosterone and androstenedione, both precursors of testosterone. Previously, nonselective inhibitors of CYP17suchasketoconazolehavebeenusedinprostate cancer treatment [29]. In contrast, abiraterone acetate has been developed to selectively and irreversibly inhibit the CYP17 enzyme (17α-hydroxylase and C17,20-lyase) [30] and demonstrated significant antitumor activities against prostate cancer in phase I/II clinical trials [31, 32]. Similar to abiraterone, TAK-700 (Orteronel) is an investigational CYP17 inhibitor, that may offer a more precise targeting of the CYP17 biosynthesis pathway by inhibiting only C17,20- lyase [33]. Clinical trials of TAK-700 are currently ongoing [34]. TOK-001 (Galeterone) is another promising investigational CYP17 inhibitor that is currently being evaluated a phase I/II clinical trial (ARMOR1: Androgen Receptor Modulation Optimized for Response 1) [35]. Uniquely, TOK-001 is not only a selective CYP17 (17α-hydroxylase and C17,20-lyase) inhibitor analogous to abiraterone acetate but also an androgen receptor modulator [36]. These new selective CYP17 enzyme inhibitors represent an important bench-to-bedside advancement, responding to the need for more potent and specific inhibitors of extra-gonadal androgen production. In a landmark phase III clinical trial from 2011, de Bono et al. reported that abiraterone acetate plus prednisone compared to prednisone alone yielded an improved median overall survival from 10.4 to 14.8 months in patients with metastatic hormonal-resistant prostate cancer after docetaxel chemotherapy (P < ). Circulating serum testosterone levels are reduced to levels of 1-2 ng/dl with abiraterone acetate much lower than the previous standard of 50 ng/dl used to define CRPC. In this trial, abiraterone plus prednisone also showed significant improvement in time to PSA progression (10.2 months versus 6.6 months; P < ), radiographic progression-free survival (PFS) (5.6 months versus 3.6 months; P < ), and PSA response rate (29.1% versus 5.5%; P < ) when compared to prednisone alone. The immediate side effects of abiraterone were manageable and primarily related to elevated mineralocorticoid levels, including hypertension, fluid retention, and hypokalemia [37].
3 Advances in Urology 3 Table 1: Hormonal therapy in prostate cancer. Class Existing drugs Investigational drugs Estrogen Diethylstilbestrol (DES) GnRH agonists Goserelin, leuprolide, triptorelin, histrelin acetate GnRH antagonists Degarelix, abarelix Antiandrogens Bicalutamide, nilutamide, flutamide, cyproterone acetate MDV3100, TOK-001 Non-specific,cytochrome P450 enzyme inhibitors Ketoconazole Specific CYP17 inhibitors Abiraterone acetate TAK-700, TOK-001 Glucocorticoids Prednisone, Dexamethasone, others Abarelix use in the United States was previously limited to a registry program and it is not actively marketed in the United States currently. Cyproterone acetate is not currently FDA approved for the treatment of prostate cancer in the United States. Hypothalamus Pituitary gland LH, FSH GnRH ACTH Leuprolide Degarelix Prednisone Testicle Orchiectomy Adrenal gland Testosterone Cytoplasm Adrenal androgens Ketoconazole Abiraterone, TAK-700, TOK-001 Prostate cancer cell Androgen receptors DNA Bicalutamide MDV3100, TOK-001 Intratumoral androgen production Figure 1: Hormonal therapy in prostate cancer. Physiologically relevant androgens for prostate cancer originate from three sources: the testicle, adrenal glands, and via intratumoral production. The sites of activity of clinically relevant hormonal therapies are illustrated here, with new and investigational treatments indicated in red. While androgen receptor signaling remains an important pathway of growth in CRPC, the currently available antiandrogens have not been able to completely block androgen receptor signaling [38]. In another area of bench-to-bedside advancement, a new generation antiandrogen (MDV3100) is now in clinical development with encouraging results. Unlike currently available antiandrogens, MDV3100 is a pure androgen receptor antagonist without agonist activity. It is differentiated from the current antiandrogens by its more effective blocking of androgen receptor nuclear translocation and coactivator recruitment of the ligand-receptor complex [39]. In a multicenter, phase I/II study involving 140 patients from 2010, Scher et al. reported that MDV3100 showed antitumor activities in patients with metastatic CRPC, including decreases in serum prostate-specific antigen of 50% or more in 78 of 140 (56%) patients, responses in soft tissue in 13 of 59 (22%) patients, stabilized bone disease in 61 of 109 (56%) patients, and conversion from unfavorable to favorable circulating tumor cell counts in 25 of 51 (49%) patients [40]. Side effects include fatigue, which generally resolved with dose reduction [40] and seizure at higher doses [41]. Phase III studies examining the efficacy of MDV3100
4 4 Advances in Urology both before and after docetaxel chemotherapy in men with CRPC are underway [34, 42]. GnRH plays a key role in the androgen axis. GnRH agonists have been used to achieve medical castration in prostate cancer for decades. Unlike the original GnRH receptor agonists, the recently approved degarelix acts as a direct GnRH antagonist, suppressing LH release without the iniital androgen flare and potential exacerbation of symptoms noted with GnRH receptor agonists [43]. GnRH antagonists such as degarelix also have a faster onset of action with less delay in the suppression of testosterone to castrate levels than GnRH agonists [44]. In a phase III clinical trial from 2008, Klotz et al. reported that when compared to leuprolide after a 1-year treatment period, degarelix was not inferior to leuprolide at maintaining low testosterone levels. In addition, degarelix achieved testosterone and PSA suppression more rapidly than leuprolide with no need for antiandrogen supplements to prevent the initial clinical flare. Manageable side effects of degarelix include flushing, injection-site pain, weight gain, and increased serum transaminase levels [45]. It is important to highlight that when compared to leuprolide, degarelix might offer better suppression of serum alkaline phosphatase (S-ALP) level and more prolonged control of skeletal metastases [46]. Furthermore, though degarelix and leuprolide both act on the GnRH receptor, reports of response to degarelix after previous resistance to GnRH agonist therapy with leuprolide have appeared [47], also potentially complicating our traditional definition of CRPC. 4. Discussion The phase III, landmark findings of the abiraterone acetate study by de Bono et al. have drawn into question our traditional definition of CRPC. Previously, phase I/II clinical trials of the CYP17 inhibitor abiraterone acetate demonstrated clinical activity in CRPC [31, 32]. This phase III study demonstrates a clear survival benefit from additional hormonal manipulation in a prostate cancer population previously described as hormone refractory. Clearly, simply defining CRPC as progressive disease with a serum testosterone level of less than 50 ng/dl is no longer adequate. The findings of de Bono et al. are consistent with other investigations showing ongoing androgen-related activity in the post-chemotherapy setting. Going forward, the definition of hormone-sensitive prostate cancer will need to incorporate the use of a potent CYP17 enzyme inhibitor such as abiraterone acetate. Accordingly, a much lower level of systemic testosterone, beyond the traditional 50 ng/dl benchmark and closer to the 1-2 ng/dl level, must be targeted to achieve complete androgen deprivation. New investigational agents such as TAK-700 and TOK-001 represent addition agents in this class of CYP17 inhibitors, currently undergoing clinical testing in CRPC [33, 35]. Additionally, the use of new generation antiandrogens, such as MDV3100, must also be integrated into our definition of hormonesensitive prostate cancer. The available clinical trial data with this drug, although early and limited, suggests substantial activity in a traditionally defined CRPC population [48]. It is exciting to envision a future with additional clinical gains from the earlier use of potent CYP17 enzyme inhibitors in the course of disease treatment or with combination therapy of abiraterone acetate and other newer agents such as MDV3100. As a general principle, selective pressures from cancer therapy typically yield resistant strains of disease with progressively more aggressive features. Currently, we do not have a good understanding of the phenotypes of advanced prostate cancer that may emerge after early treatment with much more potent hormonal therapies such as MDV3100 and abiraterone acetate. Many unanswered questions remain about the prostate cancer phenotype that will emerge after early use of CYP17 inhibition in terms of robustness, virulence, speed of disease progression, and the responsiveness to cytotoxic chemotherapy. Since John Hunter first described the link between the testis and the prostate over 200 years ago, hormonal therapy remains one of the mainstays of advanced prostate cancer treatment. After initial response, metastatic prostate cancer typically becomes resistant to standard androgen deprivation therapy. Improved survival in this setting has been demonstrated in recent clinical trials involving new agents such as the CYP17 inhibitor abiraterone acetate and the antiandrogen MDV3100, showing that CRPC remains hormonally driven even after treatment with docetaxel chemotherapy, challenging our traditional definition of hormone-sensitive disease. Even though the survival benefit is incremental in the phase III study of very advanced CRPC patients, a threshold has clearly been crossed in defining and treating advanced prostate cancer. With so many new agents for advanced prostate cancer, individual patient characteristics may become very important in the selection and monitoring of therapy. The advantages of Degarelix over previous GnRH agonists may be incremental for most CRPC patients, but the quicker fall in testosterone may be very important to those with critical metastatic or painful lesions such as spinal metastases or near-total urinary obstruction. Likewise, the combination of complete androgen deprivation with abiraterone along with the required safety medication of low-dose glucocorticoid may induce more bone disease via worsening osteoporosis. Men with preexisting bone mineral density loss in this setting may require careful monitoring of the bone mineral density and the use of early bisphosphonates. In this same light, the side effect profile of a potent antiandrogen, which will not lower circulating androgen levels by itself, may become an important consideration if monotherapy with such agents becomes accepted. Furthermore, much like breast cancer is classified and treated based on hormonal receptor characterization today, we believe that advanced prostate cancer may one day also be treated based on molecular assessment. As more is known about the molecular characterization of advanced prostate cancer, it will be imperative to develop more personalized hormonal therapy for individual patients. Taken together, one of the major challenges moving forward will be the personalized application of these new agents in those with advanced CRPC,nowthatwehavemanymorehormonalagentsatour disposal with different side effectsand mechanisms of action.
5 Advances in Urology 5 Disclosure T. w. Flaig has received honoraria from Amgen, consulted for Sanofi-Aventis, and has received study supplies from Veridex. References [1] A.Jemal,F.Bray,M.Center,J.Ferlay,E.Ward,andD.Forman, Global cancer statistics, CA Cancer Journal for Clinicians, vol. 61, no. 2, pp , [2] R. Siegel, E. Ward, O. Brawley, and A. Jemal, Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths, CA Cancer Journal for Clinicians, vol. 61, no. 4, pp , [3] F. A. Schutz and W. K. Oh, Neoadjuvant and adjuvant therapies in prostate cancer, Urologic Clinics of North America, vol. 37, no. 1, pp , [4] S. Machtens, D. Schultheiss, M. Kuczyk, M. Truss, and U. Jonas, The history of endocrine therapy of benign and malignant diseases of the prostate, World Urology, vol. 18, no. 3, pp , [5] C. Huggins and C. V. Hodges, Studies on prostatic cancer: I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. 1941, Urology, vol. 168, no. 1, pp. 9 12, [6] F. Labrie, Adrenal androgens and intracrinology, Seminars in Reproductive Medicine, vol. 22, no. 4, pp , [7] J. L. Mohler, M. A. Titus, and E. M. Wilson, Potential prostate cancer drug target: bioactivation of androstanediol by conversion to dihydrotestosterone, Clinical Cancer Research, vol. 17, no. 18, pp , [8] C. Cai and S. Balk, Intratumoral androgen biosynthesis in prostate cancer pathogenesis and response to therapy, Endocrine-Related Cancer, vol. 18, no. 5, pp , [9] C. Serrate, Y. Loriot, T. De La Motte Rouge et al., Diethylstilbestrol (DES) retains activity and is a reasonable option in patients previously treated with docetaxel for castrationresistant prostate cancer, Annals of Oncology, vol. 20, no. 5, p. 965, [10]T.Granfors,H.Modig,J.E.Damber,andR.Tomic, Longterm followup of a randomized study of locally advanced prostate cancer treated with combined orchiectomy and external radiotherapy versus radiotherapy alone, Urology, vol. 176, no. 2, pp , [11] P. Chrisp and K. L. Goa, Goserelin. A review of its pharmacodynamic and pharmacokinetic properties, and clinical use in sex hormone-related conditions, Drugs, vol. 41, no. 2, pp , [12] M. Marberger, A. V. Kaisary, N. D. Shore et al., Effectiveness, pharmacokinetics, and safety of a new sustained-release leuprolide acetate 3.75-mg depot formulation for testosterone suppression in patients with prostate cancer: a phase III, openlabel, international multicenter study, Clinical Therapeutics, vol. 32, no. 4, pp , [13] R. S. Kirby, J. M. Fitzpatrick, and N. Clarke, Abarelix and other gonadotrophin-releasing hormone antagonists in prostate cancer, BJU International, vol. 104, no. 11, pp , [14] C. Mahler, J. Verhelst, and L. Denis, Clinical pharmacokinetics of the antiandrogens and their efficacy in prostate cancer, Clinical Pharmacokinetics, vol. 34, no. 5, pp , [15] H. C. Shen and S. P. Balk, Development of androgen receptor antagonists with promising activity in castration-resistant prostate cancer, Cancer Cell, vol. 15, no. 6, pp , [16] B. K. Choi, C. H. Park, and C. I. Kim, Comparison of ketoconazole-prednisolone combination therapy with prednisolone alone in patients with hormone refractory prostate cancer, Korean Urology, vol. 41, pp , [17] I. Tannock, M. Gospodarowicz, W. Meakin, T. Panzarella, L. Stewart, and W. Rider, Treatment of metastatic prostatic cancer with low-dose prednisone: evaluation of pain and quality of life as pragmatic indices of response, Clinical Oncology, vol. 7, no. 5, pp , [18] T. W. Flaig and L. M. Glodé, Management of the side effects of androgen deprivation therapy in men with prostate cancer, Expert Opinion on Pharmacotherapy, vol. 9, no. 16, pp , [19] L. Klotz, I. McNeill, and N. Fleshner, A phase 1-2 trial of diethylstilbestrol plus low dose warfarin in advanced prostate carcinoma, Urology, vol. 161, no. 1, pp , [20] A. Nanda, M. H. Chen, M. H. Braccioforte, B. J. Moran, and A. V. D Amico, Hormonal therapy use for prostate cancer and mortality in men with coronary artery disease-induced congestive heart failure or myocardial infarction, the American Medical Association, vol. 302, no. 8, pp , [21] W. D. Figg, S. Woo, W. Zhu et al., A phase I clinical study of high dose ketoconazole plus weekly docetaxel for metastatic castration resistant prostate cancer, Urology, vol. 183, no. 6, pp , [22] E. S. Antonarakis and M. A. Eisenberger, Expanding treatment options for metastatic prostate cancer, The New England Medicine, vol. 364, no. 21, pp , [23] E. Deutsch, L. Maggiorella, P. Eschwege, J. Bourhis, J. C. Soria, and B. Abdulkarim, Environmental, genetic, and molecular features of prostate cancer, Lancet Oncology, vol.5,no.5,pp , [24] S. S. Dutt and A. C. Gao, Molecular mechanisms of castration-resistant prostate cancer progression, Future Oncology, vol. 5, no. 9, pp , [25] W. P. Harris, E. A. Mostaghel, P. S. Nelson, and B. Montgomery, Androgen deprivation therapy: progress in understanding mechanisms of resistance and optimizing androgen depletion, Nature Clinical Practice Urology, vol. 6, no. 2, pp , [26] D. A. Loblaw, K. S. Virgo, R. Nam et al., Initial hormonal management of Androgen-sensitive metastatic, recurrent, or progressive prostate cancer: 2006 Update of an American society of clinical oncology practice guideline, Clinical Oncology, vol. 25, no. 12, pp , [27] I. F. Tannock, R. de Wit, W. R. Berry et al., Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer, The New England Medicine, vol. 351, no. 15, pp , [28] D. P. Petrylak, C. M. Tangen, M. H. Hussain et al., Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer, The New England Medicine, vol. 351, no. 15, pp , [29] T. S. Vasaitis, R. D. Bruno, and V. C. Njar, CYP17 inhibitors for prostate cancer therapy, Steroid Biochemistry and Molecular Biology, vol. 125, no. 1-2, pp , 2010.
6 6 Advances in Urology [30] A. H. Reid, G. Attard, E. Barrie, and J. S. de Bono, CYP17 inhibition as a hormonal strategy for prostate cancer, Nature Clinical Practice Urology, vol. 5, no. 11, pp , [31] G. Attard, A. H. M. Reid, R. A Hern et al., Selective inhibition of CYP17 with abiraterone acetate is highly active in the treatment of castration-resistant prostate cancer, Clinical Oncology, vol. 27, no. 23, pp , [32] A. H. Reid, G. Attard, D. Danila et al., Significant and sustained antitumor activity in post-docetaxel, castration-resistant prostate cancer with the CYP17 inhibitor abiraterone acetate, Clinical Oncology, vol. 28, no. 9, pp , [33] R.Dreicer,D.B.Agus,G.R.MacVicar,J.Wang,D.MacLean, and W. M. Stadler, Safety, pharmacokinetics, and efficacy of TAK-700 in metastatic castration-resistant prostrate cancer: a phase I/II, open-label study, Clinical Oncology, vol. 28, no. 15, supplement 3084, p. 15s, [34] D. P. Petrylak, Current clinical trials in castrate-resistant prostate cancer, Current Urology Reports, vol. 12, no. 3, pp , [35] T. S. Vasaitis, R. D. Bruno, and V. C. Njar, CYP17 inhibitors for prostate cancer therapy, Steroid Biochemistry and Molecular Biology, vol. 125, no. 1-2, pp , [36] A. Molina and A. Belldegrun, Novel therapeutic strategies for castration resistant prostate cancer: inhibition of persistent androgen production and androgen receptor mediated signaling, The Urology, vol. 185, no. 3, pp , [37] J. S. de Bono, C. J. Logothetis, A. Molina et al., Abiraterone and increased survival in metastatic prostate cancer, The New England Medicine, vol. 364, no. 21, pp , [38] Y. Chen, C. L. Sawyers, and H. I. Scher, Targeting the androgen receptor pathway in prostate cancer, Current Opinion in Pharmacology, vol. 8, no. 4, pp , [39] C.Tran,S.Ouk,N.J.Cleggetal., Developmentofasecondgeneration antiandrogen for treatment of advanced prostate cancer, Science, vol. 324, no. 5928, pp , [40] H. I. Scher, T. M. Beer, C. S. Higano et al., Antitumour activity of MDV3100 in castration-resistant prostate cancer: a phase 1-2study, The Lancet, vol. 375, no. 9724, pp , [41] W.R.Foster,B.D.Car,H.Shietal., Drugsafetyisabarrier to the discovery and development of new androgen receptor antagonists, Prostate, vol. 71, no. 5, pp , [42] C. Massard and K. Fizazi, Targeting continued androgen receptor signaling in prostate cancer, Clinical Cancer Research, vol. 17, no. 12, pp , [43] H. van Poppel, Evaluation of degarelix in the management of prostate cancer, Cancer Management and Research, vol. 2, no. 1, pp , [44] P. J. Pommerville and J. G. de Boer, GnRH antagonists in the treatment of advanced prostate cancer, The Canadian Journal of Urology, vol. 17, no. 2, pp , [45] L. Klotz, L. Boccon-Gibod, N. D. Shoreetal., Theefficacy and safety of degarelix: a 12-month, comparative, randomized, open-label, parallel-group phase III study in patients with prostate cancer, BJU International, vol. 102, no. 11, pp , [46] F. H. Schröder, B. Tombal, K. Miller et al., Changes in alkaline phosphatase levels in patients with prostate cancer receiving degarelix or leuprolide: results from a 12-month, comparative, phase III study, BJU International, vol. 106, no. 2, pp , [47] R. S. Raddin, C. M. Walko, Y. E. Whang et al., Response to degarelix after resistance to luteinizing hormone-releasing hormone agonist therapy for metastatic prostate cancer, Anti- Cancer Drugs, vol. 22, no. 3, pp , [48] C. J. Ryan and D. J. Tindall, Androgen receptor rediscovered: the new biology and targeting the androgen receptor therapeutically, Clinical Oncology, vol. 29, no. 27, pp , 2011.










7 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
majority of the patients. And taking an aggregate of all trials, very possibly has a modest effect on improved survival.
 Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository:
 This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/103187/ This is the author s version of a work that was submitted to / accepted
This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: http://orca.cf.ac.uk/103187/ This is the author s version of a work that was submitted to / accepted
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Castrate resistant prostate cancer: the future of anti-androgens.
 Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Evolution or revolution in the treatment of prostate cancer
 Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Hormonotherapy of advanced prostate cancer
 Annals of Oncology 16 (Supplement 4): iv80 iv84, 2005 doi:10.1093/annonc/mdi913 Hormonotherapy of advanced prostate cancer P. Pronzato & M. Rondini Department of Oncology, Felettino Hospital, La Spezia,
Annals of Oncology 16 (Supplement 4): iv80 iv84, 2005 doi:10.1093/annonc/mdi913 Hormonotherapy of advanced prostate cancer P. Pronzato & M. Rondini Department of Oncology, Felettino Hospital, La Spezia,
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Lecture 10: Hormonal agents
 Lecture 10: Hormonal agents The survival and proliferation (growth) of some cancer cells is dependent on the action of steroid hormones. Early stage breast cancer and early stage prostate cancer are the
Lecture 10: Hormonal agents The survival and proliferation (growth) of some cancer cells is dependent on the action of steroid hormones. Early stage breast cancer and early stage prostate cancer are the
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia
 Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Risk of renal side effects with ADT. E. David Crawford University of Colorado, Aurora, CO, USA
 Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Anti-Androgen Therapies for Prostate Cancer: A Focused Review
 Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Sequencing treatment for metastatic prostate cancer
 11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
ERLEADA (apalutamide) oral tablet
 oral tablet") ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Treatment of Advanced Prostate Cancer
 Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Recent Progress in Management of Advanced Prostate Cancer
 Review Article [1] April 15, 2005 By Philip W. Kantoff, MD [2] Androgen-deprivation therapy, usually with combined androgen blockade, is standard initial treatment for advanced prostate cancer. With failure
Review Article [1] April 15, 2005 By Philip W. Kantoff, MD [2] Androgen-deprivation therapy, usually with combined androgen blockade, is standard initial treatment for advanced prostate cancer. With failure
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
A Forward Look at Options for. In Prostate Cancer
 A Forward Look at Options for Prostate Cancer Charles J Ryan, MD Associate Professor of Medicine Helen Diller Family Comprehensive Cancer Center University of California, San Francisco UC 1 SF UC SF Castration
A Forward Look at Options for Prostate Cancer Charles J Ryan, MD Associate Professor of Medicine Helen Diller Family Comprehensive Cancer Center University of California, San Francisco UC 1 SF UC SF Castration
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
reviews LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate therapy
 reviews therapy LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate Martin I. Resnick, MD, Lester Persky Professor and Chief, Department of Urology, Case Western Reserve University School
reviews therapy LHRH Agonists in the Treatment of Advanced Carcinoma of the Prostate Martin I. Resnick, MD, Lester Persky Professor and Chief, Department of Urology, Case Western Reserve University School
Prostate cancer is now the most
 : a new hormonal treatment for prostate cancer Professor Malcolm Mason, School of Medicine, Cardiff University, Velindre Hospital, Whitchurch, Cardiff - hypothalamus According to NICE, prostate cancer
: a new hormonal treatment for prostate cancer Professor Malcolm Mason, School of Medicine, Cardiff University, Velindre Hospital, Whitchurch, Cardiff - hypothalamus According to NICE, prostate cancer
The Prognostic Importance of Prostate-Specific Antigen in Monitoring Patients Undergoing Maximum Androgen Blockage for Metastatic Prostate Cancer
 Research Article TheScientificWorldJOURNAL (005) 5, 8 4 ISSN 57-744X; DOI 0.00/tsw.005.9 The Prognostic Importance of Prostate-Specific Antigen in Monitoring Patients Undergoing Maximum Androgen Blockage
Research Article TheScientificWorldJOURNAL (005) 5, 8 4 ISSN 57-744X; DOI 0.00/tsw.005.9 The Prognostic Importance of Prostate-Specific Antigen in Monitoring Patients Undergoing Maximum Androgen Blockage
Medical Treatments for Prostate Cancer
 Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc
 SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey
 Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer*
 Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
FIRMAGON/DEGARELIX. Compiled by Charles (Chuck) Maack Prostate Cancer Activist/Mentor
 Maack Prostate Cancer Activist/Mentor") FIRMAGON/DEGARELIX The Advantage of this GnRH/LHRH antagonist over that of GnRH/LHRH agonists particularly when administered to patients with known prostate cancer metastases Compiled by Charles (Chuck)
FIRMAGON/DEGARELIX The Advantage of this GnRH/LHRH antagonist over that of GnRH/LHRH agonists particularly when administered to patients with known prostate cancer metastases Compiled by Charles (Chuck)
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Urological Science xxx (2015) 1e5. Contents lists available at ScienceDirect. Urological Science. journal homepage:
 1e5. Contents lists available at ScienceDirect. Urological Science. journal homepage:") Urological Science xxx (2015) 1e5 Contents lists available at ScienceDirect Urological Science journal homepage: www.urol-sci.com Original article The efficacy of abiraterone acetate in treating Taiwanese
Urological Science xxx (2015) 1e5 Contents lists available at ScienceDirect Urological Science journal homepage: www.urol-sci.com Original article The efficacy of abiraterone acetate in treating Taiwanese
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Prostate Cancer: Vision of the Future By: H.R.Jalalian
 1 H. R. Jalalian Hematologist&Oncologist Baqiyatallah University of Medical Sciences 2 State of the art: vision on the future Diagnosis Surgery Radiotherapy Medical Oncology 3 Early Detection PSA sensitivity
1 H. R. Jalalian Hematologist&Oncologist Baqiyatallah University of Medical Sciences 2 State of the art: vision on the future Diagnosis Surgery Radiotherapy Medical Oncology 3 Early Detection PSA sensitivity
Abiraterone Acetate is an antiandrogen used in the treatment of Castration-Resistant Prostate Cancer(CRPC).
.") For the use only of an Oncologist or a Hospital or a Laboratory ABIRATERONE ACETATE TABLETS Zabiteron-250 COMPOSITION Abiraterone Acetate Tablets 250mg Each uncoated tablets contains: Abiraterone Acetate
For the use only of an Oncologist or a Hospital or a Laboratory ABIRATERONE ACETATE TABLETS Zabiteron-250 COMPOSITION Abiraterone Acetate Tablets 250mg Each uncoated tablets contains: Abiraterone Acetate
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer
 Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT
 MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
MODULE 8: PROSTATE CANCER: SCREENING & MANAGEMENT KEYWORDS: Prostate cancer, PSA, Screening, Radical Prostatectomy LEARNING OBJECTIVES At the end of this clerkship, the medical student will be able to:
The Current State of Hormonal Therapy for Prostate Cancer
 The Current State of Hormonal Therapy for Prostate Cancer The Current State of Hormonal Therapy for Prostate Cancer Beth A. Hellerstedt, MD; Kenneth J. Pienta, MD Dr. Hellerstedt is Fellow, Division of
The Current State of Hormonal Therapy for Prostate Cancer The Current State of Hormonal Therapy for Prostate Cancer Beth A. Hellerstedt, MD; Kenneth J. Pienta, MD Dr. Hellerstedt is Fellow, Division of
This article is authors accepted manuscripts in Asian Journal of Andrology.
 This article is authors accepted manuscripts in Asian Journal of Andrology. OnlineFirst Author s accepted Manuscripts are PDF versions of manuscripts that have been peer reviewed and accepted for publication,
This article is authors accepted manuscripts in Asian Journal of Andrology. OnlineFirst Author s accepted Manuscripts are PDF versions of manuscripts that have been peer reviewed and accepted for publication,
Manipulating Hormones: Androgen Suppression in Prostate Cancer Patients
 Focus on CME at the University of Queen s ManitobaUniversity Manipulating Hormones: Androgen Suppression in ostate Cancer Patients By D. Robert Siemens, MD, FRCSC Case A 62-year old man presents with complaints
Focus on CME at the University of Queen s ManitobaUniversity Manipulating Hormones: Androgen Suppression in ostate Cancer Patients By D. Robert Siemens, MD, FRCSC Case A 62-year old man presents with complaints
Hormonal Manipulations in CRPC. NW Clarke Professor of Urological Oncology Manchester UK
 Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
Hormonal Manipulations in CRPC NW Clarke Professor of Urological Oncology Manchester UK Standard Treatment of CRPC Pre 2004 (and in 2013?) PSA progression 99m Tc BS negative CT scan large lymph node component
and Sayo Suda Takeshi Kashiwabara *
 Kashiwabara and Suda BMC Cancer (2018) 18:619 https://doi.org/10.1186/s12885-018-4541-0 RESEARCH ARTICLE Open Access Usefulness of combined androgen blockade therapy with gonadotropinreleasing hormone
Kashiwabara and Suda BMC Cancer (2018) 18:619 https://doi.org/10.1186/s12885-018-4541-0 RESEARCH ARTICLE Open Access Usefulness of combined androgen blockade therapy with gonadotropinreleasing hormone
Prostate Cancer Case Study 2. Medical Student Case-Based Learning
 Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Prostate Cancer Case Study 2 Medical Student Case-Based Learning The Case of Mr. Powers Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy
Antiandrogen Therapies for non-metastatic Castration-Resistant Prostate Cancer: Effectiveness and Value
 Antiandrogen Therapies for non-metastatic Castration-Resistant Prostate Cancer: Effectiveness and Value Final Background and Scope April 9, 2018 Background Prostate cancer is the second most common cause
Antiandrogen Therapies for non-metastatic Castration-Resistant Prostate Cancer: Effectiveness and Value Final Background and Scope April 9, 2018 Background Prostate cancer is the second most common cause
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
CME Baseline Curriculum Report
 CME Baseline Curriculum Report October 14, 2010 For CME Activity: Managing Advanced Prostate Cancer in the Community Setting: A Case-based Curriculum Supported by an independent educational grant from
CME Baseline Curriculum Report October 14, 2010 For CME Activity: Managing Advanced Prostate Cancer in the Community Setting: A Case-based Curriculum Supported by an independent educational grant from
HHS Public Access Author manuscript Prostate Cancer Prostatic Dis. Author manuscript; available in PMC 2015 December 01.
 Prospective Evaluation of Low-Dose Ketoconazole Plus Hydrocortisone (HC) in Docetaxel Pre-treated Castration- Resistant Prostate Cancer (CRPC) Patients Ernest N. Lo, M.D. 1, Laurel A. Beckett, Ph.D. 1,
Prospective Evaluation of Low-Dose Ketoconazole Plus Hydrocortisone (HC) in Docetaxel Pre-treated Castration- Resistant Prostate Cancer (CRPC) Patients Ernest N. Lo, M.D. 1, Laurel A. Beckett, Ph.D. 1,
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
SAMPLE ONLY. Your Health Matters. Advanced Prostate Cancer and its Treatment A Patient Guide. Please order from Documents and Media: 415/
 Your Health Matters Advanced Prostate Cancer and its Treatment A Patient Guide UCSF Genitourinary Medical Oncology Program Charles Ryan, MD, UCSF Patient Advocates Please order from Documents and Media:
Your Health Matters Advanced Prostate Cancer and its Treatment A Patient Guide UCSF Genitourinary Medical Oncology Program Charles Ryan, MD, UCSF Patient Advocates Please order from Documents and Media:
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Management of castrate resistant disease; after first line hormone therapy fails
 Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
פ א ר מ ה P H A R x M A
 פ א ר מ ה P H A R x M A הביטאון לענייני תרופות ותראפיה ISRAEL DRUG BULLETIN Vol. 19, Bulletin No. 107 June-July 2012 Also in the Bulletin: Degarelix for Advanced Hormone-Dependent Prostate Cancer NEW TREATMENT
פ א ר מ ה P H A R x M A הביטאון לענייני תרופות ותראפיה ISRAEL DRUG BULLETIN Vol. 19, Bulletin No. 107 June-July 2012 Also in the Bulletin: Degarelix for Advanced Hormone-Dependent Prostate Cancer NEW TREATMENT
Marketing Authorisation Holder Applicant Invented name. Route of administration. Content (concentration) Member State. l form
 Member State. l form") ANNEX I LIST OF THE NAMES, PHARMACEUTICAL FORM, STRENGTH OF THE MEDICINAL PRODUCT, ROUTE OF ADMINISTRATION, APPLICANT AND MARKETING AUTHORISATION HOLDER IN THE MEMBER STATES 1 Member State Marketing Authorisation
ANNEX I LIST OF THE NAMES, PHARMACEUTICAL FORM, STRENGTH OF THE MEDICINAL PRODUCT, ROUTE OF ADMINISTRATION, APPLICANT AND MARKETING AUTHORISATION HOLDER IN THE MEMBER STATES 1 Member State Marketing Authorisation
MOLECULAR AND CLINICAL ONCOLOGY 4: , 2016
 MOLECULAR AND CLINICAL ONCOLOGY 4: 839-844, 2016 Clinical outcomes of anti androgen withdrawal and subsequent alternative anti-androgen therapy for advanced prostate cancer following failure of initial
MOLECULAR AND CLINICAL ONCOLOGY 4: 839-844, 2016 Clinical outcomes of anti androgen withdrawal and subsequent alternative anti-androgen therapy for advanced prostate cancer following failure of initial
Cabazitaxel (XRP-6258) for hormone refractory, metastatic prostate cancer second line after docetaxel
 for hormone refractory, metastatic prostate cancer second line after docetaxel") Cabazitaxel (XRP-6258) for hormone refractory, metastatic prostate cancer second line after docetaxel April 2009 This technology summary is based on information available at the time of research and a
Cabazitaxel (XRP-6258) for hormone refractory, metastatic prostate cancer second line after docetaxel April 2009 This technology summary is based on information available at the time of research and a
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Correspondence should be addressed to Alicia McMaster;
 Cancer Research Volume 2013, Article ID 308236, 5 pages http://dx.doi.org/10.1155/2013/308236 Research Article Taxpas: Epidemiological and Survival Data in Breast Cancer Patients Treated with a Docetaxel-Based
Cancer Research Volume 2013, Article ID 308236, 5 pages http://dx.doi.org/10.1155/2013/308236 Research Article Taxpas: Epidemiological and Survival Data in Breast Cancer Patients Treated with a Docetaxel-Based
2. The effectiveness of combined androgen blockade versus monotherapy.
 Relative effectiveness and cost-effectiveness of methods of androgen suppression in the treatment of advanced prostate cancer Blue Cross and Blue Shield Association, Aronson N, Seidenfeld J Authors' objectives
Relative effectiveness and cost-effectiveness of methods of androgen suppression in the treatment of advanced prostate cancer Blue Cross and Blue Shield Association, Aronson N, Seidenfeld J Authors' objectives
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Targeting GPCRs for Cancer Therapy 03/11/2014
 Targeting GPCRs for Cancer Therapy 03/11/2014 G Protein Coupled Receptors Actually 4% of the human genome GPCR dysfunction contributes to some of the most prevalent human diseases GPCRs represent 60% of
Targeting GPCRs for Cancer Therapy 03/11/2014 G Protein Coupled Receptors Actually 4% of the human genome GPCR dysfunction contributes to some of the most prevalent human diseases GPCRs represent 60% of
Introduction. Original Article: Clinical Investigation
 bs_bs_banner International Journal of Urology (2014) 21, 1239 1244 doi: 10.1111/iju.12589 Original Article: Clinical Investigation Abiraterone acetate and prednisolone for metastatic castration-resistant
bs_bs_banner International Journal of Urology (2014) 21, 1239 1244 doi: 10.1111/iju.12589 Original Article: Clinical Investigation Abiraterone acetate and prednisolone for metastatic castration-resistant
What s New in Advanced Disease (CRPC)?
?") What s New in Advanced Disease (castration resistant prostate cancer = CRC)? Matthew Rettig, MD Associate rofessor Department of Medicine Division of Hematology-Oncology Department of Urology Medical Director,
What s New in Advanced Disease (castration resistant prostate cancer = CRC)? Matthew Rettig, MD Associate rofessor Department of Medicine Division of Hematology-Oncology Department of Urology Medical Director,
Navigating Prostate Cancer Therapy. Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA
 Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Complete Androgen Blockade Safely Allows for Delay of Cytotoxic Chemotherapy in Castration Refractory Prostate Cancer
 Clinical Urology Benefit of Androgen Blockade in Prostate Cancer International Braz J Urol Vol. 36 (3): 300-307, May - June, 2010 doi: 10.1590/S1677-55382010000300006 Complete Androgen Blockade Safely
Clinical Urology Benefit of Androgen Blockade in Prostate Cancer International Braz J Urol Vol. 36 (3): 300-307, May - June, 2010 doi: 10.1590/S1677-55382010000300006 Complete Androgen Blockade Safely
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
LUNCH AND LEARN. April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology
 LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
Apalutamide in the treatment of castrate-resistant prostate cancer: evidence from clinical trials
 811450TAU0010.1177/1756287218811450Therapeutic Advances in UrologyVS Koshkin and EJ Small review-article2018 Therapeutic Advances in Urology Review Apalutamide in the treatment of castrate-resistant prostate
811450TAU0010.1177/1756287218811450Therapeutic Advances in UrologyVS Koshkin and EJ Small review-article2018 Therapeutic Advances in Urology Review Apalutamide in the treatment of castrate-resistant prostate
Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels?
 ORIGINAL PAPER DOI: 10.4081/aiua.2017.4.282 Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels? Murat Bagcioglu
ORIGINAL PAPER DOI: 10.4081/aiua.2017.4.282 Medical management in locally advanced and metastatic prostate cancer: Does changes in treatment policy have any specific effect on PSA levels? Murat Bagcioglu
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
MEETING REVIEW. Jack Barkin, MD University of Toronto, Humber River Hospital, Toronto, Ontario, Canada. Background
 MEETING REVIEW Risks, benefits, and approaches to hormonal blockade in prostate cancer Highlights from the European Association of Urology Meeting, March 20-24, 2015, Madrid, Spain Jack Barkin, MD University
MEETING REVIEW Risks, benefits, and approaches to hormonal blockade in prostate cancer Highlights from the European Association of Urology Meeting, March 20-24, 2015, Madrid, Spain Jack Barkin, MD University
Targeting the Androgen Receptor in Castration Resistant Prostate Cancer. Raoul S. Concepcion, MD,FACS IPCU January 2017
 Targeting the Androgen Receptor in Castration Resistant Prostate Cancer Raoul S. Concepcion, MD,FACS IPCU January 2017 Consultant: Myriad, CUSP, Tolmar, Integra Cloud, Cellay Speakers Bureau: Dendreon,
Targeting the Androgen Receptor in Castration Resistant Prostate Cancer Raoul S. Concepcion, MD,FACS IPCU January 2017 Consultant: Myriad, CUSP, Tolmar, Integra Cloud, Cellay Speakers Bureau: Dendreon,
Androgen synthesis inhibitors in the treatment of castration resistant prostate cancer
 (2014) 16, 387 400 2014 AJA, SIMM & SJTU. All rights reserved 1008-682X www.asiaandro.com; www.ajandrology.com Prostate Cancer Open Access INVITED REVIEW Androgen synthesis inhibitors in the treatment
(2014) 16, 387 400 2014 AJA, SIMM & SJTU. All rights reserved 1008-682X www.asiaandro.com; www.ajandrology.com Prostate Cancer Open Access INVITED REVIEW Androgen synthesis inhibitors in the treatment
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer
 agonists in prostate cancer") B88 April 2015 2.1 Community Interest Company Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer This bulletin focuses on luteinising hormone-releasing hormone (LHRH) agonists. Currently
B88 April 2015 2.1 Community Interest Company Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer This bulletin focuses on luteinising hormone-releasing hormone (LHRH) agonists. Currently
Correspondence should be addressed to Taha Numan Yıkılmaz;
 Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most