Hemikolektomie rechts OFFEN was sonst?
|
|
|
- Noel Todd
- 6 years ago
- Views:
Transcription
1 Hemikolektomie rechts OFFEN was sonst? Hermann Kessler, M.D. Ph.D., FACS Department of Colorectal Surgery Digestive Disease Institute Cleveland Clinic, Cleveland, Ohio
2 Rectal Cancer Moynihan 1908: We have not yet sufficiently realized that the surgery of malignant disease is not the surgery of organs; it is the anatomy of the lymphatic system Suggestion of high tie Cirocchi R et al, Surg Oncol 2012;21:e

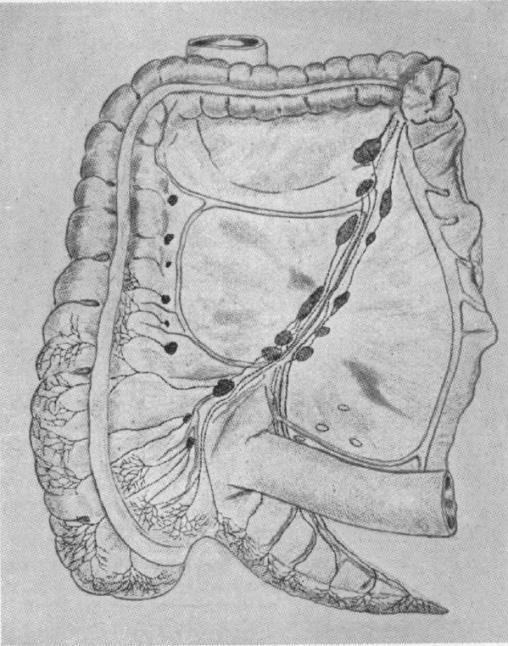
3 Ann Surg 1909; 50:


4 1982, Data from England Local recurrence of rectal cancer Common in 20-35% Cause unknown but obsession with distal margin and distal spread 90% mortality Long unpleasant death




5 Bill Heald & Phil Quirke
6 The Circumferential Resection Margin Quirke et al 1986
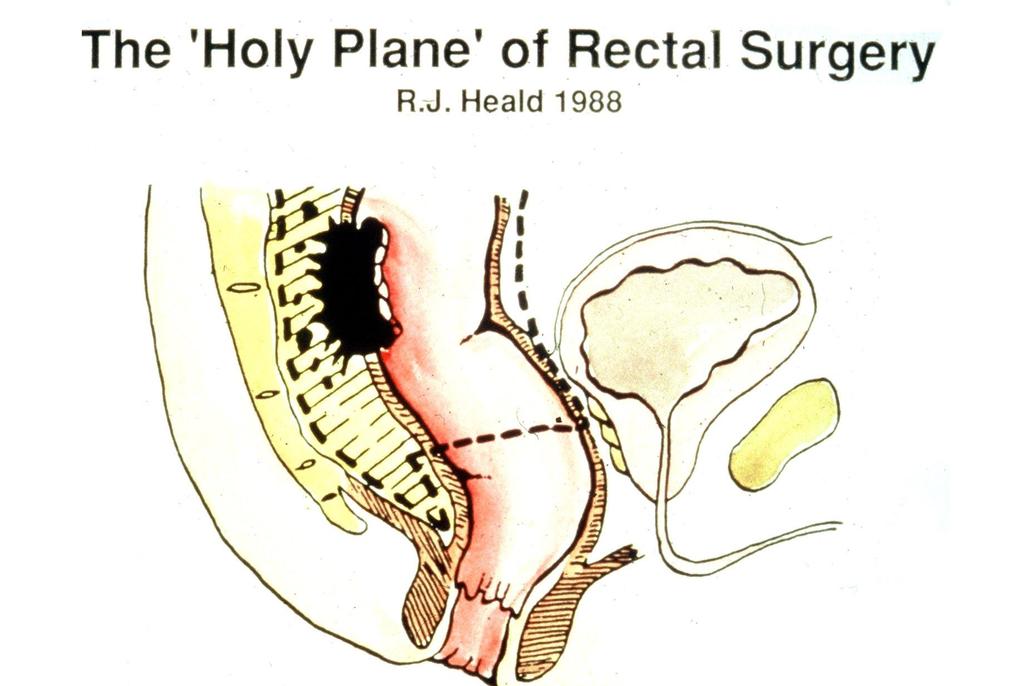
7




8 The rectal cancer story

9

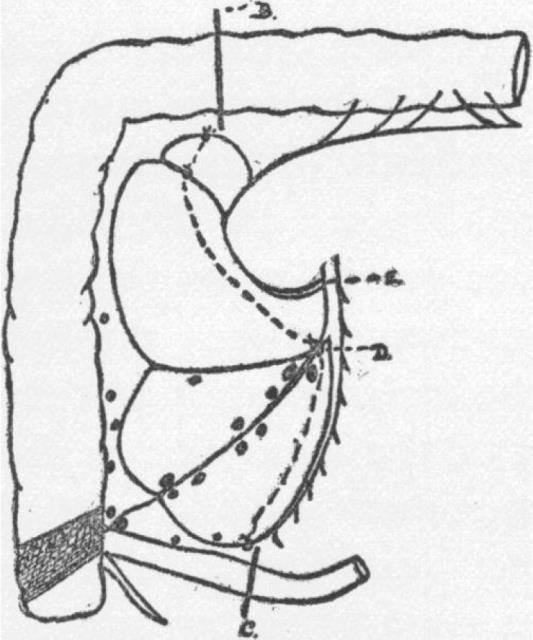
10 V. Schmieden 1940
11 Colon Cancer Survival No touch vs. Conventional Turnbull Conventional all patients* 81,6% Dukes C* 67,3% observed all patients 68,85% 52,13% Dukes C* 57,84% 28,06% * age adjusted Rupert B.Turnbull 1967 and 1970

12 R. Turnbull 1967
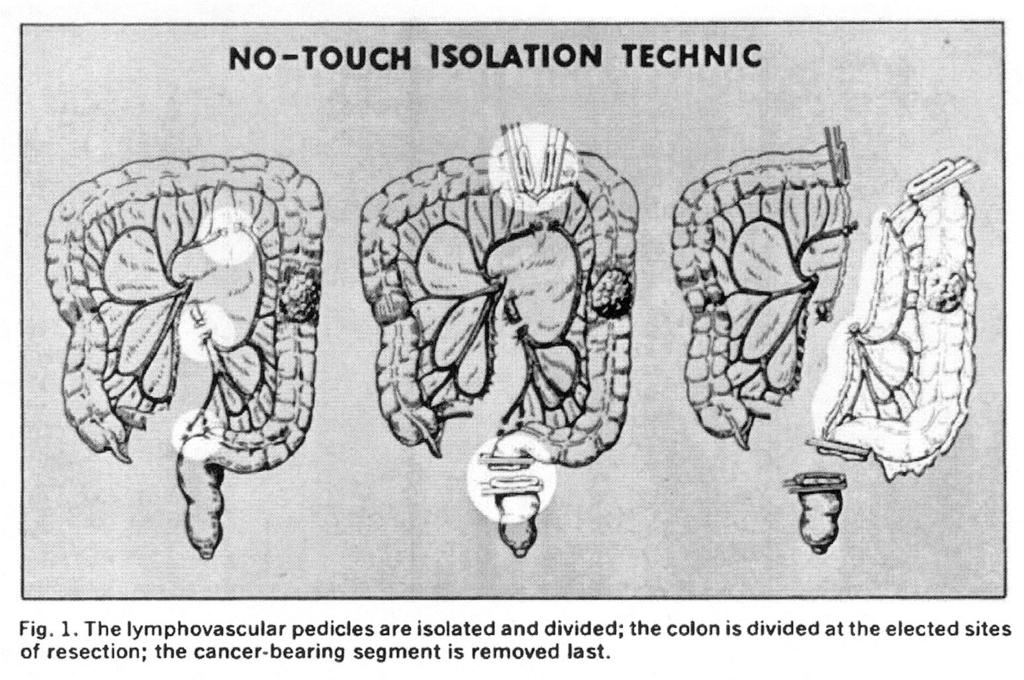
13 R.Turnbull 1967


14 Surgery of Right Sided Colon Cancer in 2010


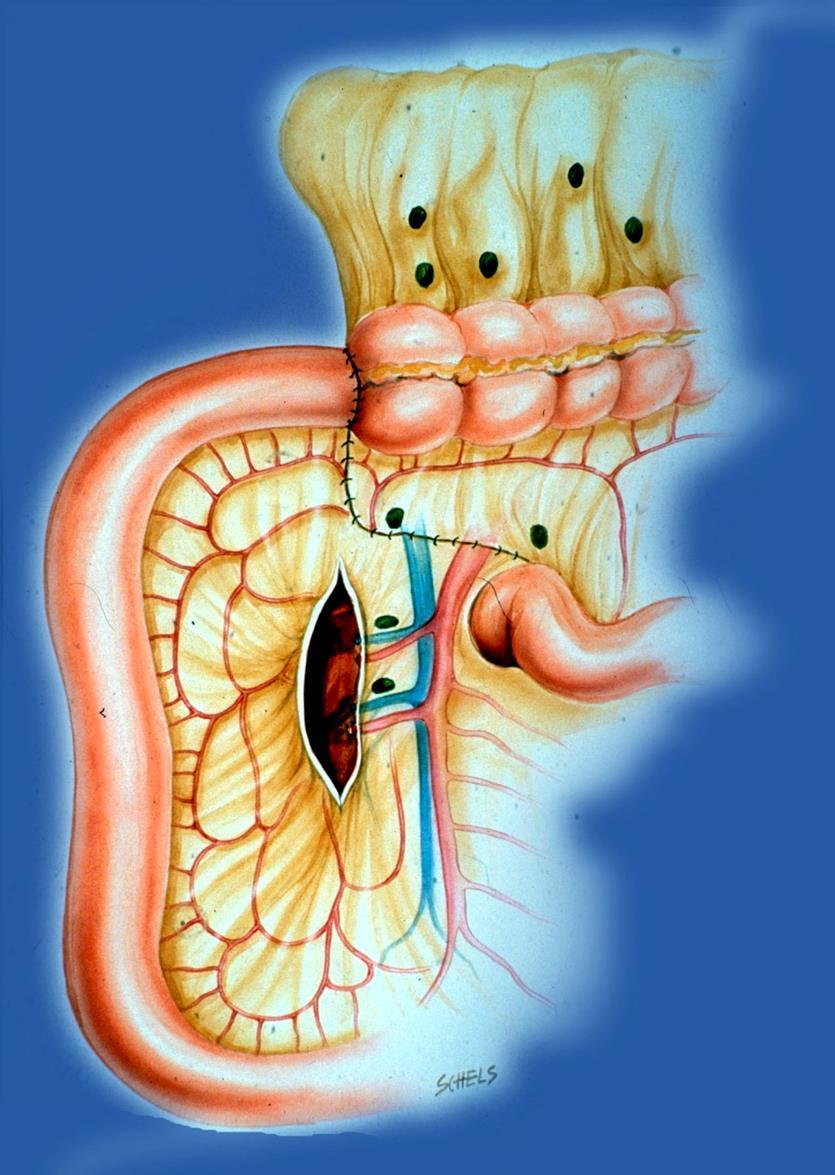
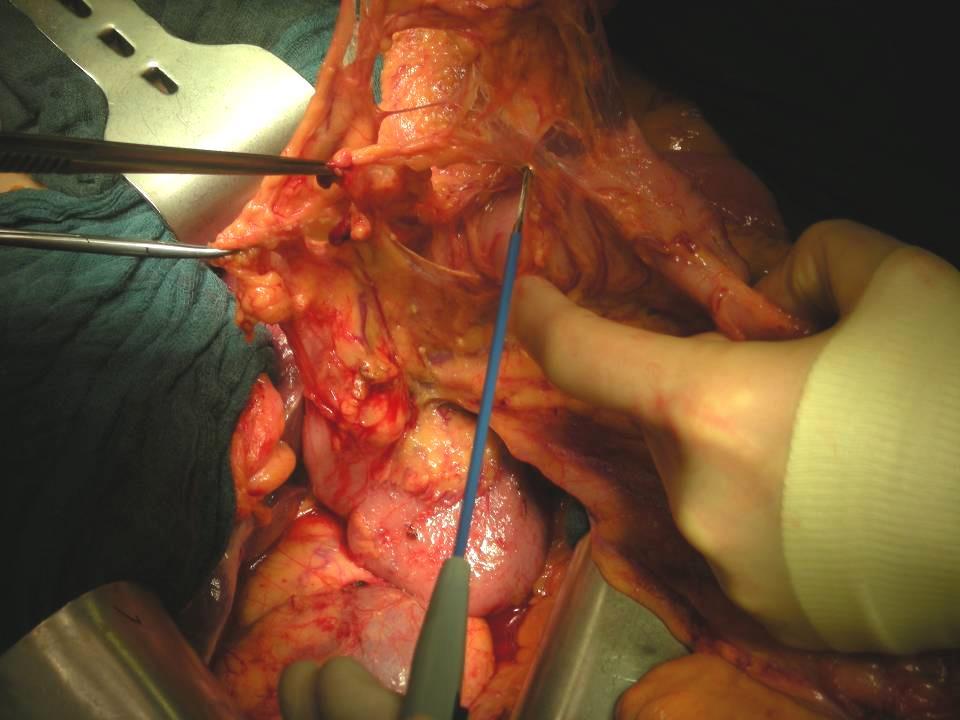
15 Colon Cancer Central Tie right branch of middle colic artery dissected, ready to clamp right colic artery ilecolic artery superior mesenteric artery

16 SGCRC Colon Carcinoma Locoregional Recurrences All patients 4-24% Stage I 0-9% Stage II 1-18% Stage III 9-38%

17 Colon Carcinoma 5-Year Survival Rates SGCRC* All Departments ERCRC all best surgeon UICC-Stage I 96.6% % 95.5% 100% UICC-Stage II 89.5% % 90.4% 96.7% UICC-Stage III 61.6% % 72.2% 80.4% R0, all stages 80.9% % 86.6% 93.6% * tumor related tumor related, no adjuvant therapy
18 Colon Carcinoma Observed Survival Rates All patients UICC stage III Middle Franconia 50,0 % 52,0 % German Study Group 52,7 % Colorectal Cancer Dept. of Surgery, Univ. of Erlangen 58,7 % 84,9 % SEERS pt1 N1 73,0 % pt3 N1 54,9 % pt3 N2 38,1 % USA very high volume * 49,6 % 44,0 % Sugihara/Tokyo 77,2 % Kube et al 2009 * Schrag et al 2010

19 Colon Cancer Cancer related 5-Year Survival Related to Periods : 90,2% : 87,2% : 84,6% : 83,6% : 82,1% Stages I-III, R0, Erlangen Registry

20 Colon Cancer Cancer related 5-Years Survival Related to Periods Stage III, R0, Erlanger Register : 81,8% : 73,7% : 74,0% : 69,0% : 62,0 %


21 Colon Cancer Paracolic Lymph Node Involvement
22
23
24 060303Hohenberger
25 Lymph node involvement < pt category Hida J et al, Cancer (2),



26 Data from Tokyo
27

28 Courtesy Prof. Solveig Anderson/Oslo
29 Colorectal Cancer Specimen Retrieval Grading of Quality Rectal planes Colonic planes Muscularis propria Intramesorectal Mesorectal Muscularis propria Intramesocolic Mesocolic Phil Quirke, Nich. West / Leeds
30 Colorectal Cancer Specimen Retrieval Grading of Quality Rectal planes Colonic planes Muscularis propria Intramesorectal Mesorectal Muscularis propria Intramesocolic Mesocolic Mesocolic plus high ties defined by measurement Phil Quirke, Nich. West / Leeds
 Regional and central lymph node dissection with high tie of suppling")
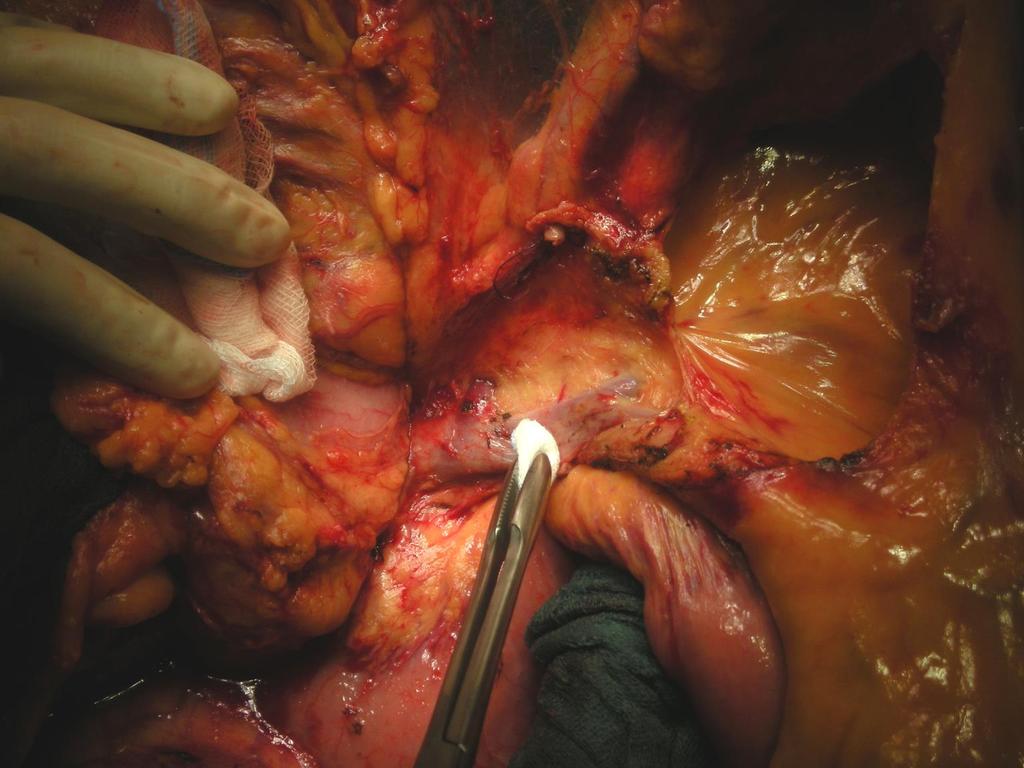
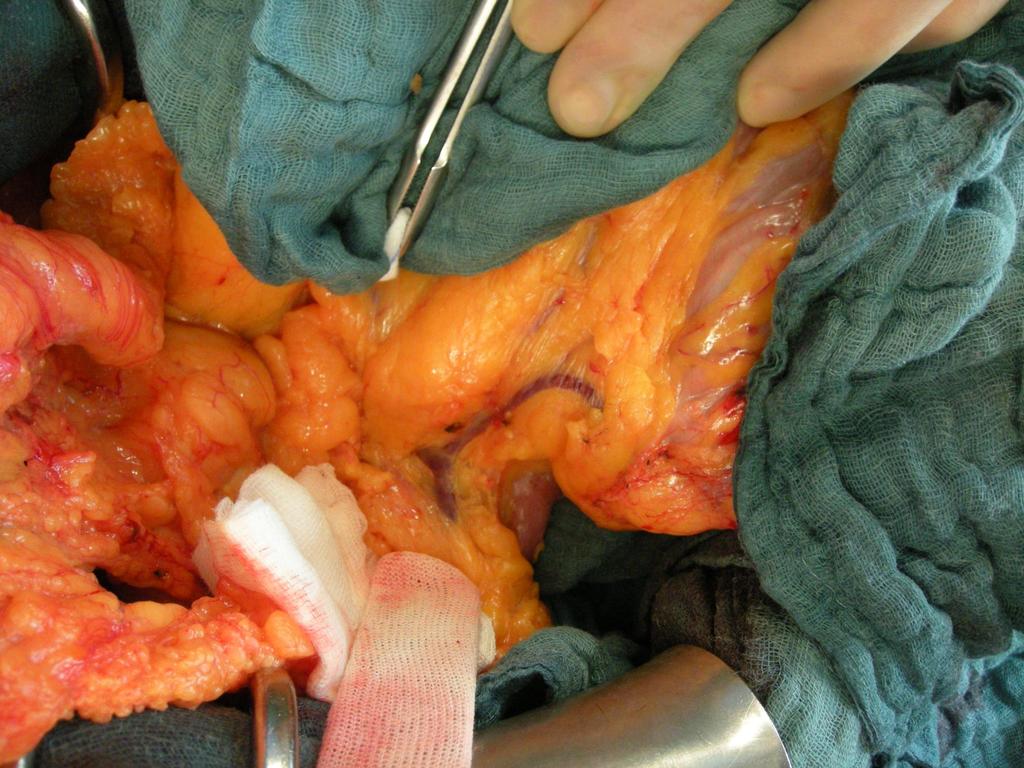
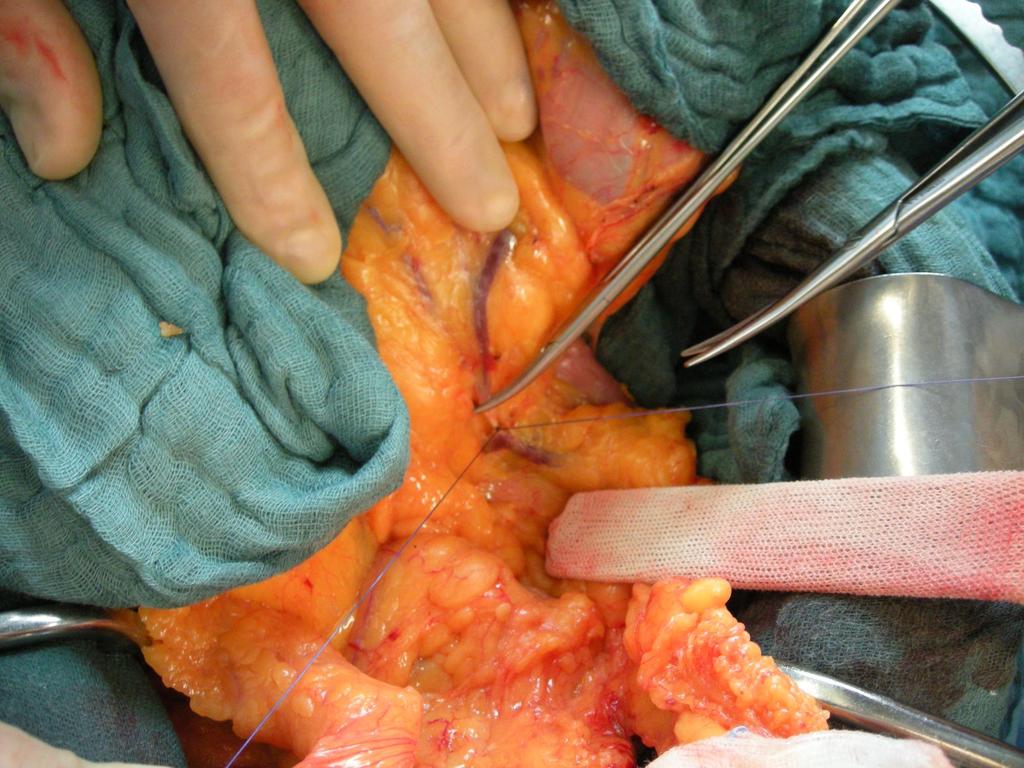
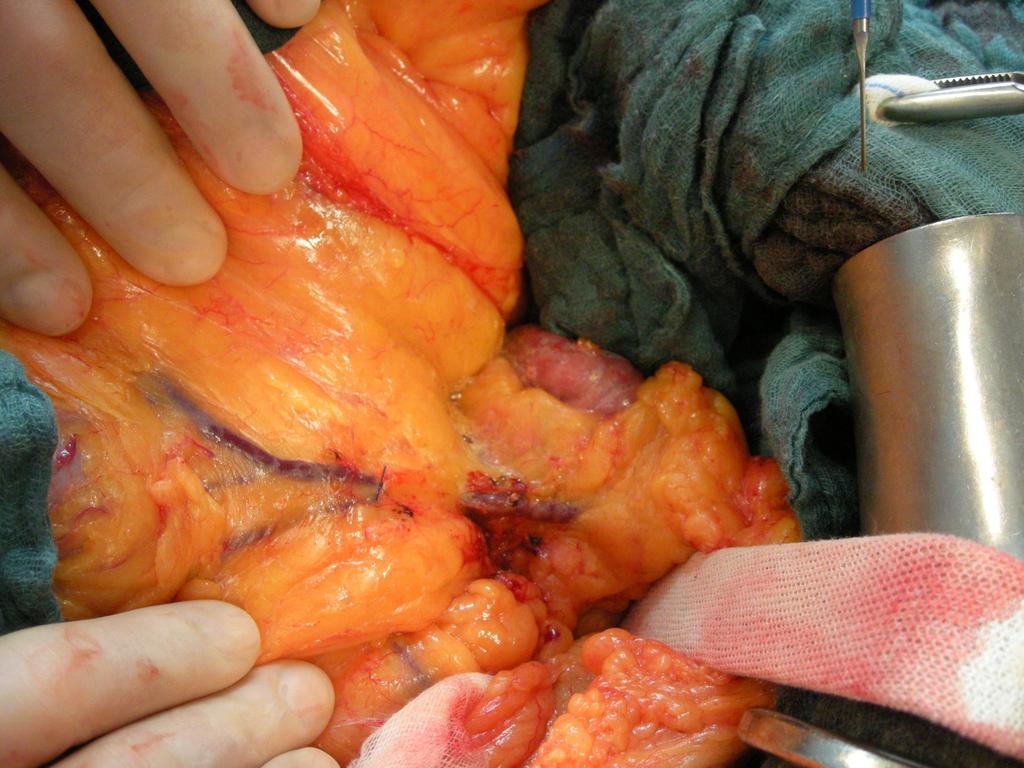
31 Surgery for Colon Cancer Complete Mesocolic Excicion (CME) Preservation of the mesocolic plane by sharp dissection off the parietal plane (turning embryology back) Regional and central lymph node dissection with high tie of suppling vessels
32
33
34
35
36

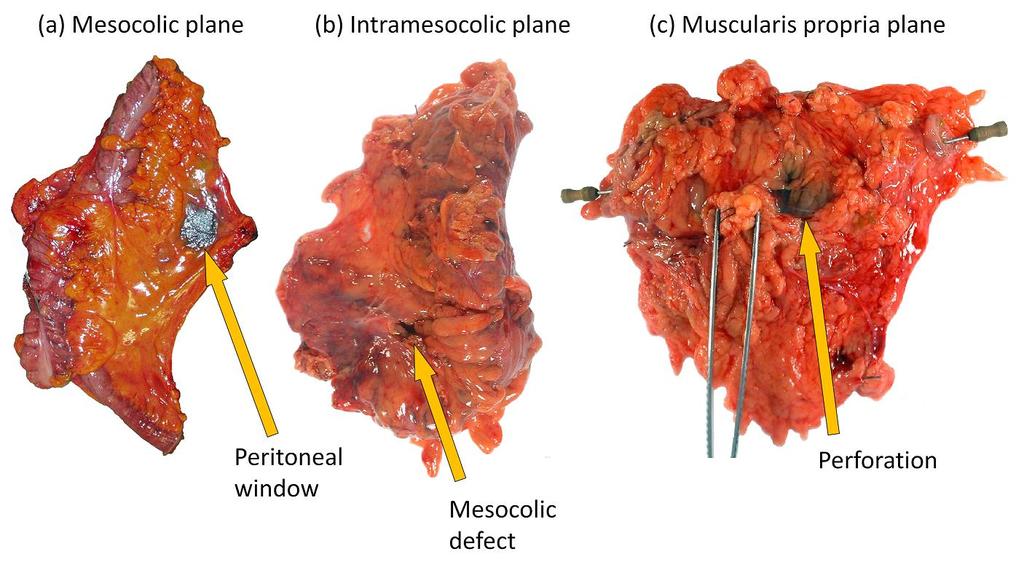
37 Colonic cancer planes of surgery Muscularis propria Intramesocolic Mesocolic plane plane plane Major defects in mesocolon Into mesocolon but not Smooth serosal/mesocolic and down onto down onto the mesentery only very muscularis propria muscularis propria minor defects Muscularis propria plane Intramesorectal plane Mesorectal plane
38 Survival probability Colon Cancer Complete Mesocolic Excision (CME) Quality of Specimen Retrieval Survival stage III cases (n=161) p= Multivariate HR = 0.45 ( ), p= Years Muscularis propria plane Intramesocolic plane Mesocolic plane
39 Universitätsklinikum Erlangen
40 Universitätsklinikum Erlangen
41 Universitätsklinikum Erlangen
42 Universitätsklinikum Erlangen
43 Universitätsklinikum Erlangen
44
45 Plane of colon cancer resections Leeds and Clasicc Plane LGI Clasicc Mesocolic and high tie 0 (0%) 0 (0)% Mesocolic 127 (32%) 41 (25%) Intramesocolic 177 (44%) 86 (53%) Muscularis propria 95 (24%) 35 (22%) Total 399 (100%) 162 (100%) Overall interobserver agreement LGI seriers 85 5%. Phil Quirke and Nick West / Leeds


46 Expert Laparoscopic surgery 69 consecutive laparoscopic CME with CVL cases 3 converted to open surgery 58 invasive cancers Undertook: Tissue morphometry Plane of surgery Lymph node yields Data compared to open gold standard
47 Open vs. laparoscopic Erlangen St. Marks Difference P value Right-sided tumours Tumour to HVT (mm) Length of large bowel (mm) Area of mesentery (mm 2 ) , , Mesocolic plane rate (%) Lymph node yield < Left-sided tumours Tumour to HVT (mm) Length of large bowel (mm) Area of mesentery (mm 2 ) , , , Mesocolic plane rate (%) Lymph node yield <0.0001
48 Japan (open vs. laparoscopic) Open Lap Difference P value Right-sided tumours Tumour to HVT (mm) Length of large bowel (mm) Area of mesentery (mm 2 ) , , Mesocolic plane rate (%) Lymph node yield Left-sided tumours Tumour to HVT (mm) Length of large bowel (mm) Area of mesentery (mm 2 ) , , , < Mesocolic plane rate (%) Lymph node yield
49 Hillerød (open vs. laparoscopic) Open Lap Difference P value Right-sided tumours Tumour to HVT (mm) Length of large bowel (mm) Area of mesentery (mm 2 ) , , , Mesocolic plane rate (%) Lymph node yield Left-sided tumours Tumour to HVT (mm) Length of large bowel (mm) Area of mesentery (mm 2 ) , , , Mesocolic plane rate (%) Lymph node yield
50 Zusammenfassung Variationsbreite der offenen Chirurgie Evidenz der Bedeutung der Dissektionsebene Muscularis propria Intramesokolisch Mesokolon erhalten Komplette Mesokolonexzision als Package Keine Evidenz, daß Laparoskopie unterlegen Qualitätskontrolle durch Pathologie essentiell

51
Kolonkarzinom ist die CME mit CVL schon Standard?
 19.02.2010 Hohenberger Kolonkarzinom ist die CME mit CVL schon Standard? Werner Hohenberger / Erlangen Friedrich-Alexander-Universität Erlangen-Nürnberg Universitätsklinikum Erlangen 19.02.2010 Hohenberger
19.02.2010 Hohenberger Kolonkarzinom ist die CME mit CVL schon Standard? Werner Hohenberger / Erlangen Friedrich-Alexander-Universität Erlangen-Nürnberg Universitätsklinikum Erlangen 19.02.2010 Hohenberger
Komplette Mesokolische Exzision (CME) Ergebnisse und Ausblicke
 Ergebnisse und Ausblicke") Komplette Mesokolische Exzision (CME) Ergebnisse und Ausblicke Werner Hohenberger Chirurgische Universitätsklinik Erlangen Friedrich-Alexander-Universität Erlangen-Nürnberg Colon Cancer Cancer related
Komplette Mesokolische Exzision (CME) Ergebnisse und Ausblicke Werner Hohenberger Chirurgische Universitätsklinik Erlangen Friedrich-Alexander-Universität Erlangen-Nürnberg Colon Cancer Cancer related
Survival after Complete Mesocolic Excision (CME) for Right Sided Coloncancer Compared to Standard Surgery
 for Right Sided Coloncancer Compared to Standard Surgery") Send Orders for Reprints to reprints@benthamscience.net 6 The Open Surgery Journal, 213, 7, 6-1 Open Access Survival after Complete Mesocolic Excision () for Right Sided Coloncancer Compared to Standard
Send Orders for Reprints to reprints@benthamscience.net 6 The Open Surgery Journal, 213, 7, 6-1 Open Access Survival after Complete Mesocolic Excision () for Right Sided Coloncancer Compared to Standard
Current innovations in colorectal surgery
 Current innovations in colorectal surgery KS Chapple Consultant Colorectal Surgeon Sheffield Teaching Hospitals NHS Trust Do we need more innovations? What innovations are there and are they worthwhile?
Current innovations in colorectal surgery KS Chapple Consultant Colorectal Surgeon Sheffield Teaching Hospitals NHS Trust Do we need more innovations? What innovations are there and are they worthwhile?
Yorkshire Cancer Research Yorkshire Bowel Cancer initiative
 Yorkshire Cancer Research Yorkshire Bowel Cancer initiative Phil Quirke, Eva Morris, Paul Finan, Nick West, Penny Wright, David Sebag- Montefiore, Matt Seymour University of Leeds What s the problem? %
Yorkshire Cancer Research Yorkshire Bowel Cancer initiative Phil Quirke, Eva Morris, Paul Finan, Nick West, Penny Wright, David Sebag- Montefiore, Matt Seymour University of Leeds What s the problem? %
Colorectal cancer (CRC) is a common disease in the
 is a common disease in the") ORIGINAL CONTRIBUTION Improving the Quality of Colon Cancer Surgery Through a Surgical Education rogram Nicholas. West, M.B.Ch.B. 1 Kate M. Sutton 1 eter Ingeholm, M.D. 2 Rikke H. Hagemann-Madsen, M.D.
ORIGINAL CONTRIBUTION Improving the Quality of Colon Cancer Surgery Through a Surgical Education rogram Nicholas. West, M.B.Ch.B. 1 Kate M. Sutton 1 eter Ingeholm, M.D. 2 Rikke H. Hagemann-Madsen, M.D.
Complete mesocolic excision for colon cancer is technically challenging but the most oncological appealing
 Editorial Complete mesocolic excision for colon cancer is technically challenging but the most oncological appealing Ionut Negoi 1,2, Mircea Beuran 1,2, Sorin Hostiuc 1,3, Massimo Sartelli 4, Federico
Editorial Complete mesocolic excision for colon cancer is technically challenging but the most oncological appealing Ionut Negoi 1,2, Mircea Beuran 1,2, Sorin Hostiuc 1,3, Massimo Sartelli 4, Federico
Complete Mesocolic Excision
 PHD THESIS DANISH MEDICAL JOURNAL Complete Mesocolic Excision An Assessment of Feasibility and Outcome Claus Anders Bertelsen This review has been accepted as a thesis together with five previously published
PHD THESIS DANISH MEDICAL JOURNAL Complete Mesocolic Excision An Assessment of Feasibility and Outcome Claus Anders Bertelsen This review has been accepted as a thesis together with five previously published
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
How much colon should be resected?
 Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Laparoscopic right-sided colon resection for colon cancer has the control group so far been chosen correctly?
 Pelz et al. World Journal of Surgical Oncology (2018) 16:117 https://doi.org/10.1186/s12957-018-1417-3 RESEARCH Open Access Laparoscopic right-sided colon resection for colon cancer has the control group
Pelz et al. World Journal of Surgical Oncology (2018) 16:117 https://doi.org/10.1186/s12957-018-1417-3 RESEARCH Open Access Laparoscopic right-sided colon resection for colon cancer has the control group
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
editoriale Optimal lymph node dissection for T3-T4 lower rectal cancer, the so-called high risk group: the Japanese experience Introduction
 G Chir Vol. 30 - n. 10 - pp. 393-399 Ottobre 2009 editoriale Optimal lymph node dissection for T3-T4 lower rectal cancer, the so-called high risk group: the Japanese experience M. YASUNO Introduction The
G Chir Vol. 30 - n. 10 - pp. 393-399 Ottobre 2009 editoriale Optimal lymph node dissection for T3-T4 lower rectal cancer, the so-called high risk group: the Japanese experience M. YASUNO Introduction The
12/7/2011. The reporting of colorectal cancer pathology: recent advances. Colorectal cancer resection specimens
 The reporting of colorectal cancer pathology: recent advances Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 Colorectal cancer resection specimens
The reporting of colorectal cancer pathology: recent advances Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 Colorectal cancer resection specimens
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Laparoscopic Wide Mesocolic Excision and Central Vascular Ligation for Carcinoma of the Colon
 646SJS0010.1177/1457496915613646Laparoscopic complete mesocolic excisiona. Ehrlich, M. Kairaluoma, J. Böhm, K. Vasala, H. Kautiainen, I. Kellokumpu Original Article Laparoscopic Wide Mesocolic Excision
646SJS0010.1177/1457496915613646Laparoscopic complete mesocolic excisiona. Ehrlich, M. Kairaluoma, J. Böhm, K. Vasala, H. Kautiainen, I. Kellokumpu Original Article Laparoscopic Wide Mesocolic Excision
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
CRC Surgery Educational Slide Deck. Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto
 CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
SMJ Singapore Medical Journal
 SMJ Singapore Medical Journal ONLINE FIRST PUBLICATION Online first papers have undergone full scientific review and copyediting, but have not been typeset or proofread. To cite this article, use the DOIs
SMJ Singapore Medical Journal ONLINE FIRST PUBLICATION Online first papers have undergone full scientific review and copyediting, but have not been typeset or proofread. To cite this article, use the DOIs
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Department of Surgery, Aizu Central Hospital, Fukushima
 Case Reports Resection of Asynchronous Quadruple Advanced Colonic Carcinomas Followed by Reconstruction with Ileal Interposition between the Transverse Colon and Rectum Sho Mineta 1, Kimiyoshi Shimanuki
Case Reports Resection of Asynchronous Quadruple Advanced Colonic Carcinomas Followed by Reconstruction with Ileal Interposition between the Transverse Colon and Rectum Sho Mineta 1, Kimiyoshi Shimanuki
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Operative Technique: Karen Horvath, MD, FACS. SCOAP Retreat June 17, 2011
 Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
New ports placement in laparoscopic central lymph nodes dissection with left colic artery preservation for sigmoid colon and rectal cancer
 223 ORIGINAL New ports placement in laparoscopic central lymph nodes dissection with left colic artery preservation for sigmoid colon and rectal cancer Jun Higashijima, Mitsuo Shimada, Takashi Iwata, Kozo
223 ORIGINAL New ports placement in laparoscopic central lymph nodes dissection with left colic artery preservation for sigmoid colon and rectal cancer Jun Higashijima, Mitsuo Shimada, Takashi Iwata, Kozo
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
COLORECTAL CANCER: PROGNOSTIC VALUES
 & COLORECTAL CANCER: PROGNOSTIC VALUES Suzana Manxhuka-Kerliu¹*, Skender Telaku², Halil Ahmetaj³, Arijeta Baruti¹, Sadushe Loxha¹, Agron Kerliu³ ¹ Institute of Pathology, Faculty of Medicine, University
& COLORECTAL CANCER: PROGNOSTIC VALUES Suzana Manxhuka-Kerliu¹*, Skender Telaku², Halil Ahmetaj³, Arijeta Baruti¹, Sadushe Loxha¹, Agron Kerliu³ ¹ Institute of Pathology, Faculty of Medicine, University
Colorectal cancer: pathology
 UK NEQAS for Molecular Pathology Colorectal cancer: pathology Nick West Pathology & Tumour Biology May 2013 Colorectal cancer (CRC) 40,695 new cases in 2010 15,708 deaths Management of CRC Surgery Main
UK NEQAS for Molecular Pathology Colorectal cancer: pathology Nick West Pathology & Tumour Biology May 2013 Colorectal cancer (CRC) 40,695 new cases in 2010 15,708 deaths Management of CRC Surgery Main
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
3rd Annual Minimally Invasive Approaches to Rectal Cancer Symposium
 presents Minimally Invasive Approaches to Rectal Cancer Symposium May 3 & 4, 2019 InterContinental Hotel and Conference Center Cleveland, Ohio Hands On Lab Limited slots available Register today! ccfcme.org/rectal2019
presents Minimally Invasive Approaches to Rectal Cancer Symposium May 3 & 4, 2019 InterContinental Hotel and Conference Center Cleveland, Ohio Hands On Lab Limited slots available Register today! ccfcme.org/rectal2019
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Differential lymph node retrieval in rectal cancer: associated factors and effect on survival
 Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Long-term follow-up of the Medical Research Council CLASICC trial of conventional versus laparoscopically assisted resection in colorectal cancer
 Original article Long-term follow-up of the Medical Research Council CLASICC trial of conventional versus laparoscopically assisted resection in colorectal cancer B. L. Green 1, H. C. Marshall 1, F. Collinson
Original article Long-term follow-up of the Medical Research Council CLASICC trial of conventional versus laparoscopically assisted resection in colorectal cancer B. L. Green 1, H. C. Marshall 1, F. Collinson
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases
 J Rural Med 2014; 9(1): 20 26 Original article Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases Eiichi Yabata, Masaru Udagawa and Hiroyuki
J Rural Med 2014; 9(1): 20 26 Original article Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases Eiichi Yabata, Masaru Udagawa and Hiroyuki
Seventh Edition Staging 2017 Colorectum. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY
 PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
A study evaluating the safety of laparoscopic radical operation for colorectal cancer
 Original Article A study evaluating the safety of laparoscopic radical operation for colorectal cancer Min-Hua Zheng, Ai-Guo Lu, Bo Feng, Yan-Yan Hu, Jian-Wen Li, Ming-Liang Wang, Feng Dong, Jing-Li Cai,
Original Article A study evaluating the safety of laparoscopic radical operation for colorectal cancer Min-Hua Zheng, Ai-Guo Lu, Bo Feng, Yan-Yan Hu, Jian-Wen Li, Ming-Liang Wang, Feng Dong, Jing-Li Cai,
The main issues of the rectal resection for carcinoma
 The main issues of the rectal resection for carcinoma - Level of the vessels transection and mobilisation of the splenic flexure - Lymphadenectomy - Distal margin - Parietal invasion of rectal wall - Functional
The main issues of the rectal resection for carcinoma - Level of the vessels transection and mobilisation of the splenic flexure - Lymphadenectomy - Distal margin - Parietal invasion of rectal wall - Functional
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Cover Page. The following handle holds various files of this Leiden University dissertation:
 Cover Page The following handle holds various files of this Leiden University dissertation: http://hdl.handle.net/1887/6119 Author: Spruit, E.N. Title: Increasing the efficiency of laparoscopic surgical
Cover Page The following handle holds various files of this Leiden University dissertation: http://hdl.handle.net/1887/6119 Author: Spruit, E.N. Title: Increasing the efficiency of laparoscopic surgical
TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy
 TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy Nam Kyu Kim M.D., Ph.D., FACS, FRCS, FASCRS Professor Department of Surgery Yonsei University College of Medicine Seoul,
TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy Nam Kyu Kim M.D., Ph.D., FACS, FRCS, FASCRS Professor Department of Surgery Yonsei University College of Medicine Seoul,
Laparoscopic total mesorectal excision (TME) with electric hook for rectal cancer
 with electric hook for rectal cancer") Technical Note Page 1 of 8 Laparoscopic total mesorectal excision (TME) with electric hook for rectal cancer Gong Chen, Rong-Xin Zhang, Zhi-Tao Xiao Department of Colorectal Surgery, Sun Yat-sen University
Technical Note Page 1 of 8 Laparoscopic total mesorectal excision (TME) with electric hook for rectal cancer Gong Chen, Rong-Xin Zhang, Zhi-Tao Xiao Department of Colorectal Surgery, Sun Yat-sen University
The Examination of Lymph Nodes Following. Surgery for Colorectal Cancer
 The Examination of Lymph Nodes Following Surgery for Colorectal Cancer Martyn Dominic Evans BM, FRCS (Gen Surg) A thesis presented for the degree of Master of Philosophy School of Medicine Cardiff University
The Examination of Lymph Nodes Following Surgery for Colorectal Cancer Martyn Dominic Evans BM, FRCS (Gen Surg) A thesis presented for the degree of Master of Philosophy School of Medicine Cardiff University
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
ESSO-EYSAC Course on Colorectal Cancer Surgery
 ESSO-EYSAC Course on Colorectal Cancer Surgery 21-23 January 2016 LJUBLJANA (SI) Young Surgeons & Alumni Club ESSO-EYSAC Course on Colorectal Cancer Surgery Chairs Ibrahim Edhemovic, Institute of Oncology
ESSO-EYSAC Course on Colorectal Cancer Surgery 21-23 January 2016 LJUBLJANA (SI) Young Surgeons & Alumni Club ESSO-EYSAC Course on Colorectal Cancer Surgery Chairs Ibrahim Edhemovic, Institute of Oncology
All along the colon: multimodality imaging and staging
 Satellite Symposium ESGAR 2011 All along the colon: multimodality imaging and staging Chairman: Prof. T. Lauenstein (Essen Germany) Invitation Sunday, May 22 nd, 2011 13:00-14:00 Venice Convention Centre,
Satellite Symposium ESGAR 2011 All along the colon: multimodality imaging and staging Chairman: Prof. T. Lauenstein (Essen Germany) Invitation Sunday, May 22 nd, 2011 13:00-14:00 Venice Convention Centre,
Neoadjuvant Therapy for Rectal Cancer is Overrated. Joon H. Lee, Research Resident University of Colorado 8/31/2009
 Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Radical lymph node resection of the retroperitoneal area for left-sided colon cancer
 Langenbecks Arch Surg (2007) 392:155 160 DOI 10.1007/s00423-006-0143-4 ORIGINAL ARTICLE Radical lymph node resection of the retroperitoneal area for left-sided colon cancer Antonios-Apostolos K. Tentes
Langenbecks Arch Surg (2007) 392:155 160 DOI 10.1007/s00423-006-0143-4 ORIGINAL ARTICLE Radical lymph node resection of the retroperitoneal area for left-sided colon cancer Antonios-Apostolos K. Tentes
WHICH LYMPH NODES SHOULD BE
 Y.K.: 82 Y.O. WOMAN WITH ANEMIA No GI symptoms. Chronic AF taking coumadin: INR=2.1. HCT=24. Anemia persists despite Rx. Colonoscopy: tumor in ascending colon. Bx: adenocarcinoma. Rx: Laparoscopic right
Y.K.: 82 Y.O. WOMAN WITH ANEMIA No GI symptoms. Chronic AF taking coumadin: INR=2.1. HCT=24. Anemia persists despite Rx. Colonoscopy: tumor in ascending colon. Bx: adenocarcinoma. Rx: Laparoscopic right
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Anatomy of the spleen. Oluwadiya KS
 Anatomy of the spleen Oluwadiya KS www.oluwadiya.com Introduction The spleen is an ovoid, usually purplish, pulpy mass about the size and shape of one's fist. It is the largest lymphoid tissue in the body
Anatomy of the spleen Oluwadiya KS www.oluwadiya.com Introduction The spleen is an ovoid, usually purplish, pulpy mass about the size and shape of one's fist. It is the largest lymphoid tissue in the body
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
The effect of rectal washout on local recurrence following rectal cancer surgery
 COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
COLORECTAL SURGERY Ann R Coll Surg Engl 208; 00: 46 5 doi 0.308/rcsann.207.0202 The effect of rectal washout on local recurrence following rectal cancer surgery SR Moosvi, K Manley, J Hernon Norfolk and
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Outcome following surgery for colorectal cancer
 Outcome following surgery for colorectal cancer Colin S McArdle* and David J Hole *University Department of Surgery, Glasgow Royal Infirmary, Glasgow and Department of Public Health, University of Glasgow,
Outcome following surgery for colorectal cancer Colin S McArdle* and David J Hole *University Department of Surgery, Glasgow Royal Infirmary, Glasgow and Department of Public Health, University of Glasgow,
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Amy S. Izon, Paul Jose, Jeremy D. Hayden & Heike I. Grabsch
 Significant Variation of Resected Mesoesophageal Tissue Volume in Two-Stage Subtotal Esophagectomy Specimens: A Retrospective Morphometric Study Amy S. Izon, Paul Jose, Jeremy D. Hayden & Heike I. Grabsch
Significant Variation of Resected Mesoesophageal Tissue Volume in Two-Stage Subtotal Esophagectomy Specimens: A Retrospective Morphometric Study Amy S. Izon, Paul Jose, Jeremy D. Hayden & Heike I. Grabsch
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
World Journal of Colorectal Surgery Volume 3, Issue 4 2013 Article 3 Sigmoidorectal Intussusception Presenting as Prolapse Per Anus in an Adult Venugopal Hg Hasmukh B. Vora Mahendra S. Bhavsar SMT.NHL
11/09/2014. Update Management of Rectal Cancer. Outline. I have no disclosures
 Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT?
 DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
DOES LOCATION MATTER IN COLORECTAL CANCER: LEFT VS RIGHT? By: Dr. Dominik Modest, Medical Department III, Hospital of the University of Munich, Germany Dr. Andrea Sartore-Bianchi, Niguarda Cancer Center,
Innovations in rectal cancer surgery TAMIS and transanal TME
 Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Innovations in rectal cancer surgery TAMIS and transanal TME A.D Hoore MD PhD, EBSQ CR Chair Departement of Abdominal Surgery University Hospitals Leuven, Belgium Actual treatment in rectal Early rectal
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Rectal Cancer. Rectal Cancer: The CCF perspective 16/11/2017. Meagan Costedio, MD, FACS, FASCRS. 38,220 new cases estimated in
 Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
Purpose. Encourage standard exchange of data between two key public health partners
 Reporting Pathology Protocols for Colorectal Cancer 2005 NAACCR Conference: June 9, 2005 Ken Gerlach: CDC-NPCR Bette Smith: Ohio Cancer Registry Kathleen Davidson-Allen: PHI/California Cancer Registry
Reporting Pathology Protocols for Colorectal Cancer 2005 NAACCR Conference: June 9, 2005 Ken Gerlach: CDC-NPCR Bette Smith: Ohio Cancer Registry Kathleen Davidson-Allen: PHI/California Cancer Registry
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January