Controversies in Gastroenterology in Asia
|
|
|
- Sara Ball
- 6 years ago
- Views:
Transcription

1 June 13-15, 2013 Berlin, Germany Prof. Joseph Sung The Chinese University of Hong Kong Controversies in Gastroenterology in Asia Disclosure of Potential Conflict of Interest: Nothing to Disclose
2 June 13-15, 2013 Berlin, Germany Controversies in Gastroenterology in Asia 1. Is PPI response different in Asia? 2. Is IBD rare in Asia? 3. Is flat lesions in colon a special feature in Asia?
3 Patients With Recurrent Rebleeding (%) IV Omeprazole Effect on Rebleeding Rates in High-Risk Patients With PUD After Endoscopic Therapy 25% 20% Endoscopy + IV omeprazole Endoscopy + placebo 21.7% 20.0% 22.5% Omeprazole Rx Reduced 15% Endosc. retreat. P < % 5% 4.2%* 5.8%* 6.7%* Transfusions P = 0.03 Length of stay P = % 3 Days 7 Days 30 Days *P <0.001 vs endoscopy + placebo. Lau JYW, et al. N Engl J Med. 2000;343:
4 Median units IV PPI reduces need of endoscopic re-rx and transfusion Omeprazole Placebo Omeprazole Placebo 25 P< P= Endoscopic retreatment Transfusion 4
5 PPI effects: Asian=European Europe Asia Brunner Cardi Corragio Daneshmend Desprez Fried Lanas Michel Perez Flores Schaffalitsky Villanueva Hasselgren Odds Ratio, 95% CI Javid Kaviani Khuroo Lau Lin Sheu Odds Ratio, 95% CI 62/852 vs. 39/ (1.11, 2.55) 8/519 vs. 25/ (0.16, 0.73) Favors treatment Favors control P= Favors treatment Favors control P=.006
6 PUB Study: IV Nexium vs Placebo Randomised, double-blind, placebo-controlled study at 91 centres in 16 countries i.v. treatment (72 hours) Oral treatment (27 days) Endoscopic Haemostasis 1. Single 2. Combo R Esomeprazole i.v. 80 mg over 30 min followed by esomeprazole i.v. 8 mg/h for 71.5 hours Placebo i.v. for 30 min followed by placebo for 71.5 hours Esomeprazole 40 mg qd Just like any other PPI, esomeprazole is not indicated for the management of peptic ulcer bleeding in the world including Malaysia ClinicalTrials.gov identifier: NCT Sung et al. Ann Intern Med 2009 Apr 7;150(7):
7 Significantly less rebleeding with IV Nexium (ITT Population) Esomeprazole Placebo P value (n=375) (n=389) Re-bleed, n 22 (5.9%) 40 (10.3%) % CI 3.7% 8.8% 7.5% 13.7% Risk reduction: 43% (PP Population) Esomeprazole Placebo P value (n=292) (n=316) Re-bleed, n 14 (4.8%) 33 (10.4%) % CI 2.6% 7.9% 6.9% 14% Risk reduction: 54% Sung et al. Ann Intern Med 2009;150:
8 Cumulative percentage (%) Re-bleeding Within 30 Days (ITT Population) Placebo 13.6% (n=53) Log-rank p= Esomeprazole 7.7% (n=29) Days from randomisation Sung et al. Ann Intern Med 2009 Apr 7;150(7):
9 Benefit irrespective of endsocopic Rx Esomeprazole n=375 Placebo n=389 Endoscopy treatment Single Rebleed No rebleed 9 (5.1) 166 (94.9) 17 (9.4) 163 (90.6) Combination Rebleed No rebleed 12 (6.3) 180 (93.8) 21 (10.5) 179 (89.5) Sung et al. Ann Intern Med 2009 Apr 7;150(7):455-64
10 Benefit more Hp positive patients Esomeprazole n=375 Placebo n=389 Hp status Negative Rebleed No rebleed 9 (9.8) 83 (90.2) 14 (11.8) 105 (88.2) Positive Rebleed No rebleed 9 (3.7) 237 (96.3) 19 (8.4) 207 (91.6) Sung et al. Ann Intern Med 2009 Apr 7;150(7):455-64
11 Oral PPI Solutions in Prevention of Rebleeding From PUD Study Endo Rx Drug/Regimen N Rebleeding P Value Comments Kuroo 1 None Omeprazole 40 mg q12hr x 5 days % Placebo % <0.001 >benefit VV, clots ARR = 25.5 NNT = 3 Javid 2 Omeprazole 40 mg q12hr x 5 days % Placebo % 0.02 ARR = 14 NNT = 7 Kaviani 3 Omeprazole 40 mg q12hr x 5 days % Placebo % ARR = 16 NNT = 6 1. Khuroo M, et al. N Engl J Med. 1997;336: Javid G, et al. Am J Med. 2001;111: Kaviani MJ, et al. Aliment Pharmacol Ther. 2003;17: VV, visible vessel. ARR, absolute risk reduction. NNT, number needed to treat.
12 Study period : Jan 1, 2008 to Sept 24, 2011 Sung et al. UEGW screened 215 randomized 348 not randomized 108 no consent 88 other clinical trials 56 On PPI 33 moribund 16 Failed endoscopic Px 6 suspected perforated ulcers 14 Previous gastric surgery 12 unable to withhold antiplatelet agent 15 other treatments 10 Cancer of stomach 105 IV 110 Oral 2 did not start treatment Acute coronary syndrome, antiplatelet agents cont d 2 Lymphoma of stomach 1 Disseminated lung cancer 95 analyzed 105 analyzed
13 Severity of Bleeding and Ulcer Characteristics Sung et al. UEGW 2012 Intravenous n=95 Oral n=105 Gastric Ulcer n, % 41 (43.2) 45 (42.9) Ulcer size >2cm n, % 14 (14.7) 15 (14.3) Helicobacter pylori infection n, % 35 (36.8) 40 (38.1) Stigmata of bleeding n Visible Vessel Clot Oozing Spurter Systolic BP < 100 mmhg n, % 18 (18.9) 24 (22.9) Hb < 9 g/dl n, % 43 (45.3) 40 (38.1) Blood transfusion before endoscopy N, % 38 (40) 51 (48.6)

14 Recurrent bleeding in 30 days Oral PPI Intravenous PPI P = 0.8, Log rank test Days Number at risk Oral IV Sung et al. UEGW 2012
15 Secondary outcomes Intravenous PPI N=95 Oral PPI N=105 P Hospital stay (days) Mean (S.D) median (range) ICU admission (no. of days) ICU admission (no. of patients) 6.2 (4.6) 4 (1-35) (3.3) 5 (3-26) Blood transfusion (units) Post randomization median (range) 2 (0-14) 1 (0-13) 0.14 Unscheduled second look EGD 2 nd endoscopic treatment Angiographic embolization Surgery 1 0 -
16 Early Administration of High-dose Intravenous Omeprazole Prior to Endoscopy in Patients with Upper Gastrointestinal Bleeding: A Double-blind Placebo-controlled Randomized Trial James Y Lau, Wai-K Leung, Justin C Wu, Francis KL Chan, Vincent Wong, Lawrence Hung, Ka-Y Cheung, Man-Y Yung, Vivian W Lee#, Philip W Chiu, Enders K Ng, Kenneth KK Lee#, Joseph JY Sung Institute of Digestive Disease and School of Pharmacy #, the Chinese University of Hong Kong, Hong Kong SAR, China N Engl J Med
17 Pre-endoscopy PPI may reduce the use of endoscopic hemostasis Omeprazole Placebo P, OR (95%CI) N=179 N=190 Endoscopy therapy n, % bleeding ulcers Others 28, 15.6% , 31.1% , 2.4 (1.5-4) Urgent intervention Surgery for hemostasis Rebleeding in 30 days day mortality
18 Pre-endoscopy PPI may reduce the use of endoscopic hemostasis Omeprazole N=179 Placebo N=190 P Mean *VAS for endoscopic therapy in cm, SD 3.7, , Blood transfusion Mean, SD 1.7, , Median range 0, , Hospital stay (all patients) Mean, SD 4.2, , Median, range 3, , Hospital stay (out-bleeders) Mean, SD 3.8, , Median, range 3, , *VAS: visual analogue scale 18
19 Outcomes of patients with PUB Endoscopic treatment n, % Signs of bleeding Spurting / oozing NBVV Clots Flat pigments Clean base Omeprazole N=110 Placebo N=112 P OR (95%CI) 19, 17.2% 40, 35.7%.002, 2.6 (1.4-5) Urgent intervention Surgery

20 Global Map of Inflammatory Bowel Disease Cosnes et al. Gastroenterology 2010; Ng et al. Gut 2013 >10 per 100,000 <4 per 100, per 100,000

21 IBD Epidemiology Worldwide Molodecky et al. Gastroenterology 2012 High Incidence 20-25/100,000 Low Incidence <5/100,000 Canada United States Europe Asia South America Africa High Incidence 10-25/100,000 Australia New Zealand
22 IBD in Hong Kong (Leong et al. 2003) hospital-based UC CD UC in Korea (Yang et al.2008) Songpa-Kangdong district UC in Japan (National IBD Registry) Goh et al. Inflamm Bowel Dis 2004
23 Why is it Important to Understand the True Incidence of IBD in Asia? 4.2 billion people live in the Asia-Pacific region (61% of the world's population) Estimate disease burden Anticipate healthcare needs Better understanding of causative factors
24 Epidemiology of IBD in Asia Limited prospective, population-based, incidence data Most reports hospital-based Little known of regional differences in disease phenotype and severity at presentation


25 Gastroenterology 2013 (epub ahead of print)
26 Study Aim To prospectively investigate the incidence of IBD across 9 countries in Asia-Pacific To determine the phenotype of IBD at diagnosis in Asia

27 Background Study Population China Guangzhou 2.6X10 6 Chengdu 2.7X10 6 Xian 8.9X10 6 Thailand Chiangmai 1.6X10 6 Bangkok 3.9X10 6 Hong Kong 3.2X10 6 Macau 5X10 5 Sri Lanka 2.2X10 6 Malaysia 8.5X10 5 Singapore 3.7X10 6 Indonesia 9X10 5 Australia Melbourne 3X10 5
28 Case Identification Diagnostic criteria Gastroenterologists, pediatricians, surgeons, radiologists, and pathologists within each hospital Suspected incident cases Referred to gastroenterologist Clinical diagnosis of IBD Reminder to all doctors every month Main investigators meet every 3 months to review case notes Cross-checking Exclude if diagnosis uncertain Follow up review of case notes 3-6 months after diagnosis Confirmed diagnosis of IBD A retrospective search of all histology reports, colonoscopy reports, medical records and pharmacy records at each hospital
29 Results 419 new IBD cases 232 (55.4%) ulcerative colitis 166 (39.6%) Crohn s disease 21 (5.0%) indeterminate colitis 58% of patients were male Median age at diagnosis was 39 years (range, 5 to 81)
30 Crude Annual Incidence of IBD (per 100,000) Ng et al. Gastroenterology 2013 (epub ahead of print) Country Crude annual incidence (per 100,000 persons) 95% confidence interval Australia Mainland China (Guangzhou) Hong Kong Macau Sri Lanka Singapore Malaysia Indonesia Thailand (Chiangmai) Thailand (Bangkok) Mainland China (Chengdu) Mainland China (Xian)
31 Ratio of Ulcerative colitis : Crohn s disease Country Ulcerative Colitis Crohn s disease UC/CD Ratio Australia Mainland China (Guangzhou) Hong Kong Macau Sri Lanka Singapore Malaysia Indonesia Thailand (Chiangmai) Thailand (Bangkok) Mainland China (Chengdu) Mainland China (Xian)
32 Disease Demographics Australia Asia P Value N (%) N (%) Age, (mean± SD) (18.67) (15.96) Sex (male) 35 (49%) 209 (60%) Median time from 5 (1-15) 6 (3-24) symptom onset to diagnosis, months (IQR) Smoking history Current Ex Never 8(11%) 19 (26%) 45 (63%) 28 (8%) 70 (20%) 250 (72%) Family history of IBD 12 (17%) 10 (3%) <0.001 Diagnosis as inpatient 18 (25%) 97 (28%) 0.637
 Location of disease Colon alone 19 (24%) Ileocolonic 40 (50%) Proximal to TI 14")
33 Isolated terminal ileal disease is uncommon Crohn s disease Terminal ileum alone 4 (5%) Location of disease Colon alone 19 (24%) Ileocolonic 40 (50%) Proximal to TI 14 (18%)



34 Colon involvement is more common Crohn s disease Location of disease Hong Kong Minnesota Ileum Colon Ileocolon Proximal
35 Disease Phenotype at Diagnosis CD location L1 (Terminal ileum) L2 (Colon) L3 (Ileocolon) L4 (Upper gastrointestinal) Australia N (%) 13 (31%) 10 (24%) 19 (45%) 2 (5%) Asia N (%) 38 (31%) 30 (24%) 56 (45%) 6 (5%) P Value CD behavior B1 (Inflammatory) B2 (Stricturing) B3 (Penetrating) B1p (Perianal) 37 (88%) 4 (10%) 1 (2%) 5 (12%) 82 (66%) 21 (17%) 23 (19%) 22 (18%) UC location E1 (Proctitis) E2 (Distal) E3 (Extensive) 7 (32%) 6 (27%) 9 (41%) 78 (37%) 67 (32%) 65 (31%)
36 Proportion (%) Evolution of disease behavior as determined by the Montreal Classification over 10 years in Chinese patients with Crohn s Disease. Chow et al. Inflamm Bowel Dis B1 Nonstricturing, nonpenetrating B2 Stricturing B3 Penetrating Time (years) (P = 0.025) (P = 0.005)
37 Cumulative survival of Chinese CD patients free from major surgery upon 10 years of follow-up Chow and Sung et al. Inflamm Bowel Dis 2008
38 Cumulative colectomy-free survival in the Chinese UC patients Chow and Sung et al. Am J Gastroenterol 2009
39 CRC Incidence Globocan 2013 Man Woman

40 Colorectal Cancer in Asia F e m a le M a le J a p a n, N a g a s a k i C ity J a p a n, M iya g i P re fe c tu re J a p a n, Y a m a g a ta P re fe c tu re S in g a p o re : C h in e s e J a p a n, O s a k a P re fe c tu re C h in a, H o n g K o n g P h ilip p in e s, M a n ila C h in a, S h a n g h a i S in g a p o re : M a la y C h in a, T ia n jin S in g a p o re : In d ia n T h a ila n d, C h ia n g M a i C o lo n R e ctu m In d ia, B o m b a y U K, S o u th T h a m e s R e g io n U S A, S E E R : W h ite C a n a d a U K, S c o tla n d U S A, S E E R : B la c k A g e -sta n d a rd ize d ra te (p e r 1 0 0,0 0 0 ) Sung et al. Lancet Oncology Lan

41 Asian Pacific Working Group Studies 860 asymptomatic subjects underwent colonoscopy in 11 cities Advanced neoplasm found in 4.5% 1.8% of proximal advanced neoplasm found in the absence of distal lesion
42 Adenoma: Screening Population (N=860) All Adenoma (%) Adv Neoplasm (%) Invasive Cancer (%) Distal Colon 76 (8.8) 19 (2.1) 6 (0.7) Proximal Colon 66 (7.7) 17 (2.0) 3 (0.3) Synchronous Lesions 26 (3.0) 3 (0.3) 0 (0) Total 168 (18.5) 39 (4.5) 9 (1.0) Byeon et al. GIE 2006




43 Pathway of colorectal carcinogenesis Adenoma-carcinoma sequence De novo pathway



44 Evidence of de novo Cancer Type I pits Type IIIs pits





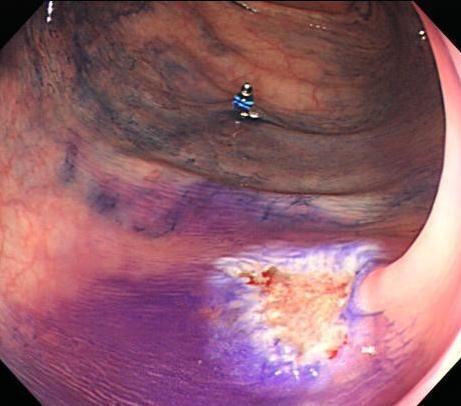
45 Flat adenoma: more difficult to find, but more dangerous lesions Chiu et al. Gut 2007
46 How common is flat and depressed lesion? Japan multi-center data Center Prevalence of depressed lesion Percentage of high grade dysplasia NCCH 2.7% (154/5634) 55.3% (47/85) Showa Univ. 2.4% (443/18310) 45.3% (139/307) Hiroshima Univ. 2.3% (187/8035) 56.8% (75/132) Tama Cancer Center 1.6% (219/13960) 61.0% (89/146) NCCHE 1.6% (128/8234) 41.0% (32/78) Kobe Univ. 1.5% (63/4154) 52.2% (12/23) Sapporo Kosei 1.4%(73/5092) 62.5% (30/48) JR Sendai 0.7% (24/3251) 60.0% (3/5) Prevalence: 1.89% (95%CI: %)
47 Is this a Japanese disease only? Western data Soetikno R et al, Gastroenterol 2006 Authors (country) and number of patients studied Jaramillo (Sweden) N = 232 Fujii (UK) N = 208 Rembacken (UK) N = 1000 Saitoh (US) N = 211 Tsuda (Sweden) N = 973 Hurlstone(UK) N = 850 % of patients with NP- CRN % of all CRN with non polypoid morphology % of all NP-CRN with high-grade dysplasia, % of flat NP-CRN with submucosal invasive carcinoma % of depressed NP-CRN with submucosal invasive carcinoma Not stated Not stated Not stated Not stated

48 New endoscopic modalities: is it better?
49 Performance of different modalitis Sensitivity (%) Specificity (%) Accuracy (%) PPV (%) NPV (%) Likelihood Ratio Endoscopic Modality Reader 1 Reader 2 Reader 1 Reader 2 Reader 1 Conventional colonoscopy NBI-Low NBI-High Chromoendoscop y-l Chromoendoscop y-h Reader 2 Reader 1 Reader 2 Reader 1 Reader 2 Reader 1 Reader 2 Chiu Chiu HM et al. Gut (in press)
50 CRC Screening Recommendation CTC Polyp <5mm 1-2 Polyp 6-9mm 3 Polyp 6-9mm Polyp >10mm Need not be reported Continue CTC Surveillance in 3 years Polypectomy Polypectomy Repeat CTC In 5-10 years Repeat colonoscopy in 3 years if 1. Adenoma >10mm 2. >3 adenoma, 3. Villous architecture in adenoma Zalis et al. Radiology 2005;236:
51 Distribution of Patients on ACR Recommendations (Overall, n=1,752) no. of patients 5 mm mm 10 mm Any size 1 to 2 polyp(s): All Adenoma ACN 3 polyps or more: All Adenoma ACN Any number of polyps: All Adenoma ACN (57.6%) 140 (84.3%) 63 (82.9%) 377 (69.3%) 3 (1.0%) 19 (11.4%) 66 (86.8%) 88 (16.2%) (61.1%) 2 (3.7%) (58.1%) 5 (1.4%) 10 9 (90%) 4 (40%) 5 5 (100%) 5 (100%) (68.1%) 11 (15.9%) (84.7%) 68 (84.0%) 424 (69.2%) 23 (13.1%) 61 (75.3%) 89 (14.5%) Sung et al. CGH % 21.3% 51
52 June 13-15, 2013 Berlin, Germany Controversies in Gastroenterology in Asia 1. Is PPI response different in Asia? 2. Is IBD rare in Asia? 3. Is flat lesions in colon a special feature in Asia?
Helicobacter pylori. Objectives. Upper Gastrointestinal Bleeding Peptic Ulcer Disease
 Upper Gastrointestinal Bleeding Peptic Ulcer Disease Pharmacotherapy Issues in Acute Management and Secondary Prevention Peter J. Zed, B.Sc., B.Sc.(Pharm), Pharm.D. Pharmacotherapeutic Specialist - Emergency
Upper Gastrointestinal Bleeding Peptic Ulcer Disease Pharmacotherapy Issues in Acute Management and Secondary Prevention Peter J. Zed, B.Sc., B.Sc.(Pharm), Pharm.D. Pharmacotherapeutic Specialist - Emergency
Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication
 Aliment Pharmacol Ther 2004; 19 (Suppl. 1): 66 70. Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication G. HOLTMANN* & C. W. HOWDEN
Aliment Pharmacol Ther 2004; 19 (Suppl. 1): 66 70. Review article: management of peptic ulcer bleeding the roles of proton pump inhibitors and Helicobacter pylori eradication G. HOLTMANN* & C. W. HOWDEN
Occult small bowel bleeding - Video capsule first
 Occult small bowel bleeding - Video capsule first Prof. Joseph Sung The Chinese University of Hong Kong Disclosure of Potential Conflict of Interest: Nothing to Disclose Obscure Gastrointestinal Bleeding
Occult small bowel bleeding - Video capsule first Prof. Joseph Sung The Chinese University of Hong Kong Disclosure of Potential Conflict of Interest: Nothing to Disclose Obscure Gastrointestinal Bleeding
Simon Everett. Consultant Gastroenterologist, SJUH, Leeds. if this is what greets you in the morning, you probably need to go see a doctor
 Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Simon Everett Consultant Gastroenterologist, SJUH, Leeds if this is what greets you in the morning, you probably need to go see a doctor Presentation Audit data and mortality NICE guidance Risk assessment
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding
 ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding Loren Laine, MD 1,2 and Dennis M. Jensen, MD 3 5 1 Section of Digestive Diseases, Yale University School of Medicine, New Haven, Connecticut,
In What Asia-Pacific Populations is CRC Screening Justified?
 WEO CRC SC Meeting APDW Taipei, December 3, 2015 In What Asia-Pacific Populations is CRC Screening Justified? K.G. YEOH MBBS, MMed, FRCP (London), FRCP (Glasg), FAMS Dean, NUS School of Medicine, Senior
WEO CRC SC Meeting APDW Taipei, December 3, 2015 In What Asia-Pacific Populations is CRC Screening Justified? K.G. YEOH MBBS, MMed, FRCP (London), FRCP (Glasg), FAMS Dean, NUS School of Medicine, Senior
Scottish Medicines Consortium
 Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
Scottish Medicines Consortium esomeprazole, 40mg vial of powder for solution for intravenous injection or infusion (Nexium I.V. ) No. (578/09) AstraZeneca 09 October 2009 The Scottish Medicines Consortium
New Techniques. Incidence of Peptic Ulcer. Changing. Contents - with an emphasis on peptic ulcer bleeding. Cause of death in peptic ulcer bleeding
 Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
Contents - with an emphasis on peptic ulcer bleeding New Techniques in Treating GI Bleeding Incidence and cause of death Acid suppression Endoscopic hemostasis Prediction of rebleeding and death Second
T he aim of a scheduled second endoscopy is to detect and
 1403 STOMACH Effect of scheduled second therapeutic endoscopy on peptic ulcer rebleeding: a prospective randomised trial P W Y Chiu, C Y W Lam, S W Lee, K H Kwong, S H Lam, D T Y Lee, S P Y Kwok... See
1403 STOMACH Effect of scheduled second therapeutic endoscopy on peptic ulcer rebleeding: a prospective randomised trial P W Y Chiu, C Y W Lam, S W Lee, K H Kwong, S H Lam, D T Y Lee, S P Y Kwok... See
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
Improved risk assessment in upper GI bleeding
 EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
EDITORIAL Improved risk assessment in upper GI bleeding Acute upper GI bleeding is the most common GI emergency, with a reported incidence in various epidemiological studies ranging from 50 to over 100
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Chromoendoscopy - Should It Be Standard of Care in IBD?
 Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
Chromoendoscopy - Should It Be Standard of Care in IBD? John F. Valentine, MD, FACG Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Utah What is the point of
James Irwin Gastroenterology Department Palmerston North Hospital. Acute Medicine Meeting Hutt Hospital. June 21, 2015
 The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
The Management of Acute Upper Gastrointestinal Bleeding James Irwin Gastroenterology Department Palmerston North Hospital Acute Medicine Meeting Hutt Hospital June 21, 2015 Outline Common Definitions and
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Disclosures. Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy. ASGE Guidelines.
 Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy Consultant for: Olympus Medtronic US Endoscopy Disclosures Joo Ha Hwang, MD, PhD Associate Professor
Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy Consultant for: Olympus Medtronic US Endoscopy Disclosures Joo Ha Hwang, MD, PhD Associate Professor
SUMMARY INTRODUCTION. Accepted for publication 11 May 2005
 Aliment Pharmacol Ther 2005; 22: 169 174. doi: 10.1111/j.1365-2036.2005.02546.x Systematic review and meta-analysis: proton-pump inhibitor treatment for ulcer bleeding reduces transfusion requirements
Aliment Pharmacol Ther 2005; 22: 169 174. doi: 10.1111/j.1365-2036.2005.02546.x Systematic review and meta-analysis: proton-pump inhibitor treatment for ulcer bleeding reduces transfusion requirements
Early Management of the Patient with Acute GI Bleeding
 Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Early Management of the Patient with Acute GI Bleeding Dr Sarah Hearnshaw Consultant Gastroenterologist Newcastle upon Tyne NHS Trust Go through.. Stats Transfusion / resuscitation PPIs When to call us
Peptic ulcer bleeding remains the most common cause of hospitalization
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:311 316 Predicting Mortality in Patients With Bleeding Peptic Ulcers After Therapeutic Endoscopy PHILIP W. Y. CHIU,* ENDERS K. W. NG,* FRANCES K. Y. CHEUNG,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:311 316 Predicting Mortality in Patients With Bleeding Peptic Ulcers After Therapeutic Endoscopy PHILIP W. Y. CHIU,* ENDERS K. W. NG,* FRANCES K. Y. CHEUNG,*
The effectiveness of telephone reminders and SMS messages on compliance with colorectal cancer screening: an open-label, randomized controlled trial
 Page1 of 5 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 The effectiveness of telephone reminders and SMS messages on compliance with colorectal cancer screening: an
Page1 of 5 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 The effectiveness of telephone reminders and SMS messages on compliance with colorectal cancer screening: an
COLON: Innovations 3 steps, 3 parts..
 COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:463 470 Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population HAN MO CHIU,*,, JAW TOWN
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:463 470 Prevalence and Characteristics of Nonpolypoid Colorectal Neoplasm in an Asymptomatic and Average-Risk Chinese Population HAN MO CHIU,*,, JAW TOWN
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient
 Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Turning off the tap: Endoscopy Blood & Guts: Transfusion and bleeding in the medical patient John Greenaway 1 Turning off the tap: Endoscopy Answer the questions Benefits and risks of endoscopy Urgency
Safety and Efficacy of Endoscopic Dilatation of Strictures in Crohn s Disease
 Safety and Efficacy of Endoscopic Dilatation of Strictures in Crohn s Disease Vinna An, Ashwinna Asairinachan, Michael Johnston, James Keck, Paul Salama, Steven Brown, Rodney Woods Department of Colorectal
Safety and Efficacy of Endoscopic Dilatation of Strictures in Crohn s Disease Vinna An, Ashwinna Asairinachan, Michael Johnston, James Keck, Paul Salama, Steven Brown, Rodney Woods Department of Colorectal
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
When to Scope in Lower GI Bleeding: It Must Be Done Now. Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA
 When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
When to Scope in Lower GI Bleeding: It Must Be Done Now Lisa L. Strate, MD, MPH Assistant Professor of Medicine University of Washington, Seattle, WA Outline Epidemiology Overview of available tests Urgent
Sangrado Gastrointestinal Alto Upper GI Bleeding
 Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Sangrado Gastrointestinal Alto Upper GI Bleeding Curso Internacional Retos Clinicos en la Gastroenterologia de Urgencias Asociacion Colombiana de Gastroenterologia 31 de Agosto, 2012 Pereira, Risaralda
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Intragastric ph With Oral vs Intravenous Bolus Plus Infusion Proton- Pump Inhibitor Therapy in Patients With Bleeding Ulcers
 Intragastric ph With Oral vs Intravenous Bolus Plus Infusion Proton- Pump Inhibitor Therapy in Patients With Bleeding Ulcers LOREN LAINE, ABBID SHAH, and SHAHROOZ BEMANIAN Division of Gastrointestinal
Intragastric ph With Oral vs Intravenous Bolus Plus Infusion Proton- Pump Inhibitor Therapy in Patients With Bleeding Ulcers LOREN LAINE, ABBID SHAH, and SHAHROOZ BEMANIAN Division of Gastrointestinal
Differentiation Between Ileocecal Tuberculosis and Crohn s Disease using a Combination of Clinical, Endoscopic and Histological Characteristics
 38 Original Article Differentiation Between Ileocecal Tuberculosis and Crohn s Disease using a Combination of Clinical, Endoscopic and Histological Characteristics Anuchapreeda S Leelakusolvong S Charatcharoenwitthaya
38 Original Article Differentiation Between Ileocecal Tuberculosis and Crohn s Disease using a Combination of Clinical, Endoscopic and Histological Characteristics Anuchapreeda S Leelakusolvong S Charatcharoenwitthaya
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Does Viral Cure Prevent HCC Development
 Does Viral Cure Prevent HCC Development Prof. Henry LY Chan Head, Division of Gastroenterology and Hepatology Director, Institute of Digestive Disease Director, Center for Liver Health Assistant Dean,
Does Viral Cure Prevent HCC Development Prof. Henry LY Chan Head, Division of Gastroenterology and Hepatology Director, Institute of Digestive Disease Director, Center for Liver Health Assistant Dean,
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Colorectal cancer screening in Asia
 Published Online January 8, 2013 Colorectal cancer screening in Asia Siew C. Ng * and Sunny H. Wong Institute of Digestive Disease, Department of Medicine and Therapeutics, Chinese University of Hong Kong,
Published Online January 8, 2013 Colorectal cancer screening in Asia Siew C. Ng * and Sunny H. Wong Institute of Digestive Disease, Department of Medicine and Therapeutics, Chinese University of Hong Kong,
Predict, Resect and discard : Yes we can! (at least in some hands)
") Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD
 CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
Quality in Endoscopy: Can We Do Better?
 Quality in Endoscopy: Can We Do Better? Erik Rahimi, MD Assistant Professor Division of Gastroenterology, Hepatology, and Nutrition UT Health Science Center at Houston McGovern Medical School Ertan Digestive
Quality in Endoscopy: Can We Do Better? Erik Rahimi, MD Assistant Professor Division of Gastroenterology, Hepatology, and Nutrition UT Health Science Center at Houston McGovern Medical School Ertan Digestive
British Society of Gastroenterology. St. Elsewhere's Hospital. National Comparative Audit of Blood Transfusion
 British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
British Society of Gastroenterology UK Com parat ive Audit of Upper Gast roint est inal Bleeding and t he Use of Blood Transfusion Extract December 2007 St. Elsewhere's Hospital National Comparative Audit
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Topic. Speaker. Session. Detection. Buffet Lunch. Session Beginner to. Expert. Tea Break. Diseases
 24 Feb 2017 (Fri) Lectures and n Venue: Cheung Kung Hai Lecturee Theatre, LKS Faculty of Medicine Co organized by Department of Medicine & Department of Surgery The University of Hong Kong & Queen Mary
24 Feb 2017 (Fri) Lectures and n Venue: Cheung Kung Hai Lecturee Theatre, LKS Faculty of Medicine Co organized by Department of Medicine & Department of Surgery The University of Hong Kong & Queen Mary
Risk assessment in UGIB: recent PCI & ACS. Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass
 Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
Risk assessment in UGIB: recent PCI & ACS Dr Martin James PhD FRCP October 20 th 2016 Nottingham Endoscopy Masterclass Clinical scenario 65 yr male Previous smoker, hyperlipidaemia, DM PCI < 48 hours Dual
Chromoendoscopy as an Adjunct to Colonoscopy
 Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Chromoendoscopy as an Adjunct to Colonoscopy Policy Number: 2.01.84 Last Review: 1/2018 Origination: 7/2017 Next Review: 7/2018 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will not provide
Accepted Manuscript. Does eradication of Helicobacter pylori cause inflammatory bowel disease? Johan Burisch, Tine Jess
 Accepted Manuscript Does eradication of Helicobacter pylori cause inflammatory bowel disease? Johan Burisch, Tine Jess PII: S1542-3565(19)30153-3 DOI: https://doi.org/10.1016/j.cgh.2019.02.013 Reference:
Accepted Manuscript Does eradication of Helicobacter pylori cause inflammatory bowel disease? Johan Burisch, Tine Jess PII: S1542-3565(19)30153-3 DOI: https://doi.org/10.1016/j.cgh.2019.02.013 Reference:
Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y.
 Digestive Endoscopy (2007) 19(s1):S145-S149. Auto-Fluorescence Imaging is useful to assess the activity of ulcerative colitis Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y. Auto-Fluorescence Imaging
Digestive Endoscopy (2007) 19(s1):S145-S149. Auto-Fluorescence Imaging is useful to assess the activity of ulcerative colitis Fujiya M, Saitoh Y, Watari J, Moriichi K, Kohgo Y. Auto-Fluorescence Imaging
Effect of oral omeprazole in reducing re-bleeding in bleeding peptic ulcers: a prospective, double-blind, randomized, clinical trial
 Aliment Pharmacol Ther 2003; 17: 211 216. doi: 10.1046/j.0269-2813.2003.01416.x Effect of oral omeprazole in reducing re-bleeding in bleeding peptic ulcers: a prospective, double-blind, randomized, clinical
Aliment Pharmacol Ther 2003; 17: 211 216. doi: 10.1046/j.0269-2813.2003.01416.x Effect of oral omeprazole in reducing re-bleeding in bleeding peptic ulcers: a prospective, double-blind, randomized, clinical
Upper GI Bleeding. HH Tsai MD FRCP FECG Consultant Gastroenterologist
 Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Upper GI Bleeding HH Tsai MD FRCP FECG Consultant Gastroenterologist Financial Disclosures I have no financial relationship with any manufacturer or supplier of any product mentioned in this talk. GI Audits:
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Disclosures. GI Motility Disorders. Gastrointestinal Motility Disorders & Irritable Bowel Syndrome
 Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
Gastrointestinal Motility Disorders & Irritable Bowel Syndrome None Disclosures Jasmine Zia, MD Acting Assistant Professor Division of Gastroenterology, University of Washington 6 th Asian Health Symposium
Development of Robotic Endoscopic Surgical Platform for Treatment of Early Gastrointestinal Cancers
 Development of Robotic Endoscopic Surgical Platform for Treatment of Early Gastrointestinal Cancers Philip WY Chiu MD, MBChB, FRCSEd, FCSHK FHKAM (Surg) Professor, Department of Surgery, Institute of Digestive
Development of Robotic Endoscopic Surgical Platform for Treatment of Early Gastrointestinal Cancers Philip WY Chiu MD, MBChB, FRCSEd, FCSHK FHKAM (Surg) Professor, Department of Surgery, Institute of Digestive
Oral versus intravenous proton pump inhibitors in preventing re-bleeding for patients with peptic ulcer bleeding after successful endoscopic therapy
 Yen et al. BMC Gastroenterology 2012, 12:66 RESEARCH ARTICLE Open Access Oral versus intravenous proton pump inhibitors in preventing re-bleeding for patients with peptic ulcer bleeding after successful
Yen et al. BMC Gastroenterology 2012, 12:66 RESEARCH ARTICLE Open Access Oral versus intravenous proton pump inhibitors in preventing re-bleeding for patients with peptic ulcer bleeding after successful
Acute Upper Gastro Intestinal (UGI) Bleeding
 Bleeding") T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
T Acute Upper Gastro Intestinal (UGI) Bleeding University Hospitals of Leicester NHS Trust Guidelines for Management of Acute Medical Emergencies 1. Has there been a GI bleed? There are also UHL trust
ESMO Preceptorship Program Head & Neck Cancer NPC: Epidemiology, diagnosis and work-up
 ESMO Preceptorship Program Head & Neck Cancer NPC: Epidemiology, diagnosis and work-up Dr. John Woo Consultant, ENT Department, PWH Honorary Clinical Professor, Department of Otorhinolaryngology, H&N Surgery
ESMO Preceptorship Program Head & Neck Cancer NPC: Epidemiology, diagnosis and work-up Dr. John Woo Consultant, ENT Department, PWH Honorary Clinical Professor, Department of Otorhinolaryngology, H&N Surgery
BENEFIT APPLICATION BLUE CARD/NATIONAL ACCOUNT ISSUES
 Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND. Fabrizio Parente
 NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
NON INVASIVE MONITORING OF MUCOSAL HEALING IN IBD. THE ROLE OF BOWEL ULTRASOUND Fabrizio Parente Gastrointestinal Unit, A.Manzoni Hospital, Lecco & L.Sacco School of Medicine,University of Milan - Italy
General and Colonoscopy Data Collection Form
 Identifier: Sociodemographic Information Type: Zip Code: Inpatient Outpatient Birth Date: m m d d y y y y Gender: Height: (inches) Male Female Ethnicity: Weight: (pounds) African American White, Non-Hispanic
Identifier: Sociodemographic Information Type: Zip Code: Inpatient Outpatient Birth Date: m m d d y y y y Gender: Height: (inches) Male Female Ethnicity: Weight: (pounds) African American White, Non-Hispanic
Prof Rupert Leong, Director of Endoscopy, Head of IBD Professor of Medicine UNSW, University of Sydney, Concord Hospital Australia IBDSydney
 10:30-10:50 25 Sept 2017 Monday A-PSDE / WEO Colorectal Cancer Screening Committee (CRCSC) Meeting Room S228 (2/F) Prof Rupert Leong, Director of Endoscopy, Head of IBD Professor of Medicine UNSW, University
10:30-10:50 25 Sept 2017 Monday A-PSDE / WEO Colorectal Cancer Screening Committee (CRCSC) Meeting Room S228 (2/F) Prof Rupert Leong, Director of Endoscopy, Head of IBD Professor of Medicine UNSW, University
Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University WCC, Melbourne
 Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University. 2014 WCC, Melbourne Outline WHO criteria to justify screening Appropriateness: Global variation in incidence
Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University. 2014 WCC, Melbourne Outline WHO criteria to justify screening Appropriateness: Global variation in incidence
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
ESMO Preceptorship Program Head & Neck Cancer NPC: Epidemiology, diagnosis and work-up
 ESMO Preceptorship Program Head & Neck Cancer NPC: Epidemiology, diagnosis and work-up Dr. John Woo Consultant, ENT Department, PWH Honorary Clinical Professor, Department of Otorhinolaryngology, H&N Surgery
ESMO Preceptorship Program Head & Neck Cancer NPC: Epidemiology, diagnosis and work-up Dr. John Woo Consultant, ENT Department, PWH Honorary Clinical Professor, Department of Otorhinolaryngology, H&N Surgery
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
C olorectal adenomas are reputed to be precancerous
 568 COLORECTAL CANCER Incidence and recurrence rates of colorectal adenomas estimated by annually repeated colonoscopies on asymptomatic Japanese Y Yamaji, T Mitsushima, H Ikuma, H Watabe, M Okamoto, T
568 COLORECTAL CANCER Incidence and recurrence rates of colorectal adenomas estimated by annually repeated colonoscopies on asymptomatic Japanese Y Yamaji, T Mitsushima, H Ikuma, H Watabe, M Okamoto, T
Dr. LEUNG Lok Hang, Will
 Direct access endoscopy booking by family physicians: evaluating a new service model and clinical predictors of positive endoscopy findings at primary care setting Dr. LEUNG Lok Hang, Will Department of
Direct access endoscopy booking by family physicians: evaluating a new service model and clinical predictors of positive endoscopy findings at primary care setting Dr. LEUNG Lok Hang, Will Department of
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Comparison of adrenaline injection and bipolar electrocoagulation for the arrest of peptic ulcer bleeding
 Gut 1999;44:715 719 715 Division of Gastroenterology, Department of Medicine, Veterans General Hospital, Taipei, Taiwan, Republic of China H-J Lin G-Y Tseng C-L Perng F-Y Lee F-Y Chang S-D Lee Correspondence
Gut 1999;44:715 719 715 Division of Gastroenterology, Department of Medicine, Veterans General Hospital, Taipei, Taiwan, Republic of China H-J Lin G-Y Tseng C-L Perng F-Y Lee F-Y Chang S-D Lee Correspondence
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases?
 How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
How to differentiate Segmental Colitis Associated with Diverticulosis and Inflammatory Bowel Diseases? Alessandro Armuzzi Lead IBD Unit Complesso Integrato Columbus Fondazione Policlinico Gemelli Università
GIQIC18 Appropriate follow-up interval of not less than 5 years for colonoscopies with findings of 1-2 tubular adenomas < 10 mm
 GI Quality Improvement Consortium, Ltd. (GIQuIC) 1 Following is an overview of the clinical quality measures in GIQuIC that can be reported to CMS for the Quality performance category of the Merit-Based
GI Quality Improvement Consortium, Ltd. (GIQuIC) 1 Following is an overview of the clinical quality measures in GIQuIC that can be reported to CMS for the Quality performance category of the Merit-Based
Continuation of Low-Dose Aspirin Therapy with Either PR or PO Administration in Patients with Peptic Ulcer Bleeding
 Continuation of Low-Dose Aspirin Therapy with Either PR or PO Administration in Patients with Peptic Ulcer Bleeding IRB Protocol Lucian Iancovici February 4, 2010 A. Study Design and Purpose Aspirin has
Continuation of Low-Dose Aspirin Therapy with Either PR or PO Administration in Patients with Peptic Ulcer Bleeding IRB Protocol Lucian Iancovici February 4, 2010 A. Study Design and Purpose Aspirin has
Colorectal Cancer Screening: A Clinical Update
 11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
Korean gastric cancer screening program, algorithms and experience.
 Korean gastric cancer screening program, algorithms and experience. Jun Haeng Lee, MD. Department of Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea Today s topics Korean cancer screening
Korean gastric cancer screening program, algorithms and experience. Jun Haeng Lee, MD. Department of Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea Today s topics Korean cancer screening
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY
 Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right?
 Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
Quality of and compliance with colonoscopy in Lynch Syndrome surveillance: are we getting it right? Hartery K 1, Sukha A 1, Thomas-Gibson S 1, Thomas H 1,2, Latchford A 1,2. 1 Wolfson Endoscopy Unit, St.
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
The Incidence Rate of Inflammatory Bowel Disease in an Urban Area of Iran: A Developing Country
 32 Original Article The Incidence Rate of Inflammatory Bowel Disease in an Urban Area of Iran: A Developing Country Mohammad Javad Zahedi 1, Sodaif Darvish Moghadam 1, Mehdi Hayat Bakhsh Abbasi 1, Masood
32 Original Article The Incidence Rate of Inflammatory Bowel Disease in an Urban Area of Iran: A Developing Country Mohammad Javad Zahedi 1, Sodaif Darvish Moghadam 1, Mehdi Hayat Bakhsh Abbasi 1, Masood
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Outcome of endoscopic treatment for peptic ulcer bleeding: Is a second look necessary? A meta-analysis
 Outcome of endoscopic treatment for peptic ulcer bleeding: Is a second look necessary? A meta-analysis Riccardo Marmo, MD, Gianluca Rotondano, MD, Maria Antonia Bianco, MD, Roberto Piscopo, MD, Antonio
Outcome of endoscopic treatment for peptic ulcer bleeding: Is a second look necessary? A meta-analysis Riccardo Marmo, MD, Gianluca Rotondano, MD, Maria Antonia Bianco, MD, Roberto Piscopo, MD, Antonio
Present Status and Perspectives of Colorectal Cancer in Asia: Colorectal Cancer Working Group Report in 30th Asia-Pacific Cancer Conference
 Present Status and Perspectives of Colorectal Cancer in Asia: Colorectal Cancer Working Group Report in 30th Asia-Pacific Cancer Conference Jpn J Clin Oncol 2010;40(Supplement 1)i38 i43 doi:10.1093/jjco/hyq125
Present Status and Perspectives of Colorectal Cancer in Asia: Colorectal Cancer Working Group Report in 30th Asia-Pacific Cancer Conference Jpn J Clin Oncol 2010;40(Supplement 1)i38 i43 doi:10.1093/jjco/hyq125
Diagnostic techniques for surveillance of dysplasia
 January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Diagnostic techniques for surveillance of dysplasia Gerhard Rogler, Department of Gastroenterology
January 27th 2017, 8th Gastro Foundation Weekend for Fellows; Spier Hotel & Conference Centre, Stellenbosch Diagnostic techniques for surveillance of dysplasia Gerhard Rogler, Department of Gastroenterology
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Pantoprazole infusion as adjuvant therapy to endoscopic treatment in patients with peptic ulcer bleeding: Prospective randomized controlled trial
 Blackwell Publishing AsiaMelbourne, AustraliaJGHJournal of Gastroenterology and Hepatology0815 93192006 Blackwell Publishing Asia Pty Ltd200621716721Original Article Pantoprazole in bleeding peptic ulcerssa
Blackwell Publishing AsiaMelbourne, AustraliaJGHJournal of Gastroenterology and Hepatology0815 93192006 Blackwell Publishing Asia Pty Ltd200621716721Original Article Pantoprazole in bleeding peptic ulcerssa
Objec-ve. Case Presenta-ons and Ques-ons to Panel. Dysplasia case 11/13/11
 Case Presenta-ons and Ques-ons to Panel UCSF IBD Symposium November 12, 2011 Moderator Fernando Velayos MD Panelists Brian Feagan, MD James Lewis, MD MSCE Robert Cima, MD Hueylan Chern, MD Sunanda Kane,
Case Presenta-ons and Ques-ons to Panel UCSF IBD Symposium November 12, 2011 Moderator Fernando Velayos MD Panelists Brian Feagan, MD James Lewis, MD MSCE Robert Cima, MD Hueylan Chern, MD Sunanda Kane,
Intermittent vs Continuous Proton Pump Inhibitor Therapy for High-Risk Bleeding Ulcers A Systematic Review and Meta-analysis
 Research Original Investigation Intermittent vs Continuous Proton Pump Inhibitor Therapy for High-Risk Bleeding Ulcers A Systematic Review and Meta-analysis Hamita Sachar, MD; Keta Vaidya, MD; Loren Laine,
Research Original Investigation Intermittent vs Continuous Proton Pump Inhibitor Therapy for High-Risk Bleeding Ulcers A Systematic Review and Meta-analysis Hamita Sachar, MD; Keta Vaidya, MD; Loren Laine,
Asia-Pacific Working Group consensus on non-variceal upper gastrointestinal bleeding
 Asia-Pacific Working Group consensus on non-variceal upper gastrointestinal bleeding Joseph J Y Sung, 1 Francis K L Chan, 2 Minhu Chen, 3 Jessica Y L Ching, 3 K Y Ho, 4 Udom Kachintorn, 3 Nayoung Kim,
Asia-Pacific Working Group consensus on non-variceal upper gastrointestinal bleeding Joseph J Y Sung, 1 Francis K L Chan, 2 Minhu Chen, 3 Jessica Y L Ching, 3 K Y Ho, 4 Udom Kachintorn, 3 Nayoung Kim,