Advanced stage HL The old and new match: BEACOPP
|
|
|
- Ethel Miller
- 6 years ago
- Views:
Transcription
1 Advanced stage HL The old and new match: BEACOPP Peter Borchmann German Hodgkin Study Group University of Cologne, Germany
2 Which answer is wrong? For patients with advanced stage HL, treatment with 6 cycles BEACOPPesc, the GHSG standard of care, results 1. In a treatment related mortality rate of 0.8%. 2. In an overall survival at 5 years of 95%. 3. In an infertility rate of about 80% in women in the age of 25 years at diagnosis. 4. In 0.3% secondary acute myeloid leukemia. 2
3 Which answer is correct? In advanced stage HL treated with BEACOPPEesc, 1. Positive early interim PET (after cycle 2) identifies a high risk group of patients 2. Residual disease is defined as any tumor > 1.5 cm at the end of chemotherapy 3. PET after the end of chemotherapy helps to identify a high risk group 4. As compared to treatment with ABVD, the superiority of BEACOPP in terms of PFS and OS is both significant and relevant in IPI low risk patients. 3
4 The old and new match: BEACOPP 1. Why do I like BEACOPPesc? 2. Why do I prefer BEACOPPesc over ABVD? 3. Can we do even better than BEACOPPesc?
5 FFTF I like BEACOPPesc, because it is very active % The GHSG HD9 trial COPP/ABVD BEACOPPbase BEACOPPesc A (64%) B (70%) C (82%) p <0, Years The GHSG HD9 study, Engert et al., J Clin Oncol, 2010, 27:
6 SURVIVAL I like BEACOPP, because my patients ask for cure % The GHSG HD9 trial p <0.001 COPP/ABVD BEACOPPbase BEACOPPesc A (75%) B (80%) C (86%) Years The GHSG HD9 study, Engert et al., J Clin Oncol, 2010, 27:
7 Engert et al., Lancet, I like BEACOPP, because it has been nicely developed: step by step, for 20 years now, including more than patients. The HD15 Study Design 8x BEACOPP escalated 6x BEACOPP escalated 8x BEACOPP Baseline-14 Restaging: PR and residual tumor >2,5 cm? No Yes PET Follow up PET - PET + Rx 30Gy residual tumor
 0.3 0.2 0.1 0.0 PR 2.5cm/PET- CR/CRu (no PET) PR 2.5cm/PET+ 0 12 24 36 48 60 Months from randomization Pts.")
8 I like BEACOPPesc, because only 11% of my patients will need Rx. Based on evidence, not on NCCN guidelines only ;- ) Time to progression Negative Predictive Value of 94% (95% CI: 92 to 96%) PR 2.5cm/PET- CR/CRu (no PET) PR 2.5cm/PET Months from randomization Pts. at Risk PET PET CR/CRu
9 I just like it, because only 6 quick courses are even better than 8

10 and because I don t like funerals

11 The old and new match: BEACOPP 1. Why do I like BEACOPPesc? 2. Why do I prefer BEACOPPesc over ABVD? 3. Can we do even better?
12 The old and new match: BEACOPP 1. Why do I like BEACOPPesc? 2. Why do I prefer BEACOPPesc over ABVD? 3. Can we do even better?
13 Because it is just better: as shown by 4 out of 4 (yes, all!) controlled and randomized studies Study Group n 5-y PFS Difference (%) p 5-y OS ABVD HD 2000 BEACOPP (4 esc + 2 std) 92 ABVD IIL BEACOPP (4 esc + 4 std) 89 IG ABVD ,7 BEACOPP IPS (4 esc + 4 std) 90,3 ABVD LYSA H IPS 0-2 BEACOPP (4 esc + 4 std) HD15 7-year PFS; 4-year PFS. 6 BEACOPPesc Difference (%)
14 You still don t believe it? Let s have a look the highest level of evidence: a metanalysis. 1,984 references were identified, referring to 77 publications, reporting 14 trials, evaluating 11 different regimens with a total of 10,011 patients and 47,033 patient-years of follow-up evaluable for the analyses of survival outcomes including 1,189 events with a average median follow-up 5.9 years Skoetz et al., Lancet Oncol,
15 BEACOPPesc is not just better. It is much better than ABVD ;- ) C Probability 0.70 Regimen 5-year OS difference *BEACOPPesc 10% (95% CI: 13% to 5%) 0.50 ABVD 6*BEACOPPesc Years

16 And BEACOPPesc is very safe! TRM acoording individual risk score: age (>40, > 50, WHO PS 2)
17 Another surprise: neither more secondary neoplasia nor more saml/mds than with ABVD! Study Group n TRM (%) HD 2000 IIL IG IPS 3-7 LYSA H34 IPS 0-2 saml/mds (%) Second neoplasia n (%) ABVD 99 n.r. 0 1 (1) BEACOPP (4 esc + 2 std) 98 n.r. 0 1 (1) ABVD (1.8) BEACOPP (4 esc + 4 std) (0.6) ABVD (2.9) BEACOPP (4 esc + 4 std) (3.7) ABVD (6.5) BEACOPP (4 esc + 4 std) (1.5) HD15 6 BEACOPPesc (2.1) 7-year PFS; 4-year PFS.
 Behringer et al.")
18 But: Almost all patients become infertile after BEACOPPesc! True or not? Looking at data can help, if one wants to know ;- ) Behringer et al., JCO, x BEACOPPEsc 2x Besc + 2x ABVD

19 The old and new match: BEACOPP 1. Why do I like BEACOPPesc? 2. Why do I prefer BEACOPPesc over ABVD? 3. Can we do even better?
20 The old and new match: BEACOPP 1. Why do I like BEACOPPesc? 2. Why do I prefer BEACOPPesc over ABVD? 3. Can we do even better?
 6x BEACOPPesc (HD15) PFS (stage III/IV) @3 y: 71% (29% failure rate) PFS (stage III/IV) @3 y: 91% (9% failure rate)")
21 Which tools do we have to improve our regimen? ABVD (E2496) 6x BEACOPPesc (HD15) PFS (stage y: 71% (29% failure rate) PFS (stage y: 91% (9% failure rate) Escalation (PFS) De-escalation (tox) PET guided Brentuximab PET guided Brentuximab


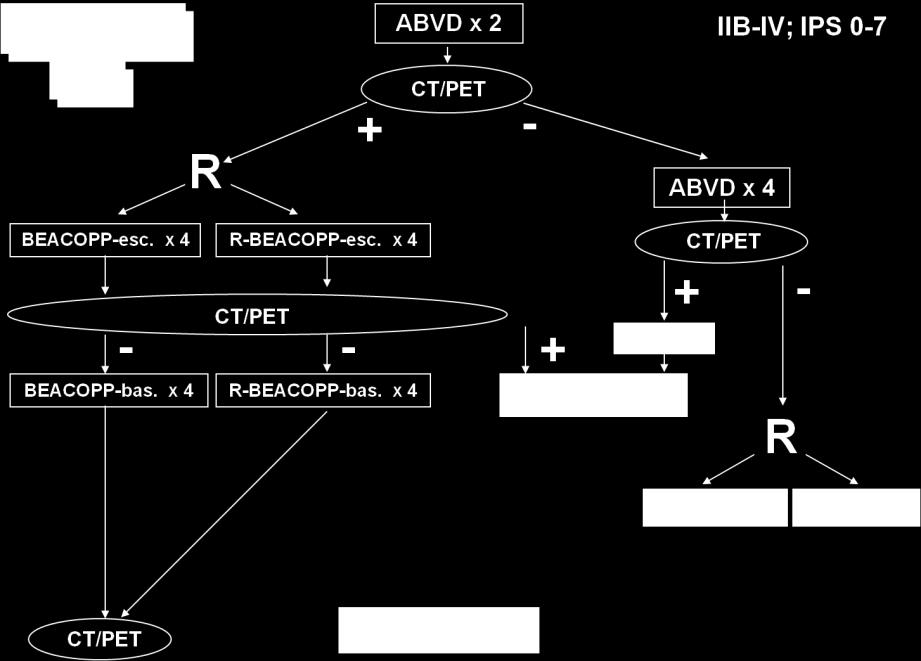
22 Borchmann et al., ASH, 2014, abs 500 HD18: testing a PET guided treatment strategy x BEACOPP escalated 440 centrally reviewed PET PET + PET x BEACOPPesc 5x R-BEACOPPesc 1x BEACOPPesc 5x BEACOPPesc 6x BEACOPPesc 2x BEACOPPesc End of therapy AND residual nodes > 2.5 cm : PET positiv: Rx
23 Assumptions and primary objective 1. Total 5-year PFS with 8x BEACOPPesc. is 86.3% (HD9/12) 2. 30% of patients will be PET positive after 2 courses (SUV uptake above mediastinal bloodpool) 3. 70% of all events will occur in PET-2 positive patients, resulting in a five year PFS of 68% for these patients Show that the addition of rituximab to our standard chemotherapy BEACOPPesc (R-BEACOPP) improves 5-year PFS to 83% (hazard ratio 0.483, i.e. rituximab more than halves the hazard) 23
24 PFS PFS of ipet positive patients in HD18 Borchmann et al., ASH, 2014, abs p = year PFS [95% CI] 8x BEACOPP, PET+ 91.4% [87.0%, 95.7%] 8x R-BEACOPP, PET+ 93.0% [89.4%, 96.6%] Difference 1.6% [-4.0%, 7.3%] 8x BEACOPP HD % x BEACOPP, PET+ 8x R-BEACOPP, PET Pts. at Risk Time [months] BEACOPP R-BEACOPP
25 GHSG HD 18 trial randomization 2 x BEACOPP esc 2 x BEACOPP centrally reviewed PET positive negative 4 x BEACOPP esc 4 x BEACOPP esc 2 x BEACOPP esc End of therapy AND residual nodes > 2.5 cm: PET positive: Rx PET negative: Follow up

26 The CD30 antigen: targeting the H-RS cell in HL with antibodies
27 Remodeling BEACOPPesc with Brentuximab vedotin Drug Day 6x BEACOPP Bleomycin 8 10 Etoposide Adriamycin 1 35 Cyclophosphamide Vincristine Brentuximab vedotin 1 Procarbazine Prednisone Dacarbazine 2-3 Dexamethasone 1-4 6x BrECADD
28 Interim analysis of the BEACOPP variant BrECADD indicate 1. an efficacy comparable to BEACOPPesc (BrECADD, n=37, CR n=35 (95%), PR n= 2 (5%)) 2. a safety profile superior to BEACOPPesc (grade 3 or 4 non-hematological toxicity 3% with 3. only 30% grade 1 or 2 neurotoxicity

 at end of treatment What do you think: how does this")

29 How can we do better? Co-primary objectives in HD21 Primary objectives: to show Non-inferiority of BrECADD in terms of PFS (observed in HD15: 91% stage II/IV at 3 years) Superiority of BrECADD regarding treatment-related morbidity (TRM) at end of treatment What do you think: how does this endpoint compare to the primary endpoint of ECHELON I, which is: improving the PFS at 3 years from 75% for ABVD to 82,5% for AVD-A? Honestly: how relevant is this objective taking into account some more relevant toxicities as neuropathy (roughly 75%!)?

30 The old and new match: BEACOPP 1. Why do I like BEACOPPesc? 2. Why do I prefer BEACOPPesc over ABVD? 3. Can we do even better than BEACOPPesc?

31 We, the GHSG, thank you for your attention! 31
32 Which answer is correct? In advanced stage HL treated with BEACOPPEesc, 1. Positive early interim PET (after cycle 2) identifies a high risk group of patients 2. Residual disease is defined as any tumor > 1.5 cm at the end of chemotherapy 3. PET after the end of chemotherapy helps to identify a high risk group 4. As compared to treatment with ABVD, the superiority of BEACOPP in terms of PFS and OS is both significant and relevant in IPI low risk patients. 32
33 Which answer is wrong? For patients with advanced stage HL, treatment with 6 cycles BEACOPPesc, the GHSG standard of care, results 1. In a treatment related mortality rate of 0.8%. 2. In an overall survival at 5 years of 95%. 3. In an infertility rate of about 80% in women in the age of 25 years at diagnosis. 4. In 0.3% secondary acute myeloid leukemia. 33
 BEACOPP de-escalation")

 HD18 (4BEA)")
34 Future developments? ABVD escalation (PFS) BEACOPP de-escalation PET guided BV PD1- Ab PET guided BV PD1- Ab Numerous IITs ongoing ECHELO N-1 (AVD-A vs ABVD, Takeda sponsor ed) X Plus A(B)VD versus ABVD Lysa AHL 2011 (2BEA + 4ABVD) HD18 (4BEA) tbeacopp HD21 (BEACOPP vs BrECADD)?
35 Current international developments ABVD escalation (PFS) BEACOPP de-escalation PET guided Brentuximab PET guided Brentuximab Numerous IITs ongoing ECHELON-1 (AVD-A vs ABVD, Takeda sponsored) HD18 (4BEA) Lysa AHL 2011 (2BEA + 4ABVD) tbeacopp HD21 (BEACOPP vs BrECADD)
 27.03.")
36 OS for ABVD (reference regimen) 5y-OS of 88% (84-91%) is the estimate for ABVD for this analysis (reference value)

37 Forest plot for OS
38 Treatment outcome after chemotherapy (primary endpoint) Treatment Outcome BrECAPP N = 33 BrECADD N = 37 Total N = 70 HD18 (6 cycles) CR or PET negative PR 28 (85%) 35 (95%) 63 (90%) (97.5%-CI 80%-96%) 91,9% Less than PR or PET positive (above liver) 5 (15%) 2 (5%) 7 (10%) (97.5%-CI 4% 20%) 7 % The lower limit of the one-sided 95% confidence interval for the number of treatment successes is 80.5%
39 Acute Toxicities 6x BRECADD (n=38) Type of Toxicity HD18* NCIC-CTC Grade III/IV (n=447) none I II III IV III/IV III/IV Hematological 1 (3%) 1 (3%) 4 (11%) 32 (84%) 36 (95%) 404 (90.4%) Organs 16 (42%) 14 (37%) 7 (18%) 1 (3%) 1 (3%) 64 (14.3%)
40 Neurotoxicity with tbeacopp (n=71, all patients after 6 cycles) Type of Toxicity NCIC-CTC Grade none I II III IV III/IV HD18* III/IV (n=447) Nervous system (sensory) Nervous system (mot.) 49 69% 70 99% 14 20% 1 1% 7 10% 1 1% 1 1% 38 5%
41 The GHSG perspective: HD21 randomization 2 x BEACOPP esc 2 x BrECADD centrally reviewed PET 4x BEACOPP esc 4x BrECADD End of therapy AND residual nodes > 2.5 cm: PET positiv: Rx PET negative: Follow up
42 Can we further improve the efficacy of BEACOPPesc? Standard treatment defining study result: Study Group Median FU n PFS (%) OS (%) HD15 Engert et al Lancet x BEACOPPesc IIL Viviani et al NEJM x ABVD BEACOPP is obviously highly active with a very high progression free and overall survival rate

43 ABVD: PET guided escalation strategy
44 S0816: Progression-Free Survival (HIV-negative) 100% 80% 60% 40% 20% Median FU = 16.1 months Patients at Risk Failed 2-Year Estimate % (95% CI: 69%, 81%) 0% Months After Registration
45 Combination with ABVD: Overview Key objectives: safety, MTD, antitumor activity Patients: 51 previously untreated HL patients (median age 33 years [range, 18 59]); disease stage: IIA bulky, n=3; IIB, n=8; IIIA, n=8; IIIB, n=9; IV, n=23; bulky disease, n=17; IPS 4, n=13 Treatment: Up to six 28-day cycles Brentuximab vedotin 0.6 (n=6), 0.9 (n=13), or 1.2 (n=6) mg/kg, days 1 and 15 (weeks 1 and 3), plus ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) Brentuximab vedotin 1.2 mg/kg (n=26) plus AVD (without bleomycin) Cycle 1 Cycle 2 Cycle 3 Brentuximab Vedotin A(B)VD Weeks Weeks 6 Cycles +/- XRT Ansell SM, et al. ASH 2012, Atlanta, GA, USA (Abstract 798)
46 Preferred term, n (%) Pulmonary toxicity in combination with A(B)VD Safety: pulmonary toxicity Events generally occurred during Cycles 3-4 Two patient deaths were associated with pulmonary toxicity Events resolved in 9 of 11 patients (82%) ABVD with brentuximab vedotin (n=25) Median time to resolution was 2.6 weeks (range, weeks) AVD with brentuximab vedotin (n=26) Any event 11 (44) 0 Pulmonary toxicity 9 (36) 0 Interstitial lung disease 1 (4) 0 Pneumonitis 1 (4) 0 8 of 11 patients with events discontinued bleomycin and were able to complete treatment with AVD combined with brentuximab vedotin Concomitant administration of brentuximab vedotin and bleomycin is contraindicated due to pulmonary toxicity Ansell SM, et al. ASH 2012, Atlanta, GA, USA (Abstract 798)
47 Peripheral neuropathy Preferred term* ABVD with brentuximab vedotin N=25 AVD with brentuximab vedotin N=26 Any event 18 (72) 20 (77) Peripheral sensory neuropathy 18 (72) 19 (73) Peripheral motor neuropathy 3 (12) 3 (12) Muscular weakness 1 (4) 2 (8) Paraesthesia 1 (4) 0 * Summary of events using a standard MedDRA query (SMQ), regardless of relationship or severity Events were managed with dose modifications Most events were Grade 1 or 2 and no events were Grade 4 or 5 One patient experienced Grade 3 events of peripheral sensory neuropathy (fingers and toes) and peripheral motor neuropathy (hands and feet) Overall, 6 of 51 patients discontinued brentuximab vedotin due to peripheral neuropathy; these discontinuations occurred in Cycles 5 or 6 Ansell SM, et al. ASH 2012, Atlanta, GA, USA (Abstract 798)
48 Anti-tumour activity DLT: No protocol-defined DLTs observed with either ABVD or AVD in combination with brentuximab vedotin (up to the maximum planned dose of 1.2 mg/kg) Antitumor activity: Response at end of frontline therapy, n (%)* ABVD with brentuximab vedotin (n=22) AVD with brentuximab vedotin (n=25) Complete remission 21 (95) 24 (96) Progressive disease 0 1 (4) Not evaluable due to AE 1 (5) ** 0 Prior to completion of frontline therapy 1 patient withdrew consent 3 patients lost to follow-up Phase 3 study ongoing to assess treatment with brentuximab vedotin in combination with AVD compared to ABVD alone in treatment-naive patients * Per Investigator ** Patient had Grade 5 pulmonary toxicity prior to end of frontline therapy Ansell SM, et al. ASH 2012, Atlanta, GA, USA (Abstract 798)
49 A(B)VD-A failure free survival Connors et al., ASH, 2014, abs Survival A-AVD Ergebnisse CR 96 % 3-y FFS 92 % 3-y OS 100 % Failure-free Survival (months) FFS (mos) 60
50 Phase III study of A-AVD vesus ABVD in advanced stage HL (NCT )
51 Primary endpoint PFS: Estimates in C25003 (ECHELON I) 3 years for stage III/IV patients PFS 6x ABVD C expected 6x AVD-A C ,5 expected
52 Targeted BEACOPP: Study flow Randomisation Patients aged CS IIB + RF ED or LMM, CS III/IV 2 x BrECAPP 2 x BrECADD Off study in case of PD Interim Staging (CT-2/PET-2) Off study in case of PD 4 x BrECAPP 4 x BrECADD End of therapy AND residual nodes > 2.5 cm: PET positiv: Gy PET negative: Follow up
53 Can we define patients at risk for treatment related mortality (TRM)? Wongso et al., JCO, 2013 Risk Factor Score Age ECOG / Karnofsky < <2 or 80 0 =2 or <80 1
Hodgkin Lymphoma Status of the art of treatment
 11.05.2016 1 Hodgkin Lymphoma Status of the art of treatment Peter Borchmann German Hodgkin Study Group University of Cologne, Germany Question No 1: Which statement regarding 1 st line treatment of early
11.05.2016 1 Hodgkin Lymphoma Status of the art of treatment Peter Borchmann German Hodgkin Study Group University of Cologne, Germany Question No 1: Which statement regarding 1 st line treatment of early
PET-Guided Treatment Approach for Advanced Stage Classical Hodgkin Lymphoma. Ranjana H. Advani, MD
 PET-Guided Treatment Approach for Advanced Stage Classical Hodgkin Lymphoma Ranjana H. Advani, MD Stanford Cancer Institute Management of Hodgkin Lymphoma Learning Objectives Review risk adapted strategies
PET-Guided Treatment Approach for Advanced Stage Classical Hodgkin Lymphoma Ranjana H. Advani, MD Stanford Cancer Institute Management of Hodgkin Lymphoma Learning Objectives Review risk adapted strategies
German Hodgkin Study Group
 German Hodgkin Study Group Deutsche Hodgkin Studiengruppe Avoiding Relapse of Hodgkin Lymphoma: Have We Moved The Needle? Andreas Engert, MD Chairman, German Hodgkin Study Group University Hospital of
German Hodgkin Study Group Deutsche Hodgkin Studiengruppe Avoiding Relapse of Hodgkin Lymphoma: Have We Moved The Needle? Andreas Engert, MD Chairman, German Hodgkin Study Group University Hospital of
ABVD versus BEACOPP arguments for ABVD. Dr Pauline BRICE Hôpital saint louis Université Paris VII PARIS
 ABVD versus BEACOPP arguments for ABVD Dr Pauline BRICE Hôpital saint louis Université Paris VII PARIS DISCLOSURES HONORARIAS: Takeda, roche GRANT RESEARCH : Millenium Takeda, AMGEN ABVD the standard chemotherapy
ABVD versus BEACOPP arguments for ABVD Dr Pauline BRICE Hôpital saint louis Université Paris VII PARIS DISCLOSURES HONORARIAS: Takeda, roche GRANT RESEARCH : Millenium Takeda, AMGEN ABVD the standard chemotherapy
ABVD or BEACOPP for advanced Hodgkin lymphoma. Not to BEACOPP. Massimo Federico University of Modena and Reggio Emilia Italy
 ABVD or BEACOPP for advanced Hodgkin lymphoma Not to BEACOPP Massimo Federico University of Modena and Reggio Emilia Italy What is the best Induction Therapy for Advanced Hodgkin Lymphoma? How to treat
ABVD or BEACOPP for advanced Hodgkin lymphoma Not to BEACOPP Massimo Federico University of Modena and Reggio Emilia Italy What is the best Induction Therapy for Advanced Hodgkin Lymphoma? How to treat
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
First Line Management of Classical Hodgkin Lymphoma
 First Line Management of Classical Hodgkin Lymphoma George Follows Cambridge University Hospitals NHS Foundation Trust george.follows@addenbrookes.nhs.uk The controversial areas Early stage non-bulky /
First Line Management of Classical Hodgkin Lymphoma George Follows Cambridge University Hospitals NHS Foundation Trust george.follows@addenbrookes.nhs.uk The controversial areas Early stage non-bulky /
Treatment of Early Stage Hodgkin Lymphoma. Massimo Federico University of Modena and Reggio Emilia Città di Lecce Hospital - GVM Care & Research
 Treatment of Early Stage Hodgkin Lymphoma Massimo Federico University of Modena and Reggio Emilia Città di Lecce Hospital - GVM Care & Research Conflict of Interest Disclosure I hereby declare the following
Treatment of Early Stage Hodgkin Lymphoma Massimo Federico University of Modena and Reggio Emilia Città di Lecce Hospital - GVM Care & Research Conflict of Interest Disclosure I hereby declare the following
Hodgkin Lymphoma Review of characteristics and treatment of elderly patients
 Hodgkin Lymphoma Review of characteristics and treatment of elderly patients Boris Böll M.D. German Hodgkin Study Group (GHSG) University Hospital Cologne OS of HL patients in all stages 1960-1967 Courtesy
Hodgkin Lymphoma Review of characteristics and treatment of elderly patients Boris Böll M.D. German Hodgkin Study Group (GHSG) University Hospital Cologne OS of HL patients in all stages 1960-1967 Courtesy
Response Adapted treatment of chl using BV in first line. Massimo Federico University of Modena and Reggio Emilia Italy
 Response Adapted treatment of chl using BV in first line Massimo Federico University of Modena and Reggio Emilia Italy From the book of 18FDG-PET in BV treatment patients 1 In the beginning Seattle Genetics
Response Adapted treatment of chl using BV in first line Massimo Federico University of Modena and Reggio Emilia Italy From the book of 18FDG-PET in BV treatment patients 1 In the beginning Seattle Genetics
Interim PET Hodgkin s Disease. Fellows talk Fellow: Shweta Jain Faculty: Ajay Gopal
 Interim PET Hodgkin s Disease Fellows talk Fellow: Shweta Jain Faculty: Ajay Gopal Why is this a Question? Early Advanced ipet ABVD + RT ABVD Pos Neg ABVD Beacopp Escalation Salvage Deescalation Talk outline
Interim PET Hodgkin s Disease Fellows talk Fellow: Shweta Jain Faculty: Ajay Gopal Why is this a Question? Early Advanced ipet ABVD + RT ABVD Pos Neg ABVD Beacopp Escalation Salvage Deescalation Talk outline
Hodgkin Lymphoma Which Group of Patients benefits from the use of BEACOPP. Volker Diehl for the German Hodgkin Study Group
 Hodgkin Lymphoma Which Group of Patients benefits from the use of BEACOPP Volker Diehl for the German Hodgkin Study Group Moscow 25.October 2007 HD8 trial design CS IA, IB, IIA,B with risk factors Random
Hodgkin Lymphoma Which Group of Patients benefits from the use of BEACOPP Volker Diehl for the German Hodgkin Study Group Moscow 25.October 2007 HD8 trial design CS IA, IB, IIA,B with risk factors Random
Elderly Patients with Hodgkin s Lymphoma: FIL experience. Massimo Federico University of Modena and Reggio Emilia
 Elderly Patients with Hodgkin s Lymphoma: FIL experience Massimo Federico University of Modena and Reggio Emilia RESULTS OF VbMp CHEMOTHERAPY REGIMEN IN ELDERLY PATIENTS WITH HODGKIN DISEASE: THE GISL
Elderly Patients with Hodgkin s Lymphoma: FIL experience Massimo Federico University of Modena and Reggio Emilia RESULTS OF VbMp CHEMOTHERAPY REGIMEN IN ELDERLY PATIENTS WITH HODGKIN DISEASE: THE GISL
LYSA PET adapted programs. O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France
 LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
Hodgkin Lymphoma in Older Patients
 Hodgkin Lymphoma in Older Patients Andrew M. Evens, DO, MSc March 26 th, 2015 Professor of Medicine Chief, Division of Hematology/Oncology Director, Tufts Cancer Center Tufts Medical Center Elderly Hodgkin
Hodgkin Lymphoma in Older Patients Andrew M. Evens, DO, MSc March 26 th, 2015 Professor of Medicine Chief, Division of Hematology/Oncology Director, Tufts Cancer Center Tufts Medical Center Elderly Hodgkin
THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982)
") EORTC Lymphoma Group THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982) J. Thomas, C. Fermé, E.M. Noordijk, H. Eghbali and M. Henry-Amar 7th International
EORTC Lymphoma Group THE EORTC-GELA TREATMENT STRATEGY IN CLINICAL STAGES I-II HL Results of the H9-F and H9-U trials (#20982) J. Thomas, C. Fermé, E.M. Noordijk, H. Eghbali and M. Henry-Amar 7th International
HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary)
") HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff
HODGKIN LYMPHOMA Updated February 2016 by Dr. Manna (PGY 5 Hematology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr. Matt Cheung (Staff
Relapsed/Refractory Hodgkin Lymphoma
 Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
ROB LOWN SOUTHAMPTON HODGKIN LYMPHOMA IN THE ELDERLY
 ROB LOWN SOUTHAMPTON HODGKIN LYMPHOMA IN THE ELDERLY EPIDEMIOLOGY HODGKIN LYMPHOMA - INCIDENCE EPIDEMIOLOGY HODGKIN LYMPHOMA - MORTALITY EPIDEMIOLOGY HODGKIN LYMPHOMA - MORTALITY BY AGE NUMBER OF PEOPLE
ROB LOWN SOUTHAMPTON HODGKIN LYMPHOMA IN THE ELDERLY EPIDEMIOLOGY HODGKIN LYMPHOMA - INCIDENCE EPIDEMIOLOGY HODGKIN LYMPHOMA - MORTALITY EPIDEMIOLOGY HODGKIN LYMPHOMA - MORTALITY BY AGE NUMBER OF PEOPLE
Hodgkin. The PET World. Sally Barrington
 Hodgkin The PET World Sally Barrington PET-CT Staging in HL PET-CT changes stage 15-30% RATHL - Advanced HL 1171 pts Stage by PET-CT compared with cect and BMB 20% stage change; upstaging 14% Most upstaging
Hodgkin The PET World Sally Barrington PET-CT Staging in HL PET-CT changes stage 15-30% RATHL - Advanced HL 1171 pts Stage by PET-CT compared with cect and BMB 20% stage change; upstaging 14% Most upstaging
Practical Application of PET adapted Therapy in Hodgkin Lymphoma
 Practical Application of PET adapted Therapy in Hodgkin Lymphoma Matthew Matasar, MD Lymphoma and Adult BMT Services Director, Lymphoma Survivorship Clinic Memorial Sloan Kettering Cancer Center New York,
Practical Application of PET adapted Therapy in Hodgkin Lymphoma Matthew Matasar, MD Lymphoma and Adult BMT Services Director, Lymphoma Survivorship Clinic Memorial Sloan Kettering Cancer Center New York,
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL):
:") Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Comparison of Three Radiation Dose Levels after EBVP Regimen in Favorable Supradiaphragmatic Clinical Stages I-II Hodgkin s Lymphoma (HL): Preliminary Results of the EORTC-GELA H9-F Trial H. Eghbali, P.
Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL
 Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Hodgkin Lymphom Aktuelle Strategien und Studien Andreas Engert, MD Chairman, German Hodgkin Study Group University Hospital of Cologne
 German Hodgkin Study Group Deutsche Hodgkin Studiengruppe Hodgkin Lymphom Aktuelle Strategien und Studien Andreas Engert, MD Chairman, German Hodgkin Study Group University Hospital of Cologne Hodgkin
German Hodgkin Study Group Deutsche Hodgkin Studiengruppe Hodgkin Lymphom Aktuelle Strategien und Studien Andreas Engert, MD Chairman, German Hodgkin Study Group University Hospital of Cologne Hodgkin
Overview of Lymphoma Clinical Trials
 Overview of Lymphoma Clinical Trials Dr Pam McKay Beatson West of Scotland Cancer Centre Lymphoma Action Patient Conference September 2018 Clinical trials medical research involving human participants
Overview of Lymphoma Clinical Trials Dr Pam McKay Beatson West of Scotland Cancer Centre Lymphoma Action Patient Conference September 2018 Clinical trials medical research involving human participants
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Printed by Martina Huckova on 10/3/2011 3:04:43 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 NCCN Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform NCCN consensus. Category 2A: The recommendation
NCCN Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform NCCN consensus. Category 2A: The recommendation
Brentuximab Vedotin. Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center
 Brentuximab Vedotin Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center U.S. Cancer Statistics 2016 300.000 249.260 224.390 200.000 180.890 Incidence 100.000 95.270 76.960
Brentuximab Vedotin Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center U.S. Cancer Statistics 2016 300.000 249.260 224.390 200.000 180.890 Incidence 100.000 95.270 76.960
Advances in CD30- and PD-1-targeted therapies for classical Hodgkin lymphoma
 Wang et al. Journal of Hematology & Oncology (2018) 11:57 https://doi.org/10.1186/s13045-018-0601-9 REVIEW Advances in CD30- and PD-1-targeted therapies for classical Hodgkin lymphoma Yucai Wang 1, Grzegorz
Wang et al. Journal of Hematology & Oncology (2018) 11:57 https://doi.org/10.1186/s13045-018-0601-9 REVIEW Advances in CD30- and PD-1-targeted therapies for classical Hodgkin lymphoma Yucai Wang 1, Grzegorz
Welcome & Introductions
 Living with Hodgkin Lymphoma Welcome & Introductions Dr. Lamar s slides are available for download at www.lls.org/programs, under the program listing. 1 Living with Hodgkin Lymphoma Living with Hodgkin
Living with Hodgkin Lymphoma Welcome & Introductions Dr. Lamar s slides are available for download at www.lls.org/programs, under the program listing. 1 Living with Hodgkin Lymphoma Living with Hodgkin
Bleomycin versus Brentuximab in Hodgkin Lymphoma: Don t Hold Your Breath
 Bleomycin versus Brentuximab in Hodgkin Lymphoma: Don t Hold Your Breath Rachel Bubik, PharmD, BCPS PGY-2 Hematology/Oncology Pharmacy Resident January 8 th, 2019 2017 MFMER slide-1 Objectives 1. Explain
Bleomycin versus Brentuximab in Hodgkin Lymphoma: Don t Hold Your Breath Rachel Bubik, PharmD, BCPS PGY-2 Hematology/Oncology Pharmacy Resident January 8 th, 2019 2017 MFMER slide-1 Objectives 1. Explain
AHSCT in Hodgkin lymphoma - indication and challenges. Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital
 AHSCT in Hodgkin lymphoma - indication and challenges Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital AHSCT in Hodgkin Lymphoma The role of AHSCT in HL Mobilisation failure
AHSCT in Hodgkin lymphoma - indication and challenges Bastian von Tresckow German Hodgkin Study Group Cologne University Hospital AHSCT in Hodgkin Lymphoma The role of AHSCT in HL Mobilisation failure
First line Treatment of HL: Differential Treatment Strategies in Newly Diagnosed Patients with Early versus Advanced Stage Disease Presented
 [Editor s note: Dr. Even's video transcript has been edited to improve readability] you today about the management of Hodgkin lymphoma in 2016. Welcome to Managing Hodgkin Lymphoma. My name is Andy Evens,
[Editor s note: Dr. Even's video transcript has been edited to improve readability] you today about the management of Hodgkin lymphoma in 2016. Welcome to Managing Hodgkin Lymphoma. My name is Andy Evens,
Brentuximab Vedotin in Lymphomas
 New Drugs In Hematology Brentuximab Vedotin in Lymphomas Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 9:15-9:45 a.m U.S. Cancer Statistics 2016 300.000
New Drugs In Hematology Brentuximab Vedotin in Lymphomas Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 9:15-9:45 a.m U.S. Cancer Statistics 2016 300.000
Lymphocyte Predominant Hodgkin s Lymphoma. Case Presentation. How would you treat the patient?
 Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Lymphocyte Predominant Hodgkin s Lymphoma Wei Ai, MD, PhD Assistant Clinical Professor University of California, San Francisco January 2010 Case Presentation 32 yo male, diagnosed with stage IIIA lymphocyte
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma
 12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
Linfoma de Hodgkin. Novos medicamentos. Otavio Baiocchi CRM-SP
 Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Firenze, settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo
 Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
On behalf of the Israel Cooperative Lymphoma Group. A. Avigdor, S. Bulvik, I. Levi, E. Dann, A. Nagler, I. Ben-Bassat and A.
 Two cycles of escalated BEACOPP followed by four cycles of ABVD utilizing early-interim PET/CT scan for patients with advanced highrisk Hodgkin s lymphoma A. Avigdor, S. Bulvik, I. Levi, E. Dann, A. Nagler,
Two cycles of escalated BEACOPP followed by four cycles of ABVD utilizing early-interim PET/CT scan for patients with advanced highrisk Hodgkin s lymphoma A. Avigdor, S. Bulvik, I. Levi, E. Dann, A. Nagler,
Jonathan W Friedberg, MD, MMSc
 I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
Gruppo Italiano Terapie Innovative nei Linfomi (G.I.T.I.L.) Dr. Andrea Gallamini S.C. Ematologia Az. Ospedaliera S. Croce e Carle, Cuneo
 Dr. Andrea Gallamini S.C. Ematologia Az. Ospedaliera S. Croce e Carle, Cuneo") Sponsor Principal Investigator Protocol Coordinators Coordinating Centre Writing committee CRO Gruppo Italiano Terapie Innovative nei Linfomi (G.I.T.I.L.) Dr. Andrea Gallamini S.C. Ematologia Az. Ospedaliera
Sponsor Principal Investigator Protocol Coordinators Coordinating Centre Writing committee CRO Gruppo Italiano Terapie Innovative nei Linfomi (G.I.T.I.L.) Dr. Andrea Gallamini S.C. Ematologia Az. Ospedaliera
Role of PET in staging and treatment of lymphomas
 Role of PET in staging and treatment of lymphomas ESMO preceptorship in lymphoma Madrid, 25 November 2016 Martin Hutchings Rigshospitalet, Copenhagen, Denmark EORTC Lymphoma Group PET in lymphoma staging
Role of PET in staging and treatment of lymphomas ESMO preceptorship in lymphoma Madrid, 25 November 2016 Martin Hutchings Rigshospitalet, Copenhagen, Denmark EORTC Lymphoma Group PET in lymphoma staging
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège. 14 th post-ash meeting, January 6 th 2011, Brussels
 Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Role of PET in staging and treatment of lymphomas
 Role of PET in staging and treatment of lymphomas ESMO preceptorship in lymphoma Lugano, 3-4 November 2017 Martin Hutchings Rigshospitalet, Copenhagen, Denmark EORTC Lymphoma Group PET in lymphoma staging
Role of PET in staging and treatment of lymphomas ESMO preceptorship in lymphoma Lugano, 3-4 November 2017 Martin Hutchings Rigshospitalet, Copenhagen, Denmark EORTC Lymphoma Group PET in lymphoma staging
Post-ESMO Berne
 Post-ESMO Berne 23.10.2015 Lymphoma Update Panagiotis Samaras Department of Oncology Hemato-Oncology Center University Hospital Zurich Diffuse Large B-Cell Lymphoma (DLBCL) PCNSL Hodgkin s Lymphoma Mantle
Post-ESMO Berne 23.10.2015 Lymphoma Update Panagiotis Samaras Department of Oncology Hemato-Oncology Center University Hospital Zurich Diffuse Large B-Cell Lymphoma (DLBCL) PCNSL Hodgkin s Lymphoma Mantle
Response-adapted frontline therapy for Hodgkin lymphoma: are we there yet?
 HODGKIN LYMPHOMA: TREATMENT TODAY AND THE CHALLENGE FOR TOMORROW Response-adapted frontline therapy for Hodgkin lymphoma: are we there yet? Peter W. M. Johnson Cancer Research UK Centre, University of
HODGKIN LYMPHOMA: TREATMENT TODAY AND THE CHALLENGE FOR TOMORROW Response-adapted frontline therapy for Hodgkin lymphoma: are we there yet? Peter W. M. Johnson Cancer Research UK Centre, University of
Radiation therapy has a dramatic effect on lymphomas, and has played an important role in treating Hodgkin
 COUNTERPOINTS Current Controversies in Hematology and Oncology Can Radiotherapy Be Omitted in Patients With Localized Hodgkin Lymphoma? Radiation therapy has a dramatic effect on lymphomas, and has played
COUNTERPOINTS Current Controversies in Hematology and Oncology Can Radiotherapy Be Omitted in Patients With Localized Hodgkin Lymphoma? Radiation therapy has a dramatic effect on lymphomas, and has played
pan-canadian Oncology Drug Review Final Clinical Guidance Report Brentuximab (Adcetris) for Hodgkin Lymphoma - Resubmission February 21, 2018
 for Hodgkin Lymphoma - Resubmission February 21, 2018") pan-canadian Oncology Drug Review Final Clinical Guidance Report Brentuximab (Adcetris) for Hodgkin Lymphoma - Resubmission February 21, 2018 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Brentuximab (Adcetris) for Hodgkin Lymphoma - Resubmission February 21, 2018 DISCLAIMER Not a Substitute for Professional Advice This report
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin
 What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
Highlights of ICML 2015
 Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Lymphocyte-Depleted Classical Hodgkin s Lymphoma: A Comprehensive Analysis From the German Hodgkin Study Group
 Published Ahead of Print on September 12, 211 as 1.12/JCO.211.36.473 The latest version is at http://jco.ascopubs.org/cgi/doi/1.12/jco.211.36.473 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R
Published Ahead of Print on September 12, 211 as 1.12/JCO.211.36.473 The latest version is at http://jco.ascopubs.org/cgi/doi/1.12/jco.211.36.473 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R
PET-imaging: when can it be used to direct lymphoma treatment?
 PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
PET-imaging: when can it be used to direct lymphoma treatment? Luca Ceriani Nuclear Medicine and PET-CT centre Oncology Institute of Southern Switzerland Bellinzona Disclosure slide I declare no conflict
Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management
 HODGKIN LYMPHOMA: NEW INSIGHTS AND NEW APPROACHES Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management Dennis A. Eichenauer 1,2 and Andreas Engert 1,2 1 First Department
HODGKIN LYMPHOMA: NEW INSIGHTS AND NEW APPROACHES Nodular lymphocyte-predominant Hodgkin lymphoma: a unique disease deserving unique management Dennis A. Eichenauer 1,2 and Andreas Engert 1,2 1 First Department
Radiation and Hodgkin s Disease: A Changing Field. Sravana Chennupati Radiation Oncology PGY-2
 Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
Radiation and Hodgkin s Disease: A Changing Field Sravana Chennupati Radiation Oncology PGY-2 History of Present Illness 19 yo previously healthy male college student began having pain in his R shoulder
News from EHA. Linfomi. Maurizio Martelli Dip. Biotecnologie Cellulari ed Ematologia Sapienza Università di Roma
 News from EHA Linfomi Maurizio Martelli Dip. Biotecnologie Cellulari ed Ematologia Sapienza Università di Roma Outline HD advanced disease first line therapy : intensity of chemotherapy and PET guided
News from EHA Linfomi Maurizio Martelli Dip. Biotecnologie Cellulari ed Ematologia Sapienza Università di Roma Outline HD advanced disease first line therapy : intensity of chemotherapy and PET guided
Radiotherapy in aggressive lymphomas. Umberto Ricardi
 Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
At initial diagnosis, patients with
 Malignant Lymphomas Decision Making and Problem Solving Current treatment and immunotherapy of Hodgkin s lymphoma Beate Klimm Roland Schnell Volker Diehl Andreas Engert The treatment of Hodgkin s lymphoma
Malignant Lymphomas Decision Making and Problem Solving Current treatment and immunotherapy of Hodgkin s lymphoma Beate Klimm Roland Schnell Volker Diehl Andreas Engert The treatment of Hodgkin s lymphoma
Head and Neck: DLBCL
 Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Hodgkin Lymphoma. Barbara Pro, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Chicago, Illinois
 Hodgkin Lymphoma Barbara Pro, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Chicago, Illinois Hodgkin Lymphoma Successes and Challenges The success 80 % of patients achieve
Hodgkin Lymphoma Barbara Pro, MD Robert H. Lurie Comprehensive Cancer Center of Northwestern University Chicago, Illinois Hodgkin Lymphoma Successes and Challenges The success 80 % of patients achieve
Lymphoma update: turning biology into cures. Peter Johnson
 Lymphoma update: turning biology into cures Peter Johnson Selected highlights of recent research 1. Using FDG-PET to modify treatment and avoid long term toxicity in Hodgkin lymphoma 2. Understanding how
Lymphoma update: turning biology into cures Peter Johnson Selected highlights of recent research 1. Using FDG-PET to modify treatment and avoid long term toxicity in Hodgkin lymphoma 2. Understanding how
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA
 Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
The case against maintenance rituximab in Follicular lymphoma. Jonathan W. Friedberg M.D., M.M.Sc.
 The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
Immune checkpoint inhibitors in lymphoma. Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust
 Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
RT in Hodgkin Lymphoma
 RT in Hodgkin Lymphoma Lesser is better? Philip Poortmans, M.D. Ph.D. Radiation oncologist Tilburg, The Netherlands Radiation dose in Hodgkin Lymphoma Introduction Current evidence Guidelines 1.0 Early
RT in Hodgkin Lymphoma Lesser is better? Philip Poortmans, M.D. Ph.D. Radiation oncologist Tilburg, The Netherlands Radiation dose in Hodgkin Lymphoma Introduction Current evidence Guidelines 1.0 Early
Emerging Treatment Options for Relapsed/Refractory Hodgkin Lymphoma
 Emerging Treatment Options for Relapsed/Refractory Hodgkin Lymphoma Presented as a Live Webinar Thursday, October 26, 2017 1:00 2:00 p.m. ET On-demand Activity Live webinar recorded and archived to be
Emerging Treatment Options for Relapsed/Refractory Hodgkin Lymphoma Presented as a Live Webinar Thursday, October 26, 2017 1:00 2:00 p.m. ET On-demand Activity Live webinar recorded and archived to be
Clinical features and outcomes of 139 Japanese patients with Hodgkin lymphoma
 Original Article Clinical features and outcomes of 139 Japanese patients with Hodgkin lymphoma Authors: Shinichi Makita 1, 4, Dai Maruyama 1, Akiko Miyagi Maeshima 2, Hirokazu Taniguchi 2, Ken-ichi Miyamoto
Original Article Clinical features and outcomes of 139 Japanese patients with Hodgkin lymphoma Authors: Shinichi Makita 1, 4, Dai Maruyama 1, Akiko Miyagi Maeshima 2, Hirokazu Taniguchi 2, Ken-ichi Miyamoto
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University
 Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Treatment of Forty Adult Patients with Hodgkin Disease; Baghdad Teaching Hospital Experience
 Original Article Treatment of Forty Adult Patients with Hodgkin Disease; Baghdad Teaching * Alaadin S. Naji* Ahmed A. AL - Saffar* Mazin A. Shubbar* Bassam F. Matti* Adil Siwan* Ammar F. Majeed* Ali M.Jawad*
Original Article Treatment of Forty Adult Patients with Hodgkin Disease; Baghdad Teaching * Alaadin S. Naji* Ahmed A. AL - Saffar* Mazin A. Shubbar* Bassam F. Matti* Adil Siwan* Ammar F. Majeed* Ali M.Jawad*
Confronto Real world e studi registrativi
 Confronto Real world e studi registrativi V. Pavone San Giovanni Rotondo 8 Novembre 2018 U.O Ematologia Az.Osp.Card.G.Panico MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY
Confronto Real world e studi registrativi V. Pavone San Giovanni Rotondo 8 Novembre 2018 U.O Ematologia Az.Osp.Card.G.Panico MEDICAL NEED IN HL OUTCOME REDUCE TOXICITY IMPROVE FIRST LINE RISK-ADAPTED STRATEGY
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies. Eric H. Rubin, MD Merck Research Laboratories
 Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES!
 Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Risk, Cure and Complications in Advanced Hodgkin Disease
 Risk, Cure and Complications in Advanced Hodgkin Disease Sandra J. Horning Stanford University, Stanford, CA Current therapy for Hodgkin disease is aimed at high cure rates and optimal survivorship. Although
Risk, Cure and Complications in Advanced Hodgkin Disease Sandra J. Horning Stanford University, Stanford, CA Current therapy for Hodgkin disease is aimed at high cure rates and optimal survivorship. Although
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Overview of Lymphoma Clinical Trials
 Overview of Lymphoma Clinical Trials Dr Pam McKay Beatson West of Scotland Cancer Centre UKONS Conference November 2018 Clinical trials Medical research involving human participants Treatment related New
Overview of Lymphoma Clinical Trials Dr Pam McKay Beatson West of Scotland Cancer Centre UKONS Conference November 2018 Clinical trials Medical research involving human participants Treatment related New
Welcome and Introductions
 Update on Hodgkin Lymphoma Matthew J Matasar, MD, MS Physician, Lymphoma and Adult BMT Services Director, Lymphoma Survivorship Clinic Memorial Sloan Kettering Cancer Center New York, NY April 1, 2016
Update on Hodgkin Lymphoma Matthew J Matasar, MD, MS Physician, Lymphoma and Adult BMT Services Director, Lymphoma Survivorship Clinic Memorial Sloan Kettering Cancer Center New York, NY April 1, 2016
Treatment Approaches in Relapsed/Refractory HL. Brentuximab Vedo=n. Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center
 Treatment Approaches in Relapsed/Refractory HL Brentuximab Vedo=n Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Thursday March 15, 2018: 10:15-10:30 am 1992 (Cell): Durkop
Treatment Approaches in Relapsed/Refractory HL Brentuximab Vedo=n Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Thursday March 15, 2018: 10:15-10:30 am 1992 (Cell): Durkop
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Limited-Stage Disease: Optimal Use of Chemotherapy and Radiation Treatment
 HODGKIN LYMPHOMA: CLINICAL CHALLENGES Limited-Stage Disease: Optimal Use of Chemotherapy and Radiation Treatment John Radford 1 1 Professor of Medical Oncology, Christie Hospital and The University of
HODGKIN LYMPHOMA: CLINICAL CHALLENGES Limited-Stage Disease: Optimal Use of Chemotherapy and Radiation Treatment John Radford 1 1 Professor of Medical Oncology, Christie Hospital and The University of
The Present: Optimizing Therapy Too Much or Too Little?
 CLINICAL ADVANCES IN HODGKIN LYMPHOMA The Present: Optimizing Therapy Too Much or Too Little? Nancy L. Bartlett 1 1 Siteman Cancer Center, Washington University, St. Louis, MO Despite the use of less toxic
CLINICAL ADVANCES IN HODGKIN LYMPHOMA The Present: Optimizing Therapy Too Much or Too Little? Nancy L. Bartlett 1 1 Siteman Cancer Center, Washington University, St. Louis, MO Despite the use of less toxic
A Practical Guide to PET adapted Therapy for Hodgkin Lymphoma
 Hello. My name is Peter Johnson. I am a Professor of Medical Oncology in Southampton in the UK and I am speaking today on behalf of Managing Hodgkin Lymphoma, and particularly, I am going to talk about
Hello. My name is Peter Johnson. I am a Professor of Medical Oncology in Southampton in the UK and I am speaking today on behalf of Managing Hodgkin Lymphoma, and particularly, I am going to talk about
Hodgkin s lymphoma: Belgian Hematology Society guidelines in diagnosis, treatment and follow-up
 214 Hodgkin s lymphoma: Belgian Hematology Society guidelines in diagnosis, treatment and follow-up V. van Hende, MD1, G. Verhoef, MD, PhD2, S. Snauwaert, MD, PhD3, V. de Wilde, MD, PhD 4, B. de Prijck,
214 Hodgkin s lymphoma: Belgian Hematology Society guidelines in diagnosis, treatment and follow-up V. van Hende, MD1, G. Verhoef, MD, PhD2, S. Snauwaert, MD, PhD3, V. de Wilde, MD, PhD 4, B. de Prijck,
Alexander Fosså, M.D. PhD.
 Alexander Fosså, M.D. PhD. Current position: Senior Consultant, Department of Medical Oncology Oslo University Hospital Focus of work: - Malignant lymphoma - Chemotherapy, immunotherapy, radiotherapy -
Alexander Fosså, M.D. PhD. Current position: Senior Consultant, Department of Medical Oncology Oslo University Hospital Focus of work: - Malignant lymphoma - Chemotherapy, immunotherapy, radiotherapy -
CME Information LEARNING OBJECTIVES
 CME Information LEARNING OBJECTIVES Assess the efficacy and safety of brentuximab vedotin in investigational settings, such as in combination with AVD for patients with newly diagnosed HL, as consolidation
CME Information LEARNING OBJECTIVES Assess the efficacy and safety of brentuximab vedotin in investigational settings, such as in combination with AVD for patients with newly diagnosed HL, as consolidation
Evolving Approaches to Primary Treatment of Hodgkin Lymphoma
 Evolving Approaches to Primary Treatment of Hodgkin Lymphoma Joseph M. Connors Two challenges confront the clinician treating Hodgkin lymphoma today: achieving a high level of effectiveness while minimizing
Evolving Approaches to Primary Treatment of Hodgkin Lymphoma Joseph M. Connors Two challenges confront the clinician treating Hodgkin lymphoma today: achieving a high level of effectiveness while minimizing
Serum levels of soluble CD30 improve International Prognostic Score in predicting the outcome of advanced Hodgkin s lymphoma
 Original article Annals of Oncology 13: 1908 1914, 2002 DOI: 10.1093/annonc/mdf333 Serum levels of soluble CD30 improve International Prognostic Score in predicting the outcome of advanced Hodgkin s lymphoma
Original article Annals of Oncology 13: 1908 1914, 2002 DOI: 10.1093/annonc/mdf333 Serum levels of soluble CD30 improve International Prognostic Score in predicting the outcome of advanced Hodgkin s lymphoma
Guidelines for the first line management of classical Hodgkin lymphoma
 guideline Guidelines for the first line management of classical Hodgkin lymphoma George A. Follows, 1 Kirit M. Ardeshna, 2 Sally F. Barrington, 3 Dominic J. Culligan, 4 Peter J. Hoskin, 5 David Linch,
guideline Guidelines for the first line management of classical Hodgkin lymphoma George A. Follows, 1 Kirit M. Ardeshna, 2 Sally F. Barrington, 3 Dominic J. Culligan, 4 Peter J. Hoskin, 5 David Linch,
XVIII. Management of nodular lymphocyte predominant Hodgkin lymphoma
 Hematological Oncology Hematol Oncol 2015; 33: 90 95 Published online in Wiley Online Library (wileyonlinelibrary.com).2226 Supplement Article XVIII. Management of nodular lymphocyte predominant Hodgkin
Hematological Oncology Hematol Oncol 2015; 33: 90 95 Published online in Wiley Online Library (wileyonlinelibrary.com).2226 Supplement Article XVIII. Management of nodular lymphocyte predominant Hodgkin
Non-Hodgkin s and Hodgkin lymphoma: using disease characteristics as a guide to treatment selection. Arnold Freedman, M.D.
 2017 Master Class for Oncologists Non-Hodgkin s and Hodgkin lymphoma: using disease characteristics as a guide to treatment selection Arnold Freedman, M.D. 2018 Master Class Course Disclosure Disclosure
2017 Master Class for Oncologists Non-Hodgkin s and Hodgkin lymphoma: using disease characteristics as a guide to treatment selection Arnold Freedman, M.D. 2018 Master Class Course Disclosure Disclosure
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Disclosures for Dr. Peter Borchmann 48 th ASH Annual meeting, Orlando, Florida
 Phase II Study of Pixantrone in Combination with Cyclophosphamide, Vincristine, and Prednisone (CPOP) in Patients with Relapsed Aggressive Non-Hodgkin s Lymphoma P Borchmann Universitaet de Koeln, Koeln,
Phase II Study of Pixantrone in Combination with Cyclophosphamide, Vincristine, and Prednisone (CPOP) in Patients with Relapsed Aggressive Non-Hodgkin s Lymphoma P Borchmann Universitaet de Koeln, Koeln,
MMAE disrupts cell division and triggers apoptosis. Pola binds to cell surface antigen CD79b. Pola is internalized; linker cleaves, releasing MMAE
 Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
La TEP dans le lymphome Impacts cliniques en Olivier Casasnovas Hématologie Clinique CHU Dijon
 La TEP dans le lymphome Impacts cliniques en 2017 Olivier Casasnovas Hématologie Clinique CHU Dijon Incidence and Anatomic Regions Detected by FDG PET Relation to Histologic Types According to World Health
La TEP dans le lymphome Impacts cliniques en 2017 Olivier Casasnovas Hématologie Clinique CHU Dijon Incidence and Anatomic Regions Detected by FDG PET Relation to Histologic Types According to World Health
NIH Public Access Author Manuscript Expert Opin Pharmacother. Author manuscript; available in PMC 2011 December 1.
 NIH Public Access Author Manuscript Published in final edited form as: Expert Opin Pharmacother. 2010 December ; 11(17): 2891 2906. doi:10.1517/14656566.2010.515979. Hodgkin s Lymphoma Therapy: Past, Present,
NIH Public Access Author Manuscript Published in final edited form as: Expert Opin Pharmacother. 2010 December ; 11(17): 2891 2906. doi:10.1517/14656566.2010.515979. Hodgkin s Lymphoma Therapy: Past, Present,
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
What is the best approach to the initial therapy of PTCL? standards of treatment? Should all
 What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
CME Information. histone deacetylase inhibition in patients with peripheral T-cell or NK/ T-cell lymphoma.
 CME Information LEARNING OBJECTIVES Appraise recent clinical research findings on the use of PET scans after initial chemotherapy to identify patients with early-stage Hodgkin lymphoma who can avoid additional
CME Information LEARNING OBJECTIVES Appraise recent clinical research findings on the use of PET scans after initial chemotherapy to identify patients with early-stage Hodgkin lymphoma who can avoid additional